Back to Journals » Patient Preference and Adherence » Volume 20
A Cross-Sectional Study on Knowledge, Attitude, and Practice of Tooth-Supported Complete Overdenture Among Middle-Aged and Elderly People: A Structural Equation Modeling Analysis
Received 24 February 2026
Accepted for publication 21 May 2026
Published 3 June 2026 Volume 2026:20 597894
DOI https://doi.org/10.2147/PPA.S597894
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Juan Cui, Gang Guo
Department of Stomatology, Changzhi People’s Hospital, Changzhi, Shanxi, 046000, People’s Republic of China
Correspondence: Gang Guo, Department of Stomatology, Changzhi People’s Hospital, Changzhi, Shanxi, 046000, People’s Republic of China, Tel +8513835519225, Email [email protected]
Introduction: Complete overdenture is an important treatment option for edentulous patients, but limited data exist on public awareness. This study aimed to assess the knowledge, attitude, and practice (KAP) regarding complete overdenture among middle-aged and elderly individuals aged 45 years and above.
Methods: A cross-sectional study was conducted from November 2023 to July 2024 at Changzhi People’s Hospital in Changzhi City.
Results: A total of 602 participants provided valid questionnaires, including 318 females (52.82%). The participants showed poor knowledge (median score: 6 [2, 11], possible range: 0– 20), positive attitude (median score: 27 [24, 30], possible range: 8– 38), and positive practice (median score: 25 [20, 27], possible range: 6– 30). The Structural equation modeling (SEM) analysis indicated that knowledge directly affected attitude (β = 0.572, P < 0.001), and attitude strongly influenced practice (β = 0.807, P < 0.001). Attitude fully mediated the association between knowledge and practice (indirect effect: β = 0.462, 95% CI: 0.392– 0.531, P < 0.001).
Conclusion: Middle-aged and elderly individuals showed poor knowledge but positive attitudes and practices regarding complete overdenture, indicating the need for targeted education.
Keywords: oral health knowledge, attitude, practice, overdenture, middle-aged, the elderly, cross-sectional study
Background
The dental health of middle-aged and elderly individuals presents major challenges, with periodontitis being the leading cause of tooth loss.1–3 In China, which is experiencing rapid population aging, adults aged 65–74 show concerning oral health conditions, with complete edentulism at 4.1% and partial edentulism exceeding 85%.4 Only 12.6% of older adults maintain good periodontal health.5 Tooth loss impairs chewing and speech and also affects social and psychological well-being.6 Complete overdenture provides a balanced treatment option. It offers greater comfort, stability, and function than traditional complete dentures, while remaining more cost-effective than full implant-supported prostheses. Patient reports show consistently higher satisfaction with complete overdenture than with conventional complete dentures.7 Studies indicate that users of complete overdenture have better chewing efficiency (30–40% higher), improved phonetics, enhanced facial appearance, and greater psychological comfort.8,9 A systematic review showed that 85% of complete overdenture users were satisfied with oral function, compared with 60% of conventional denture users.10 Despite these advantages, awareness and use of complete overdenture among middle-aged and elderly populations remain low.11,12
The Knowledge, Attitude, and Practice (KAP) model is widely used to understand health-related behaviors and guide interventions in older populations. In geriatric dentistry, the KAP model helps clarify factors that influence acceptance of dental treatments, and previous studies have shown its usefulness in improving denture use and oral health behaviors among older adults.12–14 This model is particularly valuable for identifying educational needs and designing targeted interventions for populations with specific barriers. However, to our knowledge, no studies have applied the KAP model specifically to complete overdenture among middle-aged and elderly individuals in China.
The study aimed to characterize the levels of knowledge, attitudes, and practices among middle-aged and elderly individuals in China, assess demographic differences across these domains, and employ structural equation modeling to evaluate whether the impact of knowledge on practice operates mainly through its influence on attitude.
Materials and Methods
Study Design and Subjects
This cross-sectional study was conducted from November 7, 2023 to July 2024 at Changzhi People’s Hospital in Changzhi city. Middle-aged and elderly individuals served as the study population. Ethical approval was obtained from the Changzhi People’s Hospital Ethics Committee, and informed consent was collected from all participants. Individuals aged 45 years or older were included due to their potential need for dentures. The analysis further compared middle-aged and elderly subgroups to explore differences in oral health needs and perceptions.
Participants were included if they were aged 45 years or above and could understand and complete the questionnaire independently or with minimal help. Participants were excluded if they did not voluntarily participate, had cognitive impairment affecting response accuracy, submitted duplicate questionnaires, or completed the questionnaire in less than 73 seconds or more than 1800 seconds, which were considered invalid based on pilot testing.
Procedures
The questionnaire was developed based on published literature.15 A pilot study of 30 middle-aged and elderly individuals was conducted to test the preliminary questionnaire. Adjustments were made based on feedback to improve clarity and reliability. Cronbach’s α was 0.894, indicating good internal consistency.
The final questionnaire, presented in Chinese, consisted of three dimensions and thirty-five items (Supplementary Questionnaire 1). The first section included eight demographic variables: age, gender, education, occupation, residence, missing teeth, awareness of dentures, and previous denture experience. The second section assessed knowledge with thirteen items; items 9 and 10 allowed multiple responses with cumulative scoring. Each correct response to a single-choice item was scored 1, and incorrect or unclear answers were scored 0, producing a total knowledge score of 0–20. The third section assessed attitude using eight items; item 7 was scored 1–3 based on denture preference, while the remaining items used a five-point Likert scale (1–5), giving a total score of 8–38. The fourth section evaluated practice through six items using a five-point Likert scale (1–5), yielding a total score of 6–30.
Both electronic and paper questionnaires were used to maximize participation. Paper questionnaires were distributed in the Department of Prosthodontics and the General Dentistry Clinic of Changzhi People’s Hospital by trained research assistants. A snowball sampling method was used to distribute electronic questionnaires through WeChat to patients, family members, and community members to reach individuals who might consider complete overdenture treatment. Research assistants received training on study procedures, questionnaire administration, and privacy protection. Quality control methods included repeated questionnaire checks, on-site supervision during data collection, and strict data cleaning.
Sample Size Calculation
We determined the minimum required sample size (n) using the standard formula for cross-sectional studies, assuming the maximum sample size when the proportion (p) is 0.5:
The Type I error (α) was set at 0.05, corresponding to a Z-score of 1.96 (95% confidence level). The standard error (δ) was set at 0.05. Based on these values, the required sample size was 384. Assuming a 90% effective questionnaire recovery rate, the final goal was to collect at least 430 completed questionnaires.
Statistical Analyses
Statistical analysis was performed using Stata 17.0 (Stata Corporation, College Station, TX, USA). The reliability of the questionnaire was evaluated using Cronbach’s α for the overall scale and the knowledge, attitude, and practice dimensions. Descriptive analysis showed that KAP scores were skewed and were expressed as medians and IQR. Demographic characteristics were presented as n (%). Score differences among demographic groups were examined using the Wilcoxon–Mann–Whitney test for two groups and the Kruskal–Wallis test for multiple groups. Spearman correlation coefficients were used for correlation analysis. Univariate and multivariate logistic regression analyses (using median scores as cut-off values: knowledge ≤6 vs >6, attitude ≤27 vs >27, practice ≤25 vs >25, resulting in 318 [52.82%] vs 284 [47.18%] for knowledge, 302 [50.17%] vs 300 [49.83%] for attitude, and 313 [51.99%] vs 289 [48.01%] for practice) were used to identify risk factors related to K, A, and P. Variables with P-values less than 0.1 in univariate analysis were included in multivariate models. Structural equation modeling (SEM) was used to examine the relationships among knowledge, attitude, and practice. Model fit was assessed using the root mean square error of approximation (RMSEA), incremental fit index (IFI), Tucker–Lewis index (TLI), and comparative fit index (CFI). A two-sided P-value <0.05 was considered statistically significant.
Results
Demographic Information and KAP Scores
The initial dataset contained 770 samples, of which 89 were excluded due to non-responses, leaving 681 cases. After further exclusions for response times below 73 seconds or above 1800 seconds, the final dataset comprised 602 valid cases (effective response rate: 78.18%, 602/770). Among the 602 participants, 302 (50.17%) were aged 45–55 years, 318 (52.82%) were female, and 233 (38.7%) had a high school education or less. A total of 289 (48.01%) were retired, and 504 (83.72%) lived in urban areas. The same proportion reported missing teeth. Additionally, 149 (24.75%) were familiar with complete overdenture, and 127 (21.1%) owned them. The scores for knowledge, attitude, and practice were 6 [2,11], 27 [24,30], and 25 [20,27], respectively (Table 1).
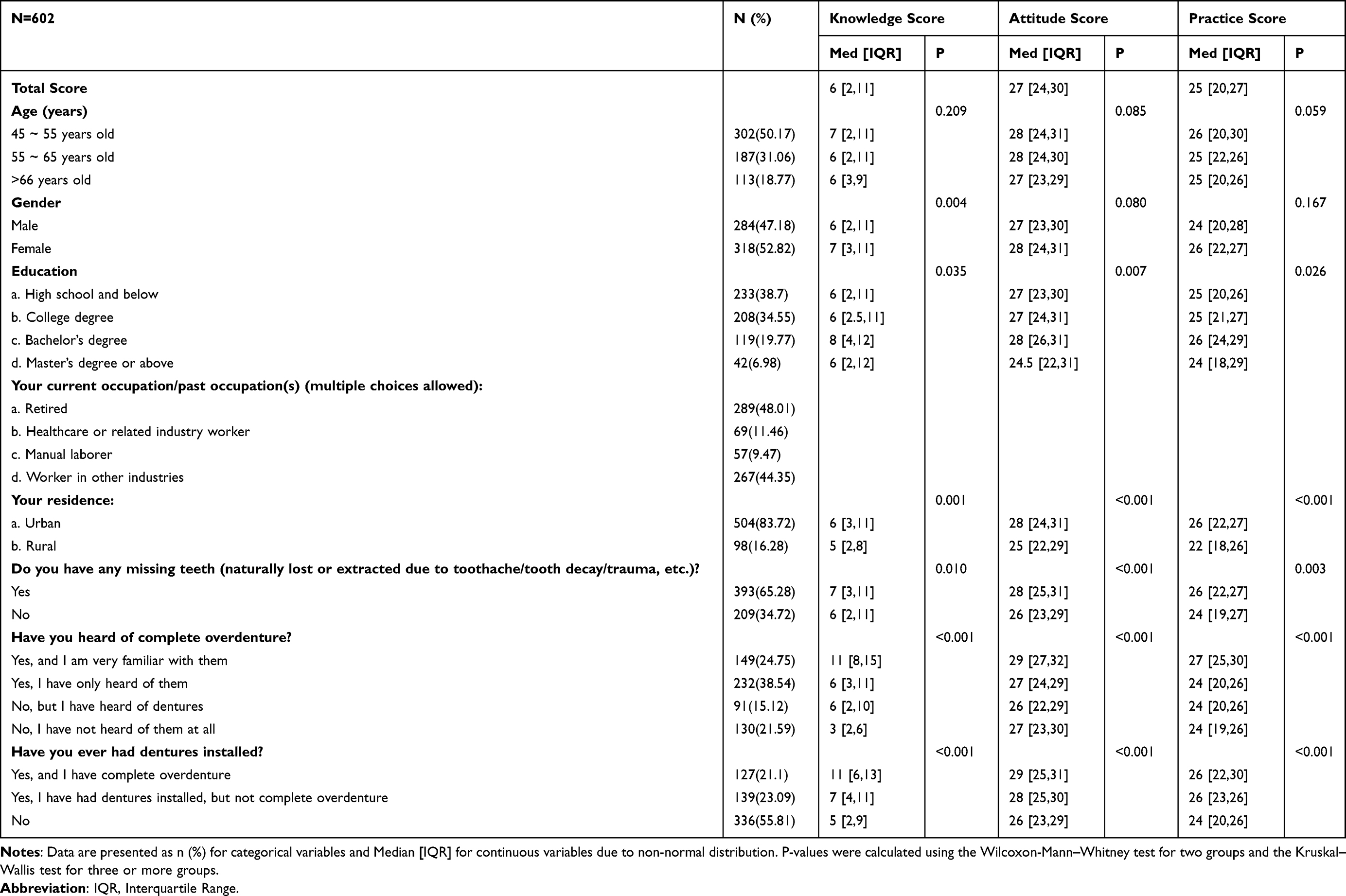 |
Table 1 Demographic Characteristics of the Participants and Comparison of Knowledge, Attitude, and Practice (KAP) Scores |
Knowledge, Attitudes and Practices
The knowledge assessment revealed substantial uncertainty among participants, particularly regarding key aspects such as the definition, indications, and functional characteristics of complete overdenture (Table S1).
Regarding attitudes, a considerable proportion of participants expressed neutral views toward the comparative effectiveness of complete overdenture. Preferences for denture type varied, with complete overdenture being the most frequently selected option. Key factors influencing denture longevity identified by participants included oral hygiene and lifestyle habits such as smoking (Table S2).
For practices, a notable proportion of participants reported inconsistent engagement in recommended behaviors. Variability was observed in adherence to professional guidance and follow-up care, indicating gaps between intention and actual practice (Table S3).
Correlation Analysis
Correlation analysis showed that knowledge was positively correlated with attitude (r = 0.5074, P < 0.001) and practice (r = 0.4582, P < 0.001). Attitude was also positively correlated with practice (r = 0.7172, P < 0.001) (Table 2).
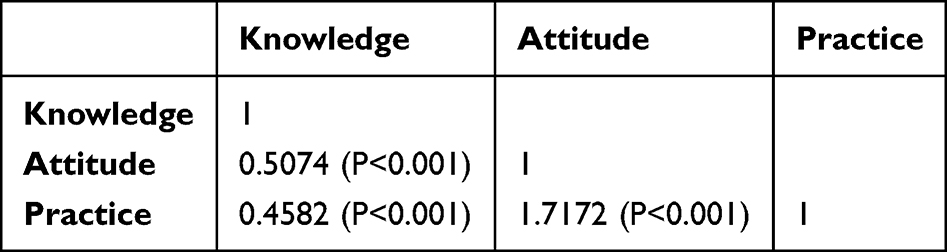 |
Table 2 Spearman Correlation Analysis Among Knowledge, Attitude, and Practice Dimensions |
Structural Equation Modeling Result
Structural equation modeling was performed to examine the hypothesized relationships among knowledge, attitude, and practice (Figure 1). The goodness-of-fit indices indicated that the model fit the data well, with all indicators meeting recommended thresholds: RMSEA = 0.057 (<0.08), SRMR = 0.058 (<0.08), TLI = 0.941 (>0.8), and CFI = 0.948 (>0.8) (Table 3). As shown in Figure 1 and Table 4, knowledge had a significant positive effect on attitude (β = 0.572, P < 0.001), and attitude had a strong positive effect on practice (β = 0.807, P < 0.001). The direct effect of knowledge on practice was not significant (P = 0.434); however, the indirect effect through attitude was significant (β = 0.462, P < 0.001).
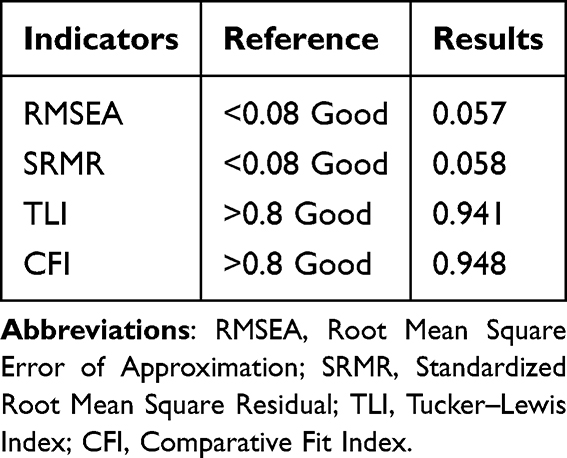 |
Table 3 Goodness-of-Fit Indices for the Structural Equation Model (SEM) |
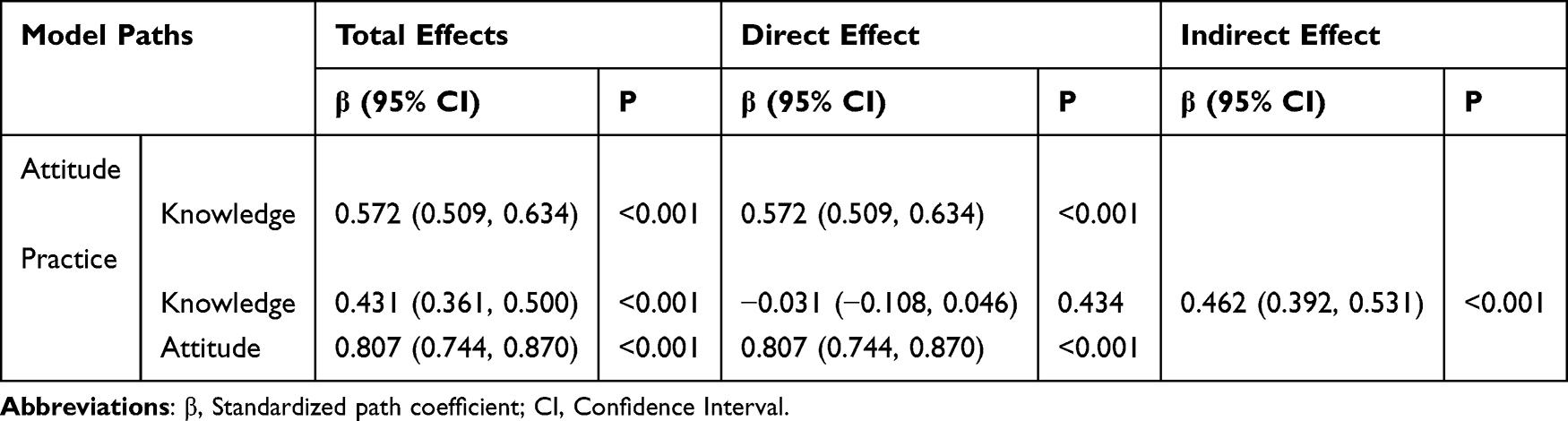 |
Table 4 Path Coefficients and Effects (Direct, Indirect, and Total) of the Structural Equation Model |
 |
Figure 1 Structural Equation Modeling (SEM) of the relationships among knowledge, attitude, and practice. |
Multivariate Logistic Regression Analysis
Multivariate logistic regression showed that being 55–65 years old (OR = 0.53, 95% CI: [0.34, 0.83], P = 0.006), being female (OR = 1.52, 95% CI: [1.05, 2.20], P = 0.023), having only heard of complete overdenture (OR = 0.26, 95% CI: [0.15, 0.43], P < 0.001), having heard of dentures (OR = 0.23, 95% CI: [0.12, 0.43], P < 0.001), having no prior awareness (OR = 0.12, 95% CI: [0.06, 0.23], P < 0.001), and not having dentures installed (OR = 0.44, 95% CI: [0.25, 0.74], P = 0.002) were independently associated with knowledge (Table S4). Knowledge score (OR = 1.24, 95% CI: [1.19, 1.30], P < 0.001) and having no prior awareness (OR = 1.94, 95% CI: [1.00, 3.77], P = 0.047) were independently associated with positive attitude (Table S5). Additionally, attitude score (OR = 1.42, 95% CI: [1.32, 1.53], P < 0.001), being very familiar with complete overdenture (OR = 0.31, 95% CI: [0.17, 0.57], P < 0.001), having only heard of complete overdenture (OR = 0.38, 95% CI: [0.17, 0.81], P = 0.012), and having heard of dentures (OR = 0.28, 95% CI: [0.13, 0.58], P = 0.001) were independently associated with practice (Table S6).
Discussion
Middle-aged and elderly individuals showed insufficient knowledge but positive attitudes and practices regarding complete overdenture. Given these gaps, it is necessary for healthcare professionals to implement targeted educational programs to improve understanding, strengthen positive attitudes, and promote proper practices related to complete overdenture in this population.
From a clinical perspective, the findings of this study have important implications for dental practice and public health strategies. The observed gap between knowledge and practice suggests that simply providing information may be insufficient to promote optimal treatment behaviors. Dental professionals should place greater emphasis on attitude-oriented communication, including motivational counseling and individualized education, to facilitate the translation of knowledge into actual treatment decisions. In addition, routine dental consultations should incorporate structured education on the indications, benefits, and maintenance requirements of tooth-supported complete overdenture, particularly for middle-aged and elderly patients with partial or complete tooth loss. Early intervention and continuous follow-up may further enhance treatment adherence and long-term outcomes.
This study provides important insights into the KAP regarding complete overdenture among middle-aged and elderly individuals. The strong positive correlations among knowledge, attitudes, and practices demonstrated by both the correlation analysis and SEM support findings from related research showing that knowledge plays a fundamental role in shaping health behaviors.16
Our findings also showed that females had higher knowledge scores, which was confirmed by multivariate logistic regression identifying gender as a significant predictor of knowledge. This difference is consistent with previous research indicating that women tend to be more proactive in seeking dental care and more responsive to dental health education.17 Furthermore, the influence of residential location on KAP scores, particularly the lower scores among rural residents compared with urban residents, suggests notable geographical disparities in access to information and dental services, a pattern commonly observed in broader healthcare studies.18 The degree of familiarity with complete overdenture significantly influenced KAP scores among middle-aged and elderly individuals. Participants who were very familiar with complete overdenture showed more positive attitudes and practices. Moreover, even those who had only heard of complete overdenture demonstrated better KAP scores than those completely unaware, highlighting the potential role of information dissemination in improving health behaviors.19,20
The findings reveal a complex pattern of understanding, acceptance, and practice related to complete overdenture among middle-aged and elderly individuals. There was substantial uncertainty in knowledge about denture details, which aligns with reports showing that inadequate information can discourage individuals from accepting advanced dental treatments.21,22 Although attitudes toward dentures were generally positive, financial considerations played a strong role in decision-making, consistent with previous findings emphasizing the dominant influence of economic factors on dental health decisions.23 Beyond general financial concerns, insurance coverage and perceived affordability were identified as key determinants of practice behaviors. Limited insurance reimbursement for complete overdenture may discourage elderly individuals from seeking or maintaining these prostheses. Policymakers should consider including overdenture rehabilitation in basic medical insurance schemes to improve access and promote oral health equity among older adults. Integrating comprehensive educational programs may help address these gaps. Such programs could use widely used social media platforms, such as WeChat in China, to deliver short and engaging educational content on the benefits and procedures of complete overdenture.24,25 Given the financial hesitations observed, addressing economic barriers is essential for improving access to complete overdenture among middle-aged and elderly individuals in China.26 Dental clinics should provide clear counseling on insurance coverage and cost-effective treatment options. Collaborations with insurance providers to offer detailed consultations may reduce financial concerns and increase patient willingness to pursue recommended treatments. Strengthening patient–dentist communication is also important. Tailoring health promotion activities to local cultural and regional contexts—such as holding free dental check-up events in rural areas or distributing customized informative pamphlets—may further enhance engagement.14,27
Despite the valuable insights obtained, this study has several limitations. First, its cross-sectional design does not allow causal inference regarding the relationships among knowledge, attitude, and practice; thus, the SEM results should be interpreted as correlational rather than causal. Second, the use of self-reported questionnaires may introduce recall bias and social desirability bias, which may affect response accuracy. In addition, the combined hospital-based and WeChat snowball sampling approach may have introduced selection bias. Participants recruited through WeChat were more likely to be urban, educated, and digitally active, whereas hospital visitors were generally more health-conscious or symptomatic, limiting representativeness of the broader middle-aged and elderly population. Furthermore, questionnaire validation relied only on internal consistency (Cronbach’s α), without external validity or construct testing, which should be addressed in future studies. Lastly, the study was conducted in Changzhi City in Shanxi Province, which may limit the generalizability of the findings to other regions or populations in China.
Conclusions
This study reveals that while middle-aged and elderly individuals generally hold positive attitudes and engage in positive practices regarding complete overdenture, their knowledge levels remain insufficient. Structural equation modeling confirmed a significant pathway where knowledge positively influences attitude, which in turn exerts a strong direct effect on practice behaviors. Consequently, to bridge the knowledge gap and promote the adoption of complete overdenture, it is essential for healthcare providers and policymakers to implement targeted educational interventions and consider integrating financial support, such as medical insurance coverage, into oral health promotion strategies.
Abbreviations
KAP, Knowledge, Attitude, and Practice; SEM, Structural Equation Modeling; IQR, Interquartile Range; CI, Confidence Interval; RMSEA, Root Mean Square Error of Approximation; FI, Comparative Fit Index; TLI, Tucker–Lewis Index.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was conducted in accordance with the Declaration of Helsinki (2000) of the World Medical Association. All methods were performed in accordance with the relevant guidelines. Ethical approval was obtained from the Changzhi People’s Hospital Ethics Committee, and informed consent was obtained from all research participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Chung M, Lee J, Song W, et al. Automatic registration between dental cone-beam CT and scanned surface via deep pose regression neural networks and clustered similarities. IEEE Trans Med Imaging. 2020;39(12):3900–9. doi:10.1109/TMI.2020.3007520
2. Könönen E, Gursoy M, Gursoy UK. Periodontitis: a multifaceted disease of tooth-supporting tissues. J Clin Med. 2019;8(8):1135. doi:10.3390/jcm8081135
3. Tian S, Dai N, Cheng X, Li L, Sun Y, Cui H. Relative trajectory-driven virtual dynamic occlusal adjustment for dental restorations. Med Biol Eng Comput. 2019;57(1):59–70. doi:10.1007/s11517-018-1867-3
4. Du M, Jiang H, Tai B, Zhou Y, Wu B, Bian Z. Root caries patterns and risk factors of middle-aged and elderly people in China. Oral Epidemiol. 2009;37(3):260–266. doi:10.1111/j.1600-0528.2009.00461.x
5. Zhou X, Xu X, Li J, et al. Oral health in China: from vision to action. Int J Oral Sci. 2018;10(1):1. doi:10.1038/s41368-017-0006-6
6. Emami E, de Souza RF, Kabawat M, Feine JS. The impact of edentulism on oral and general health. Int J Dent. 2013;2013:498305. doi:10.1155/2013/498305
7. Sharma AJ, Nagrath R, Lahori M. A comparative evaluation of chewing efficiency, masticatory bite force, and patient satisfaction between conventional denture and implant-supported mandibular overdenture: an in vivo study. J Indian Prosthodont Soc. 2017;17(4):361–372. doi:10.4103/jips.jips_76_17
8. Bajunaid SO, Alshahrani AS, Aldosari AA, et al. Patients’ satisfaction and oral health-related quality of life of edentulous patients using conventional complete dentures and implant-retained overdentures in Saudi Arabia. Int J Environ Res Public Health. 2022;19(1):557. doi:10.3390/ijerph19010557
9. Qazi A, Sundarkar P, Barabde A, Agrawal S, Bele R, Dammani B. A comparative evaluation of masticatory efficiency and patient satisfaction between single implant-supported mandibular overdentures and conventional dentures in edentulous patients: a systematic review. J Osseointegrat. 2022;14:226–236.
10. Carlsson GE. Clinical morbidity and sequelae of treatment with complete dentures. J Prosthet Dent. 1998;79(1):17–23. doi:10.1016/S0022-3913(98)70188-X
11. Thomason JM, Kelly SA, Bendkowski A, Ellis JS. Two implant retained overdentures--a review of the literature supporting the McGill and York consensus statements. J Dent. 2012;40(1):22–34. doi:10.1016/j.jdent.2011.08.017
12. Allen PF, McMillan AS. A longitudinal study of quality of life outcomes in older adults requesting implant prostheses and complete removable dentures. Clin Oral Implants Res. 2003;14(2):173–179. doi:10.1034/j.1600-0501.2003.140206.x
13. Mariño R, Calache H, Wright C, Schofield M, Minichiello V. Oral health promotion programme for older migrant adults. Gerodontology. 2004;21(4):216–225. doi:10.1111/j.1741-2358.2004.00035.x
14. Rajeh MT. Gender differences in oral health knowledge and practices among adults in Jeddah, Saudi Arabia. Clin Cosmet Investig Dent. 2022;14:235–244. doi:10.2147/CCIDE.S379171
15. Emami E, Heydecke G, Rompré PH, de Grandmont P, Feine JS. Impact of implant support for mandibular dentures on satisfaction, oral and general health-related quality of life: a meta-analysis of randomized-controlled trials. Clin Oral Implants Res. 2009;20(6):533–544. doi:10.1111/j.1600-0501.2008.01693.x
16. Cunha MA, Vettore MV, Santos TRD, Matta-Machado AT, Lucas SD, Abreu M. The role of organizational factors and human resources in the provision of dental prosthesis in primary dental care in Brazil. Int J Environ Res Public Health. 2020;17(5):1646. doi:10.3390/ijerph17051646
17. Cabezas CA, Juan DVL. Lithium disilicate occlusal surfaces on acrylic resin denture teeth in a mandibular implant-retained overdenture opposed by a maxillary removable complete denture: a clinical report. J Prosthet Dent. 2025;133(3):649–654. doi:10.1016/j.prosdent.2023.03.033
18. Shreedhar S, Raza FB, Vaidyanathan AK, Veeravalli PT. Effect of an implant-retained complete overdenture on the hearing ability of edentulous patients: a clinical pilot study. J Prosthet Dent. 2021;125(4):628–635. doi:10.1016/j.prosdent.2020.02.015
19. Adedoyin P, Adesina E, Adeyeye B, Oyesomi K, Falola H. Influence of information sources on women’s behavioural practice towards breast cancer in Lagos, Nigeria. Healthcare. 2022;10(10):1901. doi:10.3390/healthcare10101901
20. Bastani P, Bahrami MA, Kapellas K, Yusefi A, Rossi-Fedele G. Online oral health information seeking experience and knowledge, attitudes and practices of oral health among iranian medical students: an online survey. BMC Oral Health. 2022;22(1):29. doi:10.1186/s12903-022-02061-0
21. Ann Preethy N, Somasundaram S. Safety and physiologic effects of intranasal midazolam and nitrous oxide inhalation based sedation in children visiting Saveetha Dental College and Hospitals, India. Bioinformation. 2022;18(1):26–35. doi:10.6026/97320630018026
22. Salam TAA, Khinda VI, Alghamdi AM, et al. Evaluation of some dental myths among the adult population in Riyadh, Saudi Arabia: a Cross-Sectional Study. Cureus. 2023;15(1):e33759. doi:10.7759/cureus.33759
23. Kutkut A, Knudsen H, Bush H, Studts J. Comparison of implant-retained overdenture and conventional complete denture: a survey study to measure patients’ satisfaction and quality of life in dental school clinics. J Oral Implantol. 2024;50(3):266–276. doi:10.1563/aaid-joi-D-22-00096
24. Lone MA, Kumar B, Musharraf H, et al. Current trends in complete denture education in undergraduate dental colleges of Pakistan. J Pak Med Assoc. 2023;73(10):2029–2035. doi:10.47391/JPMA.9710
25. Sharma N, Shukla J, Sharma D, Mehta D, Kakde L, Bais K. Perceived status and care practices among complete denture wearers. J Pharm Bioallied Sci. 2020;12(Suppl 1):S336–s339. doi:10.4103/jpbs.JPBS_99_20
26. Rocha COM, Longhini D, Pereira RP, Lima ALO, Bonafé FSS, Arioli Filho JN. Masticatory efficiency in complete denture and single implant-retained mandibular overdenture wearers with different occlusion schemes: a randomized clinical trial. J Prosthet Dent. 2023;129(6):888–894. doi:10.1016/j.prosdent.2021.06.028
27. Cao C, Friedenreich CM, Yang L. Association of daily sitting time and leisure-time physical activity with survival among US cancer survivors. JAMA Oncol. 2022;8(3):395–403. doi:10.1001/jamaoncol.2021.6590
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge, Attitudes and Practices Towards Psoriasis Among Patients and Their Family Members
Zhang X, Du H, Liu X, Liu L, Zhang T
Clinical, Cosmetic and Investigational Dermatology 2024, 17:769-782
Published Date: 3 April 2024
Knowledge, Attitudes and Practices Toward Physical Literacy Among the College Students During COVID-19 School Closure
Ma C, Yue M, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:1629-1640
Published Date: 15 April 2024
Knowledge, Attitude and Practice of Radiologists Regarding Artificial Intelligence in Medical Imaging
Huang W, Li Y, Bao Z, Ye J, Xia W, Lv Y, Lu J, Wang C, Zhu X
Journal of Multidisciplinary Healthcare 2024, 17:3109-3119
Published Date: 4 July 2024
Knowledge, Attitude, and Practice Toward Varicocele in Patients with Varicoceles: A Cross-Sectional Study in Chinese Patients
Gong P, Shen J, Yang Y, Xue D, Lu H, Zhuang Q, Wang X, Tian Z, Chen Y, Chen C, Cao Y
International Journal of General Medicine 2024, 17:3423-3432
Published Date: 7 August 2024
Knowledge, Attitude, and Practice Towards Rehabilitation in Patients with Breast Cancer: A Cross-Sectional Study
Zhou Y, Lu Q, Yu X
Journal of Multidisciplinary Healthcare 2025, 18:1483-1492
Published Date: 12 March 2025