Back to Journals » Infection and Drug Resistance » Volume 16
A PCR-Reverse Dot Blot Hybridization Based Microfluidics Detection System for the Rapid Identification of 13 Fungal Pathogens Directly After Blood Cultures Over a Period of Time
Authors Lin C, Tang H, Hu X, Li G, Jiang T, Yang W, Xia Z, Zhu Y ![]() , Xu H, Zhou J, Shen J
, Xu H, Zhou J, Shen J ![]()
Received 3 June 2023
Accepted for publication 9 August 2023
Published 16 August 2023 Volume 2023:16 Pages 5347—5357
DOI https://doi.org/10.2147/IDR.S424156
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Chunhui Lin,1,2,* Hao Tang,3,* Xinyi Hu,1,2 Ge Li,1,2 Tong Jiang,1,2 Wensu Yang,1,2 Zhaoxin Xia,1,2 Yi Zhu,1,2 Huaming Xu,4 Jing Zhou,1,2 Jilu Shen1,2
1Clinical Laboratory, the First Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 2Clinical Laboratory, Anhui Public Health Clinical Center Hefei, Hefei, People’s Republic of China; 3Clinical Laboratory, the Second Affiliated Hospital of Anhui Medical University, Hefei, People’s Republic of China; 4Clinical Laboratory, the First Affiliated Hospital of Anhui University of Traditional Chinese Medicine, Hefei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jilu Shen, Tel +86 151 5515 2963, Email [email protected]
Introduction: It is time-consuming to identify fungal pathogens from positive blood cultures using the standard culture-based method. And delayed diagnosis of bloodstream infection leads to significantly increased mortality.
Methods: We developed a PCR-reverse dot blot hybridization combined with microfluidic chip techniques to rapidly identify 13 fungal pathogens within 3– 4 h using the sample of blood cultured over a period of time.
Results: We performed clinical validation using 43 blood culture-positive samples with a sensitivity of 96.7%, a specificity of 100%, and a concordance rate of 97.7%. Samples with different culture durations were evaluated using our approach, showing a detection rate of 85.2% at 16 h and 96.3% at 24 h; the platform could reach a detection limit of 103cfu/mL for the Candida spp. and 103 copies/mL for Aspergillus spp.
Discussion: The detection rate of the platform is much higher than the positive rates of concurrent blood cultures. This method bears substantial clinical application potential as it incorporates the microfluidic platform with low reagent consumption, automation, and low cost (about 10 dollars).
Keywords: fungemia, bloodstream infection, microfluidics, Candida auris, PCR-reverse dot blot hybridization
Introduction
Fungemia is a severe invasive fungal infection. Since the early 1990s, the incidence of sepsis caused by fungi has been growing.1 Presently, it has become a dominant cause of clinical bloodstream infection, among which candidemia is the most common.2 Research data showed that the mortality rate of candidemia is 15–35% in adults and 10–15% in newborns, reaching 60% in patients from the intensive care unit.3 Additionally, a multi-institution study revealed that delayed diagnosis of fungemia was associated with a considerable surge in mortality rates, with early and late mortality rates (7 and 30 days after diagnosis) of 13% and 30%, respectively. Moreover, mortality elevation was correlated with delayed initiation of antifungal therapy.2,4 In recent years, in addition to common pathogens like Candida albicans, Candida glabrata, and Candida tropicalis, bloodstream infections caused by other infrequent fungi have been on the rise.5 Such as Candida krusei, have natural resistance to common antifungal agents (eg, fluconazole, ketoconazole).6 Candida auris is a “super fungus” resistant to various drugs,7 so early swift identification of pathogenic fungi can effectively facilitate clinical treatment and drug selection.
Detecting pathogens from blood samples using the blood culture technique is still considered the “golden standard” for diagnosing bloodstream infection.8 However according to studies, the average positive time of Candida spp. is 48.9 h.9 In addition, blood culture needs an additional 24–48 hours to grow on the medium for identification after reporting positive. It takes longer for multiple fungal infections and is easy to miss.10 The serological examination (1,3-β-D glucan test and Galactomannitol antigen test) can help with early fungemia diagnosis to a certain extent, but it can only diagnose the genus category and cannot determine the specific species. Moreover, false positives and false negatives are predisposed to occur due to exogenous influence.11 With the constant development of molecular diagnostic technologies, increasing studies endeavor to replace cumbersome conventional culture methods with molecular techniques. Over the past few years, nucleic acid amplification tests (NAATs) have attempted to evade bacterial culture and directly extract DNA from whole blood to identify bacterial species. The Iridica Plex ID12 platform identifies sequences by multiplex PCR amplification combined with ESI-MS to confirm species; SeptiFast13 (Roche Diagnostics), a multiplex fluorescent PCR linked to probe hybridization and DNA melting analysis, distinguishes species in the same detection channel via melting temperature analysis. Nevertheless, these approaches with direct molecular detection in primary samples present low sensitivity due to low pathogen load, high background DNA content, and co-extracts interfering with or restraining the PCR reaction. Hence, diagnosis directly using whole blood without incubation remains challenging. Almost all FDA-approved molecular diagnostic tests for sepsis are post-culture techniques,8 meaning blood samples must be cultured for proliferation before diagnostic tests. In addition, several commercial kits can detect partial Saccharomyces from positive blood culture bottles, such as the PhenoTest blood culture kit14 and Candida PNA FISH assay.15 The former only targets Candida albicans and Candida glabrata, while the latter can detect Candida albicans, Candida glabrata, Candida tropicalis, Candida parapsilosis, and Candida krusei. However, the detection range is narrow, easily causing missed detection.
In this study, we adopted PCR-reverse dot blot hybridization combined microfluidic chip technology to directly detect the sample of blood cultured over a period of time. 13 species of Candida albicans, Candida glabrata, Candida tropicalis, Candida parapsilosis, Candida krusei, Candida guilliermondii, Cryptococcus neoformans, Candida lusitaniae, Candida dubliniensis, Rhodotorula dairenensis, Penicillium marneffei, Aspergillus fumigatus, and Candida auris were included. The 13 fungi were selected based on date from China Hospital Invasive Fungal Surveillance Net (CHIF-NET),16,17 including most of the strains currently circulating in China, in addition to the list of fungi of great need published by the World Health Organization.18
The microfluidic system integrates with multiple functions of the traditional molecular laboratory. Additionally, it incorporates nucleic acid extraction, PCR amplification, and PCR-reverse dot blot hybridization with microarray into a microfluidic plate made of polystyrene (PS). Functional areas interconnected through microchannels and microvalves, micropumps, micromixers, reaction chambers, and detectors were operated by customized operating platforms.19 During the experiment, all sorts of reagents were automatically added. Nucleic acid extraction, amplification, and hybridization were orderly combined, and all reactions were completed in a microfluidic chip, reducing the pollution possibility caused by separate operations. The reaction time is considerably shortened with decreased reagent usage. Moreover, the hybridization sensitivity is substantially advanced due to the high surface area-to-volume ratio in the nano-solution volume microchannel.20,21 And Compared with conventional culture methods that inoculated on solid medium after positive blood culture, a single colony was grown for matrix assisted laser desorption/ionization-time of flight mass spectrometry identification), the microfluidic chip provides a faster turnaround time, and its detection target is blood samples that have been grown in blood culture bottles for a period of time, without the need to culture to positive.It may allow for earlier antifungal interventions.
Materials and Methods
Fungal Isolates and Clinical Samples
A total of 43 samples were collected in this study, of which 34 were blood culture positive, including 21 fungal blood culture positive and 13 bacterial blood culture positive, with 9 clinical fungal isolates (Table S1). All samples were cultured and identified by matrix assisted laser desorption/ionization-time of flight mass spectrometry (MALDI-TOF MS) (BRUKER, Germany). For strains that MALDI-TOF MS could not identify, we were submitted to Sangon Biotech (Shanghai) Co, Ltd. for ITS sequencing. All samples were sourced from Anhui Province Public Health Clinical Center and the First Affiliated Hospital of Anhui Medical University. Blood culture-positive samples and clinical isolates were stored at −80° for subsequent experiments. The study involved the anonymous use of excess, abandoned patient blood cultures, whole blood samples, and clinical fungal isolation as part of standard care, which did not affect patient health and privacy. All procedures involving human subjects were conducted under appropriate ethical standards released by the Fourth Affiliated Hospital of Anhui Medical University Committee (Reference No.: LISC20210802) and the 1964 Declaration of Helsinki and subsequent amendments or similar ethical standards.
Primers and Probes
It was illustrated that fungal ribosomal DNA complexes (18S, 5.8S, 28S) were highly conserved, and their transcribed spacer sequences (ITS1 and ITS2) were highly specific.22 A universal primer reported by Zeng et al22 was applied and labeled with biotin at the 5 ‘end. A specific probe was devised for ITS1 and ITS2 using primer premier 5, and it was modified at 3′ with an Amine-C6 group. In addition, the human β-globin gene was employed as the internal reference. We cited primers from the literature by Wang et al.23 All gene sequences of different fungi and β-globin gene sequences were obtained from NCBI. The Shanghai Sangon Biotech Co., Ltd synthesized primers and probes. Sequences are shown in Table 1.
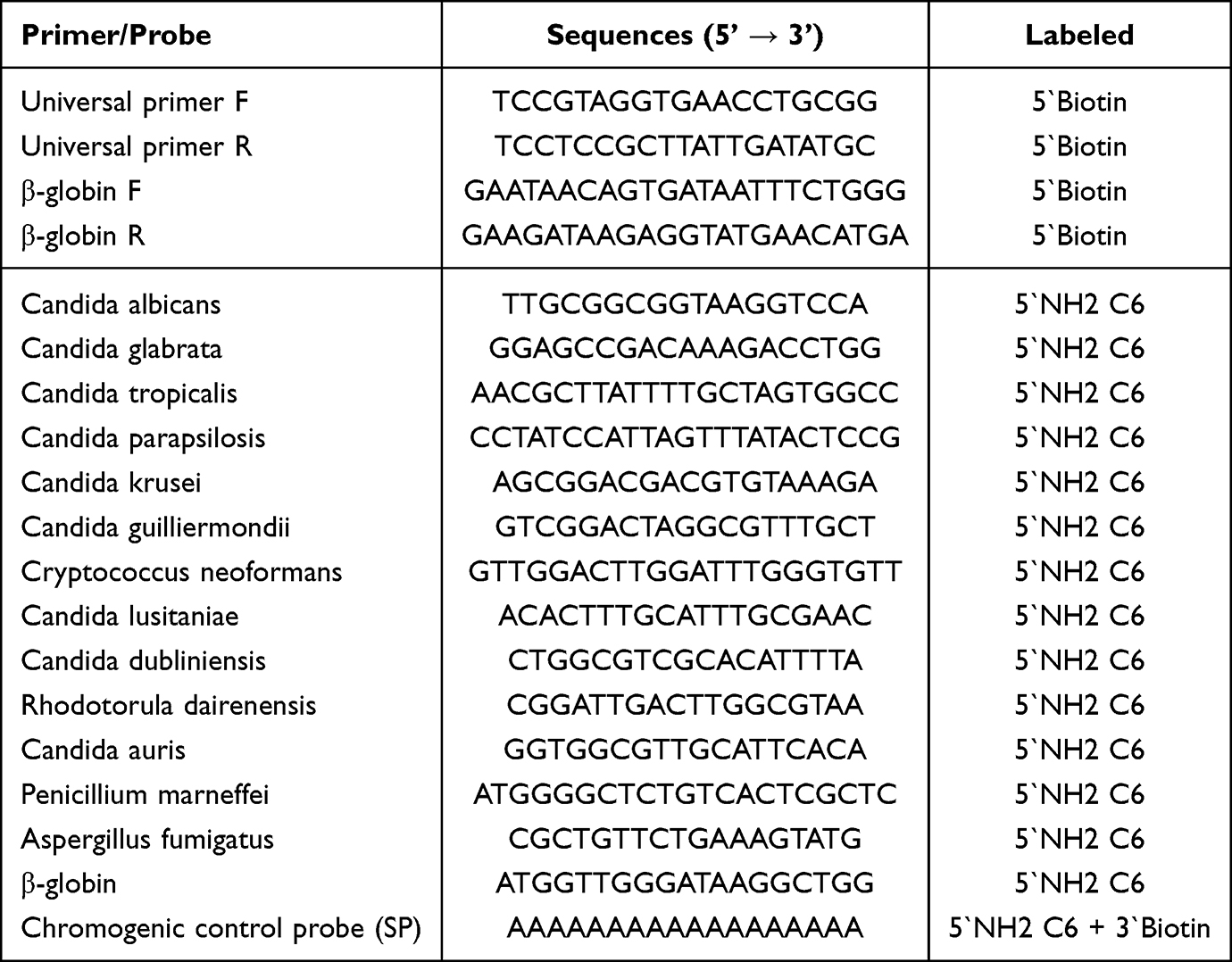 |
Table 1 Fungal Universal Primers and Specific Probes and Internal Reference Primers and Probes |
Microfluidic System
The main body of the fully automatic microfluidic chip is made of polystyrene(PS). Each sample reservoir is composed of PS substrates in the middle of the chip, and both sides are wrapped by PS film so that each sample reservoir is an enclosed structure for easy external control (Figure 1A). This chip contains three functional areas (Figure 1B). A nucleic acid extraction area: lysing fungi to release DNA, capturing and rinsing DNA with silicon-based magnetic beads, and eluting DNA bound to silicon-based magnetic beads; a PCR amplification area: pumping the eluted DNA into a PCR tube in the chip for amplification; a product hybridization analysis area: the DNA microarray in the hybridization area is a nylon membrane with high-density carboxyl groups on the surface. After being activated by 16% carbodiimide hydrochloride (EDAC), it is coupled with a specific probe modified by C6 amine to fix the probe on the surface. After amplification, PCR products were denatured into single-stranded DNA, transferred to the hybridization area, and hybridized with specific probes immobilized on the DNA microarray for color development. A corresponding control system is externally equipped to realize the regular operation of each functional area and the functional association, comprising a chip interface system, a gas source pressure controller, a temperature control component, and an image scanning component. The embedded chip interface system controls fluids in the microfluidic chip, and the bottom is welded to the gas source pressure controller. Air pressure regulation-induced PS film variation controls the liquid flow (Figure 1C). Chip fabrication and software programming were all entrusted to Beijing Bohui Innovation Biotechnology Co., Ltd.
 |
Figure 1 (A) 3D model of a custom microfluidic chip; (B) the microfluidic chip mainly includes three functional areas: DNA extraction region, PCR amplification region and hybrid analysis area; (C) the flow of microfluidics in the microfluidic chip is controlled by air pressure, when positive pressure is given, the valve closes the liquid and stops flowing, and when negative pressure is given, the valve opens and the liquid flows; (D) operation platform Genplex, including ① tube rack for placing reagents, ② microfluidic chip placement, ③ robotic arm for automatic dosing controlled by program, ④ CCD camera to take pictures to export results; (E) principle of reverse spot hybridization. |
Sample Preparation
Based on the designed automatic microfluidic platform, 13 kinds of pathogenic fungi were detected, and in addition, the specificity of 8 kinds of bacteria common in clinical bloodstream infection was verified. All pathogenic fungi and bacteria were adjusted to 0.5 McFarland turbidity. The fungal and bacterial suspension (100 μL) was mixed with 900 μL of blood and injected into a blood culture bottle for incubation. After the blood culture positivity and sample preprocessing, the samples were tested with the detection platform.
Workflow of the Microfluidic System
Sample preprocessing: blood culture medium (1 mL) was supplemented into a centrifuge tube via a pipette after blood culture, centrifuged at 12,000 r/min for 10 min with supernatant discarded. 200μL PBS buffer was added, shaken, and mixed well for later use.
All operations in this study were completed by the Genplex platform (BOHUI, Beijing). Before testing, all pre-prepared reagents were placed in corresponding wells, and the program was initiated. Genplex automatically distributed the reagents to each fungal test chip according to the program setting (Figure 1D and E). The chip operated according to the following steps:
Nucleic acid extraction: Treated samples were added with lysate and proteinase K and incubated at 37 °C for 15 minutes. Silicon-based magnetic beads and isopropyl alcohol were supplemented to capture released DNA by lysis, rinsed with rinsing buffer I and II to remove impurities, and eluted with elution buffer to obtain sample DNA. Subsequently, sample DNA was pumped into a PCR tube for amplification.
PCR amplification: Pre-prepared amplification reagents (14 μL) and internal reference amplification reagents were added into PCR tubes 1 and 2, respectively, and mixed with the sample DNA from elution. Silicone oil (10μL) was supplemented into PCR tubes 1 and 2, respectively. The amplification process: 95 °C for 2 min, 94 °C for 30s, 55 °C for 30s, 72 °C for 1 min (30 cycles), 72 °C for 4 min.
Reverse dot blot hybridization and color development: Amplified PCR products were denatured at 95 °C for 5 min. Denatured single-stranded DNA was blended with the hybridization rinsing buffer (2×SSPE/0.1% SDS), pumped into the DNA microarray at 48 °C, and incubated for 10 min. Following chip washing three times (5 min each) with hybridization rinsing buffer, horseradish peroxidase (HRP)-labeled streptavidin was pumped to the microarray for incubation for 15 min. Subsequently, the chip was washed with the hybridization rinsing buffer 3 times for 5 min each, subjected to the TMB chromogenic solution for 10 min, and washed with deionized water 3 times for 2 min each.
Imaging system: After hybridization, the chip was scanned by the CCD camera (Genplex), and the results were exported. The species of bloodstream infection fungi were determined according to chromogenic sites, assisted by the gray value of each site from ImageJ software.
Statistical Methods
Sensitivity/positive percent agreement (PPA) and specificity/negative percent agreement (NPA) with comparator method results were determined for each targeted fungal organism detected by the microfluidic chip. Sensitivity/PPA was calculated as 100× number true positive (TP)/(number TP + number false negative [FN]), while specificity/NPA was calculated as 100× number true negative (TN)/(number TN + number false positive [FP]).
Results
Fully Automatic Microfluidic Platform Construction
This fully automated microfluidic platform for detecting fungal bloodstream infection consists of the nucleic acid extraction area, PCR amplification area, and hybridization analysis area. The universal primer can simultaneously amplify the target genes of 13 detected fungi (Figure 2A). Fungal species are determined according to different chromogenic sites of DNA microarray in the hybridization analysis area. We made designs targeting DNA microarray (Figure 2B).
 |
Figure 2 (A) Universal primers amplify electrophoresis bands for 13 fungi; (B) the point design of the DNA microarray, BC point is blank control, NC point is negative control, SP point is color development control, monitor whether the probe is successfully fixed on the microarray and the process of enzyme color development, GB point is the internal reference control, monitor the whole process of the reaction; 1. Candida albicans; 2. Candida glabrata; 3. Candida tropicalis; 4. Candida parapsilosis; 5. Candida krusei; 6. Candida guilliermondii; 7. Candida auris; 8. Aspergillus fumigatus; 9. Candida lusitaniae; 10. Penicillium marneffei; 11. Candida dubliniensis; 12. Cryptococcus neoformans; 13. Rhodotorula dairenensis. |
The results showed that the research platform can correctly detect the 13 species of fungi, and no cross reaction of 8 kinds of bacteria (Figure 3).
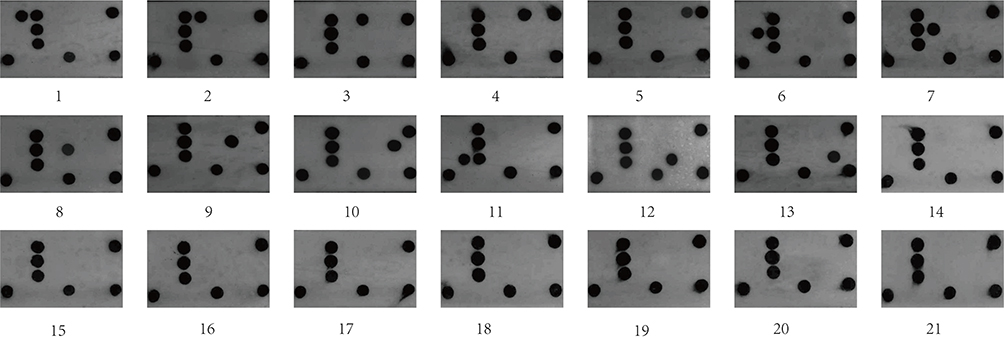 |
Figure 3 1. Candida albicans; 2. Candida glabrata; 3. Candida tropicalis; 4. Candida parapsilosis; 5. Candida krusei; 6. Candida guilliermondii; 7. Candida auris; 8. Aspergillus fumigatus; 9. Candida lusitaniae; 10. Penicillium marneffei; 11. Candida dubliniensis; 12. Cryptococcus neoformans; 13. Rhodotorula dairenensis; 14. E.coli; 15. Klebsiella pneumoniae; 16. Staphylococcus aureus; 17. Pseudomonas aeruginosa; 18. Streptococcus viridans; 19. Acinetobacter baumannii; 20. Enterococcus faecalis; 21. Enterococcus faecium. |
Condition Optimization
Reverse dot blot hybridization is the key technology of this detection platform. We optimized the conditions of reverse dot blot hybridization, including the best hybridization temperature and time. Given that Candida albicans is the most common opportunistic pathogen, it was chosen as a representative to optimize the hybridization conditions. Candida albicans samples with positive blood cultures were processed and examined. The temperature was set at 39 °C, 42 °C, 45 °C, 48 °C, and 51 °C respectively. The hybridization time was set at 30 min. After the detection, CGV was obtained by scanning for data analysis. According to the results, the optimal temperature was obtained and set with durations set as 10 min, 15 min, 20 min, 25 min, and 30 min. Following detection, CGV data were acquired via scanning and analyzed. Under different experimental conditions, no statistical difference between 48 °C and 42 °C, 45 °C and 51 °C was witnessed. Yet, our test results showed a higher gray value at 48 °C (Figure 4A), so we considered 48 °C the optimal reaction temperature. At 48 °C, different hybridization times (10–30 min) showed no statistical difference (Figure 4B). However, clinically, a shorter detection duration with an ideal outcome makes a better detection method. Thus, 10 min is the superior option. Finally, we set the optimal condition as a hybridization temperature of 48 °C and a hybridization time of 10 min.
 |
Figure 4 (A) The optimal temperature for hybridization was analyzed. The hybridization time was fixed at 30 min, and the temperature was set at 39 °C, 42 °C, 45 °C, 48 °C, and 51 °C, respectively. The bar chart represents CGV scanning results under different temperatures, and the data were expressed as mean ± SD (n = 4). One-way ANOVA was employed to compare 48 °C and 39 °C (**P<0.05), and there was no statistical difference between 48 °C and 42 °C, 45 °C and 51 °C; (B) the optimal time for hybridization was analyzed. The hybridization temperature was fixed at 48 °C, and the time was set at 10 min, 15 min, 20 min, 25 min, and 30 min. The histogram represents CGV scanning results at different times, and the data were expressed as mean ± SD (n = 4). No statistical difference was witnessed when using one-way ANOVA for comparison; (C) detection results of Candida albicans at 104 cfu/mL, 103 cfu/mL, and 102 cfu/mL; (D) detection results of Aspergillus fumigatus at 104 copies /mL, 103 copies /mL, and 102 copies /mL. |
Limit of Detection (LOD)
To evaluate the detection limit of the microfluidic detection platform for 13 pathogenic fungi, we selected Candida albicans to represent the Candida spp. and Aspergillus fumigatus to represent Aspergillus spp. A single colony was harvested from freshly cultured Candida albicans and diluted in normal saline to 0.5 McFarland turbidity. The optical density was 600 nm (OD600). The yeast was approximately equivalent to 1.0×106 cfu/mL at this time,24 then diluted to 104 cfu/mL, 103 cfu/mL, and 102 cfu/mL and mixed with an appropriate amount of blood as simulated samples standby. Considering Aspergillus fumigatus is a filamentous fungus and is unable to modulate turbidity, we constructed plasmid vectors containing the Aspergillus fumigatus gene, diluted the vectors to 104 copies /mL, 103 copies /mL, and 102 copies/mL and mixed them with an appropriate amount of blood to produce simulated samples. All backup samples were tested under optimal reaction conditions with two technical replicates per sample. The results indicated positivity with weak chromogenic dots at 103 cfu/mL and 103 copies /mL. The result was negative or the chromogenic dots were dim and extremely tough to interpret when the concentration was lower than the detection limit (Figure 4C and D). In addition, we tested all the remaining strains at 103 cfu/mL, exhibiting readable positive results (Figure S1).
Clinical Performance Validation
In order to evaluate the clinical performance of this method, we examined 43 samples collected and identified priorly (in which fungal isolates indicated blood culture positivity via artificial stimulation). The results revealed that (Figure 5A) (Figure S2), 29 of 30 fungal samples were correctly determined as positive, and 13 bacterial samples were detected as negative, with a sensitivity of 96.7%, specificity of 100%, and concordance rate of 97.7%. The missed sample was Aspergillus fumigatus, which denoted positivity after repeated detection (Table 2). In addition, to further shorten the detection process, we assessed blood cultures at 8 h, 16 h, and 24 h, respectively (Figures S3-S5). All samples were isolated strains from cultured clinical fungal samples above (except Aspergillus fumigatus and Penicillium marneffei). After incubating all isolates on Sabouraud medium for 48 h, suspensions were prepared and diluted to 10cfu/mL. 100μL of suspension was added into 900μL of blood. A blood culture was performed to simulate the average fungal concentration of sepsis patients (10 cfu/mL).25 The blood culture solution was tested at three different time intervals (8 h, 16 h, 24 h). After 8 h of culture (Figure 5B), the microfluidic platform indicated negative for all samples with negative blood culture results. At 16 h, the detection rate of the microfluidic platform was 85.2%, while blood cultures exhibited negativity. At 24 h, the detection rate of the microfluidic platform was 96.3%, and the positive rate of blood cultures was 55.6% (Table 3).
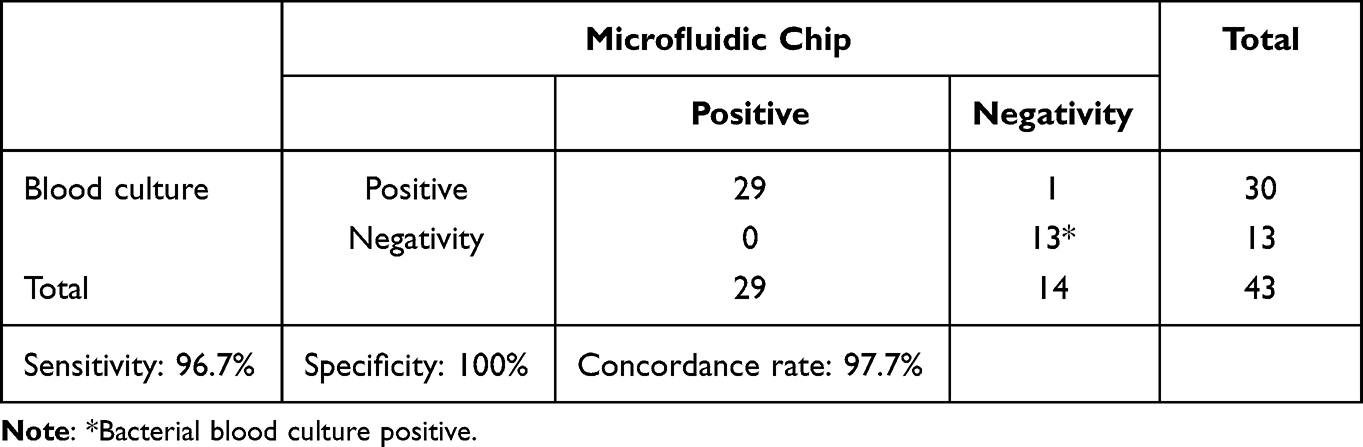 |
Table 2 Statistics of Test Results of 43 Clinical Samples |
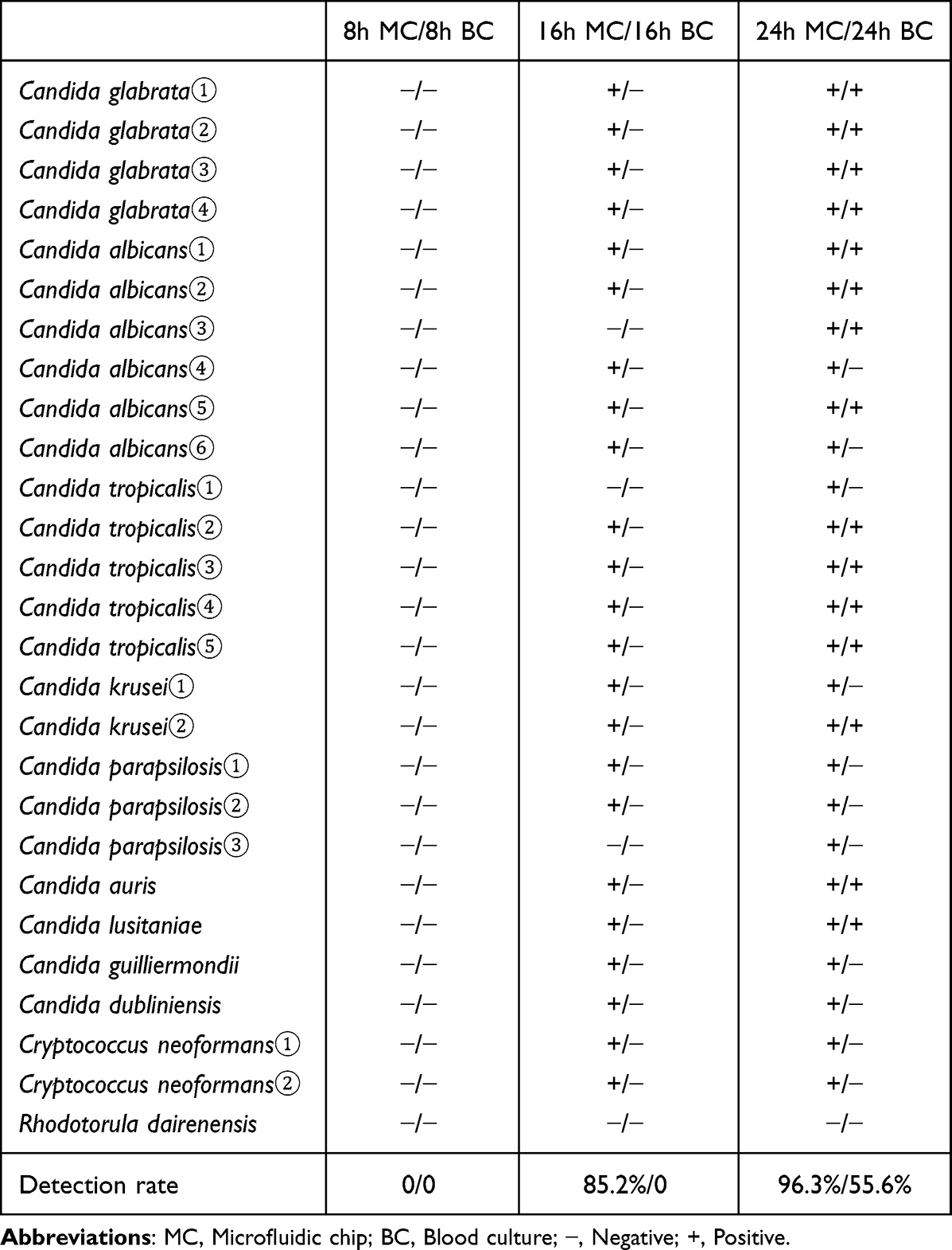 |
Table 3 Detection of 27 Yeasts at Different Culture Time Periods |
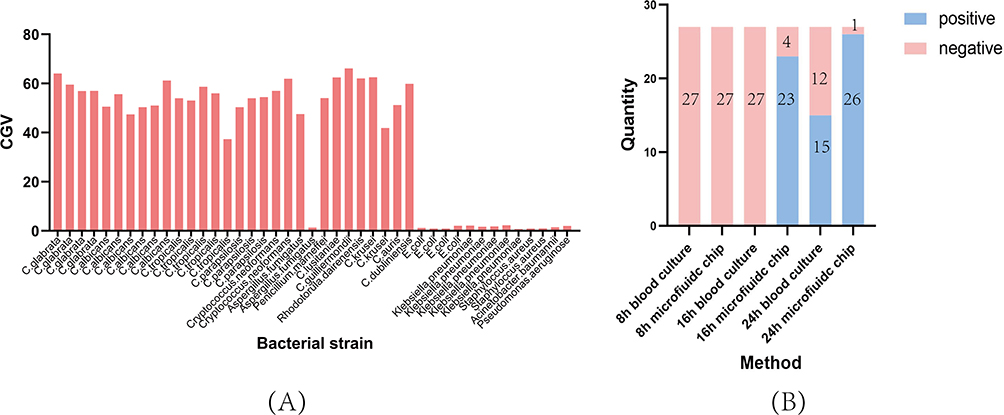 |
Figure 5 (A) Test results of 43 clinical samples, histogram representing the grayscale value of the scan; (B) the number of blood culture positive data and microfluidic chip detected in the blood culture 8h, 16h, and 24h time period. |
Discussion
In recent years, with extensive application of antitumor drugs, immunosuppressants, broad-spectrum antibiotics, the development of organ transplantation and other surgical interventions, and the spread of AIDS, fungal infections are mounting annually.26 According to the statistics of specimens from 2009 to 2014 by China Hospital Invasive Fungi Network (CHIF-NET), more than 40% of fungal infection samples were derived from blood.16 Moreover, statistically, the crude mortality rate of fungi-induced sepsis can reach 40%-70%, among which diagnosis time is one of the highest risk factors for death.27 A timely and accurate etiologic diagnosis is necessary for better instructions on clinical guidance and antifungal drug administration. The golden standard for diagnosis of bloodstream infection still relies on traditional culture. However, the slow growth of fungi prolongs the time required for diagnosis. The data showed that the average time of positive results of fungal blood culture was 48.9 hours.9 Although the use of MALDI-TOF MS has shortened the detection time to some extent, its disadvantage is that it still takes 24–48h to grow a single colony on the solid medium after positive blood culture.28
We designed PCR-reverse dot blot hybridization integrated with microfluidic chip technology to detect 13 types of pathogenic fungi simultaneously. The platform only takes 3–4 hours to detect, much faster than the traditional culture of 24–48 hours. Samples culture only require simple centrifugation before loading to the platform after blood. The process is fully automated. Corresponding operators do not need to perform special culture procedures, saving labor costs. In addition, the combination of microfluidic and DNA microarray technology reduces reagent usage with a low cost of about 10 dollars, significantly relieving patients’ economic burden. The platform incorporates traditional laboratory molecular diagnosis technologies into one chip, including nucleic acid extraction, amplification, reverse dot blot hybridization, and enzyme-linked immunoassays. The functional association among functional areas is realized through valve control, thereby reducing the possibility of pollution due to separate operations. The chip was applied to detect 43 clinical samples, suggesting good performance, wherein the sensitivity was 96.7%, the specificity was 100%, and the concordance rate was 97.7%. Furthermore, we also examined the products of blood culture after different durations. The detection rate at 24h was 96.3%, much higher than the positive rate of 55.6% by blood culture. Notably, the detection rates of Candida albicans, Candida glabrata, Candida tropicalis, Candida parapsilosis, and Candida krusei reached 100% (Table 3), indicating that this detection platform bears excellent potential for swift clinical diagnosis at 24 h of blood culture. The 16h blood culture detection rate was 85.2%, providing certain diagnostic values for critically ill patients.
Importantly, the microfluidic chip contains Cryptococcus neoformans, Candida auris, Aspergillus fumigatus, and Candida albicans which were listed as the most critical group in the list of fungal pathogens issued by the World Health Organization. And Candida auris is is an emerging multidrug-resistant fungal pathogen that has been reported to cause high mortality and nosocomial outbreaks in hospital settings.29 More than 60% of patients infected with Candida auris develop bloodstream infections, with a mortality rate of up to 60%.30 Early and rapid diagnosis of Candida auris not only initiates the right antifungal regimen, but also effectively prevents the further spread of this multidrug-resistant bacteria in hospitals in health care facilities. Besides, the platform based on PCR-reverse dot blot hybridization and microfluidic chip technologies can detect various pathogens causing major public health problems, such as pathogens causing respiratory tract infections, diarrhea pathogens, HPV typing, etc.
Undeniably, This experiment has some limitations. First, more accurate clinical detection data were unavailable due to the small number of clinical samples. Second, the villiform growth of Aspergillus fumigatus made magnetic beads adhere to villi, diminishing nucleic acid extraction efficiency and may lead to false negatives. Third, it was tricky to directly detect the original sample without proliferation owing to high background DNA content and co-extract interference to the PCR reaction. Still, with the development of nucleic acid extraction technology, we believe this platform will be able to test original samples in the near future.
Conclusion
In conclusion, We established a short time-consuming, high sensitivity, strong specificity, low cost and automated detection platform for the detection of 13 bloodstream infectious fungal pathogens, It has great clinical application prospect.
Ethics Approval and Consent to Participate
This study involved anonymous use of redundant, abandoned patient blood, which is part of the standard treatment agreements with patients in our hospital. This research does not affect patients’ health and privacy. All procedures performed in studies involving human participants were in accordance with the ethical standards of the medical ethics committee of the Fourth Affiliated Hospital of Anhui Medical University (reference number: LISC20210802) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by 2020 Anhui Provincial University Cooperative Research and Public Health Collaborative Innovation Project of Anhui Provincial Department of Education (Grant No. GXXT-2020-016), 2021 Anhui Provincial Health and Health Commission Key Scientific Research Project (Grant No. AHWJ2021a011), 2021 Anhui Provincial Medical and Health Key Specialty Construction Project (Approval number: serial number 95), 2021 Anhui Provincial Key Project of Natural Science Research in Colleges and Universities (Approval number: KJ2021ZD0032).
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Carroll KC, Reid JL, Thornberg A, et al. Clinical Performance of the Novel GenMark Dx ePlex Blood Culture ID Gram-Positive Panel. J Clin Microbiol. 2020;58(4). doi:10.1128/JCM.01730-19
2. Guinea J. Global trends in the distribution of Candida species causing candidemia. Clin Microbiol Infect. 2014;20(Suppl 6):5–10. doi:10.1111/1469-0691.12539
3. Arias S, Denis O, Montesinos I, Cherifi S, Miendje Deyi VY, Zech F. Epidemiology and mortality of candidemia both related and unrelated to the central venous catheter: a retrospective cohort study. Eur j Clin Microbiol Infect Dis. 2017;36(3):501–507. doi:10.1007/s10096-016-2825-3
4. Ferrer R, Martin-Loeches I, Phillips G, et al. Empiric antibiotic treatment reduces mortality in severe sepsis and septic shock from the first hour: results from a guideline-based performance improvement program. Crit Care Med. 2014;42(8):1749–1755. doi:10.1097/CCM.0000000000000330
5. Suleyman G, Alangaden GJ. Nosocomial Fungal Infections: epidemiology, Infection Control, and Prevention. Infect Dis Clin North Am. 2021;35(4):1027–1053. doi:10.1016/j.idc.2021.08.002
6. Jamiu AT, Albertyn J, Sebolai OM, Pohl CH. Update on Candida krusei, a potential multidrug-resistant pathogen. Med Mycol. 2021;59(1):14–30. doi:10.1093/mmy/myaa031
7. Rhodes J, Fisher MC. Global epidemiology of emerging Candida auris. Curr Opin Microbiol. 2019;52:84–89. doi:10.1016/j.mib.2019.05.008
8. Sinha M, Jupe J, Mack H, Coleman TP, Lawrence SM, Fraley SI. Emerging Technologies for Molecular Diagnosis of Sepsis. Clin Microbiol Rev. 2018;31(2). doi:10.1128/CMR.00089-17
9. Ransom EM, Alipour Z, Wallace MA, Burnham CA. Evaluation of Optimal Blood Culture Incubation Time To Maximize Clinically Relevant Results from a Contemporary Blood Culture Instrument and Media System. J Clin Microbiol. 2021;59(3). doi:10.1128/JCM.02459-20
10. Riedel S, Carroll KC. Early Identification and Treatment of Pathogens in Sepsis: molecular Diagnostics and Antibiotic Choice. Clin Chest Med. 2016;37(2):191–207. doi:10.1016/j.ccm.2016.01.018
11. Lee N, Kym D. Clinical Usefulness of Serum (1,3)-β-D-glucan to predict invasive candidiasis in patients with severe burn trauma. J Microbiol Immunol Infection. 2022;55(1):138–146. doi:10.1016/j.jmii.2021.02.004
12. Opota O, Jaton K, Greub G. Microbial diagnosis of bloodstream infection: towards molecular diagnosis directly from blood. Clin Microbiol Infect. 2015;21(4):323–331. doi:10.1016/j.cmi.2015.02.005
13. Dark P, Blackwood B, Gates S, et al. Accuracy of LightCycler(®) SeptiFast for the detection and identification of pathogens in the blood of patients with suspected sepsis: a systematic review and meta-analysis. Intensive Care Med. 2015;41(1):21–33. doi:10.1007/s00134-014-3553-8
14. Pancholi P, Carroll KC, Buchan BW, et al. Multicenter Evaluation of the Accelerate PhenoTest BC Kit for Rapid Identification and Phenotypic Antimicrobial Susceptibility Testing Using Morphokinetic Cellular Analysis. J Clin Microbiol. 2018;56(4). doi:10.1128/JCM.01329-17
15. Abdelhamed AM, Zhang SX, Watkins T, et al. Multicenter evaluation of Candida QuickFISH BC for identification of Candida species directly from blood culture bottles. J Clin Microbiol. 2015;53(5):1672–1676. doi:10.1128/JCM.00549-15
16. Xiao M, Sun ZY, Kang M, et al. Five-Year National Surveillance of Invasive Candidiasis: species Distribution and Azole Susceptibility from the China Hospital Invasive Fungal Surveillance Net (CHIF-NET) Study. J Clin Microbiol. 2018;56(7). doi:10.1128/JCM.00577-18
17. Xiao M, Chen SC, Kong F, et al. Distribution and Antifungal Susceptibility of Candida Species Causing Candidemia in China: an Update From the CHIF-NET Study. J Infect Dis. 2020;221(Suppl 2):S139–s47. doi:10.1093/infdis/jiz573
18. Fisher MC, Denning DW. The WHO fungal priority pathogens list as a game-changer. Nat Rev Microbiol. 2023;21(4):211–212. doi:10.1038/s41579-023-00861-x
19. Zhu H, Fohlerová Z, Pekárek J, Basova E, Neužil P. Recent advances in lab-on-A-chip technologies for viral diagnosis. Biosens Bioelectron. 2020;153:112041. doi:10.1016/j.bios.2020.112041
20. Pandey CM, Augustine S, Kumar S, et al. Microfluidics Based Point-of-Care Diagnostics. Biotechnol J. 2018;13(1):1700047. doi:10.1002/biot.201700047
21. Sackmann EK, Fulton AL, Beebe DJ. The present and future role of microfluidics in biomedical research. Nature. 2014;507(7491):181–189. doi:10.1038/nature13118
22. Zeng X, Kong F, Halliday C, et al. Reverse line blot hybridization assay for identification of medically important fungi from culture and clinical specimens. J Clin Microbiol. 2007;45(9):2872–2880. doi:10.1128/JCM.00687-07
23. Wang R, Wu J, He X, Zhou P, Shen Z. A sample-in-answer-out microfluidic system for the molecular diagnostics of 24 HPV genotypes using palm-sized cartridge. Micromachines. 2021;12(3):67.
24. Zhang SX, Carroll KC, Lewis S, et al. Multicenter Evaluation of a PCR-Based Digital Microfluidics and Electrochemical Detection System for the Rapid Identification of 15 Fungal Pathogens Directly from Positive Blood Cultures. J Clin Microbiol. 2020;58(5). doi:10.1128/JCM.02096-19
25. Tang H, Li R, Xu H, et al. Direct-on-Target Microdroplet Growth Assay for Detection of Bacterial Resistance in Positive Blood Cultures. Infect Drug Resist. 2021;14:4611–4617. doi:10.2147/IDR.S336987
26. Loh JT, Lam KP. Fungal infections: immune defense, immunotherapies and vaccines. Adv Drug Deliv Rev. 2023;196:114775. doi:10.1016/j.addr.2023.114775
27. Pappas PG, Lionakis MS, Arendrup MC, Ostrosky-Zeichner L, Kullberg BJ. Invasive candidiasis. Nat Rev Dis Primers. 2018;4:18026. doi:10.1038/nrdp.2018.26
28. Tsuchida S, Umemura H, Nakayama T. Current Status of Matrix-Assisted Laser Desorption/Ionization-Time-of-Flight Mass Spectrometry (MALDI-TOF MS) in Clinical Diagnostic Microbiology. Molecules. 2020;25(20):4775. doi:10.3390/molecules25204775
29. Meis JF, Chowdhary A. Candida auris: a global fungal public health threat. Lancet Infect Dis. 2018;18(12):1298–1299. doi:10.1016/S1473-3099(18)30609-1
30. Park JY, Bradley N, Brooks S, Burney S, Wassner C. Management of Patients with Candida auris Fungemia at Community Hospital, Brooklyn, New York, USA, 2016-2018(1). Emerg Infect Dis. 2019;25(3):601–602. doi:10.3201/eid2503.180927
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.