Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
A Random Forest–Based Risk Prediction Model for Non-Response to Methylphenidate in Children with Attention Deficit Hyperactivity Disorder
Authors Lei Y, Li F, Xiao L, Lei C, Tang Y, Zou D
Received 23 April 2026
Accepted for publication 19 June 2026
Published 9 July 2026 Volume 2026:22 617475
DOI https://doi.org/10.2147/NDT.S617475
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jun Chen
Yuan Lei,1 Fang Li,1 Linyan Xiao,2 Chaolan Lei,1 Yunli Tang,1 Deng Zou1
1Department of Pediatrics, The Fourth Hospital of Changsha (Integrated Traditional Chinese and Western Medicine Hospital of Changsha, Changsha Hospital of Hunan Normal University), Changsha, Hunan, 410219, People’s Republic of China; 2Child Development and Behavior Center, Liuyang Maternal and Child Health Hospital, Changsha, Hunan, 410300, People’s Republic of China
Correspondence: Deng Zou, Department of Pediatrics, The Fourth Hospital of Changsha (Integrated Traditional Chinese and Western Medicine Hospital of Changsha, Changsha Hospital of Hunan Normal University), No. 200, Section 4 Jinxing North Road, Wangcheng District, Changsha, Hunan, 410219, People’s Republic of China, Email [email protected]
Objective: To develop and validate a prediction model based on the random forest algorithm to assess the risk of non-response to methylphenidate (MPH) in children with attention deficit hyperactivity disorder (ADHD), thereby providing decision support for individualized clinical treatment.
Methods: A total of 150 children with ADHD who received MPH treatment were prospectively and consecutively enrolled. Based on changes in the Swanson, Nolan, and Pelham Rating Scale, Fourth Edition (SNAP-IV) scores after 3 months of treatment, patients were classified into a treatment response group (n = 116) and a non-response group (n = 34). Differences in clinical characteristics, pre-treatment clinical assessment scales, and laboratory parameters were compared. A random forest algorithm was used to construct the prediction model. Feature importance was evaluated based on the decrease in node impurity.
Results: Serum 25-hydroxyvitamin D [25(OH)D], cortisol, S100β protein, brain-derived neurotrophic factor (BDNF), and urinary catecholamines were lower in the treatment non-response group. The combined subtype of ADHD, higher SNAP-IV total score, lower 25(OH)D levels, and lower dopamine levels were independent risk factors for non-response. In the random forest model, SNAP-IV score had the highest feature importance. The model, incorporating clinical characteristics, pre-treatment clinical assessment scales, and laboratory indicators, demonstrated excellent predictive performance in the test set (AUC=0.883; 95% confidence interval: 0.811– 0.956) and an overall accuracy of 86.67%.
Conclusion: The random forest–based prediction model can accurately identify children with ADHD who are unlikely to respond to MPH treatment.
Keywords: methylphenidate, attention deficit hyperactivity disorder, random forest, treatment response, prediction model
Introduction
Attention deficit hyperactivity disorder (ADHD), a neurodevelopmental disorder featured by inattention and impulsivity,1 has a global prevalence of approximately 5%–7% among children.2 This disorder impairs academic performance, social functioning, and family dynamics in affected children. Moreover, its impact often persists into adulthood, imposing substantial burdens on individuals, families, and society.3
Methylphenidate (MPH), a first-line central nervous system stimulant, effectively alleviates core symptoms in most children with ADHD and is recommended as a cornerstone treatment in both domestic and international clinical guidelines.4,5 However, considerable interindividual variability in treatment response has been observed in clinical practice. Approximately 20%–30% of children show a poor response to initial standard treatment and are considered non-responders.6,7 These patients not only fail to benefit from therapy but may also experience unnecessary adverse drug effects, delays in receiving effective interventions, and increased psychological and financial burdens on their families due to repeated treatment failures. Therefore, early and accurate identification, prior to treatment initiation, of children at high risk of non-response to MPH represents a critical clinical challenge for achieving individualized precision medicine and optimizing initial treatment strategies in ADHD.
Current studies on predicting MPH treatment response have primarily focused on single or limited dimensions, such as clinical subtypes, symptom severity, or selected neuropsychological features.8,9 While these studies provide insights into variability in treatment outcomes, their predictive performance remains limited. Moreover, most rely on traditional linear statistical approaches, which are insufficient to fully capture the complex, nonlinear interactions underlying disease characteristics and treatment response. In recent years, emerging evidence has explored associations between serum biomarkers and ADHD symptoms or treatment outcomes.10 However, studies integrating such biomarkers with multidimensional clinical indicators into predictive models remain scarce.
Machine learning algorithms, particularly random forest, have demonstrated advantages in handling high-dimensional data, capturing complex interactions, and mitigating overfitting, and have shown promise in prognostic prediction within psychiatry.11 As an ensemble learning approach, random forest constructs multiple decision trees and aggregates their predictions, allowing it to effectively model nonlinear relationships and interactions among heterogeneous predictors. Furthermore, it can rank variable importance, thereby facilitating the identification of clinically relevant factors. However, compared with conventional regression models, random forest may provide less intuitive interpretation of the effects of individual variables.
Several studies have explored machine learning approaches for predicting treatment outcomes in ADHD. Kim et al12 demonstrated that machine learning models integrating demographic, neuropsychological, environmental, and biological features could distinguish responders from non-responders to methylphenidate treatment. More recently, Chen et al13 reported that machine learning models incorporating neuroimaging radiomic features achieved promising performance in predicting methylphenidate treatment response. These findings support the feasibility of applying machine learning techniques to individualized treatment prediction in ADHD. However, most existing studies have relied on neuroimaging data or a limited range of predictors, and few have comprehensively integrated routine clinical characteristics, multidimensional assessment scales, and laboratory biomarkers into a unified prediction framework. Therefore, the application of random forest models for predicting MPH response in children with ADHD remains relatively limited and warrants further investigation.
Accordingly, the present study aims to develop a comprehensive prediction model based on the random forest algorithm by integrating demographic characteristics, clinical subtypes, comorbidities, multidimensional pre-treatment assessment scales, and relevant laboratory indicators. We hypothesized that this model could more accurately predict the risk of non-response to MPH in children with ADHD, thereby assisting clinicians in pre-treatment risk stratification.
Materials and Methods
Study Design
This single-center, prospective observational cohort study was designed to explore risk factors for non-response to MPH in children with ADHD and to construct a predictive model. The study protocol was approved by the institutional ethics review board of The Fourth Hospital of Changsha (Integrated Traditional Chinese and Western Medicine Hospital of Changsha, Changsha Hospital of Hunan Normal University) (No. CSSDSYY-YXLL-SC-2024-03-14). Written informed consent was obtained from the legal guardians of all child participants, and verbal assent was obtained from the children themselves after a full explanation of the study procedures in age-appropriate language, prior to study commencement. This study was conducted in accordance with the principles of the Declaration of Helsinki.14 All data were anonymized to protect patient privacy.
Study Population
Children with ADHD who were newly diagnosed at our hospital and scheduled to initiate MPH treatment between March 2024 and November 2025 were prospectively and consecutively enrolled. All participants completed baseline assessments prior to treatment and were followed for at least 3 months. The final follow-up was completed in February 2026.
Inclusion criteria: (1) diagnosis of ADHD according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5);15 (2) age 6–14 years; (3) first-time treatment with extended-release MPH; (4) no contraindications to MPH treatment, including but not limited to cardiovascular disease, hypertension, or other medical conditions that could be exacerbated by MPH; (5) no history of neurological disorders or other severe systemic diseases; and (6) complete clinical data available.
Exclusion criteria: (1) presence of severe systemic diseases, intellectual disability, pervasive developmental disorders, schizophrenia, or other severe psychiatric disorders; (2) prior pharmacological treatment for ADHD; and (3) substantial missing data.
Clinical Data Collection
Baseline data were prospectively collected using standardized case report forms, with selected demographic information verified through the hospital electronic medical record system. Collected clinical characteristics included age, sex, body mass index (BMI), family history, mode of delivery, ADHD clinical subtype, disease duration, and comorbidities (language disorders and specific learning disorders).
For clinical assessment scales, the SNAP-IV, Conners Rating Scale (parent version), Chinese Wechsler Intelligence Scale for Children (C-WISC), and Weiss Functional Impairment Rating Scale–Parent Report (WFIRS-P) were utilized:
SNAP-IV was used to quantitatively assess the severity of core ADHD symptoms.16 A 4-point Likert scale (0–3) was applied (“not at all” = 0, “just a little” = 1, “quite a lot” = 2, “very much” = 3). The mean item scores for the inattention subscale (items 1–9) and hyperactivity/impulsivity subscale (items 10–18) were calculated by dividing the total score by the number of items. Higher scores indicate greater symptom severity.
Conners Parent Symptom Questionnaire (PSQ) was used to comprehensively assess a wide range of behavioral problems associated with ADHD.17 The questionnaire was completed by parents using a 4-point Likert scale (0–3), with scores calculated as the mean item score (total score divided by number of items). Higher scores indicate greater severity.
C-WISC18 includes four core indices, Verbal Comprehension, Perceptual Reasoning, Working Memory, and Processing Speed, and integrates 10 core subtests to comprehensively assess overall cognitive ability. Higher scores indicate better cognitive function.
WFIRS-P was used to objectively evaluate the extent of functional impairment in daily life caused by ADHD symptoms.19 A 4-point Likert scale (0–3) was applied, and scores were calculated as the mean item score. Higher scores indicate greater impairment.
Laboratory Measurements
For detection of serum biomarkers, 5 mL of fasting venous blood was collected from the antecubital vein in the morning prior to treatment. After standing, samples were centrifuged at 3000 r/min for 10 minutes to separate serum, which was aliquoted and stored at −80°C. Serum levels of 25(OH)D, cortisol, S100 calcium-binding protein β (S100β), prolactin (PRL), 5-hydroxytryptamine (5-HT), and brain-derived neurotrophic factor (BDNF) were measured using ELISA kits (Enzyme-linked Biotechnology, Shanghai, China). Measurements were conducted using a BioTek ELx800 fully automated microplate reader (BioTek Instruments, Inc., Winooski, VT, USA).
Participants were instructed to collect 24-hour urine samples prior to treatment. Collection containers were preloaded with 30 g of sodium dihydrogen citrate (10 g/L) as a preservative. Samples were stored at 4°C and protected from light during collection. After completion, total urine volume was recorded, the sample was thoroughly mixed, and 5 mL was collected for analysis. Concentrations of norepinephrine (NE) and dopamine in urine were measured using high-performance liquid chromatography–tandem mass spectrometry (HPLC–MS/MS).
All measurements were performed in triplicate for each sample, and the mean value was used as the final result. Analytical precision was assessed by calculating intra-assay and inter-assay coefficients of variation (CV). The intra-assay CV was calculated based on three replicate measurements of the same sample within a single plate using the formula: CV (%) = (standard deviation / mean) × 100%. Laboratory personnel were blinded to patients’ clinical information and group allocation.
Definition of Treatment Response and Grouping
Treatment efficacy was evaluated after 3 months of MPH therapy. Response was defined based on strict symptom remission criteria using the SNAP-IV core symptom items (items 1–18) assessed at 3 months. The treatment response group (remission) was defined as having a mean item score ≤1 across items 1–18, with all individual item scores ≤1 (ie., no longer meeting DSM-5 diagnostic criteria for ADHD).15 The non-response group included those who did not meet these criteria. This grouping served as the primary outcome variable.
A single-blind design was applied. All participants returned for follow-up after 3 months of MPH treatment, and treatment efficacy was independently evaluated by a researcher blinded to baseline clinical characteristics. Group assignment was strictly based on SNAP-IV scoring.
Statistical Analysis
Data analysis was performed using R software (version 4.5.1) and SPSS software (version 27.0; IBM Corp., Armonk, NY, USA). Continuous variables were expressed as mean ± standard deviation and compared using the independent samples t-test. Categorical variables were presented as frequencies (percentages) and compared using the chi-square test. Variables with P < 0.05 in univariate analysis were included in multivariable logistic regression to identify independent predictors. A random forest algorithm was used to construct the prediction model. Bootstrap resampling was applied to generate the training set, and 500 decision trees were built. At each node split, the number of randomly selected features was set to the square root of the total number of features. Out-of-bag error was used for internal validation of model performance. Feature importance was assessed based on the decrease in node impurity (Gini index). Model performance in the test set was comprehensively evaluated using the area under the receiver operating characteristic curve (AUC), calibration curves, Brier score, and decision curve analysis (DCA). All statistical tests were two-sided, and P < 0.05 was considered statistically significant.
Results
Comparison of Clinical Characteristics
A total of 150 children with ADHD were included in this study. According to the SNAP-IV assessment after 3 months of MPH treatment (Table 1), 116 patients were classified into the response group and 34 into the non-response group. There were no significant differences between the groups in age, sex, BMI, disease duration, family history, mode of delivery, or the presence of language disorders (all P > 0.05). However, the proportion of comorbid specific learning disorders was significantly higher in the non-response group than in the response group (P = 0.041). In addition, the distribution of ADHD subtypes differed significantly between the two groups (P = 0.007).
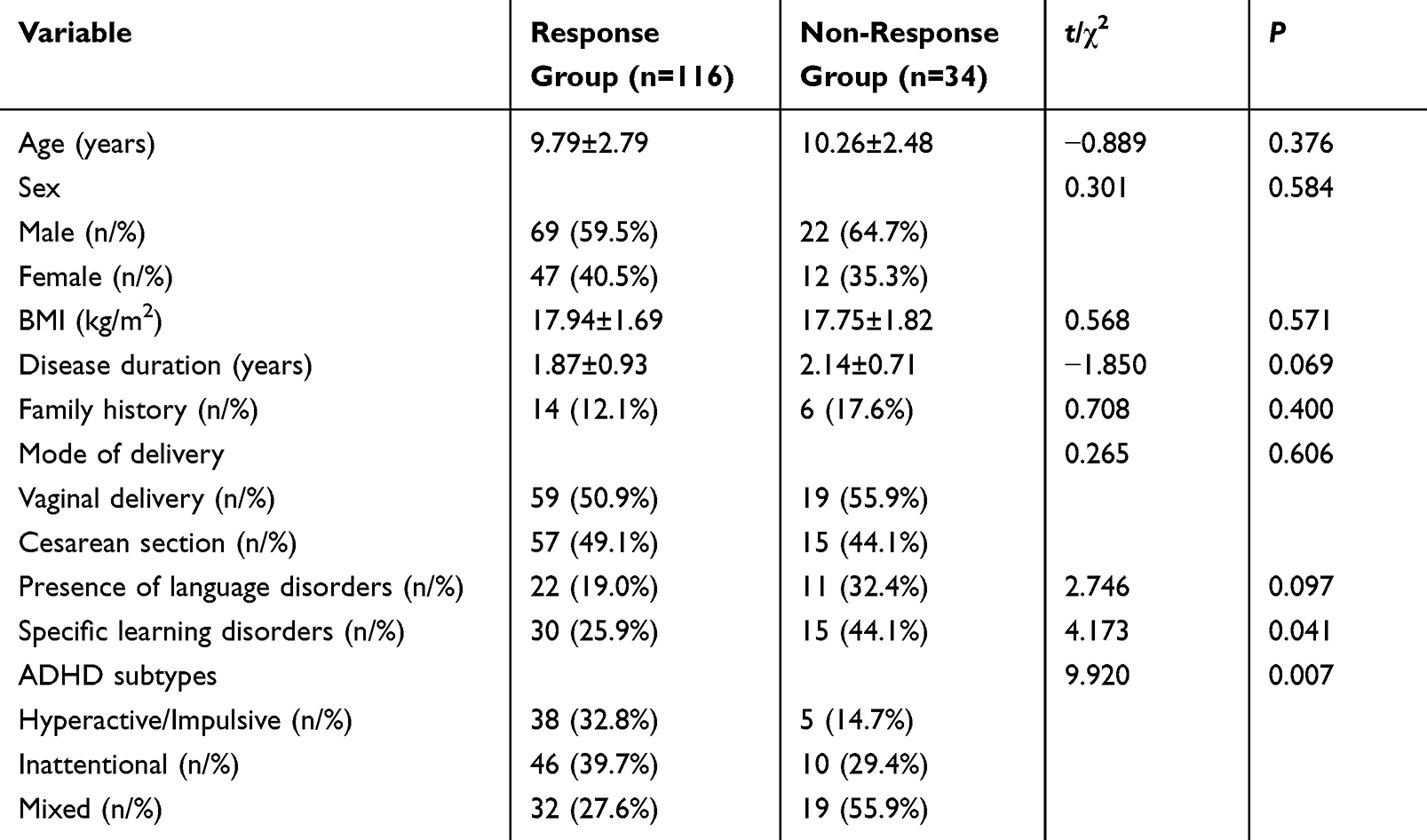 |
Table 1 Comparison of Clinical Characteristics Between Groups |
Comparison of Pre-Treatment Clinical Assessment Scales
Pre-treatment clinical assessment results showed significant differences between the response and non-response groups in terms of core ADHD symptoms, cognitive function, and functional impairment (Table 2). The non-response group had significantly higher SNAP-IV scores than the response group (P < 0.001), and PSQ scores were also markedly elevated (P < 0.001), indicating more severe inattention, hyperactivity/impulsivity symptoms, and behavioral problems. In contrast, cognitive function, as assessed by C-WISC, was significantly higher in the response group than in the non-response group (P < 0.001). Furthermore, the non-response group exhibited significantly greater overall functional impairment on the WFIRS-P (P < 0.001). These findings indicate that children with ADHD who did not respond to MPH treatment had more severe baseline symptoms, lower cognitive function, and more pronounced functional impairment prior to treatment.
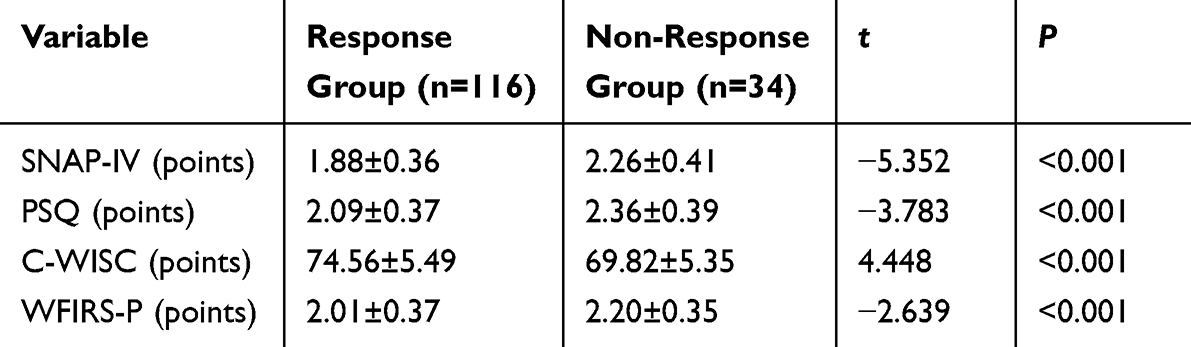 |
Table 2 Comparison of Pre-Treatment Clinical Assessment Scale Scores Between Groups |
Comparison of Pre-Treatment Laboratory Parameters
Analysis of pre-treatment laboratory parameters (Table 3) demonstrated that serum levels of 25(OH)D, COR, S100β, and BDNF were significantly higher in the response group than in the non-response group (all P < 0.05). In addition, urinary catecholamine levels, including NE and dopamine, were significantly higher in the response group (all P < 0.05). However, no significant differences were observed between the two groups in serum PRL or 5-HT levels (both P > 0.05).
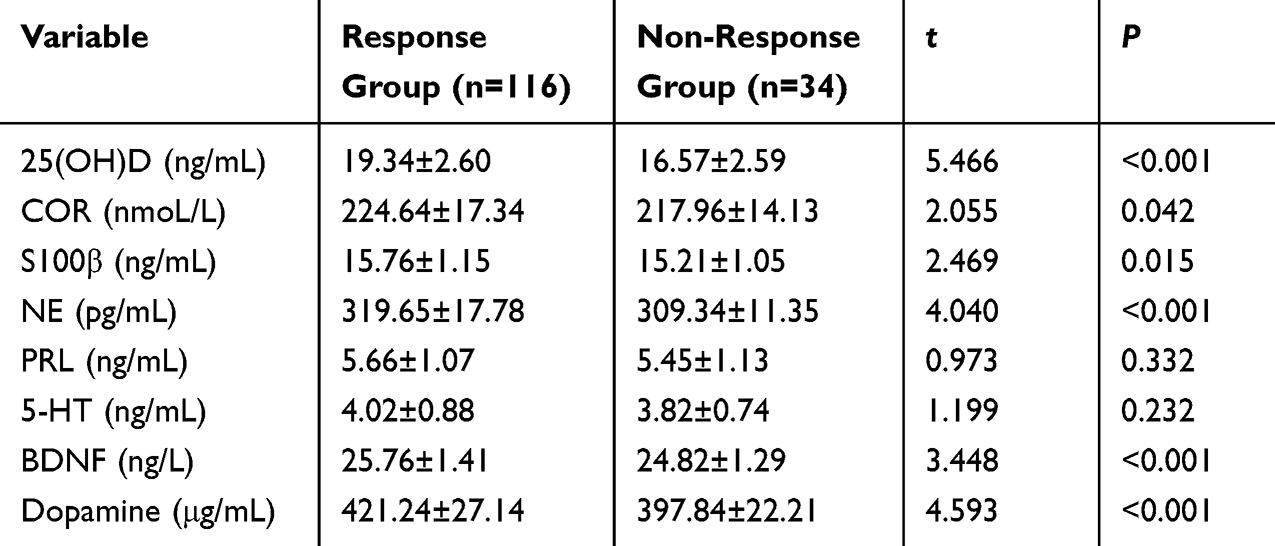 |
Table 3 Comparison of Pre-Treatment Laboratory Parameters Between Groups |
Multivariable Logistic Regression Analysis of Non-Response to MPH
Multivariable logistic regression analysis suggested that ADHD subtype, higher pre-treatment SNAP-IV total score, lower urinary dopamine levels, and lower serum 25(OH)D levels may be associated with an increased risk of non-response to MPH treatment after adjustment for potential confounders (Table 4). However, given the limited number of outcome events relative to the number of variables included in the model, these findings should be interpreted as exploratory.
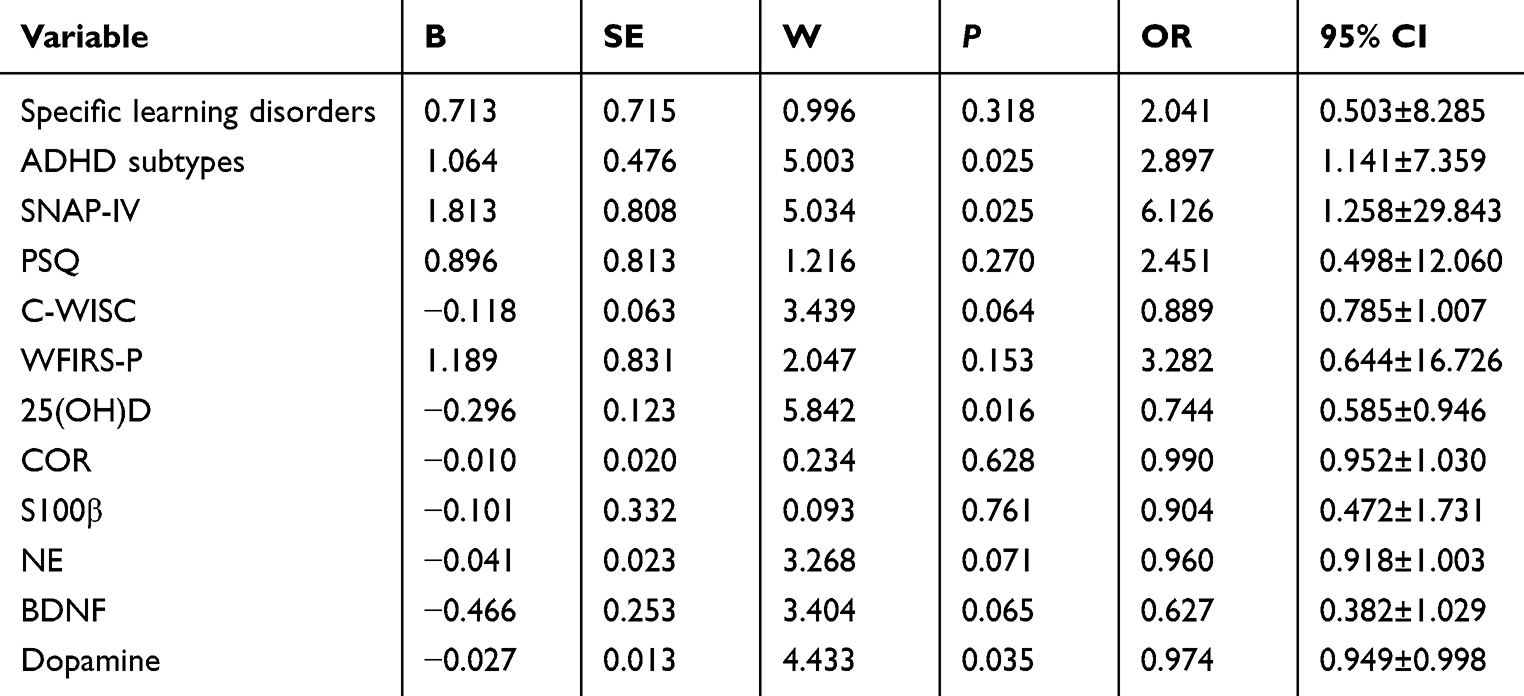 |
Table 4 Multivariable Logistic Regression Analysis of Non-Response to MPH |
Other variables, including comorbid specific learning disorders, PSQ, C-WISC, and WFIRS-P scores, as well as serum levels of S100β, COR, and BDNF and urinary NE levels, did not show significant associations in the multivariable analysis (all P > 0.05).
Overall, these results suggest that specific clinical phenotypes, baseline symptom severity, and alterations in vitamin D and dopamine levels may be potential factors associated with treatment non-response, which warrant further validation in larger cohorts.
Construction and Performance Evaluation of the Random Forest Model
To predict the risk of non-response to MPH in children with ADHD, a random forest model was constructed by incorporating all variables with P < 0.05 in the univariate analysis, including clinical characteristics, clinical assessment scale scores, and laboratory parameters. Feature importance, assessed by the mean decrease in Gini index (Figure 1A), indicated substantial variability in the contribution of different predictors. Among all variables, SNAP-IV score had the highest importance, followed by 25(OH)D, dopamine, and PSQ. The importance of C-WISC, NE, BDNF, COR, WFIRS-P, and S100β decreased sequentially. ADHD subtype and comorbid specific learning disorders contributed minimally to model prediction.
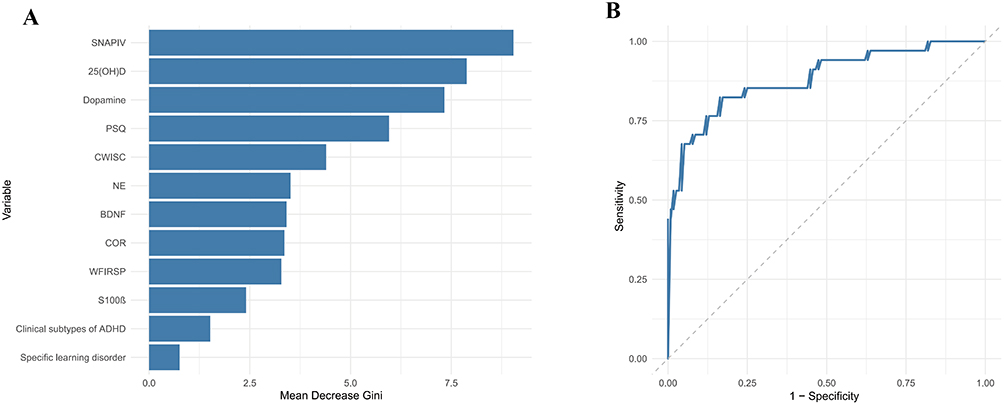 |
Figure 1 Construction of the random forest model (A) Variable importance analysis of the random forest model. (B) ROC curve. |
The out-of-bag error rate of the model in the training set was 13.21%, indicating good internal consistency and stability. Receiver operating characteristic curve analysis demonstrated an AUC of 0.883 (95% confidence interval: 0.811–0.956) (Figure 1B). In the test set, the overall prediction accuracy of the model was 86.67%, indicating strong discriminative ability in distinguishing responders from non-responders to MPH treatment.
Model Calibration and Clinical Utility
Calibration analysis (Figure 2A) showed that the bootstrap-corrected calibration curve (B = 1000 resamples) closely approximated the ideal diagonal line. The Brier score was 0.109, indicating good calibration performance and minimal deviation between predicted probabilities and observed outcomes. The Hosmer–Lemeshow goodness-of-fit test demonstrated no significant difference (χ2 = 8.312, df = 8, P = 0.404), further confirming good agreement between predicted and observed risks.
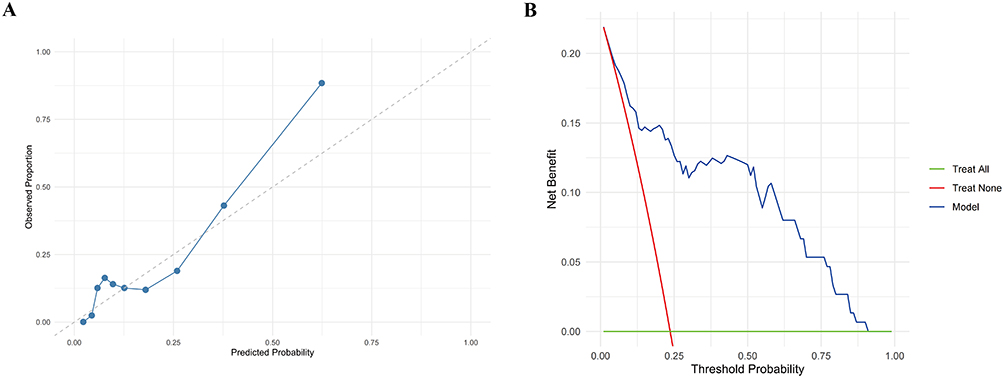 |
Figure 2 Model calibration and clinical utility (A) calibration curve of the random forest model. (B) DCA. |
DCA (Figure 2B) showed that the model provided a positive net benefit across a threshold probability range of 0.01–0.50, with a maximum net benefit of 0.219. These results indicate that the model offers meaningful clinical utility, even at relatively low risk thresholds, and may support clinical decision-making.
Discussion
In this study, a random forest model was developed to predict the risk of non-response to MPH in children with ADHD based on clinical characteristics, clinical assessment scales, and laboratory parameters, and its performance was compared with that of multivariable logistic regression analysis. The results demonstrated that the random forest model exhibited good discrimination, calibration, and clinical applicability in both the training and test sets. Variable importance analysis indicated that SNAP-IV score, 25(OH)D, dopamine, and PSQ were the most influential predictors, suggesting that treatment response to MPH is determined, to a certain extent, by both clinical phenotypes and biological characteristics.
In the present study, SNAP-IV score showed the highest importance in the random forest model and was also identified as an independent risk factor in the multivariable logistic regression analysis, highlighting its critical role in predicting non-response to MPH. The SNAP-IV scale is widely used to assess the severity of core ADHD symptoms, and its total score directly reflects the severity of inattention and hyperactivity/impulsivity. Previous studies have demonstrated that baseline symptom severity is a key predictor of treatment response, with more severe symptoms generally associated with poorer response to pharmacotherapy.20,21 This phenomenon may be related to greater neurocognitive impairment, as children with more severe baseline symptoms may exhibit more pronounced deficits in executive function and emotional regulation, which could jointly influence treatment outcomes. The findings of this study further confirm that elevated pre-treatment SNAP-IV scores are independently associated with non-response to MPH, underscoring the importance of baseline symptom severity in predicting treatment outcomes.
In addition, serum 25(OH)D levels and urinary dopamine levels demonstrated significant predictive value in both models and were identified as independent risk factors for non-response to MPH, which has important pathophysiological implications. Vitamin D is not only involved in calcium and phosphorus metabolism but also influences dopamine synthesis by regulating the expression of tyrosine hydroxylase. Vitamin D receptors are widely distributed in brain regions rich in dopaminergic neurons.22 Clinical studies have also shown that children with ADHD generally have lower serum 25(OH)D levels, which are negatively correlated with SNAP-IV scores, and that vitamin D supplementation can significantly improve core ADHD symptoms.10 Dopamine is the primary target of MPH, which increases synaptic dopamine levels by blocking the dopamine transporter. Low baseline dopamine levels may indicate insufficient functional reserve of the dopaminergic system, thereby reducing the therapeutic efficacy of MPH.23 The findings of this study are consistent with these mechanistic insights and further support the critical roles of vitamin D and dopamine in modulating response to MPH from a clinical perspective.
It is noteworthy that ADHD subtype was identified as an independent risk factor in the multivariable logistic regression analysis but demonstrated minimal importance in the random forest model. This discrepancy reflects the inherent differences between the two analytical approaches: logistic regression focuses on the independent net effect of each variable, whereas random forest evaluates the overall predictive contribution by capturing nonlinear relationships and interactions. The combined subtype of ADHD may be inherently associated with higher SNAP-IV scores and lower dopamine levels, and its predictive information may be subsumed by these continuous variables in the random forest model. This observation is consistent with previous studies showing that random forest models can more effectively integrate multidimensional predictive information and often outperform traditional logistic regression models.24 Similarly, another study using a random forest model to predict response to neurofeedback therapy in ADHD also demonstrated favorable predictive accuracy.11 Collectively, these findings highlight the unique advantages of machine learning approaches, such as random forest, in capturing complex, nonlinear, and interactive relationships, thereby serving as a valuable complement to conventional regression methods.
The random forest model developed in this study demonstrated good discrimination, calibration, and net clinical benefit, indicating its potential clinical utility. Previous studies have often relied on neuroimaging or genetic markers to construct predictive models, such as random forest models based on polygenic risk scores derived from gene sets.25 However, these approaches are often costly and less accessible, limiting their clinical applicability. In contrast, the present study utilized readily obtainable clinical characteristics, assessment scales, and routine laboratory parameters, offering advantages of non-invasiveness, simplicity, and low cost, making it more feasible for implementation in primary healthcare settings. This model may assist clinicians in identifying children at high risk of non-response to MPH prior to treatment initiation, thereby enabling early optimization of treatment strategies, such as incorporating behavioral therapy, switching medications, or adjusting dosage regimens.
Despite its strengths, including a prospective design, standardized procedures, and integration of multidimensional variables, this study has several limitations. First, as a single-center study, all participants were recruited from the same hospital, which may introduce selection bias, and the generalizability of the model to other populations and clinical settings requires further validation. Second, the sample size was relatively small, particularly in the non-response group, which may affect model stability and generalizability; thus, multicenter studies with larger sample sizes are needed for external validation. Third, the follow-up period was limited to 3 months, which allows assessment of short-term treatment efficacy but does not capture long-term treatment outcomes or the risk of symptom relapse. Given that ADHD is a chronic neurodevelopmental disorder, long-term prediction of treatment response is also clinically important. Moreover, information regarding concurrent non-pharmacological interventions was not systematically collected and therefore could not be incorporated into the present model. As such interventions may influence treatment outcomes, their omission may have introduced residual confounding and potentially affected predictive accuracy. Finally, due to study constraints, multimodal biological data such as genetic and neuroimaging markers were not included; incorporation of these deeper-level features may further enhance predictive performance. Future studies should therefore focus on multicenter, large-sample, long-term prospective designs, with more comprehensive assessment of treatment-related factors, as well as integration of multimodal data, to further validate and optimize the model and improve its generalizability and clinical applicability.
Conclusion
In this prospective observational cohort study, a random forest model based on clinical characteristics, assessment scales, and laboratory parameters effectively predicted the risk of non-response to MPH in children with ADHD. SNAP-IV score, serum 25(OH)D level, and urinary dopamine level were identified as key predictors. The model relies on readily accessible clinical indicators and offers advantages of simplicity and low cost, providing a practical tool for clinicians to identify high-risk patients before treatment initiation and to optimize therapeutic strategies early. However, given the limitations of a relatively small sample size and single-center design, further multicenter external validation is warranted, along with exploration of multimodal data integration to enhance model generalizability.
Ethics Statement
The study protocol was approved by the institutional ethics review board of The Fourth Hospital of Changsha (Integrated Traditional Chinese and Western Medicine Hospital of Changsha, Changsha Hospital of Hunan Normal University) (No. CSSDSYY-YXLL-SC-2024-03-14). Written informed consent was obtained from the legal guardians of all child participants. Verbal assent was obtained from the children themselves, with those aged 8 years and older also signing a child assent form. All consents were obtained after a full explanation of the study procedures in age-appropriate language, prior to study commencement. This study was conducted in accordance with the principles of the Declaration of Helsinki. All data were anonymized to protect patient privacy.
Funding
This study was supported by Changsha Natural Science Foundation (No. kq2502298).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Leffa DT, Caye A, Rohde LA. ADHD in children and adults: diagnosis and prognosis. Curr Top Behav Neurosci. 2022;57:1–10. doi:10.1007/7854_2022_329
2. Joshi HM, Angolkar M. Prevalence of ADHD in Primary School Children in Belagavi City, India. J Atten Disord. 2021;25(2):154–160. doi:10.1177/1087054718780326
3. Harpin VA. The effect of ADHD on the life of an individual, their family, and community from preschool to adult life. Arch Dis Child. 2005;90(Suppl 1):i2–7. doi:10.1136/adc.2004.059006
4. Vertessen K, Luman M, Swanson JM, et al. Methylphenidate dose-response in children with ADHD: evidence from a double-blind, randomized placebo-controlled titration trial. Eur Child Adolesc Psychiatry. 2024;33(2):495–504. doi:10.1007/s00787-023-02176-x
5. Inci Izmir SB, Ipci M, Ercan ES. Methylphenidate significantly improves neurocognitive impairments in children with ADHD. Psychiatry Res. 2022;311:114492. doi:10.1016/j.psychres.2022.114492
6. D’Aiello B, Di Vara S, De Rossi P, Pretelli I, Vicari S, Menghini D. Moderators and other predictors of methylphenidate response in children and adolescents with ADHD. Int J Environ Res Public Health. 2022;19(3):1640. doi:10.3390/ijerph19031640
7. Ermers NJ, Hagoort K, Scheepers FE. The predictive validity of machine learning models in the classification and treatment of major depressive disorder: state of the art and future directions. Front Psychiatry. 2020;11:472. doi:10.3389/fpsyt.2020.00472
8. Volkow ND, Swanson JM. Variables that affect the clinical use and abuse of methylphenidate in the treatment of ADHD. Am J Psychiatry. 2003;160(11):1909–1918. doi:10.1176/appi.ajp.160.11.1909
9. Piacentino D, De Rossi P, Kotzalidis GD, et al. Methylphenidate challenge test in adults with attention deficit/hyperactivity disorder (ADHD): clinical effects and their predictors. Hum Psychopharmacol. 2020;35(5):e2740. doi:10.1002/hup.2740
10. Mohammadpour N, Jazayeri S, Tehrani-Doost M, et al. Effect of vitamin D supplementation as adjunctive therapy to methylphenidate on ADHD symptoms: a randomized, double blind, placebo-controlled trial. Nutr Neurosci. 2018;21(3):202–209. doi:10.1080/1028415X.2016.1262097
11. Hoseini R, Shalbaf A. An explainable machine learning-based approach to predicting treatment response for neurofeedback in ADHD. Sci Rep. 2025;15(1):43162. doi:10.1038/s41598-025-27246-9
12. Kim JW, Sharma V, Ryan ND. Predicting methylphenidate response in adhd using machine learning approaches. Int J Neuropsychopharmacol. 2015;18(11):pyv052. doi:10.1093/ijnp/pyv052
13. Chen M, van der Pal Z, Poirot MG, et al. Prediction of methylphenidate treatment response for ADHD using conventional and radiomics T1 and DTI features: secondary analysis of a randomized clinical trial. Neuroimage Clin. 2025;45:103707. doi:10.1016/j.nicl.2024.103707
14. World Medical A. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
15. Association AP. Diagnostic and statistical manual of mental disorders. Journal. 2013.
16. Swanson JM, Nolan W, Pelham WE. The SNAP-IV rating scale. Journal. 1992.
17. B RA. Hyperactive children: a handbook for diagnosis and treatment. Journal. 1982;132–134.
18. Gong YX, Cai TS. Zhong Guo Xiu Ding Wei Shi Er Tong Zhi Li Liang Biao (C-WISC) Shou Ce. Journal. 1993.
19. Weiss MD, Hammer J, Quarles RH. Weiss functional impairment rating scale (wfirs) - parent report. university of british columbia. J. Neurosci. Res. 2000;62:772–780. doi:10.1002/1097-4547(20001215)62:6<772::AID-JNR3>3.0.CO;2-X
20. Pagnier M. Predicting the response of children and adolescents with adhd to methylphenidate: a systematic review. J Atten Disord. 2023;27(12):1377–1392. doi:10.1177/10870547231177234
21. Arnett AB, Rutter TM, Stein MA. Neural markers of methylphenidate response in children with attention deficit hyperactivity disorder. Front Behav Neurosci. 2022;16:887622. doi:10.3389/fnbeh.2022.887622
22. Cui X, Pertile R, Liu P, Eyles DW. Vitamin D regulates tyrosine hydroxylase expression: n-cadherin a possible mediator. Neuroscience. 2015;304:90–100. doi:10.1016/j.neuroscience.2015.07.048
23. Aster HC, Romanos M, Walitza S, et al. Responsivity of the Striatal Dopamine System to Methylphenidate-A Within-Subject I-123-beta-CIT-SPECT Study in Male Children and Adolescents With Attention-Deficit/Hyperactivity Disorder. Front Psychiatry. 2022;13:804730. doi:10.3389/fpsyt.2022.804730
24. Garcia-Argibay M, Zhang-James Y, Cortese S, Lichtenstein P, Larsson H, Faraone SV. Predicting childhood and adolescent attention-deficit/hyperactivity disorder onset: a nationwide deep learning approach. Mol Psychiatry. 2023;28(3):1232–1239. doi:10.1038/s41380-022-01918-8
25. Barnett EJ, Zhang-James Y, Faraone SV. Improving machine learning prediction of adhd using gene set polygenic risk scores and risk scores from genetically correlated phenotypes. Am J Med Genet B Neuropsychiatr Genet. 2025;198(8):200–209. doi:10.1002/ajmg.b.33043
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Machine Learning Based Prediction of Postoperative Acute Kidney Injury Risk in Coronary Artery Bypass Grafting Patients
Zhang Y, Cai D, Deng Y, Wang Z, Zhang Z, Zhang H, Wang Q, Feng S, Sun L, Wei J
Clinical Interventions in Aging 2025, 20:2033-2048
Published Date: 15 November 2025
Enhancing Methylphenidate’s Neurocognitive Effects in Pediatric ADHD with Adaptive Digital Therapy: A Randomized Controlled Trial
Chen X, Wang S, Yang X, Yu C, Ni F, Yang J, Tian Y, Ye J, Liu H, Chen X, Luo R
Psychology Research and Behavior Management 2026, 19:550150
Published Date: 13 February 2026
Predicting Intrahepatic Cholestasis of Pregnancy: A Retrospective Cohort Study of a Comprehensive Clinical Prediction Model
Liang H, Tian Y, Gao J, Teng J
International Journal of General Medicine 2026, 19:570357
Published Date: 27 February 2026
The Effect of Drug Holidays on Metacognitive and Theory of Mind Skills of Children Diagnosed with Attention Deficit Hyperactivity Disorder: Preliminary Findings
Köksal M, Sari M, İmrek Y, Öztürk Y, Özyurt G, Tufan AE
Neuropsychiatric Disease and Treatment 2026, 22:573124
Published Date: 3 July 2026