")
Back to Journals » OncoTargets and Therapy » Volume 14
A Rare Case of Primary Signet-Ring Cell Cervical Carcinoma: Early Stage with Independent Bilateral Ovarian Metastases
Authors Li S, Gan F, Luo M, Luo P
Received 6 January 2021
Accepted for publication 24 February 2021
Published 23 March 2021 Volume 2021:14 Pages 2101—2107
DOI https://doi.org/10.2147/OTT.S300424
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alberto Bongiovanni
Shiyun Li, Fuqiang Gan, Manling Luo, Puying Luo
Department of Gynecology, Jiangxi Provincial People’s Hospital Affiliated to Nanchang University, Nanchang, Jiangxi, People’s Republic of China
Correspondence: Puying Luo
Department of Gynecology, Jiangxi Provincial People’s Hospital Affiliated to Nanchang University, No. 152, Aiguo Road, Donghu District, Nanchang, Jiangxi, 330006, People’s Republic of China
Tel/Fax +86-0791-86897371
Email [email protected]
Background: Primary signet-ring cell carcinoma of the uterine cervix (PSRCCC) is defined as a mucinous carcinoma. PSRCCC with independent bilateral ovarian metastases has not been previously reported in the literature.
Case Presentation: Herein we describe a case of PSRCCC with ovarian involvement. The patient underwent a detailed complete physical examination, and surgery was then performed to resect all of the tumors. All tumors expressed human papillomavirus 18 no distant tumors were detected, and estrogen receptor and progesterone receptor testing were negative, suggesting that the cervix was the primary site.
Conclusion: This is the first report of a case of PSRCCC metastasis to bilateral ovaries only. Conservative management of human papillomavirus-associated type endocervical adenocarcinomas with independent ovarian metastases should be considered.
Keywords: conservative management, transtubal spread
Introduction
Cervical adenocarcinoma accounts for approximately 25% of all cancers of the cervix cancer.1 The International Endocervical Adenocarcinoma Criteria and Classification categorizes endocervical adenocarcinomas (ECAs) on the basis of morphologic features linked to etiology (ie, human papilloma virus [HPV] infection), resulting in separation of ECAs into HPV-associated (HPVA) and non-HPV-associated (NHPVA) types.2 Signet-ring cell carcinoma is a mucinous adenocarcinoma, and <9% of signet-ring cell carcinomas are of the HPVA type.2 To date, less than 26 cases of primary signet-ring cell carcinoma of the uterine cervix(PSRCCC) have been reported. Herein, we describe a case of PSRCCC with independent bilateral ovarian metastases which have not been reported previously in the literature. Probable pathways and new strategies for the clinical management of ovarian metastasis from HPVA type endocervical adenocarcinomas are also briefly reviewed.
Case Presentation
The patient was a 35-year-old Chinese woman, gravida 5, para 2, who was admitted to our hospital in August 2019 with postcoital vaginal bleeding that had been present for the last 3 months. Gynecologic examination revealed that the whole cervix was enlarged and exhibited a 1.5 cm reddish exophytic mass, and colposcopy depicted an atypical blood vessel image suggestive of adenocarcinoma (Figure 1A). The vaginal mucosa was intact, the size of the uterus body was normal, and a large pelvic mass was present. Cervical pathology was obtained in August 2019, revealed a poorly differentiated adenocarcinoma with a signet-ring cell pattern (Figure 1B).
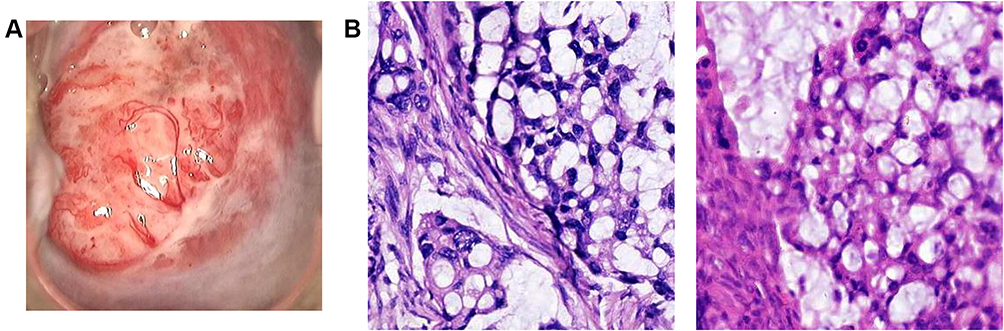 |
Figure 1 Primary signet-ring cell carcinoma of the uterine cervix in the biopsy. (A) Colposcope image of the cervical mass. (B) Histopathological findings of the cervical (left) and ovarian (right) lesion (hematoxylin and eosin stain, ×200 magnification). |
The results of bilateral breast examination and plain computed tomography of the thorax were within normal limits. Upper gastrointestinal system endoscopy and colonoscopy were performed, but no primary tumor site was detected. Plain and enhanced computed tomography and magnetic resonance imaging of the abdomen depicted an adnexal mass on the right side and a cervical mass (Figure 2A). Laboratory tests revealed high carcinoembryonic antigen (83.37 ng/mL) and Ca19-9 (816.7 U/mL) levels. DNA extracted from selected cervical tissues revealed the presence of type 18 HPV.
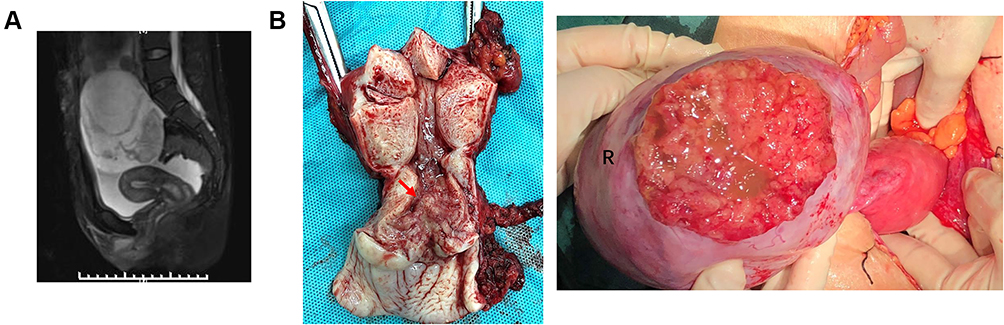 |
Figure 2 Ovarian involvement associated with the cervical adenocarcinomatous lesion. (A) Computed tomography depicting the pelvic lesion with a solid-cystic appearance. (B) The cervix and right ovary during surgery. |
The patient was managed for the International Federation of Gynecology and Obstetrics 2018 classification stage IB2 cervical cancer. She underwent radical surgery in August 2019 with extensive total hysterectomy, bilateral salpingo-oophorectomy, omentectomy, appendectomy and pelvic and para-aortic lymphadenectomies. Intraoperative abdominal examination revealed bilateral masses in the ovaries approximately 12 cm × 10 cm × 5 cm on the right side and 4 cm × 3 cm × 3 cm on the left side (Figure 2B). Histopathology revealed lymphovascular space involvement, no tumor involvement space, parametrium, fallopian tube, and the para-aortic and pelvic lymph nodes. The ovarian masses were brittle, ulcerated, filled with light-yellow-colored mucus, and exhibited clear boundaries and mobility. An invasive growth of approximately 3.0 cm × 2.5 cm × 1.0 c m was evident approximately 2.5 cm outside the cervical mouth (Figure 2B). The histopathological and immunohistochemical patterns of the glandular lesions of the cervix and the ovary were identical (Figure 1B), with immunohistochemical positivity for CK7, p16, carcinoembryonic antigen, Ki-67 and D2-40 and immunohistochemical negativity for estrogen receptor, progesterone receptor (ER/PR) (Figure 3A), alpha-fetoprotein, p53. Polymerase chain reaction analysis of ovarian tissue detected HPV18 gene fragments (Figure 3B).In September 2019, positron emission tomography/computed tomography conducted approximately depicted no increase in fluorodeoxyglucose uptake. The patient received four cycles of platinum plus paclitaxel and whole pelvic radiotherapy with DT46Gy/23FX from September 2019 to January 2020 and achieved a stable response (SD). No tumor site was detected in plain and enhanced computed tomography and magnetic resonance imaging of the abdomen in January 2021.
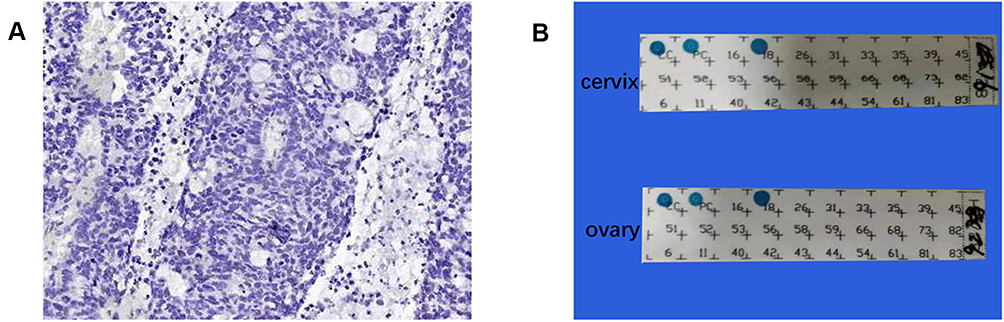 |
Figure 3 Immunohistochemical staining and polymerase chain reaction results of the cervical lesion. (A) Tumor cell nuclei were negative for estrogen receptor. (B) The presence of human type 18 papillomavirus in cervical and ovarian tissue. |
The patient whose case is described in this report has provided written informed consent for its publication. Institutional approval for publication is not applicable to the report.
Discussion
Only 25 previously reported cases of PSRCCC were located during the compilation of the current report (Table 1). In some of those reports, the origin of the primary tumor was not verified. Hitherto, no cases of PSRCCC with independent bilateral ovarian metastases have been reported. The key characteristics of PSRCCC with ovarian involvement are shown in Table 2. The prevalence of ovarian metastasis of adenocarcinomas ranged from 5.5% to-12.5%, compared with 0.0% to 1.3% for squamous cell carcinoma.3 The presence of identical HPV types in ovarian and endocervical tumors has been cited as evidence of the cervical origin of those tumors.4 In the present, the HPV18 expression, apparent lack of distant tumors finds and ER and PR negativity supported the conclusion that the cervix was the primary site.5,6
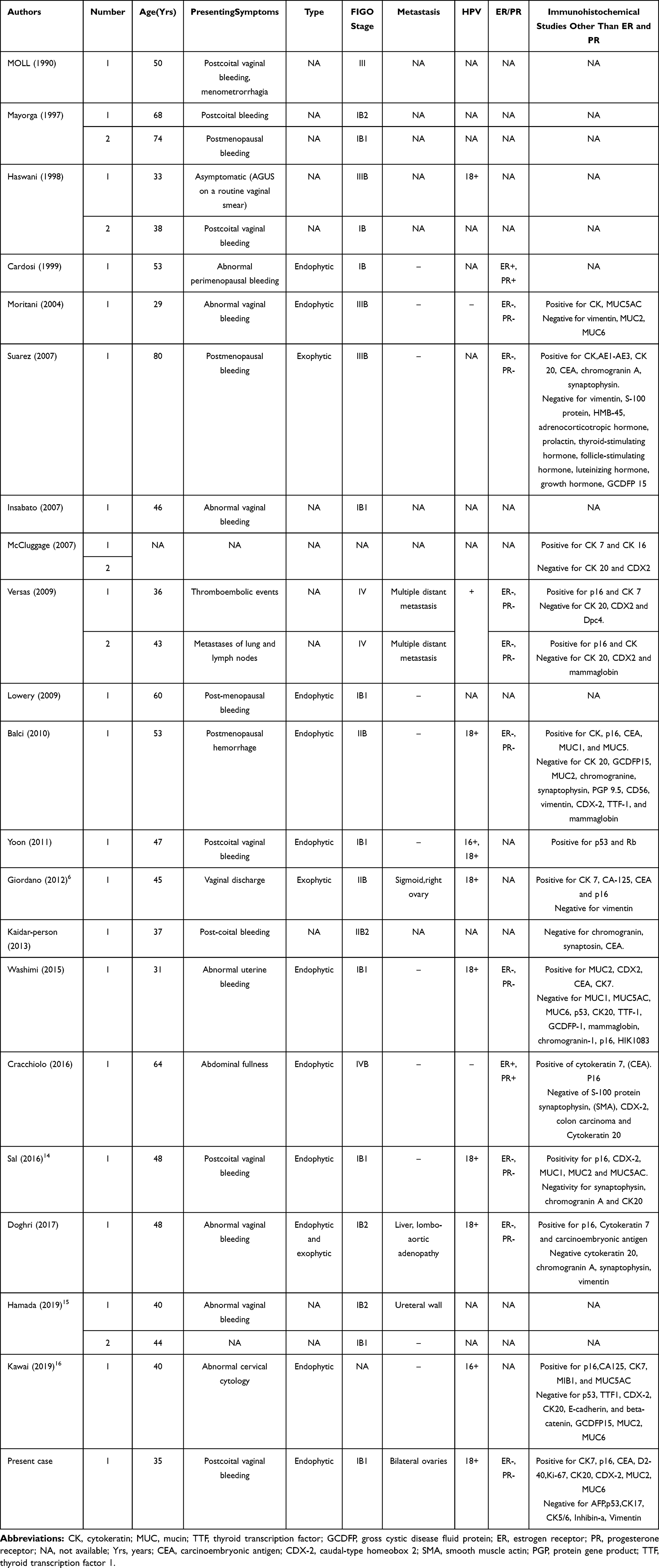 |
Table 1 Summary of Cases of Primary Signet-Ring Cell Carcinoma of the Cervix, Modified from Giordano, Sal, Hamada et al |
 |
Table 2 Key Points of Primary Signet-Ring Cell Carcinoma of the Uterine Cervix (PSRCCC) with Ovarian Involvement |
After perusing the relevant research, we concluded that there are at least four possible pathways for the spread of cervical carcinoma to the ovary. One is via lymphatic/vascular channels, another is intraepithelial spread via fallopian tube epithelium, a third is transcoelomic spread between peritoneal surfaces, and a fourth is tumor cell exfoliation and transtubal spread.7,8 In the current case, the cervical adenocarcinoma exceeds 1 cm, no tumor cells were detected in the corpus uteri or fallopian tubes via pathological examination, and no distant neoplasm invasiveness was detected via positron emission tomography. We suggest that the probable route was tumor cell exfoliation and transtubal spread, and that exfoliated cervical adenocarcinoma cells may have travelled along the fallopian tubes into the peritoneal cavity.
It is not unequivocally clear why in the current case tumors only metastasized to the ovary. The theory of “seed and soil” is rooted in the contention that “when a plant goes to seed, its seeds are carried in all directions, but they can only live and grow if they fall on congenial soil”.9 Ovulatory cycles and a rich blood supply result in the ovaries forming an inflammatory microenvironment that is potentially conducive to tumor growth.8 Vascular space and pelvic lymph nodes are benign, reducing the possibility of vascular metastasis and lymph node metastasis. We speculate that in this context, exfoliative tumor cells only propagate in “congenial soil” – the ovaries – because they are indolent. The fact that ovarian metastasis is more common in younger women supports this view.10 Indolent metastases are typically early-stage, unifocal, intraparenchymal, exhibit independent growth within the ovary in the absence of diseases at other sites, and often exceed the size of at the primary site.8 All of those characteristics were evident in the current case, thus we surmise that the indolent cells selectively propagated in the ovaries.
Mounting evidence suggests that transtubal spread is typically limited to the ovaries and associated with a relatively favorable prognosis.8,11,12 In 29 cases with documented follow-up, all 12 patients with single-site ovarian metastasis were alive at the end of follow-up.13 In the present case, an ovarian mass was full of pale-yellow mucus and there was a 5-cm ulceration on the right side. Unexpectedly no tumor cells were detected via cytological examinations of peritoneal wash fluid after surgery, and no intraperitoneal spread was evident after 12 months. This suggests relative indolence compared with primary ovarian cancer. The patient did opt to undergo chemotherapy, but observation only would have been another option. In case of HPVA ECAs with independent ovarian metastases, conservative management should be considered.
Conclusions
This report describes the first published case of PSRCCC metastasis to bilateral ovaries only. Conservative management should be considered in cases of HPVA ECAs with independent ovarian metastases.
Abbreviations
IECC, The International Endocervical Adenocarcinoma Criteria and Classification; ECAs, endocervical adenocarcinomas; ER, Estrogen Receptor; PR, Progesterone Receptor; HPV, human papilloma virus; HPVA, human papilloma virus-associated; NHPVA, human papilloma virus-unassociated or non-human papilloma virus-associated; PSRCCC, primary signet-ring cell carcinoma of the uterine cervix; FIGO, International Federation of Gynecology and Obstetrics classification.
Ethics Approval and Consent to Participate
This case report does not involve human trials, so institutional approval for publication is not applicable. The patient whose case is described in this report has provided written informed consent for its publication.
Consent for Publication
The patient provided informed consent for the anonymous publication of data.
Acknowledgments
This research was supported by the Administration of Traditional Chinese Medicine of Jiangxi Province, China (grants No:2020A0177) and the Health Commission of Jiangxi Province, China (grants No:202110004).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Cohen PA, Jhingran A, Oaknin A, et al. Cervical cancer. Lancet (London, England). 2019;393:169–182. doi:10.1016/S0140-6736(18)32470-X
2. Stolnicu S, Hoang L, Chiu D, et al. Clinical outcomes of HPV-associated and unassociated endocervical adenocarcinomas categorized by the International Endocervical Adenocarcinoma Criteria and Classification (IECC). Am J Surg Pathol. 2019;43:466–474. doi:10.1097/PAS.0000000000001224
3. Chen J, Wang R, Zhang B, et al. Safety of ovarian preservation in women with stage I and II cervical adenocarcinoma: a retrospective study and meta-analysis. Am J Obstet Gynecol. 2016;215:
4. Veras E, Srodon M, Neijstrom ES, et al. Metastatic HPV-related cervical adenocarcinomas presenting with thromboembolic events (Trousseau Syndrome): clinicopathologic characteristics of 2 cases. Int J Gynecol Pathol. 2009;28:134–139. doi:10.1097/PGP.0b013e318186a83b
5. Arfi A, Hequet D, Bataillon G, et al. HPV DNA integration site as proof of the origin of ovarian metastasis from endocervical adenocarcinoma: three case reports. BMC Cancer. 2019;19:375. doi:10.1186/s12885-019-5582-8
6. Giordano G, Pizzi S, Berretta R, et al. A new case of primary signet-ring cell carcinoma of the cervix with prominent endometrial and myometrial involvement: immunohistochemical and molecular studies and review of the literature. World J Surg Oncol. 2012;10:7. doi:10.1186/1477-7819-10-7
7. Horn LC, Höhn AK, Stark S, et al. Endocervical adenocarcinoma in situ (AIS) with ovarian and pulmonary involvement: report of a case and review of the literature suggesting a “seed and soil hypothesis”. J Cancer Res Clin Oncol. 2019;145:2061–2069. doi:10.1007/s00432-019-02966-4
8. Casey L, Singh N. Metastases to the ovary arising from endometrial, cervical and fallopian tube cancer: recent advances. Histopathology. 2020;76:37–51. doi:10.1111/his.13985
9. Virchow R. Cellular pathology. As based upon physiological and pathological histology. Lecture XVI–Atheromatous affection of arteries. 1858. Nutr Rev. 1989;47:23–25. doi:10.1111/j.1753-4887.1989.tb02747.x
10. Zhou L, Sun CT, Lin L, et al. Independent risk factors for ovarian metastases in stage IA-IIB cervical carcinoma. Acta Obstet Gynecol Scand. 2019;98:18–23. doi:10.1111/aogs.13442
11. Chang MC, Nevadunsky NS, Viswanathan AN, et al. Endocervical adenocarcinoma in situ with ovarian metastases: a unique variant with potential for long-term survival. Int J Gynecol Pathol. 2010;29:88–92. doi:10.1097/PGP.0b013e3181acefbf
12. Abozina A, Singh N, Blake C. Transtubal spread of a superficially invasive cervical adenocarcinoma to the ovaries after 11 years. Int J Gynecol Pathol. 2020;39:296–300. doi:10.1097/PGP.0000000000000603
13. Ronnett BM, Yemelyanova AV, Vang R, et al. Endocervical adenocarcinomas with ovarian metastases: analysis of 29 cases with emphasis on minimally invasive cervical tumors and the ability of the metastases to simulate primary ovarian neoplasms. Am J Surg Pathol. 2008;32:1835–1853. doi:10.1097/PAS.0b013e3181758831
14. Sal V, Kahramanoglu I, Turan H, et al. Primary signet ring cell carcinoma of the cervix: a case report and review of the literature. Int J Surg Case Rep. 2016;21:1–5. doi:10.1016/j.ijscr.2016.02.007
15. Hamada K, Baba T, Takaori A, et al. Primary signet ring cell carcinoma of uterine cervix and related disease: two case reports and a review. Int Cancer Conf J. 2019;8:157–163. doi:10.1007/s13691-019-00375-5
16. Kawai S, Torii Y, Kukimoto I, et al. A case of primary signet-ring cell carcinoma of the cervix containing full genome of human papillomavirus 16. Indian J Pathol Microbiol. 2019;62:146–148. doi:10.4103/IJPM.IJPM_507_17
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.