Back to Journals » Psychology Research and Behavior Management » Volume 19
Enhancing Methylphenidate’s Neurocognitive Effects in Pediatric ADHD with Adaptive Digital Therapy: A Randomized Controlled Trial
Authors Chen X, Wang S, Yang X, Yu C, Ni F, Yang J, Tian Y, Ye J, Liu H, Chen X ![]() , Luo R
, Luo R
Received 27 June 2025
Accepted for publication 6 January 2026
Published 13 February 2026 Volume 2026:19 550150
DOI https://doi.org/10.2147/PRBM.S550150
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mei-Chun Cheung
Xiaolu Chen,1 Sihan Wang,2 Xiaowen Yang,1 Chunmei Yu,1 Fang Ni,1 Jie Yang,1 Yu Tian,1 Jiucai Ye,1 Hao Liu,1 Xiang Chen,3 Rong Luo1
1Department of Pediatrics, West China Second University Hospital; Key Laboratory of Obstetrics & Gynecologic and Pediatric Diseases and Birth Defects of the Ministry of Education, Sichuan University, Chengdu, 610041, People’s Republic of China; 2Neuro Weave, Co., Ltd., Shanghai, 200001, People’s Republic of China; 3Fangcun Quanxiang (Beijing) Technology Co., Ltd, Beijing, 100010, People’s Republic of China
Correspondence: Rong Luo, Department of Pediatrics, West China Second University Hospital; Key Laboratory of Obstetrics & Gynecologic and Pediatric Diseases and Birth Defects of the Ministry of Education, Sichuan University, No. 20, Section 3, Renmin South Road, Chengdu, 610041, People’s Republic of China, Tel +86-13882050273, Email [email protected]
Background: Digital therapeutics have emerged as promising adjuncts to pharmacological treatment for attention-deficit/hyperactivity disorder (ADHD), yet evidence from rigorously designed trials remains limited. This study aimed to evaluate the additive neurocognitive benefits of an adaptive digital therapy (Focus Pro) when combined with methylphenidate (MPH) in children with ADHD.
Methods: In the present single-center, double-blind, randomized controlled trial, 85 children (6– 12 years old) diagnosed with ADHD were assigned to receive MPH plus Focus Pro (n=44) or MPH alone (n=41) over an eight-week treatment period, with follow-up assessments at week 12. The digital therapy consisted of daily 25-minute sessions that targeted attention and executive functioning. The primary outcomes included objective neurocognitive measures assessed by the Test of Variables of Attention (TOVA), alongside secondary outcomes based on parent-reported scales (Swanson, Nolan, and Pelham Rating Scale, Fourth Edition [SNAP-IV], Weiss Functional Impairment Rating Scale, and Clinical Global Impressions-Severity). The analysis employed mixed repeated-measures ANOVA under an intention-to-treat framework.
Results: Although both groups exhibited comparable improvements on subjective measures, the combination group demonstrated significantly greater gains in objective neurocognitive performance, particularly on TOVA attention comparison scores, at week eight (p=0.006, Cohen’s d=0.809). Furthermore, a significant group effect was observed (F=8.478, p=0.005), with improvements sustained through post-intervention follow-up. Early symptom reduction was noted in both groups (week four, p< 0.001), but merely the combined therapy group maintained enhanced objective performance, revealing a divergence between subjective and objective outcomes.
Conclusion: The integration of adaptive digital therapy with MPH can significantly enhance neurocognitive outcomes in pediatric ADHD, particularly in sustained attention and inhibitory control. These findings highlight the clinical potential of personalized digital tools, and underscore the importance of incorporating objective assessments when evaluating digital interventions.
Keywords: attention deficit hyperactivity disorder, digital therapeutics, methylphenidate, randomized controlled trial, neuropsychological tests, executive function
Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a common neurodevelopmental condition marked by persistent and developmentally inappropriate patterns of inattention, hyperactivity, and impulsivity.1 Increasing evidence points to the widespread, subtle dysregulation of gene expression across multiple brain regions, as a key contributor to the disrupted neural circuits and cognitive impairments observed in ADHD. With a global prevalence of approximately 8%, ADHD ranks among the most frequently diagnosed pediatric psychiatric disorders.2
Present standard treatments for ADHD adopt a multimodal approach, which combines pharmacological and psychosocial interventions to target core symptoms and related functional impairments.3 Stimulant medications (primarily methylphenidate [MPH] and amphetamines) remain as the most prescribed pharmacotherapies, offering robust symptom control.4 Complementary psychosocial strategies, including cognitive behavioral therapy (CBT),5 parent management training (PMT),6 and educational interventions,7 aim to mitigate disruptive behaviors, and foster self-regulation and adaptive functioning. Individual counseling offers structured support for emotional and behavioral challenges, while peer-support networks can enhance parental resilience by facilitating shared experiences and resource access.8
Despite its benefits, traditional CBT-based interventions face several limitations. The requirement for repeated in-person visits imposes temporal and geographic burdens, which can hinder early detection, reduce treatment adherence, and strain caregiver engagement. Furthermore, the absence of real-time monitoring complicates efforts to dynamically track symptom progression and tailor interventions. These constraints underscore the need for scalable, flexible, and accessible therapeutic alternatives.
Digital therapeutics (DTx) have emerged as a promising solution, harnessing digital platforms to deliver real-time, personalized interventions that transcend spatiotemporal limitations. Defined by the Digital Therapeutics Alliance,9 DTx refers to software-driven, evidence-based interventions designed to prevent, manage, or treat medical disorders, particularly chronic conditions amenable to behavioral modification. It is emerging as a transformative paradigm in pediatric healthcare, where accessibility, engagement, and personalization are especially critical. Although only a limited number of prescription digital therapeutics have been authorized for pediatric use, early examples already demonstrate both feasibility and therapeutic benefit for conditions such as attention-deficit/hyperactivity disorder (ADHD). In ADHD management, digital therapies have employed platforms, such as virtual reality,10 serious games,11 and wearable devices,12 in order to enhance attention, executive function, and academic performance.
Recent randomized controlled trials (RCTs) have demonstrated the potential of DTx to augment standard ADHD treatments. For instance, combining virtual reality-based cognitive training with MPH has yielded superior improvements in core ADHD symptoms, when compared to medication alone.13 Similarly, Larsen et al14 reported that a computer-based attention training game enhanced both attentional capacity and academic performance. A large-scale trial conducted by Kollins et al15 further reinforced these findings, showing significant symptom reduction with a novel digital intervention. A meta-analysis has also highlighted improvements in attention, executive function, and working memory through game-based digital strategies.16
However, despite the encouraging findings, the efficacy of digital therapies in ADHD remains under debate. Inconsistencies across studies highlight the need for more rigorous evaluations and optimization of intervention design. Notably, few digital interventions fully leverage the adaptive capabilities of artificial intelligence (AI). Most of these rely on pre-programmed difficulty levels, lacking the ability to tailor intervention intensity to the users’ evolving cognitive profiles, which is particularly crucial during childhood and adolescence, when executive and perceptual capacities are rapidly developing.17 However, furthermore, uniform or static difficulty settings often fail to accommodate individual variability, reducing engagement, and limiting therapeutic benefit.
In addition, platform-specific constraints may impact intervention efficacy. Desktop-based programs that rely on mouse and keyboard inputs may introduce ergonomic challenges and cognitive load, adversely affecting performance and accuracy in cognitive assessments.18 Conversely, although mobile devices offer portability, their limited screen size may impair visual processing and responsiveness.19 These considerations suggest that input modality and display characteristics are critical, yet are underappreciated determinants, of digital therapy success.
The present study addresses these gaps by developing and evaluating an adaptive, AI-assisted DTx platform designed for pediatric ADHD. The present system incorporates real-time feedback loops to dynamically adjust task difficulty based on the user’s performance, minimizing ceiling and floor effects, and optimizing treatment efficacy. The interventions were delivered through child-friendly, touch-based interfaces on portable tablets, ensuring developmental appropriateness, and facilitating sustained engagement.
The investigators posit that the integration of AI with DTx has the potential to transform ADHD care. By leveraging continuous performance data and adjusting interventions in real time, AI-enhanced platforms may deliver greater cognitive gains within shorter treatment windows. In order to test this hypothesis, a randomized controlled trial was conducted to determine whether the addition of adaptive digital therapy to standard MPH treatment can improve neurocognitive outcomes in children with ADHD, with a particular focus on sustained attention and executive control.
Methods
Study Design and Participants
Study Design
The present prospective, single-center, double-blind, randomized controlled trial with a parallel-group design was conducted in accordance with a pre-specified protocol, aiming to minimize bias and enhance study rigor. Ethics approval was obtained from the Medical Ethics Committee of West China Second University Hospital, Sichuan University (Approval no. 2022–176), all methods were carried out in accordance with relevant guidelines and with the Declaration of Helsinki. A written informed consent was secured from all participants and their legal guardians. The study was registered with the Chinese Clinical Trial Registry (ChiCTR2200064983).
The present study employed a mixed repeated-measures design, with one between-subject factor (group: experimental vs control) and one within-subject factor (time: baseline [week zero], week four, week eight, and week 12). The analysis explored the main effects of time and group, as well as their interaction, using repeated-measures ANOVA with appropriate post-hoc testing.
Participants
At baseline, a total of 89 children (6–11 years old) were assessed for eligibility. Among these children, one child was excluded due to the use of amlodipine, rather than MPH, and an additional three children were excluded for failing to meet the minimum Swanson, Nolan, and Pelham Rating Scale, Fourth Edition (SNAP-IV) score required for inclusion (SNAP-IV <24). Ultimately, 85 children were enrolled and randomized into the present study, with 44 children allocated to the experimental group (received Focus Pro in combination with MPH) and 41 children allocated to the control group (received MPH alone). During the 12-week study period, a total of 10 children withdrew or were excluded: four children from the control group (one child was excluded due to significant bias and three children were excluded due to early dropout prior to week four) and six children from the experimental group (one child was excluded due to protocol bias and five children were excluded due to attrition). The overall dropout rate was approximately 10%, which was slightly higher than anticipated. The flow diagram of participants is presented in Figure 1.
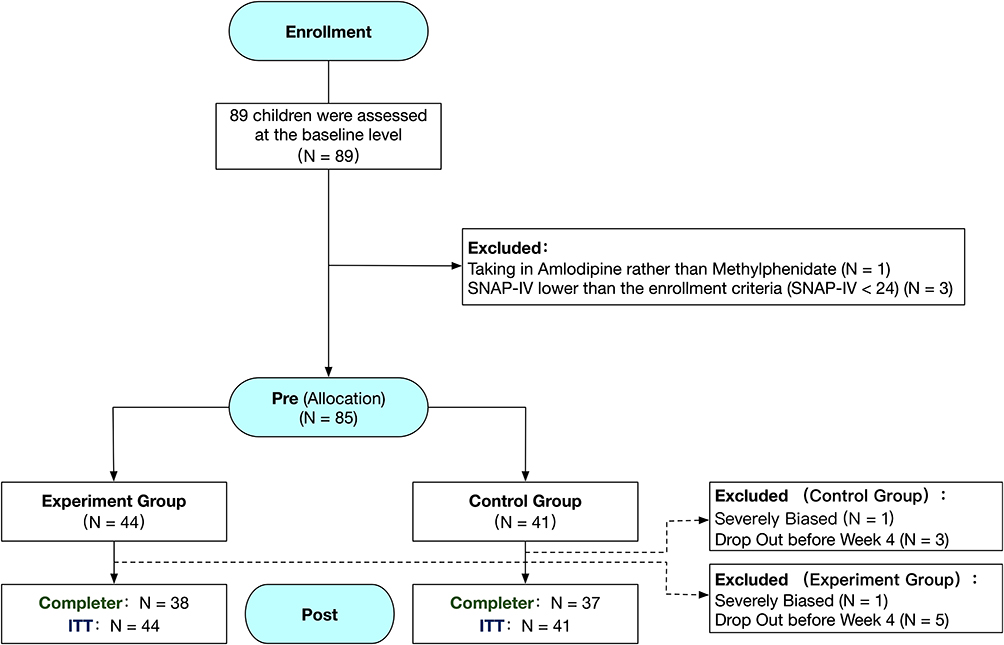 |
Figure 1 Flowchart of study participants. |
Eligibility Criteria
At baseline (week zero), all participants were screened for eligibility, in accordance with the International Conference on Harmonisation (ICH) Good Clinical Practice guidelines. The study protocol was reviewed and approved by the Institutional Review Board. The eligible participants were children between 6–12 years old, of any gender, who met the diagnostic criteria for ADHD, specifically the predominantly inattentive type or combined type that involved both inattentiveness and hyperactivity/impulsivity, as defined by the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5).
In order to qualify for the study, the participants were required to have a score of 24 or higher for SNAP-IV, and a Clinical Global Impressions-Severity (CGI-S) score of at least 4, indicating moderate or greater symptom severity. Intellectual functioning was assessed using the Child Wechsler Intelligence Scale, and merely participants who had a score of 80 or above were considered eligible. Furthermore, the participants were required to have been receiving a stable dose of MPH for at least 30 days prior to enrollment, and were expected to remain on the same regimen and dosage throughout the duration of the study. In addition to meeting these core criteria, the participants were required to demonstrate adequate compliance capacity, and willingness to complete all study assessments and procedures.
The exclusion criteria were carefully defined to minimize potential confounding factors, and ensure the reliability of outcome measures. Children with any known neurodevelopmental disorders, such as cerebral palsy, epilepsy, or adrenoleukodystrophy (ALD), as well as children with serious psychiatric comorbidities, including schizophrenia, were excluded. Children whose attentional difficulties could be attributed to sensory impairments, particularly hearing loss, were not eligible to participate. Furthermore, the present study excluded children who previously received systemic treatment with two different categories of ADHD medications without a favorable response, as well as children who recently used ADHD medications other than MPH, or engaged in any non-pharmacologic ADHD interventions within the past month.
Further exclusions included children with visual impairments, such as color blindness, or other conditions that can interfere with the use of the DTx software. Children with a history of gaming addiction, or children suspected of having substance use or dependency within the past six months were excluded due to potential compliance and safety concerns. Children with motor impairments, including physical deformities, or functional limitations of the hands or arms that can hinder device use, were also deemed ineligible. In addition, children with a history of suicidal ideation or behaviors, as determined by the clinical assessment, were not permitted to enroll. Children presently enrolled in another clinical trial or investigational study within the previous month were excluded to avoid cross-study contamination. Finally, children who were judged by the research team to be otherwise unsuitable for the study, based on medical or behavioral concerns, were not included.
Randomization and Blinding
Randomization was performed using the SAS PROC PLAN by an independent biostatistician uninvolved in the clinical trial. The participants were sequentially enrolled and assigned study equipment according to pre-generated random numbers. Allocation concealment was maintained to ensure that neither the investigators nor the participants could influence the group assignment. The control group did not lack a digital-therapy counterpart, as both the control and intervention groups received a combination of medication and game-based activities. The only difference was that children in the control group played conventional games without therapeutic components, whereas those in the intervention group engaged with the digital therapeutic game. The type and content of the games were closely matched across groups to minimize unintended experimenter effects arising from differences in task format, information exposure, or other procedural factors.
In order to minimize assessment bias, the outcome raters were blinded to the group allocation. The raters independently administered and scored the behavioral assessments. Prior to trial initiation, all research personnel received training from the device manufacturer to ensure standardized protocol adherence. Quality assurance and monitoring were conducted by independent clinical inspectors to ensure compliance with the study protocol. At trial completion, the data was thoroughly cleaned and validated using structured query forms.
Treatment
MPH, which is the first-line pharmacological treatment recommended by ADHD guidelines, was used as the pharmacological base to ensure comparability. Participants in the experimental group received MPH combined with adaptive digital therapy Focus Pro (25-minute sessions, five days per week for eight weeks), while participants in the control group received MPH monotherapy for the same duration.
Between August 2022 and March 2023, 85 eligible participants were randomized to the experimental group (MPH + Focus Pro) or control group (MPH only), and received treatment under the supervision of the Department of Pediatric Neurology at West China Second University Hospital of Sichuan University.
Outcomes and Assessment
The primary outcome measures included both the subjective and objective indices of attention-related function. Week 8 was designated as the primary time point. From week 0 to week 8, all children received their assigned intervention, and outcomes were measured to assess its immediate effects. Week 12 served as the secondary endpoint. From week 0 to week 12, participants underwent regular assessments to evaluate both immediate and potentially sustained effects of the intervention.
Subjective symptoms were assessed using SNAP-IV,20 which is a widely validated parent-report instrument designed to quantify the core ADHD symptoms defined in the Diagnostic and Statistical Manual of Mental Disorders, fourth edition (DSM-IV). The scale consists of 18 items, and is equally divided between domains of inattention and hyperactivity/impulsivity. In the present study, the analysis included the total scores, improvement rates from baseline, and domain-specific scores for inattention (items 1–9) and hyperactivity/impulsivity (items 10–18).
In addition to symptom severity, functional outcomes were assessed using the Weiss Functional Impairment Rating Scale-Parent Report (WFIRS-P), which is a 50-item parent-rated instrument that evaluates six key domains of functional impairment commonly affected in ADHD, including family life, school performance, daily living skills, self-concept, social functioning, and risk behaviors. WFIRS-P has been recognized as a sensitive tool for tracking the real-world impact of ADHD and its treatment.
Global clinical severity was rated by trained clinicians using the CGI-S scale,21 which is a one-item observer-rated measure of illness severity on a 7-point scale that ranges from 1 (normal) to 7 (among the most severely ill).
Objective neurocognitive function was measured using the Test of Variables of Attention (TOVA), which is a computerized continuous performance test (CPT) widely employed for the diagnosis and treatment monitoring of ADHD. The visual version of TOVA was used in the present study due to its independence from language and cultural influences, allowing for standardized assessment across participants. The test involves the responses to visual or auditory stimuli through a highly sensitive microswitch (±1 ms accuracy), and generates a comprehensive profile that includes variability in response time, mean response speed, impulsivity (commission errors), and vigilance (omission errors). These scores were compared against extensive normative datasets, including over 1700 individuals for the visual version and 2600 individuals for the auditory version, as well as a reference sample of clinically diagnosed ADHD individuals.
Among the various TOVA metrics, the Attention Comparison Score (ACS) was a key indicator used in the present study. This score quantifies the deviation of the participant’s performance from the ADHD diagnostic reference group, with values below zero indicating stronger alignment with ADHD-like performance. ACS was calculated using the following composite formula: attention comparison score = calibration constant + standard score of response time (half 1) + standard score of D prime (half 2) + standard score of variability (total).
The additional primary TOVA variables analyzed included the following:
- Response time variability (RTV): the standard deviation of correct response latencies, used as a measure of attentional consistency;22
- Correct response time: the average latency for accurate responses, with slower reaction times especially noted in the initial, less stimulating portion of the task among individuals with ADHD;
- D′ (d-prime): derived from the signal detection theory, this sensitivity index reflects the ability to discriminate between target and non-target stimuli over time, and is sensitive to fatigue and attentional decline, both of which are commonly observed in ADHD.
Sample Size and Statistical Power
The sample size was determined through an a priori power analysis using G*Power (version 3.1). For the primary outcome, a repeated-measures ANOVA with a between–within interaction was planned to detect a moderate effect size (f = 0.25), with a two-sided alpha of 0.05, power of 0.80, two groups, and four repeated measurements. Assuming a correlation of 0.5 among repeated measures and a nonsphericity correction (ε) of 1, the analysis indicated that at least 24 participants per group were required. Both the intention-to-treat sample (44 in the intervention group and 41 in the control group) and the per-protocol sample (38 and 37, respectively) exceeded this minimum, ensuring adequate statistical power for detecting both main and interaction effects.
Assessment of Statistical Assumptions
Statistical assumptions were verified prior to analysis. Mauchly’s Test of Sphericity23 was applied to determine whether the assumption of sphericity was met for repeated-measures analysis. If this assumption was violated (p<0.05), a correction was made using the Greenhouse-Geisser (GG) adjustment for W <0.75 or the Huynh-Feldt (HF) adjustment for W ≥0.75.
Results
Baseline Characteristics
In order to maintain the methodological integrity of the trial, the data was analyzed following the intention-to-treat (ITT) principle,24 whereby participants were included in their originally assigned treatment groups, regardless of adherence or protocol deviations. This approach preserves the randomization benefits and provides a realistic estimation of treatment effectiveness in practical settings.
Missing data, which were minimal in the present study, were addressed using mean imputation, wherein missing values were substituted with the mean score for the relevant time point and variable. The sensitivity analysis revealed no statistically significant differences in baseline characteristics between participants with missing data and participants with complete datasets, thereby affirming the robustness of the ITT dataset. The distribution of baseline demographic and clinical characteristics is presented in Table 1.
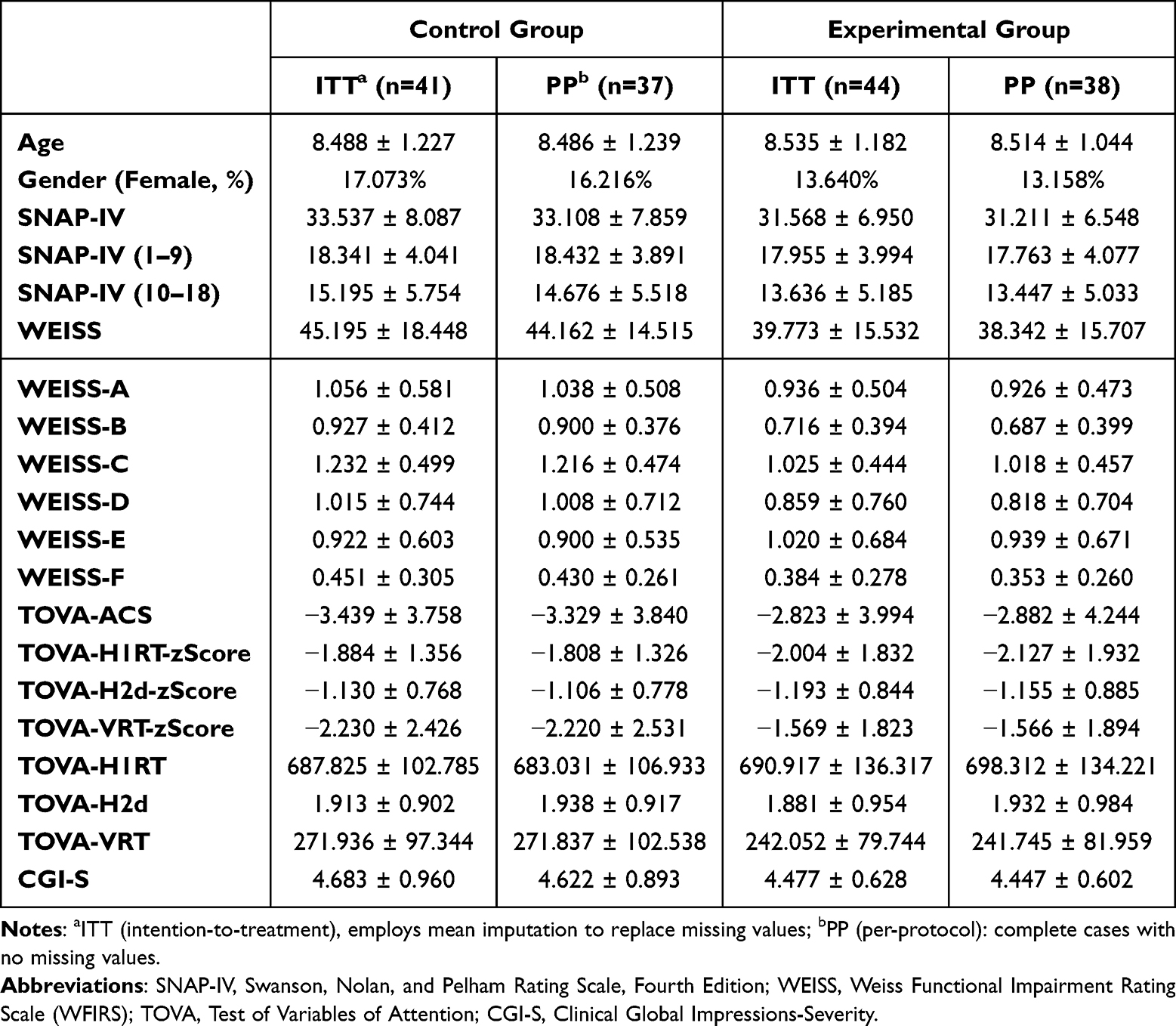 |
Table 1 Baseline Characteristics of Participants in the Experimental and Control Groups |
SNAP-IV Symptom Score Changes
Mixed repeated-measures analysis of variance (ANOVA) was conducted to evaluate the changes in SNAP-IV scores over time between the experimental and control groups. Mauchly’s test indicated a violation of sphericity assumption (W<0.75). Therefore, GG corrections were applied to the degrees of freedom. A significant main effect of time was observed (FGG_Correction = 64.307, p<0.001, η2=0.247), indicating that the SNAP-IV scores significantly changed over the course of the study. However, the main effect of the group was not statistically significant (F(1, 83) = 2.494, p=0.118, η2=0.013), suggesting no overall difference in symptom severity between the experimental and control groups across time.
The post-hoc comparisons using Tukey’s method revealed no significant differences in SNAP-IV scores between the two groups at baseline, week eight, or week 12. The within-group analysis revealed that both groups experienced a significant reduction in SNAP-IV scores between baseline and week four (experimental group: p<0.001, Cohen’s d=1.099, 95% CI: 0.497 to 1.683; control group: p<0.001, Cohen’s d=1.090, 95% CI: 0.521 to 1.676). However, no additional significant changes were observed from week four to week eight, or from week eight to week 12 in either group (Figure 2).
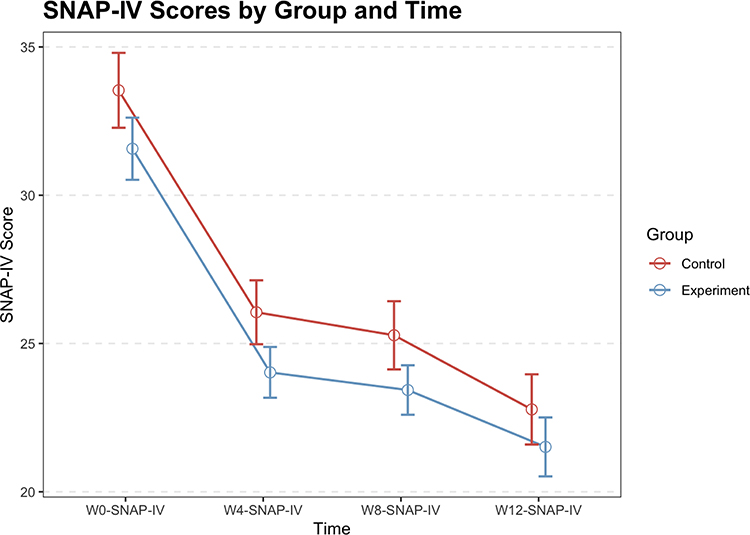 |
Figure 2 Swanson, Nolan, and Pelham Rating Scale, Fourth Edition (SNAP-IV) scores over time for the control and experimental groups. No significant between-group differences were detected at week four, week eight, or week 12. |
Functional Impairment (Weiss Functional Impairment Rating Scale [WFIRS]) Score Changes
The analysis of functional impairment using WFIRS revealed a violation of the sphericity assumption (W<0.75), prompting the application of GG correction. Furthermore, the significant main effect of time was identified (FGG_Correction=17.480, p<0.001, η2=0.074), indicating meaningful changes in functional impairment over time. However, the main effect of the group was not significant (F(1, 83)=0.717, p=0.399, η2=0.005), suggesting comparable levels of functional improvement between the experimental and control groups.
Tukey’s post-hoc analysis revealed no significant between-group differences at baseline, week eight, or week 12. The within-group analyses revealed that the control group experienced a significant improvement in functional impairment from baseline to week four (p<0.001, Cohen’s d=0.768, 95% CI: 0.234 to 1.302), with no further significant changes observed between week four and week eight, or between week eight and week 12. The experimental group similarly revealed a significant improvement from baseline to week four (p=0.022, Cohen’s d=0.506, 95% CI: 0.008 to 1.005), but no significant changes occurred thereafter (Figure 3).
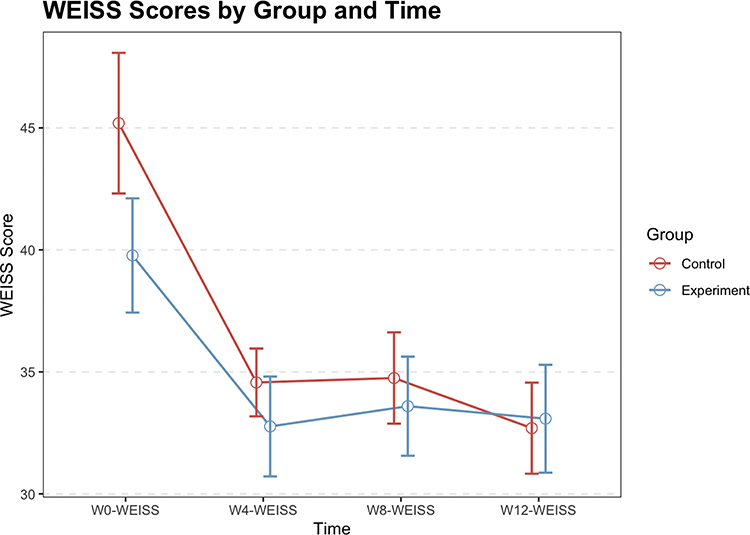 |
Figure 3 Weiss Functional Impairment Rating Scale (WFIRS) scores over time for the control and experimental groups. No significant differences were observed between the experimental and control groups at week four, week eight, or week 12. |
Clinical Global Impression-Severity Score Changes
Mixed repeated-measures ANOVA was performed to assess the changes in CGI-S scores over time between the two groups. The assumption of sphericity was met, and no correction was required. The analysis revealed the significant main effects of time (F=44.978, p<0.001, η2=0.235). The significant time effect suggested that the CGI-S scores meaningfully changed across the study period. The main effect of group was statistically significant (p = 0.012), indicating an overall difference between the intervention and control groups across all time points. However, post-hoc comparisons at individual time points did not show statistically significant differences once adjustments for multiple testing were applied.
The within-group analysis revealed that both groups experienced significant reductions in CGI-S scores from baseline to week four (control group: p<0.001, Cohen’s d=0.889, 95% CI: 0.237 to 1.542; experimental group: p<0.001, Cohen’s d=0.930, 95% CI: 0.294 to 1.566). However, no further significant changes were observed between groups at week four (Cohen’s d=0.308, 95% CI: −0.380 to 0.997), week eight (Cohen’s d=0.379, 95% CI: −0.311 to 1.070) or week twelve (Cohen’s d=0.480, 95% CI: −0.214 to 1.174), indicating that the greatest symptom improvement occurred during the initial treatment phase (Figure 4).
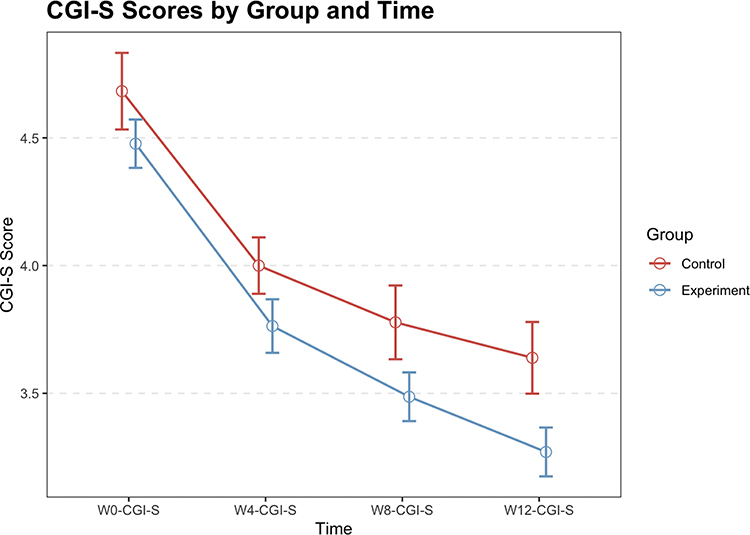 |
Figure 4 Clinical Global Impressions-Severity (CGI-S) scores over time for the control and experimental groups. No significant between-group differences were observed at week four, week eight, or week 12. |
Neurocognitive Performance (TOVA) Score Changes
The analysis of objective attentional performance using TOVA revealed a violation of sphericity assumption, as indicated by Mauchly’s test (W>0.75). Accordingly, GG corrections were applied to the degrees of freedom. The main effect of time was not statistically significant (FGG_Correction = 1.059, p=0.361), suggesting that, overall, the TOVA scores did not significantly change across the four assessment time points.
However, the significant main effect of the group was observed (F(1, 83)=8.478, p=0.005, η2=0.063), indicating a meaningful difference in attentional performance between the experimental and control groups across the study period. Although no significant between-group differences were detected at baseline, week four, or week 12, a statistically significant advantage for the experimental group emerged at week eight (p=0.006, Cohen’s d=0.809, 95% CI: 0.092 to 1.527), reflecting the enhanced neurocognitive outcomes associated with the combined digital therapy and pharmacological intervention.
The within-group comparisons revealed no significant changes in TOVA scores over time for either group. Neither the control nor the experimental group exhibited significant improvements between baseline and week four, between week four and week eight, or between week eight and week 12. These results suggest that although subjective symptom improvements occurred early in treatment, objective neurocognitive enhancement was more pronounced at the mid-point (week eight) in participants who received the combined intervention (Figure 5).
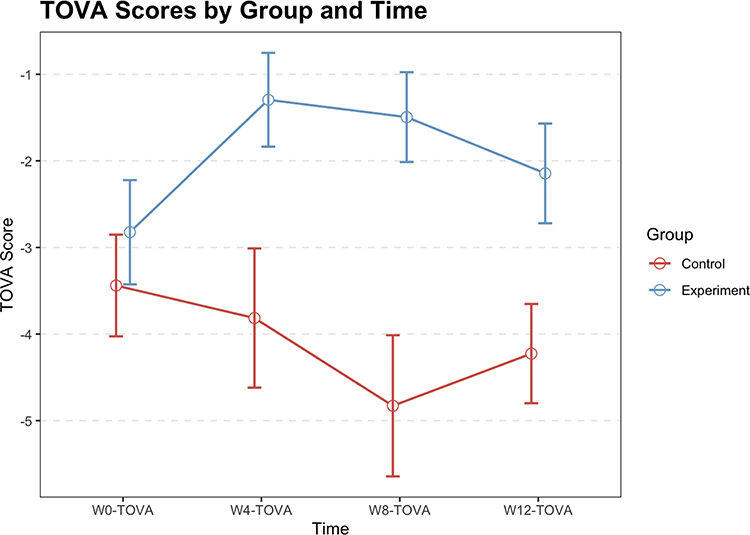 |
Figure 5 Test of Variables of Attention (TOVA) scores over time for the control and experimental groups. A significant difference was observed between the experimental and control groups at week eight (p=0.006), while no significant differences were found at baseline, week four, or week 12. No within-group differences were detected across any of the time points. |
Discussion
The present study explored the potential of a novel adaptive DTx platform, which was delivered via portable tablet devices and driven by intelligent algorithms, in order to augment pharmacological treatment in pediatric ADHD. By tailoring task difficulty and interface dynamics to the developmental profile of younger users, the system offers an individualized therapeutic experience that enhances engagement, and may influence core neurocognitive processes. Although the intervention’s impact was not consistently captured by parent-reported subjective scales, improvements in objective cognitive outcomes, such as those measured by TOVA, suggested that adaptive digital approaches may provide unique neurocognitive benefits beyond those conferred by medication alone.
The critical innovation of this digital intervention lies in its use of dynamic difficulty adjustment. Unlike traditional fixed-intervention platforms, this system continuously adapts to the user’s evolving cognitive state, providing a personalized challenge calibrated to skill level, attentional fluctuations, and task engagement. Prior research has demonstrated the superiority of such adaptive formats over static models, particularly in enhancing visual attention and response control.15 The ability to modulate difficulty in real-time not only sustains immersion, but also supports attentional persistence, which is a known limitation in children with ADHD. This feature aligns with prior findings, indicating that dynamic, gamified experiences promote motivation, which is a critical factor for therapeutic adherence and neuroplastic engagement.
The integration of gamification into neuropsychological rehabilitation has shown growing promise, offering an engaging and immersive format that fosters active participation. Game-based interventions capitalize on fundamental psychological mechanisms (goal setting, reward feedback, and skill progression), thereby enhancing treatment adherence and reinforcing therapeutic goals. These design elements mirror motivational strategies observed in successful behavioral interventions, and extend these into the digital realm, allowing for consistent, scalable delivery. Importantly, digital platforms offer the potential to incorporate social components, facilitating peer support and clinician interaction, both of which have been shown to enhance outcomes in youth mental health settings.
Broader literature supports the inclusion of psychosocial and behavioral interventions as first-line treatments for ADHD, particularly in combination with pharmacotherapy.25 The present findings contribute to this growing body of work by highlighting how DTx, particularly those that employ adaptive, game-based strategies, can serve as effective adjuncts. Notably, the present study adds to recent meta-analytic evidence, demonstrating that digital interventions can meaningfully enhance executive function (effect size=0.71, 95% CI: 0.37–1.04) and working memory (effect size=0.48, 95% CI: 0.21–0.76), which are outcomes that are closely tied to academic and behavioral functioning.16
Interestingly, the benefits of digital therapy in the present study appeared to persist even after the active intervention period. At four weeks, post-intervention, children who received the combined digital and pharmacologic treatment maintained superior performance on objective cognitive tests, when compared to children who received the medication alone. This suggests that adaptive digital interventions may help consolidate or extend treatment gains, potentially by reinforcing the underlying neurocognitive circuits involved in attention and executive regulation. Such sustained effects underscore the potential of DTx to offer not just symptomatic relief but also enduring functional improvements.
However, this enhanced performance was not paralleled by the differences in parent-rated outcomes, such as the SNAP-IV, WFIRS, or CGI-S scales. Similar discrepancies have been noted in previous studies,26 in which game-based digital therapies improved objective attention measures without significantly altering subjective ratings. Several possible explanations may account for this divergence. First, subjective ratings are often influenced by observer bias, expectancy effects, and contextual factors unrelated to neurocognitive change. Second, objective tools, such as TOVA, specifically target attentional control and inhibitory function, which are core domains that may be more sensitive to subtle changes induced by digital engagement. Third, the congruence between the demands of TOVA and digital training tasks may have led to task-specific performance enhancements, reflecting a degree of near transfer.
Neurophysiological regulation is shaped by multiple interacting factors, and individual heterogeneity can exert complex and bidirectional effects on treatment outcomes. For example, motivational deficits in ADHD involve intricate neural mechanisms: neuroimaging studies have shown altered reward circuitry, including reduced reward sensitivity in the ventral striatum and orbitofrontal cortex,27 as well as heightened amygdala responsiveness to delayed rewards.28 Clinical improvements in ADHD symptoms do not always correspond to neurophysiological changes, in part because treatment response varies across individuals. Consequently, incorporating a neuropsychological dimension into the diagnostic process has been proposed to better identify cognitive, motivational, and energetic subtypes.29–31 In addition, common comorbidities such as learning disabilities must be considered, as they may complicate intervention strategies that require substantial learning or adaptation.32
The digital therapeutic approach in this study is grounded in the premise that computer-based cognitive training can remediate core neuropsychological deficits in ADHD. It aims to enhance key cognitive processes, including processing speed, working memory, and inhibitory control, thereby facilitating the targeted modulation of brain networks.33 These interventions operate on the principle of “brain training”: repeated activation of specific cognitive resources promotes structural plasticity and helps address fundamental deficits in ADHD, producing strengthening effects analogous to physical exercise.34 Behavioral genetics research further shows that ADHD symptoms, along with related cognitive and motivational deficits, frequently co-occur within families.35 If such deficits mediate causal risk for ADHD, then interventions that directly target and improve the underlying neural circuits should, in principle, lead to clinical improvement.
The mechanisms through which digital interventions ameliorate ADHD symptoms appear to involve two phases. The first phase is marked by broad but transient effects, reflected in increased activation of brain regions directly involved in the cognitive tasks used during training. These changes generally remain limited to the training period and do not persist afterward.36 The second phase involves more enduring neural modifications, including the reorganization of cortical representations and synaptic remodeling. This process is characterized by an expansion of activation areas accompanied by reduced activation intensity in task-related regions and decreased reliance on attentional control networks.37 Such reorganization produces qualitative network-level improvements, including reduced interference among competing resting-state networks. Structural changes in gray and white matter microstructure have also been documented, in some cases paralleling these functional adaptations.38 These structural modifications likely represent the most durable benefits of digital intervention–based cognitive training.
In addition, placebo-like effects cannot be ruled out. Increased attention and interaction inherent to digital therapy may have temporarily improved motivation or self-regulation, especially in a pediatric population that is highly responsive to novelty and feedback mechanisms. This possibility is further supported by the rapid early improvement observed in subjective ratings across both groups by week four, despite the absence of continued gains in objective performance thereafter. These patterns suggest that subjective and objective measures may tap into the distinct facets of therapeutic response, and highlight the need for multi-modal assessment strategies when evaluating novel interventions.
To address missing data and ensure the robustness of our findings, we selected the imputation method based on the specific characteristics of the dataset. Mean imputation was chosen after careful evaluation of the data structure. The dataset contained four discrete time points (weeks 0, 4, 8, and 12), and missingness followed a monotonic dropout pattern, meaning that once data were missing at any time point, all subsequent values for that participant were also missing. No intermittent missingness occurred. Under these conditions, linear extrapolation would rely on only two or three available time points and would likely introduce systematic bias by imposing trends that did not reflect the actual data. In addition, per-protocol analysis demonstrated nonlinear changes across time, with different magnitudes of change between weeks 0 to 4 and weeks 4 to 8, further indicating that linear imputation methods would distort the underlying trajectories.
To mitigate these issues, we used two complementary strategies: a per-protocol analysis that excluded all participants with missing values, and a mean imputation approach, applied as a practical form of multiple imputation, to retain more participants while minimizing bias. Given the study’s design, the monotonic dropout pattern, and the nonlinear structure of the observations, mean imputation was more appropriate than linear mixed models and provided a methodologically sound approach that aligned with the empirical characteristics of the data.
Taken together, these findings support the therapeutic potential of adaptive digital interventions in the management of pediatric ADHD. Furthermore, these highlight the importance of integrating objective cognitive assessments alongside traditional scales to more fully capture intervention effects. Future research should aim to further delineate the mechanisms of action underlying DTx, examine the long-term maintenance of gains, and explore how these tools can be optimized for individualized, developmentally appropriate care.
Limitations
The present study has several limitations. First, the data collection overlapped with the coronavirus disease 2019 (COVID-19) pandemic, which forced a shift from in-person to online assessments, and led to a higher dropout rate. This may have affected data completeness, and reduced the statistical power. Second, as a single-center study, the findings may not be generalized to broader populations. A larger multi-center trial would help confirm these results. In addition, DTx remains an emerging field, and there are challenges in applying traditional evaluation methods to this novel approach. While digital tools hold significant promise, refinements are still needed to support their seamless integration into real-world clinical practice and to strengthen their ecological validity. Continued development will be essential to enhance their practicality and effectiveness in everyday healthcare settings. Future research should incorporate comprehensive qualitative measures, especially because our participants are children who are still developing their expressive abilities and the accuracy with which they convey their perceptions. It is therefore important to continually reassess assumptions about usability and user experience from the child’s perspective. This approach will help reduce interpretative bias introduced by externally imposed frameworks and improve the reliability of the findings. Such efforts will provide a strong foundation for designing more effective digital therapeutics tailored to pediatric populations.
Collectively, these strategies will inform more robust intervention design and elevate the quality of evidence guiding the application of digital health technologies in clinical care.
Data Sharing Statement
The data supporting this study’s findings are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
Ethics approval was obtained from the Medical Ethics Committee of West China Second University Hospital, Sichuan University (Approval no. 2022-176). A written informed consent was secured from all participants and their legal guardians. The study was registered with the Chinese Clinical Trial Registry (ChiCTR2200064983).
Acknowledgments
We would like to thank Xuejing Chen for the technical support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Chengdu Medical Research Project (No. 2023003) and the Sichuan Provincial Department of Science and Technology Regional Innovation Cooperation Project (No. 2020YFQ0021).
Disclosure
Sihan Wang was employed by NeuroWeave Co., Ltd., Shanghai. Author Xiang Chen is affiliated with Fangcun Quanxiang (Beijing) Technology Company, which develops digital therapeutic tools for ADHD. This affiliation is disclosed for transparency. The company had no influence on the study design, data analysis, or interpretation of results. The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as potential conflicts of interest.
References
1. American Psychiatric Association (APA). Diagnostic and Statistical Manual of Mental Disorders (DSM-5®). American Psychiatric Publishing; 2013.
2. Ayano G, Demelash S, Gizachew Y, Tsegay L, Alati R. The global prevalence of attention deficit hyperactivity disorder in children and adolescents: an umbrella review of meta-analyses. J Affect Disord. 2023;339:860–14. doi:10.1016/j.jad.2023.07.071
3. Conners CK, Epstein JN, March JS, et al. Multimodal treatment of ADHD in the MTA: an alternative outcome analysis. J Am Acad Child Adolesc Psychiatry. 2001;40(2):159–167. doi:10.1097/00004583-200102000-00010
4. Gross MD. Origin of stimulant use for treatment of attention deficit disorder. Am J Psychiatry. 1995;152(2):298–299.
5. Safren SA, Otto MW, Sprich S, Winett CL, Wilens TE, Biederman J. Cognitive-behavioral therapy for ADHD in medication-treated adults with continued symptoms. Behav Res Ther. 2005;43(7):831–842. doi:10.1016/j.brat.2004.07.001
6. Barkley RA. Defiant Children: A Clinician’s Manual for Assessment and Parent Training.
7. Barkley RA. Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis and Treatment.
8. Antshel KM, Olszewski AK. Cognitive behavioral therapy for adolescents with ADHD. Child Adolesc Psychiatr Clin N Am. 2014;23(4):825–842. doi:10.1016/j.chc.2014.05.001
9. Digital Therapeutics Alliance. 2020. Available from: https://dtxalliance.org.
10. Corrigan N, Păsărelu CR, Voinescu A. Immersive virtual reality for improving cognitive deficits in children with ADHD: a systematic review and meta-analysis. Virtual Real. 2023;1–20. doi:10.1007/s10055-023-00768-1
11. Bruce CR, Unsworth CA, Dillon MP, et al. Hazard perception skills of young drivers with Attention Deficit Hyperactivity Disorder (ADHD) can be improved with computer based driver training: an exploratory randomised controlled trial. Accid Anal Prev. 2017;109:70–77. doi:10.1016/j.aap.2017.10.002
12. Ayearst LE, Brancaccio RM, Weiss MD. Improving on-task behavior in children and youth with ADHD: wearable technology as a possible solution. J Pediatr Neuropsychol. 2023;9(4):175–182. doi:10.1007/s40817-023-00152-6
13. Williams L, Hall CL, Brown S, et al. Optimising medication management in children and young people with ADHD using a computerised test (QbTest): a feasibility randomised controlled trial. Pilot Feasibility Stud. 2021;7(1):68. doi:10.1186/s40814-021-00788-1
14. Larsen LB, Daley D, Lange AM, Sonuga-Barke E, Thomsen PH, Rask CU. Effect of parent training on health-related quality of life in preschool children with attention-deficit/hyperactivity disorder: a secondary analysis of data from a randomized controlled trial. J Am Acad Child Adolesc Psychiatry. 2021;60(6):734–744.e733. doi:10.1016/j.jaac.2020.04.014
15. Kollins SH, DeLoss DJ, Cañadas E, et al. A novel digital intervention for actively reducing severity of paediatric ADHD (STARS-ADHD): a randomised controlled trial. Lancet Digit Health. 2020;2(4):e168–e178. doi:10.1016/S2589-7500(20)30017-0
16. Oh S, Choi J, Han DH, Kim E. Effects of game-based digital therapeutics on attention deficit hyperactivity disorder in children and adolescents as assessed by parents or teachers: a systematic review and meta-analysis. Eur Child Adolesc Psychiatry. 2024;33(2):481–493. doi:10.1007/s00787-023-02174-z
17. Luna B. Developmental changes in cognitive control through adolescence. Adv Child Dev Behav. 2009;37:233–278.
18. Kargar N, Choobineh AR, Razeghi M, Keshavarzi S, Meftahi N. Posture and discomfort assessment in computer users while using touch screen device as compared with mouse-keyboard and touch pad-keyboard. Work. 2018;59(3):341–349. doi:10.3233/WOR-182685
19. Quinn JT, Schmidt RA, Zelaznik HN. Target-size influences on reaction time with movement time controlled. J Mot Behav. 1980;12(4):239–261. doi:10.1080/00222895.1980.10735224
20. Swanson JM. School-Based Assessments and Interventions for ADD Students. Irvine, CA: K.C. publishing; 1992.
21. Leon AC, Shear MK, Klerman GL, Portera L, Rosenbaum JF, Goldenberg I. A comparison of symptom determinants of patient and clinician global ratings in patients with panic disorder and depression. J Clin Psychopharmacol. 1993;13(5):327–331. doi:10.1097/00004714-199310000-00005
22. Leark RA, Greenberg LK, Kindschi CL, Dupuy TR, Hughes SJ. Test of Variables of Attention: Clinical Manual. Los Alamitos, CA: The TOVA Company; 2007.
23. Girden ER. ANOVA: Repeated Measures. Sage Publications, Inc.; 1992.
24. Barretto Dos Santos Lopes Batista K, Thiruvenkatachari B, O’Brien K. Intention-to-treat analysis: are we managing dropouts and missing data properly in research on orthodontic treatment? A systematic review. Am J Orthod Dentofacial Orthop. 2019;155(1):19–27.e13. doi:10.1016/j.ajodo.2018.08.013
25. Shrestha M, Lautenschleger J, Soares N. Non-pharmacologic management of attention-deficit/hyperactivity disorder in children and adolescents: a review. Transl Pediatr. 2020;9(Suppl 1):S114–s124. doi:10.21037/tp.2019.10.01
26. Sun TH, Yeom JW, Choi KY, et al. Potential effectiveness of digital therapeutics specialized in executive functions as adjunctive treatment for clinical symptoms of attention-deficit/hyperactivity disorder: a feasibility study. Front Psychiatry. 2023;14:1169030. doi:10.3389/fpsyt.2023.1169030
27. Plichta MM, Scheres A. Ventral-striatal responsiveness during reward anticipation in ADHD and its relation to trait impulsivity in the healthy population: a meta-analytic review of the fMRI literature. Neurosci Biobehav Rev. 2014;38:125–134. doi:10.1016/j.neubiorev.2013.07.012
28. Lemiere J, Danckaerts M, Van Hecke W, et al. Brain activation to cues predicting inescapable delay in adolescent Attention Deficit/Hyperactivity Disorder: an fMRI pilot study. Brain Res. 2012;1450:57–66. doi:10.1016/j.brainres.2012.02.027
29. de Zeeuw P, Weusten J, van Dijk S, van Belle J, Durston S. Deficits in cognitive control, timing and reward sensitivity appear to be dissociable in ADHD. PLoS One. 2012;7(12):e51416. doi:10.1371/journal.pone.0051416
30. Fair DA, Bathula D, Nikolas MA, Nigg JT. Distinct neuropsychological subgroups in typically developing youth inform heterogeneity in children with ADHD. Proc Natl Acad Sci U S A. 2012;109(17):6769–6774. doi:10.1073/pnas.1115365109
31. Lambek R, Tannock R, Dalsgaard S, Trillingsgaard A, Damm D, Thomsen PH. Validating neuropsychological subtypes of ADHD: how do children with and without an executive function deficit differ? J Child Psychol Psychiatr. 2010;51(8):895–904. doi:10.1111/j.1469-7610.2010.02248.x
32. Coghill D, Banaschewski T, Cortese S, et al. The management of ADHD in children and adolescents: bringing evidence to the clinic: perspective from the European ADHD Guidelines Group (EAGG). Eur Child Adolesc Psychiatry. 2023;32(8):1337–1361.
33. Willis SL, Schaie KW. Cognitive training and plasticity: theoretical perspective and methodological consequences. Restor Neurol Neurosci. 2009;27(5):375–389. doi:10.3233/RNN-2009-0527
34. Sonuga-Barke E, Brandeis D, Holtmann M, Cortese S. Computer-based cognitive training for ADHD: a review of current evidence. Child Adolesc Psychiatr Clin N Am. 2014;23(4):807–824. doi:10.1016/j.chc.2014.05.009
35. Kuntsi J, Pinto R, Price TS, van der Meere JJ, Frazier-Wood AC, Asherson P. The separation of ADHD inattention and hyperactivity-impulsivity symptoms: pathways from genetic effects to cognitive impairments and symptoms. J Abnorm Child Psychol. 2014;42(1):127–136. doi:10.1007/s10802-013-9771-7
36. Vinogradov S, Fisher M, de Villers-Sidani E. Cognitive training for impaired neural systems in neuropsychiatric illness. Neuropsychopharmacology. 2012;37(1):43–76. doi:10.1038/npp.2011.251
37. Olesen PJ, Westerberg H, Klingberg T. Increased prefrontal and parietal activity after training of working memory. Nat Neurosci. 2004;7(1):75–79. doi:10.1038/nn1165
38. Takeuchi H, Sekiguchi A, Taki Y, et al. Training of working memory impacts structural connectivity. J Neurosci. 2010;30(9):3297–3303. doi:10.1523/JNEUROSCI.4611-09.2010
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Effect of Drug Holidays on Metacognitive and Theory of Mind Skills of Children Diagnosed with Attention Deficit Hyperactivity Disorder: Preliminary Findings
Köksal M, Sari M, İmrek Y, Öztürk Y, Özyurt G, Tufan AE
Neuropsychiatric Disease and Treatment 2026, 22:573124
Published Date: 3 July 2026