Back to Journals » Journal of Multidisciplinary Healthcare » Volume 14
A Non-Infectious Uveitis Multidisciplinary Clinic in a Tertiary Referral Center: Clinical Impact and Added Value
Authors Leal I, Romão VC ![]() , Mano S, Khmelinskii N, Campanilho-Marques R, Ponte C, Macieira C, Oliveira-Ramos F, Vieira-Sousa E, Rosa CM, Rodrigues W, Abegão Pinto L
, Mano S, Khmelinskii N, Campanilho-Marques R, Ponte C, Macieira C, Oliveira-Ramos F, Vieira-Sousa E, Rosa CM, Rodrigues W, Abegão Pinto L ![]() , Marques-Neves C, Fonseca JE
, Marques-Neves C, Fonseca JE
Received 1 December 2020
Accepted for publication 29 January 2021
Published 22 March 2021 Volume 2021:14 Pages 695—704
DOI https://doi.org/10.2147/JMDH.S292981
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Inês Leal,1,2 Vasco C Romão,3,4 Sofia Mano,1,2 Nikita Khmelinskii,3,4 Raquel Campanilho-Marques,3,4 Cristina Ponte,3,4 Carla Macieira,3 Filipa Oliveira-Ramos,3,4 Elsa Vieira-Sousa,3,4 Carlos Miranda Rosa,3 Walter Rodrigues,1,2 Luís Abegão Pinto,1,2 Carlos Marques-Neves,1,2 João Eurico Fonseca3,4
1Ophthalmology Department, Hospital de Santa Maria, Centro Hospitalar Univeristário Lisboa Norte, Centro Académico de Medicina de Lisboa, Lisbon, Portugal; 2Centro de Estudos das Ciências da Visão, Clínica Universitária de Oftalmologia, Faculdade de Medicina, Universidade de Lisboa, Lisbon, Portugal; 3Rheumatology Department, Hospital de Santa Maria, Centro Hospitalar Universitário Lisboa Norte, Centro Académico de Medicina de Lisboa, Lisbon, Portugal; 4Rheumatology Research Unit, Instituto de Medicina Molecular, Faculdade de Medicina, Universidade de Lisboa, Lisbon, Portugal
Correspondence: Inês Leal
Hospital de Santa Maria, Centro Hospitalar Universitário Lisboa Norte Fax +351 21 780 5653
Email [email protected]
Abstract: Non-infectious uveitis (NIU) is a group of sight-threatening diseases that generates significant burden for the healthcare systems due to its adverse outcomes, irreversible structural complications in the eye with loss of visual function, limited clinical expertise and low-grade evidence for best practice. The usefulness of multidisciplinary care, specifically close collaboration between Rheumatologists and Ophthalmologists in NIU, has been emphasized in the literature. In this paper, the assessment tools and protocols used in our clinic are depicted and an overview of our activity with a brief description of the patients included in our registry, between 2018 and 2020 is provided. The cohort of 290 patients assessed in our NIU clinic, their demographics, sources of referral, details about immunosuppression treatment, and internal and external collaborations is described. This experience-based manuscript aims to describe the general functioning of our multidisciplinary NIU clinic, highlighting the benefits and drawbacks of multidisciplinary team management in patients with NIU, ultimately initiating a dialogue on what an NIU clinic should be and providing information for newly NIU clinics start-up. In conclusion, establishing a standardized and multidisciplinary clinic in NIU allows to systematically observe and follow-up this infrequent disease at a tertiary hospital level, thus improving quality of care delivery and research avenues.
Keywords: uveitis, ophthalmology, rheumatology
Introduction
Uveitis comprises a heterogeneous group of inflammatory diseases of the uvea of both infectious and non-infectious etiologies.1 Specifically, non-infectious uveitis (NIU) results from an immune-mediated response to ocular antigens. Complications of uveitis can be sight threatening, severely impairing quality of life.1–4 It has an estimated prevalence of 121/100,000 people in adults and 29/100,000 people in children, being more common in western countries.5,6 Hence, there is a significant burden for the healthcare systems and the working-age population associated with NIU.7,8 In particular, NIU is associated with late and often incorrect diagnosis, adverse outcomes, irreversible structural complications, limited clinical expertise and low-grade evidence for best practice.3,7
Multidisciplinary teams (MDT) have been recognized in the literature as the core model for managing complex chronic conditions. They are able to provide the most differentiated care to patients,9,10 requiring pro-active and multidirectional relationship between the clinicians involved in the patient care delivery.11 In 2017, the Fundamentals Of Care for Uveitis (FOCUS) study group suggested that patients with NIU may benefit from the input from more than one medical specialty3 and the added value of this collaboration has been demonstrated elsewhere.8 Moreover, this initiative underlined the lack of guidelines to make the dialog between Rheumatology and Ophthalmology clinicians effective.3 The usefulness of these clinics and close collaboration between Rheumatologists and Ophthalmologists in NIU has been shown in literature elsewhere.12–15 To fill this need related to the complexity of the management of NIU patients, a multidisciplinary approach has been embraced, since 2018, in Hospital de Santa Maria, Centro Hospitalar Universitário Lisboa Norte (CHULN), a tertiary referral hospital. Our goal is to promote optimal management of patients with NIU, offering adequate multidisciplinary care, to standardize diagnostic investigation to newly referred patients, and to provide innovative registry tools and research support.
Ethical approval for this study was obtained from the CHULN Ethics Committee.
The aim of this experience-based manuscript is to describe the general functioning of our NIU clinic, highlighting the benefits and drawbacks of multidisciplinary team management in patients with NIU, ultimately initiating a dialogue on what an NIU clinic should be. In addition, we describe the assessment tools and protocols used and provide an overview of our activity with a brief description of the patients included in our registry, Uveite.pt, between 2018 and 2020.
Non-Infectious Uveitis Outpatient Clinic
Description
In Portugal, treatment for NIU is accessible in several ophthalmology public services. In general, there is an ophthalmologist subspecialized in ocular inflammation or a consultant with a special interest in uveitis that provides care to these patients. Portugal has not yet implemented a structured post-graduated training to allow subspecializing on uveitis. Since 2018, the Ophthalmology Department of CHULN has developed a dedicated NIU clinic, hereinafter referred as CHULN-NIU clinic, with the unconditional support of the Rheumatology Department. In 2020, this outpatient clinic gave a major contribution to the development of a specifically designed online electronic medical record Uveite.pt (the Portuguese registry of ocular inflammatory diseases).
Currently, this uveitis outpatient clinic is run by two Consultant Ophthalmologists (IL, SM) and by one Ophthalmology trainee (according to the trainees’ rotation schedule). We provide a fast-track approach to signalized patients: 1) patients identified in our Emergency Department, 2) children with a clinical suspicion or new diagnosis of juvenile idiopathic arthritis (JIA), 3) patients with sight-threatening disease and/or needing urgent Ophthalmology assessment in this setting. All patients with the final diagnosis of ocular inflammation or with the need for follow-up in this clinic (eg children which JIA undergoing long-term uveitis screening) are registered in Uveite.pt. Milestones recognized as crucial in the development of the CHULN-NIU clinic16 are depicted in Figure2, Figure 1 and focus areas are shown in Table 1.
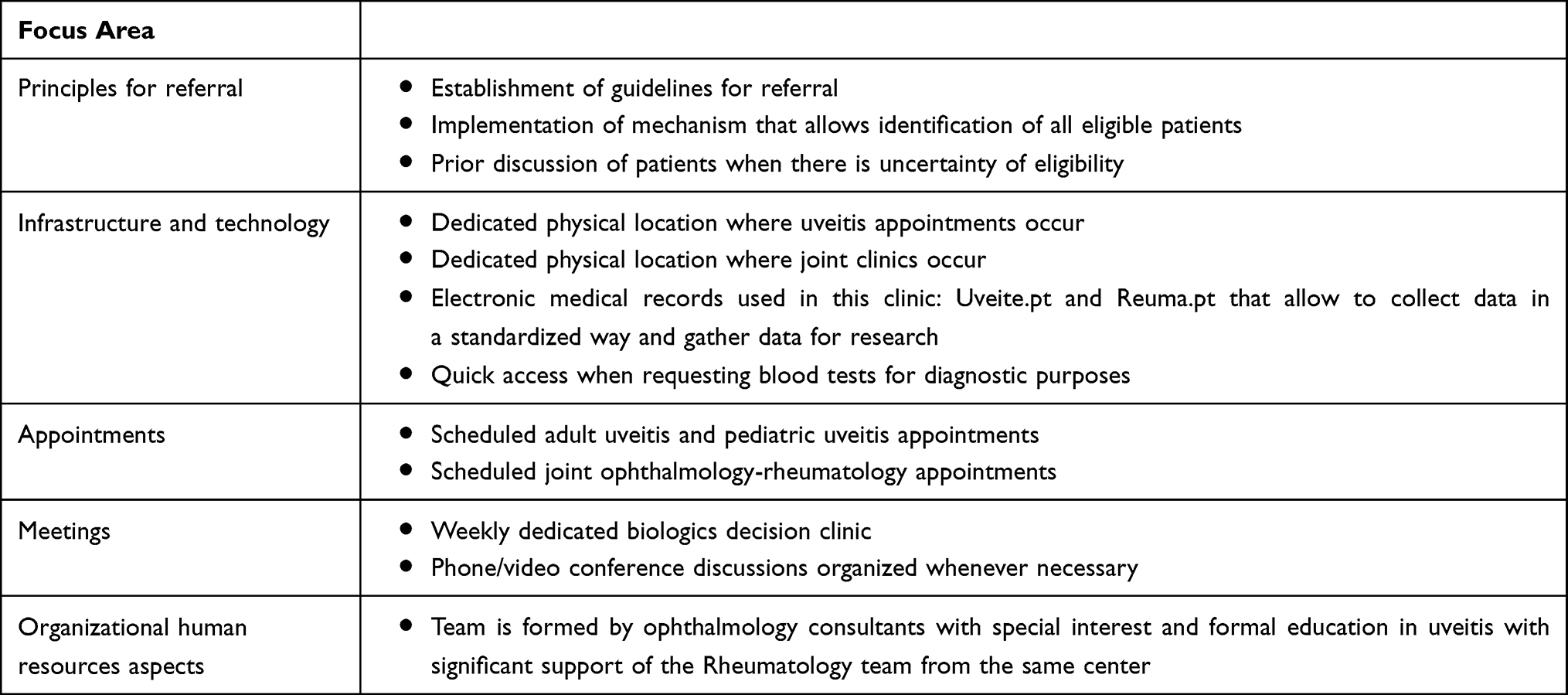 |
Table 1 Focus Areas of CHULN NIU-Rheumatology Team |
 |
Figure 1 Milestones towards a successful ophthalmology-rheumatology multidisciplinary team (MDT). Adapted from Snipelisky, D. et al. How to Develop a Cardio- Oncology Clinic. Heart Fail. Clin. 13, 347–359 (2017), with permission from Elsevier.16 |
Assessment Tools
The CHULN-NIU clinic uses an electronic medical record (EMR) platform named Uveite.pt. Uveite.pt, the Ocular Inflammatory Diseases Portuguese Register, was developed by the Portuguese Society of Ophthalmology (SPO), with the collaboration of the Portuguese Society of Rheumatology, as it was designed with the same structure as the previously developed Reuma.pt, the Rheumatic Diseases National Register.17,18 This plan began in 2017. This is a nation-wide customized web-based platform for uveitis patients where prospective clinical information can be recorded. This platform can be utilized for both clinical practice and real-world-based research. It works as a central repository and reporting tool that can analyze patient data to produce easy-to-interpret national and inter-practice benchmark reports. The database information security was approved by the Portuguese National Commission for Data Protection and the ethics committees of the participating institutions. Registered patients are required to sign an informed consent. All identifiable data is encrypted, only accessible through an individual password attributed to clinicians, who can only visualize data related to their center. Specifically for uveitis, this platform has several advantages: the ability to record information in a standardized way; electronic forms specifically designed to monitor ocular inflammatory activity and to capture drug history, focusing on immunosuppressants and/or intravitreal injections; a pre-biologic therapy checklist; the possibility of standardized measuring and follow-up of visual acuity, intraocular inflammation grading or central macular thickness over time with the aid of automatic generated charts and graphics; summary charts showing the patients’ clinical status; and the generation of a final summary report for each given appointment. Furthermore, it allows patients to answer remotely to patient-reported outcomes measures (PROM), thus involving them in their own care. The adoption of this platform enables standardization and improvement of clinical practice in uveitis. It can apprehend the repercussion of medical and surgical treatments in ocular inflammatory disorders, supporting clinicians in the strict monitorization of drug adverse reactions and surgical outcomes. Unquestionably, Uveite.pt became a crucial decision-making tool in the CHULN-NIU clinic. A composite figure of Uveite.pt screens is available as Supplementary Data in Supplementary Figure 1.
In order to complement clinical outcomes, we also emphasize the completion of PROMs in our clinic. Specifically, we are implementing two questionnaires among NIU patients: the Work Productivity and Activity Impairment (WPAI) Uveitis Questionnaire19,20 and the Health-Related Productivity Questionnaire (HRPQ).21 While the former is an instrument developed to the amount of both absenteeism (work time missed) and presenteeism (reduced on-the-job effectiveness) due to uveitis, the latter was developed as a brief, self-administered instrument for the collection of work productivity data within clinical trials and survey data collections. In close collaboration with the HRPQ authors, our department is seeking the validation of this questionnaire among Portuguese patients with uveitis.21 Finally, in an international collaboration with Pediatric Rheumatology, our Ophthalmology Department is participating in the cross-cultural validation of the Portuguese version of the effect of Youngsters’ Eyesight on Quality of Life Questionnaire (EYE-Q).22
Blood Testing in Uveitis
We have developed specific laboratory profiles in the CHULN clinical pathology electronic platform to standardize the blood test requests for all newly diagnosed NIU patients, both at baseline and during disease monitoring. These blood test profiles have been developed with the support of the Manchester Uveitis Clinic. For instance, when assessing a patient with posterior uveitis or pediatric uveitis for the first time, we can, with a single click, select all required blood tests for that given patient. Naturally, this quick selection of blood tests is flexible and allows customizing it to the individual patient. This method has the advantage of being timesaving to the NIU team and helpful for the non-uveitis-dedicated ophthalmologists who contact the patient for the first time in the Emergency Department before referral. Assessing a patient for the first time in the CHULN-NIU clinic with already available blood tests significantly expedites the diagnostic march and aids initial treatment decisions. Currently, the following standardized blood profiles are available: non-granulomatous anterior uveitis, granulomatous anterior uveitis, intermediate uveitis, posterior or panuveitis, scleritis, retinal vasculitis and pediatric uveitis and it is possible to eliminate/add blood tests according to the specific case. Uveite.pt also enables to directly upload the output of these blood tests, creating a prospective monitoring of laboratory data. Blood or ocular fluids obtained during workup are collected for storage in a dedicated collection of the Biobanco-IMM, Lisbon Academic Medical Centre, specifically created to support this clinic.
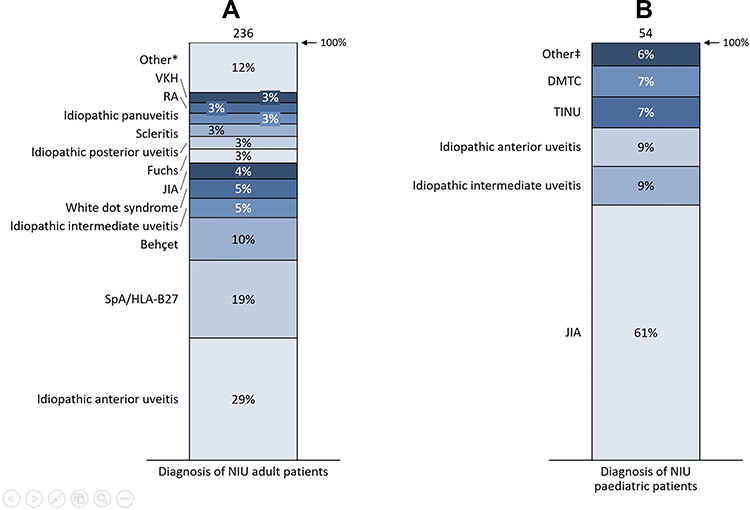 |
Figure 2 Diagnosis of adult (A) and pediatric patients (B) referred to the CHULN-NIU clinic. Abbreviations: SpA, spondyloarthritis; NIU, non-infectious uveitis; HLA, human leucocyte antigen; JIA, juvenile idiopathic-arthritis; RA, rheumatoid arthritis; VKH, Vogt-Koyanagi-Harada syndrome; TINU, tubulointerstitial nephritis and uveitis syndrome; MCTD, mixed connective tissue disease. Notes: Other*: Cogan syndrome, mixed connective tissue disease, episcleritis, multiple sclerosis uveitis, Posner-Schlossman syndrome, retinal vasculitis, systemic lupus erythematosus, sarcoidosis, Takayasu syndrome, granulomatosis with polyangiitis, Other‡: idiopathic panuveitis, retinal vasculitis, scleritis. |
Experience
A total of 290 patients were referred and assessed in the CHULN-NIU clinic between June 2018 and June 2020 (Table 2). Of these, 59.31% were female (n=172) and 18.6% (n=54) were pediatric patients (age < 18). Patients’ mean age was 36.9±19.62 (range: 2–90) years old. Overall, referrals were made by Ophthalmology (61%, n= 177), Rheumatology (32.4%, n=94), Pediatrics (1.03%, n=3), Emergency Medicine (3.10%, n=9), Internal Medicine (1.38%, n=4), Infectiology (0.3%, n=1), and Occupational Medicine (0.34%, n=1) departments; one patient was referred from another hospital (0.34%, n=1). Diagnosis of adult and pediatric patients is depicted in Figure 3. Details about csDMARD (conventional synthetic disease-modifying antirheumatic drugs) and bDMARD (biological disease-modifying antirheumatic drugs) treatment are detailed in Figures 3 and 4. Regarding adult patients, 162 (68,4%) were not on any DMARDs and 18 (7,6%) were simultaneously under csDMARD and bDMARD during any time of their follow-up. Considering pediatric patients, 24 (45,3%) were not on any DMARD and 12 (22,6%) were simultaneously under csDMARD and bDMARD during any time of their follow-up.
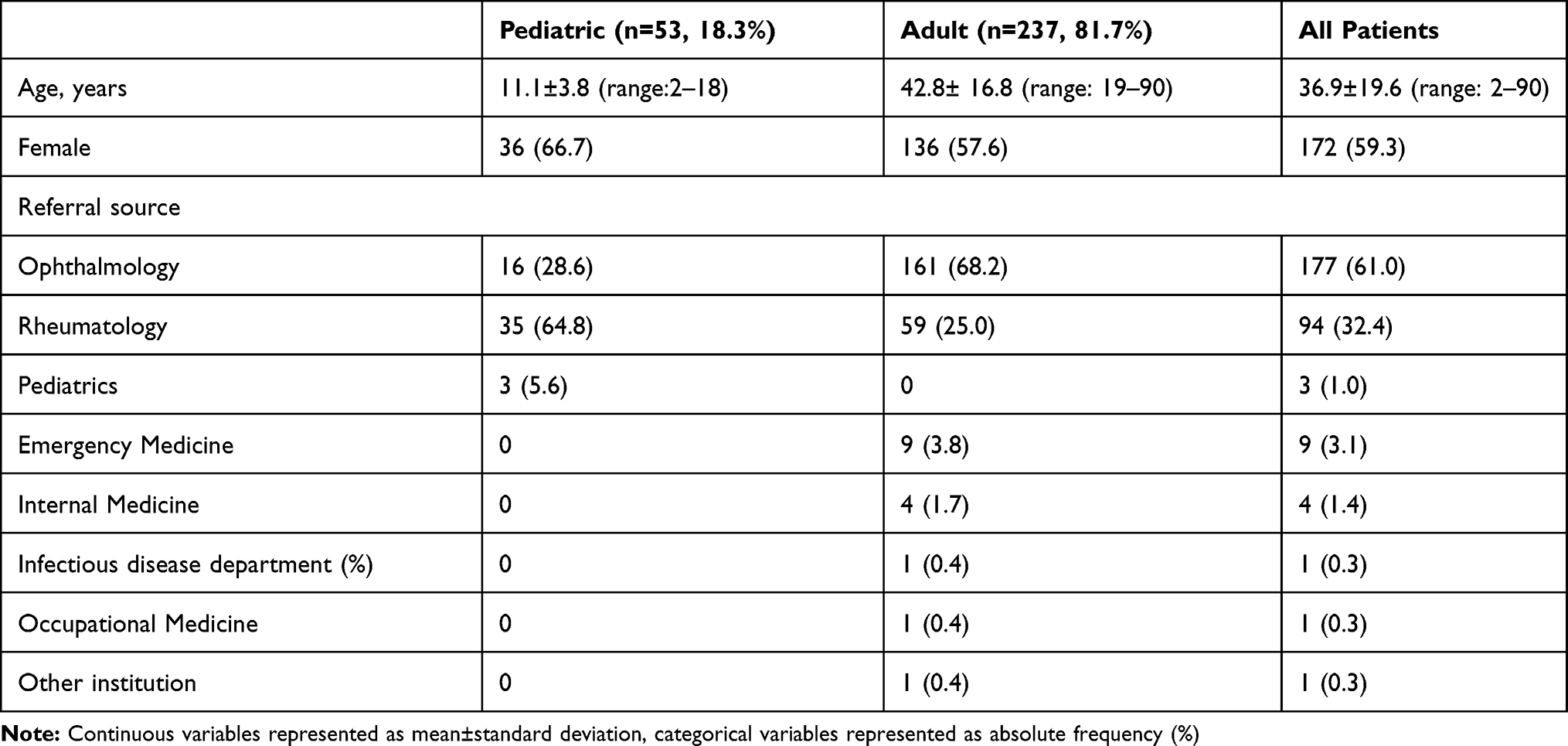 |
Table 2 Demographics and Referrals of the Patients Observed at the CHULN-NIU Clinic (June 2018–June 2020) |
 |
Figure 3 Conventional synthetic DMARD treatment of NIU adult (A) and pediatric (B) patients. Abbreviations: NIU, non-infectious uveitis; MTX, methotrexate; AZA, azathioprine; MMF, Mycophenolate mofetil; SSA, salazopyrine; CsA, Cyclosporine A; csDMARD, conventional synthetic disease-modifying antirheumatic drugs. |
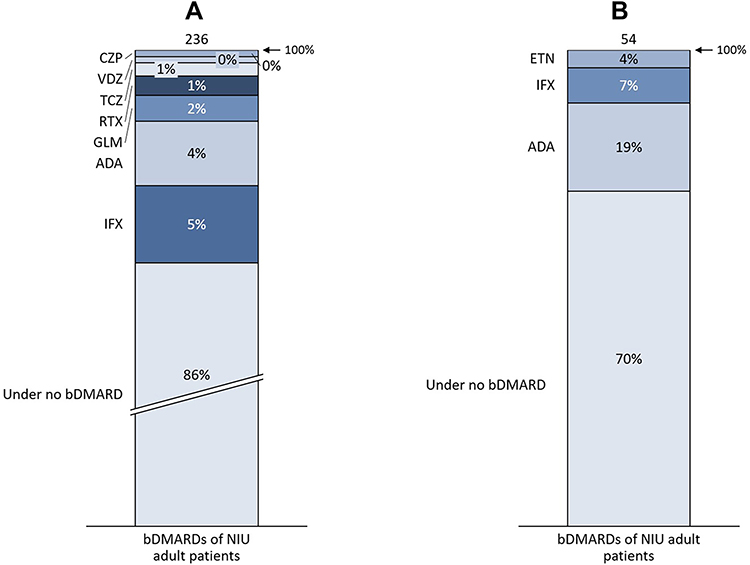 |
Figure 4 Biologic treatment of adult (A) and pediatric (B) patients. Abbreviations: NIU, non-infectious-uveitis; IFX, infliximab; ADA, adalimumab; GLM, golimumab; RTX, rituximab; TCZ, tocilizumab; VDZ, vedolizumab; CZP, certolizumab; ETN, etanercept. |
Management of Immunosuppressive Treatment
Although with limited evidence in the literature, systemic immunosuppression treatment is widely used to treat NIU. Drugs generally prescribed for NIU include corticosteroids, csDMARD (mainly T-cell inhibitors such as cyclosporine and tacrolimus and anti-metabolites such as methotrexate, mycophenolate mofetil and azathioprine) and bDMARD, mainly tumor necrosis factor agents inhibitors (anti-TNF), among others. Due to its related adverse effects (specially bone marrow suppression, liver and renal toxicity) patients regularly treated with these drugs need frequent monitorisation.3,23 In our clinic, the two Ophthalmologist Consultants are responsible to initiate, prescribe and monitor adverse effects from csDMARD (mainly T-cell inhibitor and anti-metabolites). To safely monitor these patients, during appointments we regularly fill a team shared spreadsheet containing a list of all patients on csDMARD and the dates and results of blood tests. Moreover, when a patient is on biologic treatment, the follow-up for monitoring disease progression is done in the Ophthalmology clinic, but specifically for bDMARD monitoring purposes the patient undergoes trimestral physical exam and blood tests at the Rheumatology day-care unit. When patients have a concurrent systemic rheumatic disease, they have also follow-up with the Rheumatology team according to their specific underlying disease.
Internal Collaborations – Multidisciplinary Continuous Work with the Rheumatology Department and Bonds with the Glaucoma Team in Ophthalmology Department
Despite regular interaction between several medical specialties, we must emphasize the close relationship established between Ophthalmologists dedicated to this clinic and the Rheumatology Department of CHULN. It was largely because of this close proximity that the development of the NIU clinic was able to take place. In particular, one of the current Ophthalmologists working in the clinic (IL), did a six-month rotation in the Rheumatology Department, in order to get acquainted with patients’ diagnosis, investigations, and correct management in a rheumatology setting. Most importantly, this was also fundamental to gain expertise in managing DMARD treatment. Regular interactions with specific Rheumatology clinics include frequent discussion and referrals to and from the Pediatric Rheumatology clinic, Vasculitis clinic (described elsewhere)24 and Spondyloarthritis clinic. The NIU clinic also offers continuous support to Rheumatology inpatients, providing urgent ophthalmologic examinations for patients with suspected ocular involvement of systemic diseases.
Other significant internal collaborations are detailed below separately because of their specificity:
Weekly Dedicated Biologics Decision Clinic
Pre-immunosuppression work-up is vital to plan long-term treatment with systemic drugs.3,25 It is essential that all past medical history is carefully reviewed, that certain secondary causes of NIU are excluded, and that a minimum work-up is performed in order to safely start a bDMARD. To plan for treatment escalation, more specifically to initiate bDMARD, the Ophthalmology clinicians join the Rheumatology Department weekly biologics decision clinic. This joint meeting allows for open and detailed discussions of each case, bringing focus to the patient current disease, findings, investigations, prognosis, best treatment and possible adverse effects. These are actively discussed not only with the clinician who attended the patient in the clinic but also with the rest of the team, benefitting from the group experience and knowledge. Moreover, in cases in which primary or secondary failure to bDMARD is diagnosed, a team discussion of therapeutic options is crucial to ensure that patients receive the best care possible. Moreover, these alternatives are further discussed with the patient, in a shared decision basis.
Joint Ophthalmology-Rheumatology Clinic
In complex cases, whenever there is a need to clarify a challenging diagnosis and establish common therapeutic goals, the patient is observed in a joint clinic. This clinic does not occur on a fixed schedule but is organized whenever needed. In the same Ophthalmology room where this joint clinic takes place, two computers and desks are available, as well as a couch examination and a slit lamp, allowing to run Ophthalmology and Rheumatology examinations in the same place and time. The goal is to provide a one-stop service for such patients, so that their care is jointly planned, and they are able to consult the required specialists and undergo investigations and/or treatment with the minimum number of hospital visits. After the first visit, which generally expedites a diagnosis and/or a therapeutic shared decision, the patient may maintain joint clinics or can pursue separate future appointments, according to the clinical setting. This joint clinic is available for adult patients (in collaboration with a Rheumatology Consultant mainly dedicated to Spondyloarthritis and/or Vasculitis) and for children (in collaboration with a Pediatric Rheumatologist).
Shared Care with Glaucoma Team
Uveitic glaucoma is a common and devastating cause of irreversible sight-loss in uveitis, affecting up to 20% of uveitis patients. The successful treatment of uveitic glaucoma is undoubtedly correlated with prompt and immediate therapeutic shared decisions, ideally between an uveitis and glaucoma subspecialist.26 In our clinic, we have a very solid collaboration, offering a prompt referral (generally on the same day or at least the same week when glaucoma is diagnosed) to the glaucoma head team (LAP), whenever necessary. This shared care allows refinement of the glaucoma medical therapy and, more importantly, expedites patients that need more invasive procedures to lower intraocular pressure, namely glaucoma filtering surgeries. Surgery is particularly effortful in these patients, not only due to the inflammatory nature of the underlying condition but also to the patients’ relatively young age – both risk factors for surgical failure. Surgical options are therefore particularly challenging and involve techniques not routinely used in non-tertiary hospitals. Moreover, when glaucoma surgery is performed, peri-operatively immunosuppression is always actively discussed between uveitis and glaucoma teams, in order to achieve the best surgical goals in this exceptionally challenging clinical entity.
External Collaborations and Research
Collaborations have been established between the CHULN-NIU clinic and international centers which have been nurtured throughout time to support knowledge exchange. The CHULN-NIU clinic benefits from the close collaboration and support of two international uveitis clinics with large experience in the field: Manchester Royal Eye Hospital Uveitis Clinic (formerly supervised by Professor Nicholas Jones, currently supervised by Miss Laura Steeples) and Fundación Jimenez Dias Uveitis Clinic (Doctor Ester Carreño). Discussions about challenging cases are regularly held, and joint scientific projects in the field of uveitis are ongoing.
Discussion
Uveitis comprises a group of inflammatory diseases of the eye, many of which do not have a fully understood pathophysiology, an established diagnosis or a standardized treatment.27–30 Moreover, inflammatory eye diseases are infrequent when compared to other common ophthalmological conditions. These two factors playing together may pose significant challenges in patient management.
The UK Department of Health defines an MDT as a
Group of people of different health-care disciplines, which meets together at a given time (whether physically in one place, or by video or teleconferencing) to discuss a given patient and who are each able to contribute independently to the diagnostic and treatment decisions.31
Multidisciplinary teamwork in NIU involves coordinated efforts from people with diverse backgrounds and expertise, coming together in the management of a patient, aiming at best care. These health professionals play a vital role in providing adequate, evidence-based and cost-effective care.9,32,33 MDTs have been recognized to contribute to better coordination of care, development of clinical skills, and dissemination of the most recent evidence-based management recommendations.34 These teams guarantee that a full range of therapeutic options are considered early so that patients receive appropriate and timely treatments. Specifically, in our sample we think that the way this NIU clinic is organized enhances a corticoid-sparing approach in our patients, decreasing morbidity and optimizing prognosis.8 Active discussion of medical history and investigations, reviewing imaging exams in the team, can be an authentic game-changer when it comes to decision-making in entangled cases.35 Not only patients but also clinicians benefit from multidisciplinary work. Indeed, greater job fulfillment and satisfaction have been suggested as a result of working in an MDT.36 These teams are also more prone to develop collaborative research, engage in multidisciplinary clinical trials and offer educational opportunities to medical students and/or specialty trainees who can take unprecedented advantages from the insight of a multidisciplinary management of patients.35,36
Despite the existence of informal discussion between clinicians from different specialties, a formalized and structured MDT is absolutely vital to increase the chances of successful management of patients with NIU, thus improving their prognosis. From our perspective, maintaining this structure and regular communication between peers demands significant coordination, being permanently aware of relevant literature, well-functioning team-work, and efficient and smooth routines.
With regards to the Ophthalmology and Rheumatology joint clinic, we feel that these clinics are more patient-friendly. Patients are more involved, are better able to ask questions at the same visit rather than having to do so separately with both specialties, weeks apart. Discussions regarding the choice of therapy are tailored to fit the needs and expectations of each individual patient. A patient-centered approach is thus considered essential to provide optimal care to these patients. Therefore, in every decision, we integrate individual psychosocial aspects, comorbidities, patients and families’ preferences into the management plan. Regular and easy contacts between Ophthalmology and Rheumatology teams, even outside the joint clinic (e.g.: frequent emails and phone calls that are part of our routine interaction) allow us to quickly answer questions that would not always require a full rheumatology workup, such as whether to change/initiate csDMARD, interpretation and management when in presence of drugs side effects, etc.
One of the greatest challenges that has been recognized in the literature is the increased staff number that is required for the provision of multidisciplinary care. Although public services have been recognized to be best able to provide an MDT service, funding has been recognized to be a barrier to allow organization and access to these services.37 In our experience, in a large tertiary academic center, this has been largely overcome by the drive and eagerness to collaborate of all the health care professionals of the MDT.
When analyzing the referrals to our NIU clinic of our sample it is contrasting that around 65% of the pediatric referrals were done by Rheumatologists, while only 25% of adult patients were referred from this specialty. The large proportion of children referred from Rheumatology to the NIU clinic is explained by the need for a structured regular ophthalmological screening program of JIA children, whereas in adults there is virtually no systemic rheumatic disease requiring ophthalmology screening among ophthalmological asymptomatic patients. Therefore, in the adult group the majority of referrals to the NIU clinic (around 68%) have been originated from other Ophthalmology clinics, either originating in elective General Ophthalmology appointments or from Eye Casualty.
In our paper, around 21% of the adult patients were on csDMARD and 14% on bDMARD. These values correlate fairly well with a recent monocentric retrospective study published in 2020 including 157 adult patients followed in a multidisciplinary clinic with Ophthalmologists and Rheumatologists. In this study, around 21% of patients were on csDMARD and 6% of patients were on bDMARD. The highest proportion of patients on bDMARD may be explained partially by the fact that the CHULN Rheumatology Department is one of the busiest in the country, receiving complex cases and, therefore, possibly prescribing more often bDMARD than other Portuguese centers. When comparing our pediatric sample with published data, we find that in our sample around 48% of children were on csDMARD and 30% on bDMARD. In a North American study34 describing the epidemiology of pediatric uveitis including 527 children, 6% of children were on bDMARD and 27% on csDMARD. Although our results differ to some extent from those, this American study includes 10% of patients with a diagnosis of infectious uveitis and, therefore, not treated with immunosuppression. Moreover, this study included patients visits dated before 2005, and the use of DMARDs for pediatric uveitis was not as widespread as nowadays.
A limitation of our work is the relatively short period of functioning of this clinic; however, we aimed with this report to fine-tune our procedures and workflow. A second limitation is the lack of key performance indicators which we plan to assess in due time and publish in the future.
Conclusion
In summary, a formal standardized MDT approach to a complex disease such as NIU, including patient pathways for diagnosis and follow-up, treatment protocols and standardized EMR, allows for knowledge exchange and broadening of expertise in this field, ultimately offering cutting-edge care for patients with NIU. As such, establishing a standardized and multidisciplinary clinic in NIU allows to systematically observe and follow-up this infrequent disease at a tertiary hospital level, thus improving quality of care delivery and research avenues. Hereafter, we plan to maintain our teamwork, enriching our clinical experience with increasing numbers of patients in our cohort captured in Uveite.pt and flourishing the national and international collaborations in uveitis that have been launched.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Cordero-Coma M, Sobrin L. Anti–tumor necrosis factor-α therapy in uveitis. Surv Ophthalmol. 2015;60(6):575–589. doi:10.1016/j.survophthal.2015.06.004
2. Caspi RR. A look at autoimmunity and inflammation in the eye. J Clin Invest. 2010;120(9):3073–3083. doi:10.1172/JCI42440
3. Dick AD, Rosenbaum JT, Al-Dhibi HA, et al. Guidance on noncorticosteroid systemic immunomodulatory therapy in noninfectious uveitis: Fundamentals Of Care for UveitiS (FOCUS) initiative. Ophthalmology. 2018;125(5):757–773. doi:10.1016/j.ophtha.2017.11.017
4. Leal I, Rodrigues FB, Sousa DC, et al. Efficacy and safety of intravitreal anti-tumour necrosis factor drugs in adults with non-infectious uveitis - a systematic review. Acta Ophthalmol. 2018;96(6):e665–e675. doi:10.1111/aos.13699
5. Thorne JE, Suhler E, Skup M, et al. Prevalence of noninfectious uveitis in the United States. JAMA Ophthalmol. 2016;21287:1–8. doi:10.1001/jamaophthalmol.2016.3229
6. Tsirouki T, Dastiridou A, Symeonidis C, et al. A focus on the epidemiology of uveitis. Ocul Immunol Inflamm. 2018;26(1):2–16. doi:10.1080/09273948.2016.1196713
7. Thorne JE, Skup M, Tundia N, et al. Direct and indirect resource use, healthcare costs and work force absence in patients with non-infectious intermediate, posterior or panuveitis. Acta Ophthalmol. 2016;94(5):e331–e339. doi:10.1111/aos.12987
8. Van Bentum RE, Van den Berg JM, Wolf SE, et al. Multidisciplinary management of auto-immune ocular diseases in adult patients by ophthalmologists and rheumatologists. Acta Ophthalmol. 2020:1–7. doi:10.1111/aos.14548
9. Ugwumadu L, Chakrabarti R, Williams-Brown E, et al. The role of the multidisciplinary team in the management of deep infiltrating endometriosis. Gynecol Surg. 2017;14(1):1. doi:10.1186/s10397-017-1018-0
10. Cobo-Ibáñez T, Villaverde V, Seoane-Mato D, et al. Multidisciplinary dermatology–rheumatology management for patients with moderate-to-severe psoriasis and psoriatic arthritis: a systematic review. Rheumatol Int. 2016;36(2):221–229. doi:10.1007/s00296-015-3377-z
11. Cosmai L, Porta C, Perazella MA, et al. Opening an onconephrology clinic: recommendations and basic requirements. Nephrol Dial Transplant. 2018;33(9):1503–1510. doi:10.1093/ndt/gfy188
12. Venkatesh P, MacRae M, Fleck BW. Lothian combined paediatric ophthalmology and rheumatology service [3]. Br J Ophthalmol. 2006;90(12):1549–1550. doi:10.1136/bjo.2006.098905
13. Abd El Latif E. AB1090 analysis of a cohort of patients attending a combined ophthalmology-rheumatology clinic in a tertiary referral centre in egypt. Ann Rheum Dis. 2018;77(Suppl2):1654LP–1655. doi:10.1136/annrheumdis-2018-eular.1627
14. la Mora A, De, Aurrecoechea E, Del Corral AD, Calvo J. Rheumatology-ophthalmology collaborative uveitis units may improve the diagnostic and therapeutic approach of this pathology: experience from a uveitis unit in a secondary Spanish Hospital. J Arthritis. 2016;5(5). doi:10.4172/2167-7921.1000215
15. Aurrecoechea E, Del Corral AD, de la Mora A, Calvo-Aén J, Romera E. Rheumatology-ophthalmology collaborative uveitis units may improve the diagnostic approach of this pathology: experience from a uveitis unit in a secondary Spanish Hospital.
16. Snipelisky D, Park JY, Lerman A, et al. How to develop a cardio-oncology clinic. Heart Fail Clin. 2017;13(2):347–359. doi:10.1016/j.hfc.2016.12.011
17. Santos MJ, Canhão H, Faustino A, Fonseca JE. Reuma.pt – a case study. Acta Med Port. 2016;29(2):83. doi:10.20344/amp.7243
18. Santos MJ, Canhão H, Mourão AF, et al. Reuma.pt contribution to the knowledge of immune-mediated systemic rheumatic diseases. Acta Reumatol Port. 2017;2017(3):232–239.
19. Zhang W, Bansback N, Boonen A, Young A, Singh A, Anis AH. Validity of the work productivity and activity impairment questionnaire–general health version in patients with rheumatoid arthritis. Arthritis Res Ther. 2010;12(5):R177–R177. doi:10.1186/ar3141
20. Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4(5):353–365. doi:10.2165/00019053-199304050-00006
21. Kumar RN, Hass SL, Li JZ, Nickens DJ, Daenzer CL, Wathen LK. Validation of the Health-Related Productivity Questionnaire Diary (HRPQ-D) on a sample of patients with infectious mononucleosis: results from a Phase 1 multicenter clinical trial. J Occup Environ Med. 2003;45(8):899–907. doi:10.1097/01.jom.0000083039.56116.79
22. Angeles-Han ST, Yeh S, McCracken C, et al. Using the effects of youngsters’ eyesight on quality of life questionnaire to measure visual outcomes in children with uveitis. Arthritis Care Res. 2015;67(11):1513–1520. doi:10.1002/acr.22627
23. Angeles‐Han ST, Lo MS, Henderson LA, et al. Childhood arthritis and rheumatology research alliance consensus treatment plans for juvenile idiopathic arthritis–associated and idiopathic chronic anterior uveitis. Arthritis Care Res. 2019;71(4):482–491. doi:10.1002/acr.23610
24. Khmelinskii N, Seixas MI, Ponte C, Fonseca JE, Macieira C. The added value of a vasculitis clinic in a tertiary referral hospital. Acta Med Port. 2018;31(11):614–617. doi:10.20344/amp.9875
25. Barry RJ, Nguyen QD, Wlee R, Imurray P, Denniston AK. Pharmacotherapy for uveitis: current management and emerging therapy. Clin Ophthalmol. 2014;8:1891–1911. doi:10.2147/OPTH.S47778
26. Friedman DS, Holbrook JT, Ansari H, et al. Risk of elevated intraocular pressure and glaucoma in patients with uveitis: results of the multicenter uveitis steroid treatment trial. Ophthalmology. 2013;120(8):1571–1579. doi:10.1016/j.ophtha.2013.01.025
27. Long M, Tao S, Vega D, Jiang T, Wen Q, Sophia L. Big data and uveitis. Ophthalmology. 2016;8(5):444–454. doi:10.1158/1940-6207.CAPR-14-0359.Nrf2-dependent
28. Lee RW, Nicholson LB, Sen HN, et al. Autoimmune and autoinflammatory mechanisms in uveitis. Semin Immunopathol. 2014;36(5):581–594. doi:10.1007/s00281-014-0433-9
29. Durrani OM, Tehrani NN, Marr JE, Moradi P, Stavrou P, Murray PI. Degree, duration, and causes of visual loss in uveitis. Br J Ophthalmol. 2004;88(9):1159–1162. doi:10.1136/bjo.2003.037226
30. Dick AD, Forrester JV, Liversidge J, Cope AP. The role of tumour necrosis factor (TNF-??) in experimental autoimmune uveoretinitis (EAU). Prog Retin Eye Res. 2004;23(6):617–637. doi:10.1016/j.preteyeres.2004.06.005
31. Health D of. Manual for Cancer Services. London; 2004.
32. Wagner EH. Effective teamwork and quality of care. Med Care. 2004;42(11):1037–1039. doi:10.1097/01.mlr.0000145875.60036.ed
33. Liu A, Yoo ER, Siddique O, Perumpail RB, Cholankeril G, Ahmed A. Hepatic encephalopathy: what the multidisciplinary team can do. J Multidiscip Healthc. 2017;10:113–119. doi:10.2147/JMDH.S118963
34. Rosell L, Wihl J, Hagberg O, Ohlsson B, Nilbert M. Function, information, and contributions: an evaluation of national multidisciplinary team meetings for rare cancers. Rare Tumors. 2019;11:203636131984169. doi:10.1177/2036361319841696
35. Fleissig A, Jenkins V, Catt S, Fallowfield L. Multidisciplinary teams in cancer care: are they effective in the UK? Lancet Oncol. 2006. doi:10.1016/S1470-2045(06)70940-8
36. Haward R, Amir Z, Borrill C, et al. Breast cancer teams: the impact of constitution, new cancer workload, and methods of operation on their effectiveness. Br J Cancer. 2003. doi:10.1038/sj.bjc.6601073
37. Singh-Grewal D. Multidisciplinary paediatric rheumatology services in Australia and New Zealand. Med J Aust. 2017;206(2):97–97.e1. doi:10.5694/MJA16.00710
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.