Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
A Multidisciplinary Intragastric Balloon Care Pathway for Weight Management in a Tertiary Malaysian Centre: Clinical Practice Framework
Authors Gill T, Loo GH ![]() , Muthkumaran G, Kosai NR
, Muthkumaran G, Kosai NR
Received 21 December 2025
Accepted for publication 10 April 2026
Published 1 May 2026 Volume 2026:19 590735
DOI https://doi.org/10.2147/JMDH.S590735
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Theeran Gill, Guo Hou Loo, Guhan Muthkumaran, Nik Ritza Kosai
Upper GI & Metabolic Surgery Unit, Department of Surgery, Faculty of Medicine, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia
Correspondence: Guo Hou Loo, Upper GI & Metabolic Surgery Unit, Department of Surgery, Faculty of Medicine, Universiti Kebangsaan Malaysia, Kuala Lumpur, Malaysia, Email [email protected]
Background: Obesity is a chronic disease with major metabolic, physical, and psychosocial consequences. Intragastric balloon (IGB) therapy is a minimally invasive endoscopic or device-based option that can bridge the gap between lifestyle intervention and bariatric surgery for selected patients. Despite expanding use, many centres lack a standardized multidisciplinary pathway to ensure appropriate selection, peri-procedural safety, nutrition support, and structured follow-up.
Objective: To describe the development and implementation framework of a standardized multidisciplinary IGB care pathway in a tertiary Malaysian centre, including patient selection, peri-procedural pharmacotherapy, nutritional protocols, safety monitoring, and follow-up scheduling.
Methods: This is a clinical practice framework describing protocol development based on local practice needs, alignment with national recommendations, and evidence-informed considerations. The pathway consolidates: (1) patient selection and assessment algorithm, (2) standardized medication regimen, (3) dietitian-led post-procedure nutritional support options, and (4) structured clinic follow-up milestones.
Practice Framework: The pathway defines indications (including Asian population considerations), anticipated efficacy expectations, adverse effect management, serious complication awareness, nutrition regimens using commonly available oral nutritional supplements, and staged follow-up at 2 weeks, 4 months, 8 months, and 1 year. It also outlines local device options used in the institution and key counseling points for durability and weight regain prevention.
Conclusion: A standardized multidisciplinary intragastric balloon care pathway provides a structured approach to delivering IGB therapy in routine clinical practice. Its clinical effectiveness requires validation through prospective outcome-based studies. It may serve as a practical reference for centres developing endobariatric services in similar healthcare settings.
Keywords: intragastric balloon, obesity, bariatric endoscopy, patient care team, nutritional support, Malaysia
Introduction
Obesity is a chronic, relapsing disease characterised by excessive adiposity and associated metabolic, mechanical, and psychosocial complications. It is strongly associated with increased risk of type 2 diabetes mellitus, hypertension, dyslipidaemia, obstructive sleep apnoea, osteoarthritis, and several malignancies, contributing to significant morbidity, premature mortality, and reduced quality of life.1–3 Beyond clinical consequences, obesity imposes a substantial economic burden on healthcare systems and society.4
In Malaysia, obesity prevalence has risen sharply over the past two decades. The National Health and Morbidity Survey (NHMS) 2019 reported that 33.7% of Malaysian adults were obese, and a further 32.3% were overweight using Asian body mass index (BMI) cut-offs.5 Obesity prevalence increases with age and is evident across urban and rural populations. Data from the Malaysian Cohort study, involving more than 100,000 multiethnic participants, demonstrated a baseline obesity prevalence of approximately 17.7%, highlighting the magnitude of the problem at a national level.6
Lifestyle modification remains the cornerstone of obesity management; however, long-term effectiveness is limited, with high rates of weight regain observed in real-world settings.7 Access to pharmacotherapy and bariatric surgery remains limited by multiple factors, including stringent eligibility criteria, perioperative risk in patients with significant comorbidities, cost constraints, and limited availability of specialised surgical services in certain regions.8 These barriers contribute to a therapeutic gap between conservative management and definitive surgical intervention, particularly in resource-variable healthcare systems.
Intragastric balloon (IGB) therapy is an established endoscopic or device-based intervention that induces weight loss through gastric space occupation, delayed gastric emptying, and enhanced satiety. Meta-analyses have demonstrated that IGB therapy produces greater short-term total body weight loss compared with lifestyle intervention alone.9–11 However, IGB is a temporary intervention, and the durability of weight loss after balloon removal is variable, underscoring the importance of structured follow-up and multidisciplinary support.12
Despite increasing utilization, there is limited published guidance on standardized multidisciplinary IGB care pathways tailored to Asian populations and resource-limited healthcare systems. Variability in patient selection, peri-procedural symptom control, nutritional management, and follow-up practices may compromise outcomes and safety.13 This paper describes the development of a standardized multidisciplinary intragastric balloon care pathway implemented in a tertiary Malaysian centre, providing a reproducible clinical practice framework applicable to similar settings.
Methods
Study Design and Scope
This manuscript describes the development and implementation of a standardized multidisciplinary intragastric balloon (IGB) care pathway in a tertiary academic medical centre in Malaysia. The pathway was designed as a clinical practice framework to guide patient selection, peri-procedural management, nutritional support, adverse event monitoring, and structured follow-up for patients undergoing IGB therapy. This work does not involve collection or analysis of individual patient-level data and does not report clinical outcomes.
Rationale for Pathway Development
The care pathway was developed in response to increasing utilisation of IGB therapy and observed variability in routine clinical practice, particularly in patient selection, peri-procedural symptom management, nutritional adequacy during early intolerance, and consistency of follow-up. The aim was to establish a reproducible and pragmatic framework that could improve safety, standardisation, and multidisciplinary coordination while remaining adaptable to local resource availability and patient needs.
Evidence-Informed Framework and Local Adaptation
The care pathway was developed through a combination of targeted literature review, adaptation of international guideline recommendations, and expert consensus within the multidisciplinary team. Iterative refinement was performed based on institutional clinical experience and feasibility within the local healthcare setting. Particular consideration was given to Asian population characteristics, including lower body mass index thresholds associated with metabolic risk, and to the operational realities of a public tertiary care setting. The framework integrates evidence-based concepts while allowing flexibility in device selection and nutritional formulations based on availability and patient-specific factors.
Multidisciplinary Team Structure
The pathway is delivered through a coordinated multidisciplinary team comprising surgeons and/or endoscopists responsible for patient assessment, procedural planning, and complication management; dietitians responsible for nutritional counseling, structured oral nutritional support, and tolerance monitoring; and nursing or clinic coordination staff responsible for appointment scheduling, patient education, and early symptom triage. Anaesthesia support is involved for selected patients based on clinical risk and procedural requirements.
Patient Assessment and Selection
Patients considered for IGB therapy undergo comprehensive clinical assessment, including measurement of anthropometric parameters, evaluation of obesity-related comorbidities, review of previous weight management attempts, and assessment of readiness for structured follow-up. Indications and contraindications are assessed systematically to ensure patient safety and appropriateness of therapy. Patient counseling emphasises expected weight loss, the temporary nature of IGB therapy, common early intolerance symptoms, and the importance of long-term lifestyle modification following balloon removal.
Peri-Procedural Management
Peri-procedural management includes a standardized pharmacological strategy aimed at reducing early gastrointestinal intolerance and preventing dehydration. This typically includes acid suppression, antiemetic therapy, antispasmodic agents, and supportive medications as clinically indicated. Patients are provided with clear instructions regarding medication use and red-flag symptoms requiring urgent medical attention.
Nutritional Support Pathway
A structured dietitian-led nutritional support pathway is implemented immediately following IGB placement to mitigate risks of inadequate oral intake, protein deficiency, dehydration, and constipation during the early post-procedural period. Oral nutritional supplementation strategies are individualized based on patient tolerance, metabolic comorbidities such as diabetes, and resource availability, with reassessment and adjustment during follow-up visits.
Follow-Up and Monitoring
Patients are reviewed in a structured follow-up schedule at two weeks, four months, eight months, and one year following IGB placement. Follow-up visits focus on symptom assessment, nutritional adequacy, weight trajectory, complication surveillance, and reinforcement of behavioural and lifestyle interventions. Additional interim reviews are arranged when clinically indicated.
Ethical Considerations
Ethical approval was not required for this manuscript as it describes a clinical practice framework and does not involve research on human participants or analysis of identifiable patient data.
Multidisciplinary Intragastric Balloon Care Pathway
Overview of the Care Pathway
The intragastric balloon (IGB) care pathway was developed to provide a standardized, multidisciplinary framework for the delivery of IGB therapy in a tertiary Malaysian centre (Figure 1). The pathway integrates patient selection, peri-procedural management, nutritional support, adverse event surveillance, and structured follow-up, recognizing obesity as a chronic disease requiring coordinated long-term management rather than a single procedural intervention. The primary objective of this pathway is to improve consistency of care, enhance patient safety, and optimise tolerability and adherence throughout the IGB treatment course.
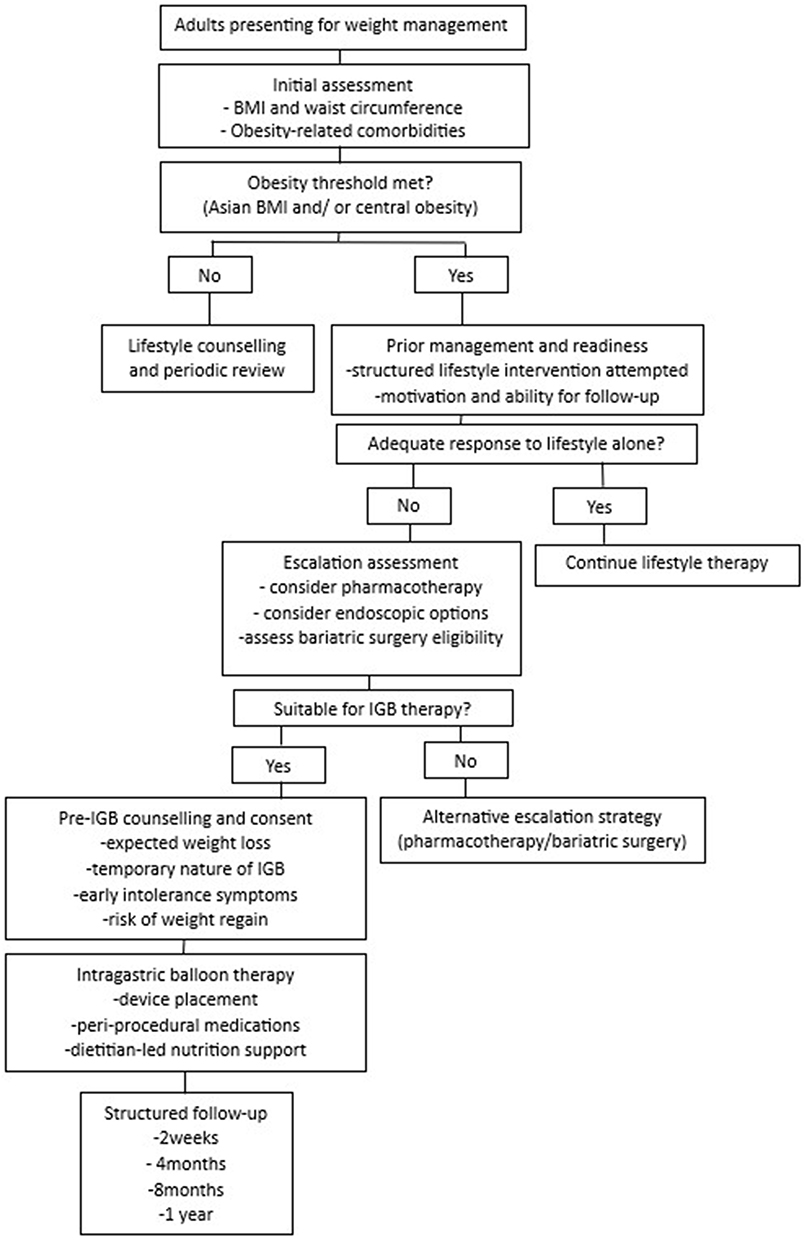 |
Figure 1 Assessment and selection algorithm for adult obesity and escalation to intragastric balloon therapy. This author-developed algorithm outlines a structured approach to the assessment of adults presenting for weight management, incorporating anthropometric evaluation, assessment of obesity-related comorbidities, prior response to lifestyle intervention, and readiness for treatment escalation. Patients meeting obesity thresholds who fail to achieve adequate weight loss with lifestyle measures alone undergo further evaluation for escalation strategies, including pharmacotherapy, intragastric balloon therapy, or bariatric surgery where appropriate. Intragastric balloon therapy is positioned as a minimally invasive, time-limited intervention delivered within a multidisciplinary care pathway with structured follow-up and long-term weight management planning. The algorithm is intended to support clinical decision-making and does not replace individualized clinical judgment. |
Patient Assessment and Selection
All patients considered for IGB therapy undergo a comprehensive pre-procedural assessment. This includes documentation of anthropometric parameters such as body weight, body mass index, and waist circumference, alongside evaluation of obesity-related comorbidities, including type 2 diabetes mellitus, hypertension, dyslipidaemia, metabolic syndrome, and obstructive sleep apnoea. A detailed history of previous weight management attempts is obtained to ensure that lifestyle-based interventions have been appropriately trialled prior to escalation.5,8
Patient eligibility is assessed using locally adopted criteria consistent with Asian population considerations, recognizing the increased cardiometabolic risk at lower BMI thresholds.5,8 Candidates are typically adults who have failed to achieve or maintain clinically meaningful weight loss with lifestyle modification alone and who are willing to engage in structured follow-up. Contraindications to IGB therapy, including prior major upper gastrointestinal surgery, active gastrointestinal pathology, significant coagulopathy, pregnancy, or inability to comply with follow-up requirements, are systematically excluded.9,13
A critical component of the assessment process is patient counseling. Patients are counselled regarding the expected magnitude of weight loss, the temporary nature of IGB therapy, the likelihood of early gastrointestinal intolerance, and the risk of weight regain following balloon removal if long-term lifestyle and behavioural changes are not sustained.12
Device and Procedural Considerations
The pathway accommodates the use of different IGB devices depending on institutional availability and patient suitability, including both endoscopically placed and swallowable balloon systems. Available intragastric balloon devices differ in placement technique (endoscopic versus swallowable systems), volume capacity, duration of implantation, and requirement for anaesthesia support. Device selection in this pathway is guided by patient-specific factors, including tolerance for endoscopy, comorbidity profile, anticipated adherence, and resource availability. While device-specific technical considerations may vary, the care pathway standardises all surrounding clinical processes, including patient preparation, symptom management, nutritional support, and follow-up. This approach allows flexibility in device selection while maintaining consistency in patient care delivery.9,13
Procedures are performed by trained bariatric surgeons in an appropriate clinical setting. Anaesthesia support is considered for patients with increased procedural risk, anticipated airway difficulty, severe obesity, or when endoscopic balloon placement is required. In contrast, swallowable balloon systems may be performed without sedation in carefully selected low-risk patients, improving accessibility in resource-variable settings.
Peri-Procedural Pharmacological Management
Early gastrointestinal intolerance following IGB placement is common and represents a major determinant of patient comfort and continuation of therapy.9,11 To mitigate these effects, the pathway incorporates a structured peri-procedural pharmacological strategy aimed at reducing nausea, vomiting, abdominal discomfort, and reflux. A summary of the suggested peri-procedural pharmacological regimen used to reduce early gastrointestinal intolerance and related symptoms is outlined in Table 1.
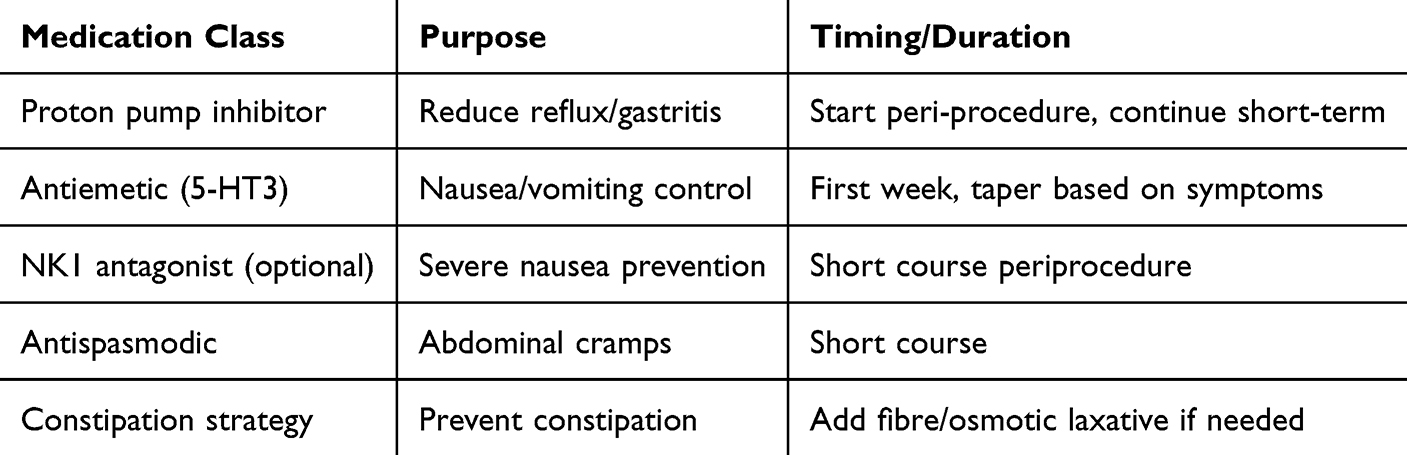 |
Table 1 Suggested Peri-Procedural Medication Regimen for Symptom Prevention and Early Intolerance Management |
The pharmacological strategies described are based on a combination of published evidence and institutional clinical practice, reflecting commonly adopted approaches for mitigating early gastrointestinal intolerance associated with intragastric balloon therapy.
Patients are commenced on acid suppression therapy to minimise gastric irritation and reflux symptoms. Antiemetic agents are prescribed prophylactically during the initial post-procedural period, with escalation strategies available for patients experiencing persistent symptoms. Antispasmodic medications may be used to alleviate abdominal cramping. Patients receive clear instructions regarding medication adherence and are educated on warning symptoms that warrant prompt medical review, such as persistent vomiting, inability to tolerate oral intake, severe abdominal pain, or gastrointestinal bleeding.10,11
Post-Procedural Nutritional Support
Nutritional management is a central component of the IGB care pathway, particularly during the early post-procedural phase when oral intake is frequently limited by nausea, vomiting, and early satiety. Reduced intake during this period increases the risk of dehydration, protein deficiency, and constipation if not proactively addressed.13,14 The structured early oral nutritional support framework implemented during the first two weeks following intragastric balloon placement is summarised in Table 2.
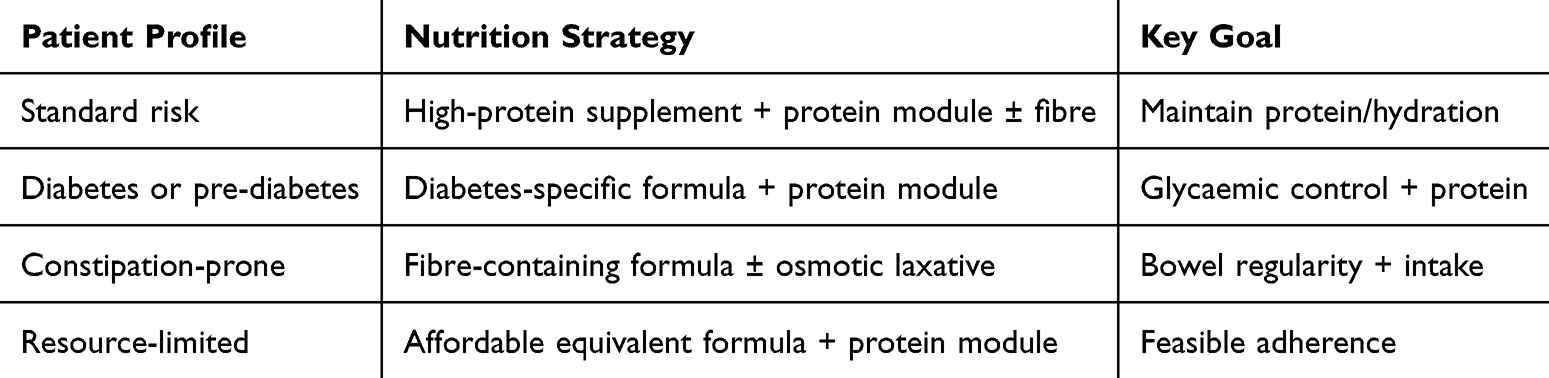 |
Table 2 Structured Early Oral Nutritional Support Framework (First 2 Weeks Post-IGB) |
The pathway incorporates dietitian-led structured nutritional support to mitigate these risks. Immediately following balloon placement, patients commence oral nutritional supplementation tailored to their metabolic profile, tolerance, and resource availability. Nutritional strategies are designed to ensure adequate protein intake while maintaining hydration and minimising gastrointestinal discomfort. Patients with diabetes or impaired glycaemic control are offered diabetes-specific nutritional formulations, while fibre-containing options or adjunctive agents may be used for patients prone to constipation.14 The initial supplementation phase is typically continued for approximately two weeks, after which patients are reassessed by a dietitian and the nutritional plan is adjusted based on tolerance, intake adequacy, and clinical progress. Following the initial two-week supplementation phase, patients are gradually transitioned to a structured solid diet under dietitian supervision, with emphasis on adequate protein intake, portion control, and behavioural modification to support sustained weight loss.
Adverse Event Monitoring and Safety Considerations
Patients are informed that mild to moderate gastrointestinal symptoms are common during the initial period following IGB placement and usually improve with time and supportive management.9–11 The pathway includes clear guidance on monitoring symptom severity and duration, as well as defined thresholds for escalation of care.
Symptoms suggestive of complications include persistent or severe abdominal pain, inability to tolerate oral intake beyond the expected adaptation period, gastrointestinal bleeding, progressive abdominal distension suggestive of balloon hyperinflation, and signs of bowel obstruction that may indicate balloon migration.
Serious adverse events associated with IGB therapy are rare but potentially serious. These include balloon migration, gastric or oesophageal injury or perforation, ulceration, spontaneous balloon hyperinflation, and acute pancreatitis.9–11 Patients receive explicit instructions on red-flag symptoms and are provided with direct access pathways for urgent clinical assessment should concerning symptoms arise. Strict adherence to recommended balloon duration is emphasised to minimise device-related complications.11
In resource-limited settings, early recognition and timely referral to centres with endoscopic or surgical capability are critical for managing serious complications. Where immediate intervention is not available, initial stabilisation with fluid resuscitation, symptom control, and expedited transfer should be prioritised.
Follow-Up and Long-Term Planning
Structured follow-up is a core element of the care pathway. Patients are routinely reviewed at two weeks following IGB placement to assess symptom control, medication adherence, hydration status, and nutritional adequacy. Subsequent reviews are scheduled at four months, eight months, and one year to monitor weight trajectory, screen for complications, and reinforce behavioural and lifestyle interventions.
Each follow-up visit has defined clinical objectives. The 2-week review focuses on early intolerance and nutritional adequacy; the 4-month review assesses weight response and dietary adherence; the 8-month visit evaluates readiness for balloon removal and long-term strategy planning; and the 1-year follow-up assesses weight maintenance and need for adjunct therapies.
Follow-up milestone is led by a designated member of the multidisciplinary team. The 2-week review is typically coordinated by the surgical team with input from dietitians, focusing on early symptom control, hydration status, and medication adherence. The 4-month visit emphasises dietitian-led nutritional optimisation and behavioural reinforcement. The 8-month review involves reassessment by both surgical and dietetic teams to evaluate weight trajectory, tolerance, and preparation for balloon removal where applicable. The 1-year follow-up focuses on long-term weight maintenance strategies, including consideration of adjunct pharmacotherapy or escalation to bariatric surgery where appropriate.
Balloon removal is typically recommended within 6 to 12 months depending on device specifications to minimise complication risk. In Asian populations, IGB therapy may be considered at lower BMI thresholds (≥27.5 kg/m2 with comorbidities or ≥30 kg/m2 without) in line with regional metabolic risk profiles.
The pathway explicitly positions IGB therapy as part of a broader chronic disease management strategy. Weight regain following balloon removal is a recognised limitation of IGB therapy, highlighting the importance of sustained lifestyle modification and, where appropriate, adjunct pharmacotherapy or bariatric surgery for eligible patients.12,15
Discussion
This manuscript presents a structured multidisciplinary intragastric balloon care pathway developed for routine clinical practice in a tertiary Malaysian centre. While the efficacy and safety of IGB therapy are well documented, outcomes in real-world settings are highly dependent on patient selection, early intolerance management, nutritional adequacy, and continuity of follow-up.9–12
A key strength of this pathway is the emphasis on standardized patient selection and counseling. Asian populations develop metabolic complications at lower BMI thresholds compared with Western populations, supporting the use of lower BMI cut-offs for intervention as adopted in Malaysian clinical practice guidelines.5,8 Clear expectation-setting regarding the temporary nature of IGB therapy and the risk of weight regain after removal is essential to align patient goals and reduce dissatisfaction.12
The proposed framework aligns with key principles outlined in international bariatric and endoscopic guidelines, including structured patient selection, multidisciplinary care, and defined follow-up pathways. However, adaptations were made to reflect local healthcare resource availability and population-specific considerations, particularly the use of lower BMI thresholds in Asian populations, where cardiometabolic risk occurs at lower levels of adiposity.
Early gastrointestinal intolerance is common following balloon placement and represents a major cause of early balloon removal.10,11 Prophylactic pharmacotherapy using acid suppression, antiemetics, and antispasmodics has been shown to reduce symptom severity and improve tolerability, supporting the inclusion of a standardized peri-procedural medication regimen in this pathway.11
Nutritional compromise during the early post-procedural period is another critical but under-recognised issue. Reduced intake, vomiting, and early satiety increase the risk of dehydration, protein deficiency, and constipation.13,14 Dietitian-led structured oral nutritional supplementation, as incorporated in this protocol, aims to mitigate these risks while maintaining flexibility based on patient comorbidities, tolerance, and resource availability.
Serious adverse events associated with IGB therapy, including balloon migration, gastric perforation, spontaneous hyperinflation, and acute pancreatitis, are rare but potentially life-threatening.9,10 Structured patient education, defined red-flag symptoms, and timely access to endoscopic or surgical care are essential safety components of any IGB programme.
Weight regain following balloon removal remains a significant limitation of IGB therapy. Long-term studies demonstrate diminishing differences between IGB-treated patients and lifestyle-only cohorts over time.12 This underscores the importance of positioning IGB as part of a chronic disease management strategy rather than a standalone intervention. Integration with lifestyle modification, pharmacotherapy, or bariatric surgery where appropriate is crucial for sustained benefit.8,15
The proposed care pathway has been implemented in our institution since 2021, during which time it has been applied in routine clinical practice for patients undergoing intragastric balloon therapy. Although formal outcome analysis was not performed as part of this manuscript, preliminary institutional observations suggest improved consistency in early symptom management, enhanced patient adherence to follow-up, and a perceived reduction in premature balloon removal due to intolerance. These observations remain hypothesis-generating and require validation in prospective outcome-based studies.
The framework described in this paper is pragmatic and scalable, utilising commonly available medications and nutritional supplements, and clearly delineating multidisciplinary roles. Although this manuscript does not report patient outcome data, it provides a structured template that may reduce practice variability and enhance safety and care quality in centres offering IGB therapy. Future prospective studies evaluating clinical outcomes using this pathway are warranted.
This study has several limitations. First, it does not include patient-level outcome data, limiting evaluation of the real-world effectiveness of the proposed pathway. Second, the framework is based partly on institutional practice and expert consensus, which may affect generalisability. Third, implementation feasibility may vary across healthcare settings with differing resource availability. Future prospective studies are required to validate clinical outcomes and assess the impact of this pathway on safety, tolerability, and long-term weight management.
Conclusion
A standardized multidisciplinary intragastric balloon care pathway provides a structured approach to delivering IGB therapy in routine clinical practice. While this framework aims to improve consistency, safety, and patient support, its clinical effectiveness requires validation through prospective outcome-based studies. It may serve as a practical and reproducible reference for centres developing endobariatric services in similar healthcare settings.
Ethics Approval and Consent to Participate
Not applicable. This manuscript describes a clinical practice framework/care pathway and does not report patient-level data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No source of funding.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Obesity and Overweight. Geneva: WHO; 2024.
2. Blüher M. Obesity: global epidemiology and pathogenesis. Nat Rev Endocrinol. 2019;15(5):288–9. doi:10.1038/s41574-019-0176-8
3. Bray GA, Kim KK, Wilding JPH. Obesity: a chronic relapsing progressive disease process. Obes Rev. 2017;18(7):715–723. doi:10.1111/obr.12551
4. Tremmel M, Gerdtham UG, Nilsson PM, Saha S. Economic burden of obesity: a systematic literature review. Int J Environ Res Public Health. 2017;14(4):435. doi:10.3390/ijerph14040435
5. Institute for Public Health (IPH). National Health and Morbidity Survey (NHMS) 2019: Non-Communicable Diseases, Healthcare Demand and Health Literacy. Ministry of Health Malaysia; 2020.
6. Jamal R, Syed Zakaria SZ, Kamaruddin MA, et al. Cohort profile: The Malaysian Cohort (TMC) project. Int J Epidemiol. 2015;44(2):423–431. doi:10.1093/ije/dyu089
7. Mann T, Tomiyama AJ, Westling E, Lew AM, Samuels B, Chatman J. Medicare’s search for effective obesity treatments: diets are not the answer. Am Psychol. 2007;62(3):220–233. doi:10.1037/0003-066X.62.3.220
8. Ministry of Health Malaysia. Clinical Practice Guidelines: Management of Obesity (Second Edition). Putrajaya: MOH; 2023.
9. Imaz I, Martínez-Cervell C, García-álvarez EE, Sendra-Gutiérrez JM, González-Enríquez J. Safety and effectiveness of the intragastric balloon for obesity. Obes Surg. 2008;18(7):841–846. doi:10.1007/s11695-007-9331-8
10. Ponce J, Woodman G, Swain J, et al. The REDUCE pivotal trial: a randomized sham-controlled study of the Orbera intragastric balloon. Obesity. 2015;23(11):2277–2283.
11. Gaur S, Levy S, Mathus-Vliegen L, et al. Balloon-related adverse events in intragastric balloon therapy: a systematic review. Gastrointest Endosc. 2019;89(6):1110–1121.
12. Mathus-Vliegen EMH, Tytgat GNJ. Intragastric balloon for treatment-resistant obesity: safety, tolerance, and efficacy of 1-year balloon treatment followed by a 1-year balloon-free follow-up. Gastrointest Endosc. 2005;61(1):19–27. doi:10.1016/S0016-5107(04)02406-X
13. ASGE Bariatric Endoscopy Task Force. Endoscopic bariatric therapies. Gastrointest Endosc. 2015;81(5):1073–1086. doi:10.1016/j.gie.2015.02.023
14. Mechanick JI, Apovian C, Brethauer S, et al. Clinical practice guidelines for perioperative nutrition, metabolic, and nonsurgical support of patients undergoing bariatric procedures. Obesity. 2020;28(4):O1–O58. doi:10.1002/oby.22719
15. Rubino F, Puhl RM, Cummings DE, et al. Joint international consensus statement for ending stigma of obesity. Nat Med. 2020;26(4):485–497. doi:10.1038/s41591-020-0803-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Influence of the Brain-Derived Neurotrophic Factor Gene Polymorphism on Weight Loss Following Intragastric Balloon Intervention: A Cross-Sectional Study
Al-Serri A, Al-Janahi HA, Jamal MH, AlTarrah D, Ziyab AH, Al-Bustan SA
Diabetes, Metabolic Syndrome and Obesity 2024, 17:4299-4306
Published Date: 19 November 2024
Long-Term Clinical Outcomes and Cost-Effectiveness of Bariatric Surgery for Type 2 Diabetes in Malaysia: A 10-Year Retrospective Cohort Study
Galvan JAA, Loo GH, Kosai NR, Yeong CH, Chinna K, Nordin RB, Lee KKC, Mustafa N
Journal of Multidisciplinary Healthcare 2026, 19:590099
Published Date: 8 July 2026