Back to Journals » Infection and Drug Resistance » Volume 19
A Novel Model for Predicting Post-Craniotomy Meningitis Using Early Postoperative Risk Stratification: A Multi-Center Retrospective Study
Authors Zhao J, Chen X, Wu L, Li C, Zhao W, Shi G
Received 3 May 2026
Accepted for publication 15 June 2026
Published 20 June 2026 Volume 2026:19 381721
DOI https://doi.org/10.2147/IDR.S381721
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Jingwei Zhao,1 Xiyu Chen,1 Lei Wu,1 Chenglong Li,2 Weiping Zhao,3 Guangzhi Shi1
1Department of Critical Care, Beijing Tiantan Hospital of Capital Medical University, Beijing, 100070, People’s Republic of China; 2Department of Neurosurgery, Shanxi Provincial People’s Hospital, Taiyuan, Shanxi, 030012, People’s Republic of China; 3Department of Neurosurgery, Inner Mongolia Peoples’ Hospital, Hohhot, Inner Mongolia, 010017, People’s Republic of China
Correspondence: Guangzhi Shi, Department of Critical Care, Beijing Tiantan Hospital of Capital Medical University, Beijing, 100070, People’s Republic of China, Email [email protected]
Purpose: Early prediction of post-craniotomy meningitis (PCM) is critical for optimizing prognosis. Given the limitations of existing prediction tools, this study sought to develop and externally validate a novel model for early postoperative risk stratification and prediction of PCM.
Patients and Methods: Data were retrospectively collected from three Chinese hospitals. Least absolute shrinkage and selection operator (LASSO) and backward stepwise logistic regression were utilized to select independent predictors for nomogram construction. Nomogram performance was further evaluated by areas under the receiver operating characteristic curves (AUC) (discrimination), calibration plots (calibration) and decision curve analysis (clinical applicability). Meanwhile, pairwise comparisons of AUCs were performed to compare predictive performance between the model and the individual independent predictors. Additionally, a practical probability threshold of 30% was proposed based on the decision curve analysis to evaluate the model’s performance in terms of sensitivity and specificity.
Results: According to their admitted hospitals, 694 patients were allocated to the training cohort, and 309 comprised the external validation cohort. Within the training cohort, postoperative CSF leak, intraoperative/postoperative ventricular drain placement, and trans-sinusal surgery were identified as independent predictors (all P< 0.001). Then, a new nomogram was built based on these predictors and demonstrated good discrimination in both the training (AUC=0.890, 95% CI 0.864– 0.912) and external validation (AUC=0.824, 95% CI 0.777– 0.865) cohorts, alongside satisfactory calibration and clinical utility. Further pairwise comparisons confirmed the nomogram’s superiority over each single predictor across both cohorts (all P< 0.001). Furthermore, applying a practical decision threshold of 30% yielded well-balanced early-warning performance for the model, with sensitivities > 0.70 and specificities > 0.90 in both groups.
Conclusion: Our novel model exhibited favorable performance and clinical applicability, and was found to outperform the individual predictors. Accordingly, this newly built model seems a practical warning tool, though better-designed studies are needed for its further refinement.
Keywords: craniotomy, meningitis, independent predictor, predictive modeling, external validation, pairwise comparison
Introduction
Post-craniotomy meningitis (PCM) is known to be a major infectious complication after neurosurgery, with high rates of mortality and disability.1–3 Inspiringly, there is growing evidence that the disastrous outcomes of this severe infection can be potentially improved through timely diagnosis and treatment.4–6 Accordingly, early postoperative risk stratification of PCM appears crucial, as it may facilitate earlier case identification and initiation of infection control measures.
In previous studies, numerous predictors of PCM, such as postoperative cerebrospinal fluid (CSF) leakage, external lumbar or ventricular drainage, surgical duration, surgery through a sinus, diabetes mellitus, perioperative steroid use, etc., have been intensively investigated.7–13 However, to date, the predictive modeling of PCM remains little explored. Even among the very few prediction models reported in the literature, neither were further validated using an external cohort.14,15 Thus, it is necessary to continue the development of new stratification and forecasting models for PCM, particularly those with external validation.
Over recent years, the nomogram, a visual modeling tool capable of integrating diverse variables, has been increasingly utilized in clinical research settings. So far, this modeling tool has shown good performance for predicting the occurrence, progression and prognosis of various diseases,16–19 including certain neurosurgical central nervous system (CNS) infections. For example, the nomogram has been reported to be predictive of mortality in patients infected with post-neurosurgical meningitis and the development of external ventricular or lumbar drainage-related meningitis (though no external verification was performed for the corresponding models either).20–22
In light of the above, we designed this retrospective multi-institution investigation and employed a nomogram-based approach to establish a novel model for predicting PCM through early postoperative risk stratification. Moreover, considering the main limitation of the existing studies, our newly developed model was evaluated on an independent external dataset curated in the present multicenter study.
Material and Methods
Study Design and Population
This is a multicenter, retrospective cohort study conducted at three medical institutions (one university-affiliated and two public hospitals) in China. We retrospectively reviewed patients who underwent scheduled or emergency craniotomy consecutively at the university-affiliated hospital (Beijing Tiantan Hospital affiliated to Capital Medical University) between October 2021 and March 2022. We also screened a consecutive series of cases receiving craniotomy from August 2022 to January 2023 at the two other public hospitals (Inner Mongolia Peoples’ Hospital and Shanxi Provincial People’s Hospital).
Patients were excluded from the study if they were under 18 years old. Those who died within the first 48 hours following craniotomy and had no clear diagnostic clues to PCM during this period were excluded as well. This exclusion criterion was set to avoid a possible underestimation of the occurrence of PCM in our study, given that this infectious complication typically presents 3 to 7 days postoperatively.23,24 In addition, patients with suspected or confirmed CNS infections (eg, bacterial meningitis or ventriculitis, fungal meningitis or meningoencephalitis, viral encephalitis or meningitis, intracranial or spinal abscess, etc) prior to the craniotomy were excluded. Lastly, we also eliminated patients lacking sufficient data to determine the study outcome (ie, the diagnosis of PCM based on the criteria published by the Centers for Disease Control and Prevention/National Healthcare Safety Network [CDC/NHSN] in 2008;25 for the specific contents of the criteria, see the section “Study Outcome” below), as well as those with incomplete medical records for any of the key variables included in our final analysis (see the “Data Collection” section for details).
After the above exclusion, the remaining patients were included in the final analysis. The enrolled patients were then divided into training and external validation cohorts according to the hospitals where they were admitted. That is, those treated at the university-affiliated hospital (Beijing Tiantan Hospital of Capital Medical University) were categorized as the training cohort, while the others who were hospitalized at the two public hospitals (Shanxi Provincial People’s Hospital and Inner Mongolia Peoples’ Hospital) comprised the external validation cohort.
Data Collection
To ensure stringent data quality control and cross-center consistency, a standardized and unified paper-based case report form was designed in advance and utilized across all three participating institutions. Prior to data extraction, all data collectors (LW, CL, and WZ) underwent standardized training to align and unify their understanding of variable definitions and the study outcome (see the following two paragraphs). After the initiation of data collection, data for analysis were manually extracted by a single dedicated investigator at each center through reviewing the medical charts of the patients enrolled, and subsequently recorded into the standardized case report forms. Following the completion of data entry, the principal investigator of this study (GS) comprehensively cross-checked and verified all the extracted data across all three centers based on the submitted case report forms to ensure absolute accuracy and consistency.
Taking into account that the present study aimed to develop a model for early postoperative risk stratification of PCM (as stated above in the “Introduction” section), our focus was mainly on data recorded during the perioperative period (defined in this article as the time window from 24 hours before to 48 hours after craniotomy), such as whether the patients used perioperative prophylactic antibiotics or steroid therapy, whether they were operated via a trans-sinusal approach, whether they were implanted with foreign bodies (eg, vascular clips, dural substitutes, etc) or intracranial pressure (ICP) monitoring devices during surgery, and whether they had lumbar or ventricular drain placed intraoperatively or postoperatively. Moreover, we documented whether those patients underwent emergency re-do craniotomy through the same surgical incision within the first postoperative 48 hours, and if they received invasive ventilation in the same time frame. Apart from these, other perioperative variables including surgical type (emergent or elective), operative duration, volume of intraoperative bleeding, surgical wound class (clean, clean‐contaminated, or dirty)8,26 and the occurrence of postoperative CSF leakage, were gathered as well. Additionally, information regarding demographics (age, gender), chronic comorbidities (diabetes mellitus [DM], hypertension, cardiovascular disease [CVD], chronic renal failure [CRF], chronic obstructive pulmonary disease [COPD] and malignancies), smoking status (current, former, or never smokers) and alcohol consumption (non-, light, moderate, or heavy drinkers) was also extracted from those patients’ medical charts.
Study Outcome
The final outcome of this study was the development of PCM as defined by the 2008 CDC/NHSN criteria.26 Details of the criteria were as follows: 1) pathogens cultured from CSF; 2) at least one of the following signs or symptoms with no other recognized cause: fever (>38°C), headache, stiff neck, meningeal signs, cranial nerve signs, or irritability, and at least one of the following: a) increased white blood cells, elevated protein level, and/or decreased glucose level in CSF, b) pathogens seen on gram stain of CSF, c) pathogens cultured from blood, d) positive antigen test of CSF, blood, or urine, e) diagnostic single antibody titer (Immunoglobulin M) or 4-fold increase in paired sera (Immunoglobulin G) for pathogen. PCM diagnosis required the presence of either criteria 1) or 2), or both, and the diagnosis was also determined by reviewing the medical records. Each record was thoroughly and comprehensively examined until patient discharge or hospital death to ascertain whether or not PCM had occurred during hospitalization. In addition, if a foreign body was implanted at the craniotomy, then the time period of the record review was extended to 1 year postoperatively. It must be mentioned that, generally, patients who have undergone craniotomy at our participating centers will return to their original hospitals for follow-up visits every three to six months for at least 1 year after surgery. Thus, complete medical records over the first year following the craniotomy were available for our study participants. Also, for patients diagnosed with PCM, the time from surgery to infection onset was calculated (in days).
Statistical Analyses
All statistical analyses in our study were performed with R software (version 3.6.3; R Foundation for Statistical Computing), and each statistical test was two-sided. Categorical data were expressed as numbers and percentages (%). Continuous variables were presented as mean ± standard deviation (SD) or median with interquartile range (IQR) based on the normality of the data distribution. The normality of distribution was assessed by Shapiro–Wilk test. Differences in variables between the training and external validation cohorts were compared using independent sample t test, Chi-square test, and Mann–Whitney U-test, as appropriate, and a P value<0.05 was considered statistically significant. In the training cohort, potential predictive factors for PCM were screened out via least absolute shrinkage and selection operator (LASSO) regression, and the factors selected in LASSO regression were further incorporated into a multivariate logistic regression model using backwards stepwise selection to identify the independent predictors of PCM. The results of the multivariate logistic regression analysis were reported as odds ratios (OR) plus 95% confident intervals (CI) with the P values, and the variables with P < 0.05 were taken as independent predictors. Subsequently, those independent predictors identified in the logistic regression analysis were integrated to build a nomogram model. Then, the graphic model was subject to both internal and external validations using the training and external validation cohorts, respectively. Validation of the model (either internal or external) included evaluations of discrimination, calibration and clinical applicability. The model’s discrimination abilities were reflected by the area under the receiver operating characteristic curves (AUC) with their corresponding 95% CIs, while its calibration and clinical applicability were estimated via the calibration plots and decision curve analysis (DCA), respectively. Besides, a pairwise comparison between the nomogram model and each of the independent predictors was done separately for the training and external validation cohorts. The comparison results were also displayed as the AUCs along with the associated 95% CIs, and the pairwise differences between those AUCs were further calculated together with their according 95% CIs as well as the respective standard errors (SE) and P values (statistical significance set at P<0.05 as well). Furthermore, to assess model capabilities in real-world clinical decision-making scenarios, a practical probability threshold of 30% was proposed based on the DCA, and its corresponding sensitivity and specificity, along with their respective 95% CI as well, were calculated for both cohorts to determine its actual risk-stratification ability and predictive performance. This 30% threshold was specifically chosen considering the high severity of PCM and the critical clinical need for its early identification, where even a moderate pre-test probability justifies aggressive early surveillance and timely clinical intervention.21
Results
General Characteristics and Study Outcome
In total, 2109 consecutive patients from the 3 participating hospitals who had undergone craniotomy during the respective study period (ie, October 2021 to March 2022, or August 2022 to January 2023) were retrospectively screened for potential eligibility Of these, 328 cases were aged under 18 years and 167 cases died within 48 hours postoperatively without any documented clinical or laboratory signs suggestive of PCM; all of them were therefore first eliminated. Then, among the remaining 1614 patients, 611 were further excluded, including 19 who lacked information on PCM diagnosis, 438 with incomplete data for the other key study variables, and 54 with suspected or proven CNS infections prior to craniotomy. Eventually, 1003 subjects were retained for the final analyses. These 1003 individuals were subsequently divided into the training (n=694) and external validation (n=309) cohorts according to the hospital where the craniotomy was performed (Training: the university-affiliated hospital; External Validation: the two public hospitals). The detailed flow of the patients’ enrolment and allocation was summarized in Figure 1.
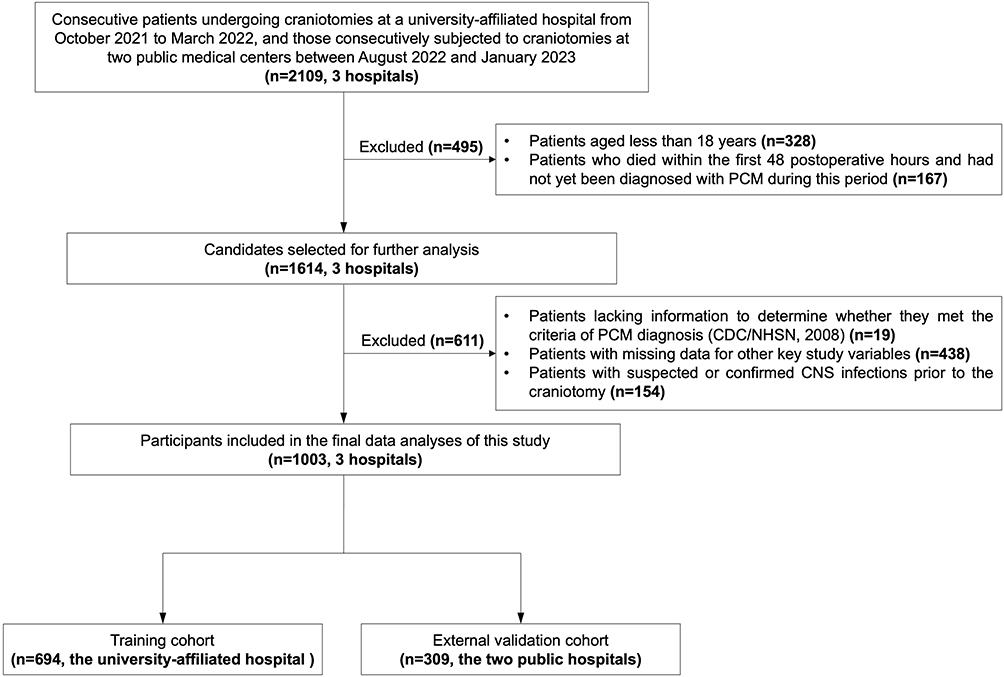 |
Figure 1 Flowchart of patient enrollment and grouping. Bold text highlights the specific patient sample sizes (n) and the corresponding number of participating medical centers at key screening milestones and exclusion nodes. Here, “the university-affiliated hospital” represents Beijing Tiantan Hospital of Capital Medical University; “the two public hospitals” represent Shanxi Provincial People’s Hospital and Inner Mongolia Peoples’ Hospital, respectively. Abbreviations: PCM, post-craniotomy meningitis; CDC, the Centers for Disease Control and Prevention; NHSN, National Healthcare Safety Network; CNS, central nervous system. |
Table 1 presents the comparison of general characteristics and the study outcome for the training and external validation cohorts. In the training cohort, the mean age was 49.9±14.8 years, 38.2% (265/694) were female and 14.4% (100/694) eventually developed PCM. Among this cohort, 236 patients (34.0%) reported a history of hypertension, 76 (11.0%) had a history of diabetes mellitus (DM), 160 (23.1%) had a history of cardiovascular diseases (CVD), 13 (1.9%) had chronic renal failure, 21 (3.0%) had chronic obstructive pulmonary disease and 114 (16.4%) were complicated with malignancies. Besides, 80.1% of the cohort (556/694) were former or current smokers, and 5.8% (40/694) were moderate or heavy drinkers. During the perioperative period (from 24 hours before to 48 hours after craniotomy), 340 patients (49.0%) from this training group were managed with steroids, whereas prophylactic antibiotics were given to the whole group of subjects (694/694, 100%). Intraoperatively, 616 patients (88.8%) out of this group were implanted with foreign bodies and 164 (23.6%) had ICP monitors placed. Within the first 48 hours after craniotomy, there were 61 patients (8.8%) in the group receiving ventricular drain placement, 39 patients (5.6%) undergoing lumbar drainage, 471 patients (67.0%) experiencing invasive ventilation, 29 (4.1%) having an emergency re-do craniotomy and 20 (2.9%) developing postoperative CSF leakage. As for the other perioperative characteristics of this study cohort, the distribution of surgical wound classification was clean 88.6% (615 cases), clean-contaminated 9.1% (63 cases), and dirty 2.3% (16 cases), while the number of patients operated upon through a trans-sinusal approach was 63 (9.1%). In addition, the median surgical duration for this cohort was 5.0 (IQR 4.0–6.0) hours, the median volume of intraoperative blood loss was 400 (IQR 300–600) mL, and 41.6% of these cases (289/694) were subjected to emergency surgery with the others undergoing elective surgery (58.4% [405/694]). Compared to the training cohort, the external validation cohort showed no significant differences in most of the general characteristics, except for the duration of surgery (5.0 [IQR 4.0–6.0] hours vs. 4.5 [IQR 3.3–6.0] hours; P<0.001) and the volume of intraoperative bleeding (400 [IQR 300–600] mL vs. 300 [IQR 150–500] mL; P<0.001). In terms of the study outcome, on the other hand, the proportion of patients suffering from PCM was substantially higher in the external validation group (21.4% [66/309] vs. 14.4% [100/694]; P=0.006). Additionally, among those who developed PCM, the median time from surgery to infection onset was comparable between the two cohorts, with 5 (IQR 3–7) days in the training cohort and 5 (IQR 3–8) days in the validation cohort (P=0.612). For more details on the characteristics and study outcome of these 2 cohorts, please refer to Table 1.
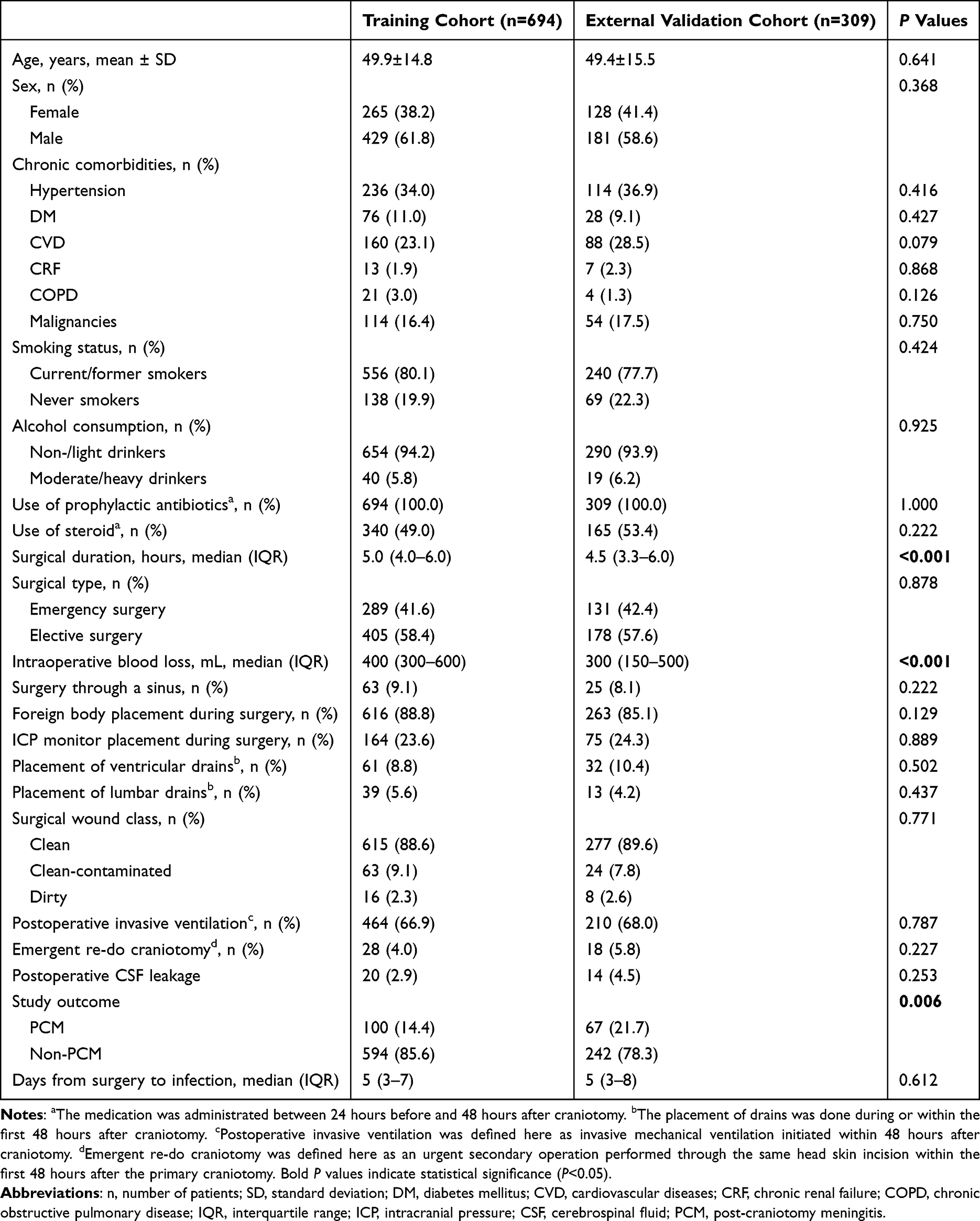 |
Table 1 General Characteristics and Outcome of the Study Population |
Selection of Independent Predictors for PCM
To seek out potential predictors for PCM, all of the variables mentioned in the above paragraph (see also Table 1), except for the study outcome as well as the timing of infection onset, were taken into consideration. Hence, a total of 24 candidate variables from the training cohort were involved in the LASSO regression. The results of this regression analysis are displayed in Figure 2. Specifically, the binomial deviance curve for penalty parameter selection is summarized in Figure 2A, and the coefficient trajectories of candidate variables are presented in Figure 2B. Through the LASSO method, 8 potential predictors with nonzero coefficients, including use of perioperative steroids, surgical duration, surgical type, intraoperative or postoperative placement of ventricular and lumbar drains, surgical wound class, postoperative CSF leak, and surgery through a sinus, were screened out (Figure 2B).
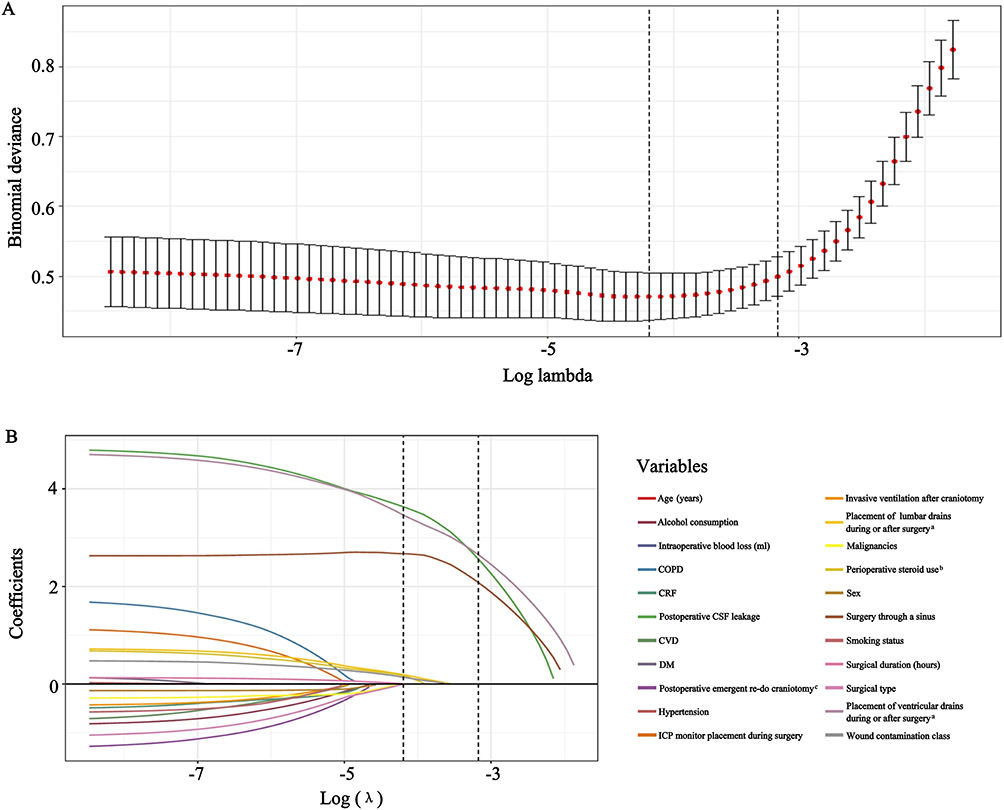 |
Figure 2 LASSO regression analysis to select the potential predictors of PCM. (A) Binomial deviance profiles for candidate variables. (B) LASSO coefficient profiles of candidate variables. “a”: The placement of drains was done during or within the first 48 hours after craniotomy; “b”: The medication was administrated between 24 hours before and 48 hours after craniotomy; “c”: Postoperative emergent re-do craniotomy was defined here as an emergent operation performed through the same incision within the first 48 hours after the initial craniotomy. Abbreviations: LASSO, least absolute shrinkage and selection operator; PCM, post-craniotomy meningitis; COPD, chronic obstructive pulmonary disease; CRF, chronic renal failure; CSF, cerebrospinal fluid; CVD, cardiovascular diseases; DM, diabetes mellitus; ICP, intracranial pressure. |
The 8 potential predictors were then entered into a multivariate backward stepwise logistic regression analysis to identify independent predictors for PCM. Results from the logistic regression revealed that postoperative CSF leak (OR 78.08, 95% CI 17.04–357.81; P<0.001), intraoperative or postoperative placement of ventricular drains (OR 104.21, 95% CI 38.79–279.96; P<0.001), and surgery through a sinus (OR 14.75, 95% CI 4.56–47.74; P<0.001) were the factors independently predictive of PCM (Figure 3), whereas the other five were not (all P values>0.05, Figure 3).
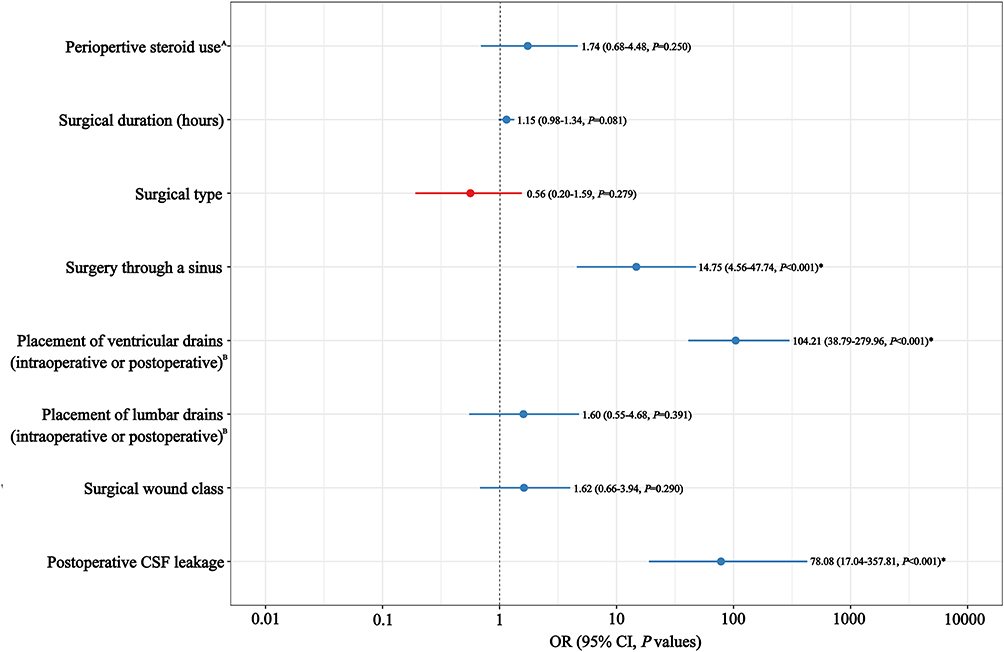 |
Figure 3 Forest plot showing the results of multivariate logistic regression analysis for PCM prediction. “A”: The medication was administrated between 24 hours before and 48 hours after craniotomy; “B”: The placement of drains was done during or within the first 48 hours after craniotomy; “*”: The independent predictors identified for PCM (all P values<0.01). Abbreviations: PCM, post-craniotomy meningitis; CSF, cerebrospinal fluid; OR, odds ratio; CI, confidence interval. |
Construction of the Nomogram
The identified independent predictors (as described above) were integrated to establish a novel nomogram for early postoperative risk stratification and prediction of PCM (abbreviated as “Nomo-PCM”, Figure 4). To interpret the “Nomo-PCM”, a procedure could be carried out as follows: first, a variable was located; second, a vertical line was drawn towards the “Points” axis (top axis) to determine the points of the variable; next, the above 2 steps were repeated for the other variables and the points obtained for each variable were then added up; ultimately, the overall sum of the points from all those variables were located on the “Total points” axis and a line was plotted downward to the “Risk of PCM” axis (bottom axis) to determine the possibility of PCM development.
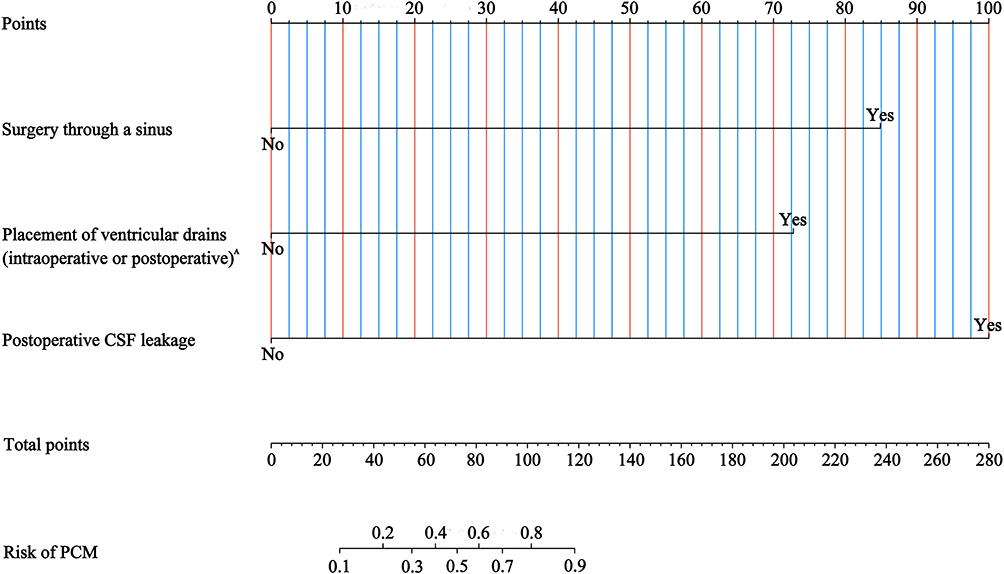 |
Figure 4 Nomogram for early postoperative risk stratification of PCM (Nomo-PCM). “A”: The placement of drains was done during or within the first 48 hours after craniotomy. Abbreviations: PCM, post-craniotomy meningitis; CSF, cerebrospinal fluid. |
To make the “Nomo-PCM” easier to use in clinical practice, we have developed a free dynamic prediction tool: https://bjtth-shigz.shinyapps.io/dynnomapp/. Individual, patient-level predictive analyses using this nomogram can be performed on the above website.
Internal and External Validation of Nomo-PCM
We validated Nomo-PCM internally and externally in the training and the external validation cohorts, respectively, and the newly built model demonstrated satisfactory performance in both cohorts in terms of discrimination, calibration, and clinical utility.
Specifically, Nomo-PCM showed good discrimination in the training group, with an AUC of 0.890 (95% CI 0.864–0.912, Figure 5A). In the external validation cohort, the AUC was 0.824 (95% CI 0.777–0.865, Figure 5B), also revealing a good discrimination. Moreover, we found that the internal calibration curve of the training cohort was highly coincident with the ideal diagonal line (Figure 6A), demonstrating good calibration of the model. Likewise, a good consistency between the predicted results of this model and the observed results was found in the external calibration curve as well (Figure 6B), though the curve of this validation cohort was not as close to the ideal diagonal line as that derived from the training group (Figure 6A vs. B). Furthermore, the DCA curve of the training group revealed that Nomo-PCM had a significant net benefit within the range of threshold probabilities from approximately 20% to 80%, indicating a favorable clinical applicability (Figure 7A). Similarly, the DCA showed that the clinical utility of Nomo-PCM in the external validation group was roughly comparable to that in the training cohort (Figure 7A), despite its slightly smaller net benefit as illustrated in Figure 7B
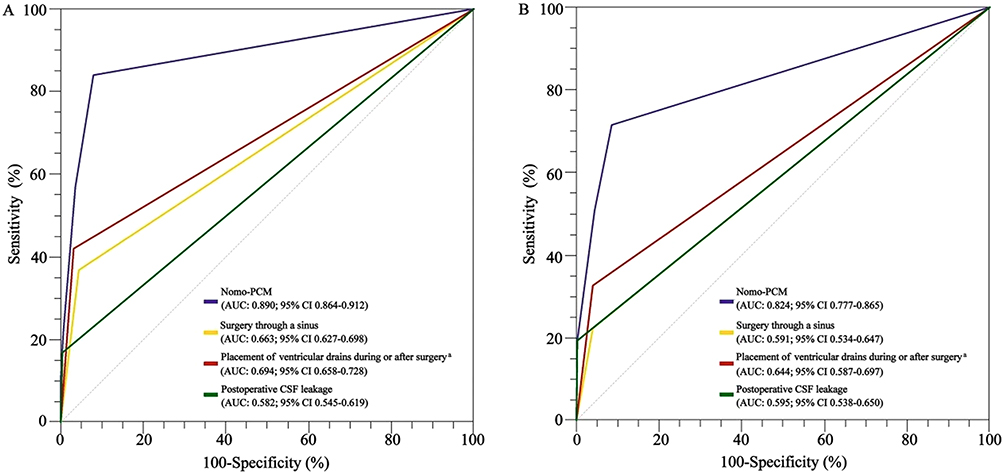 |
Figure 5 ROC curves of Nomo-PCM and the other independent predictors of PCM. (A) Training cohort. (B) External validation cohort. “a”: The placement of drains was done during or within the first 48 hours after craniotomy. Abbreviations: ROC, receiver operating characteristic; Nomo-PCM, nomogram for early postoperative risk of PCM; PCM, post-craniotomy meningitis; AUC, area under ROC curves; CI, confidence interval; CSF, cerebrospinal fluid. |
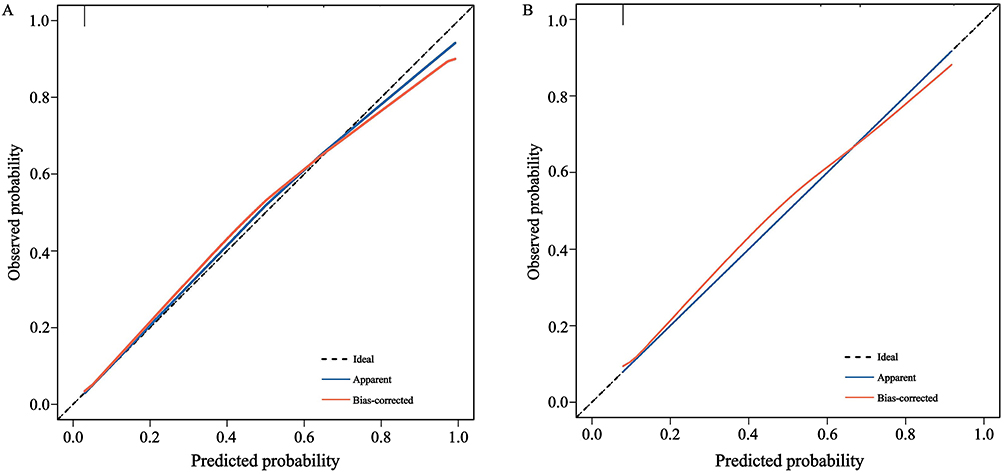 |
Figure 6 Calibration plots of Nomo-PCM for the training cohort (A) and external validation cohort (B). Abbreviations: Nomo-PCM, nomogram for early postoperative risk stratification of PCM; PCM, post-craniotomy meningitis. |
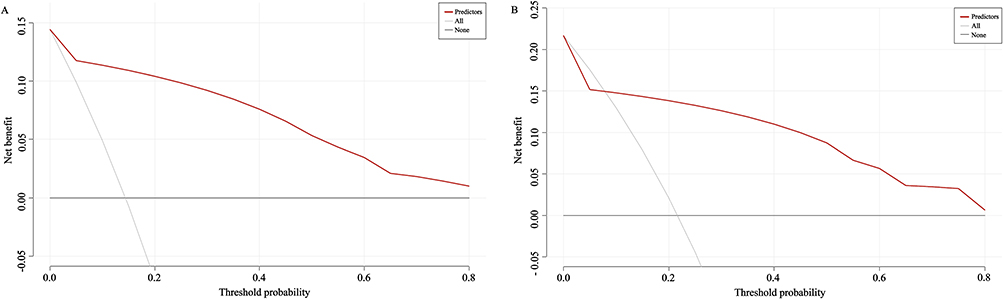 |
Figure 7 Decision curve analysis (DCA) for Nomo-PCM in the training cohort (A) and external validation cohort (B). Abbreviations: Nomo-PCM, nomogram for early postoperative risk stratification of PCM; PCM, post-craniotomy meningitis. |
Additionally, to further verify and highlight the predictive discrimination of Nomo-PCM, its AUCs for predicting PCM were pairwise compared with those of the three independent predictors identified by the logistic regression described above (in both the training and external validation cohorts separately) (see also Figure 5A and B). Findings from these pairwise comparisons confirmed that Nomo-PCM was indeed significantly superior to any of the independent predictors alone in discriminating patients at high risk for PCM (all P values<0.001) (Table 2), regardless of the training (Nomo-PCM vs. Surgery through a sinus: AUC difference=0.277 [95% CI 0.165–0.288], SE=0.031; Nomo-PCM vs. Intraoperative or postoperative placement of ventricular drains: AUC difference=0.196 [95% CI 0.143–0.249], SE=0.027; Nomo-PCM vs. Postoperative CSF leak: AUC difference=0.307 [95% CI 0.247–0.367], SE=0.031) and external validation (Nomo-PCM vs. Surgery through a sinus: AUC difference=0.233 [95% CI 0.151–0.315], SE=0.042; Nomo-PCM vs. Intraoperative or postoperative placement of ventricular drains: AUC difference=0.180 [95% CI 0.109–0.252], SE=0.036; Nomo-PCM vs. Postoperative CSF leak: AUC difference=0.229 [95% CI 0.152–0.306], SE=0.039) groups (Table 2).
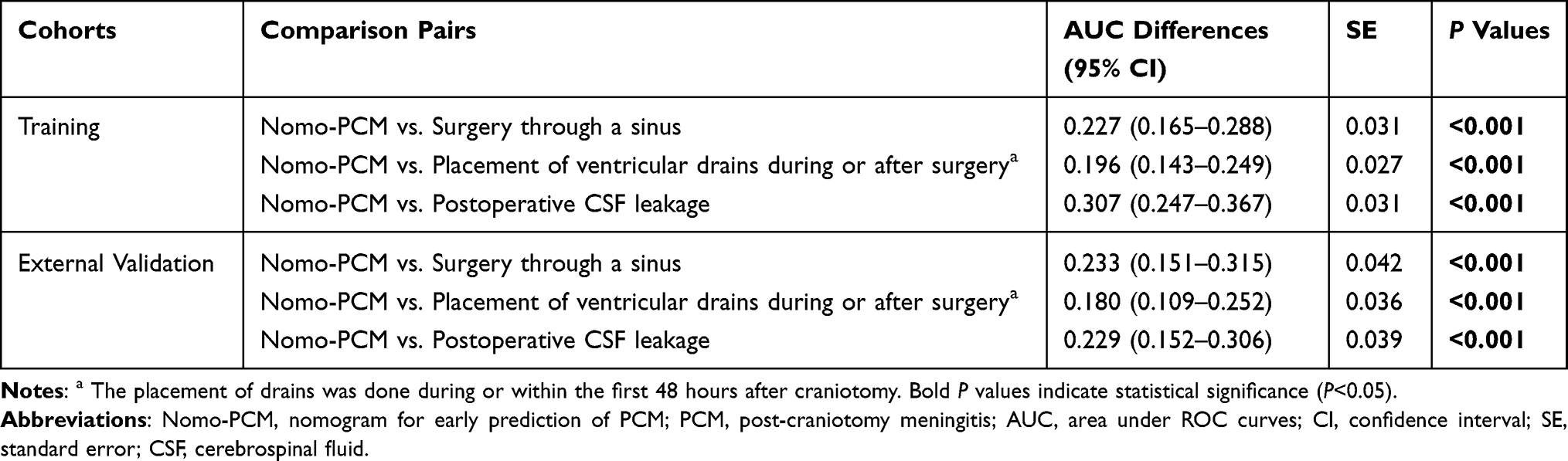 |
Table 2 Pairwise Comparison of Discrimination Performance Between Nomo-PCM and the Other Independent Predictors for PCM |
Lastly, to further facilitate the real-world clinical application of Nomo-PCM, a practical decision threshold of 30% was selected. Its predictive metrics were then calculated across both the training and external validation cohorts. In the training group, the probability threshold of 30% yielded a sensitivity of 0.840 (95% CI 0.782–0.898) and a specificity of 0.921 (95% CI 0.875–0.967). In the external validation cohort, the 30% threshold presented a sensitivity of 0.716 (95% CI 0.634–0.798) and a specificity of 0.913 (95% CI 0.851–0.975).
Discussion
In this study, a novel model for early (within 48 hours postoperatively) risk stratification and prediction of PCM was established by combining three relevant independent predictors, ie, postoperative CSF leak, intraoperative or postoperative placement of ventricular drains, and surgery through a sinus Moreover, this predictive model was validated both in the training (internal validation) and external validation cohorts using ROC curves, calibration plots plus DCA, demonstrating favorable discrimination, calibration, and clinical utility. In addition, we conducted pairwise comparisons between the model and each of the three independent predictors mentioned above, and found that the discriminative performance of our model was significantly superior to that of any single one of those independent predictors in either the training or external validation groups. Furthermore, a pragmatic decision threshold of 30% was proposed based on DCA, yielding a well-balanced clinical early-warning performance of the new model with acceptable sensitivity and specificity across both cohorts.
Our analyses identified postoperative CSF leak as one of the independent predictors for PCM. Likewise, similar findings had also been documented in previous studies, and there have been almost no other conflicting reports about this risk factor to date.8,11–13,15 Such consistent results strongly suggested that the presence of CSF leak after craniotomy was a relatively robust and reliable predictor of PCM. Furthermore, the present research exhibited that the occurrence of postoperative CSF leak was correlated with an over 70-fold increased risk for PCM. This observed risk is much higher than those described in prior literature,8,11–13,15 which means that the presence of postoperative CSF leak is not only a reliable but also a somewhat strong predictor. It is therefore not difficult to understand why this predictor could be successfully used for the construction of our nomogram. In fact, the reason why postoperative CSF leak can become a valid and strong predictor of PCM is evident: CSF leak is a result of dural and arachnoid laceration with fistula formation and this meningeal injury can easily lead to the invasion of pathogenic bacteria.27
Placement of ventricular drain during or after craniotomy is another frequently reported factor that is independently predictive of PCM.7,9–14 This finding is further supported by the results of our study. Moreover, our study revealed that the external ventricular drain placement (intraoperative or postoperative) was a stronger predictor of PCM, with a more than 100 times increased risk. Such an observation can obviously be attributed to the invasive nature of external ventricular drain insertion, which carries a high risk of intracranial contamination, particularly when the procedure is performed postoperatively in non-sterile or non-operating room settings (eg, intensive care units)28,29 In fact, infectious meningitis is highly prevalent not only among patients undergoing craniotomy but also in those managed with external ventricular drainage alone.30,31 It is thus quite understandable why the placement of ventricular drain (intraoperative or postoperative) could also play a key role in our modeling process.
In the present work, we also identified surgery through a sinus as an independent predictor associated with PCM. Compared to the other two predictors discussed above, this one has rarely been investigated in the existing literature. Even so, our study’s results regarding this predictor are quite similar to the findings from the limited extant research,9 indicating the reliability of this surgical approach for predicting PCM, at least to some extent. In addition, our current work demonstrated that surgery through a sinus was also a relatively strong predictor, conferring a nearly 14 times greater risk for developing PCM, although this risk value was somewhat lower than those for the other two independent predictors (ie, postoperative CSF leak and placement of ventricular drains during or after surgery) The underlying mechanism behind the observed association between this surgical approach and the occurrence of PCM might be that trans-sinus surgery would lead to an abnormal intracranial-extracranial communication via the anterior cranial fossa, thereby increasing the possibility of intracranial bacterial contamination.32,33 In view of this mechanism, it is not surprising then that surgery through a sinus was able to be incorporated into the “Nomo-PCM”.
Notably, the exceptionally high ORs for postoperative CSF leak and placement of ventricular drain were accompanied by wide confidence intervals, which reflects a potential sparse data bias or quasi-complete separation in our training cohort. This statistical bias potentially inflates the individual effect sizes of these two variables within our newly developed model. Fortunately, we subsequently performed an external validation on an independent cohort and obtained favorable discriminative ability and relatively stable calibration, thereby partially addressing the generalizability issue of our model to some extent. Still, it must be acknowledged that external validation alone is insufficient to fully guarantee the model’s stability and reproducibility in broader, more diverse populations.
As described above, one significant highlight of this study is that our newly established predictive model was validated using external as well as internal datasets. Prior to this study, however, none of the similar models that have been reported had, to our knowledge, undergone independent external validation. That is to say, our model seems to be more reliable and generalizable compared to the existing ones, suggesting its better potential for clinical use. Another highlight of the present work is the investigation into the discriminative abilities of those independent predictors identified by our analyses, along with further comparisons of these abilities with that of the newly developed model. Also, as far as we are aware, there is currently little to no research available specifically seeking to explore the individual predicting power of those PCM-related predictors, although many risk factors for this infection have been reported in literature.7–15 Our study precisely addressed this knowledge gap and found that none of the single predictors was superior to the “Nomo-PCM” in predicting PCM, which underscores the value of the current modeling analysis. A third strength of this study is that we did not merely present a theoretical model, but further proposed a practical probability threshold of 30% to directly guide real-world application of the model. As this threshold demonstrated satisfactory predictive performance in both cohorts, Nomo-PCM appears to be a potential early warning tool that allows clinicians to confidently risk-stratify PCM patients and initiate timely clinical interventions.21,34
Additionally, in the present study, it is worth noting that the baseline incidence of PCM was significantly higher in the external validation group than in the training cohort (P=0.006). Conversely, the vast majority of clinical characteristics, including chronic comorbidities, surgical wound classification, and the independent predictors (ie, postoperative CSF leakage, ventricular drain placement and surgery through a sinus), etc, showed no statistically significant differences between the two groups. This relative homogeneity largely implies that the overall disease severity and underlying patient risk profiles were comparable across groups and centers. Interestingly, the only significant variances in clinical parameters were that the training cohort had longer surgical durations and greater intraoperative blood loss (both P<0.001), which traditionally correlate with increased infectious risks.12,13,26 Thus, the observed disparity in PCM rates between the two cohorts is more likely reflective of inter-institutional heterogeneity regarding localized infection control, perioperative care, or empirical antibiotic management, etc. Despite this, our model still exhibited consistent discriminative performance across centers (both AUCs>0.8). To a certain extent, such a relatively stable performance further contextualizes and highlights the generalizability and clinical validity of this model when applied to actual, real-world clinical settings.
Still, there are several limitations of note in the present work. The first major limitation is the potential exclusion bias introduced by excluding patients who died without clear diagnostic clues to PCM within 48 hours postoperatively. Although this exclusion criterion was intended to minimize possible confounding from early post-surgical mortality, such a design might have theoretically underestimated the true incidence of PCM and thus affected model performance. To address this concern, a sensitivity analysis was performed in parallel, evaluating the model under two extreme scenarios: either classifying a baseline-proportional subset of the 167 excluded patients as PCM cases or treating them all as non-PCM controls. In both scenarios, the analysis consistently demonstrated that the independent predictors remained robustly significant (P<0.01) with negligible AUC fluctuations (<0.01), suggesting minimal pragmatic impact on model stability.35 Furthermore, it must be acknowledged that a robust comparison of baseline characteristics and disease severity between the included and excluded patients was not performed. Consequently, in addition to the aforementioned exclusion bias, the potential for subtle selection bias cannot be entirely ruled out.35 The second drawback is the retrospective nature of this study, which restricted our analyses only to the information available in the medical records. As a result, several other factors which have been identified in previous literature as important independent predictors of PCM, such as the acute physiology and chronic health evaluation (APACHE) III score and the American Society of Anesthesiologists (ASA) score, etc.,7,9 were unable to be analyzed in this study due to incomplete or missing data, and thus were not incorporated into our nomogram. Another limitation was the lack of inclusion of laboratory variables in our modeling analysis, whereas there have been findings that certain laboratory risk factors (eg, serum C-reactive protein levels, CSF lactate, and CSF neutrophils, etc) are also independently associated with the occurrent of PCM.15 A further notable shortcoming of this retrospective work is the lack of detailed microbiological characterization of the PCM cases, particularly regarding the specific pathogen profiles. Considering the substantial microbiological variations in PCM across regions, this deficiency may theoretically limit the interpretability and broader applicability of our findings.8,12,13 Moreover, within the current retrospective study, advanced strategies for handling missing data, such as multiple imputation, were unable to be implemented due to the present data availability.35,36 As can be seen, the major reason for all the above defects was incomplete medical records due to the retrospective design, which suggests that our current model still has great potential to be further improved in the future by optimizing the study design, as well as by integrating more diverse data. The third drawback of this work lies in the relatively limited representation of our study cohort. In spite of the fact that the study population were drawn from more than one hospital, our current research actually is a small-scale, multicenter study involving only three medical institutions. Moreover, the three institutions were all major tertiary hospitals in their respective regions, which are equipped with the finest available medical resources and thus able to provide the best possible clinical care. As a consequence, it remains uncertain whether our model can be generalized to a larger patient population, especially those in low-resources clinical settings such as secondary care hospitals.
Conclusion
Despite the limitations discussed above, we have successfully developed and provided a novel model for early postoperative risk stratification of PCM (ie, Nomo-PCM) in the present study, and this new predictive model was internally and externally validated with satisfactory discrimination, calibration, and clinical applicability Furthermore, our newly developed model has been demonstrated to outperform the individual independent predictors in its discriminative power. In addition, the established practical decision threshold of 30% further enhances the model’s clinical utility by offering a quantified early-warning benchmark. As such, “Nomo-PCM” appears to be a practical tool for earlier identification of PCM and may potentially assist in more timely management of this infectious complication. Still, future larger-scale, multi-center studies that involve hospitals with more diverse representations and employ more rigorous designs (eg, perspective designs capable of incorporating more comprehensive data) would be needed, to further verify and refine the present model.
Abbreviations
PCM, post-craniotomy meningitis; LASSO, least absolute shrinkage and selection operator; AUC, area under the receiver operating characteristic curves; CSF, cerebrospinal fluid; CI, confidence interval; CNS, central nervous system; CDC, Centers for Disease Control; NHSN, National Healthcare Safety Network; ICP, intracranial pressure; DM, diabetes mellitus; CVD, cardiovascular disease; CRF, chronic renal failure; COPD, chronic obstructive pulmonary disease; SD, standard deviation; IQR, interquartile range; OR, odds ratio; DCA, decision curve analysis; SE, standard error; Nomo-PCM, nomogram for early postoperative risk stratification of PCM; ROC, receiver operating characteristic; APACHE, acute physiology and chronic health evaluation; ASA, American Society of Anesthesiologists.
Data Sharing Statement
The data used in this study are available from the corresponding author (Guangzhi Shi, Email: [email protected]), upon reasonable demand.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki, and approved by the respective ethics committees of all participating centers, ie, Beijing Tiantan Hospital of Capital Medical University (Approval No. KYSQ 2025–377–01), Shanxi Provincial People’s Hospital (Approval No. 2025–309) and Inner Mongolia Peoples’ Hospital (Approval No. YWLCSYLL–2025–010–23). Moreover, the ethics committees of all three hospitals allowed for a waiver of patient consent due to the observational and retrospective design of the work. Accordingly, strict patient data confidentiality was maintained throughout the study. All patient data were fully anonymized and de-identified prior to analysis. No identifiable personal information was retained in the study database. Moreover, all clinical records were handled in accordance with local data protection laws and regulations, ensuring complete patient confidentiality.
Consent for Publication
Not applicable as all figures and tables presented in this manuscript are original.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the China International Medical Foundation (2022–N–01–09), and Wu Jieping Medical Foundation (320.6750.2023–13–7).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Reichert MC, Medeiros EA, Ferraz FA. Hospital-acquired meningitis in patients undergoing craniotomy: incidence, evolution, and risk factors. Am J Infect Control. 2002;30(3):158–15. doi:10.1067/mic.2002.119925
2. Wang KW, Chang WN, Huang CR, et al. Post-neurosurgical nosocomial bacterial meningitis in adults: microbiology, clinical features, and outcomes. J Clin Neurosci. 2005;12(6):647–650. doi:10.1016/j.jocn.2004.09.017
3. Valdoleiros SR, Torrão C, Freitas LS, Mano D, Gonçalves C, Teixeira C. Nosocomial meningitis in intensive care: a 10-year retrospective study and literature review. Acute Crit Care. 2022;37(1):61–70. doi:10.4266/acc.2021.01151
4. Filka J, Huttova M, Kurak J, et al. Inappropriately treated nosocomial meningitis is associated with higher mortality and more neurologic sequellae than appropriately treated meningitis. J Infect Chemother. 1999;5(2):108–109. doi:10.1007/s101560050019
5. Fang CT, Chen YC, Chang SC, Sau WY, Luh KT. Klebsiella pneumoniae meningitis: timing of antimicrobial therapy and prognosis. QJM. 2000;93(1):45–53. doi:10.1093/qjmed/93.1.45
6. Rodríguez-Lucas C, Fernández J, Martínez-Sela M, et al. Pseudomonas aeruginosa nosocomial meningitis in neurosurgical patients with intraventricular catheters: therapeutic approach and review of the literature. Enferm Infecc Microbiol Clin. 2020;38(2):54–58. doi:10.1016/j.eimc.2019.04.003
7. Federico G, Tumbarello M, Spanu T, et al. Risk factors and prognostic indicators of bacterial meningitis in a cohort of 3580 postneurosurgical patients. Scand J Infect Dis. 2001;33(7):533–537. doi:10.1080/00365540110026557
8. Korinek AM, Baugnon T, Golmard JL, van Effenterre R, Coriat P, Puybasset L. Risk factors for adult nosocomial meningitis after craniotomy: role of antibiotic prophylaxis. Neurosurgery. 2006;59(1):126–133. doi:10.1227/01.neu.0000243291.61566.21
9. Kourbeti IS, Jacobs AV, Koslow M, Karabetsos D, Holzman RS. Risk factors associated with postcraniotomy meningitis. Neurosurgery. 2007;60(2):317–326.
10. Chen C, Zhang B, Yu S, et al. The incidence and risk factors of meningitis after major craniotomy in China: a retrospective cohort study. PLoS One. 2014;9(7):e101961. doi:10.1371/journal.pone.0101961
11. Kourbeti IS, Vakis AF, Ziakas P, et al. Infections in patients undergoing craniotomy: risk factors associated with post-craniotomy meningitis. J Neurosurg. 2015;122(5):1113–1119. doi:10.3171/2014.8.JNS132557
12. Chen CH, Chang CY, Lin LJ, et al. Risk factors associated with postcraniotomy meningitis: a retrospective study. Medicine. 2016;95(31):e4329. doi:10.1097/MD.0000000000004329
13. Shi ZH, Xu M, Wang YZ, et al. Post-craniotomy intracranial infection in patients with brain tumors: a retrospective analysis of 5723 consecutive patients. Br J Neurosurg. 2017;31(1):5–9. doi:10.1080/02688697.2016.1253827
14. Chen S, Cui A, Yu K, Huang C, Zhu M, Chen M. Risk Factors Associated with Meningitis after Neurosurgery: a Retrospective Cohort Study in a Chinese Hospital. World Neurosurg. 2018;111:e546–e563. doi:10.1016/j.wneu.2017.12.110
15. Hernández Ortiz OH, García García HI, Muñoz Ramírez F, et al. Development of a prediction rule for diagnosing postoperative meningitis: a cross-sectional study. J Neurosurg. 2018;128(1):262–271. doi:10.3171/2016.10.JNS16379
16. Dong YM, Sun J, Li YX, et al. Development and Validation of a Nomogram for Assessing Survival in Patients With COVID-19 Pneumonia. Clin Infect Dis. 2021;72(4):652–660. doi:10.1093/cid/ciaa963
17. Liu L, Wang H, Zhao B, Liu X, Sun Y, Mao Y. Nomogram to predict the progression of patients with primary membranous nephropathy and nephrotic syndrome. Int Urol Nephrol. 2022;54(2):331–341. doi:10.1007/s11255-021-02859-x
18. Liu H, Li J, Guo J, Shi Y, Wang L. A prediction nomogram for neonatal acute respiratory distress syndrome in late-preterm infants and full-term infants: a retrospective study. EClinicalMedicine. 2022;50:101523. doi:10.1016/j.eclinm.2022.101523
19. Lang L, Wang T, Xie L, et al. An independently validated nomogram for individualised estimation of short-term mortality risk among patients with severe traumatic brain injury: a modelling analysis of the CENTER-TBI China Registry Study. EClinicalMedicine. 2023;59:101975. doi:10.1016/j.eclinm.2023.101975
20. Zheng G, Wang S, Lv H, Zhang G. Nomogram Analysis of Clinical Characteristics and Mortality Risk Factor of Non-Fermentative Gram-Negative Bacteria-Induced Post-Neurosurgical Meningitis. Infect Drug Resist. 2022;15:6379–6389. doi:10.2147/IDR.S385502
21. Zhang Y, Zeng Q, Fang Y, Wang W, Chen Y. Risk Prediction of Central Nervous System Infection Secondary to Intraventricular Drainage in Patients with Intracerebral Hemorrhage: development and Evaluation of a New Predictive Model Nomogram. Ther Innov Regul Sci. 2022;56(4):651–658. doi:10.1007/s43441-022-00403-2
22. Wang P, Song W, Cheng S, Shuai Y, Yang J, Luo S. Establishment of a Nomogram for Predicting Lumbar Drainage-Related Meningitis: a Simple Tool to Estimate the Infection Risk. Neurocrit Care. 2021;34(2):557–565. doi:10.1007/s12028-020-01076-1
23. Kong Y, Ye Y, Ma J, Shi G. Accuracy of heparin-binding protein for the diagnosis of nosocomial meningitis and ventriculitis. Crit Care. 2022;26(1):56. doi:10.1186/s13054-022-03929-x
24. Kong Y, Zhou D, Ye Y, Li Z, Shi G. Cerebrospinal Fluid Heparin-Binding Protein Improves the Evaluation of Functional Outcomes in Postcraniotomy Meningitis and Ventriculitis. Neurocrit Care. 2025;43(1):59–68. doi:10.1007/s12028-025-02224-1
25. Horan TC, Andrus M, Dudeck MA. CDC/NHSN surveillance definition of health care-associated infection and criteria for specific types of infections in the acute care setting. Am J Infect Control. 2008;36(5):309–332. doi:10.1016/j.ajic.2008.03.002
26. Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR. Guideline for prevention of surgical site infection, 1999. Hospital Infection Control Practices Advisory Committee. Infect Control Hosp Epidemiol. 1999;20(4):250–280. doi:10.1086/501620
27. DeConde AS, Suh JD, Ramakrishnan VR. Treatment of cerebrospinal fluid rhinorrhea. Curr Opin Otolaryngol Head Neck Surg. 2015;23(1):59–64. doi:10.1097/MOO.0000000000000124
28. Remeš F, Tomáš R, Jindrák V, Vaniš V, Setlík M. Intraventricular and lumbar intrathecal administration of antibiotics in postneurosurgical patients with meningitis and/or ventriculitis in a serious clinical state. J Neurosurg. 2013;119(6):1596–1602. doi:10.3171/2013.6.JNS122126
29. Citerio G, Signorini L, Bronco A, Vargiolu A, Rota M, Latronico N. for Infezioni LIquorali Catetere Correlate Study Investigators. External Ventricular and Lumbar Drain Device Infections in ICU Patients: a Prospective Multicenter Italian Study. Crit Care Med. 2015;43(8):1630–1637. doi:10.1097/CCM.0000000000001019
30. Ramanan M, Lipman J, Shorr A, Shankar A. A meta-analysis of ventriculostomy-associated cerebrospinal fluid infections. BMC Infect Dis. 2015;15(1):3. doi:10.1186/s12879-014-0712-z
31. Fu P, Zhang Y, Zhang J, Hu J, Sun Y. Prediction of Intracranial Infection in Patients under External Ventricular Drainage and Neurological Intensive Care: a Multicenter Retrospective Cohort Study. J Clin Med. 2022;11(14):3973. doi:10.3390/jcm11143973
32. Ciric I, Ragin A, Baumgartner C, Pierce D. Complications of transsphenoidal surgery: results of a national survey, review of the literature, and personal experience. Neurosurgery. 1997;40(2):225–237. doi:10.1097/00006123-199702000-00001
33. Morse JC, Chandra RK. Is there still a role for cranialization in modern sinus surgery? Curr Opin Otolaryngol Head Neck Surg. 2021;29(1):53–58. doi:10.1097/MOO.0000000000000691
34. Patel BS, Steinberg E, Pfohl SR, Shah NH. Learning decision thresholds for risk stratification models from aggregate clinician behavior. J Am Med Inform Assoc. 2021;28(10):2258–2264. doi:10.1093/jamia/ocab159
35. Ye T. Potential selection bias when subjects were excluded because of missing values. Am J Emerg Med. 2020;38(3):681. doi:10.1016/j.ajem.2019.12.003
36. Schafer JL, Olsen MK. Multiple Imputation for Multivariate Missing-Data Problems: a Data Analyst’s Perspective. Multivariate Behav Res. 1998;33(4):545–571. doi:10.1207/s15327906mbr3304_5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and External Validation of a Machine Learning Model for Predicting Wound Infection in Diabetic Foot Ulcers
Nie X, Jiang Y, Meng X, Liu J, Zhao H, Chen Y, Wang J, Lu T
Diabetes, Metabolic Syndrome and Obesity 2026, 19:586810
Published Date: 7 March 2026