Back to Journals » Journal of Hepatocellular Carcinoma » Volume 12
A Grading System of Intratumoral Tertiary Lymphoid Structure for Combined Hepatocellular-Cholangiocarcinoma: A Multicenter Pathological Study
Authors Wang H ![]() , Qian YW, Zhao Y, Sheng X, Xia CY, Chen HZ, Cong WM, He MX, Dong H
, Qian YW, Zhao Y, Sheng X, Xia CY, Chen HZ, Cong WM, He MX, Dong H ![]()
Received 23 September 2025
Accepted for publication 18 December 2025
Published 25 December 2025 Volume 2025:12 Pages 3011—3027
DOI https://doi.org/10.2147/JHC.S568933
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Mohamed Shaker
Han Wang,1,2,* You-Wen Qian,1,* Yun Zhao,3,* Xia Sheng,4 Chun-Yan Xia,5 Hong-Zhen Chen,6 Wen-Ming Cong,1 Miao-Xia He,2 Hui Dong1
1Department of Pathology, Eastern Hepatobiliary Surgery Hospital, Naval Medical University, Shanghai, People’s Republic of China; 2Department of Pathology, Changhai Hospital, Naval Medical University, Shanghai, People’s Republic of China; 3Department of Pathology, Huadong Hospital, Fudan University, Shanghai, People’s Republic of China; 4Department of Pathology, Minhang Hospital, Fudan University, Shanghai, People’s Republic of China; 5Department of Pathology, Changzheng Hospital, Naval Medical University, Shanghai, People’s Republic of China; 6Department of Pathology, Affiliated Hospital of Hangzhou Normal University, Hangzhou Normal University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Hui Dong, Department of Pathology, Eastern Hepatobiliary Surgery Hospital, Naval Medical University, Shanghai, People’s Republic of China, Tel +86 021-81875191, Email [email protected] Miao-Xia He, Department of Pathology, Changhai Hospital, Naval Medical University, Shanghai, People’s Republic of China, Tel +86 021-31162259, Email [email protected]
Purpose: Tertiary lymphoid structure (TLS) has been well-established across multiple tumor types for predicting efficacy of immunotherapy and prognostic evaluation. However, its role in combined hepatocellular-cholangiocarcinoma (cHCC-CCA) remains unclear. Refinement of TLS pathological assessment could potentially optimize postoperative management in these patients. This study aimed to develop a practical histopathological grading system of intratumoral TLS to improve prognostic stratification of cHCC-CCA patients.
Patients and Methods: A cohort of 310 cHCC-CCA patients undergoing hepatectomy with curative intent was analyzed. Three pathologists re-evaluated pathological slides to establish a four-tier TLS grading system: TLS 0 (absent), TLS 1 (immature TLS only), TLS 2a [single mature TLS (mTLS)], and TLS 2b (multiple mTLS). Associations with recurrence-free survival (RFS), overall survival (OS), early RFS (≤ 1 year), late RFS (> 1 year), and recurrence patterns were assessed. Predictive factors for TLS were also investigated.
Results: Patients were stratified into TLS 0 (29.4%), TLS 1 (51.6%), TLS 2a (6.8%), and TLS 2b (12.3%). Survival outcomes significantly correlated with TLS presence and maturation. Median RFS increased stepwise: 0.24 years (TLS 0), 0.49 years (TLS 1), 1.13 years (TLS 2a), and 1.16 years (TLS 2b) (P< 0.001). Median OS also improved progressively: 1.32 years (TLS 0), 2.20 years (TLS 1), 3.24 years (TLS 2a), and 10.04 years (TLS 2b) (P< 0.001). TLS presence was associated with increased extrahepatic recurrence. The TLS grading system emerged as an independent prognostic factor for RFS, OS, and early RFS. Smaller tumor diameter was the sole significant predictive factor for both TLS and mTLS.
Conclusion: This novel TLS grading system effectively stratifies prognosis in cHCC-CCA, with increasing intratumoral mTLS indicating better outcomes. This practical method can be integrated into routine pathological reporting to aid clinical decision-making.
Plain Language Summary: The TLS grading system proposed in this study is a histopathology-based, straightforward method which can provide more granular pathological information for patients with cHCC-CCA to facilitate prognostic stratification and has the potential to be applied in routine clinicopathological work.
Keywords: mixed hepatocellular cholangiocarcinoma, TLS, prognosis, pathological assessment, immunotherapy, early recurrence
Introduction
Combined hepatocellular-cholangiocarcinoma (cHCC-CCA) represents a rare tumor entity, accounting for 0.4–14.2% of primary liver cancers,1 and demonstrates poorer prognosis compared to hepatocellular carcinoma (HCC)2 and intrahepatic cholangiocarcinoma (iCCA).3 Surgical resection and liver transplantation remain the only methods proven to prolong survival for patients with cHCC-CCA.4 To date, cHCC-CCA is predominantly evaluated under the pathological diagnostic paradigm of iCCA, lacking an independent protocol.5 As pathologists, we hope to refine the histological diagnosis of cHCC-CCA to provide valuable prognostic parameters and enhance prognostic stratification, in order to offer more granular morphological information to optimize treatment selection.
The success of immunotherapy across multiple malignancies has prompted the clinical imperative for comprehensive immune microenvironment profiling. Tertiary lymphoid structure (TLS), as ectopic lymphocytic aggregates, contain B-cells, T-cells, and dendritic cells, which are typically organized into distinct functional compartments: a B-cell follicle mainly composed of naive B cells, surrounding a germinal center composed of highly proliferative B cells; and a T-cell area mainly composed of T-cells and dendritic cells.6 Just like its analog secondary lymphoid organ, TLS can also provide a specialized niche to maximize cell-cell contact, thereby enabling the generation of adaptive immune responses and facilitating the encounter between antigen-loaded antigen-presenting cells from tissues and naive lymphocytes derived from blood.7
TLS has been observed to be closely associated with improved prognosis and enhanced efficacy of immunotherapy in various malignancies8 and has garnered significant attention from oncology researchers.9 Previous studies have shown that HCC, iCCA, and cHCC-CCA exhibit distinct immune microenvironments. Specifically, HCC demonstrates higher myeloid cell infiltration compared to iCCA, while displaying lower proportions of T/NK cells.10 Furthermore, CD163+CD204+ tumor-associated macrophages of the immunosuppressive cells are less in cHCC-CCA than in HCC, whereas cHCC-CCA harbors higher levels of CD3+ T cells compared to iCCA.11 Moreover, intratumoral TLS correlates with reduced early recurrence risk12 and enhanced response to immunotherapy in HCC.13 Similarly, intratumoral TLS presence in iCCA was also confirmed to be associated with improved clinical outcomes.14,15 While TLS has shown prognostic significance in both HCC and iCCA, its role in cHCC-CCA remains undefined. Considering the limited TLS-related research in cHCC-CCA, we suggest a stratified TLS histopathological assessment system specifically tailored for cHCC-CCA should be well-established, in order to achieve a comprehensive evaluation for patients with this distinct tumor entity.
As such, we aim to conduct a multicenter study to establish a standardized histopathological grading system for TLS, incorporating localization patterns, maturation status, and number metrics, with the ultimate goal of developing an evidence-based prognostic algorithm for clinicians.
Materials and Methods
Patients
This retrospective study analyzed consecutive patients with primary cHCC-CCA who underwent hepatectomy with curative intent at six medical centers (Eastern Hepatobiliary Surgery Hospital, Changhai Hospital, Changzheng Hospital, Huadong Hospital, Minhang Hospital, and Affiliated Hospital of Hangzhou Normal University) between January 2013 and December 2017. The diagnostic criteria for cHCC-CCA were based on the 5th edition of the World Health Organization (WHO) Classification of Digestive System Tumors.5 The patients with recurrent cHCC-CCA, patients with neoadjuvant therapies, patients with pathological identification of heterologous differentiation components (eg, chondroid morphology), and patients without complete crucial clinical information were excluded from this study (Supplementary Figure 1).
Data Collection and Definitions
We collected comprehensive data from the electronic medical record system of the medical centers, including patient demographics, serological tests, surgical procedures, and pathological evaluation outcomes. Demographic information was recorded from the first admission. Serological results were gathered from the most recent tests prior to surgery. The hepatectomy techniques were categorized as anatomical and non-anatomical resections according to the Tokyo 2020 terminology of liver anatomy and resections.16 Gross pathological information (eg, tumor diameter, tumor number, surgical margin distance, macroscopic tumor thrombus) was documented based on the pathological reports. Three board-certified pathologists, blinded to patients’ clinical data, re-evaluated the histopathological slides to assess tumor differentiation, microvascular invasion (MVI),17 perineural invasion (PNI),18 TLS, and hepatic cirrhosis. All H&E-stained sections (4~6 tumor/peritumoral regions; 1~2 normal liver parenchyma) were analyzed per patient. For patients with multiple liver tumors, pathological analysis was based on the largest cHCC-CCA lesion. Tumor-node-metastasis (TNM) staging was performed using the American Joint Committee on Cancer Staging Manual (8th edition).19
TLS and Its Grading System
TLS histologically presents as an organized lymphocyte aggregate. Based on the presence or absence of germinal centers, TLS is classified into two categories: immature TLS (iTLS) and mature TLS (mTLS). Moreover, given that the prognostic significance and evaluation criteria of peritumoral TLS remain inconclusive (Supplementary Figure 2),20–22 this grading system focuses on the intratumoral TLS. The criteria for the established TLS grading system are detailed below: TLS 0: No TLS; TLS 1: only intratumoral iTLS; TLS 2: presence of intratumoral mTLS (TLS 2a: single intratumoral mTLS; TLS 2b: multiple intratumoral mTLS) (Figure 1). Immunohistochemical markers (eg, CD20 to identify B-cells, CD3 to detect T-cells, and CD21/CD23/CD35 to delineate dendritic cells) were selectively used only when the assessment of TLS maturity was ambiguous (Supplementary Figure 3).
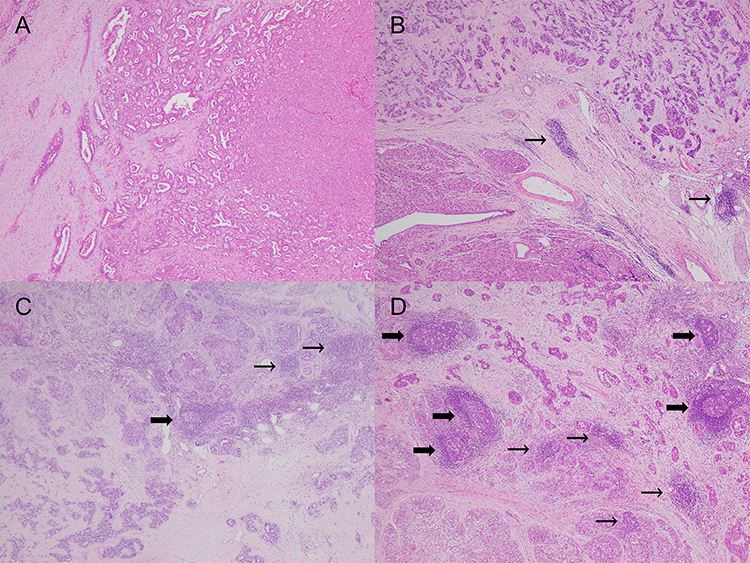 |
Figure 1 Representative histopathological images of different TLS grading in cHCC-CCA (40× magnification). (A) TLS 0; (B) TLS 1; (C) TLS 2a; (D) TLS 2b. Thin arrows: iTLS; Bold arrows: mTLS. Abbreviations: TLS, tertiary lymphoid structure; iTLS, immature TLS; mTLS, mature TLS; cHCC-CCA, combined hepatocellular-cholangiocarcinoma. |
Follow Up and Study Endpoints
The postoperative surveillance was implemented every 2–3 months during the initial 2-year period after surgery, progressing to 3–6 months intervals thereafter for all patients. A standardized monitoring regimen encompassed tumor marker analysis (α-fetoprotein and carbohydrate antigen 19–9), hepatitis B virus deoxyribonucleic acid load (limited to hepatitis B surface antigen [HBsAg]-positive patients), and abdominal imaging modalities (ultrasonography, computed tomography, or magnetic resonance imaging). We also collect the information of the application of postoperative adjuvant transarterial chemoembolization. The intervention was conducted between 1~3 months after hepatectomy, using a lipiodol and chemotherapeutic agents-based therapeutic protocol. Suspected recurrence, when detected through imaging or serum markers, activated multidisciplinary review to optimize therapeutic strategies according to systemic performance, hepatic functional capacity, and tumor burden parameters.
Clinical outcomes were measured through the following endpoints: 1) Recurrence-free survival (RFS), defined as the interval from surgery to histologically/radiologically confirmed relapse or last follow-up; 2) Overall survival (OS), spanning resection date to mortality or censoring; 3) Early RFS (≤1 year); and 4) Late RFS (>1 year). Recurrence patterns were categorized as intrahepatic (hepatic parenchymal or intrahepatic vascular or biliary involvement), extrahepatic (distant metastases or lymph node dissemination), or combined presentations, with the surveillance continuing until February 2025.
Statistical Analysis
Continuous variables were shown as mean ± standard deviation or median [interquartile range] and categorical variables were described as frequencies (percentages). Comparative analyses of continuous variables between cohorts were executed through parametric (Student’s t-test or one-way analysis of variance) or nonparametric equivalents (Mann–Whitney U or Kruskal–Wallis test). Categorical variables were evaluated using the χ2-test or Fisher’s exact probability method. The concordance among three pathologists was evaluated using Fleiss kappa coefficient. The strength of agreement was stratified as follows: poor (κ=0.01–0.20), limited (κ=0.21–0.40), moderate (κ=0.41–0.60), strong (κ=0.61–0.80), and exceptional concordance (κ=0.81–1.00). The Kaplan-Meier curve with the log-rank method was employed for survival analyses. Univariable and multivariable Cox regression modeling was utilized to identify survival risk factors. The discrimination capacity of models was evaluated via Harrell’s C-index. Univariable and multivariable logistic regression analyses were used to screen for TLS-related predictive factors. The predictive effect was further validated by the value of area under the curve. The variables showing marginal associations (P<0.2) in univariable screenings were included in multivariable analyses. The multivariable models were visualized through forest plots. A P value less than 0.05 was determined to be statistically significant. All computations were implemented using R version 4.4.2 (R Foundation, Vienna).
Results
Baseline Characteristics
A total of 310 patients with cHCC-CCA were included in this study. Among them, 271 (87.4%) and 39 (12.6%) patients were male and female, respectively. The mean ± standard deviation age of all patients was 52.7 ± 10.3 years. The median tumor diameter was 4.4 cm [2.8 cm, 6.9 cm], with 208 and 102 patients presenting solitary and multifocal tumors, respectively. Two hundred and thirty-six patients (76.1%) were classified as TNM stage I–II and 74 (23.9%) patients were classified as stage III–IV. The numbers and percentages of the TLS 0, TLS 1, TLS 2a, and TLS 2b groups were 91 (29.4%), 160 (51.6%), 21 (6.8%) and 38 (12.3%), respectively. The Fleiss kappa coefficient among three pathologists was 0.823, indicating exceptional concordance. The percentages of cHCC-CCA patients with TLS and mTLS were 70.6% and 19.0%, respectively. All patients with mTLS were also found to have iTLS. The baseline features of all the groups are shown in Table 1. Patients with TLS were associated with significantly lower direct bilirubin, aspartate amino transferase, γ-glutamyl transpeptidase, alkaline phosphatase, lactate dehydrogenase, international normalized ratio, prothrombin time, and carcinoembryonic antigen, higher albumin, prealbumin, lymphocyte, and red blood cell, lower percentage of diabetes, HBV DNA load ≤1×103IU/mL, multiple tumor, and TNM stage III–IV, as well as smaller tumor diameter when compared with patients without TLS (all P<0.05). The levels of neutrophil and tumor diameter significantly and gradually decline with the TLS grading.
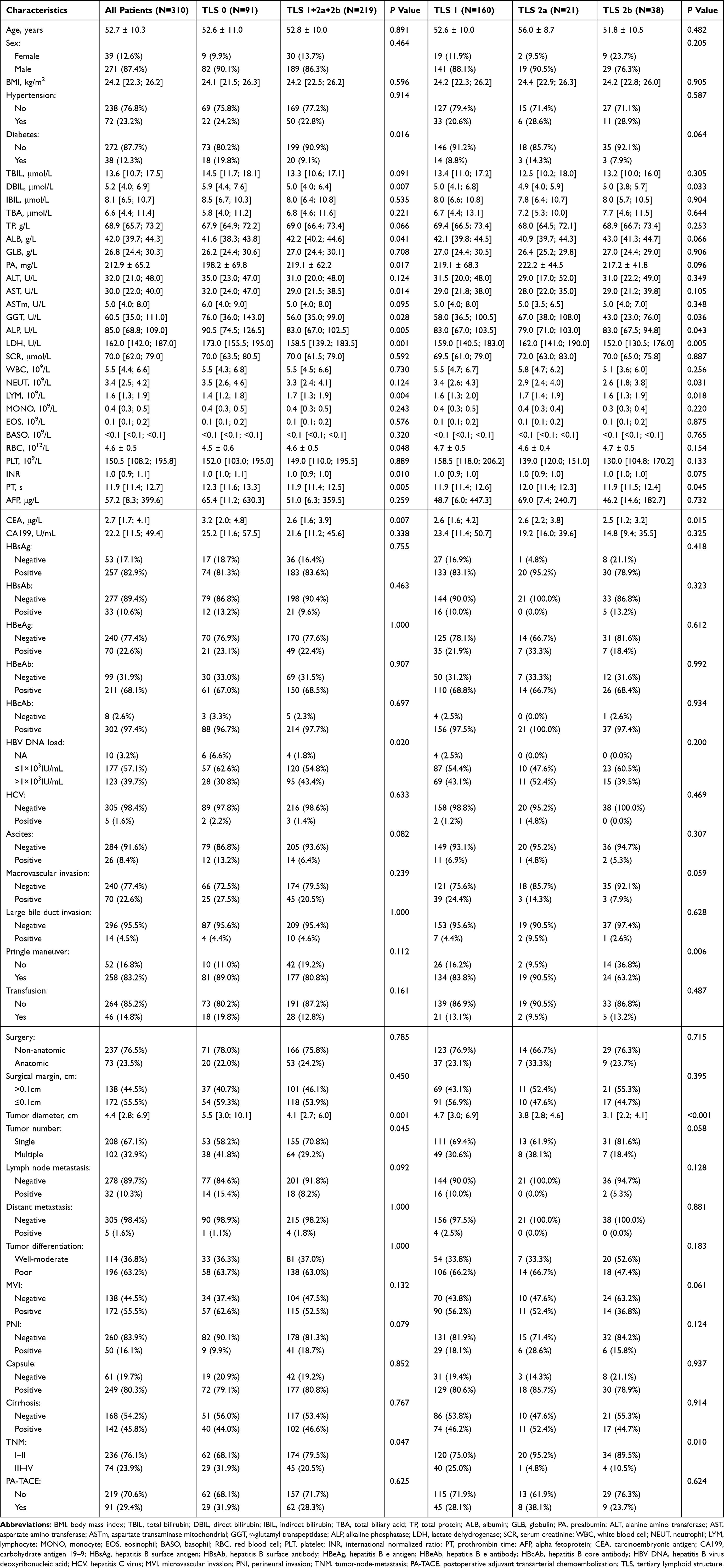 |
Table 1 Baseline Characteristics of All Patients |
Impact of TLS and Its Grading System on the Prognosis and Recurrence Pattern
The median follow-up time, median RFS, and median OS for all the 310 patients were 8.52 years [7.61 years, 9.81 years], 0.43 years [0.14 years, 2.02 years], and 2.20 years [0.78 years, 10.04 years], respectively. There were 7 patients who experienced postoperative 30-day death (constituent percentage: 2.26%).
The median RFSs of TLS 0 group (TLS negative) and TLS 1+2a+2b group (TLS positive) were 0.24 years [0.11 years, 0.89 years] and 0.72 years [0.18 years, 2.53 years], respectively (Figure 2A, P=0.004). The median OSs of corresponding groups were 1.32 years [0.55 years, 3.31 years] and 2.67 years [1.14 years, not reached], respectively (Figure 2B, P<0.001). Early RFS was significantly different between the two groups (Figure 2C, P<0.001) but not for late RFS (Figure 2D, P=0.532). The 1-, 2-, 3- and 5-year RFS rates for the patients in the corresponding two groups were 23.3%, 19.6%, 15.9%, 11.9% vs 40.4%, 27.7%, 22.1%, 19.0%, respectively. The corresponding OS rates were 55.5%, 37.0%, 28.8%, 21.6% vs 76.3%, 57.5%, 45.9%, 38.0%, respectively.
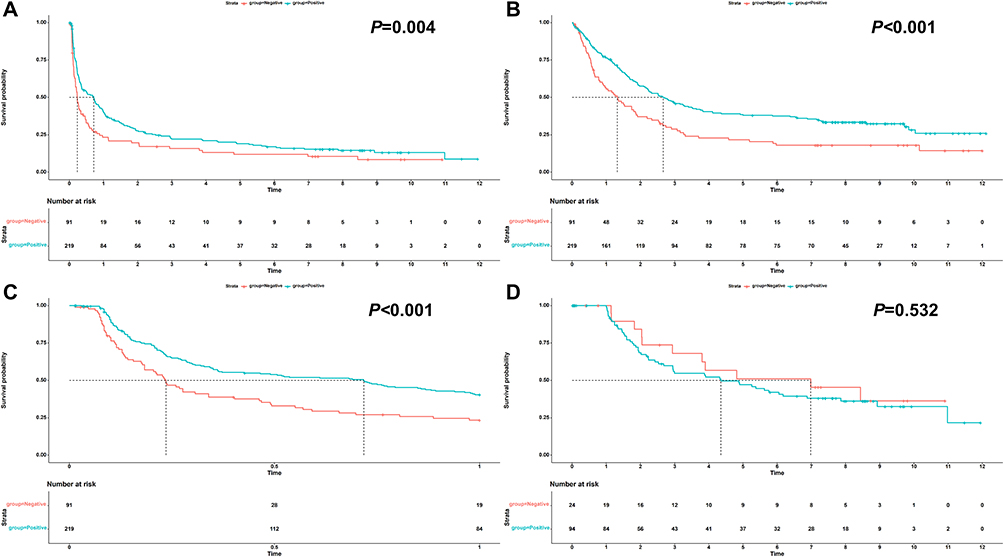 |
Figure 2 Impact of TLS on the prognosis of cHCC-CCA. (A) RFS; (B) OS; (C) early RFS; (D) late RFS. Abbreviations: TLS, tertiary lymphoid structure; cHCC-CCA, combined hepatocellular-cholangiocarcinoma; RFS, recurrence-free survival; OS, overall survival. |
The median RFSs of TLS 0 group (absence of TLS), TLS 1 group (presence of iTLS) and TLS 2 group (presence of mTLS) were 0.24 years [0.11 years, 0.89 years], 0.49 years [0.15 years, 2.02 years], and 1.13 years [0.24 years, 6.17 years], respectively (Figure 3A, P=0.002, TLS 0 vs TLS 1, P=0.051; TLS 0 vs TLS 2, P<0.001; TLS 1 vs TLS 2, P=0.021). The median OSs of corresponding groups were 1.32 years [0.55 years, 3.31 years], 2.20 years [0.86 years, not reached], and 4.11 years [1.97 years, 10.04 years], respectively (Figure 3B, P<0.001, TLS 0 vs TLS 1, P=0.009; TLS 0 vs TLS 2, P<0.001; TLS 1 vs TLS 2, P=0.047). Early RFS was significantly different among the three groups (Figure 3C, P<0.001, TLS 0 vs TLS 1, P=0.010; TLS 0 vs TLS 2, P<0.001; TLS 1 vs TLS 2, P=0.013) but not for late RFS (Figure 3D, P=0.745, TLS 0 vs TLS 1, P=0.464; TLS 0 vs TLS 2, P=0.725; TLS 1 vs TLS 2, P=0.658). The 1-, 2-, 3- and 5-year RFS rates for the patients in the three groups were 23.3%, 19.6%, 15.9%, 11.9% vs 35.5%, 25.6%, 19.3%, 15.7% vs 54.3%, 33.7%, 30.0%, 28.1%, respectively. The corresponding OS rates were 55.5%, 37.0%, 28.8%, 21.6% vs 71.5%, 51.5%, 42.1%, 34.6% vs 89.6%, 73.8%, 56.2%, 47.1%, respectively.
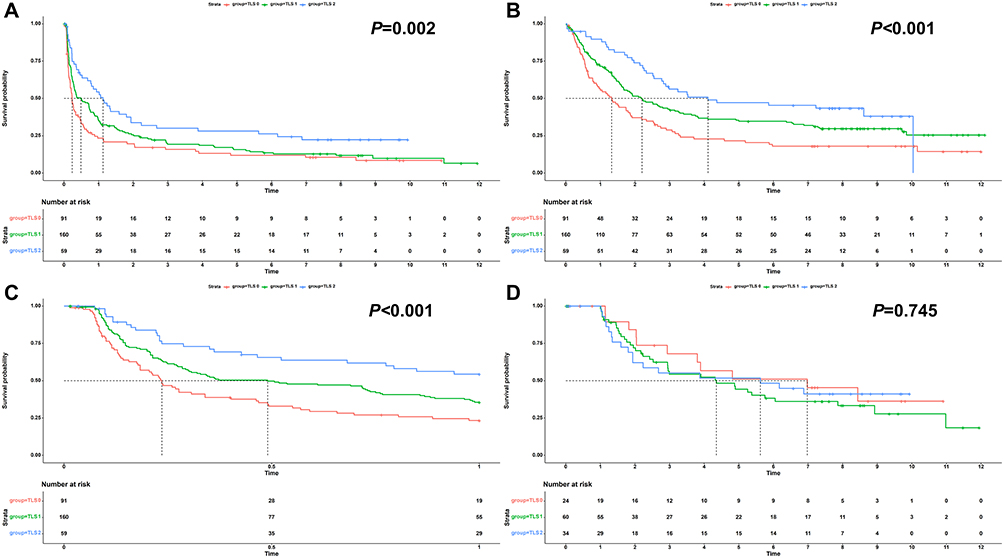 |
Figure 3 Impact of iTLS and mTLS on the prognosis of cHCC-CCA. (A) RFS; (B) OS; (C) early RFS; (D) late RFS. Abbreviations: iTLS, immature tertiary lymphoid structure; mTLS, mature tertiary lymphoid structure; cHCC-CCA, combined hepatocellular-cholangiocarcinoma; RFS, recurrence-free survival; OS, overall survival. |
The median RFSs of the TLS 0, TLS 1, TLS 2a, TLS 2b groups were 0.24 years [0.11 years, 0.89 years], 0.49 years [0.15 years, 2.02 years], 0.80 years [0.23 years, 1.60 years], and 1.16 years [0.29 years, not reached], respectively (Figure 4A, P=0.003, TLS 0 vs TLS 1, P=0.051; TLS 0 vs TLS 2a, P=0.149; TLS 0 vs TLS 2b, P<0.001; TLS 1 vs TLS 2a, P=0.629; TLS 1 vs TLS 2b, P=0.010; TLS 2a vs TLS 2b, P=0.174). The corresponding median OSs were 1.32 years [0.55 years, 3.31 years], 2.20 years [0.86 years, not reached], 3.24 years [1.97 years, 8.61 years], and 10.04 years [2.14 years, 10.04 years], respectively (Figure 4B, P<0.001, TLS 0 vs TLS 1, P=0.009; TLS 0 vs TLS 2a, P=0.088; TLS 0 vs TLS 2b, P<0.001; TLS 1 vs TLS 2a, P=0.737; TLS 1 vs TLS 2b, P=0.020; TLS 2a vs TLS 2b, P=0.105). Early RFS was significantly different among the four groups (Figure 4C, P<0.001, TLS 0 vs TLS 1, P=0.010; TLS 0 vs TLS 2a, P=0.021; TLS 0 vs TLS 2b, P<0.001; TLS 1 vs TLS 2a, P=0.233; TLS 1 vs TLS 2b, P=0.019; TLS 2a vs TLS 2b, P=0.532) but not for late RFS (Figure 4D, P=0.335, TLS 0 vs TLS 1, P=0.464; TLS 0 vs TLS 2a, P=0.151; TLS 0 vs TLS 2b, P=0.770; TLS 1 vs TLS 2a, P=0.281; TLS 1 vs TLS 2b, P=0.248; TLS 2a vs TLS 2b, P=0.153). The 1-, 2-, 3- and 5-year RFS rates for the patients in the four groups were 23.3%, 19.6%, 15.9%, 11.9% vs 35.5%, 25.6%, 19.3%, 15.7% vs 50.0%, 15.0%, 15.0%, 15.0% vs 56.7%, 44.8%, 38.8%, 35.8%, respectively. The corresponding OS rates were 55.5%, 37.0%, 28.8%, 21.6% vs 71.5%, 51.5%, 42.1%, 34.6% vs 95.2%, 70.2%, 50.1%, 30.1% vs 86.6%, 75.8%, 59.4%, 56.6%, respectively.
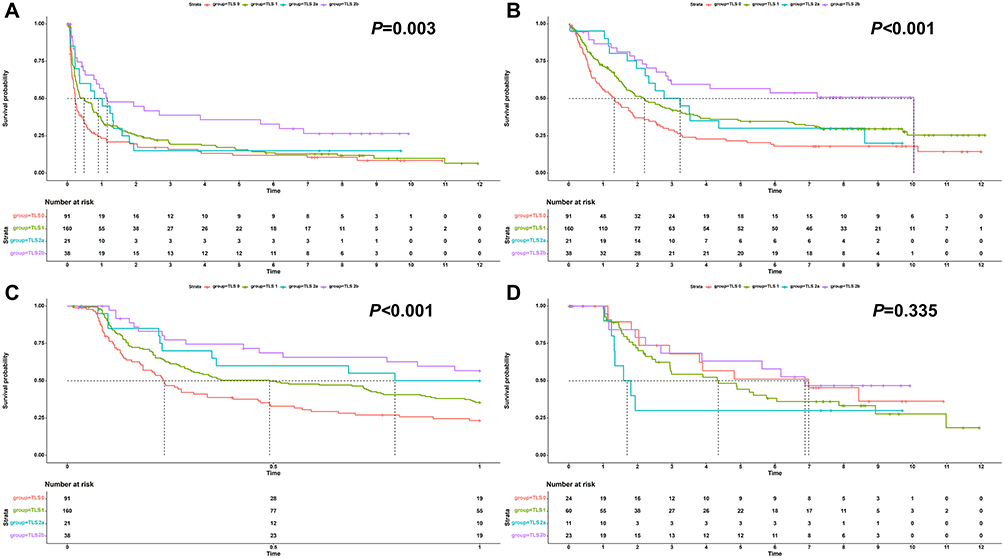 |
Figure 4 Impact of TLS grading system on the prognosis of cHCC-CCA. (A) RFS; (B) OS; (C) early RFS; (D) late RFS. Abbreviations: TLS, tertiary lymphoid structure; cHCC-CCA, combined hepatocellular-cholangiocarcinoma; RFS, recurrence-free survival; OS, overall survival. |
For hepatitis B virus-infected patients (HBsAg-positive patients, N=257), whether stratified by TLS negative/positive (Supplementary Figure 4), TLS 0/1/2 classification (Supplementary Figure 5), or TLS 0/1/2a/2b classification (Supplementary Figure 6), similar statistical outcomes were consistently observed. Statistically significant differences were demonstrated in RFS, OS, and early RFS between groups. However, there was no differences in prognosis for the HBsAg-negative patients (N=53, Supplementary Figures 7−9).
The comparison of prognosis shows no significant difference between the patients with and without peritumoral mTLS (mTLS adjacent to the tumor margin, Supplementary Figure 10).
Two hundred and fifty-six patients were recorded with recurrence patterns. The recurrence patterns of patients with and without TLS are shown in Figure 5. The patients without TLS had a higher incidence of intrahepatic recurrence (P=0.012).
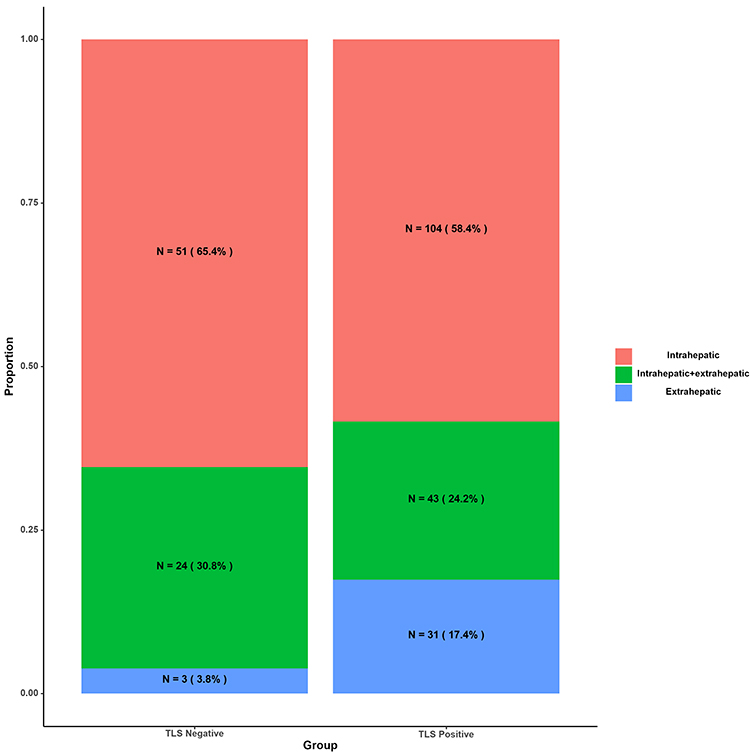 |
Figure 5 Recurrence patterns of cHCC-CCA patients with absence or pretense of TLS. Abbreviations: cHCC-CCA, combined hepatocellular-cholangiocarcinoma; TLS, tertiary lymphoid structure. |
Prognostic Factors of RFS, OS, Early RFS, and Late RFS
The results of univariable Cox regression analyses of RFS, OS, early RFS, and late RFS are shown in Supplementary Tables 1−4. Multivariable analysis confirmed that age, macrovascular invasion, tumor number, tumor differentiation, MVI, PNI, and TLS grading system were independent factors for RFS [Figure 6A, C-index=0.703, 95% confidence interval (CI): 0.672–0.734]. Globulin, macrovascular invasion, tumor diameter, tumor number, MVI, PNI, and TLS grading system were independent factors for OS (Figure 6B, C-index=0.725, 95% CI: 0.692–0.758). Age, lymphocyte, tumor number, tumor differentiation, MVI, PNI, and TLS grading system were independent factors for early RFS (Figure 6C, C-index=0.712, 95% CI: 0.677–0.747). Albumin, basophil, tumor number, and PNI were independent factors for late RFS (Figure 6D, C-index=0.663, 95% CI: 0.585–0.741).
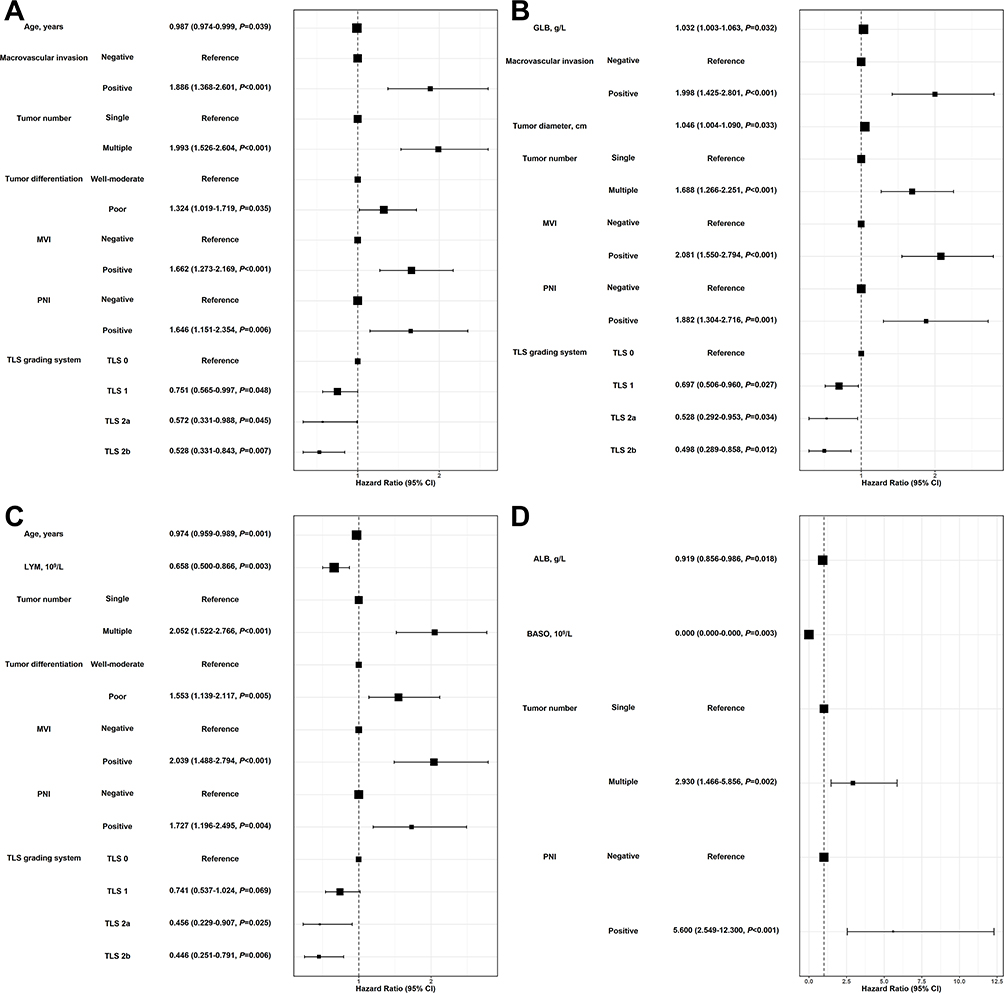 |
Figure 6 Multivariable Cox regression analysis of the prognosis of cHCC-CCA patients. (A) RFS; (B) OS; (C) early RFS; (D) late RFS. Abbreviations: cHCC-CCA, combined hepatocellular-cholangiocarcinoma; RFS, recurrence-free survival; OS, overall survival; MVI, microvascular invasion; PNI, perineural invasion; GLB, globulin; LYM, lymphocyte; ALB, albumin; BASO, basophil; CI, confidence interval. |
Predictive Factors on TLS
The results of univariable logistic regression analysis of TLS-related predictive factors and mTLS-related predictive factors are shown in Supplementary Tables 5 and 6, respectively. Multivariable analysis suggested that diabetes, prothrombin time, tumor diameter, and PNI were independent factors for TLS (Figure 7, area under the curve: 0.705). It was challenging to construct a multivariable predictive model of mTLS with all included variables having a P value less than 0.05. Tumor diameter was the optimal predictive factor (area under the curve: 0.698).
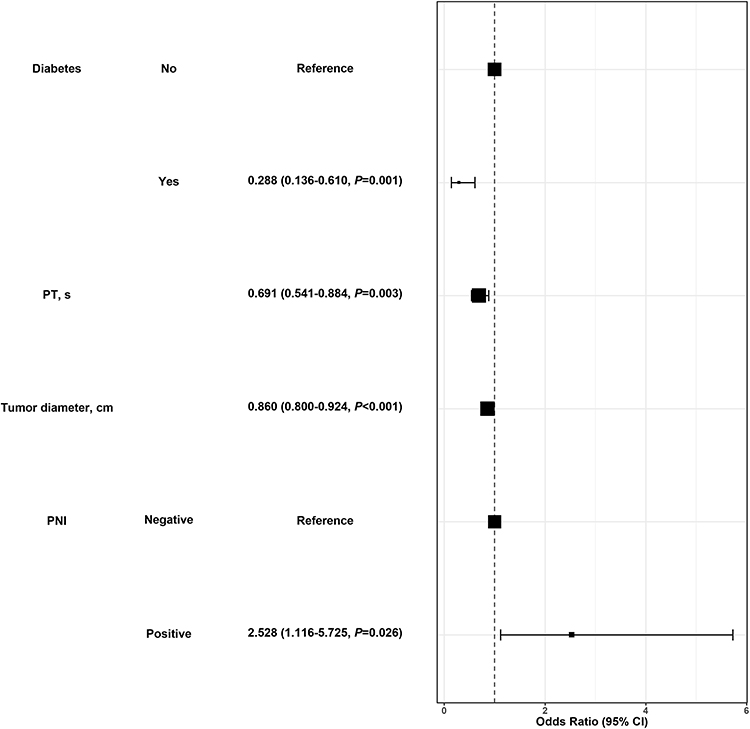 |
Figure 7 Multivariable logistic analysis of the predictive factors of TLS. Abbreviations: TLS, tertiary lymphoid structure; PT, prothrombin time; PNI, perineural invasion. |
Discussion
Because of its heterogeneous composition and aggressive behavior, cHCC-CCA still lacks a systematic diagnostic and therapeutic paradigm.23 For pathologists, identifying easily interpretable histopathological parameters that correlate with prognosis and treatment efficacy remains a critical focus for this tumor entity. In recent years, TLS has gradually transitioned from research concept to routine pathological practice. TLS is a pathological phenomenon of ectopic lymphoid aggregates induced by tumor that is indicative of favorable prognosis across various malignancies.24,25 Moreover, a study has shown that the presence of TLS often indicates more tumor-infiltrating lymphocytes, CD8+ T cells, and higher PD-L1 expression levels, which are typically associated with enhanced efficacy of immunotherapy.26 Based on our previous study27 and another study from a Chinese team,28 cHCC-CCA was also confirmed to have these correlations, which drive us to develop a straightforward, practical, and cost-effective TLS grading system based solely on histology in order to realize bench to bedside. Leveraging a large-scale multicenter cohort, this work aims to empower pathologists in delivering granular pathological insights to stratify the clinical outcomes of cHCC-CCA patients, ultimately supporting clinical decision-making.
During the pathological evaluation of TLS and establishment of the histopathological grading system, our team reached three consensus points. First, if iTLS is continuously subclassified into vague, ill-defined clusters of lymphocytes or round-shaped clusters of lymphocytes without germinal center formation, diagnostic discordance frequently arises among pathologists due to interpretive variability in assessing the morphology and dimensions of lymphocyte aggregates. In contrast, the interpretation of mTLS exhibits excellent interobserver consistency, and even when disagreements occur, they can be resolved through delineation of the follicular dendritic cells via CD21, CD23, and CD35 immunohistochemical staining. Therefore, we propose that binary classification of TLS maturity (iTLS vs mTLS) offers superior feasibility in clinical practice. Second, previous studies have confirmed that the peritumoral TLS have the significance of indicating a better21,22 or worse29 prognosis for HCC patients. Based on our observations, cHCC-CCA frequently shows variable degrees of band-like distributed immune cells along the tumor edge, which creates ambiguity about whether this phenomenon should be classified as iTLS. Consequently, our investigation only explored the prognostic impact of peritumoral mTLS, but no significant prognostic association was found. Based on these findings, our histological grading system focuses on intratumoral TLS. Third, the majority of tumors included in this study underwent a standardized seven-point baseline sampling30 which is recommended by China Liver Cancer Guidelines for the Diagnosis and Treatment of Hepatocellular Carcinoma,31 ensuring generalizable applicability across medical centers. We emphasize that this TLS grading system should therefore be implemented synergistically with this sampling protocol. Based on this consensus, we established a TLS grading system incorporating three histopathological parameters: distribution, maturation status, and quantity of TLS. Few studies have integrated TLS characteristics into a grading system. Most existing research employed complex scoring strategies for TLS stratification;14,32,33 these approaches pose significant implementation challenges in clinical practice and may increase interobserver variability. In contrast, our grading system enhances clinical utility through streamlined evaluation of the most operationally feasible parameters.
Survival analyses validated this grading system as an effective prognostic stratification tool for cHCC-CCA patients. The maturation and density of TLS significantly predicted better clinical outcomes. Specifically, compared to TLS-negative patients, iTLS (TLS 1 group) demonstrated marginally significant improvement in RFS and OS, while mature TLS (TLS 2 group) showed statistically superior RFS and OS. The prognosis of cHCC-CCA patients showed a stepwise improvement pattern based on this grading system. TLS-mediated prognostic benefits notably manifested in early RFS. Interestingly, previous studies have shown diverging perspectives regarding the definition of early recurrence of HCC, with some proposing a 2-year threshold34,35 while others advocated for a 1-year criterion.36,37 Based on our subgroup analyses, TLS2 group revealed comparable 1-year early RFS benefits between the single mTLS (TLS 2a) and multiple mTLS (TLS 2b) groups. However, the recurrence-preventive effect of TLS suddenly diminished after 1 year in TLS 2a group, with subsequent clustered recurrence. Based on these observations, we propose defining early RFS as 1 year rather than 2 years for cHCC-CCA management. Another noteworthy result was that although patients with TLS had a lower recurrence rate, they were more prone to extrahepatic recurrence compared to those without TLS. This seems contradictory to the conventional understanding that extrahepatic recurrence is more aggressive. Regarding this result, previous studies found that during the formation and maturation of TLS, immune cell infiltration and aggregation are predominantly mediated by the proliferation of high endothelial venules. However, tumor cells can induce structural remodeling of high endothelial venules, creating a microenvironment conducive to tumor metastasis.38 Additionally, ectopic lymphatic vessels can form within the tumor, which can transport tumor-derived factors to facilitate the establishment of pre-metastatic niches.39 Therefore, TLS-positive patients may have a richer distribution of pro-metastatic vascular within the tumor, which can facilitate lymphovascular invasion that leads to distant metastasis. Therefore, we recommend that TLS-positive cHCC-CCA patients should undergo more comprehensive imaging evaluations to avoid missing potential distant recurrences.
Multivariable analysis revealed that the absence of diabetes, lower prothrombin time, smaller tumor diameter, and the presence of PNI were positively correlated with TLS detection in patients with cHCC-CCA. First, the absence of diabetes and lower prothrombin time reflect milder steatotic liver disease and hepatitis-related fibrosis, respectively, indicating better liver condition. This suggests that patients with a normal liver are more likely to form structured anti-tumor immune responses compared to patients with chronic inflammation. Second, smaller tumor diameter was the only common significant predictor for both TLS and mTLS, implying that TLS are more likely to emerge in early cHCC-CCA and inhibit tumor progression. However, the failure to construct a multivariable model for mTLS highlights the need for more quantifiable and obtainable preoperative parameters to improve prediction accuracy. Third, the positive correlation between PNI and TLS detection was unexpected. Our analysis showed that TLS 2a group had the highest rate of PNI and the presence of PNI is closely associated with tumor involvement in the perihilar region.18 The perihilar area is a convergence zone for lymphatic drainage and often contains inherent lymphocyte aggregates,40 which were also classified as TLS or mTLS during diagnosis. Whether such lymphoid aggregates should be defined as TLS requires further investigation. This observation may also explain the concentrated recurrence around 1 year in the TLS 2a group, suggesting that this group contains a subset of patients with PNI and poor prognosis.
As far as we know, this study represents the first multicenter study to comprehensively investigate the prognostic significance of TLS in cHCC-CCA patients, and establishes a histopathological grading system that effectively stratifies RFS and OS with favorable clinicopathological applicability and feasibility. For cHCC-CCA patients lacking TLS, clinicians should implement more active postoperative anti-recurrence interventions and adopt more frequent imaging surveillance with liver-focused evaluation protocols. For TLS-positive cHCC-CCA patients, immunotherapy could be considered as postoperative adjuvant therapy but must be accompanied by comprehensive radiological assessments for detecting potential extrahepatic metastases. Given the limited treatment options for cHCC-CCA, this TLS grading system may inform rational patient selection strategies for future immunotherapy clinical trials.
However, there are still some limitations: First, most of the patients in this study had hepatitis B virus infection. Our study further validated the efficacy of this TLS grading system in HBsAg-positive patients. However, in HBsAg-negative patients, due to limited sample size and heterogeneous etiological profiles, no statistically significant differences were observed. Therefore, further studies are still required to validate the value of this histopathological grading system in cHCC-CCA patients with other etiologies. Second, we conducted Cox regression analyses to develop multivariable prognostic models for RFS, OS, early RFS, and late RFS. Although this methodology is well-established, emerging studies have explored alternative approaches to explore risk factors of clinical prognosis,41,42 and their clinical applicability and validity warrant further investigation in future research. Third, due to the limitation of the study period, there was an inevitable lack of application of immune checkpoint inhibitors among the included patients, which restricts the exploration of the correlations between our TLS grading system and the efficacy of immunotherapy. Immunotherapy has been the first-line treatment for advanced HCC and iCCA31 and is gradually extending to the comprehensive management of primary liver cancer. Emerging studies suggest that TLS may serve as a critical indicator for therapeutic response of neoadjuvant immunotherapy in HCC.43 Recent evidence also demonstrated that the value of TLS in predicting responses to postoperative adjuvant immunotherapy also showed significant potential in HCC patients.13 Therefore, we recommend incorporating TLS assessment into routine pathological reporting for all primary liver cancer patients. Fourth, the inherent rarity of cHCC-CCA constrained the subgroup sample sizes. Consequently, this TLS grading system still necessitates validation via large-scale, multi-institutional prospective studies to establish its clinical applicability.
Conclusion
Based on the maturity and quantity of intratumoral TLS, we developed a four-tier histopathological grading system of TLS and validated its prognostic discrimination in a large multicenter cohort of patients with cHCC-CCA. In contrast, the prognostic significance of peritumoral mTLS in cHCC-CCA patients remains unclear. Particular attention should be given to identifying and evaluating TLS adjacent to nerves within the perihilar area, due to its unclear prognostic significance. Using one year as the cutoff value for early recurrence in cHCC-CCA was demonstrated to be clinically meaningful based on prognostic trends with different TLS grading. Although the presence of TLS represented a declined recurrence rate, it also suggested a higher likelihood of extrahepatic recurrence. Therefore, these patients should undergo more comprehensive postoperative monitoring. Only smaller tumor diameter correlated positively with mTLS. This TLS grading system demonstrates strong clinical utility in diagnostic practice by enabling refined prognostic stratification in cHCC-CCA and may support future immunopathological evaluation. We recommend integrating this system into routine diagnostic practice for cHCC-CCA to provide more granular pathological information for clinical decision-making.
Abbreviations
cHCC-CCA, combined hepatocellular-cholangiocarcinoma; HCC, hepatocellular carcinoma; iCCA, intrahepatic cholangiocarcinoma; TLS, tertiary lymphoid structure; WHO, World Health Organization; MVI, microvascular invasion; PNI, perineural invasion; TNM, tumor-node-metastasis; iTLS, immature TLS; mTLS, mature TLS; RFS, recurrence-free survival; OS, overall survival.
Data Sharing Statement
The data that support the results of this study are available from the corresponding author (Dr. Hui Dong, E-mail: [email protected]; Dr. Miao-Xia He, E-mail: [email protected]) on reasonable request.
Ethics Approval and Informed Consent
The study protocol complied with the Declaration of Helsinki and was approved by the Institutional Review Board of Eastern Hepatobiliary Surgery Hospital (EHBHKY2022-H010-P001) and confirmed by other centers. Written informed consent for research was obtained from all patients preoperatively.
Funding
We received funding from the Noncommunicable Chronic Diseases-National Science and Technology Major Project (No. 2023ZD0500100), Shanghai Leading Talent Program of Eastern Talent Plan (No. BJWS2024084), Shanghai Municipal Health Commission Seed Program for Research and Translation of New Medical Technologies (NO. 2024ZZ1026), Shanghai Science and Technology Innovation Action Plan-Medical Innovation Research Project (No. 22Y11908700), Naval Medical University Basic Medical Research Project (No. 2023NQ095), and Take-off Project Talent Program of EHBH (No. TF2024XSJJ02).
Disclosure
The author(s) report no conflicts of interest in this work.
References
1. Schizas D, Mastoraki A, Routsi E, et al. Combined hepatocellular-cholangiocarcinoma: an update on epidemiology, classification, diagnosis and management. Hepatobiliary Pancreat Dis Int. 2020;19(6):515–523. doi:10.1016/j.hbpd.2020.07.004
2. Tang Y, Wang L, Teng F, Zhang T, Zhao Y, Chen Z. The clinical characteristics and prognostic factors of combined hepatocellular carcinoma and cholangiocarcinoma, hepatocellular carcinoma and intrahepatic cholangiocarcinoma after surgical resection: a propensity score matching analysis. Int J Med Sci. 2021;18(1):187–198. doi:10.7150/ijms.50883
3. Song P, Midorikawa Y, Nakayama H, et al. Patients’ prognosis of intrahepatic cholangiocarcinoma and combined hepatocellular-cholangiocarcinoma after resection. Cancer Med. 2019;8(13):5862–5871. doi:10.1002/cam4.2495
4. Ye L, Schneider JS, Ben Khaled N, et al. Combined hepatocellular-cholangiocarcinoma: biology, diagnosis, and management. Liver Cancer. 2024;13(1):6–28. doi:10.1159/000530700
5. WHO Classification of Tumours Editorial Board. WHO Classification of Tumours, Digestive System Tumours.
6. Engelhard VH, Rodriguez AB, Mauldin IS, Woods AN, Peske JD, Slingluff CL. Immune cell infiltration and tertiary lymphoid structures as determinants of antitumor immunity. J Immunol. 2018;200(2):432–442. doi:10.4049/jimmunol.1701269
7. Schumacher TN, Thommen DS. Tertiary lymphoid structures in cancer. Science. 2022;375(6576):eabf9419. doi:10.1126/science.abf9419
8. Sautès-Fridman C, Petitprez F, Calderaro J, Fridman WH. Tertiary lymphoid structures in the era of cancer immunotherapy. Nat Rev Cancer. 2019;19(6):307–325. doi:10.1038/s41568-019-0144-6
9. Peyraud F, Guegan JP, Vanhersecke L, et al. Tertiary lymphoid structures and cancer immunotherapy: from bench to bedside. Med. 2025;6(1):100546. doi:10.1016/j.medj.2024.10.023
10. Jiang S, Lu H, Pan Y, et al. Characterization of the distinct immune microenvironments between hepatocellular carcinoma and intrahepatic cholangiocarcinoma. Cancer Lett. 2024;588:216799. doi:10.1016/j.canlet.2024.216799
11. Yagi N, Suzuki T, Mizuno S, et al. Component with abundant immune-related cells in combined hepatocellular cholangiocarcinoma identified by cluster analysis. Cancer Sci. 2022;113(5):1564–1574. doi:10.1111/cas.15313
12. Calderaro J, Petitprez F, Becht E, et al. Intra-tumoral tertiary lymphoid structures are associated with a low risk of early recurrence of hepatocellular carcinoma. J Hepatol. 2019;70(1):58–65. doi:10.1016/j.jhep.2018.09.003
13. Su JY, Li JR, Pan LX, et al. Tertiary lymphoid structures in HCC: influence on immune cell profiles in tumors and on efficacy of adjuvant PD-1 inhibitor therapy after hepatectomy. Hepatology. 2025. doi:10.1097/hep.0000000000001433
14. Ding GY, Ma JQ, Yun JP, et al. Distribution and density of tertiary lymphoid structures predict clinical outcome in intrahepatic cholangiocarcinoma. J Hepatol. 2022;76(3):608–618. doi:10.1016/j.jhep.2021.10.030
15. Shang T, Jiang T, Lu T, et al. Tertiary lymphoid structures predict the prognosis and immunotherapy response of cholangiocarcinoma. Front Immunol. 2023;14:1166497. doi:10.3389/fimmu.2023.1166497
16. Wakabayashi G, Cherqui D, Geller DA, et al. The Tokyo 2020 terminology of liver anatomy and resections: updates of the Brisbane 2000 system. J Hepatobiliary Pancreat Sci. 2022;29(1):6–15. doi:10.1002/jhbp.1091
17. Wang H, Chen JJ, Yin SY, et al. A grading system of microvascular invasion for patients with hepatocellular carcinoma undergoing liver resection with curative intent: a multicenter study. J Hepatocell Carcinoma. 2024;11:191–206. doi:10.2147/jhc.S447731
18. Wang H, Zhou YY, Chen HZ, et al. Perineural invasion as a prognostic determinant in combined hepatocellular-cholangiocarcinoma: a multicenter pathological study. J Gastrointest Surg. 2025;29(9):102155. doi:10.1016/j.gassur.2025.102155
19. Chun YS, Pawlik TM, Vauthey JN. Edition of the AJCC cancer staging manual: pancreas and hepatobiliary cancers. annals of surgical oncology. Ann Surg Oncol. 2018;25(4):845–847. doi:10.1245/s10434-017-6025-x
20. Hu L, Li X, Yang C, Zhou B, Du C, Jiang N. Prognostic value of tertiary lymphoid structures in hepatocellular carcinoma: a meta-analysis and systematic review. Front Immunol. 2024;15:1390938. doi:10.3389/fimmu.2024.1390938
21. Li H, Liu H, Fu H, et al. Peritumoral tertiary lymphoid structures correlate with protective immunity and improved prognosis in patients with hepatocellular carcinoma. Front Immunol. 2021;12:648812. doi:10.3389/fimmu.2021.648812
22. Long S, Li M, Chen J, et al. Spatial patterns and MRI-based radiomic prediction of high peritumoral tertiary lymphoid structure density in hepatocellular carcinoma: a multicenter study. J Immunother Cancer. 2024;12(12):e009879. doi:10.1136/jitc-2024-009879
23. Chu KJ, Kawaguchi Y, Wang H, Jiang XQ, Hasegawa K. Update on the diagnosis and treatment of combined hepatocellular cholangiocarcinoma. J Clin Transl Hepatol. 2024;12(2):210–217. doi:10.14218/jcth.2023.00189
24. Li X, Zhang X, Cao Z, et al. Tertiary lymphoid structures: allies of cancer immunotherapy. Immunology. 2025. doi:10.1111/imm.70020
25. Wang H, Qian YW, Dong H, Cong WM. Pathologic assessment of hepatocellular carcinoma in the era of immunotherapy: a narrative review. Hepatobiliary Surg Nutr. 2024;13(3):472–493. doi:10.21037/hbsn-22-527
26. Ahn B, Ahn HS, Shin J, et al. Characterization of lymphocyte-rich hepatocellular carcinoma and the prognostic role of tertiary lymphoid structures. Liver Int. 2024;44(5):1202–1218. doi:10.1111/liv.15865
27. Gan X, Dong W, You W, et al. Spatial multimodal analysis revealed tertiary lymphoid structures as a risk stratification indicator in combined hepatocellular-cholangiocarcinoma. Cancer Lett. 2024;581:216513. doi:10.1016/j.canlet.2023.216513
28. Gong W, Zhang S, Tian X, et al. Tertiary lymphoid structures as a potential prognostic biomarker for combined hepatocellular-cholangiocarcinoma. Hepatol Int. 2024;18(4):1310–1325. doi:10.1007/s12072-024-10694-2
29. Zhang T, Lei X, Jia W, et al. Peritumor tertiary lymphoid structures are associated with infiltrating neutrophils and inferior prognosis in hepatocellular carcinoma. Cancer Med. 2023;12(3):3068–3078. doi:10.1002/cam4.5227
30. Sheng X, Ji Y, Ren GP, et al. A standardized pathological proposal for evaluating microvascular invasion of hepatocellular carcinoma: a multicenter study by LCPGC. Hepatol Int. 2020;14(6):1034–1047. doi:10.1007/s12072-020-10111-4
31. Zhou J, Sun H, Wang Z, et al. China Liver Cancer (CNLC) guidelines for the diagnosis and treatment of hepatocellular carcinoma (2024 edition). Liver Cancer. 2025;14(6):779–835. doi:10.1159/000546574
32. Zhang C, Wang XY, Zuo JL, et al. Localization and density of tertiary lymphoid structures associate with molecular subtype and clinical outcome in colorectal cancer liver metastases. J Immunother Cancer. 2023;11(2):e006425. doi:10.1136/jitc-2022-006425
33. Li Z, Jiang Y, Li B, et al. Development and validation of a machine learning model for detection and classification of tertiary lymphoid structures in gastrointestinal cancers. JAMA Network Open. 2023;6(1):e2252553. doi:10.1001/jamanetworkopen.2022.52553
34. Tsilimigras DI, Bagante F, Moris D, et al. Recurrence patterns and outcomes after resection of hepatocellular carcinoma within and beyond the barcelona clinic liver cancer criteria. Ann Surg Oncol. 2020;27(7):2321–2331. doi:10.1245/s10434-020-08452-3
35. Nevola R, Ruocco R, Criscuolo L, et al. Predictors of early and late hepatocellular carcinoma recurrence. World J Gastroenterol. 2023;29(8):1243–1260. doi:10.3748/wjg.v29.i8.1243
36. Hong SK, Jin XL, Suh S, et al. Different Risk factors for early and late recurrence after curative resection of hepatocellular carcinoma. World J Surg. 2022;46(1):197–206. doi:10.1007/s00268-021-06308-9
37. Shinkawa H, Tanaka S, Takemura S, et al. Nomograms predicting extra- and early intrahepatic recurrence after hepatic resection of hepatocellular carcinoma. Surgery. 2021;169(4):922–928. doi:10.1016/j.surg.2020.10.012
38. Vella G, Guelfi S, Bergers G. High endothelial venules: a vascular perspective on tertiary lymphoid structures in cancer. Front Immunol. 2021;12:736670. doi:10.3389/fimmu.2021.736670
39. Mustapha R, Ng K, Monypenny J, Ng T. Insights into unveiling a potential role of tertiary lymphoid structures in metastasis. Front Mol Biosci. 2021;8:661516. doi:10.3389/fmolb.2021.661516
40. Ohtani O, Ohtani Y. Lymph circulation in the liver. Anat Rec. 2008;291(6):643–652. doi:10.1002/ar.20681
41. Song Q, Wang H, Bao J, et al. Systems biology approach to studying proliferation-dependent prognostic subnetworks in breast cancer. Sci Rep. 2015;5:12981. doi:10.1038/srep12981
42. Zheng W, Zhang J, Song Q, Xu Y, Zhu M, Ma J. Rac family small gtpase 3 correlates with progression and poor prognosis in bladder cancer. DNA Cell Biol. 2021;40(3):469–481. doi:10.1089/dna.2020.5613
43. Shu DH, Ho WJ, Kagohara LT, et al. Immunotherapy response induces divergent tertiary lymphoid structure morphologies in hepatocellular carcinoma. Nat Immunol. 2024;25(11):2110–2123. doi:10.1038/s41590-024-01992-w
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.