Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
A Multicenter Retrospective Study: Impact of First-Line Treatment Strategies on second-Line Efficacy and Safety of Regorafenib with or Without PD-1 Inhibitors in Unresectable Hepatocellular Carcinoma
Authors Ma W, Li Y, Lu Y, Liang Z, Yu H, Han J, Liu J ![]() , Wang W, Peng C, Cheng J
, Wang W, Peng C, Cheng J
Received 7 May 2025
Accepted for publication 12 August 2025
Published 16 September 2025 Volume 2025:12 Pages 2123—2137
DOI https://doi.org/10.2147/JHC.S456712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David Gerber
Weihong Ma,1,2,* Yinyin Li,1,* Yinying Lu,1,2 Zhipeng Liang,3 Hongli Yu,1,2 Jie Han,1,2 Jiaqi Liu,1,2 Wenjing Wang,1,2 Caiyun Peng,1 Jiamin Cheng1
1Senior Department of Hepatology, The 5th Medical Center of the PLA General Hospital, Beijing, People’s Republic of China; 2Chinese PLA Medical School, Beijing, People’s Republic of China; 3Guizhou Medical University, Guizhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiamin Cheng, Email [email protected] Caiyun Peng, Email [email protected]
Purpose: Amid the era of targeted-immunotherapy for hepatocellular carcinoma (HCC), the selection of second-line therapy following failure of diverse first-line regimens remains inadequately explored. This multicenter study aimed to assess how first-line treatment strategies impact the efficacy and safety of second-line regorafenib—either alone or in combination with PD-1 inhibitors—in patients with unresectable HCC (uHCC). Specifically, we focused on two key populations: patients who failed first-line tyrosine kinase inhibitor (TKI) monotherapy, and a rapidly expanding cohort who progressed after first-line TKI plus PD-1 inhibitor combination therapy, and to address the critical clinical dilemma of whether to continue immunotherapy in the second line.
Patients and Methods: This retrospective study enrolled 288 uHCC patients from five centers, stratified into two cohorts based on first-line therapy: 126 patients with first-line TKI monotherapy (Pre-Monotherapy cohort) and 162 with first-line TKI+PD-1 combination therapy (Pre-Combination cohort). All received second-line regorafenib alone or with PD-1 inhibitors. Primary endpoints were overall survival (OS) and progression-free survival (PFS); secondary endpoints included progression-free survival (PFS),objective response rate (ORR), disease control rate (DCR), and safety.
Results: In the Pre-Monotherapy cohort, regorafenib plus PD-1 significantly improved outcomes versus regorafenib alone: mPFS (10.5 vs 4.7 months, p< 0.001), mOS (18.9 vs 14.0 months, p=0.003), ORR (29.69% vs 4.84%, p< 0.001), and DCR (89.06% vs 67.74%, p=0.004). In the Pre-Combination cohort, no significant differences were observed in PFS (9.2 vs 6.3 months, p=0.062), OS (16.2 vs 13.2 months, p=0.13), ORR (22.33% vs 15.25%, p=0.276), or DCR (82.52% vs 74.58%, p=0.227).
Conclusion: Second-line regorafenib plus PD-1 inhibitors yields significant clinical benefits in uHCC patients who failed first-line TKI monotherapy. However, in those who progress following first-line TKI plus PD-1 inhibitor therapy, continuing immunotherapy in the second line confers no additional efficacy, underscoring the need to explore alternative strategies. This study provides the first evidence-based guidance for the unmet clinical scenario of “first-line targeted-immunotherapy failure”, highlighting the importance of precision sequential therapy tailored to first-line regimens.
Keywords: hepatocellular carcinoma, different first-line treatment, second-line treatment
Introduction
Hepatocellular carcinoma (HCC) is a common malignant tumor, ranking third in global cancer mortality, with its death rate expected to rise steadily over the next decade.1 Due to its stealthy pathogenesis, varied malignancy, and tendency to metastasize, many tumors are diagnosed at advanced stages. These patients have missed the chance for curative surgery and must depend on systemic therapy to extend their overall survival.2 In the past few years, sorafenib, lenvatinib, and donafenib, which are multi-kinase inhibitors, have been recognized as the primary targeted therapy for uHCC.3,4 The first-line systemic treatment of uHCC has entered a new era of targeted-immunotherapy combination, driven by the widespread clinical use of immune checkpoint inhibitors (ICIs) and significant advancements in Phase III clinical trials like IMbrave150, CARES-310, and LEAP-002.5–7 However, most patients still inevitably experience disease progression, underscoring an urgent need to optimize second-line treatment strategies—particularly as the population of patients failing first-line targeted-immunotherapy combination therapy is rapidly expanding.
As a novel oral multi-target kinase inhibitor, regorafenib is the first globally approved second-line standard treatment for uHCC patients who have not benefited from sorafenib therapy. Yet its modest survival benefit (mOS extension of ~2.8 months) highlights the need for more effective approaches.8 The integration of immune checkpoint inhibitors (ICIs) has emerged as a promising direction: Preclinical studies indicate that regorafenib inhibits the vascular endothelial growth factor receptor (VEGFR) and the JAK1/2-STAT1 and MAPK signaling pathways, while increasing PD-L1 expression in tumors. It also normalizes tumor vasculature, enhancing CD8+ T cell infiltration and thereby boosting the efficacy of PD-1 antibodies.9,10 The findings provide a robust theoretical basis for the concurrent application of regorafenib and PD-1 inhibitors. However, clinical evidence supporting this combination regimen has historically focused on patients with disease progression after first-line TKI monotherapy.11,12 While these studies have validated the efficacy of the regorafenib-PD-1 combination in this subgroup, they leave a critical gap: there is a paucity of relevant research on the cohort of patients who progress after first-line targeted-immunotherapy combinations (eg, TKI plus PD-1 inhibitors).
With the increasing adoption of targeted-immunotherapy combinations for liver cancer, a growing proportion of patients now receive TKI plus PD-1 inhibitor combinations as first-line therapy. This shift has created a pressing clinical dilemma: for patients who progress after first-line TKI plus PD-1 inhibitor therapy, does continuing immunotherapy in the second line confer benefit? Current clinical guidelines offer limited direction for this specific scenario. Although multiple studies have investigated regorafenib-based second-line regimens, none have systematically compared regorafenib monotherapy versus regorafenib-PD-1 inhibitor combinations—stratified by first-line treatment history. This represents a critical gap, given the substantial biological and therapeutic distinctions between failure after TKI monotherapy versus failure after combination therapy.
This study is the first to address this gap, evaluating the efficacy of second-line regorafenib (with or without PD-1 inhibitors) in two well-defined cohorts: patients failing first-line TKI monotherapy and those failing first-line TKI+PD-1 combination therapy. By focusing on the impact of first-line treatment strategies on second-line efficacy, we aim to validate the role of the regorafenib-PD-1 combination in patients failing first-line TKI monotherapy, clarify whether continuing immunotherapy benefits patients progressing after first-line combination therapy; and provide evidence-based guidance for personalized sequential therapy—ultimately filling a key knowledge gap in current HCC management.
Materials and Methods
Study Design and Patients
Between April 2019 and December 2023, we gathered demographic, clinical, and survival information from uHCC patients received regorafenib in combination with PD-1 inhibitors or regorafenib as second-line treatment after experiencing failure of first-line therapy at five leading medical institutions in China. This retrospective study was approved by the Institutional Ethics Committee on January 5, 2023 (approval number KY-2022-12-79-1). The study complied with the 2013 update of the Declaration of Helsinki principles and individual consent for this retrospective study was waived.
This study established two main cohorts based on different first-line treatment strategies, including the monotherapy cohort (Pre-Monotherapy) and the combination therapy cohort (Pre-Combination therapy). The first cohort comprised 126 patients who received TKI monotherapy as their initial treatment; The second group consisted of 162 patients who received combination therapy as their initial treatment. We assessed the effectiveness and safety of regorafenib alone compared to its combination with PD-1 inhibitors in each cohort.
The study included patients with histologically confirmed HCC per international guidelines,13–15 who had progressed after first-line therapy with TKI monotherapy (sorafenib/lenvatinib) or TKIs combined with a PD-1 inhibitor (Sintilimab/Pembrolizumab/Tislelizumab). Participants received regorafenib as a second-line treatment for at least one 28-day cycle, had Child-Pugh A or B liver function, an ECOG performance status of ≤2, and at least one measurable lesion according to the Modified Response Evaluation Criteria in Solid Tumors for HCC.16 Comprehensive CT/MRI and laboratory data were collected from treatment initiation until death or the study’s end on January 8, 2025.Exclusion criteria encompassed: (I) any current or past malignant tumors other than HCC; (II) concurrent administration of different targeted therapies with regorafenib as a second-line treatment; (III) Have serious underlying health problems, such as heart disease, lung disease, or kidney disease; (IV) incomplete or lost follow-up; (V) participation in other clinical intervention studies while on regorafenib.
Study Procedures
Following the failure of initial treatment, patients were allocated to receive either regorafenib with a PD-1 inhibitor or regorafenib alone, depending on their clinical condition, financial situation, and their doctor’s recommendation. The initial dosage of regorafenib was established at 80 to 160 mg, administered orally on a daily basis. This dosage was subsequently adjusted according to the patient’s tolerance level, with modifications made to ensure optimal tolerability. The treatment regimen involved a 3-week cycle, with patients receiving therapy for a total of 4 weeks, followed by a 1-week discontinuation period. The treating physician decides on dose adjustments or therapy discontinuation according to the type and severity of adverse events (AEs). In certain situations, the dose can be decreased to 80 mg daily, and in rare instances, it may be further reduced to 40 mg. The choice of PD-1 inhibitor is not limited to a specific brand, including sintilimab, Tislelizumab, and pembrolizumab, and the dose is administered every 3 weeks as directed by the manufacturer. Treatment was continued until the disease progression based on mRECIST criteria, clinical progression is observed (ECOG performance score of 3 or more or symptoms worsen), death, or if toxicity is deemed unacceptable Physicians may incorporate additional treatment modalities into the second-line regimen, including transarterial chemoembolization (TACE), hepatic arterial infusion chemotherapy (HAIC), radiation therapy, or optimal supportive care, as deemed appropriate.
The follow-up period length was calculated starting from the first day regorafenib was given. Patient baseline characteristics were gathered within a week before starting regorafenib treatment. The patient information gathered included the following: Gender, hepatitis B virus infection, Child-Pugh score, grade, ALBI score, BCLC stage, alpha-fetoprotein (AFP), albumin, total bilirubin, cirrhosis, ascites, macrovascular invasion, extrahepatic metastasis, lymph node metastasis, prior systemic treatment, prior local treatment. The localized approach for second-line therapy, the initial dosage of regorafenib, and other related factors. During the treatment phase, the efficacy of the treatment and adverse drug reactions should be evaluated once during each follow-up period according to the patient’s symptoms, vital signs, laboratory tests, and other measures. The present study was terminated on January 8, 2025.
Efficacy and Safety Analyses
To assess the long-term efficacy of later-line treatment, overall survival (OS) was chosen as the primary endpoint, measured from the initiation of regorafenib treatment to death or the latest follow-up. Secondary endpoints included progression-free survival (PFS), tumor objective response rate (ORR), disease control rate (DCR), and safety analysis. For tumour assessment, CT or MRI according to mRECIST was performed at baseline and every 2–3 months during follow-up. Two radiologists, each with over 15 years of experience, analyzed the image data. For patients with tumors in the liver and lesions outside it, CR (complete response) is defined as all lesions, both intrahepatic and extrahepatic, reaching CR, while PR (partial response) is defined as liver lesions reaching PR and extrahepatic lesions reaching CR or PR. SD (stable disease) was defined as the stability of intrahepatic lesions with concurrent CR, PR, or SD of extrahepatic lesions, or stability of extrahepatic lesions with concurrent CR, PR, or SD of intrahepatic lesions. Progressive disease (PD) was identified by its occurrence in either extrahepatic or intrahepatic lesions. Adverse events were assessed according to CTCAE version 5.0.17
Statistical Methods
Continuous variables are presented as mean ± SD or median (25th, 75th percentile), and categorical variables are expressed as counts with percentages. Baseline data for the two groups were analyzed using χ² or Fisher’s exact tests for categorical variables, and t-tests or Mann–Whitney U-tests for continuous variables. The χ²-test or Fisher’s test was employed to compare ORR, DCR, and AEs across the two groups. Univariate and multivariate Cox proportional regression analyses were performed to identify independent prognostic risk factors for survival, with findings presented as hazard ratios (HR) and 95% confidence intervals (CI). Multivariate analyses were performed on variables with a P value below 0.10 identified in the univariate analyses. Subgroup analysis employed the Cox regression model to compare PFS and OS between the groups across different variables, generating a forest plot with corresponding hazard ratios (HRs) and 95% confidence intervals (CIs). The stratified Log rank test was employed to compare OS and PFS, and the Kaplan-Meier method was utilized to estimate their respective curves. All tests were two-sided, with statistical significance set at P<0.05. Statistical analyses were conducted using R version 4.2.1.
Results
Study Patients and Baseline Characteristics
Between April 2019 and December 2023, 343 uHCC patients were enrolled in this study to receive regorafenib as a second-line treatment. According to the study protocol, 55 patients were excluded due to failure to meet the inclusion criteria. Ultimately, 288 eligible patients were included in this study (Figure 1). The cohort had an average age of 56 years, with 89.6% being male. All patients were infected with HBV or HCV, and most were at BCLC stage C (n=227, 79.1%). Most patients received interventional therapy as part of their first-line treatment (n=241, 83.7%), and a majority began regorafenib therapy at a 160 mg dose (n=191, 66.3%). Baseline demographic and clinical characteristics were similar between the two treatment groups in each cohort (Table 1). Furthermore, baseline characteristics were similar between the regorafenib and regorafenib-PD-1 groups in the overall population.(Supplementary Table S1).
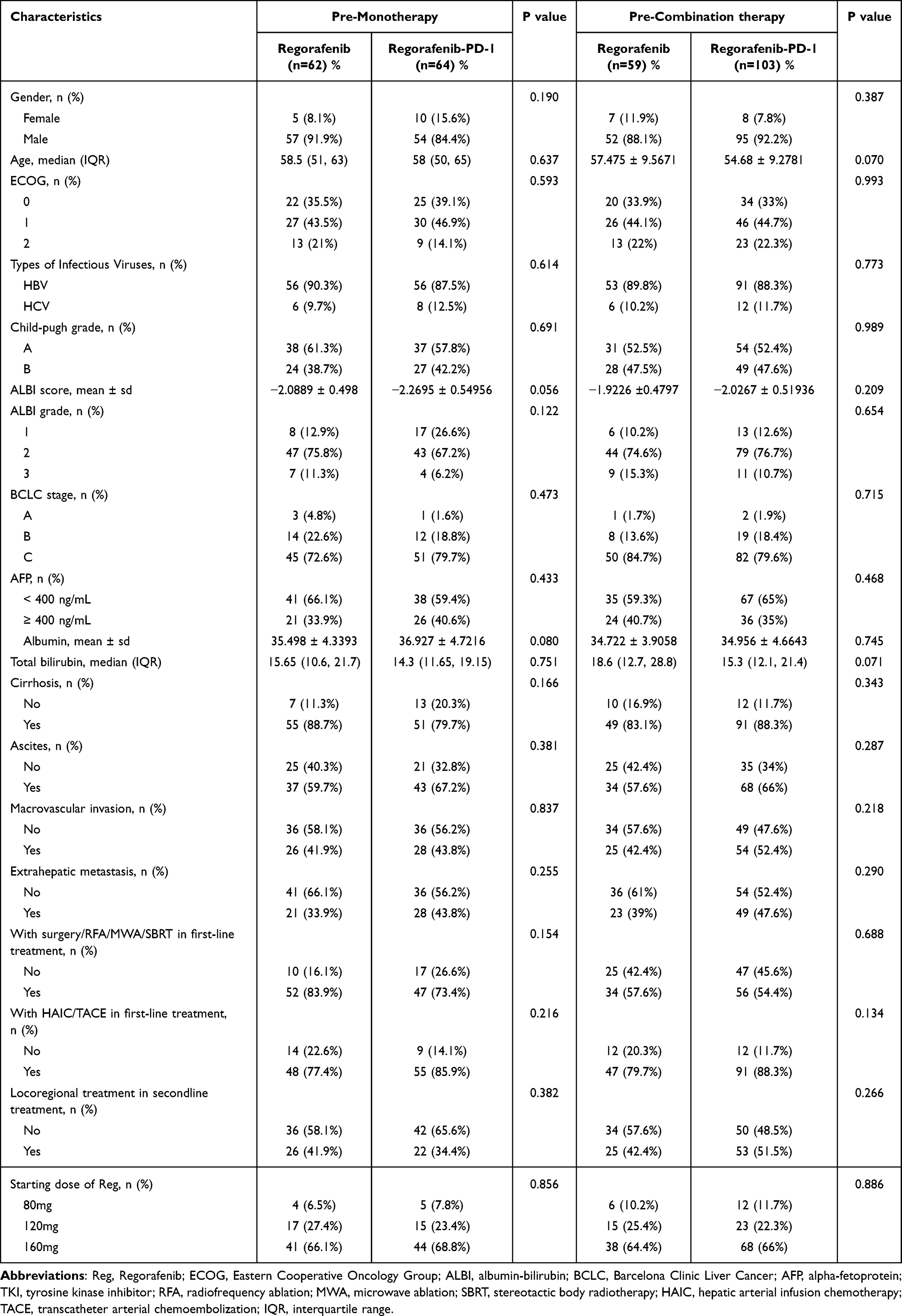 |
Table 1 Demographic and Clinical Characteristics of Patients at Second-Line Treatment Initiation |
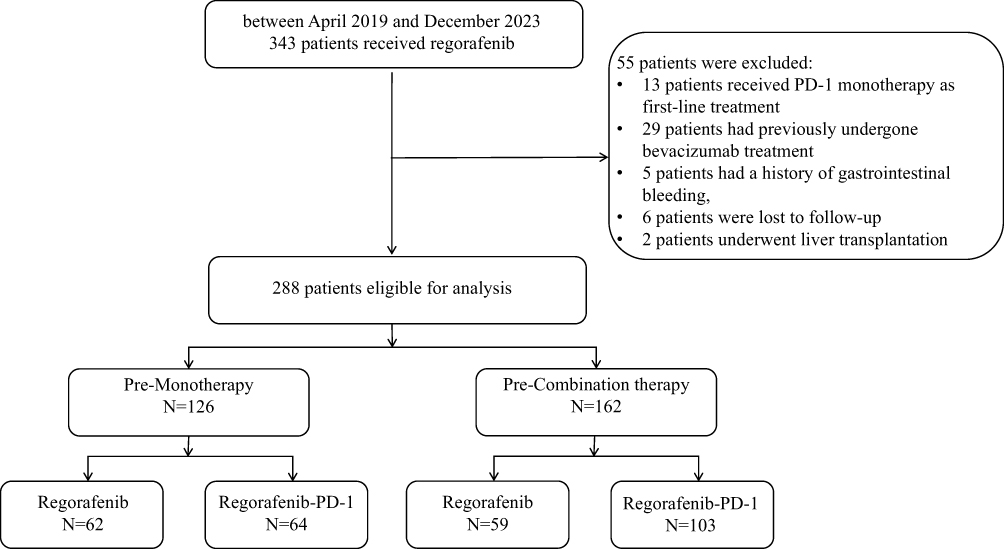 |
Figure 1 Flowchart of study population. |
Monotherapy Before Regorafenib
In the Pre-Monotherapy cohort, 62 patients (49.21%) received regorafenib and 64 patients (50.79%) received regorafenib-PD-1. A significant difference was observed in PFS and OS between the two groups (Figure 2). The regorafenib group had a median PFS of 4.7 months (95% CI, 4.4–7.4 months), compared to 10.5 months (95% CI, 7.4-?) in the other group. The median overall survival (mOS) was 14.0 months (95% CI, 12.0–17.3 months) for the regorafenib group and 18.9 months (95% CI, 15.8–27.5 months) for the Regorafenib-PD-1 group. In terms of efficacy, the objective response rate (ORR) was significantly higher in the regorafenib-PD-1 group at 29.69% compared to 4.84% in the regorafenib group (P<0.001). The DCR in the Regorafenib-PD-1 group was 89.06%, significantly higher than the 67.74% observed in the regorafenib group (P=0.004) (Table 2).
 |
Table 2 Treatment Responses in the Overall Cohort and Two Sub-Cohorts by mRECIST |
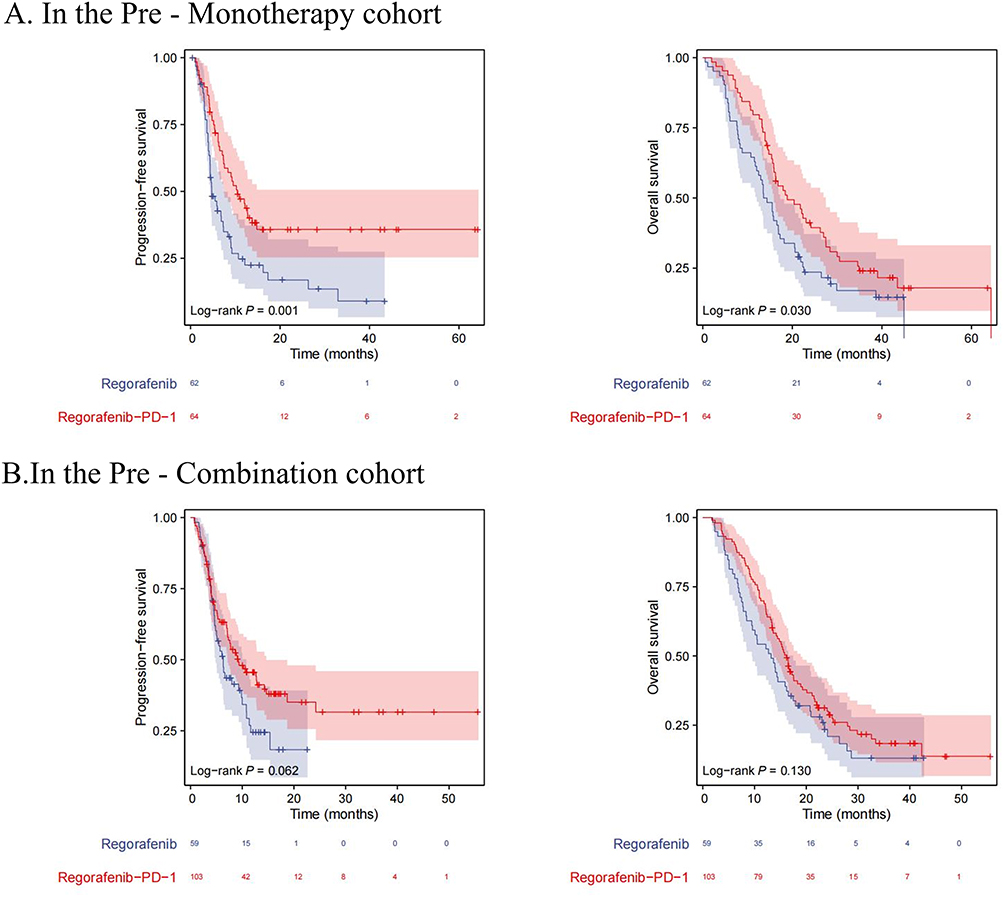 |
Figure 2 Illustrates progression-free and overall survival in both the Pre-Monotherapy cohort (A) and the Pre-Combination therapy cohort (B). |
Multivariate analysis identified regorafenib plus PD-1 as a second-line treatment (HR=0.422, 95% CI 0.268–0.665, p<0.001), male gender (HR=0.389, 95% CI 0.208–0.729, p=0.003), AFP levels ≥ 400 ng/mL (HR=1.712, 95% CI 1.072–2.732, p=0.024) and Total bilirubin (HR=1.012, 95% CI 1.005–1.019, p<0.001) as independent prognostic factors for PFS (Table 3). Furthermore, multivariate analysis revealed that regorafenib plus PD-1 treatment (HR=0.527, 95% CI: 0.345–0.807, p=0.003), Total bilirubin (HR=1.013, 95% CI 1.006–1.021, p<0.001) and BCLC C (HR=8.519, 95% CI: 1.158–62.670, p=0.035) were identified as independent prognostic factors for OS (Table 4).
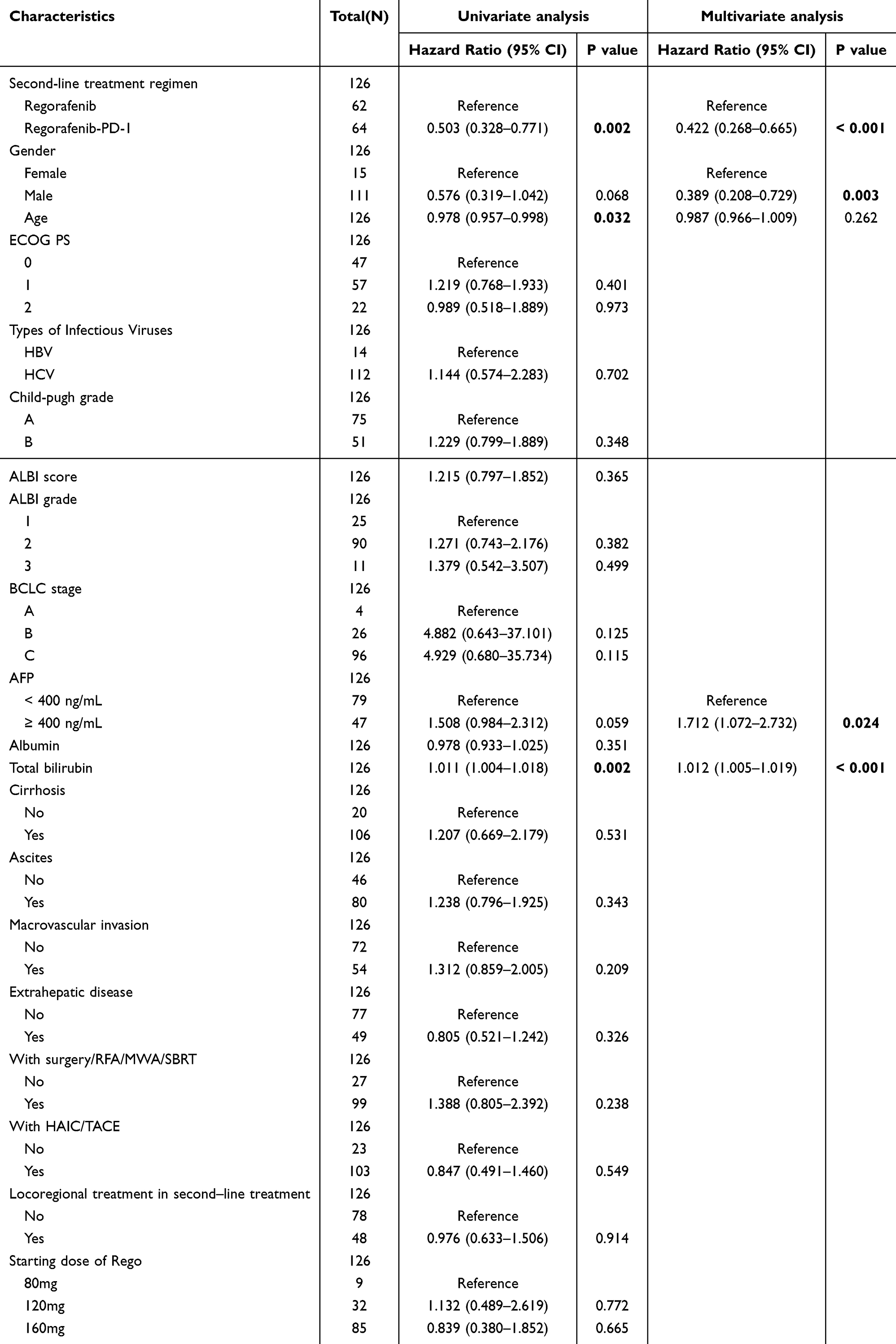 |
Table 3 Presents Both Univariate and Multivariate Analyses of Factors Linked to Progression-Free Survival (PFS) Within the Pre-Monotherapy Cohort |
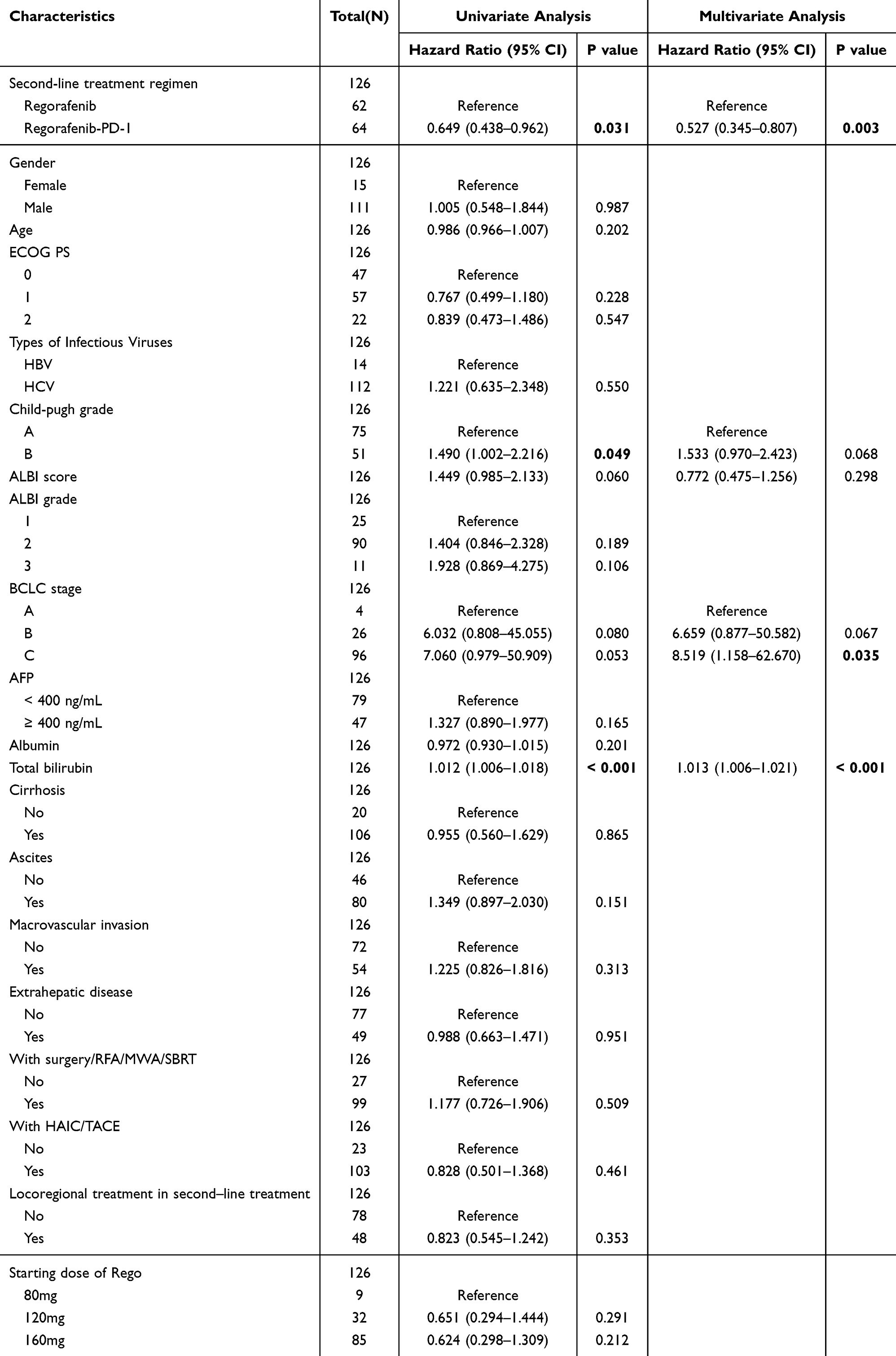 |
Table 4 Presents Both Univariate and Multivariate Analyses of Factors Linked to Overall Survival (OS) in the Pre-Monotherapy Cohort |
Subgroup analyses were conducted based on different clinical characteristics and treatment choices. The enhancement in PFS with regorafenib combined with PD-1 inhibitors was sustained across nearly all subgroups, except for those with BCLC stage B. In patients with BCLC stage B, the preference for local therapies in second-line treatment may account for the improved PFS observed with second-line monotherapy, despite the lack of significant difference in OS. We speculate that the choice of this treatment approach may have influenced the observed outcomes. A trend towards longer OS with regorafenib plus PD-1 compared to regorafenib monotherapy was observed across all subgroups (Figure 3).
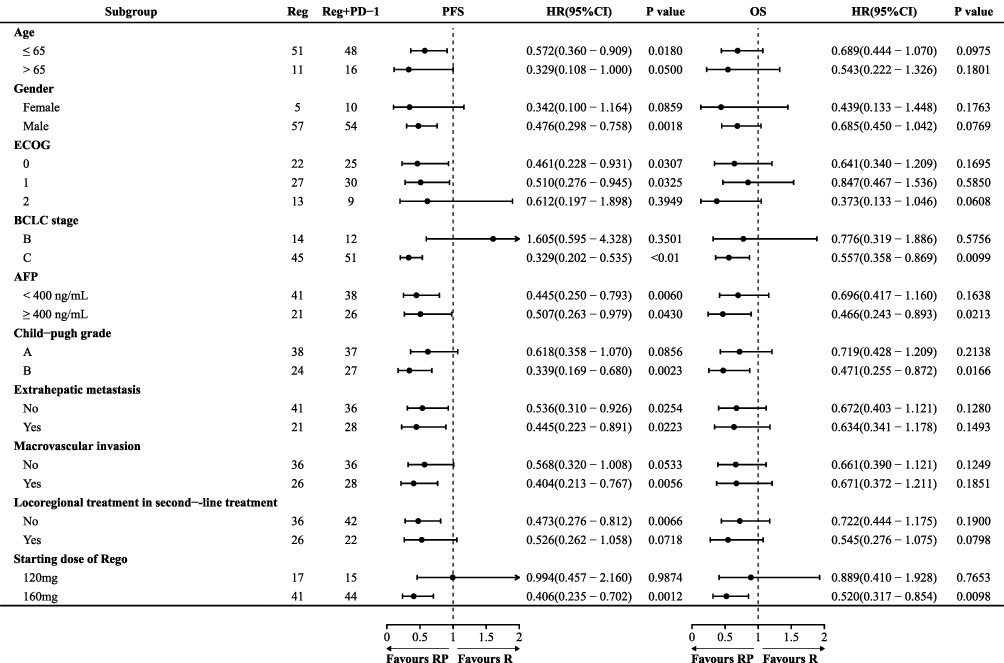 |
Figure 3 Presents a univariable Cox regression analysis for subgroups of patients in the Pre-Monotherapy cohort, comparing those treated with regorafenib alone to those receiving regorafenib combined with a PD-1 inhibitor. Reference, Reg group. |
Treatment-related adverse events (TRAEs) are shown in Table 5. The incidence of treatment-related adverse events (TRAEs) was higher in patients treated with regorafenib combined with a PD-1 inhibitor than in those receiving regorafenib alone (81.25% vs 58.06%, P=0.005). The occurrence of grade 3 or 4 TRAEs was comparable between the groups (20.31% vs 14.52%, P=0.392). In this cohort, the likelihood of developing pneumonitis and neutropenia was significantly higher in patients receiving regorafenib combined with PD-1 inhibitors than in those receiving regorafenib alone.
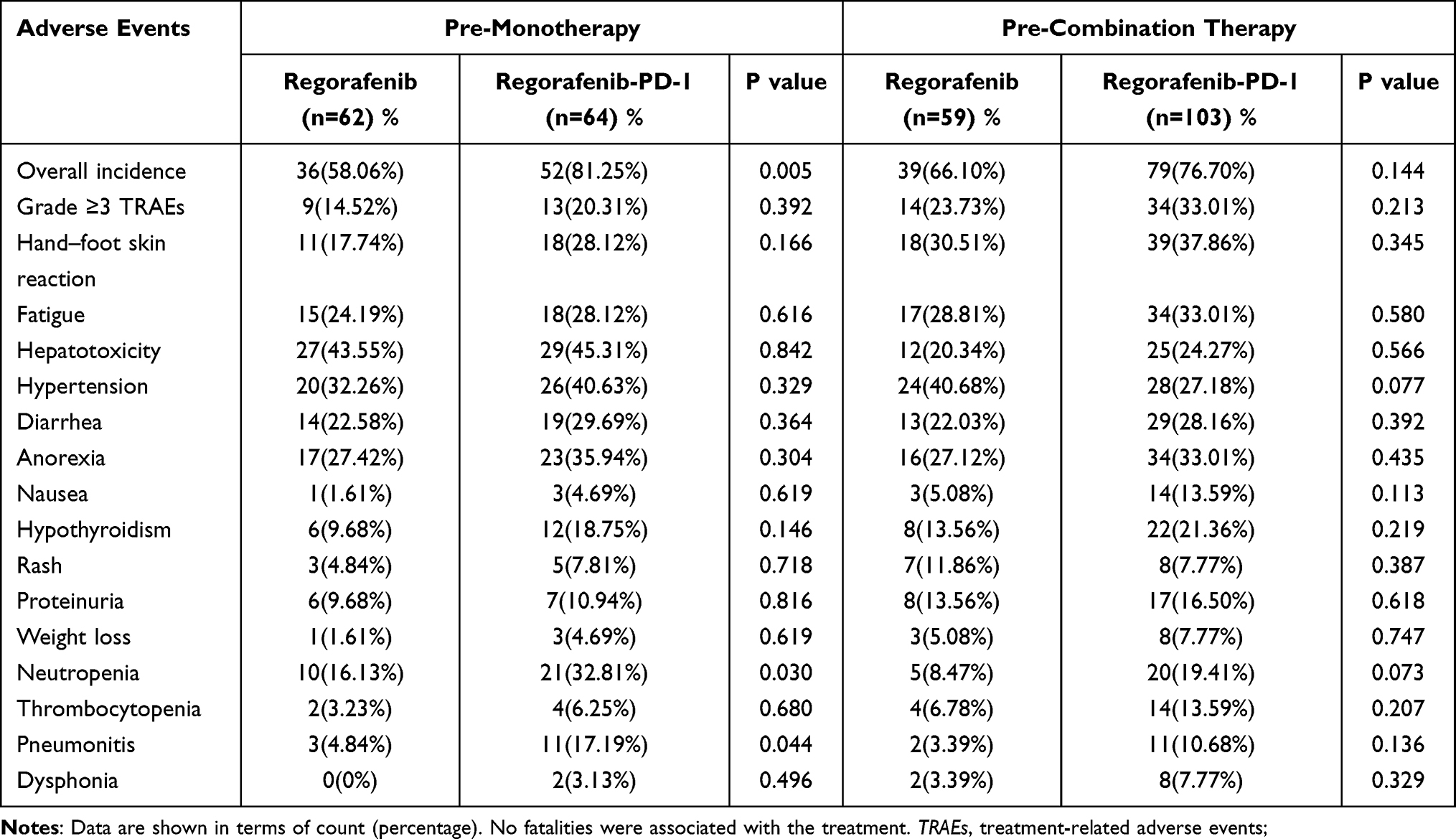 |
Table 5 TRAEs |
Combination Therapy Before Regorafenib
In the Pre-Combination therapy cohort, there were no significant differences in PFS, OS, ORR, and DCR between the groups. The mPFS was 6.3 months (95% CI, 4.8–10.8 months) for the regorafenib group and 9.2 months (95% CI, 7.2–14.7 months) for the Regorafenib-PD-1 group (P=0.062). The median overall survival (mOS) was 13.2 months for the regorafenib group and 16.2 months for the Regorafenib-PD-1 group (P=0.13) as shown in Figure 2. The objective response rate (ORR) was 22.33% in the Regorafenib-PD-1 group, marginally higher than the 15.25% observed in the regorafenib group (P=0.276). In addition, the DCR in the Regorafenib-PD-1 arm was 82.52%, which was also higher than in the regorafenib arm (82.52%vs.74.58%, P=0.227) (Table 2). Multivariate analysis identified the presence of ascites (HR=0.617, 95% CI 0.413–0.921, p=0.018) and the use of surgery/RFA/MWA/SBRT in first-line treatment (HR=0.563, 95% CI 0.378–0.840, p=0.005) as independent prognostic factors for PFS (Supplementary Table S2). In the multivariate analysis of OS, no independent prognostic factors with statistical significance were identified.
Subgroup analysis in this study cohort demonstrated a notable enhancement in overall survival (OS) for most subgroups treated with regorafenib and PD-1 inhibitors, except for patients over 65, those with an ECOG performance status of 2, individuals at BCLC stage B, and those who underwent locoregional treatment as second-line therapy (Figure 4). This finding may be due to elderly patients and those with poorer health being more prone to adverse events with long-term combination therapy. Furthermore, patients with BCLC stage B more frequently undergo local treatment options in second-line therapy, which could explain why the efficacy of regorafenib monotherapy is more pronounced in these specific subgroups.
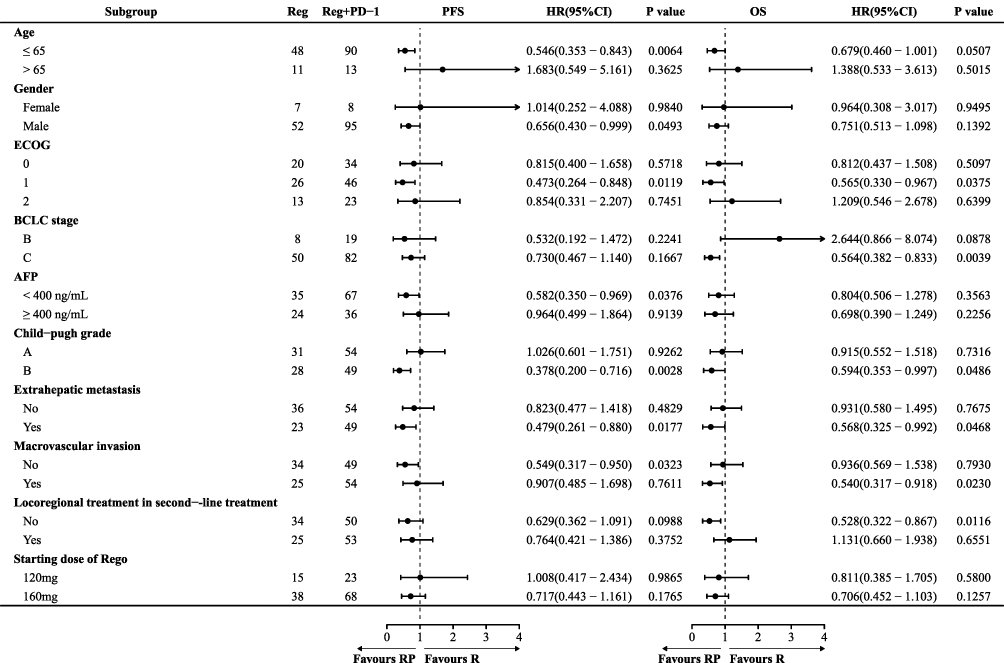 |
Figure 4 Presents a univariable Cox regression analysis of subgroups within the Pre-Combination therapy cohort, comparing patients treated with regorafenib monotherapy to those receiving regorafenib combined with a PD-1 inhibitor. Reference: Reg group. |
During the follow-up, no mortality linked to the treatment was observed. The occurrence of treatment-related adverse events and serious grade 3/4 reactions was comparable between the regorafenib and Regorafenib-PD-1 groups, with any grade events at 66.10% versus 76.70% (P=0.144) and grade 3/4 events at 23.73% versus 33.01% (P=0.213) (Table 5). There was no significant difference in the incidence of any grade or grade 3/4 TRAEs between the two groups. The incidences of any grade and grade 3/4 TRAEs were similar across the groups. In the regorafenib group, the most common TRAEs of any grade were hypertension (40.68%), hand-foot skin reaction (30.51%), and fatigue (28.81%).
Discussion
This study is the first to classify and evaluate second-line treatments for HCC based on first-line treatment patterns, thoroughly analyzing the efficacy and safety of regorafenib combined with PD-1 after the failure of different first-line therapies. Patients were categorized into two cohorts based on first-line treatment regimens: Pre-Monotherapy and Pre-Combination therapy. The findings indicated that in the Pre-Monotherapy group, combining regorafenib with a PD-1 inhibitor significantly enhanced patient outcomes compared to using regorafenib by itself. However, in the Pre-Combination therapy cohort, the efficacy of switching to regorafenib and continuing with immunotherapy was comparable to that of regorafenib alone. These findings indicate that the effectiveness and safety of second-line combination regimens can differ greatly based on the initial treatment method, underscoring the need for personalized second-line strategies in clinical practice tailored to patients’ first-line treatment history and disease characteristics.
Significant clinical benefits were observed in patients from the Pre-Monotherapy cohort who received regorafenib and PD-1 inhibitors in a second-line treatment setting. This finding further corroborates previous preclinical findings. Research has demonstrated that regorafenib enhances the recognition and elimination of cancer cells by natural killer (NK) cells by inhibiting the STAT3 signalling pathway and increasing the expression of NKG2D ligands.10,18 This, in turn, helps to overcome immunosuppression and boost antitumour immunity. Regorafenib has been shown to decrease tumor-associated macrophages (TAMs) and shift blood vessel polarization from the tumor-promoting M2 phenotype to the tumor-inhibiting M1 phenotype.19 Regorafenib enhances the antitumor immune response by promoting CD8+ T cell growth and activation through its effects on macrophages.9,20,21 Regorafenib stabilizes the tumor immune environment by targeting the colony-stimulating factor 1 receptor (CSF1R). This action decreases the number of macrophages that enter the tumor.22,23 Our research aligns with prior clinical studies, demonstrating that for patients with disease progression after sorafenib or lenvatinib treatment, second-line therapy with regorafenib combined with PD-1 inhibitors is more effective than regorafenib alone. These consistent discoveries further enhance the credibility and reliability of our research outcomes.24
In patients previously treated with first-line combination immunotherapy, regorafenib combined with PD-1 inhibitors showed no statistically significant efficacy difference compared to regorafenib alone in the second-line setting, although the combination therapy exhibited numerical advantages in ORR, DCR, mPFS, and mOS. The absence of notable differences between the two groups in the Pre-Combination therapy cohort may be partly due to some patients experiencing first-line therapy failure from T-cell exhaustion instead of TKI resistance, resulting in reduced effectiveness of PD-1 inhibitor rechallenge. For these patients, combining other agents such as CTLA-4 or TIGIT inhibitors with regorafenib might potentially enhance therapeutic outcomes. However, these hypotheses require further clinical studies to validate their efficacy and safety.
Nonetheless, this research has certain limitations. The study’s statistical power is weakened due to the limited number of included studies and the relatively small sample size. Secondly, all the studies are retrospective, which could result in selection bias. Future research will involve prospective, interventional studies with larger cohorts to validate the efficacy and safety of combining regorafenib with PD-1 inhibitors in patients unresponsive to different first-line therapies and undergoing second-line treatment. We aim to identify prognostic indicators and biomarkers influencing the efficacy of regorafenib combined with PD-1 treatment in advanced HCC patients, facilitating personalized and precise therapy for uHCC.
Conclusion
The combination of regorafenib and PD-1 may increase the effectiveness for uHCC patients who have not benefited from first-line TKI therapy. Administering regorafenib, either alone or with PD-1, as a second-line treatment after progression from first-line TKI and PD-1 therapy does not significantly affect efficacy. These findings indicate that combining regorafenib with PD-1 might not provide additional benefits for certain uHCC patient subgroups, influencing second-line treatment decisions.
Data Sharing Statement
The datasets generated and/or analyzed during the present study may be obtained from the corresponding authors, Caiyun Peng and Jiamin Cheng, upon reasonable request.
Institutional Review Board Statement
This retrospective conformed to the Declaration of Helsinki and was approved by Institutional Ethics Committee of the Fifth Medical Center of the People’s Liberation Army General Hospital on January 5, 2023 (approval number KY-2022-12-79-1). The study was conducted in accordance with the principles of the 2013 revised Declaration of Helsinki. As a retrospective study, it involved no biological sample collection or invasive interventions throughout the process, posing no anticipated harm to the subjects. Furthermore, stringent measures have been implemented to eliminate the risk of personal privacy disclosure. For these reasons, individual informed consent for this study was waived.
Acknowledgments
We are truly grateful to all the clinical physicians from the Hepatic Disease and Oncology Department of the Fifth Medical Center of the Chinese PLA General Hospital for their wholehearted support in collecting the clinical information of patients for this research. Additionally, we would like to extend our special thanks to Professor Ji Dong for his meticulous guidance and invaluable suggestions during the research design and manuscript preparation process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (NO. 82272956).
Disclosure
The authors declare no conflicts of interest.
The abstract of this article was presented as a poster at the 2025 ASCO Annual Meeting, which included interim study results. This poster abstract was published in the “Poster Abstracts” section of Journal of Clinical Oncology.
The hyperlink is: https://ascopubs.org/doi/10.1200/JCO.2025.43.16_suppl.4088
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. Zeng H, Chen W, Zheng R, et al. Changing cancer survival in China during 2003-15: a pooled analysis of 17 population-based cancer registries. Lancet Glob Health. 2018;6(5):e555–e567. doi:10.1016/S2214-109X(18)30127-X
3. Wu D, Jia B, Jia M, Zhao H, Zhao H, Zhou J. Comparative efficacy and safety of systemic therapy for advanced hepatocellular carcinoma: a systematic review and network meta-analysis. Front Oncol. 2023;13:1274754. doi:10.3389/fonc.2023.1274754
4. Cappuyns S, Corbett V, Yarchoan M, Finn RS, Llovet JM. Critical appraisal of guideline recommendations on systemic therapies for advanced hepatocellular carcinoma: a review. JAMA Oncol. 2024;10(3):395–404. doi:10.1001/jamaoncol.2023.2677
5. Cheng AL, Qin S, Ikeda M, et al. Updated efficacy and safety data from IMbrave150: atezolizumab plus bevacizumab vs. sorafenib for unresectable hepatocellular carcinoma. J Hepatol. 2022;76(4):862–873. doi:10.1016/j.jhep.2021.11.030
6. Qin S, Chan SL, Gu S, et al. Camrelizumab plus rivoceranib versus sorafenib as first-line therapy for unresectable hepatocellular carcinoma (CARES-310): a randomised, open-label, international Phase 3 study. Lancet. 2023;402(10408):1133–1146. doi:10.1016/S0140-6736(23)00961-3
7. Llovet JM, Kudo M, Merle P, et al. Lenvatinib plus pembrolizumab versus lenvatinib plus placebo for advanced hepatocellular carcinoma (LEAP-002): a randomised, double-blind, phase 3 trial. Lancet Oncol. 2023;24(12):1399–1410. doi:10.1016/S1470-2045(23)00469-2
8. Bruix J, Qin S, Merle P, et al. Regorafenib for patients with hepatocellular carcinoma who progressed on sorafenib treatment (RESORCE): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2017;389(10064):56–66. doi:10.1016/S0140-6736(16)32453-9
9. Shigeta K, Matsui A, Kikuchi H, et al. Regorafenib combined with PD1 blockade increases CD8 T-cell infiltration by inducing CXCL10 expression in hepatocellular carcinoma. J Immunother Cancer. 2020;8(2):e001435. doi:10.1136/jitc-2020-001435
10. Tai WT, Chu PY, Shiau CW, et al. STAT3 mediates regorafenib-induced apoptosis in hepatocellular carcinoma. Clin Cancer Res. 2014;20(22):5768–5776. doi:10.1158/1078-0432.CCR-14-0725
11. Liu K, Wu J, Xu Y, Li D, Huang S, Mao Y. Efficacy and safety of regorafenib with or without PD-1 inhibitors as second-line therapy for advanced hepatocellular carcinoma in real-world clinical practice. Onco Targets Ther. 2022;15:1079–1094. doi:10.2147/OTT.S383685
12. Yan T, Huang C, Peng C, et al. A multi-center retrospective study on the efficacy and safety of regorafenib vs. regorafenib combined with PD-1 inhibitors as a second-line therapy in patients with advanced hepatocellular carcinoma. Ann Transl Med. 2023;11(2):109. doi:10.21037/atm-22-6614
13. Benson AB, D’Angelica MI, Abbott DE, et al. Hepatobiliary cancers, version 2.2021, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2021;19(5):541–565. doi:10.6004/jnccn.2021.0022
14. Marrero JA, Kulik LM, Sirlin CB, et al. Diagnosis, staging, and management of hepatocellular carcinoma: 2018 practice guidance by the American association for the study of liver diseases. Hepatology. 2018;68(2):723–750. doi:10.1002/hep.29913
15. Bruix J, Sherman M. American association for the study of liver D. Management of hepatocellular carcinoma: an update. Hepatology. 2011;53(3):1020–1022. doi:10.1002/hep.24199
16. Llovet JM, Lencioni R. mRECIST for HCC: performance and novel refinements. J Hepatol. 2020;72(2):288–306. doi:10.1016/j.jhep.2019.09.026
17. Freites-Martinez A, Santana N, Arias-Santiago S, Viera A. Using the common terminology criteria for adverse events (CTCAE - version 5.0) to evaluate the severity of adverse events of anticancer therapies. Actas Dermosifiliogr. 2021;112(1):90–92. doi:10.1016/j.ad.2019.05.009
18. Granito A, Marinelli S, Forgione A, et al. Regorafenib combined with other systemic therapies: exploring promising therapeutic combinations in HCC. J Hepatocell Carcinoma. 2021;8:477–492. doi:10.2147/JHC.S251729
19. Abou-Elkacem L, Arns S, Brix G, et al. Regorafenib inhibits growth, angiogenesis, and metastasis in a highly aggressive, orthotopic colon cancer model. Mol Cancer Ther. 2013;12(7):1322–1331. doi:10.1158/1535-7163.MCT-12-1162
20. Zhou D, Luan J, Huang C, Li J. Tumor-associated macrophages in hepatocellular carcinoma: friend or foe ? Gut Liver. 2021;15(4):500–516. doi:10.5009/gnl20223
21. Pan Y, Yu Y, Wang X, Zhang T. Tumor-associated macrophages in tumor immunity. Front Immunol. 2020;11:583084. doi:10.3389/fimmu.2020.583084
22. Zopf D, Fichtner I, Bhargava A, et al. Pharmacologic activity and pharmacokinetics of metabolites of regorafenib in preclinical models. Cancer Med. 2016;5(11):3176–3185. doi:10.1002/cam4.883
23. Cannarile MA, Weisser M, Jacob W, Jegg AM, Ries CH, Ruttinger D. Colony-stimulating factor 1 receptor (CSF1R) inhibitors in cancer therapy. J Immunother Cancer. 2017;5(1):53. doi:10.1186/s40425-017-0257-y
24. Tu X, Yang J, Zheng Y, et al. Immunotherapy combination with regorafenib for refractory hepatocellular carcinoma: a real-world study. Int Immunopharmacol. 2022;113(Pt B):109401. doi:10.1016/j.intimp.2022.109401
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Efficacy and Safety of an Immune Checkpoint Inhibitor in Combination with Regorafenib Therapy as Second-Line Regimen for Patients with Unresectable Hepatocellular Carcinoma
Li J, Jia Y, Shao C, Li Y, Song J
Therapeutics and Clinical Risk Management 2023, 19:329-339
Published Date: 5 April 2023