Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
A Nomogram Predicting the Risk of Anxiety in Third-Trimester pregnancy in Pregnant Women with CTDs
Authors Xu S, Zhong X, Cai X, Wu J, Wang H, Ni S, Yang M ![]() , Dong C
, Dong C ![]() , Gu Z
, Gu Z
Received 8 August 2025
Accepted for publication 24 January 2026
Published 13 February 2026 Volume 2026:19 559273
DOI https://doi.org/10.2147/JMDH.S559273
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Krzysztof Laudanski
Shu Xu,1,* Xiuli Zhong,1,* Xingfeng Cai,1,* Jiawen Wu,2 Hanxiao Wang,2 Shiwen Ni,2 Mei Yang,2 Chen Dong,2 Zhifeng Gu3
1School of Nursing and Rehabilitation, Nantong University, Nantong, Jiangsu, People’s Republic of China; 2Research Center of Clinical Medicine, Affiliated Hospital of Nantong University, Nantong, Jiangsu, People’s Republic of China; 3Department of Rheumatology and Immunology, Affiliated Hospital of Nantong University, Nantong, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chen Dong, Research Center of Clinical Medicine, Research Center of Nursing, Research Center of Clinical Immunology, Affiliated Hospital of Nantong University, Nantong, Jiangsu, People’s Republic of China, Email [email protected] Zhifeng Gu, Department of Rheumatology, Research Center of Clinical Medicine, Research Center of Nursing, Research Center of Clinical Immunology, Affiliated Hospital of Nantong University, Nantong, Jiangsu, People’s Republic of China, Tel +86-13706291941, Email [email protected]
Purpose: Connective tissue diseases (CTDs) is a group of autoimmune diseases that damage multiple systems and can cause anxiety in pregnant women. The aim of this study was to identify risk factors of anxiety during third-trimester pregnancy among CTDs patients and to develop a predictive model to improve clinical outcomes.
Patients and Methods: A total of 226 pregnant women with CTDs and 226 normal pregnant women were enrolled in this study during third-trimester pregnancy. This study analyzed risk factors for late pregnancy anxiety in pregnant women with CTDs using binary logistic regression. The probability of anxiety occurrence is predicted by nomogram and further validated by decision curve analysis (DCA), receiver operating characteristic curve (ROC), calibration curve.
Results: Anxiety levels were found to be significantly higher in pregnant women with CTDs compared to the control group (4.64± 2.92 VS 3.97± 2.44, P = 0.008). These results suggest that anxiety plays a critical role during the third trimester of pregnancy in this particular population. A total of 33 pregnant women with CTDs (14.6%) reported anxiety in third-trimester pregnancy. Risk factors associated with anxiety in third-trimester pregnancy include sleep disturbances (OR=4.226, 95CI% = 1.508– 11.843), pregnancy stress (OR=1.121, 95CI% = 1.069– 1.175) and family dysfunction (OR = 4.710, 95CI% =1.004– 22.184).
Conclusion: The nomogram has clinical utility and robustly predicts the associated anxiety model. During third-trimester pregnancy, sleep disturbances, pregnancy stress, and family dysfunction increase the risk of anxiety in pregnant women with CTDs, which can result in an increased likelihood of emergency cesarean sections and more postpartum blood loss at 2 hours.
Keywords: connective tissue diseases, adverse postnatal outcomes, anxiety, nomogram
Introduction
Connective tissue diseases (CTDs) are autoimmune diseases characterized by non-specific inflammation, including lupus, rheumatoid arthritis (RA), Sjogren’s syndrome (PSS), and antiphospholipid syndrome (APS), which tend to occur in women, especially during their childbearing age.1 CTDs increases the risk of adverse pregnancy outcomes (APOs) such as pre-eclampsia, thrombosis with fetal miscarriage and preterm delivery in pregnant women.2,3 A controlled study from Portugal showed that the PSS group had a higher rate of miscarriage and congenital heart block in newborns compared to healthy controls.4 The experience of previous APOs, prolonged medication during pregnancy, and concerns about the health of the fetal can all lead to anxiety in pregnant women with CTDs.5
Anxiety is among the most prevalent psychological challenges faced by expectant mothers. While postnatal mental health has been extensively documented, anxiety specifically during the third trimester remains an area that warrants more targeted investigation.5–9 A study from China showed that the prevalence of anxiety in third-trimester pregnancy in normal pregnant women is about 29%.10 In contrast, there are no studies focusing on anxiety in pregnant women with CTDs, who are at high risk of pregnancy complications. Previous studies have shown that due to disease mechanisms, CTDs are risk factors for anxiety. When the blood-brain barrier is disrupted in lupus, autoantibodies associated with the disease cross the blood-brain barrier and attack the hippocampus, causing neuronal death and triggering mental disorders such as anxiety.11 A review from Australia suggests that rheumatoid arthritis, through mechanisms such as inflammatory imbalances, pain, and fatigue, may increase the risk of anxiety, indicating a strong association and possible co-morbidity between the two conditions.12 In the third trimester of pregnancy, even though pregnant women with CTDs are ready to become mothers, concerns about APOs continue to pose a significant concern, thereby increasing their risk of third-trimester pregnancy anxiety. Pregnancy is more challenging for women with CTDs. Beyond regular rheumatological medication, they often experience a hypercoagulable state (clinically indicated by elevated D-dimer levels) and coagulation disorders. The necessity of long-term low-molecular-weight heparin injections to manage these thrombotic risks acts as a significant psychological stressor, heightening their anxiety regarding maternal and fetal safety during third trimester.13
Pregnant women with CTDs represent a distinct clinical population. However, there are no reports specifically focusing on third-trimester pregnancy anxiety in this group, as prior research has predominantly centered on their fertility intentions.14,15 Therefore, the aim of this study was to explore the risk factors for anxiety in third-trimester pregnancy in pregnant women with CTDs and to perform the initial construction and validation of a nomogram model. The nomogram can visualize the numbers and quickly help rheumatology and obstetrics and gynaecology healthcare professionals to screen for people at high risk of anxiety and improve the efficiency of multidisciplinary management of pregnancies in CTDs.
Methods
Participants
This study examined 26 variables that were potentially associated with anxiety. According to statistical requirements, the sample size should be five to ten times the number of variables in the study. Taking a potential dropout rate of 10% into account, the final sample size was determined to be between 143 and 286. Between October 1, 2023, and February 15, 2025, a total of 470 participants were recruited at the Affiliated Hospital of Nantong University, including 244 patients in the CTDs group and 226 healthy controls. In the CTDs group, 18 participants were excluded due to withdrawal of consent, leaving 226 cases for final analysis. All 226 questionnaires from the healthy control group were valid. Maternal and fetal outcomes were successfully tracked for all included participants.
This study has been approved by the Ethics Committee of Nantong University Affiliated Hospital (NO.2024-K204-01). All pregnant women were informed of the specific details of the study and signed informed consent forms prior to completing the questionnaire. Our research complies with the Declaration of Helsinki.
Inclusion Criteria
- Age ≥ 18 years and all participants reported no history of clinically diagnosed psychiatric disorders. (2) Clear articulation and the ability to fluently answer midwives’ questions or independently complete questionnaires in Chinese. (3) Women who were pregnant and had reached 28 weeks of gestation or more were selected for this study. They were chosen to take part in the research and sign informed consent forms. (4) Multidisciplinary pregnancy management was used and the diagnosis of CTDs was confirmed by a rheumatologist based on the test results according to clinical guidelines. (5) Healthy pregnant women must have no history of any other diseases.
Exclusion Criteria
- Pregnant women under the age of 18. (2) Individuals who did not participate, those who dropped out midway, and those who failed to communicate effectively or did not complete the questionnaire correctly. (3) Prenatal ultrasound, amniocentesis, and non-invasive DNA testing can detect abnormalities in pregnant women. (4) The history of mental disorders such as schizophrenia and bipolar disorder. (5) Pregnant women in the control group with a history of other diseases.
Collection of Clinical Data
The week of gestation was determined by the obstetrician, according to the time of the last menstrual period in case of accurate menstruation, and according to the B-mode Ultrasound in case of irregular menstruation. If the number of days of gestation suggested by early pregnancy ultrasound differs by more than five days from the last menstrual period, the tendency is to calculate the week of gestation based on the ultrasound findings. After obtaining consent from the mother and her family, a dedicated obstetric nurse and pediatric nurse are responsible for collecting maternal-fetal outcomes based on the medical record management system.
Definition and standard preterm birth are defined as delivery at 28 to less than 37 weeks of gestation (196 to 258 days). Premature rupture of membranes referred to the spontaneous rupture of membranes prior to the onset of labor. Birth weight categories were defined as extremely low birth weight (<1000g), very low birth weight (<1500g), low birth weight (<2500g), normal birth weight (2500–4000g), and macrosomia (≥4000g).
The Apgar score assessed neonatal status via five signs: heart rate, respiratory effort, muscle tone, reflex irritability, and skin color, with each scored from 0 to 2. Neonatal asphyxia was diagnosed by a 1- or 5-minute Apgar score ≤7, failure to establish effective breathing, and an umbilical artery pH <7.15, following the exclusion of other causes. Induction of labor was defined as the pharmacological or mechanical initiation of labor prior to spontaneous onset for vaginal delivery.
Questionnaire Scale
Socio-Demographic Data
A self-designed, self-administered questionnaire was utilized to collect baseline sociodemographic data. The collected variables included age, height and weight, place of residence, educational level, medical insurance, occupation, per capita income, family structure, family relationships, and sleep status over the previous month.
Hospital Anxiety and Depression Scale, HADS
HADS has been used to evaluate anxiety and depression in clinical studies of rheumatic immune diseases such as systemic lupus erythematosus. The scale has a total of 14 items, including two sub-scales of HADS-anxiety and HADS-depression, with 7 items, respectively. Respondents chose the option that best matched their feelings based on their mood in the previous month. The score range of each item is 0–3 points, and the score of the sub-scale is calculated separately. A score >7 points means that the patient has anxiety/depression, and the higher the score, the more serious the patient’s condition.16 A Cronbach’s alpha of 0.853 was obtained for this scale within our sample, indicating a high level of reliability.
Family APGAR Index, APGAR
It was first proposed by Smilksteinin in 1978 and has good reliability and validity.17 The scale includes 5 dimensions including family fitness, cooperation, growth, emotion and affinity density. One dimension corresponds to one item. The score range of one item is 0–2 points, and the total score is 0–10 points. If the total score is less than 7, it indicates a possible family dysfunction.18,19 The Cronbach’s alpha for the scale in this study was 0.897.
Pregnancy Stress Rating Scale, PSRS
The PSRS is a scale developed by Chinese scholars in 1983 to assess stress during pregnancy. The scale has a total of 30 items. Each item is scored on a scale of 0–3, with a total score range of 0–90, with higher scores representing more severe pregnancy stress in pregnant women.20,21 In our study, the scale had a Cronbach’s alpha of 0.935.
Data Analysis
All statistical analyses were performed using SPSS (Version 27.0) and RStudio (Version 2024). Continuous variables are expressed as median±standard deviation (M±SD), while categorical variables are presented as percentages (%). During univariate analyses, independent samples t-tests were used for continuous variables, and chi-square tests or Fisher’s exact tests were used for categorical variables. Variables with P<0.05 were further included in multivariate analyses to identify independent risk factors for late anxiety in CTDs by binary logistic regression, and nomogram models were built based on the regression results. We mainly applied “rms”, “pROC”, and “rmda” from the R package for nomogram construction and validation, “ggplot2” package was used for plotting. To evaluate the performance of the nomogram model, this study applied the following methods: (1) Discriminative ability assessment: The area under the receiver operating characteristic curve (AUC) and concordance index (C-index) were used to quantify the model’s predictive discrimination for the target event. (2) Calibration verification: Calibration curves were employed to visualize the consistency between predicted probabilities and observed outcomes, complemented by statistical validation via the Hosmer-Lemeshow test. (3) Clinical utility analysis: Decision curve analysis (DCA) was conducted to calculate individual net benefits across different threshold probabilities, evaluating the practical value of the predictive model in clinical decision-making.
Results
A total of 226 pregnant women with CTDs and 226 common pregnant women participated in this study. As illustrated in Figure 1, pregnant women with CTDs exhibit significantly elevated anxiety levels during third-trimester pregnancy, surpassing those of the health control group. Figure 2A and B display postpartum blood loss distributions using bar charts, showing significantly higher abnormal values in the connective tissue disease group versus health control. The remaining comparisons of maternal and fetal outcomes are detailed in Table S1.
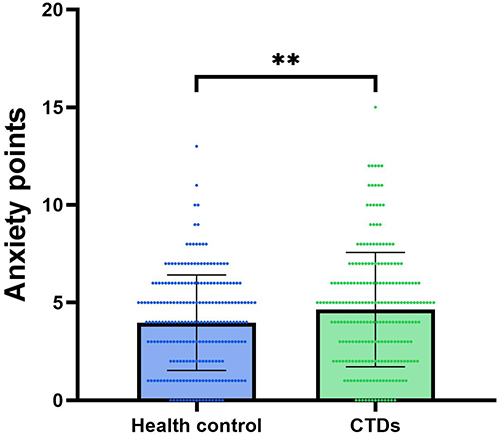 |
Figure 1 The bar chart shows that the difference in total Hads-anxiety scores between pregnant women with CTDs in late-term pregnancy and healthy controls was significant (P<0.01), with a more severe anxiety status. ** P < 0.05. |
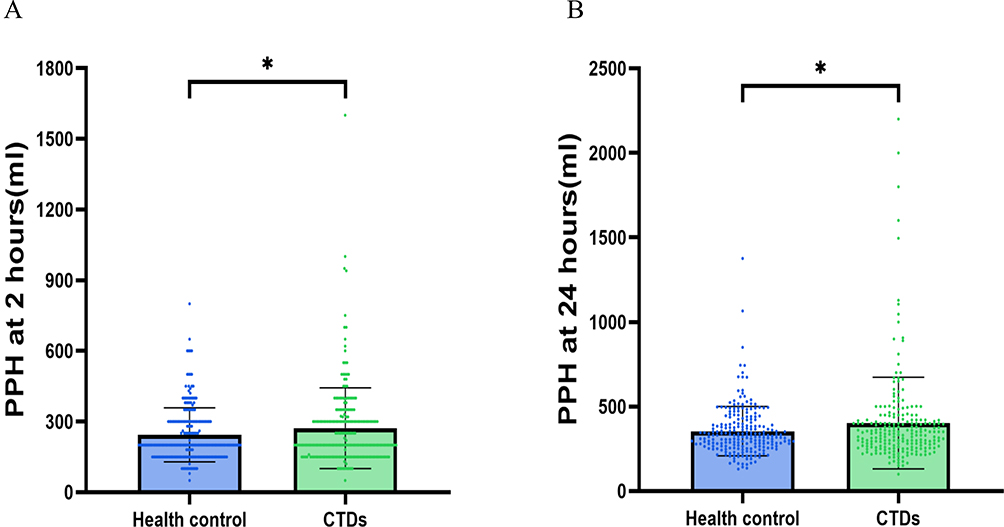 |
Figure 2 (A) and (B) The bar chart results showed abnormal values of postpartum blood loss in pregnant women with CTDs compared to normal mothers, indicating that CTDs mothers are at risk of adverse pregnancy outcomes (APOs). * P < 0.05. |
As shown in Table 1, the results of the univariate analysis revealed that a higher proportion of anxious pregnant women with CTDs had a non-nuclear family structure (living with the couple’s parents) (72.7% VS 50.3%, P = 0.017) and poor relationships with family members (27.3% VS 6.2%, P < 0.001) than non-anxious pregnant women with CTDs. Pregnancy stress scores were higher for anxious pregnant women with CTDs (23.73±13.34 VS 10.35±7.70, P < 0.001) and a higher percentage of them had sleep disturbances (93.9% VS 67.4%, P = 0.002). As shown in Table 2, the variables that were statistically significant (P < 0.05) in the univariate analysis were included in the logistic regression analysis. This analysis identified sleep disturbances (β = 1.552, 95% CI = 1.004–22.184, P = 0.049), pregnancy stress (β = 0.114, 95% CI = 1.069–1.175, P < 0.001), and family dysfunction (β = 1.441, 95% CI = 1.508–11.843, P = 0.006) as independent risk factors for third trimester pregnancy anxiety in pregnant women with CTDs.
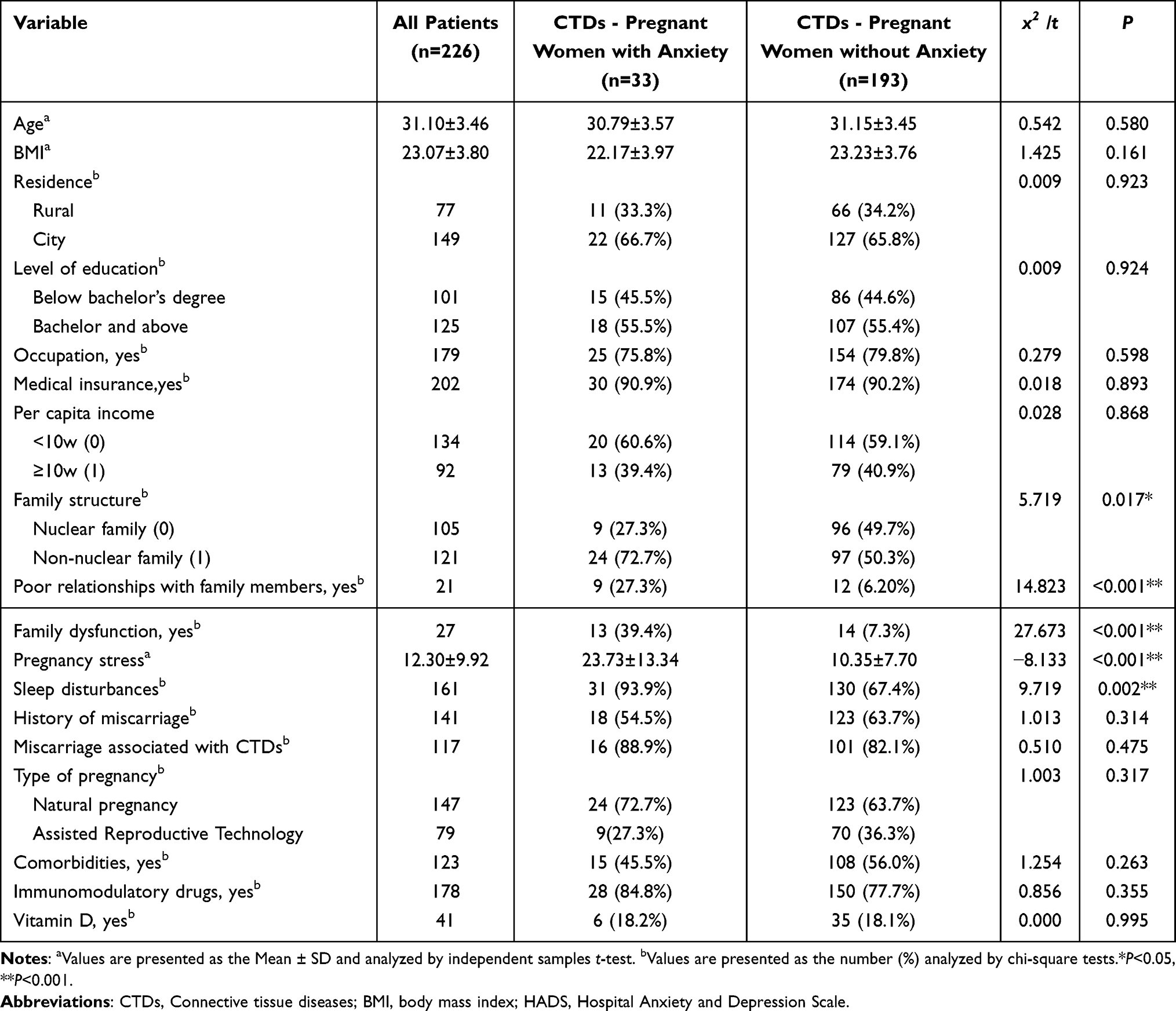 |
Table 1 Baseline Characteristics of All Pregnant Women with CTDs in Third Trimester Pregnancy |
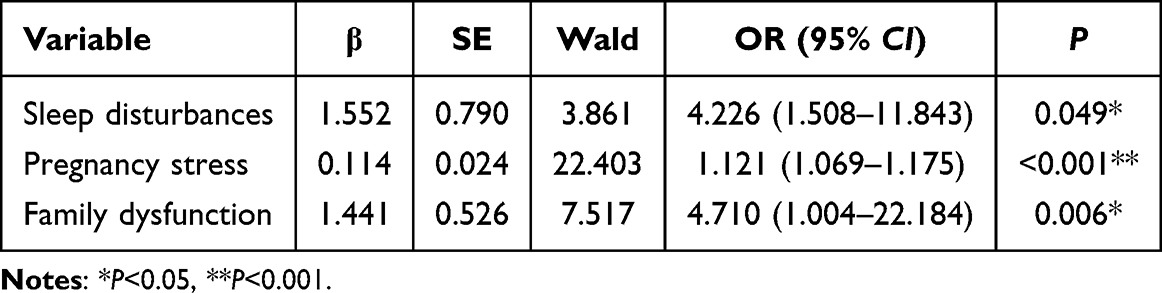 |
Table 2 Multivariate Analysis of Independent Risk Factors for Late-Term Pregnancy Anxiety in CTDs |
Three independent risk factors, pregnancy stress, sleep disturbances and family dysfunction, were used to enter the nomogram model for anxiety prediction (Figure 3). The C-index of the nomogram was 0.854 (95% CI = 0.825–0.883), and the Hosmer–Lemeshow good of fit test chi-square value was 4.85, with a P-value of 0. 77. The predictive model was calibrated by Bootstrap (n=1000) and the predicted probabilities were highly consistent with the actual predictions, well calibrated and can be used for clinical risk prediction (Figure 4). The discrimination of the nomogram model was assessed by the ROC curve, and the AUC of the nomogram model was 0.866 (95% CI = 0.801–0.932), with a specificity and sensitivity of 75.6% and 84.4%, respectively, and an optimal cut-off value of 0.112 (Figure 5). The prediction curve in the DCA was above the “None” line and the “All” line when the risk threshold was between 0% and 69%, demonstrating the clinical practicability of the model (Figure 6).
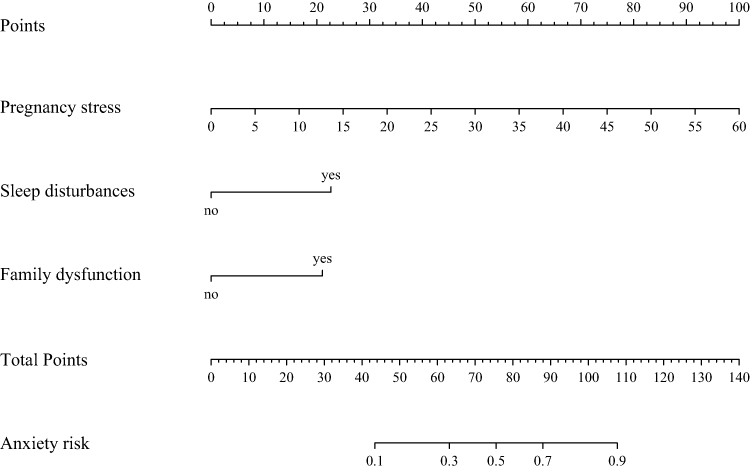 |
Figure 3 The nomogram predicts the risk of anxiety during the late-term pregnancy in pregnant women with CTDs. The value of each variable has a score on the point scale axis, and the total anxiety score is calculated by adding up these scores. This total is then projected onto the lower point scale axis to estimate the probability of experiencing anxiety during late-term pregnancy in pregnant women with CTDs. |
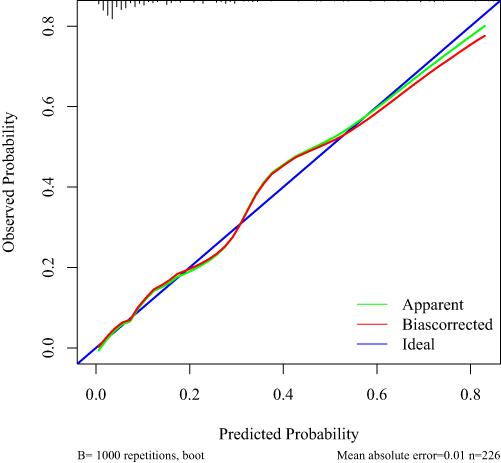 |
Figure 4 The x-axis represents the probability predicted by the line chart, and the y-axis represents the actual probability of CTDs in pregnant women experiencing anxiety in the late-term pregnancy. The ideal, perfect prediction corresponds to the 45-degree blue solid line. The green solid line represents the entire cohort (n = 226), and the red solid line shows the actual predictive performance of the line chart after bias correction using bootstrap (B = 1000 repetitions). |
 |
Figure 5 The nomogram model’s ability to discriminate was evaluated using the receiver operating characteristic (ROC) curve. The area under the curve (AUC) for the nomogram model was found to be 0.866 (95% CI = 0.801–0.932). The respective specificity and sensitivity were 75.6% and 84.4%, and the optimal cut-off value was 0.112. |
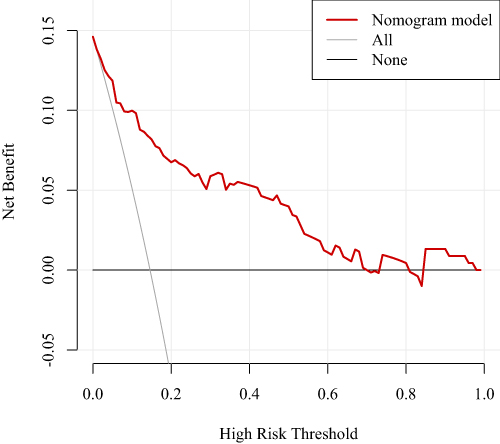 |
Figure 6 The decision curve analysis (DCA) was used to assess the clinical utility of the model. The results show that the predictive power of the model exceeds the extremes of the “ALL” and “None” curves. This result indicates that the model has good clinical predictive ability. |
As shown in Table 3, patients in the anxiety group exhibited a significantly higher incidence of emergency caesarean sections (35.7% VS 10.3%, P = 0.011) and increased postpartum blood loss at 2 hours (366.76±297.35 VS 255.57±133.57, P = 0.042). However, this difference in blood loss was not statistically significant at 24 hours. Regarding other maternal and neonatal parameters—such as gestational age, overall mode of delivery, duration of labour, birth weight, and Apgar scores—no significant differences were observed between the two groups.
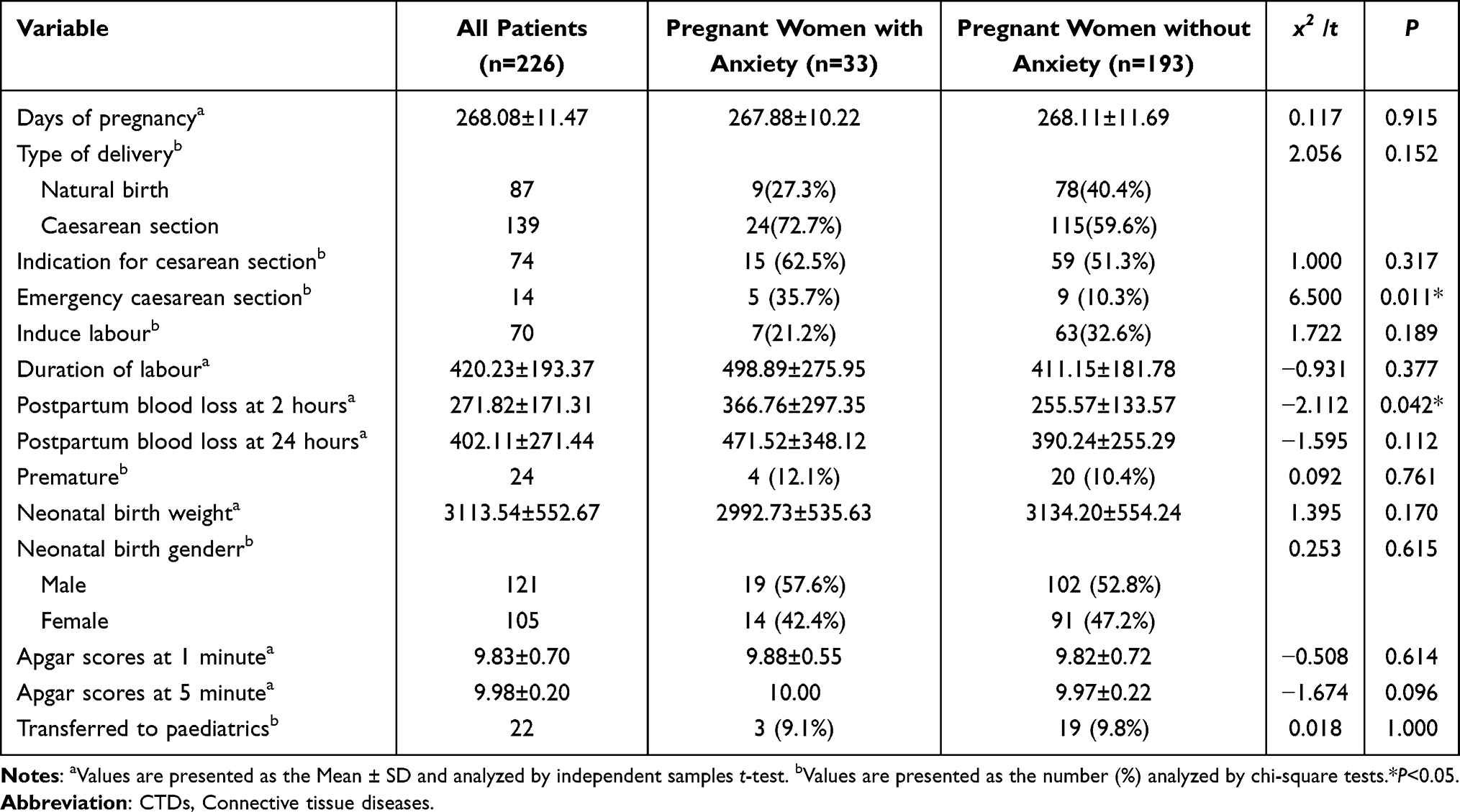 |
Table 3 Maternal and Fetal Outcomes in CTDs Patients with and without Anxiety |
Discussion
Anxiety was high in third-trimester pregnancy in pregnant women with CTDs, contributing to a higher incidence of emergency cesarean sections and an increase in postpartum blood loss at 2 hours compared with non-anxious pregnant women with CTDs. Our study suggests that in third-trimester pregnancy, anxiety in pregnant women with CTDs may be associated with pregnancy stress, sleep disturbances, and family dysfunction. We further constructed a nomogram model based on this risk factor, and our results suggest that the model can be used to assist in individualized assessment and decision-making regarding the risk of anxiety in third-trimester pregnancy in pregnant women with CTDs.
In the third trimester, the prevalence and severity of sleep disorders—such as habitual snoring and restless leg syndrome—often peak.22 These disturbances are not merely symptomatic but serve as a critical physiological trigger; specifically, sleep deprivation activates the hypothalamic-pituitary-adrenal (HPA) axis, which precipitates maternal anxiety and, crucially, induces systemic hypertension.23 This sleep-driven hypertensive state functions as a secondary vascular insult in the context of CTDs. While autoantibodies in CTDs patients directly compromise the placental endothelium, the added hemodynamic stress from poor sleep exacerbates intravascular thrombosis and hypoperfusion. Consequently, sleep-induced hypertension acts as a catalyst that amplifies the baseline risk of eclampsia in CTDs pregnancies.24 Therefore, interventions targeting sleep quality are vital not only for psychological relief but as a strategic approach to stabilize blood pressure and protect placental integrity, ultimately mitigating adverse eclamptic outcomes.
In pregnant women with CTDs, our findings demonstrated that pregnancy stress exerts a profound influence on third-trimester anxiety (P < 0.001), acting as its primary independent driver. While women with CTDs often harbor a strong desire for children, the inherent complexities and risks associated with their condition make the course of pregnancy exceptionally challenging.15,25 This stress, which accumulates from the pre-conception phase through the third trimester, is compounded by persistent apprehension regarding fetal safety, eventually precipitating into clinical anxiety. This state of anxiety, as a direct consequence of prolonged stress, has far-reaching implications for neonatal health, including the potential impairment of motor and language development.26 A study conducted in Shanghai further illustrates this trajectory, demonstrating that the psychological burden of the third trimester carries tangible risks for the offspring, specifically increasing allergic susceptibility in early childhood.27 Thus, the anxiety induced by sustained pregnancy stress represents a critical threat to offspring health, with the potential for long-term neurodevelopmental and psychiatric consequences.28
Our study identified family factors as playing a crucial role in third-trimester pregnancy anxiety among pregnant women with CTDs. Non-nuclear family structure, poor family relationships, and family dysfunction were found to be associated with anxiety (P < 0.05). Notably, family dysfunction was an independent risk factor for third-trimester pregnancy anxiety in women with CTDs (P < 0.001). A study of disabled people in China suggests that relationships with family members are key to good family functioning.29 Family functioning can be promoted through positive relationships with family members, which can alleviate negative emotions such as anxiety. Family dysfunction was found to be strongly associated with anxiety in pregnant women with CTDs in our study. This result is consistent with a study of normal pregnant women in China.30 Patients are particularly sensitive to family functioning support. When family functioning is suboptimal, patients may perceive a lack of care from family members, leading them to face pregnancy-related challenges alone. As individuals with chronic diseases, pregnant women with CTDs typically require more familial care than healthy pregnant women.31 In the absence of adequate family support and amid persistent family dysfunction, these women may develop prolonged anxiety. During the third-trimester pregnancy, negative emotions peak or continue to rise, further affecting the development of the infant’s amygdala.32
Family structure greatly influences late pregnancy anxiety in this population. The results suggest that pregnant women who live in non-nuclear families are more likely to be anxious. Traditional Chinese culture is influenced by Confucianism, and the culture of filial piety affects both parents and children.33 However, when these children become mothers themselves and develop their own perspectives on pregnancy health, they are still often expected to defer to their parents’ opinions.34 Due to the unique nature of disease-complicated pregnancy, pregnant women with CTDs may not always receive pregnancy-related advice from their parents. This disparity can trigger family conflicts, strain interpersonal relationships, disrupt family functioning, diminish social support, and exacerbate anxiety in these women. We recommend that pregnant women with CTDs be provided with the option to choose a family environment that makes them feel comfortable. This approach can help enhance family functioning, improve social support, and alleviate their anxiety.
Pregnant women with CTDs, especially those with lupus and APS, have an increased risk of postpartum blood loss during labor due to coagulation disorders, which is consistent with our study.35 We found that anxious pregnant women with CTDs had more postpartum blood loss at 2 hours compared to pregnant women with CTDs without anxiety (366.76±297.35 VS 255.57±133.57, P = 0.042). Excessive postpartum blood loss increases the likelihood of maternal anaemia.36 Anaemia can further stimulate the immune system of pregnant women with CTDs, this can be fatal to a weakened woman in labor.37 It was found by our study that emergency caesarean delivery was more likely to be faced by anxious pregnant women with CTDs (35.7% VS 10.3%, P = 0.011), which has rarely been reported before. Globally, the incidence of emergency caesarean sections has exceeded 20%.38 While this saves the lives of women in labor, it also causes them both physical and psychological harm, especially psychological disorders.39 A qualitative study from Ghana suggests that emergency caesarean sections can cause maternal anxiety and depression, affecting daily life and socialization after birth and undermining the happiness of being a mother.40 Anxiety increases the likelihood of emergency caesarean section, and emergency caesarean section can further exacerbate maternal anxiety. In pregnant women with CTDs, anxiety negatively impacts pregnancy outcomes. Therefore, rheumatology and obstetrics departments should collaborate on pregnancy monitoring, especially regarding psychological care in third-trimester pregnancy.41
The nomogram, based on our study results, helps clinicians quickly predict the risk of anxiety in third trimester for CTDs patients. During prenatal visits, doctors can use this nomogram chart to assess the patient. They check the specific risk factors included in the model. The points for each factor are added up to get a total score. Finally, the overall probability of anxiety is determined by this total score. This tool is simple and convenient, which improves clinical efficiency. It helps doctors identify high-risk patients early and provide timely intervention.
Conclusion
Generally, third trimester pregnant women with CTDs show higher anxiety than healthy women, which is harmful to pregnancy outcomes. We found that sleep disturbances, pregnancy stress, and family dysfunction are key factors affecting this anxiety. Given these findings, we recommend forming a multidisciplinary team. This team should try to assess sleep quality, pregnancy stress and family dysfunction. Suggestions for care include helping the woman keep a regular sleep schedule, relieving stress (for example, with music), and asking family members to help with care. For severe cases, consulting a psychologist might be helpful. This study presents the first nomogram for predicting anxiety in CTDs patients during third-trimester pregnancy, aiding clinical assessment through visualized risk. This study has some limitations. First, because of its cross-sectional design, we cannot confirm cause-and-effect relationships. The links we found between maternal anxiety and pregnancy outcomes show association but do not prove that anxiety directly leads to these outcomes. Second, this was a single-center study, which may limit how well our results apply to other groups of patients. Finally, the lack of long-term follow-up means we could not track the health of mothers and fetal over time. Future multicenter longitudinal studies are needed to investigate psychological factors in such special populations throughout the pregnancy continuum.
Acknowledgment
We sincerely thank all the pregnant women who participated in this study.
Consent for Publication
All authors have approved the manuscript and agree with this submission.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (82502178, 82402102), China Postdoctoral Science Foundation (2024M751535), Jiangsu Funding Program for Excellent Postdoctoral Talent, Postgraduate Research & Practice Innovation Program of Jiangsu Province (KYCX24_3592), Jiangsu Provincial Medical Key Discipline Cultivation Unit (JSDW202205), Jiangsu Provincial Research Hospital (YJXYY202204), Natural Science Foundation of Jiangsu Province (BK20241838, BK20251836), Science and technology Project of Nantong City (XNBH00031655), Science Foundation of Nantong Municipality (JC2024029), and Special Research Project of Nantong Municipal Health Commission (QNZ2025002).
Disclosure
The authors have declared no competing interests in this work.
References
1. Joy GM, Arbiv OA, Wong CK, et al. Prevalence, imaging patterns and risk factors of interstitial lung disease in connective tissue disease: a systematic review and meta-analysis. Eur Respir Rev. 2023;32(167):220210. doi:10.1183/16000617.0210-2022
2. Zhang S, Han X, Liu W, Wen Q, Wang J. Pregnancy in patients with systemic lupus erythematosus: a systematic review. Arch Gynecol Obstet. 2023;308(1):63–12. doi:10.1007/s00404-022-06718-7
3. Tarter L, Bermas BL. Expert perspective on a clinical challenge: lupus and pregnancy. Arthritis Rheumatol. 2023.
4. Barros T, Braga J, Abreu MI, et al. Sjögren’s syndrome and pregnancy: a Portuguese case-control study. Reumatologia. 2022;60(5):311–317. doi:10.5114/reum.2022.120754
5. Grigoriadis S, Graves L, Peer M, et al. Maternal anxiety during pregnancy and the association with adverse perinatal outcomes: systematic review and meta-analysis. J Clin Psychiatry. 2018;79(5). doi:10.4088/JCP.17r12011.
6. van der Zee-van den Berg AI, Boere-Boonekamp MM, Groothuis-Oudshoorn CGM, Reijneveld CGM, van der Zee-van den Berg AI. Postpartum depression and anxiety: a community-based study on risk factors before, during and after pregnancy. J Affect Disord. 2021;286:158–165. doi:10.1016/j.jad.2021.02.062
7. Hadfield K, Akyirem S, Sartori L, et al. Measurement of pregnancy-related anxiety worldwide: a systematic review. BMC Pregnancy Childbirth. 2022;22(1):331. doi:10.1186/s12884-022-04661-8
8. Nisar A, Xiang H, Perin J, et al. Impact of an intervention for perinatal anxiety on breastfeeding: findings from the happy mother-healthy baby randomized controlled trial in Pakistan. Int Breastfeed J. 2024;19(1):53. doi:10.1186/s13006-024-00655-8
9. Ding W XX, Xu YL, Zhu SJ, et al. Maternal anxiety during pregnancy and adverse birth outcomes: a systematic review and meta-analysis of prospective cohort studies. J Affect Disord. 2014;159:103–110. doi:10.1016/j.jad.2014.02.027
10. Zhou C, Weng J, Tan F, et al. Pregnancy-related anxiety among Chinese pregnant women in mid-late pregnancy under the two-child policy and its significant correlates. J Affect Disord. 2020;276:272–278. doi:10.1016/j.jad.2020.07.099
11. Han X, Xu T, Ding C, et al. Neuronal NR4A1 deficiency drives complement-coordinated synaptic stripping by microglia in a mouse model of lupus. Signal Transduct Target Ther. 2022;7(1):50. doi:10.1038/s41392-021-00867-y
12. Meade T, Joyce C, Perich T, Manolios N, Conaghan PG, Katz P. Prevalence, severity, and measures of anxiety in rheumatoid arthritis: a systematic review. Arthritis Care Res. 2023.
13. Ambati A, Knight JS, Zuo Y. Antiphospholipid syndrome management: a 2023 update and practical algorithm-based approach. Curr Opin Rheumatol. 2023;35(3):149–160. doi:10.1097/BOR.0000000000000932
14. Wang X, Li J, Liang Q, et al. Reproductive concerns and contributing factors in women of childbearing age with systemic lupus erythematosus. Clin Rheumatol. 2022;41(8):2383–2391. doi:10.1007/s10067-022-06156-5
15. Liang Q, Wang X, He Q, et al. Factors associated with fertility intention among women with systemic lupus erythematosus in China: a cross-sectional study. Int J Rheum Dis. 2023;26(12):2419–2429. doi:10.1111/1756-185X.14927
16. Annunziata MA, Muzzatti B, Bidoli E, et al. Hospital anxiety and depression scale (hads) accuracy in cancer patients. Support Care Cancer. 2020;28(8):3921–3926. doi:10.1007/s00520-019-05244-8
17. Smilkstein G. The family APGAR: a proposal for a family function test and its use by physicians. J Fam Pract. 1978;6(6):1231–1239.
18. Shao R, He P, Ling B, et al. Prevalence of depression and anxiety and correlations between depression, anxiety, family functioning, social support and coping styles among Chinese medical students. BMC Psychol. 2020;8(1):38. doi:10.1186/s40359-020-00402-8
19. Karimi Z, Taheri-Kharameh Z, Sharififard F. Cultural adaption and psychometric analysis of family APGAR scale in iranian older people. Korean J Fam Med. 2022;43(2):141–146. doi:10.4082/kjfm.21.0028
20. Ma D, Sun S, Qian J, et al. Predictors of pregnancy stress and psychological birth trauma in women undergoing vaginal delivery: a cross-sectional study in China. BMC Pregnancy Childbirth. 2023;23(1):596. doi:10.1186/s12884-023-05890-1
21. Ayraler A, Ş A T, Özkök S. Pregnancy school education program in mother friendly training and research hospital impact on stress and anxiety. Rev Assoc Med Bras. 2023;69(8):e20230279. doi:10.1590/1806-9282.20230279
22. de Mola C L, Carpena MX, Dias IM, Meucci R, Goicochea-Romero A, Cesar J. Sleep and its association with depressive and anxiety symptoms during the last weeks of pregnancy: a population-based study. Sleep Health. 2023;9(4):482–488. doi:10.1016/j.sleh.2023.05.003
23. Miller HE, Simpson SL, Hurtado J, et al. Associations between anxiety, sleep, and blood pressure parameters in pregnancy: a prospective pilot cohort study. BMC Pregnancy Childbirth. 2024;24(1):366. doi:10.1186/s12884-024-06540-w
24. Petri M. Antiphospholipid syndrome. Transl Res. 2020;225:70–81. doi:10.1016/j.trsl.2020.04.006
25. Tani C, Zucchi D, Bellis E, et al. Patient care pathways for pregnancy in rare and complex rheumatic diseases: results from an international survey. J Rheumatol. 2023;50(7):934–938. doi:10.3899/jrheum.220773
26. Rogers A, Obst S, Teague SJ, et al. Association between maternal perinatal depression and anxiety and child and adolescent development: a meta-analysis. JAMA Pediatr. 2020;174(11):1082–1092. doi:10.1001/jamapediatrics.2020.2910
27. Shi YY, Wei Q, Ma X, Zhang Y, Wang L, Shi HJ. Maternal affective and stress-related factors during pregnancy affect the occurrence of childhood allergic diseases: a Shanghai MCPC study. J Psychosom Res. 2023;165:111142. doi:10.1016/j.jpsychores.2022.111142
28. Ståhlberg T, Khanal P, Chudal R, Luntamo T, Kronström K, Sourander A. Prenatal and perinatal risk factors for anxiety disorders among children and adolescents: a systematic review. J Affect Disord. 2020;277:85–93. doi:10.1016/j.jad.2020.08.004
29. Wang B, Yuan D, Zhong X, Yang F, Fu H. Family function, anxiety and depression in adults with disabilities: a network analysis. Front Public Health. 2023;11:1181203. doi:10.3389/fpubh.2023.1181203
30. Huang J, Xu L, Xu Z, et al. The relationship among pregnancy-related anxiety, perceived social support, family function and resilience in Chinese pregnant women: a structural equation modeling analysis. BMC Womens Health. 2022;22(1):546. doi:10.1186/s12905-022-02145-7
31. Mestre TD, Caldeira EV, Lopes MJ. Family self-care in chronic disease management: an evolving care pattern? SAGE Open Nurs. 2024;10:23779608231226069. doi:10.1177/23779608231226069
32. Marr MC, Graham AM, Feczko E, et al. Maternal perinatal stress trajectories and negative affect and amygdala development in offspring. Am J Psychiatry. 2023;180(10):766–777. doi:10.1176/appi.ajp.21111176
33. Shen C, Wang DN, Gao Z XX, Dong R, Gu C, Gao ZF. A study on the impact of the number of family generations on intergenerational support for centenarians: a study in a Chinese ‘longevity city’. Psychogeriatrics. 2023;23(6):908–917. doi:10.1111/psyg.13009
34. Peng S, Lai X, Qiu J, et al. Living with parents-in-law increased the risk of postpartum depression in Chinese women. Front Psychiatry. 2021;12:736306. doi:10.3389/fpsyt.2021.736306
35. Fang QY, Gan DH, Huang J, Lian F. Pregnancy outcomes and risk factors for thrombocytopenia in pregnant patients with systemic lupus erythematosus. BMC Pregnancy Childbirth. 2025;25(1):344. doi:10.1186/s12884-025-07451-0
36. Mansukhani R, Shakur-Still H, Chaudhri R. Maternal anaemia and the risk of postpartum haemorrhage: a cohort analysis of data from the WOMAN-2 trial. Lancet Glob Health. 2023;11(8):e1249–e1259. doi:10.1016/S2214-109X(23)00245-0
37. Canny SP, Orozco SL, Thulin NK, Hamerman JA. Immune Mechanisms in Inflammatory Anemia. Annu Rev Immunol. 2023;41:405–429. doi:10.1146/annurev-immunol-101320-125839
38. Pope JE. Management of fatigue in rheumatoid arthritis. RMD Open. 2020;6(1):e001084. doi:10.1136/rmdopen-2019-001084
39. Orovou E, Antoniou E, Zervas I, Sarantaki A. Prevalence and correlates of postpartum PTSD following emergency cesarean sections: implications for perinatal mental health care: a systematic review and meta-analysis. BMC Psychol. 2025;13(1):26. doi:10.1186/s40359-025-02344-5
40. Saansong AOA, Adoma PO, Nkrumah J, Gbagbo FY. Experience and perceived impact of anxiety and depression on quality of life following emergency caesarean section among women in Ghana: a qualitative study. BMJ Open. 2024;14(11):e086069. doi:10.1136/bmjopen-2024-086069
41. Huang W, Wu T, Jin T, et al. Maternal and fetal outcomes in pregnant women with rheumatoid arthritis: a systematic review and meta-analysis. Clin Rheumatol. 2023;42(3):855–870. doi:10.1007/s10067-022-06436-0
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Nomogram-Based Study: A Way Forward to Predict the Anxiety Status in Medical Staff During the COVID-19 Pandemic
Liu Z, Khan NH, Wang L, Zhang CY, Ji XY
Journal of Multidisciplinary Healthcare 2022, 15:2725-2733
Published Date: 30 November 2022
A Nomogram Predicting Decreased Quality of Life in Patients with Keloids
Xu S, Huang Y, Zhang L, Wu Y, Zhang H, Wu J, Gu Z, Dong C
Clinical, Cosmetic and Investigational Dermatology 2026, 19:564610
Published Date: 6 January 2026