Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
A Meta-Analysis of the Antidepressant Responses in Pivotal Trials on Esketamine Nasal Spray and Atypical Antipsychotics
Authors Wang L, Chen X, Gu X ![]() , De Smedt H, Popova V, Fu DJ
, De Smedt H, Popova V, Fu DJ ![]() , Canuso CM, Drevets WC, Chen G
, Canuso CM, Drevets WC, Chen G
Received 13 April 2023
Accepted for publication 15 December 2023
Published 27 December 2023 Volume 2023:19 Pages 2857—2870
DOI https://doi.org/10.2147/NDT.S417027
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Lien Wang,1,2 Xiaowei Chen,1 Xiaojing Gu,1 Heidi De Smedt,3 Vanina Popova,3 Dong-Jing Fu,4 Carla M Canuso,4 Wayne C Drevets,2 Guang Chen2
1Janssen Research & Development, LLC, Janssen Pharmaceutical Companies of Johnson & Johnson, Shanghai, People’s Republic of China; 2Janssen Research & Development, LLC, Janssen Pharmaceutical Companies of Johnson & Johnson, Brisbane, CA, USA; 3Janssen Research & Development, LLC, Janssen Pharmaceutical Companies of Johnson & Johnson, Beerse, Belgium; 4Janssen Research & Development, LLC, Janssen Pharmaceutical Companies of Johnson & Johnson, Raritan, NJ, USA
Correspondence: Guang Chen, Janssen Fellow, Scientific Director, Translational Research, Mood DAS, Neuroscience Therapeutic Area, Janssen R & D, LLC, Janssen Pharmaceutical Companies of Johnson and Johnson, 3210 Merryfield Row, Room 1908, San Diego, CA, 92121, USA, Tel +1 (240) 602 7950, Email [email protected]
Purpose: This meta-analysis assessed whether atypical antipsychotics (AAPs) and esketamine nasal spray (ESK-NS), which are mechanistically distinct, differ in antidepressant outcomes.
Patients and Methods: Data were extracted from 12 trials of ESK-NS or AAPs in depressed patients (4276) with inadequate response or resistance to conventional antidepressants. Montgomery-Åsberg Depression Rating Scale (MADRS) score reductions from baseline and response rates (≥ 50% reduction) were analyzed.
Results: At endpoint, the estimated MADRS score reduction of pooled ESK-NS arms was greater than pooled AAP arms (+9.16 points, p < 0.0001). The reduction also was greater in the pooled control arms of the ESK-NS trials than the pooled control arms of the AAP trials (+7.57 points, p < 0.0001). The mean difference in the reductions between pooled ESK-NS and control arms was 1.87 points greater than that between pooled AAP and control arms, but this difference was not significant (95% CI: − 4.49, 0.74, p = 0.16). Relative to their respective control arms, the mean difference in response rates was 25% for the pooled ESK-NS and 9% for the pooled AAP arms; the mean response rate was 16% greater in the pooled ESK-NS studies than the pooled AAP studies (p = 0.0004). Comparisons against specific AAPs showed mean differences in the MADRS score reductions at 1 week between the experimental and control arms that were numerically larger in the ESK-NS trials than in the aripiprazole trials (mean difference of 1.71 points, p = 0.06) and the brexpiprazole trials (mean difference of 2.05 points, p = 0.02).
Conclusion: The ESK-NS arms showed numerically larger MADRS score reductions at week-1 and endpoint, and a significantly larger response rate compared with AAP arms. Prospective studies involving direct comparisons are warranted to compare the relative efficacy between these treatment regimens.
Keywords: major depressive disorder, treatment resistant depression, adjunctive and conjunctive treatment, atypical antipsychotics, esketamine nasal spray, rapid-acting
Introduction
Major depressive disorder (MDD) is the leading cause of disability worldwide.1 In the US, the 12-month prevalence of MDD is 10.4%, and the lifetime prevalence is 20.6%.2 About 20–30% of individuals with MDD ultimately manifest treatment-resistant depression (TRD).3 Although no universal definition currently exists, health authorities generally define TRD as a failure to achieve response during the current major depressive episode following at least two different antidepressant treatments administered at an adequate dose and duration.4 Results from the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) trial support the consensus that response and remission rates decrease significantly in patients who have not achieved response after two distinct treatment trials.5 TRD results in higher mortality rates, especially from suicide, higher socio-occupational disability, increased direct and indirect costs, decreased quality of life, and additional burden on families and society as a whole.6–8 Therefore, unmet medical need exists for novel and mechanistically distinct treatments which have greater effectiveness, more rapid onset of action, and long-term relief of depressive symptoms for MDD patients who manifest treatment resistance.9
Current pharmacological treatment strategies for TRD consist of switching (from one antidepressant to another), augmentation (adding a non-antidepressant agent to an antidepressant), combination (of two or more antidepressants), and optimization (of dosage and duration) approaches.10,11 Among the augmentation therapies, the atypical antipsychotic (AAP) agents aripiprazole, brexpiprazole, and quetiapine have been approved by the US FDA as adjunctive treatments for patients who manifest MDD along with inadequate response to current oral antidepressant therapies.12 For the treatment of TRD, the AAP olanzapine in combination with the antidepressant fluoxetine has been approved by the FDA.12 Recently, esketamine (the S-enantiomer of ketamine racemate) nasal spray (ESK-NS) used in conjunction with an oral antidepressant was approved by the FDA for the treatment of TRD as well as for MDD with acute suicidal ideation or behavior.13 Physical therapies, such as electroconvulsive therapy and transcranial magnetic stimulation, are also treatment choices for TRD; however, physical therapies for TRD are not in the scope of the current study.14
ESK is the S-enantiomer of ketamine, an N-methyl-D-aspartate (NMDA) receptor antagonist. ESK is 2- to 2.5-fold more potent than ketamine racemate at inhibiting this receptor.15 The antidepressant effects of both ketamine and ESK putatively occur through direct NMDA receptor blockade on inhibitory interneurons, resulting in an increase in fast excitatory glutamate transmission and brain-derived neurotrophic factor release.16,17 Additionally, at exposures corresponding to the antidepressant dose range, these drugs have been shown to stimulate synaptogenesis in preclinical models of depression-like behavior.18,19 The mechanisms of Ketamine/Esketamine have also been shown to go beyond NMDA antagonism and may act as multimodal agent in regulation of tonic membrane influx of Ca2+ and Na+, synaptic protein translation, neuroplasticity, and modulation of glycogen synthase kinase-3β.20 The mechanisms of action of ketamine and ESK-NS are distinct from those of conventional antidepressants, which predominantly rely on monoamine reuptake inhibition, as well as of AAPs, which putatively act through monoamine receptor antagonism.21,22 Given these differences, it has been hypothesized that the combination of these agents may produce additive, or synergistic antidepressant effects.23,24
Dold et al performed a meta-analysis of trial endpoint data comparing the efficacy of add-on treatment of antidepressants using ESK-NS versus AAPs.25 This analysis included trials in patients with MDD who had experienced an inadequate response to antidepressants. The authors reported a higher mean difference of MADRS total score reduction between active (ie, experimental agents), and their comparison control arms for the pooled ESK-NS trials compared to the pooled AAP trials. Notably, continued use of the antidepressant to which patients had shown inadequate response was implemented in both the experimental treatment and control arms in the AAP trials, while newly initiated antidepressants were used in the experimental treatment and control arms in the ESK-NS trials. This previous meta-analysis included data from AAP trials that did not result in or did not support the FDA approval for use as adjunctive therapies in MDD or TRD. However, including these data in the meta-analysis conceivably may have introduced bias against the AAPs in general. Herein, we report the results of a meta-analysis comparing data from ESK-NS and AAP studies that were limited to publicly available, Phase-3 pivotal trials which supported the FDA approval for each agent tested. Comprehensive analyses were performed at both study endpoints and earlier timepoints, and the response rates at the study endpoints also were examined.
Methods
Data Source
Studies were identified using the FDA new drug application (NDA) approval package on the FDA website (https://www.accessdata.fda.gov/scripts/cder/daf/index.cfm). We used both generic and brand names as search terms: “Abilify” for aripiprazole, “Rexulti” for brexpiprazole, “Symbyax” for olanzapine and fluoxetine, “Seroquel XR” for quetiapine, and “Spravato” for ESK-NS. Study-related datasets were extracted from the study publications in Medline/PubMed or directly from the FDA NDA approval package.
Study Selection
Study selection was conducted independently by two authors (LW and GC). All included trials supported the FDA approval. The trials evaluated the efficacy of an AAP (aripiprazole, brexpiprazole, or quetiapine) approved in the US for the adjunctive treatment of MDD, an AAP (olanzapine) in combination with fluoxetine approved for use in TRD, or ESK-NS used conjunctively with an oral antidepressant for TRD. The full text of relevant studies was reviewed, and the following inclusion criteria were used: (1) Trial design: acute phase (4–12 weeks), phase-3, double-blind (DB), RCTs; (2) Study population: a) male or female adult patients ages 18–65 years, inclusive; b) diagnosis of a current episode of MDD; c) participants must have experienced inadequate response to at least one trial of conventional antidepressant treatment prior to enrollment; (3) Intervention: in the active (intervention) arms, participants received either AAPs administered adjunctively with oral antidepressants or ESK-NS in conjunction with oral antidepressants, and in the control arms, participants received placebo (IN or P.O.) with adjunctive or conjunctive oral antidepressants. Outcome measures were a) the mean change of depressive symptoms, evaluated using the mean change in Montgomery-Åsberg Depression Rating Scale (MADRS) total score from baseline to study endpoint as well as to the end of weeks 1, 2 and 4 during the DB induction phase; b) response rates at endpoint, defined as the proportion of patients who achieved at least a 50% reduction in the MADRS score from baseline (Supplementary Table S1).
Data Extraction
Study datasets were extracted systemically by one author (LW) and reviewed by another author (GC). The weekly mean MADRS total score changes from baseline during the DB induction phase of ESK-NS were extracted directly from the publications, while those of AAPs were extracted from figures with available mean and standard error layout in the study publications using GetData Graph Digitizer software version 1.16.0.20 (http://getdata-graph-digitizer.com/index.php).
Quality Assessment
The methodological quality of the included studies was assessed by two reviewers (LW and XG) using Cochrane Risk of Bias 2 (RoB 2.0) tools26 in the following domains: randomization process, deviation from the intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result, with discrepancies resolved by discussion and consensus recommendation.
Statistical Analysis
Meta-analysis was conducted using the R package “metafor” on summary-level data (ie, mean, standard deviation and group size) from each study.27 Least squares mean of MADRS total score change from baseline to endpoint with 95% CI was used as the outcome. The response rates were calculated as raw proportions. The mean difference (95% CI) of the MADRS total score reduction and the response rates between experimental and control arms were used to evaluate treatment effectiveness. When a study included multiple treatment arms, the effects from all arms were pooled using the recommended method in the Cochrane Handbook for Systematic Reviews of Interventions (section 16.5.4).26 Formulas are available at: https://handbook-5-1.cochrane.org/chapter_7/table_7_7_a_formulae_for_combining_groups.htm. Statistical significance was defined as two-sided p-value < 0.05.
A random effects meta-regression model allowing different amounts of residual heterogeneity between subgroups (defined by an individual drug or by pooled AAPs and ESK-NS) was applied with the restricted maximum likelihood method. The contributions of specific baseline characteristics [age, body mass index (BMI), weight, sex, race, duration of current episode, lead-in phase non-responder rate and baseline MADRS total score] to the net active treatment effect were assessed by including the individual baseline characteristic value (by study) as a variable in the regression model. The same analysis was performed for weekly estimation of the net active treatment effect. For the analysis of response rate, the treatment effect was calculated as raw proportions, and the same procedure of meta-regression was applied to obtain the estimated pooled rates. Sensitivity analysis was conducted on logit transformed rates to confirm the response rate results. The possible presence of publication bias was assessed using funnel-plot.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Protocols were reviewed and approved by an institutional review board.
Results
Study Characteristics
A total of 12 trials were included: two aripiprazole studies,28,29 two brexpiprazole studies,30,31 four olanzapine plus fluoxetine studies,32–34 two quetiapine studies,35,36 and two ESK-NS studies.37,38 A total of 4276 randomized patients were included in the analysis. Of these, 2565 patients were allocated to AAPs or ESK-NS plus antidepressant treatment (aripiprazole, n = 373; brexpiprazole, n = 644; olanzapine, n = 589; quetiapine, n = 616; ESK-NS, n = 343) and the remaining 1711 patients were randomized to control plus antidepressant treatment (aripiprazole, n = 366; brexpiprazole, n = 412; olanzapine, n = 408; quetiapine, n = 303; ESK-NS, n = 222). Regarding the antidepressants assigned during the DB induction phase, most of the AAP trials continued the antidepressants to which the patient had experienced inadequate response during the lead-in or screening phases [except in 2 olanzapine trials32,33 which used newly initiated fluoxetine], while the ESK-NS trials adopted a newly initiated antidepressant which differed from the antidepressant used during the prospective observation phase and could not be one to which the patient already had nonresponse (in the current episode) or had not tolerated (lifetime) (Supplementary Table S1). No major differences were reported in patient demographics and baseline characteristics in ESK-NS compared to control arms in the Phase 3 trials in TRD.37,38
The baseline characteristics of the included studies are listed in Table 1 along with an indication of trials for which baseline data were not available. Compared with patients from AAP trials, those from the ESK-NS trials showed significantly higher baseline mean MADRS total scores (+9.4 points, 95% CI [7.0 to 11.8], p < 0.0001; indicating greater severity of symptoms), significantly longer duration of the current depressive episode (+97.2 weeks, 95% CI [56.4 to 137.9], p < 0.0001), and significantly lower mean BMI (−1.5, 95% CI [−2.8 to −0.2], p = 0.02). Therefore, these parameters were used as covariates in modeling the mean difference between drug categories. In contrast, mean age, weight, sex and race distribution, and lead-in phase non-responder rate did not differ significantly between the AAP and ESK-NS trials. Details of the studies and baseline characteristics are listed in Supplementary Tables S1 and S2.
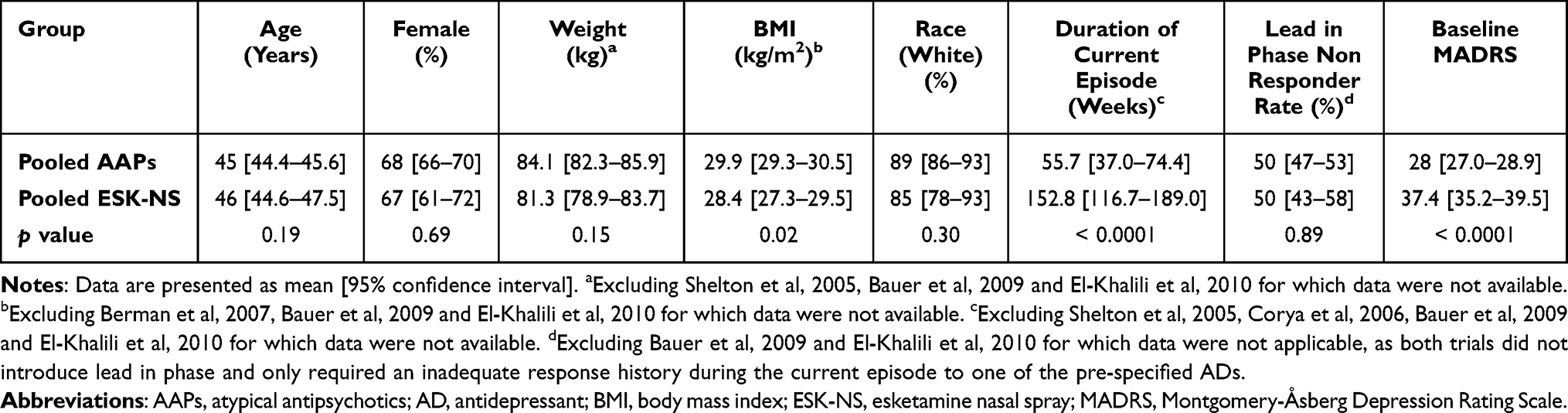 |
Table 1 Baseline Characteristics of Pivotal Trials on AAPs and ESK-NS Resulted in FDA Approvals |
Quality Assessment
The risk of bias of the included studies was assessed in the following 5 domains (Supplementary Figure S1): D1 – randomization process; D2 – deviations from the intended interventions; D3 – missing outcome data; D4 – measurement of the outcome; D5 – selection of the reported result. All the studies were randomized, but only 4 of the 12 studies clearly described the procedures for both random allocation sequence generation and allocation sequence concealment. Regarding the D2 and D3 domains, only two ESK-NS studies clearly stated the blinding of participants, study site personnel, and outcome assessors (by applying remote raters), and 8 studies applied an appropriate statistical analysis to estimate the effect of assignment to interventions. All but two studies provided evidence that the result was not biased by missing outcome data, and all 12 studies were free from selective reporting bias. The overall methodological quality of the included studies did not show evidence of a publication bias (Supplementary Figure S2).
MADRS Total Score Reductions at Endpoint
Regarding study design features, the DB period duration and trial endpoints differed between ESK-NS trials (4 weeks) and AAP trials (6 to 12 weeks) (Supplementary Table 1). The MADRS total score reductions for the active (AAPs or ESK-NS) and control arms and for the mean differences between arms at trial endpoints are shown in Figure 1. The estimated MADRS total score reduction of the pooled ESK-NS groups was significantly greater than that of the pooled AAP groups (by 9.16 points, p < 0.0001, Figure 1A). Significantly greater estimated MADRS total score reduction was also observed in the pooled control arms from ESK-NS trials compared to that of the pooled control arms from AAP trials (by 7.57 points, p < 0.0001, Figure 1B). In addition, the meta-regression analysis with baseline MADRS total score as a covariate indicated that in both cases, the differences between the AAP and ESK-NS trials were significantly influenced by the variation in baseline MADRS total score (p = 0.03 for active treatment; p = 0.02 for control).
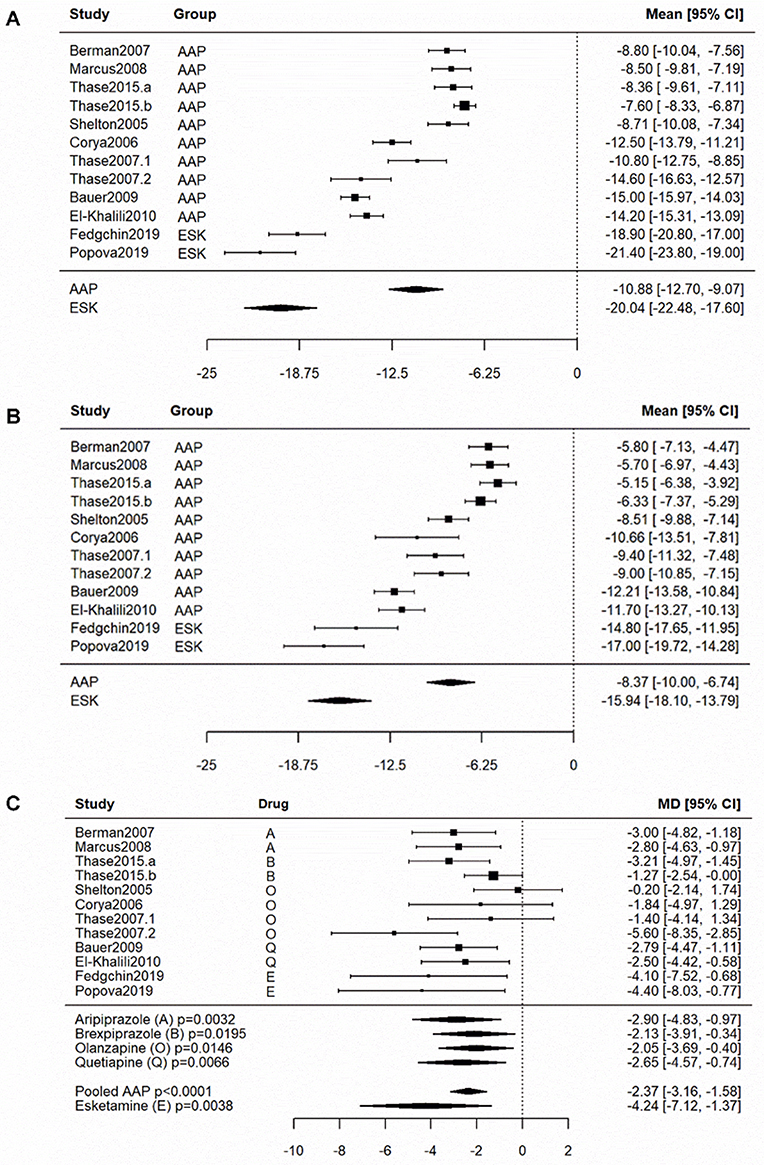 |
Figure 1 Effects and mean differences in pivotal AAPs and ESK-NS trials that resulted in FDA approvals at study endpoint. The reduction of least squares mean MADRS total score in (A) the active (ESK-NS and AAPs) arms and (B) the control arms, as well as (C) the MD between active and control arms from individual studies is shown in the forest plot, with 95% CI. The pooled effect sizes for individual drugs, AAPs and ESK-NS were estimated by random effects regression model, including the subgroup information as a factor variable. Pairwise comparison of MADRS total score reduction between pooled estimates of AAPs and ESK-NS was conducted significant greater reduction in ESK-NS trials: (A) Active arms: AAPs vs ESK-NS, p < 0.0001; (B) Control arms: AAPs vs ESK-NS, p < 0.0001. The net treatment effect is significant for all the drugs, as well as pooled AAPs and ESK-NS, as indicated by p-values. Pair-wise comparison of the estimated MD between ESK-NS and the individual AAP or pooled AAPs was conducted with no statistical significance observed: (C) ESK-NS vs aripiprazole, p = 0.45; ESK-NS vs brexpiprazole, p = 0.22; ESK-NS vs olanzapine, p = 0.19; ESK-NS vs quetiapine, p = 0.37; ESK-NS vs pooled AAPs, p = 0.16. All p-values are two sided. It is noteworthy that continuing antidepressants were used in both active and control arms of AAP trials, and that newly initiated antidepressants were on-board in both active and control arms of ESK-NS trials. Abbreviations: AAPs, atypical antipsychotics; ESK-NS, esketamine nasal spray; MADRS, Montgomery-Åsberg Depression Rating Scale; MD, mean difference. |
The mean difference between active and control arms is illustrated in Figure 1C. The estimated mean difference of all individual AAP arms showed significantly larger MADRS total score reductions over their control arms (aripiprazole: −2.90, 95% CI [−4.83 to −0.97], p = 0.0032; brexpiprazole: −2.13, 95% CI [−3.91 to −0.34], p = 0.0195; olanzapine: −2.05, 95% CI [−3.69 to −0.40], p = 0.0146; quetiapine: −2.65, 95% CI [−4.57 to −0.74], p = 0.0066; Figure 1C). The estimated mean difference of pooled AAP arms demonstrated significantly larger reductions over control (−2.37, 95% CI [−3.16 to −1.58], p < 0.0001; Figure 1C). The estimated mean difference of the ESK-NS arms also showed significantly larger MADRS score reductions over their control arms (4.24, 95% CI [−7.2 to −1.3], p=0.0038; Figure 1C). The estimated mean difference in the reduction points differentiating ESK-NS trials and AAP trials, as indicated by model-based indirect comparison, was 1.87 points on the MADRS, but this difference was not significant (95% CI [−4.49 to 0.74], p = 0.16) in the model. The overall residual heterogeneity of mean difference among the trials is moderate (I2 = 36.9%). Separate meta-regression analysis was conducted to examine the potential contribution of the covariates including age, BMI, weight, race, sex, duration of current episode, lead-in phase non-responder rate, and baseline MADRS total score. None of the factors had a statistically significant contribution to the overall heterogeneity of the mean difference in total MADRS score reduction at endpoint, and thus these factors were not included in the final model (Supplementary Table S3).
Response Rates at Endpoint
The pooled ESK-NS arms and their pooled corresponding control arms revealed higher response rates (between active (ESK-NS or AAPs) treatment arms: +33%, p = 0.0006; between control arms: +18%, p = 0.0572; Figure 2) compared with those of the pooled AAPs and their control arms, respectively. The mean difference in response rates between ESK-NS and its control arms was 25% (p<0.0001). The mean difference in response rates between the pooled AAP versus their control arms was 9% (p<0.0001). The mean difference in response rates between ESK-NS and its control arms was significantly larger than that between AAPs and their control arms (+16%, 95% CI [0.07 to 0.25], p=0.0004; Figure 2). Meta-regression analysis was also conducted and revealed that none of the covariates tested had a statistically significant contribution to the overall heterogeneity of the mean difference in response rates (Supplementary Table S4). The result was further confirmed by additional sensitivity analysis with logit transformed rates, which yielded the same conclusion (Supplementary Table S5).
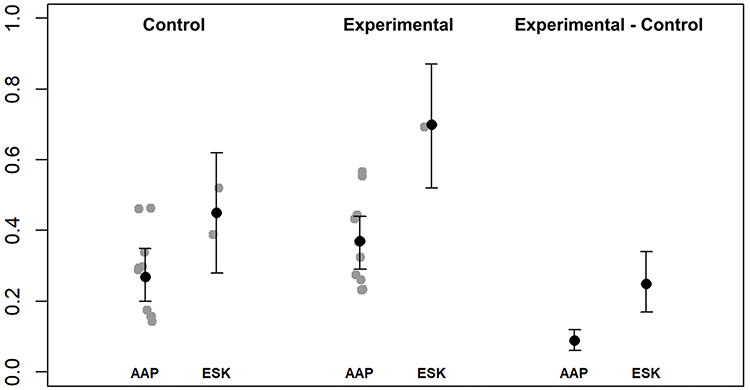 |
Figure 2 Response rates in pivotal AAPs and ESK-NS trials that resulted in FDA approvals. Study endpoint from individual studies, grouped by AAPs and ESK-NS, were shown as grey dots. The pooled rates with 95% CI for subgroups were estimated by random effects regression model with subgroup as a factor variable. Pairwise comparison between AAPs and ESK-NS was conducted for the control and active arms, as well as the mean difference of response rate between the active and control arms: Response rate: Control, p = 0.0572; Active, p = 0.0006; Mean difference, p = 0.0004. All the p-values are two sided. Abbreviations: AAPs, atypical antipsychotics; AD, antidepressant; ESK-NS, esketamine nasal spray. |
Time Course of MADRS Total Score Reductions
To explore the time course of antidepressant effects, the mean reductions in MADRS total score reported for time intervals earlier than the trial endpoints were extracted for each study. These data were obtained from figures showing the mean and standard error values in the publications reporting the pivotal trial data for aripiprazole and brexpiprazole, and from the clinical study reports of the pivotal ESK-NS trials. At the week one timepoint, the MADRS total score reductions of the AAP and ESK-NS arms and their corresponding control arms are shown in Figures 3A and 3B. The residual heterogeneity of the mean difference among all trials at week one was 0. Meta-regression analysis revealed two covariates, lead-in phase non-responder rate and baseline MADRS total score, which contributed significantly to the overall heterogeneity of the mean difference in the total MADRS score reduction at week one (Lead-in phase non-responder rate: p=0.017; Baseline MADRS total score: p=0.019, Supplementary Table S6). The covariate adjusted mean difference values are shown in Figure 3C and indicated significantly greater antidepressant responses in three of the pooled active arms (aripiprazole: −1.24, 95% CI [−2.09 to-0.39], p = 0.0043; brexpiprazole: −0.89, 95% CI [−1.61 to −0.18], p = 0.0142; ESK-NS: −2.95, 95% CI [−4.50 to −1.40], p = 0.0002; Figure 3C). Moreover, the mean difference values comparing the ESK-NS arms relative to its control arms were higher than those for aripiprazole (mean difference = −1.71; 95% CI [−3.47 to 0.05], p = 0.057) and brexpiprazole (mean difference = −2.05; 95% CI [−3.79 to −0.32], p = 0.02). At the week two and week four timepoints, the ESK-NS arm showed numerically higher mean difference values than those of the aripiprazole and brexpiprazole arms, but these differences were not significant (p > 0.05, data not shown).
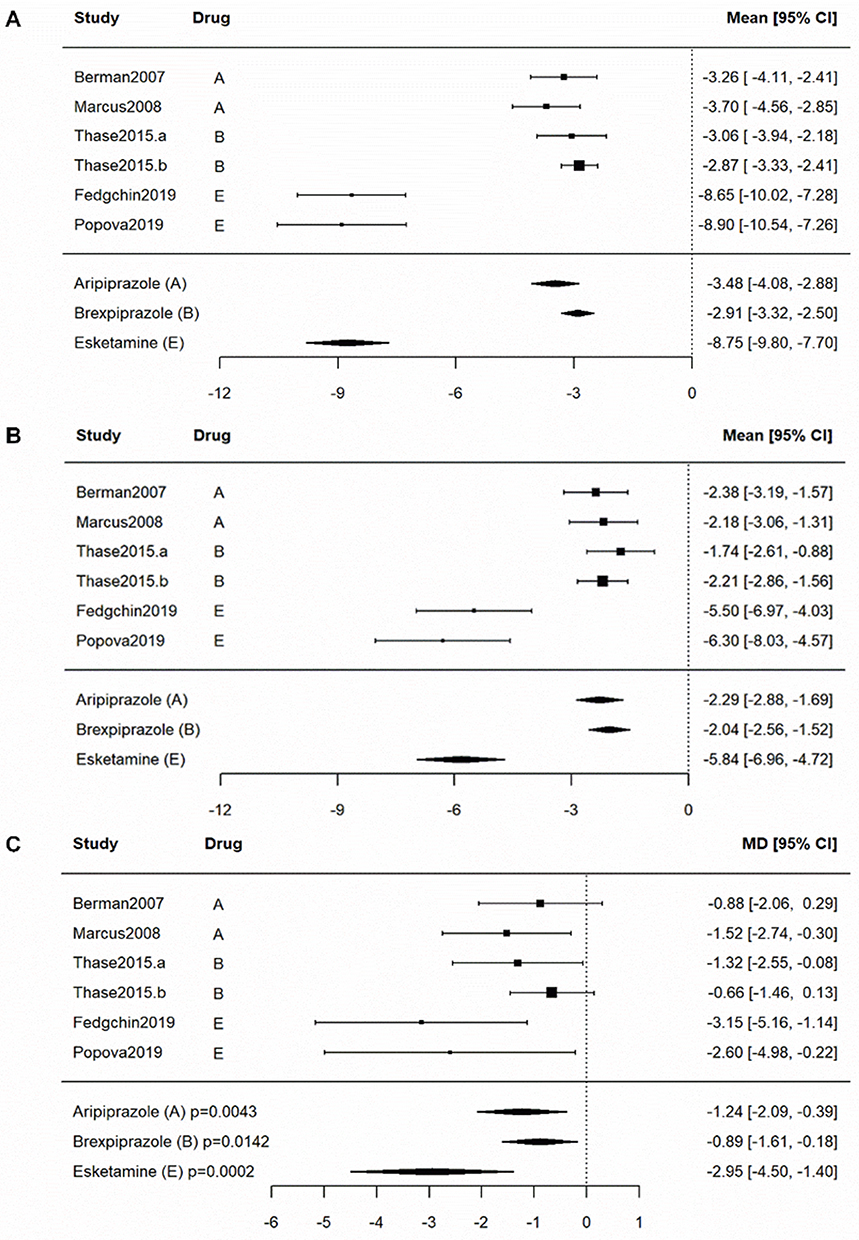 |
Figure 3 Effects and mean differences in pivotal AAPs and ESK-NS trials that resulted in FDA approvals at end of week one. The available reduction of least squares mean MADRS total score in (A) active and (B) control arms, and (C) the MD between the active and control arms on least squares mean MADRS total score reduction at week one timepoint in aripiprazole, brexpiprazole and ESK-NS studies were shown in the forest plot, including 95% CI. The pooled effect of individual drugs at week one was estimated by random effects regression model by including the drug arm as a factor variable. The MD were significant for all drugs, as indicated by p-values in the figure. Pairwise comparison indicated the MD of ESK-NS exhibited 1.71 more points MADRS total score reduction than that of aripiprazole and 2.05 more points reduction than that of brexpiprazole: (C) ESK-NS vs aripiprazole, p = 0.057; ESK-NS vs brexpiprazole, p = 0.02. All the p-values are two sided. Abbreviations: AAPs, atypical antipsychotics; ESK-NS, esketamine nasal spray; MD, mean difference. |
Discussion
This meta-analysis provided a model-based, indirect comparison of the antidepressant treatment outcomes obtained in trials of ESK-NS or AAPs in participants with MDD who had manifested either inadequate response or resistance to conventional antidepressant treatment. At the trial endpoint, the ESK-NS trials showed a numerically greater reduction in MADRS scores in the experimental treatment versus the control arms, compared to the corresponding experimental treatment versus control arms from the AAP trials, but this difference was not significant. The mean antidepressant response rate, defined by a reduction in MADRS score of at least 50%, was significantly larger in the ESK-NS trials than in the AAP trials. In addition, at the week one timepoint, the ESK-NS trials showed significantly and numerically larger treatment effects, respectively, than brexpiprazole and aripiprazole trials.
A 2-point difference on the MADRS between drug and comparator at study endpoint is generally considered to reflect a clinically meaningful difference in depression severity.39 The mean difference of the MADRS score reduction at the week one timepoint and study endpoint was 2.95 and 4.24 points in the ESK-NS trials, respectively, and approximately 1 and 2.37 points in the AAP trials, respectively. Within each treatment class, the differences between the experimental treatment and control arms were statistically significant. Notably, the MADRS reductions observed in response to the control treatment in the ESK-NS trials (which consisted of a newly added oral antidepressant drug which the participant had not previously tried and failed), the mean difference in MADRS total score reductions in these trials was nearly twice as large as those observed in the AAP trials at endpoint, consistent with the results of a previous meta-analysis.25 The meta-analysis by Dold et al included all Phase-2 and −3 RCTs with both positive and negative outcomes reported for six AAPs. In contrast, the current study only included the pivotal Phase-3 RCTs used to support the efficacy of regulatory filings for the four AAPs which have received FDA approval.25 Thus, an additional 8 studies40–46 were included in the analysis by Dold et al. In the cohort that included these additional 8 studies along with those considered herein, the corresponding MADRS total score reductions and mean difference were also examined, and the results are shown in Supplementary Figure 3. Consistent with the results we report in Figure 1C, and the results reported by Dold et al, the pooled estimates obtained using the expanded number of AAP trials and the same ESK-NS trials demonstrated significantly larger reductions over control; specifically, the mean difference values were −2.06 (95% CI [−2.61 to −1.51], p < 0.0001) and −4.24 (95% CI [−6.94 to −1.54], p = 0.0021) for the pooled AAPs and ESK-NS, respectively. The estimated mean difference of ESK-NS had 2.18 more points of MADRS total score reduction than that of the pooled AAPs (95% CI [−4.73 to 0.37], p = 0.0933), as indicated by model-based indirect comparison. In addition, the size of difference in the mean response rate between the experimental treatment and control arms was 16% higher in the ESK-NS trials than that in the AAP trials. These data further suggest that ESK-NS produces an antidepressant response that is larger and achieved earlier in the treatment course compared with AAPs (ie, by 4 weeks in the ESK-NS trials vs 6–12 weeks in the AAP trials).
The current meta-analysis also suggests a larger mean difference in MADRS score reduction between ESK-NS and its control arm at the end of week one of the DB induction phase compared to that of aripiprazole and brexpiprazole (nominal p-values of 0.057 and 0.02, respectively), potentially suggesting an onset of efficacy advantage in favor of ESK-NS over AAPs. Our previous ESK-NS studies demonstrated superiority over control in producing significant MADRS score reductions as early as day 2 (ie, 24 hours after the first ESK-NS administration).37,38 However, since the AAP trials considered herein did not include such early time points, we were not able to compare treatment effectiveness between AAPs and ESK-NS treatment at day 2 in the current meta-analysis. Instead, the first timepoint at which data could be compared was at the end of the first treatment week.
The observed larger effect size in the ESK-NS trials compared to the AAP trials is noteworthy given that the ESK-NS trials had a shorter DB treatment phase duration (4 vs 6–12 weeks) and that there were higher antidepressant responses in the control arms of the ESK-NS trials than those in the control arms of the AAP trials. The latter observation may have been attributable to the design difference that in most of the studies involving AAPs, the AAP was added to an oral antidepressant to which the patient had already experienced inadequate response, whereas in the ESK-NS trials the oral antidepressant added to each study arm was selected to be one that the participant had not previously received with negative outcome. Therefore, the interpretation of these results requires consideration of the limitations in making comparisons across studies, especially given the design differences extant between trials.
In this regard, several design differences between the trials considered herein merit comment. First, the treatment resistance status of the included patients from the AAP and ESK-NS trials was different. The results indicated that most patients from the ESK-NS trials had 2 to 3 previously failed trials, defined by none to minimal response at screening, while most patients from the AAP trials had experienced 1 to 2 previously failed trials defined either as none to minimal response or as partial response at screening. In addition, the patients who entered the ESK-NS trials on average manifested a relatively longer duration in the current episode compared to those who entered the AAP trials (Table 1 and Supplementary Table S2). Based on these differences, the patients in the ESK-NS trials putatively would have been expected to show a smaller antidepressant response to subsequent treatment trials.5
Second, the severity of depression in the study populations differed between the AAP and ESK-NS trials. Specifically, the patients in the ESK-NS trials had a higher baseline MADRS total score (ie, greater severity of depressive symptoms) compared to those in the AAP trials. Such a severity difference was partially due to the study design difference of the rating scale inclusion criteria during the screening phase and the non-response inclusion criteria during the lead-in phase between the AAP and ESK-NS trials. Although all of the studies included in the meta-analysis used the MADRS to assess the primary endpoint of change in depression severity, most of the AAP trials also required a minimum Hamilton Depression Rating Scale (HAMD)-17 score at screening of between 18 and 22, which approximately corresponds to a MADRS score of 23 to 28,47 compared to the inclusion criterion of MADRS score ≥28 in the ESK-NS trials. Additionally, most AAP trials required a HAMD-17 score of at least 14 to 18 (approximating a MADRS score of 18 to 23) at the end of the lead-in phase, compared to the minimum MADRS total score ≥28 required in the ESK-NS trials. Although it may be hypothesized that the TRD patients in ESK-NS trials have more dynamic range in which to show depression improvement, this tendency would likely be offset by the limitation that the patients with TRD had already been through at least two rounds of adequate treatments with antidepressants and not only remained more severely depressed (See above), they also had shown less improvement during at least two prior treatment trials, and thus were presumably more difficult to treat. To address the possibility that differences in baseline severity influenced the absolute change in severity measured across the treatment trials, we used baseline severity as a covariate in modeling the mean difference between drug categories. Nevertheless, potential differences in baseline severity across trials are less likely to influence the differential response rates found between the ESK-NS and AAP trials, which provided the most significant difference across drug classes identified in our meta-analysis. By convention, an antidepressant “response” is defined as a change in depression rating scale score of ≥50%, and the response rate is the proportion of participants within each study arm who achieve this level of improvement. During the treatment period, a participant with greater baseline severity therefore needs to manifest a larger absolute reduction than a patient with a lesser baseline severity to qualify as an antidepressant “response”. Therefore, this proportionality putatively removes any advantage that may be conferred for patients with greater baseline severity in achieving a clinical response, and thus would not be expected to account for the greater response rate obtained in our meta-analysis between ESK-NS and AAPs.
Third, the profile of adverse effects was different between the AAP and ESK-NS trials. One of the adverse effects for the ESK-NS treatment that was distinct from the control treatment was dissociation. The possibility that treatment emergent adverse events may have produced functional unblinding in patients could not be completely excluded. To address this possibility, blinded remote raters were employed to perform the MADRS assessments via telephone in the ESK-NS pivotal trials, a design feature that limited the sensitivity for detecting treatment associated changes in affect. In contrast, none of the AAP trials reported using blinded remote raters (Supplementary Figure S1). Nevertheless, the adverse events associated with AAPs hold similar potential of TEAE induced functional unblinding effect in study participants. Most adverse effects for AAP treatment are distinct from those of their control treatment (an oral antidepressant drug), including activating TEAEs such as akathisia and restlessness, sedating TEAEs such as somnolence and sedation, and weight gain. While the impact of such limitations on the meta-analysis results is difficult to quantify or statistically control, it is noteworthy that a post-hoc analysis of the ESK-NS trial data showed that neither the presence nor the severity of dissociation was correlated with or served as a mediator of the antidepressant responses in these trials (Chen et al, 2022 (PMID: 35022754)). These data suggest that the relatively large antidepressant effect size produced during ESK-NS treatment was not attributable to functional unblinding caused by dissociation in patients. Moreover, research evaluating the comparability of MADRS ratings obtained by blinded remote raters versus face-to-face raters has shown no significant difference between mean scores and high intraclass correlations for ratings obtained on the same patient.48
Fourth, differences in treatment regimens and study procedures between the AAP and ESK-NS trials may have introduced nonspecific or exaggerated control effects that differed across trial types. ESK-NS was administered twice weekly with a single-dose titration period of only 4 days, whereas AAPs were administered daily with a dose titration period ranging from 2 to 4 weeks. The more frequent study visits and extra observation from research staff in the ESK-NS trials would have been expected to increase nonspecific placebo effects,49,50 putatively masking antidepressant effects by ESK-NS. This design difference thus would have putatively biased results in the direction opposite to that actually found by meta-analysis.
Fifth, in most of the AAP trials, the conventional antidepressant continued during the DB treatment phase was the same agent that had proven inadequate in producing an antidepressant response during the lead-in or screening phase, while the ESK-NS trials instead introduced a newly initiated oral antidepressant which patients had not previously tried unsuccessfully (Supplementary Table S1). This difference may have increased both the likelihood of responding to the control treatment and the magnitude of expectancy bias in the control arm of the ESK-NS studies. For example, the patients entering the ESK-NS trials knew they would receive a new treatment to which they had not previously failed to respond in both study arms. In contrast, the patients in most of the AAP trials knew that they would receive either a new drug (the AAP) or a placebo, which would be added to the drug to which they had already experienced an inadequate response. This design difference arguably biased against showing an efficacy signal in the ESK-NS trials. Consistent with these concerns, our analysis revealed a significantly greater MADRS total score reduction at endpoint (Figure 1B) and higher response rate (Figure 2A) in the control arms (ie, control plus the newly initiated antidepressant) of the ESK-NS trials, compared to the control arms (ie, control plus the continuing antidepressants) of the AAP trials. The higher control responses in the ESK-NS trials and the expectation related control effect due to the switch to a new antidepressant and/or receipt of a new mechanistic treatment (ESK-NS vs AAPs) previously have been discussed elsewhere.51,52 These design issues conceivably increase the challenge for an active treatment to surpass the higher control effect encountered in a trial design like that used in the ESK-NS pivotal trials. Taken together, the combined effects of these differences on the responses of both active treatment and control arms limit the validity of comparisons across drug types using the extant studies.
Given the differences in study design and clinical severity between the AAP and ESK-NS trials, interpretation of the differential antidepressant effectiveness observed in indirect comparisons between ESK-NS and AAP treatment requires caution. Ultimately, direct comparisons in which patient samples are randomized to eliminate clinical and demographic differences between treatment arms are needed to corroborate the results from indirect comparisons. Thus, it is noteworthy that the results of the indirect comparisons reported here and in Dold et al appear directionally consistent with those from a recent direct comparison involving participants with TRD randomized to receive either ESK-NS or quetiapine XR in conjunction with an SRI/SNRI that had elicited non-response, and in which the adjunctive ESK-NS arm showed superiority over the adjunctive quetiapine XR arm in the proportions of participants achieving remission.53
Notably, one outcome measure that was not compared in our meta-analysis was the remission rate. This rate is defined generally as the proportion of patients whose MADRS total score at the end of the DB period had decreased below a prespecified threshold, although the threshold used to define remission varied across the included studies (Supplementary Table S1). In addition, reaching remission requires a smaller decrement in the depression rating scale scores for patients who are less severely depressed at study entry. Finally, antidepressant trials generally show main effects of time, such that the depression severity tends to decrease progressively as the DB period increases. Thus, the proportion of patients reaching the threshold for remission increases for longer duration trials. Considering the significant differences in baseline severity, duration of the DB period (to study endpoint), and remission rate criteria applied between the AAP and ESK-NS trials, the comparison of remission rate at endpoint between trial types was not included in our meta-analysis.
Finally, this analysis was conducted on very strictly selected RCT studies for a specific purpose, which allowed greater methodological rigor, however does not fully capture the reality of TRD clinical practice, where complex psychiatric and medical comorbidities occur, as well as longer disease histories and more frequent recurrences. With recent real-world studies of Esketamine become available, a systematic review with wider scope can help to better depict the landscape of TRD treatment.54–56 In conclusion, the results of this meta-analysis suggest that these mechanistically different adjunctive or conjunctive antidepressant agents differed in their antidepressant outcomes. However, the interpretation of these results is limited by differences in trial design, patient characteristics, trial duration, dosing regimen, and nature of the control condition (ie, presence of newly initiated antidepressant) in the ESK-NS trials versus the AAP trials. Prospective head-to-head studies are needed to corroborate these results and to elucidate the factors that contribute to the differential responses to ESK-NS and AAP when used together with conventional antidepressants in the management of MDD patients manifesting antidepressant treatment resistance.
Acknowledgments
Authors thank study participants, without whom this study would never have been accomplished, and all the investigators, their medical, nursing and laboratory staff for their participation in these studies. Writing and editorial support were provided by Colleen Elliott, PhD of CME Sciences, LLC, and funded by Janssen Pharmaceuticals, Inc.
Disclosure
Dr Lien Wang was a full time employee of Jassen Research and Development during the donduct of the study. Dr Xiaowei Chen is a full time employee of Janssen Research & Development and stockholder of Johnson & Johnson, outside the submitted work. Dr Heidi De Smedt is a full time employee of Jassen Research & Development and stockholder of Johnson & Johnson, outside the submitted work. Dr Xiaojing Gu was an employee of Johnson & Johnson China (Inv), outside the submitted work. Dr Vanina Popova is a full-time Employee of Janssen Research & Development, Shareholder of J&J Stock, outside the submitted work. Dr Dong-Jing Fu reports I’m a full time employee of Janssen Research & Development, LLC and stockholder of Johnson&Johnson. Dr Carla Canuso Full-time employee of Janssen Research & Development, Shareholder in Johnson & Johnson, outside the submitted work. Dr Wayne Drevets is a full time employee of Janssen Research & Development, of Johnson & Johnson, outside the submitted work; In addition, Dr Wayne Drevets has a patent Compositions and Methods for the treatment of depression pending to Johnson & Johnson; and I own equity in Johnson & Johnson. Dr Guang Chen was an employee of Janssen, during the conduct of the study. The authors report no other conflicts of interest in this work.
All authors participated in the original design of the studies (LW, XC, GC), monitoring of data quality (LW, XC, XG, GC) and contributed to the data interpretation (LW, XC, XG, GC), development and review of this manuscript (all authors) and confirm that they have read the journal’s position on issues involved in ethical publication and affirm that this report is consistent with those guidelines. All authors meet ICMJE criteria and all those who fulfilled those criteria are listed as authors. All authors had access to the study data, provided direction and comments on the manuscript, made the final decision about where to publish these data and approved submission to this journal. None of the authors had concerns about the validity of the study or competing interests which would have created a bias in the reporting of the results and conclusion.
References
1. World Health Organization. Depression and other common mental disorders global health estimates; 2017. Available from: https://www.who.int/publications/i/item/depression-global-health-estimates.
2. Hasin DS, Sarvet AL, Meyers JL, et al. Epidemiology of Adult DSM-5 major depressive disorder and its specifiers in the United States. JAMA Psychiatry. 2018;75:336–346. doi:10.1001/jamapsychiatry.2017.4602
3. Fekadu A, Wooderson SC, Markopoulo K, et al. What happens to patients with treatment-resistant depression? A systematic review of medium to long term outcome studies. J Affective Disorders. 2009;116:4–11. doi:10.1016/j.jad.2008.10.014
4. Gaynes B, Asher G, Gartlehner G, et al. Definition of treatment-resistant depression in the medicare population. Technology Assessment Program–Technical Assessment; 2018. Available from: https://www.cms.gov/Medicare/Coverage/DeterminationProcess/downloads/id105TA.pdf.
5. Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR* D report. Am J Psychiatry. 2006;163:1905–1917. doi:10.1176/ajp.2006.163.11.1905
6. Johnston KM, Powell LC, Anderson IM, Szabo S, Cline S. The burden of treatment-resistant depression: a systematic review of the economic and quality of life literature. J Affective Disorders. 2019;242:195–210. doi:10.1016/j.jad.2018.06.045
7. Bergfeld IO, Mantione M, Figee M, et al. Treatment-resistant depression and suicidality. J Affect Disord. 2018;235:362–367. doi:10.1016/j.jad.2018.04.016
8. Blazer DG. Depression in late life: review and commentary. J Gerontol a Biol Sci Med Sci. 2003;58:249–265. doi:10.1093/gerona/58.3.M249
9. Thase ME. Current and emerging treatments to address unmet needs in MDD. J Clin Psych. 2019;80. doi:10.4088/JCP.AL18009BR1C
10. Ionescu DF, Rosenbaum JF, Alpert JE. Pharmacological approaches to the challenge of treatment-resistant depression. Dialog Clin Neurosci. 2015;17:111. doi:10.31887/DCNS.2015.17.2/dionescu
11. Shelton RC, Osuntokun O, Heinloth AN, Corya SA. Therapeutic options for treatment-resistant depression. CNS Drugs. 2010;24:131–161. doi:10.2165/11530280-000000000-00000
12. McIntyre RS, Filteau M-J, Martin L, et al. Treatment-resistant depression: definitions, review of the evidence, and algorithmic approach. J Affective Disorders. 2014;156:1–7. doi:10.1016/j.jad.2013.10.043
13. SPRAVATO™ Highlights of Prescribing Information. Janssen Pharmaceuticals I, Titusville NJ; 2019. https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/211243lbl.pdf.
14. Menon V, Varadharajan N, Faheem A, Andrade C. Ketamine vs electroconvulsive therapy for major depressive episode: a systematic review and meta-analysis. JAMA Psychiatry. 2023;80:639–642. doi:10.1001/jamapsychiatry.2023.0562
15. Zanos P, Moaddel R, Morris PJ, et al. Ketamine and ketamine metabolite pharmacology: insights into therapeutic mechanisms. Pharmacol Rev. 2018;70:621–660. doi:10.1124/pr.117.015198
16. Duman RS, Li N, Liu RJ, Duric V, Aghajanian G. Signaling pathways underlying the rapid antidepressant actions of ketamine. Neuropharmacology. 2012;62:35–41. doi:10.1016/j.neuropharm.2011.08.044
17. Monteggia LM, Zarate C. Antidepressant actions of ketamine: from molecular mechanisms to clinical practice. Curr Opin Neurobiol. 2015;30:139–143. doi:10.1016/j.conb.2014.12.004
18. Duman RS, Aghajanian GK. Synaptic dysfunction in depression: potential therapeutic targets. Science. 2012;338:68–72. doi:10.1126/science.1222939
19. Duman RS, Aghajanian GK, Sanacora G, Krystal JH. Synaptic plasticity and depression: new insights from stress and rapid-acting antidepressants. Nat Med. 2016;22:238–249. doi:10.1038/nm.4050
20. d’Andrea G, Pettorruso M, Lorenzo GD, et al. Rethinking ketamine and esketamine action: are they antidepressants with mood-stabilizing properties? Eur Neuropsychopharmacol. 2023;70:49–55. doi:10.1016/j.euroneuro.2023.02.010
21. Artigas F, Nutt DJ, Shelton R. Mechanism of action of antidepressants. Psychopharmacol Bull. 2002;36:123–132.
22. Wright BM, Eiland EH, Lorenz R. Augmentation with atypical antipsychotics for depression: a review of evidence‐based support from the medical literature. Pharmacother J Human Pharmacol Drug Ther. 2013;33:344–359. doi:10.1002/phar.1204
23. Rogoz Z. Combined treatment with atypical antipsychotics and antidepressants in treatment-resistant depression: preclinical and clinical efficacy. Pharmacol Rep. 2013;65:1535–1544. doi:10.1016/S1734-1140(13)71515-9
24. Spina E, de Leon J. Clinically relevant interactions between newer antidepressants and second-generation antipsychotics. Expert Opin Drug Metab Toxicol. 2014;10:721–746. doi:10.1517/17425255.2014.885504
25. Dold M, Bartova L, Kasper S. Treatment response of add-on esketamine nasal spray in resistant major depression in relation to add-on second-generation antipsychotic treatment. Inter J Neuropsychopharmacol. 2020;23:440–445. doi:10.1093/ijnp/pyaa034
26. Higgins JP. Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons; 2019.
27. Viechtbauer W. Conducting meta-analyses in R with the metafor package. Journal of Statistical Software. 2010;36:1–48. doi:10.18637/jss.v036.i03
28. Berman RM, Marcus RN, Swanink R, et al. The efficacy and safety of aripiprazole as adjunctive therapy in major depressive disorder: a multicenter, randomized, double-blind, placebo-controlled study. J Clin Psych. 2007;68:843–853. doi:10.4088/JCP.v68n0604
29. Marcus RN, McQuade RD, Carson WH, et al. The efficacy and safety of aripiprazole as adjunctive therapy in major depressive disorder: a second multicenter, randomized, double-blind, placebo-controlled study. J Clin Psychopharmacol. 2008;28:156–165. doi:10.1097/JCP.0b013e31816774f9
30. Thase ME, Youakim JM, Skuban A, et al. Efficacy and safety of adjunctive brexpiprazole 2 mg in major depressive disorder: a phase 3, randomized, placebo-controlled study in patients with inadequate response to antidepressants. J Clini Psych. 2015;76:1224–1231. doi:10.4088/JCP.14m09688
31. Thase ME, Youakim JM, Skuban A, et al. Adjunctive brexpiprazole 1 and 3 mg for patients with major depressive disorder following inadequate response to antidepressants: a phase 3, randomized, double-blind study. J Clini Psych. 2015;76:1232–1240. doi:10.4088/JCP.14m09689
32. Corya SA, Williamson D, Sanger TM, et al. A randomized, double‐blind comparison of olanzapine/fluoxetine combination, olanzapine, fluoxetine, and venlafaxine in treatment‐resistant depression. Depression Anxiety. 2006;23:364–372. doi:10.1002/da.20130
33. Shelton RC, Williamson DJ, Corya SA, et al. Olanzapine/fluoxetine combination for treatment-resistant depression: a controlled study of SSRI and nortriptyline resistance. J Clin Psych. 2005;66:1289–1297. doi:10.4088/JCP.v66n1012
34. Thase ME, Corya SA, Osuntokun O, et al. A randomized, double-blind comparison of olanzapine/fluoxetine combination, olanzapine, and fluoxetine in treatment-resistant major depressive disorder. J Clini Psych. 2007;68:224–236. doi:10.4088/JCP.v68n0207
35. Bauer M, Pretorius HW, Constant EL, et al. Extended-release quetiapine as adjunct to an antidepressant in patients with major depressive disorder: results of a randomized, placebo-controlled, double-blind study. J Clin Psychiatry. 2009;70:540–549. doi:10.4088/JCP.08m04629
36. El-Khalili N, Joyce M, Atkinson S, et al. Extended-release quetiapine fumarate (quetiapine XR) as adjunctive therapy in major depressive disorder (MDD) in patients with an inadequate response to ongoing antidepressant treatment: a multicentre, randomized, double-blind, placebo-controlled study. Inter J Neuropsychopharmacol. 2010;13:917–932. doi:10.1017/S1461145710000015
37. Fedgchin M, Trivedi M, Daly EJ, et al. Efficacy and safety of fixed-dose esketamine nasal spray combined with a new oral antidepressant in treatment-resistant depression: results of a randomized, double-blind, active-controlled study (TRANSFORM-1). Inter J Neuropsychopharmacol. 2019;22:616–630. doi:10.1093/ijnp/pyz039
38. Popova V, Daly EJ, Trivedi M, et al. Efficacy and safety of flexibly dosed esketamine nasal spray combined with a newly initiated oral antidepressant in treatment-resistant depression: a randomized double-blind active-controlled study. Am J Psychiatry. 2019;176:428–438. doi:10.1176/appi.ajp.2019.19020172
39. Montgomery SA, Möller H-J. Is the significant superiority of escitalopram compared with other antidepressants clinically relevant? Inter Clin Psychopharmacol. 2009;24:111–118. doi:10.1097/YIC.0b013e32832a8eb2
40. Bauer M, Hefting N, Lindsten A, Josiassen MK, Hobart M. A randomised, placebo-controlled 24-week study evaluating adjunctive brexpiprazole in patients with major depressive disorder. Acta Neuropsychiatr. 2019;31:27–35. doi:10.1017/neu.2018.23
41. Berman RM, Fava M, Thase ME, et al. Aripiprazole augmentation in major depressive disorder: a double-blind, placebo-controlled study in patients with inadequate response to antidepressants. CNS Spectr. 2009;14:197–206. doi:10.1017/S1092852900020216
42. Fava M, Mischoulon D, Iosifescu D, et al. A double-blind, placebo-controlled study of aripiprazole adjunctive to antidepressant therapy among depressed outpatients with inadequate response to prior antidepressant therapy (ADAPT-A Study). Psychother Psychosom. 2012;81(2):87–97. doi:10.1159/000332050
43. Hobart M, Skuban A, Zhang P, et al. A randomized, placebo-controlled study of the efficacy and safety of fixed-dose brexpiprazole 2 mg/d as adjunctive treatment of adults with major depressive disorder. J Clin Psychiatry. 2018;79. doi:10.4088/JCP.17m12058
44. Hobart M, Skuban A, Zhang P, et al. Efficacy and safety of flexibly dosed brexpiprazole for the adjunctive treatment of major depressive disorder: a randomized, active-referenced, placebo-controlled study. Curr Med Res Opin. 2018;34:633–642. doi:10.1080/03007995.2018.1430220
45. Kamijima K, Higuchi T, Ishigooka J, et al. Aripiprazole augmentation to antidepressant therapy in Japanese patients with major depressive disorder: a randomized, double-blind, placebo-controlled study (ADMIRE study). J Affect Disord. 2013;151:899–905. doi:10.1016/j.jad.2013.07.035
46. Kamijima K, Kimura M, Kuwahara K, Kitayama Y, Tadori Y. Randomized, double-blind comparison of aripiprazole/sertraline combination and placebo/sertraline combination in patients with major depressive disorder. Psychiatry Clin Neurosci. 2018;72:591–601. doi:10.1111/pcn.12663
47. Leucht S, Fennema H, Engel RR, Kaspers-Janssen M, Szegedi A. Translating the HAM-D into the MADRS and vice versa with equipercentile linking. J Affective Disorders. 2018;226:326–331. doi:10.1016/j.jad.2017.09.042
48. Kobak KA, Williams JB, Jeglic E, Salvucci D, Sharp IR. Face-to-face versus remote administration of the Montgomery-Asberg depression rating scale using videoconference and telephone. Depress Anxiety. 2008;25:913–919. doi:10.1002/da.20392
49. Finniss DG, Kaptchuk TJ, Miller F, Benedetti F. Biological, clinical, and ethical advances of placebo effects. Lancet. 2010;375:686–695. doi:10.1016/S0140-6736(09)61706-2
50. Rutherford BR, Roose SP. A model of placebo response in antidepressant clinical trials. Am J Psychiatry. 2013;170:723–733. doi:10.1176/appi.ajp.2012.12040474
51. Curkovic M, Kosec A, Bamvita J-M, Dorvil H, Fleury M-J. Significance of participants’ expectations in managing the placebo effect in antidepressant research. Frontiers in Psychiatry. 2019;10:10. doi:10.3389/fpsyt.2019.00010
52. Kasper S, Dold M. Factors contributing to the increasing placebo response in antidepressant trials. World Psychiatry. 2015;14:304. doi:10.1002/wps.20245
53. Reif A, Bitter I, Buyze J, et al. Esketamine nasal spray versus quetiapine for treatment-resistant depression. N Engl J Med. 2023;389:1298–1309. doi:10.1056/NEJMoa2304145
54. Martinotti G, Vita A, Fagiolini A, et al. Real-world experience of esketamine use to manage treatment-resistant depression: a multicentric study on safety and effectiveness (REAL-ESK study). J Affect Disord. 2022;319:646–654. doi:10.1016/j.jad.2022.09.043
55. Martinotti G, Dell’Osso B, Di Lorenzo G, et al. Treating bipolar depression with esketamine: safety and effectiveness data from a naturalistic multicentric study on esketamine in bipolar versus unipolar treatment-resistant depression. Bipolar Disord. 2023;25:233–244. doi:10.1111/bdi.13296
56. Samalin L, Rothärmel M, Mekaoui L, et al. Esketamine nasal spray in patients with treatment-resistant depression: the real-world experience in the French cohort early-access programme. Int J Psychiatry Clin Pract. 2022;26:352–362. doi:10.1080/13651501.2022.2030757
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Clinical Relevance of Adjunctive Cariprazine Treatment in Patients with Major Depressive Disorder: Post Hoc Analyses from a Phase III Study
Papakostas GI, Masand PS, Clayton AH, Maletic V, Adams JL, Rekeda L, Singh MK, Kerolous M
Neuropsychiatric Disease and Treatment 2026, 22:561112
Published Date: 1 April 2026