Back to Journals » Patient Preference and Adherence » Volume 20
A Network Analysis of Medication Literacy and Associated Psychological Factors in Patients with Coronary Heart Disease and Diabetes
Authors Liang X ![]() , Lu M, Zou L, Chen C, Huang X, Li L, Zhang J, Wang R
, Lu M, Zou L, Chen C, Huang X, Li L, Zhang J, Wang R
Received 21 April 2026
Accepted for publication 17 June 2026
Published 3 July 2026 Volume 2026:20 618817
DOI https://doi.org/10.2147/PPA.S618817
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Xin Liang 1,*, Miaoji Lu1,*, Lewen Zou1, Ciyu Chen2, Xinhui Huang1, Lixia Li3, Junfeng Zhang4, Rui Wang1
1School of Nursing, Guangdong Pharmaceutical University, Guangzhou, Guangdong, People’s Republic of China; 2Department of Neurology, The First Affiliated Hospital of Guangdong Pharmaceutical University, Guangzhou, Guangdong, People’s Republic of China; 3School of Public Health, Guangdong Pharmaceutical University, Guangzhou, Guangdong, People’s Republic of China; 4Department of Nursing, Songshan Lake Central Hospital of
Dongguan City, Dongguan, Guangdong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Rui Wang, School of Nursing, Guangdong Pharmaceutical University, 283 Jianghai Avenue, Haizhu District, Guangzhou, Guangdong, 510310, People’s Republic of China, Email [email protected]
Junfeng Zhang, Department of Nursing, Songshan Lake Central Hospital of Dongguan City, Dongguan, Guangdong, 523320, People’s Republic of China, Email [email protected]
Purpose: To investigate the level of medication literacy and explore the conditional associations among medication literacy, beliefs about medicines, self-efficacy for appropriate medication use, and illness perceptions in patients with coronary heart disease and comorbid diabetes mellitus using network analysis.
Methods: A convenience sample of 417 patients with coronary heart disease and diabetes mellitus was recruited from two Grade A tertiary hospitals and a community health center in Guangdong, China between January and August 2025. Measures included a general information questionnaire, the Self-Assessment Scale for Medication Literacy in Patients with Coronary Heart Disease Comorbidity Diabetes, the Chinese version of the Beliefs about Medicines Questionnaire-Specific, the Chinese version of the Self-Efficacy for Appropriate Medication Use Scale, and the Chinese version of the Brief Illness Perception Questionnaire. Statistical analyses were conducted using SPSS 27.0 and R Studio. The network structure was estimated with the EBICglasso algorithm. Expected influence was used to identify central nodes, and bridge expected influence was used to identify bridge nodes. The stability and accuracy of the network were examined using case-dropping and bootstrap procedures.
Results: The average score of medication literacy was 77.09± 10.29. The network showed that the edge weight between node S1 (medication use under difficult circumstances) and node M5 (calculation) was 0.24, which was the largest among cross-network edges. The average node predictability was 48.6%. M2 (comprehension) had the largest expected influence index (0.89), and MB1 (necessity of medication) had the largest bridge expected influence index (0.35). The 95% confidence intervals for the edge weights were narrow. The correlation stability coefficients for both expected influence and bridge expected influence were 0.751.
Conclusion: Patients with coronary heart disease and diabetes mellitus exhibited a moderate level of medication literacy. Network analysis identified M2 (comprehension) as a core node and MB1 (necessity of medication) as a key bridge node, suggesting that they may be considered potential priorities for assessment and intervention development.
Keywords: coronary heart disease, diabetes mellitus, medication literacy, network analysis
Introduction
With the increasing prevalence of chronic diseases and population aging, multimorbidity has become a major global health challenge, imposing substantial burdens on patients, healthcare professionals, and healthcare systems. Coronary heart disease (CHD) and diabetes mellitus (DM) is one of the most common and harmful comorbidity patterns,1 with a comorbidity rate as high as 32.2%.2 CHD and DM are closely interrelated and may mutually influence disease progression. Individuals with type 2 diabetes carry approximately 1.5 to 2 times the risk of atherosclerotic cardiovascular disease (ASCVD) relative to the general population,3 which substantially raises their risk of ASCVD events and all-cause mortality.4
Currently, pharmacotherapy remains the cornerstone of disease management and secondary prevention in this population. Patients with both CHD and DM experience a chronic and prolonged disease course, requiring long-term, regular, and accurate medication use to prevent disease recurrence and progression. However, due to the complex pathophysiology of both conditions and the need for long-term polypharmacy, these patients are prone to issues such as poor medication adherence, inadequate medication management, and medication safety risks,5,6 which seriously impair physical function, clinical outcomes, and quality of life.
The World Health Organization (WHO) launched the Global Patient Safety Challenge “Medication Without Harm”, which has identified “polypharmacy and high-risk situations” as a priority area for action, aiming to significantly reduce preventable medication-related harm.7 Medication literacy (ML), derived from the concept of health literacy,8 is an important indicator of medication safety. ML has been defined as the degree to which individuals can obtain, comprehend, communicate, calculate and process patient-specific information about their medications to make informed medication and health decisions in order to safely and effectively use their medications, regardless of the mode by which the content is delivered (e.g., written, oral, or visual).9 As such, ML represents the contextual application of health literacy within the medication use setting.10
Existing evidence indicates that ML is generally inadequate among patients with CHD.11,12 Similarly, many patients with DM demonstrate only moderate or low levels of ML.13 Currently, no specific study has investigated ML in patients with both CHD and DM. However, given that the interaction between these two diseases leads to more complex medication regimens,14 the present study hypothesizes that the level of ML in patients with both conditions is lower than that in patients with either CHD or DM.
Notably, ML is associated with a range of psychological factors, including medication beliefs, self-efficacy for appropriate medication use, and illness perceptions.15–17 The Common-Sense Model (CSM) provides a theoretical framework for understanding the relationships among the aforementioned variables. According to the CSM, when confronted with a health threat, individuals form illness representations that include both cognitive and emotional dimensions. These representations subsequently guide information processing and behavioral decision-making through a feedback loop of “representation-coping-appraisal”.18 In the context of CHD and DM, patients’ illness perceptions, medication beliefs, and self-efficacy may therefore be relevant to how they understand, evaluate, and use medication-related information. The Health Belief Model (HBM) offers a complementary perspective by emphasizing the roles of perceived threat, perceived benefits, perceived barriers, cues to action, and self-efficacy in health-related decision-making.19 Taken together, these theoretical perspectives provide a rationale for examining ML, medication beliefs, self-efficacy for appropriate medication use, and illness perceptions within the same analytical framework.
It is noteworthy that most existing studies investigating the relationships among ML, self-efficacy for appropriate medication use, medication beliefs, and illness perception have predominantly relied on traditional correlation and regression methods focusing on pairwise associations. Although these methods can identify associations between variables, they are less able to describe the overall pattern of complex multivariate interrelationships among these factors. Network analysis is a visual and statistical approach that can estimate conditional associations among variables and identify statistically central or bridging nodes within a network. While well established in psychology,20,21 its use is increasingly growing in chronic disease research. For example, Zhang et al used network analysis to examine the interrelationships among self-stigma, insomnia, depression, and anxiety in patients with chronic diseases, identifying self-stigma emotions and daytime conditions as important core symptoms and several psychological symptoms as bridge symptoms.22 Chen et al applied trajectory network analysis to chronic disease trajectories among Chinese adults aged ≥45 years and found that arthritis acted as a starting node, while digestive diseases, hypertension, heart disease, and dyslipidemia occupied central positions in the disease trajectory network.23 Together, these studies suggest that network analysis is useful for identifying highly connected or bridging components within complex chronic disease-related systems. However, few studies have applied this approach to medication literacy and its psychosocial correlates among patients with CHD and DM.
In summary, this study aimed to investigate the level of ML in patients with CHD and DM and to use network analysis to explore the conditional associations among ML, medication beliefs, self-efficacy for appropriate medication use, and illness perceptions. Given that each of these variables is a multidimensional construct, and to reduce model complexity while enhancing the interpretability and clinical readability of the network model, the dimensions of each variable were selected as nodes in the network model.
Methods
Study Design and Participants
This was a cross-sectional network analysis conducted between January 2025 and August 2025 in Guangdong Province, China. Participants were recruited using convenience sampling from the cardiology and endocrinology inpatient wards and outpatient clinics of two tertiary Grade A hospitals, as well as from the outpatient clinic of one community health service center. These recruitment settings were selected because patients with CHD and DM are routinely treated and followed up in these clinical departments.
The inclusion criteria were as follows: (1) aged ≥18 years; (2) diagnosed with CHD according to the diagnostic criteria for stable coronary heart disease and diagnosed with diabetes according to relevant diagnostic criteria;24,25 (3) had received medication treatment for more than 3 months after being diagnosed with CHD and comorbid diabetes; (4) able to communicate, read, and understand basic Chinese; and (5) provided written informed consent. The exclusion criteria were as follows: (1) severe comorbid conditions, such as malignancy or renal failure; and (2) history of cognitive impairment, psychiatric disorders, severe hearing impairment, or communication disorders.
Sample Size
For network analysis, the sample size was determined by the total parameters, which were obtained by adding the threshold parameters (number of nodes) and pairwise association parameters [number of nodes × (number of nodes - 1)/2].20 This study included 12 nodes (M1-M5; S1-S2; MB1-MB2; DB1-DB3), resulting in 78 parameters to be estimated (12 threshold parameters +12 × 11/2 pairwise association parameters). Considering a requirement of 3–5 participants per parameter and accounting for a 20% rate of potentially invalid questionnaires, a minimum sample size of 293 participants was required. Furthermore, for sparse networks consisting of 20 or fewer nodes, a sample size of at least 350 is recommended to achieve moderate sensitivity, high specificity, and high edge weight correlation.26 In this study, the network consisted of 12 nodes, and the final sample included 417 participants, which was considered adequate for data analysis.
Measures
The General Information Questionnaire
This questionnaire was designed by the researchers and included three sections: sociodemographic data, disease-related data, and medication-related data. Sociodemographic information included age, gender, body mass index (BMI), educational level, marital status, employment status, place of residence, living arrangement, monthly household income, and medical payment method. Disease-related data included disease duration, family history, number of complications, frequency of hospitalizations, and smoking and drinking status. Medication-related data included duration of pharmacological treatment, monthly expenses for the treatment of CHD and DM, sources of medication, and whether the patient had received relevant medication education.
The Self-Assessment Scale for Medication Literacy in Patients with Coronary Heart Disease Comorbidity Diabetes
In 2024, Liu Haiting and colleagues in China developed the Self-Assessment Scale for Medication Literacy in Patients with CHD and DM based on the conceptual model of medication literacy.27 The scale included 23 items in 5 dimensions including acquisition, comprehension, communication, evaluation and calculation. A five-point Likert scale was used, ranging from “never” to “always,” scored from 1 to 5. The total score is the sum of all items, ranging from 23 to 115, with higher scores indicating a higher level of medication literacy. The total Cronbach’s α coefficient of the scale was 0.911; the retest reliability was 0.948; the average content validity index was 0.997. In this study, the Cronbach’s α coefficient of the scale was 0.941.
The Chinese Version of Beliefs About Medicines Questionnaire-Specific (BMQ-Specific)
The Beliefs about Medicines Questionnaire-Specific (BMQ-Specific) was developed by Horne et al.28 In this study, the Chinese version developed by Lv et al29 was used to assess patients’ beliefs about medications prescribed for specific health conditions. The questionnaire consists of two dimensions: necessity and concern, with each dimension containing five items. Participants are asked to rate their agreement using a five-point Likert scale. The score for each dimension ranges from 5 to 25, with higher scores indicating stronger necessity beliefs or stronger medication concerns. The overall medication belief score is calculated as the difference between the necessity score and the concerns score, ranging from −20 to +20. A positive difference indicates that patients perceive the necessity of taking medication as outweighing their concerns about potential side effects; conversely, a negative difference suggests that concerns about side effects outweigh the perceived necessity. The content validity index of the scale was 0.90, and the Cronbach’s α coefficient was 0.770. In the present study, the Cronbach’s α coefficients for the overall BMQ-Specific, necessity subscale, and concern subscale were 0.703, 0.855, and 0.790, respectively.
The Chinese Version of the Self-Efficacy for Appropriate Medication Use Scale (SEAMS)
The Self-efficacy for Appropriate Medication Use Scale (SEAMS) was developed by Risser and his research team.30 It is designed to assess patients’ confidence in taking medications appropriately under various circumstances and has been used in patients with chronic diseases. The scale consists of 13 items across two dimensions: medication use under difficult circumstances and medication use under uncertain circumstances. Each item is rated on a three-point Likert scale, with scores ranging from 1 (“not confident”) to 3 (“very confident”). Higher scores indicate greater self-efficacy for appropriate medication use. The SEAMS was translated into Chinese by Dong et al in 2015.31 For the Chinese version of the SEAMS, the Cronbach’s α coefficient was 0.934. In the present study, the Cronbach’s α coefficient was 0.872.
The Chinese Version of the Brief Illness Perception Questionnaire (BIPQ)
The Brief Illness Perception Questionnaire (BIPQ) was developed by Broadbent et al16 in 2006 and later translated and adapted into Chinese by Mei Yaqi et al.32 It is widely used to assess illness perception in patients with chronic diseases. The questionnaire consists of nine items covering three dimensions: cognitive representation of illness, emotional representation of illness, and illness coherence. Item 9, which assesses perceived causes of illness, is an open-ended item and is not included in the total score. The first eight items are rated on a scale from 0 to 10, with items 3, 4, and 7 reverse-scored. The total score is the sum of the item scores, ranging from 0 to 80, with higher scores indicating a greater perceived threat of the illness. Mei Yaqi et al validated the Chinese version of the BIPQ in breast cancer patients, reporting a Cronbach’s α of 0.77.32 The Chinese version of the BIPQ has also shown applicability in populations with CHD and DM. Li Jiamin et al33 reported a Cronbach’s α of 0.895 in patients with CHD; Xu Lixian et al34 reported a Cronbach’s α of 0.830 in older adults with type 2 diabetes; and Yang Han et al35 reported a Cronbach’s α coefficient of 0.735 in middle-aged and young adults with type 2 diabetes. In the present study, the Cronbach’s α coefficient of the scale was 0.784.
Data Collection
After rigorous screening according to the inclusion and exclusion criteria, eligible patients were invited to participate in this study. During data collection, participants’ rights, privacy, and confidentiality were protected. For inpatients, researchers first screened potentially eligible patients through the electronic medical record system and then approached those who met the eligibility criteria when their condition was stable and they were receiving routine medication treatment. For outpatients and community clinic patients, eligible patients were identified with the assistance of clinicians during routine visits and were invited to complete the survey while waiting for medication dispensing. Using standardized instructions, the investigators explained that the purpose of the survey was to understand patients’ daily medication practices and their level of medication literacy. Written informed consent was obtained from all participants before questionnaire administration. Data were collected using paper-based questionnaires, and relevant clinical information was verified through the hospital electronic medical record system when necessary. All questionnaires were collected on site. A total of 425 questionnaires were distributed. After excluding questionnaires with apparent patterned responses, such as identical answers across all items, or logical inconsistencies, 417 valid questionnaires were retained, yielding a valid response rate of 98.12%.
Data Analysis
Descriptive Statistics
There were no missing data in this study. Descriptive statistical analysis of baseline data was conducted in SPSS 27.0. Continuous variables with a normal distribution were presented as mean ± standard deviation (Mean ± SD), while non-normally distributed data were described using the median (interquartile range) [M (P25, P75)]. Categorical variables were presented as frequencies and percentages [n (%)].
Common Method Bias Test
To examine the potential influence of common method variance, Harman’s single-factor test was conducted. All items from the four scales were entered into an unrotated principal component analysis after reverse-coded items were appropriately transformed. The proportion of variance explained by the first unrotated factor was examined, and a value below the commonly used threshold of 40% was considered indicative of no serious common method bias.36
Network Analysis
Zero-order correlations and network analysis were performed using R version 4.5.1. A two-sided test with p < 0.05 was considered statistically significant.
The five dimensions of the Self-Assessment Scale for Medication Literacy in Patients with CHD and DM (acquisition, comprehension, communication, evaluation, and calculation), the two dimensions of the SEAMS (medication use under difficult circumstances and medication use under uncertain circumstances), the two dimensions of the BMQ-Specific (necessity of medication and concern of medication) and the three dimensions of the BIPQ (cognitive representation, emotional representation, and understanding of the illness) were included as network nodes. Nodes from the same scale were assigned to the same subnetwork. The network structure was estimated using the “EBICglasso” algorithm from the “qgraph” package, with the hyperparameter gamma set to the default value of 0.5.20 Based on the assumption of multivariate normality, this model uses partial correlations to quantify conditional dependencies between variables.20 Associations between nodes were examined using Pearson correlation analysis. Edges in the network represent partial correlations between two nodes after controlling for all other variables in the network.37
The predictability of each node was calculated using the “mgm” and “predict” functions from the “mgm” package, and the average predictability was computed.38 Predictability reflects the proportion of a node’s variance that can be predicted by the variances of its connected nodes, while average predictability indicates the extent to which the network nodes can be mutually predicted.
Node centrality was assessed using the “centralityPlot” function from the “qgraph” package.39 Bridge centrality was computed using the “bridge” function from the “networktools” package.40 Given the presence of both positive and negative edges in the network, the Expected Influence (EI) coefficient and Bridge Expected Influence (BEI) coefficient were calculated based on the two-step estimation method.41 Both the EI and BEI coefficient were standardized (z-scores) for visualization and comparative interpretation. Nodes with BEI rankings in the top 20% were selected as bridge nodes.40 Bootstrap difference tests for edge weights and for centrality indices were performed using the “differenceTest” function from the “bootnet” package. Pairwise differences in EI and BEI were evaluated, and the null hypothesis of no difference was rejected if the 95% bootstrap confidence interval for the difference did not include zero (equivalent to two-sided p < 0.05). The results were visualized as gray-black significance matrices (black squares indicate significant differences). Due to the involvement of multiple observational nodes in the study, the significance threshold after Bonferroni correction would have become extremely stringent, resulting in insufficient statistical power. Therefore, no adjustment for multiple comparisons was made in this study.
The precision of edge weights and the stability of node centrality were evaluated using the “bootnet” function from the “bootnet” package.20 A non-parametric bootstrap with 1000 iterations was applied to compute 95% confidence intervals (CIs) for edge weights and the correlation stability coefficient (CS-C). Narrower 95% CIs indicate greater precision in edge weight estimation.20 CS-C represents the maximum proportion of samples that can be removed while still preserving a strong correlation (r > 0.7) with the centrality metrics of the original data (α = 0.05). Values above 0.25 are considered acceptable, and values exceeding 0.5 indicate good stability.20
Ethics and Informed Consent Statement
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The study was reviewed and approved by the Ethics Committee of Dongguan Songshan Lake Central Hospital (Approval No. 2024–65) on December 21, 2024. Written informed consent was obtained from all participants prior to their inclusion in the study.
Results
Demographics and Clinical Characteristics
A total of 417 patients with CHD and DM were included in this study. The participants’ ages ranged from 36 to 92 years, with a mean age of 68.24 ± 10.39 years, and 59.5% were male. Regarding education level, 37.6% had primary education or below, 85.1% were married, and 42.7% lived with their spouse. Monthly household income ranged from 5000 to 6999 CNY in 35.9% of participants, and 98.1% were covered by medical insurance. In terms of body mass index (BMI), 42.9% were within the range of 18.5–23.9 kg/m2. The duration of CHD combined with DM was ≤5 years in 83.5% of patients, 71.9% had no CHD- or DM-related complications, and 36.9% had been on pharmacological treatment for ≥11 years. Regarding medication education, 46.3% occasionally received guidance, and 49.9% obtained their medications from hospitals. Detailed demographic and clinical characteristics of the patients are presented in Table 1.
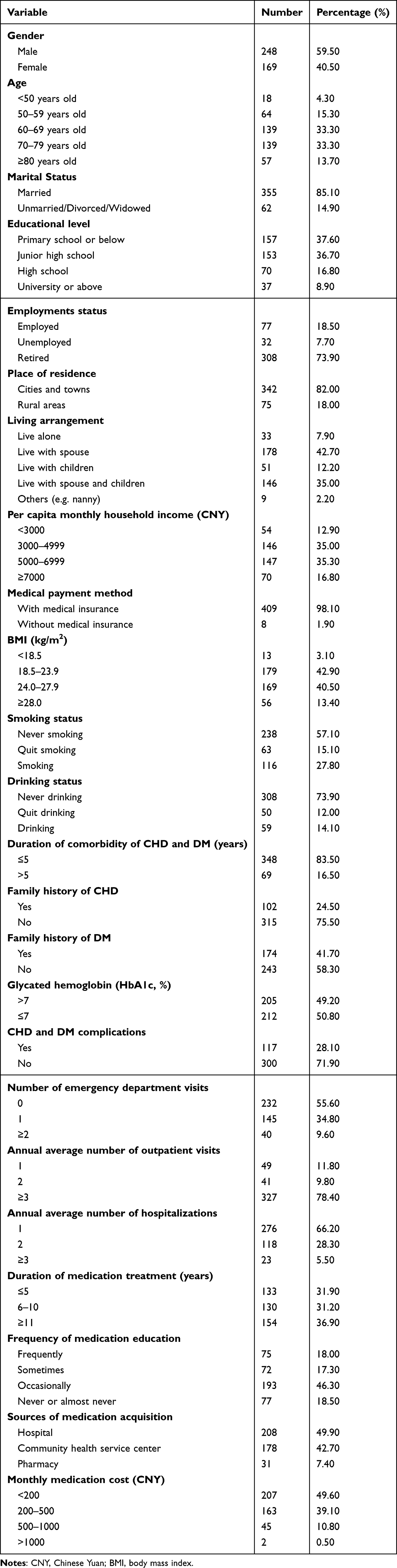 |
Table 1 Demographic and Clinical Characteristics of Study Participants (N = 417) |
Levels of ML, Medication Beliefs, Self-Efficacy for Appropriate Medication Use, and Illness Perception
In this study, the total ML score among patients with CHD and DM was 77.09 ± 10.29. The mean scores for the five dimensions were as follows: acquisition (16.78 ± 2.64), comprehension (23.70 ± 3.49), communication (9.57 ± 1.58), evaluation (10.39 ± 1.73), and calculation (16.65 ± 2.53). For medication beliefs, the total score was 6.26 ± 4.57, with scores of 19.84 ± 3.02 for necessity of medication and 13.58 ± 3.23 for concerns of medication. The total score for self-efficacy for appropriate medication use was 30.21 ± 4.71, including 12.58 ± 2.27 for under uncertain circumstances and 17.63 ± 2.82 for under difficult circumstances. The total score for illness perception was 40.52 ± 7.01, with subdimension scores of 26.52 ± 4.59 for cognitive representation, 10.29 ± 2.45 for emotional representation, and 3.70 ± 1.34 for understanding of the illness. Complete results for all variables and dimensions are summarized in Table 2.
 |
Table 2 The Means, Centrality Indices (with 95% Bootstrap Confidence Intervals), and Predictability for Each Dimension (N = 417) |
Common Method Bias Test
Harman’s single-factor test showed that the first unrotated factor accounted for 28.36% of the total variance, which was below the commonly used threshold of 40%.36 This result suggested that common method bias was unlikely to be a serious concern in the present study.
Network Analysis
Network Structure
Before network estimation, zero-order Pearson correlation coefficients were calculated to describe the overall bivariate associations among the study variables, as shown in Figure 1. In general, the five dimensions of medication literacy were positively correlated with medication necessity and self-efficacy for appropriate medication use (under difficult and uncertain circumstances), while showing negative correlations with medication concerns and the three dimensions of illness perception.
 |
Figure 1 Zero-order Pearson correlations among study variables (N = 417). Notes: Blue indicates positive correlations, red indicates negative correlations. *P < 0.05, **P < 0.01, ***P < 0.001. S1: medication use under difficult circumstances; S2: medication use under uncertain circumstances; MB1: necessity of medication; MB2: concern of medication; DB1: cognitive representation of illness; DB2: emotional representation of illness; DB3: understanding of illness; M1: acquisition; M2: comprehension; M3: communication; M4: evaluation; M5:calculation. |
The mean, SD, centrality indices, bridge centrality indices, and predictability values of all nodes are presented in Table 2. As shown in Figure 2, the estimated network contained 44 nonzero edges among 66 possible edges, including 22 positive and 22 negative edges. The signed edge weights ranged from −0.143 to 0.464. The mean edge weight was 0.038. The exact edge weights of all nonzero edges are provided in Table 3.
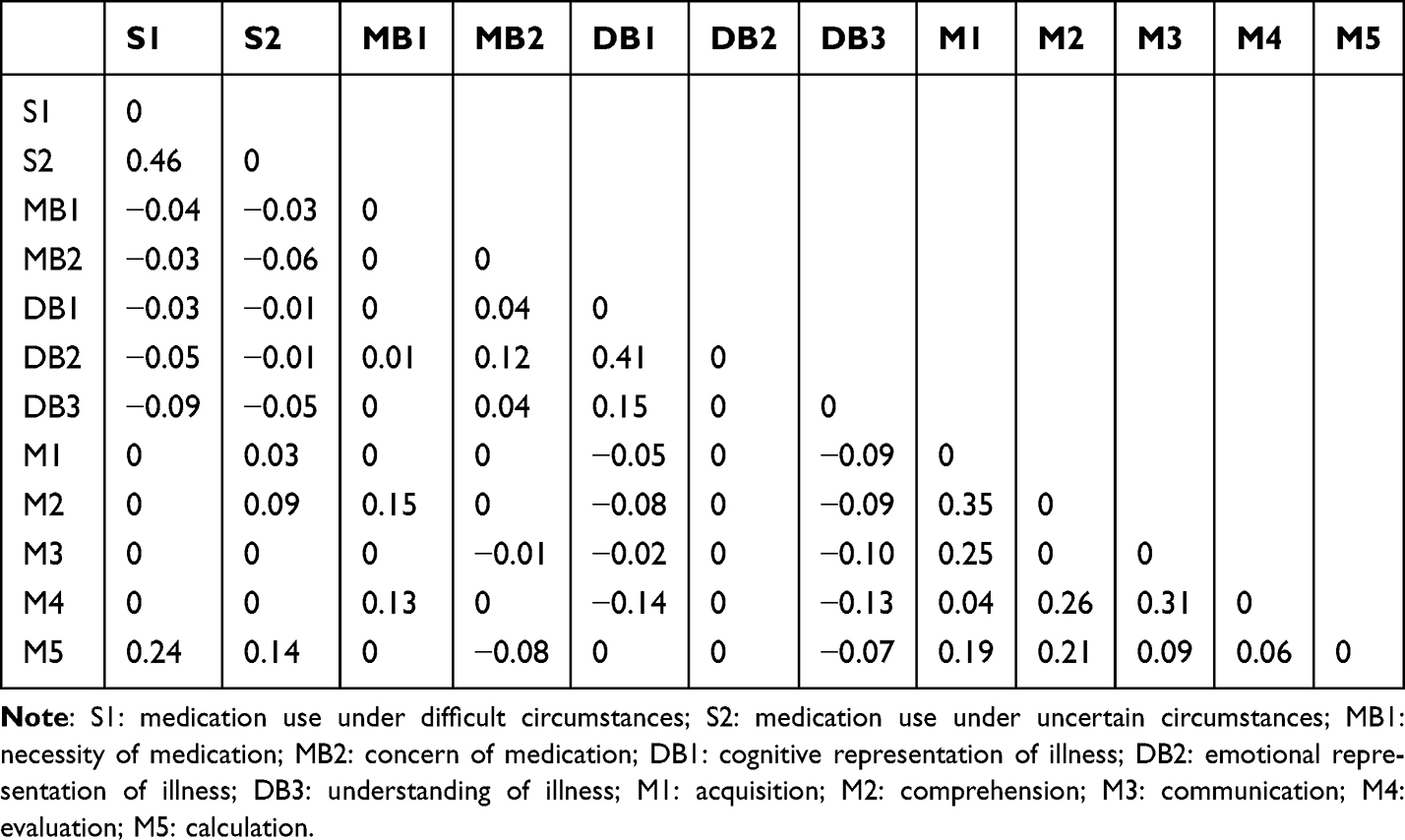 |
Table 3 The Edge Weights in the Network Model of Medication Literacy, Medication Beliefs, Self-Efficacy for Appropriate Medication Use, and Illness Perception (N = 417) |
 |
Figure 2 Network structure of medication literacy and psychological factors. Notes: Nodes represent the dimensions of medication literacy and psychological factors included in the network model. Edges represent regularized partial correlations between two nodes after controlling for all other nodes in the network. Blue solid edges indicate positive associations, and red dashed edges indicate negative associations. Edge thickness is proportional to the magnitude of the corresponding edge weight, with thicker edges indicating stronger associations. The pie around each node indicates node predictability (R2). |
Among cross-subnetwork connections, the edge weight between S1(medication use under difficult circumstances)-M5 (calculation) was the largest (edge weight = 0.24). MB1 (necessity of medication) was positively correlated with M2 (comprehension) and M4 (evaluation), with edge weights of 0.15 and 0.13, respectively. M5 (calculation) was positively correlated with S2 (medication use under uncertain conditions) (edge weight = 0.14). Of note, node M4 (evaluation) was negatively correlated with DB1 (cognitive representation of illness) and DB3 (understanding of illness), with edge weights of −0.14 and −0.13, respectively.
Node Predictability
The average predictability was 48.6%. As shown in Table 2, among all nodes, M2 (comprehension) showed the highest predictability value (71.0%). Notably, all five dimensions of ML (M1-M5), both dimensions of self-efficacy for appropriate medication use (S1-S2), and DB1 (cognitive representation of illness) showed predictability values of approximately 50% or higher. In contrast, MB1 (necessity of medication) and MB2 (concern of medication) showed low predictability values of 14.4% and 15.0%, respectively.
Network Nodes’ Centrality and Bridge Centrality
The EI coefficient and BEI coefficient of network nodes were shown in Figures 3 and 4 and Table 2. Among all nodes, M2 (comprehension) demonstrated the highest EI coefficient, indicating that interventions targeting the improvement of patients’ ability to comprehend medication information may produce the strongest cascading activation effects on other variables in the network. DB3 (understanding of the illness) exhibited negative and low centrality indices in the network analysis (EI = −0.487; BEI = −1.159; predictability = 0.478), indicating its relatively peripheral position and weak direct connections with core variables such as medication literacy, medication beliefs, and self-efficacy for appropriate medication use.
 |
Figure 3 Expected influence coefficients of network nodes. Notes: Expected influence is a centrality index that reflects the sum of all edge weights connected to a node. Higher values indicate stronger overall connections with other nodes in the network. |
 |
Figure 4 Bridge expected influence coefficients of network nodes. Notes: Bridge expected influence is a bridge centrality index that reflects the sum of edge weights connecting a node with nodes from other predefined communities. Higher values indicate stronger cross-community connections. |
Among the bridge nodes, MB1 (necessity of medication) demonstrated the highest BEI coefficient (0.35), identifying it as a important bridge between the medication beliefs subnetwork and the medication literacy subnetwork. Thus, in clinical practice, strengthening patients’ belief in medication necessity may represent the most efficacious psychological pathway to improving medication literacy. Bootstrapped difference tests were conducted to compare the centrality indices between nodes. The results of the expected influence (EI) difference test and bridge expected influence (BEI) difference test are presented in Figure 5 and 6, respectively. These results showed that some pairwise differences in EI and BEI were statistically significant; however, not all nodes differed significantly from one another.
 |
Figure 5 Bootstrapped difference tests for expected influence. Notes: Black squares indicate statistically significant differences between the expected influence values of two nodes, whereas gray squares indicate non-significant differences. The values on the diagonal represent the estimated expected influence values for each node. |
 |
Figure 6 Bootstrapped difference tests for bridge expected influence. Notes: Black squares indicate statistically significant differences between the bridge expected influence values of two nodes, whereas gray squares indicate non-significant differences. The values on the diagonal represent the estimated bridge expected influence values for each node. |
Test of the Accuracy of Network Edge Weights and the Stability of Node Centrality
As shown in Figures 7 and 8, bootstrapping procedures indicated narrow 95% confidence intervals for edge weights, suggesting good precision. Typically, the Correlation Stability Coefficient should exceed 0.25, with a preferred value greater than 0.5. The correlation stability coefficients for EI and BEI were 0.751, indicating that even after removing up to 75.1% of the samples (for EI and BEI), centrality measure rankings estimated from the reduced datasets remained strongly correlated with the full dataset.
 |
Figure 7 Accuracy of edge-weight estimates based on nonparametric bootstrap. Notes: The plot shows the 95% bootstrap confidence intervals of edge weights based on 1000 nonparametric bootstrap samples. Narrower intervals indicate greater precision of edge-weight estimation. |
 |
Figure 8 Case-dropping bootstrap stability of centrality indices. Notes: The plot shows the stability of expected influence and bridge expected influence under the case-dropping bootstrap procedure. The correlation stability coefficient was calculated to evaluate the robustness of centrality estimates. |
Discussion
Level of ML in Patients with CHD and DM
The results of this study showed that the ML score of patients with CHD and DM was 77.09 ± 10.29, with an item mean score of 3.35 ± 0.45, and the scoring rate was 67.03% (calculated as total score divided by maximum possible score × 100%, 77.09/115 × 100%), indicating a moderate level of ML. Although the measurement tool for ML used in this study has not been reported in previous literature, the findings are consistent with existing research on ML, suggesting that there remains substantial room for improvement in this patient population. Among the various dimensions of ML, the evaluation dimension scored the highest (3.46 ± 0.58), indicating that patients possess relatively strong abilities in accessing medication information, self-monitoring of medication use, and observing adverse drug reactions.12,42,43 The communication dimension scored the lowest (3.19±0.53), reflecting insufficient willingness among patients to proactively communicate medication-related information with healthcare providers, family members, or others. Based on these findings, clinical interventions should prioritize enhancing patients’ medication-related communication skills with both healthcare professionals and family members, serving as a key strategy for improving overall medication literacy.
Edges Between Subnetworks
Across different subnetworks, the edge between S1 (medication use under difficult circumstances) and M5 (calculation) exhibited the strongest connection (edge weight = 0.24) and showed a positive association. This finding suggests that medication-related calculation ability may be closely associated with patients’ confidence in adhering to medication under difficult circumstances among patients with CHD and DM.
Previous studies have reported that calculation ability may play a critical role in supporting self-efficacy in medication use when patients face difficulties in medication management.43,44 Patients with CHD and DM typically face complex medication regimens, which involve multiple hypoglycemic agents, antiplatelet drugs, lipid-lowering medications, and others.14 The clinical relevance of this issue is further supported by a regional cross-sectional study among patients with chronic diseases, which reported that nearly one-quarter of participants were nonadherent to their medications, with side effects and forgetfulness identified as important reasons for nonadherence.45 These factors may represent examples of difficult medication-taking situations in which patients need adequate medication-related skills and confidence to maintain regular medication use.
The American Diabetes Association (ADA)’s Standards of Care in Diabetes emphasizes that for patients requiring insulin therapy, a strategy of “adjusting mealtime doses based on anticipated needs” should be adopted, which requires patients to possess certain calculation ability. Patients need to be able to perform numerical calculations to determine the total number of pills they need to take daily, as well as to identify and respond to potential side effects in order to effectively manage their medication regimen.46 Calculation ability serves as a foundational ability for patients to cope with medication complexity and mitigate medication-related risks. Strong calculation ability not only helps patients interpret blood glucose values and calculate medication dosages but also enables them to understand medication risks, plan medication timing and doses in advance, and solve practical medication-related problems through logical thinking and mathematical skills, ultimately making appropriate health-related decisions.43
Therefore, when patients possess sufficient medication-related calculation skills, they can more effectively address various medication-related issues in real-world medication scenarios, thereby enhancing their confidence in taking medications regularly as prescribed. Furthermore, the study by Bouclaous et al demonstrated that patients with higher levels of self-efficacy tend to exhibit stronger calculation ability.43 Thus, a positive cycle may exist between calculation ability and confidence in adhering to medication under difficult circumstances: stronger computational ability may support patients with CHD and DM to perform various complex medication-related calculations, thereby enhancing their medication self-efficacy in challenging situations; this confidence in “believing one can adhere to medication in difficult situations” may motivate patients to more proactively embrace such challenges and further improve their computational skills through learning.
Hence, to strengthen the relationship and strive to establish a positive cycle between medication literacy and self-efficacy for appropriate medication use among patients with CHD and DM, healthcare providers should proactively explore effective methods to enhance patients’ calculation ability. In clinical nursing practice, this can be achieved by enhancing medication education through the integration of dose-calculation aids, scenario-based simulations, and feedback-driven instruction.47
Core Node
This study showed that M2 (comprehension) had the highest EI and predictability, suggesting that M2 occupied a statistically central position in the network comprising ML, self-efficacy for appropriate medication use, medication beliefs, and illness perception among patients with CHD and DM. This finding indicates that M2 had the strongest overall pattern of associations with other variables in the network. Comprehension refers to the ability to understand medication-related information received or obtained from different sources and plays a critical role in safe and effective medication use.48 The qualitative study by Xu et al emphasized that understanding one’s medications is crucial for enhancing the confidence of older patients with CHD in adhering to their medication regimens.49 According to the Knowledge-Attitude-Practice Theory, when patients with CHD and DM acquire and understand medication information, they may develop medication beliefs and adjust illness perceptions.50 Taken together, these findings indicate that medication comprehension is not only a key component of ML but also closely related to self-efficacy for appropriate medication use, medication beliefs, and illness perceptions. Thus, medication comprehension should be regularly assessed and considered a high-priority target for ML interventions, especially in patients with complex long-term comorbid conditions.
It is noteworthy that the three illness perception nodes (DB1–DB3) showed lower EI than most ML dimensions (M1–M5) in this network. This result should not be interpreted as indicating that illness perception is unimportant. Rather, it may suggest that illness perception plays a more distal or background role in the network. Several explanations may account for this finding. First, ML is directly embedded in daily medication use and may therefore have stronger direct connections with self-efficacy for appropriate medication use and medication beliefs. Previous studies have supported close associations among ML, medication self-efficacy, medication beliefs, and medication adherence in patients with chronic diseases.42,51 In contrast, illness perception reflects patients’ cognitive and emotional representations of illness, and its influence on medication-related behaviors may be more indirect.52 Second, patients with CHD and DM often experience long-term disease management, and their illness perceptions may have become relatively stable over time. By contrast, ML may be more directly influenced by current medication education, medication-taking experience, and healthcare communication, making it more closely connected with other modifiable factors in the network.
Therefore, the lower centrality of illness perception nodes does not mean that illness perception should be ignored. Instead, it suggests that ML dimensions may serve as more immediate intervention targets, while illness perception should be considered an important psychological background factor that may influence medication-related behaviors through beliefs, self-efficacy, and coping processes.
Bridge Node
In this network model, MB1 (necessity of medication) showed the highest BEI, indicating the strongest cross-community associations among ML, self-efficacy for appropriate medication use, medication beliefs, and illness perception in patients with CHD and DM. Based on the edge-weight results, MB1 was positively associated with M2 (comprehension) and M4 (evaluation), with edge weights of 0.15 and 0.13, respectively. In contrast, the connections between MB1 and self-efficacy for appropriate medication use or illness perception nodes were relatively weak. These findings suggest that the bridging role of MB1 was mainly reflected in its associations with ML dimensions, particularly comprehension and evaluation, rather than in direct connections with illness perception or self-efficacy nodes. Medication necessity refers to patients’ beliefs about the need for prescribed medication to control disease and prevent adverse outcomes. The positive associations between MB1 and the ML dimensions of comprehension and evaluation suggest that patients who better understand and evaluate medication information may be more likely to recognize the value of long-term pharmacotherapy. This interpretation is consistent with previous evidence showing that ML is related to medication beliefs and medication adherence in patients with chronic diseases.42 It is also broadly consistent with the Necessity-Concerns Framework, which emphasizes that medication-taking behavior is related to patients’ perceived need for treatment and their concerns about potential adverse consequences.53 In addition, Jiang et al reported that medication belief profiles differed among patients with type 2 diabetes and that patients with stronger necessity beliefs and lower concern beliefs tended to show better medication adherence.54 These studies support the importance of assessing both medication necessity and concerns in patients with long-term chronic diseases.
Therefore, clinical interventions may consider medication necessity as a potential target for improving medication management in patients with CHD and DM. Healthcare professionals should assess patients’ beliefs about the necessity during clinical consultations and follow-up visits, especially among patients with insufficient medication understanding or concerns about long-term drug use. Individualized medication education using plain language, medication lists, figurative explanations, visual materials, popular science videos, or illustrated educational materials may help patients better understand the purpose and benefits of long-term pharmacotherapy. These strategies may strengthen patients’ perceived necessity of medication and support appropriate medication use, but their effectiveness should be further evaluated in future intervention studies.
Limitations
Several limitations of this study should be acknowledged. First, participants were recruited using convenience sampling from two tertiary Grade A hospitals and one community health service center in Guangdong Province. As a non-probability sampling method, convenience sampling may have introduced selection bias and may limit the generalizability of the findings. Therefore, caution is needed when extending the findings to patients with CHD and comorbid DM in other healthcare settings, rural areas, or less developed regions. Second, all variables were assessed using self-reported questionnaires, which may be subject to reporting biases, such as social desirability bias and recall bias. Although Harman’s single-factor test suggested that common method bias was unlikely to be a serious concern in this study, the possibility of common method variance cannot be completely ruled out. Third, the cross-sectional design precludes causal inference. Therefore, the central and bridge nodes identified in this network should be interpreted as statistical associations rather than causal determinants or confirmed intervention targets. Longitudinal and interventional studies are needed to clarify the temporal and potentially causal relationships among medication literacy, medication beliefs, self-efficacy for appropriate medication use, and illness perception. Fourth, the network model was limited by the variables and node levels included in the analysis. Demographic, clinical, and medication-related variables, such as educational level, age, disease duration, and medication regimen characteristics, were not incorporated into the network estimation, and the observed edges may therefore have been confounded or moderated by unmodeled variables. In addition, this study used dimension-level scores as network nodes. Although this approach reduced model complexity and improved interpretability, it may have obscured item-level heterogeneity within each dimension and may have strengthened associations between dimensions from the same scale. Finally, although the network showed acceptable stability, some nodes, particularly medication belief nodes, had relatively low predictability, suggesting that part of their variance may be explained by factors not included in the current network. Future studies should use probability sampling or more diverse multicenter samples, combine self-reported data with objective medication-related indicators, and consider covariate-adjusted networks, subgroup network comparisons, moderated network models, or item-level and multilevel network analyses to further validate and extend these findings.
Conclusion
This study employed network analysis to investigate the current status of ML and its complex relationships with medication beliefs, self-efficacy for appropriate medication use, and illness perceptions in patients with CHD and DM. The results revealed an overall moderate level of ML among the patients. Network analysis identified M2 (comprehension) as a statistically central node within the network, while MB1 (necessity of medication) served as a statistically critical bridge node. Based on these findings, clinical interventions may benefit from focusing on patients’ medication comprehension, reinforcement of medication necessity beliefs. This study provides an important theoretical foundation for developing targeted strategies to improve ML in patients with CHD and DM, although further longitudinal or interventional studies are needed to establish causality.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author, Rui Wang, upon reasonable request.
Ethics and Informed Consent Statement
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki. The study was reviewed and approved by the Ethics Committee of Dongguan Songshan Lake Central Hospital (Approval No. 2024-65) on December 21, 2024. Written informed consent was obtained from all participants prior to their inclusion in the study.
Acknowledgments
We give our sincere thanks to all patients with coronary heart disease and diabetes who participated in this study, and particularly like to thank the Nursing Departments of all participating hospitals for their dedicated support and collaboration.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received no additional funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Fan J, Sun Z, Yu C, et al. Multimorbidity patterns and association with mortality in 0.5 million Chinese adults. Chin Med J. 2022;135(6):648–20. doi:10.1097/CM9.0000000000001985
2. Einarson TR, Acs A, Ludwig C, et al. Prevalence of cardiovascular disease in type 2 diabetes: a systematic literature review of scientific evidence from across the world in 2007–2017. Cardiovasc Diabetol. 2018;17(1):83. doi:10.1186/s12933-018-0728-6
3. Ahmad A, Lim LL, Morieri ML, et al. Precision prognostics for cardiovascular disease in type 2 diabetes: a systematic review and meta-analysis. Commun Med. 2024;4(1):11. doi:10.1038/s43856-023-00429-z
4. Joseph JJ, Deedwania P, Acharya T, et al. Comprehensive management of cardiovascular risk factors for adults with type 2 diabetes: a scientific statement from the American Heart Association. Circulation. 2022;145(9):e722–e759. doi:10.1161/CIR.0000000000001040
5. Dovjak P. Polypharmacy in elderly people. Wien Med Wochenschr. 2022;172(5):109–113. doi:10.1007/s10354-021-00903-0
6. Niu YX, Guo YP, Zhang CH, et al. Medication experiences of patients with chronic multimorbidities: a qualitative meta-synthesis. Chin J Nurs. 2023;58(22):2777–2784.
7. World Health Organization. Medication without harm. Available from: https://www.who.int/initiatives/medication-without-harm.
8. Committee on Safety of Medicines Working Group on Patient Information. Always Read the Leaflet: Getting the Best Information with Every Medicine. London: The Stationery Office; 2005.
9. Pouliot A, Vaillancourt R, Stacey D, et al. Defining and identifying concepts of medication literacy: an international perspective. Res Social Adm Pharm. 2018;14(9):797–804. doi:10.1016/j.sapharm.2017.11.005
10. Gentizon J, Hirt J, Jaques C, et al. Instruments assessing medication literacy in adult recipients of care: a systematic review of measurement properties. Int J Nurs Stud. 2021;113:103785. doi:10.1016/j.ijnurstu.2020.103785
11. Qiao L, Ding S, Zhong Z, et al. Association between social support and medication literacy in Chinese patients with coronary heart disease. Front Cardiovasc Med. 2021;8:705783. doi:10.3389/fcvm.2021.705783
12. Zheng F, Ding S, Lai L, et al. Relationship between medication literacy and medication adherence in inpatients with coronary heart disease in Changsha, China. Front Pharmacol. 2020;10:1537. doi:10.3389/fphar.2019.01537
13. Levic M, Bogavac-Stanojevic N, Ubavic S, Krajnovic D. Pharmacotherapy literacy level and predictors of low literacy among diabetes mellitus type 2 patients in Serbia. BMC Public Health. 2023;23(1):1822. doi:10.1186/s12889-023-16639-y
14. Virani SS, Newby LK, Arnold SV, et al. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA guideline for the management of patients with chronic coronary disease: a report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2023;148(9):e9–e119. doi:10.1161/CIR.0000000000001168
15. Liu Z, Lu X, Li Y, et al. The correlation between medication self-management with rational medication use self-efficacy and medication literacy in patients with stroke. Patient Prefer Adherence. 2025;19:941–953. doi:10.2147/PPA.S507404
16. Lu T, Yang Z, Chen P, et al. Influencing factors of medication literacy among community-dwelling older adult patients with hypertension: a study based on social learning theory. Front Pharmacol. 2023;14:1184701. doi:10.3389/fphar.2023.1184701
17. Zhang ZY, Bao L, Ding W, et al. Qualitative study of medication literacy in patients after percutaneous coronary intervention. Chin. Nurs. Res. 2024;22(5):803–808.
18. Hagger MS, Orbell S.The common sense model of illness self-regulation: a conceptual review and proposed extended model.Health Psychol Rev.2022.16;3;347–377. doi:10.1080/17437199.2021.1878050
19. Alyafei A, Easton-Carr R. The health belief model of behavior change. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
20. Epskamp S, Borsboom D, Fried EI. Estimating psychological networks and their accuracy: a tutorial paper. Behav Res Methods. 2018;50(1):195–212. doi:10.3758/s13428-017-0862-1
21. Miao J, Wu Y, Yuan J, et al. Network analysis of interpersonal sensitivity and self-efficacy in nursing students. BMC Nurs. 2025;24(1):63. doi:10.1186/s12912-025-02725-6
22. Zhang X, Lin R, Zhang Z, et al. Comorbidity network of self-stigma, insomnia, and mental health in chronic disease patients: a network analysis. Psychol Res Behav Manag. 2025;18:2333–2345. doi:10.2147/PRBM.S529940
23. Chen J, Zhang F, Zhang Y, et al. Trajectories network analysis of chronic diseases among middle-aged and older adults: evidence from the China Health and Retirement Longitudinal Study (CHARLS). BMC Public Health. 2024;24(1):559. doi:10.1186/s12889-024-17890-7
24. Chinese Society of Cardiology, Chinese Medical Association; Interventional Cardiology Group; Chinese Society of Cardiology, Chinese Medical Association; Atherosclerosis and Coronary Heart Disease Group. Guideline on the diagnosis and treatment of stable coronary artery disease. Zhonghua xin xue guan bing za zhi. 2018;46(9):680–694. doi:10.3760/cma.j.issn.0253-3758.2018.09.004.
25. Alberti KG, Zimmet PZ. Definition, diagnosis and classification of diabetes mellitus and its complications. Part 1: diagnosis and classification of diabetes mellitus. Provisional report of a WHO Consultation. Diabet Med. 1998;15(7):539–553
26. Constantin M, Cramer AOJ. Sample Size Recommendations for Estimating Cross-Sectional Network Models. Tilburg University; 2018.
27. Liu HT, Wang YM, Zheng BB, et al. Development and reliability and validity test of the medication literacy self-rating Scale for patients with coronary heart disease and diabetes mellitus. Chin J Nurs. 2024;59(9):1065–1072.
28. Horne R, Weinman J. Patients’ beliefs about prescribed medicines and their role in adherence to treatment in chronic physical illness. J Psychosom Res. 1999;47(6):555–567. doi:10.1016/S0022-3999(99)00057-4
29. Si ZX, Zhou M, Cao GQ, et al. Reliability and validity of the Chinese version of the Beliefs about Medicines Questionnaire-Specific in patients with anticoagulation after heart valve replacement. J Nurs Sci. 2013;28(4):20–23.
30. Risser J, Jacobson TA, Kripalani S. Development and psychometric evaluation of the Self-efficacy for Appropriate Medication Use Scale (SEAMS) in low-literacy patients with chronic disease. J Nurs Meas. 2007;15(3):203–219. doi:10.1891/106137407783095757
31. Dong XF, Liu YJ, Wang AX. Reliability and validity of the Chinese version Self-efficacy for Appropriate Medication Use Scale. J Nurs Sci. 2015;30(11):47–49.
32. Mei YQ, Li HP, Yang YJ, et al. Reliability and validity of Chinese version of the Brief Illness Perception Questionnaire in patients with breast cancer. J. Nurs. 2015;22(24):11–14. doi:10.16460/j.issn1008-9969.2015.24.011
33. Li JM, Li Y, Qin JW, et al. Path analysis of the status and influencing factors of heart-focused anxiety in patients with coronary heart disease. Mod Preventive Med. 2025;52(1):15–20. doi:10.20043/j.cnki.MPM.202407264
34. Xu LX, Cui LP, Chen SQ, et al. Aging expectation status and influencing factors of elderly diabetic patients. J Nurs Administrat. 2025;25(1):39–43.
35. Yang H, Sun QY, Xiao SY, et al. Analysis of the current status and influencing factors of fear of disease progression in young and middle-aged patients with type 2 diabetes mellitus. Chongqing Med. 2023;52(21):3349–3354.
36. Podsakoff PM, MacKenzie SB, Lee JY, et al. Common method biases in behavioral research: a critical review of the literature and recommended remedies. J Appl Psychol. 2003;88(5):879–903. doi:10.1037/0021-9010.88.5.879
37. Chen F, Zhao X, Qian X, et al. Relationships among sleep quality, anxiety, and depression among Chinese nurses: a network analysis. J Affect Disord. 2025;389:119587. doi:10.1016/j.jad.2025.119587
38. Haslbeck JMB, Waldorp LJ. mgm: estimating time-varying mixed graphical models in high-dimensional data. J Stat Softw. 2020;93(8):1–46. doi:10.18637/jss.v093.i08
39. Wilkinson L. ggplot2: elegant graphics for data analysis by Wickham H. Biometrics. 2011;67(2):678–679. doi:10.1111/j.1541-0420.2011.01616.x
40. Jones PJ, Ma R, McNally RJ. Bridge centrality: a network approach to understanding comorbidity. Multivariate Behav Res. 2021;56(2):353–367. doi:10.1080/00273171.2019.1614898
41. Dal Santo F, González-Blanco L, García-Portilla MP, et al. From gut to brain: a network model of intestinal permeability, inflammation, and psychotic symptoms in schizophrenia. Eur Neuropsychopharmacol. 2024;79:32–37. doi:10.1016/j.euroneuro.2023.10.004
42. Jiang S, Zhu Z, Liao G, et al. Relationship between medication literacy and beliefs among persons with type 2 diabetes mellitus in Guangdong, China. Patient Prefer Adherence. 2023;17:2039–2050. doi:10.2147/PPA.S420383
43. Bouclaous C, Azar LJ, Barmo N, et al. Levels and correlates of numeracy skills in Lebanese adults with diabetes: a cross-sectional study. Int J Environ Res Public Health. 2022;19(17):10557. doi:10.3390/ijerph191710557
44. Liu H, Yao Z, Shi S, et al. The mediating effect of self-efficacy on the relationship between medication literacy and medication adherence among patients with type 2 diabetes. Patient Prefer Adherence. 2023;17:1657–1670. doi:10.2147/PPA.S413385
45. Prabahar K, Albalawi MA, Almani L, et al. Assessment of medication adherence in patients with chronic diseases in Tabuk, Kingdom of Saudi Arabia. J Res Pharm Pract. 2020;9(4):196–201. doi:10.4103/jrpp.JRPP_20_97
46. Alhomoud F, Alsaeed W, Alzainaldain F, et al. Think before you take: understanding adult medication literacy in Saudi Arabia. Patient Prefer Adherence. 2025;19:1973–1990. doi:10.2147/PPA.S536578
47. Talevski J, Wong Shee A, Rasmussen B, et al. Teach-back: a systematic review of implementation and impacts. PLoS One. 2020;15(4):e0231350. doi:10.1371/journal.pone.0231350
48. Neiva Pantuzza LL, Nascimento ED, Crepalde-Ribeiro K, et al. Medication literacy: a conceptual model. Res Social Adm Pharm. 2022;18(4):2675–2682. doi:10.1016/j.sapharm.2021.06.003
49. Xu M, SHS L, Zhu L, Huang X. Understanding medication self-management at home among older adults with coronary artery disease: a qualitative study. Patient Prefer Adherence. 2025;19:3069–3082. doi:10.2147/PPA.S537115
50. Chen X, Xiao F, Miao Y, et al. Behaviors and influencing factors of Chinese oncology nurses towards frailty care: a cross-sectional study based on knowledge-attitude-practice theory in 2024. PLoS One. 2025;20(1):e0313822. doi:10.1371/journal.pone.0313822
51. Wang W, Luan W, Zhang Z, et al. Association between medication literacy and medication adherence and the mediating effect of self-efficacy in older people with multimorbidity. BMC Geriatr. 2023;23(1):378. doi:10.1186/s12877-023-04072-0
52. Mobini S, Allahbakhshian A, Shabanloei R, et al. Illness perception, self-efficacy, and medication adherence in patients with coronary artery disease: a path analysis of conceptual model. SAGE Open Nurs. 2023;9:23779608231171772. doi:10.1177/23779608231171772
53. Horne R, Chapman SC, Parham R, et al. Understanding patients’ adherence-related beliefs about medicines prescribed for long-term conditions: a meta-analytic review of the Necessity-Concerns Framework. PLoS One. 2013;8(12):e80633. doi:10.1371/journal.pone.0080633
54. Jiang S, Luo T, Zhu Z, et al. Latent profile analysis of medication beliefs in patients with type 2 diabetes in the hospital-home transition and comparison with medication adherence. Patient Prefer Adherence. 2024;18:839–853. doi:10.2147/PPA.S450107
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Serum FGF23 and DPP4 Levels as Biomarkers for Coronary Artery Disease Severity in Type 2 Diabetic Patients with Coronary Heart Disease
Zhong X, Liang Z, Liao H, Zhan Y, Li G, Wu H, Li J
International Journal of General Medicine 2025, 18:1757-1764
Published Date: 28 March 2025
Hs-CRP, Diabetic Status, and Adverse Events Among Patients Receiving Statin Therapy Following PCI—A Prospective Registry-Based Study
Chen X, Wang HY, Sun W, Lin Z, Qiao Z, Bian X, Yin D, Feng L, Zhu C, Song W, Wang H, Jia L, Dong Q, Dou K
Journal of Inflammation Research 2025, 18:9261-9274
Published Date: 15 July 2025
Analysis Impact of Positive Psychological Capital on Quality of Life Among Patients Post Percutaneous Coronary Intervention: A Cross-Sectional Study
Kudelati Z, Yin S, Chen S, Han S, Yuan S, Wang H
Journal of Multidisciplinary Healthcare 2025, 18:7413-7421
Published Date: 11 November 2025