Back to Journals » OncoTargets and Therapy » Volume 16
A Comprehensive Review of Interventional Clinical Trials in Patients with Bone Metastases
Authors Shen F, Huang J ![]() , Yang K
, Yang K ![]() , Sun C
, Sun C ![]()
Received 21 April 2023
Accepted for publication 21 June 2023
Published 29 June 2023 Volume 2023:16 Pages 485—495
DOI https://doi.org/10.2147/OTT.S415399
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Arseniy Yuzhalin
Video abstract presented by Fei Shen.
Views: 109
Fei Shen, Jihe Huang, Kejia Yang, Chunhua Sun
Department of Orthopedics, Suzhou Wuzhong People’s Hospital, Suzhou, People’s Republic of China
Correspondence: Fei Shen; Chunhua Sun, Department of Orthopedics, Suzhou Wuzhong People’s Hospital, No. 61 Dongwu North Road, Wuzhong District, Suzhou, Jiangsu Province, 215128, People’s Republic of China, Email [email protected]; [email protected]
Abstract: Bone metastasis is one of the most important factors associated with poor prognosis for patients with prostate, breast, thyroid, and lung cancer. In the past two decades, 651 clinical trials, including 554 interventional trials, were being registered in ClinicalTrials.gov and pharma.id.informa.com to combat bone metastases from different perspectives. In this review, we comprehensively analyzed, regrouped, and discussed all the interventional trials on bone metastases. Clinical trials were re-grouped into bone-targeting agents, radiotherapy, small molecule targeted therapy, combination therapy, and others, based on the different mechanisms of action including modifying the bone microenvironment and preventing the growth of cancer cells. We also discussed the potential strategies that might improve overall survival and progression-free survival of patients with bone metastases in the future.
Keywords: bone metastases, clinical trials, interventional, ClinicalTrials.gov, pharma.id.informa.com
Introduction
Bone metastasis is defined as the metastasis of the cancer cells from primary sites to the bones, which increases the risk of skeletal-related events (SREs), such as bone pain, pathological bone fractures, and even spinal cord compression that requires emergency surgery. Bone is one of the most common sites for metastases in cancer. Worldwide, more than 1.5 million cancer patients will eventually develop bone metastases, making bone one of the most common metastatic sites.1 Many cancers can result in distant metastases, but up to 70% of skeletal metastases originate from prostate and breast cancers.2 It has been reported that only about 0.02% of cancer cells entering the circulation produce clinically detectable metastases, indicating metastasis formation process is highly inefficient.3 However, once metastases occur, they lead to 90% of cancer-associated mortality.4 Therefore, There is an urgent need to develop effective new drugs, explore novel combination therapies, and make new treatment strategies to improve patient outcome.
Based on the predominant radiographic appearances of lysis or sclerosis in the bone, bone metastases can be classified as osteolytic or osteoblastic bone lesions, respectively. As in many patients with multiple myeloma or lung cancer, in which osteoclast-mediated bone resorption dominates, once bone destruction occurs focally, the so-called “punched out” lytic lesion forms. In contrast, in patients with prostate cancer, increased osteoblast activity leads to the dense osteosclerotic appearance of the metastatic bone lesions.5 When both lytic and sclerotic components coexist in one metastatic bone lesion, mixed lesions develops. Mixed lesions occur in many tumor types, especially in patients with metastatic breast cancer.
The highly dynamic bone microenvironment results from the complex cell types, such as osteocytes, osteoblasts, osteoclasts, immune cells, hematopoietic stem cells, adipocytes, and endothelial cells, and the dialogue between those cells and tumor cells.6 The functional roles of cellular and extracellular components of bone microenvironment in the initiation and progression of bone metastases were well studied and comprehensively reviewed.7 Molecular characterization could help unravel the biological interactions between bone microenvironment and tumor cells and eventually prevent bone metastasis by developing specific therapeutic strategies. Preclinical models of bone metastasis indicated that the infiltrated cancer cells disrupt the coordinated process regulating bone remodeling. In the early stage of bone metastases, tumors can influence the bone marrow microenvironment by preparing for invasion through the formation of pre-metastatic niches.8,9 In turn, the bone microenvironment supports the survival and clonal selection of tumor cells after colonization, such as immune escape, immunomodulation, and reprogramming of stromal signature and angiogenesis.10 The concept of “vicious cycle” was widely accepted to explain the mechanism that governs the growth of bone metastases. Once established in bone, metastasized tumors modify their immediate environment to support their own survival and growth.11–14 Importantly, tumors and bone share overlapping signaling pathways, providing the fundamental basis for therapeutic targets, such as RANK and RANKL which were detected in breast cancer samples and associated with tumor propagation, bone metastases, and a poor prognosis in both clinical and preclinical studies.15 Nowadays, by interrupting the “vicious cycle” of bone metastasis, RANKL inhibition and bisphosphonates have been successfully approved for the treatment of patients with bone metastases from many sorts of solid tumors, including prostate and breast cancers.
Randomized clinical trials, developed by regulatory agencies, researchers, drug developers, and statisticians, are conducted to reduce the uncertainty over the safety and efficacy of an intervention.
Given the inherent complexity, potential cost, and timelines of clinical developments of new interventions against bone metastases, learning the lessons from the past, no matter whether it is failure or success, will be crucial for future successes of new treatment development. Until now, interventional clinical trials for therapies relating to treatment of bone metastases have not been systemically analyzed and reviewed yet. Thus, this systematic review provides an overview of clinical trials designed to evaluate the trends of interventions in the treatment of bone metastases during the last two decades.
Data Collection
On 1 October 2022, two datasets of 520 and 235 clinical studies related to bone metastases were obtained from ClinicalTrials.gov (a resource including all interventional studies and provided by the US National Library of Medicine) (Table S1) and pharma.id.informa.com (Pharmaprojects, including only drug development database developed by INFORMA) (Table S2), respectively. The term [Bone metastases] was used as the keyword for search. After 104 overlapped clinical trials were removed, data from these two datasets were combined and a new table with 651 clinical trials was generated (Table S3) (Figure 1).
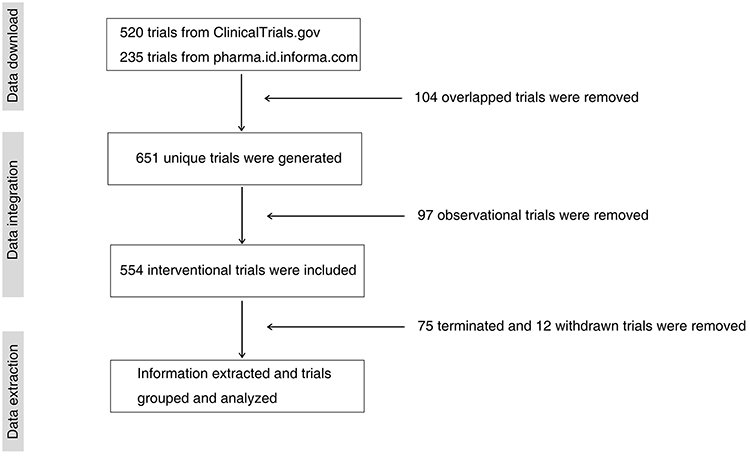 |
Figure 1 Flowchart of clinical trial selection for bone metastases. |
The new table contains the following information extracted from the website: TrialTrove ID, NCT number, trial title, trial phase (early phase I, I/II, II, II/III, III, III/IV, IV); trial status; sponsor; sponsor type; study type (interventional, observational or others); treatments; treatment summary; treatment type; targets; combination target 1; combination target 2; start date; patient gender; locations and the record URL (Table S3). The datasets were analyzed using sorts of parameters in Microsoft Excel. Information regarding terminologies can be obtained from Clinical Trials Transformation Initiative website.
Characteristics and Trends of Trials
Our data collection identified 651 trials involving bone metastases, and our review was started based on these clinical trials. Among them, only 97 are observational clinical trials; all the rest 554 are interventional clinical trials. Thirty-two from observational trials had no treatment information and were excluded from the total clinical trials identified. Sixty-four interventional clinical trials had missing information regarding the start date of the trials, but were not excluded from the dataset except that those data were not used for analysis of the year trend. The clinical trials were sponsored by academia (252, 40.7%), industry (198, 32%), and the collaboration of industry and academia (169, 27.3%) (Figure 2A). Of the 619 clinical trials, 569 had country information. For those with country information, 494 were conducted by a single country, and the remaining 75 by multiple countries. Clinical trials were conducted mainly in United States (233) either as a single country (196) or as collaborative partner (27) with other countries, followed by France (61) and China (62) (Figure 2B). A total of 206 clinical trials had missing information regarding phase stage. Of the 439 clinical trials with phase stage, phase II (including phase I/II) trials were in the majority (212, 48.3%), followed by phase I (62, 14.1%), phase III (including II/III) (100, 22.8%), and phase IV trials (including III/IV) (65, 14.8%) (Figure 2C). For the trend of clinical trials on bone metastases over time, the total number of trials fluctuated over the past 20 years with two peaks in 2006 and 2015, respectively. However, the total number of trials tended to decrease gradually since 2020 (Figure 2D). Additionally, 93 interventional trials are still underway, including 13 open, 12 not recruiting, 14 active but not recruiting, 47 recruiting, and 7 planned clinical trials. Those clinical trials were included in this review since they are representing the current direction and progress of treatment in bone metastases.
 |
Figure 2 (A) Sponsors of clinical trials for bone metastases. (B) Country distributions of clinical trials. (C) Phase stages of clinical trials. (D) Trends of clinical trials of bone metastases. |
Classification of Interventional Trials
Among the 554 interventional trials, 75 and 12 were terminated or withdrawn, respectively. Next we focused on the review of the rest of the 467 interventional trials, which are listed in Figure 3. Interventional clinical trials for bone metastases, including combination therapy (52, 11.1%) and single agent therapy, made up of bone-targeting agent (BTA, including bisphosphonates and RANKL inhibitors) (78, 16.7%), radiotherapy external beam radiotherapy (EBRT) and targeted radionuclide therapy (106, 22.7%), and small molecule targeted therapy (SMTT, 88, 18.4%), accounted for the vast majority, and the rest of the trials were grouped as “others” (143, 30.6%) which were further divided into calcium balance agents (10, 2.1%), chemotherapy (15, 3.2%), immunotherapy (9, 1.9%), orthopedic surgery (8, 1.7%), ablation (9, 1.9%), diagnostic performance (15, 3.2%), ultrasound (17, 3.6%), and others (60, 12.8%). The treatment groups and the detailed information of their phase stages were extracted and are shown in Figure 3.
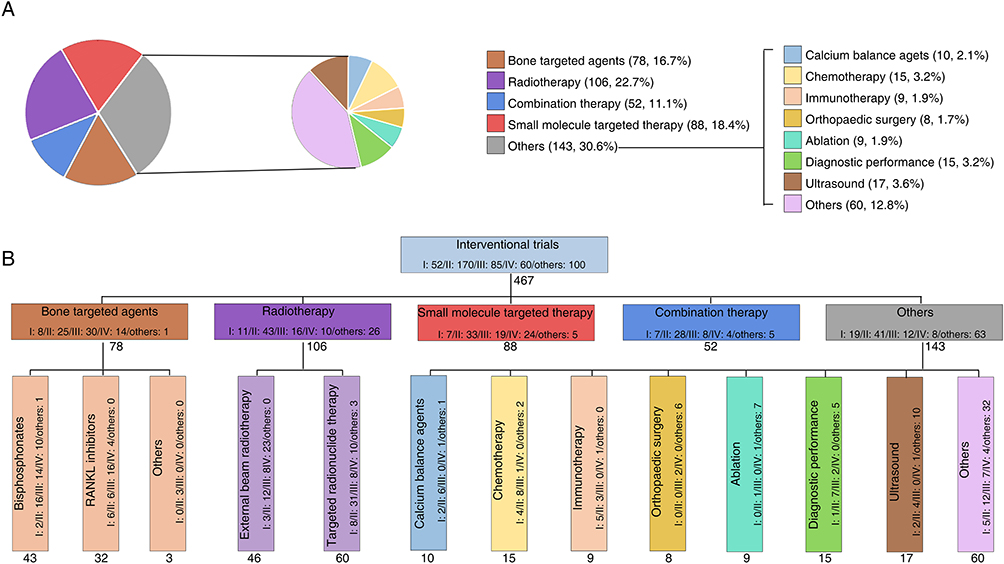 |
Figure 3 Phase stages of different treatment groups for bone metastases in interventional clinical trials. (A) Types of therapy for treating bone metastases. (B) Phase stages in different interventional groups. |
Discussion
This systematic review provided substantial information on the interventional clinical trials for the treatments of bone metastases in the last two decades. Treatment decisions depend on whether the bone metastases are widespread or localized, on the nature of the original malignancy, and the appearance of the metastases outside of bone. Cure is only a realistic aim in the treatment of bone metastases and the tumors affecting the bones. However, multidisciplinary management, including BAT (bisphosphonates and RANKL inhibitors), radiotherapy (EBRT and targeted radionuclide therapy), SMTT, systemic therapy with orthopedic surgery, cytotoxic chemotherapy, and other therapies, can still effectively prevent disease progression, palliate morbidity associated with skeletal lesions, and improve quality of life.
Bone-Targeting Agent
In the past two decades, BTA accounts for 16.7% (78/467) of all interventional clinical trials (Figure 3B). Up to the present, BTA has become the standard of care for the prevention and treatment of bone metastasis-associated skeletal complications in patients with solid tumors.16,17 Biochemical data indicated that bone resorption mediated by osteoclast cells is important not only in breast and lung cancer-derived osteolytic bone metastases but also in osteoblastic lesions from prostate cancers. Therefore, the osteoclast is a primary therapeutic target for bone metastases irrespective of the original tissue of the tumor. BTA provides an additional treatment approach for bone pain relief across a range of tumor types, which seems to be independent of radiographic appearance of metastases and the nature of the underlying tumor.18
BTA consists of bisphosphonate (55.1%, 43/78) and anti-RANK ligand (RANKL) antibody (41%, 32/78) in clinical trials (Figure 3B). For these clinical trials, the primary end point was the influence of BTAs on the number of patients experiencing SREs, the time to the first SREs, and the rate of SREs as evaluated by either a simple annual rate or more complex multiple event analysis methods.
The bisphosphonates are pyrophosphate analogs, characterized by a P-C-P-containing central structure that makes bisphosphonates resistant to phosphatase activity and promotes its binding to a mineralized matrix of bone. Bisphosphonates reduce osteoclast activity by promoting osteoclast apoptosis, by decreasing osteoclast progenitor development, and by disrupting several biochemical processes involved in osteoclast function.19 In addition, bisphosphonates appear to have a beneficial effect on osteoblasts.20 Both the intravenous formulations of pamidronate (zoledronic acid and ibandronate) and the oral agents (ibandronate and clodronate) show useful clinical efficacy in patients with bone metastases originating from breast cancer. Placebo-controlled randomized trials have shown that bisphosphonates reduce bone pain and biochemical markers of bone resorption in patients with osteoblastic bone lesions that are associated with advanced prostate cancer.21 A randomized phase III, placebo-controlled trial has shown that, compared with placebo, zoledronic acid significantly reduced the overall risk for SRE(s) by almost 30%, doubled the time to the first SRE, and reduced the proportion of patients with at least one SRE during bone metastases from many sorts of solid tumors other than prostate and breast cancer.22,23
Anti-RANKL antibody has a high RANKL binding ability, preventing its interaction with RANK in a way similar to osteoprotegerin which inhibits RANK signaling and bone resorption by binding to RANKL.21 Denosumab was the only anti-RANKL antibody observed in the clinical trials ranging from phase I to phase IV. Compared to zoledronic acid, denosumab has been shown to be more efficient in the prevention of SREs from breast cancer, prostate cancer, and other advanced solid tumors and was generally well tolerated.24–26 Denosumab has been shown to effectively reduce the risk for any clinical fracture, prevent breast cancer treatment-induced bone loss, and improve disease-free survival in women with breast cancer receiving an aromatase inhibitor.27–29 Denosumab treatment was associated with bone loss prevention and a significantly reduced incidence of new vertebral fractures in men with prostate cancer receiving ADT.29,30 Compared with placebo, denosumab significantly delayed the time to first bone metastases and increased bone metastasis-free survival by a median of 4.2 months in men with non-metastatic CRPC. However, this effect was not considered sufficient to change clinical practice due to no improvement in overall survival (OS) in patients with CRPC and relatively high cumulative incidence of osteonecrosis of the jaw.31 Compared to zoledronic acid, denosumab was associated with better overall survival in patients with lung cancer and bone metastases.32 In the ABCSG-18 trial, adjuvant denosumab treatment results in better disease-free survival, bone metastasis-free survival, and OS in patients with early hormone receptor-positive breast cancer on aromatase inhibitor therapy.33
The aim of the use of BTAs is to reduce subsequent complications and to delay the appearance of first SRE from bone metastases. The extent to which patients benefit from BTAs treatment depends on several critical factors, such as the origin and stage of bone metastases, the time when treatment is initiated after the diagnosis, which BTA treatment is used first, how long the treatments will last, and finally the physician’s judgment and the compliance of patients.34 However, no randomized data are available to support whether BTA treatment should be initiated in all patients with bone metastases as soon as bone metastases are diagnosed. Meanwhile, no approved tool was reported to predict which patients will eventually develop SREs. Based on the benefits of BTAs to patients with bone metastases, they are recommended to be initiated in the vast majority of patients as soon as the diagnosis of bone metastases with or without symptoms.35
Radiotherapy
In our dataset, radiotherapy (22.7%, 106/467) comprises EBRT (43.4%, 46/106) and targeted radionuclide therapy (56.6%, 60/106) (Figure 3B). Radiotherapy is performed primarily to improve quality of life by relieving pain, prevent pathologic fractures, and maintain skeletal function. Osteoclast activation was reported to be associated with painful osteolytic metastasis which leads to higher rate of pathological fractures. The extent of beneficial effects of radiotherapy on bone pain mainly depends on its capability to diminish osteoclast activation, promote ossification of osteolytic lesions, and kill tumor cells eventually.36 Partial or complete pain relief was shown to occur rapidly, benefiting 40% of responders within 10 days.37 Side effects of palliative radiotherapy for bone metastases depend on which body area was treated. Spinal cord compression is a medical emergency requiring urgent magnetic resonance imaging to confirm the diagnosis. Radiotherapy alone (for patients with poor prognosis) or combined with surgical intervention (for patients with good performance status) should be given to patients with urgent spinal cord compression (SCC) after the initial dexamethasone treatment.38 Radionuclide therapy was reported to be superior to EBRT in that normal tissues may partially be spared by delivering the radiation more specifically to the tumor.39 Radium-223 (α-emitting radiopharmaceutical 223radium dichloride), strontium-89 (β-emitting radiopharmaceutical 89strontium), and samarium-153 (ethylene diamine tetramethylene phosphonate-153samarium) are the main radionuclide therapies studied in clinical trials, accounting for 60% (36/60), 10% (6/60), and 15% (15/60), respectively (Table S3). The rest accounted for 15% of the radionuclide therapies, including Sn-117m-DTPA, Ho-166-DOTMP, and Re-188-HEDP. These radiopharmaceuticals preferentially target newly formed bone matrix, causing DNA damage and cell death.40,41 Approval has been given for 223Ra for the treatment of men with CRPC and symptomatic bone metastases, but no known visceral metastases; 223Ra significantly improved overall survival and delayed new symptomatic skeletal events by 3.6 months and 5.8 months, respectively, in patients with metastatic castration-resistant prostate cancer (mCRPC) who failed or were unfit for docetaxel, receiving 223Ra or placebo in addition to best standard of care.42 Samarium-153 and strontium-89 are approved for the occasional use to relieve bone metastasis-derived bone pain.43
Modern radiotherapy techniques like stereotactic body radiotherapy (SBRT), which delivers a high ablative biological dose in one to several fractions in a short treatment course and results in prompt pain relief and excellent disease control with acceptable toxicity, have been established as a safe and effective treatment option for bone metastases. The symptom relief and safety of SBRT in the treatment of metastases in spinal bone have been well established.44–48 However, contrary to conventional EBRT, SBRT is still not the standard of care treatment for patients with bone metastases due to the lack of consistent dose schedule in previous studies. No formal evidence in clinical practice is available to lead to definitive conclusions on the superiority of one regimen over another. In terms of the use of SBRT in bone metastases other than spine, limited studies were published to evaluate its effect on pain control and safety.
Small Molecule Targeted Therapy (SMTT)
Over the past two decades, the strategy of cancer treatment has shifted tremendously, from broad-spectrum cytotoxic chemotherapies to targeted therapies.49 Compared with traditional chemotherapies, SMTTs have high potency and low toxicity by specifically targeting cancer cells but sparing normal cells. There were 88 clinical trials related to SMTTs, accounting for 18.84% (88/467) of total interventional trials (Figure 3B). Among 88 SMTTs, 63 (71.6%) were related to zibotentan, a potent antagonist of endothelin A. However, compared with docetaxel alone, phase III trials of docetaxel in combination with zibotentan failed to improve OS in patients with mCRPC.50,51 Tyrosine kinase inhibitor (22.7%, 20/88) was ranked second among SMTTs, targeting BCR-ABL, EGFR, VEGF, and mTOR (Table S3).
In patients with advanced ER+/HER2- breast cancer who failed on prior nonsteroidal aromatase inhibitor therapy, exemestane in combination with mTOR inhibitor, everolimus, significantly increased the median progression-free survival compared to exemestane alone. Additionally, bone marker levels increased under the treatment of exemestane alone, but decreased when combined with everolimus.52,53 By suppressing increased bone turnover by exemestane, everolimus plus exemestane significantly decreases disease progression in the bone.52 This clinical finding may result from mTOR inhibitor which disrupts the mTOR signaling pathway required for RANKL and M-CSF mediated osteoclast survival.54
In the phase III METEOR trial, dual tyrosine kinase inhibitor, cabozantinib, that targets both c-MET and VEGFR2, was related to a significant improvement of overall survival and progression-free survival in renal cell cancer patients with bone metastases.55
Other SMTTs, such as RON receptor tyrosine kinase inhibitor, Src kinase inhibitors, and cathepsin K inhibitors, were either in early clinical development or withdrawn due to the lack of efficacy or severe side effects.41,56
Many SMTTs are still in their early stages of preclinical development, and there are still challenges for the future translation of these SMTTs to the clinic. BTA can be considered as an exceptionally good example of SMTTs in bone metastasis treatment. However, no other SMTT has been discovered as successfully as BTA in bone metastasis treatment even decades after the approval of BTAs. Several challenges have to be overcome to increase the success of SMTTs in bone metastasis treatment: 1) How to increase the metabolic stability and prolong the plasma circulation time; 2) How to deliver the SMTTs specifically to the metastatic bone lesions; 3) How to greatly reduce the cytotoxicity of SMTTs to normal organs; 4) How to overcome de novo and acquired resistance due to the complex and dynamic microenvironments and original tumor itself. With the success of antibody-drug conjugates (ADC) in clinic, this strategy can also be used as a new direction of SMTTs development in bone metastases in the future.
Combination Therapy
By combining two or more therapeutic agents, combination therapy results in more efficient tumor killing by achieving synergistic anticancer activity, improves treatment outcomes by reducing the emergence of drug resistance, and reduces the toxicity by decreasing the dosage of the individual drug.57,58 We collected 52 combination therapy trials for patients with bone metastases accounting for 11.1% (52/467) of all interventional trials (Figure 3B). Radiotherapy, BTA, and chemotherapy are the cornerstones of the combination therapy, representing 48.1% (25/52), 44.2% (23/52), and 30.8% (16/52) of the combination therapy trials. As we discussed before, the combination of mTOR inhibitor, everolimus, plus aromatase inhibitor, exemestane, was presented as a good example of combination therapy in the treatment of breast cancer with bone metastases.52,54 Combination therapies of Ra-223 with chemotherapeutic agents (cabazitaxel and docetaxel), hormonal therapies (enzalutamide and abiraterone), poly-ADP ribose polymerase (PARP) inhibitors (niraparib and olaparib), or immunotherapy (atezolizumab and pembrolizumab) in patients with bone metastases from mCRPC were comprehensively reviewed by Cursano et al.59 One small size, retrospective clinical study indicated that radiotherapy combined with BTA was superior to BTA alone for the treatment of osteolytic bone metastasis.60 With the rapid development of high throughput drug screens, CRISPR-cas9 knockout based gene dependence screens, and single cell sequencing, more new vulnerabilities will be discovered as potential targets to antagonize the emergence of treatment-resistant tumors. Furthermore, some of them may even be targeted in advance to prevent the onset of resistance by combining with the standard of care.
Future Perspective
Although progress has been achieved in the management of SREs and improvement of patients’ lives, treatments do not address the specific issues of the patients with bone metastases such as tumor dormancy and colonization, acquired resistance from the treatment, or improvement of overall survival. Over the past several decades, our knowledge to understand both the mechanism of action and possible resistance to the treatment of bone metastases has changed dramatically due to the development of preclinical and clinical studies. Improvement in progression-free survival and, ultimately, in OS is the final goal of the treatment in patients with bone metastases. To achieve this goal, more efforts can be focused on the study of the molecular mechanism of tumor heterogeneity, utilizing the new large-scale screens and other new advanced technologies in early diagnosis and prognosis evaluation of bone metastases.
Targeting Intratumor Heterogeneity of Bone Metastases
Tumor heterogeneity of both cancer cells and cells composing the tumor microenvironment, which contributes to drug resistance and compromises treatment outcomes, is one of the major problems in bone metastasis treatment. Tumor heterogeneity of bone metastases not only comes from the primary tumors, such as tumors from breast,61 prostate,62 lung,62 thyroid,63 and kidney64, but also from the bone microenvironment which further adds complexity to tumor heterogeneity by introducing cooperative reciprocal interactions among tumor cells, the mineralized bone matrix, osteoclasts and osteoblasts.65 This complexity of tumor heterogeneity greatly hinders progress in drug development in bone metastases, reflecting the extraordinarily high failure rate of drugs developed for this disease, and may explain the reason why the number of new registered clinical trials for bone metastases decreases since 2019 (Figure 2D). Therefore, better understanding of inherent features underlying the dynamic heterogeneity within the tumor ecosystem and the application of this knowledge for the future treatment design are essential for the development of effective and durable therapeutic strategies for patients with bone metastases.
So far, our knowledge about the functional role of intratumoral heterogeneity in cancers is largely obtained from the analysis of bulk tumor specimens, especially from different types of bulk sequencing; however, diverse subpopulations, mixed nonmalignant cells, and dynamic evolution of cancer cells during continuous treatment limit the characterization of the underlying mechanism of intratumoral heterogeneity. Single-cell sequencing technologies are emerging, advancing, and promising sequencing strategies with considerable potential to unveil the complex architecture of clonal heterogeneity of cancers. Currently, single-cell sequencing technologies can be used to analyze not only tumor heterogeneity, but also other metastasis-related malignant biological characteristics, such as microenvironment and drug resistance, and construction of metastasis-related cell maps for monitoring the dynamics of metastasis and identifying new vulnerabilities to targeted therapy.66–68 Single-cell sequencing includes a series of technologies that evaluate cells at the genomic, epigenomic, transcriptomic, and proteomic levels between primary sites and metastases, but also before and after drug treatments.69 Single-cell sequencing has been used in a clinical trial to build a risk prediction model of bone-related events and verify the comprehensive treatment of bone metastases in patients with non-small cell lung cancer (NCT04568291).
Discovering Novel Vulnerabilities of Bone Metastases
Due to the complexity of original tumors themselves and crosstalk between tumor and its microenvironment, treatment options for bone metastases are still limited, among which the most recently approved treatment was approved years ago. In the previous several years, the newly registered treatments for bone metastases even started to decrease. It is the urgent task not only for the researchers but also for the clinicians to discover new treatments to improve the survival of patients with bone metastases. As promising approaches to screen out new potential therapies for bone metastases, large-scale screens, such as drug screen and CRISPR screen, have already shown their power in the discovery of previously unknown molecular mechanisms and uncovering new vulnerabilities of tumors in preclinical studies. The first drug screening was conducted in small-size cancer cell lines by the National Cancer Institute (NCI) in the 1980s. To date, over 100,000 compounds have been screened in more than 1000 cancer cell lines by many different institutes either in academia or in industries, such as NCI, the Sanger Institute, the Broad Institute, the Institute for Molecular Medicine Finland, GlaxoSmithKline, the MGH cancer center, Novartis, Berkeley National Laboratory, and Genentech.70 Recent advances in technology and screening techniques have allowed high-throughput screening of drug-drug combinations71–73 as well as the ability to pool cancer cell lines together for both in vitro and in vivo drug screening.74 Large-scale drug screening was also reported to be used in the repurposing of previously FDA-approved drugs in pancreatic cancers.75
Genetic screenings provide new approaches for dissecting all facets of cell biology, including genes, functions, and mechanisms involved in a given biological process or phenotype. CRISPR screen, not only for programmable DNA editing with wide type Cas9,76 but also for transcriptional and epigenomic regulation by using dead Cas9D10A/H840A (dCas9), has emerged as one of the most powerful and flexible types of genetic screening.77,78 Importantly, the CRISPR cas9 edited cells can be compared between different time points and combined with different challenges, such as drug treatment in cancer cells for the study of drug resistance and discovery of new vulnerabilities for bone metastases. Single-cell sequencing can also be used to combine with CRISPR screens to simultaneously determine the gRNAs which produce a perturbation and meanwhile the corresponding transcriptome profiles at the single cell level. It is expected that CRISPR screens will be used in the study of the molecular mechanism of bone metastases and the discovery of new treatment options for patients with this disease.
Summary
Bone is among the sites with the most frequent metastases, especially from breast, prostate, and lung cancer. SREs are one of the major issues for patients with bone metastases, leading to serious negative consequences for those patients. Bone metastasis treatment is mainly aimed at relief of SREs and preventing disease progression. In this review, we analyzed the clinical studies related to bone metastases downloaded from ClinicalTrials.gov and pharma.id.informa.com. We found that limited new treatment options finally went to the final steps of clinical trials and the number of clinical trials for bone metastases did not increase too much in the past decade and even started to decrease in recent years. Our comprehensive analysis provides valuable information regarding the current treatments of bone metastases which may be helpful to investigators and also industry for future decisions. We also provided many advanced technologies for the future study of the molecular mechanism and future development of treatment options in patients with bone metastatic cancer.
Data Sharing Statement
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or conflict with the subject matter or materials discussed in the manuscript.
References
1. Weilbaecher KN, Guise TA, McCauley LK. Cancer to bone: a fatal attraction. Nat Rev Cancer. 2011;11(6):411–425. doi:10.1038/nrc3055
2. Hernandez RK, Wade SW, Reich A, et al. Incidence of bone metastases in patients with solid tumors: analysis of oncology electronic medical records in the United States. BMC Cancer. 2018;18(1):44. doi:10.1186/s12885-017-3922-0
3. Luzzi KJ, MacDonald IC, Schmidt EE, et al. Multistep nature of metastatic inefficiency: dormancy of solitary cells after successful extravasation and limited survival of early micrometastases. Am J Pathol. 1998;153(3):865–873. doi:10.1016/S0002-9440(10)65628-3
4. Chaffer CL, San Juan BP, Lim E, et al. EMT, cell plasticity and metastasis. Cancer Metastasis Rev. 2016;35(4):645–654. doi:10.1007/s10555-016-9648-7
5. Macedo F, Ladeira K, Pinho F, et al. Bone metastases: an overview. Oncol Rev. 2017;11(1):321. doi:10.4081/oncol.2017.321
6. Croucher PI, McDonald MM, Martin TJ. Bone metastasis: the importance of the neighbourhood. Nat Rev Cancer. 2016;16(6):373–386. doi:10.1038/nrc.2016.44
7. Hofbauer LC, Bozec A, Rauner M, et al. Novel approaches to target the microenvironment of bone metastasis. Nat Rev Clin Oncol. 2021;18(8):488–505. doi:10.1038/s41571-021-00499-9
8. Wortzel I, Dror S, Kenific CM, et al. Exosome-mediated metastasis: communication from a distance. Dev Cell. 2019;49(3):347–360. doi:10.1016/j.devcel.2019.04.011
9. Paiva AE, Lousado L, Guerra DAP, et al. Pericytes in the premetastatic niche. Cancer Res. 2018;78(11):2779–2786. doi:10.1158/0008-5472.CAN-17-3883
10. Fidler IJ. The pathogenesis of cancer metastasis: the ‘seed and soil’ hypothesis revisited. Nat Rev Cancer. 2003;3(6):453–458. doi:10.1038/nrc1098
11. Yoneda T, Hiraga T. Crosstalk between cancer cells and bone microenvironment in bone metastasis. Biochem Biophys Res Commun. 2005;328(3):679–687. doi:10.1016/j.bbrc.2004.11.070
12. Guise TA. The vicious cycle of bone metastases. J Musculoskelet Neuronal Interact. 2002;2(6):570–572.
13. Mundy GR. Metastasis to bone: causes, consequences and therapeutic opportunities. Nat Rev Cancer. 2002;2(8):584–593. doi:10.1038/nrc867
14. Mundy GR. Mechanisms of bone metastasis. Cancer. 1997;80(8 Suppl):1546–1556.
15. Schramek D, Leibbrandt A, Sigl V, et al. Osteoclast differentiation factor RANKL controls development of progestin-driven mammary cancer. Nature. 2010;468(7320):98–102. doi:10.1038/nature09387
16. Coleman R, Body JJ, Aapro M, et al. Bone health in cancer patients: ESMO clinical practice guidelines. Ann Oncol. 2014;25(Suppl 3):iii124–iii137. doi:10.1093/annonc/mdu103
17. Van Poznak C, Somerfield MR, Barlow WE, et al. Role of bone-modifying agents in metastatic breast cancer: an American society of clinical oncology-cancer care Ontario focused guideline update. J Clin Oncol. 2017;35(35):3978–3986. doi:10.1200/JCO.2017.75.4614
18. Wong R, Wiffen PJ. Bisphosphonates for the relief of pain secondary to bone metastases. Cochrane Database Syst Rev. 2002;2002(2):CD002068. doi:10.1002/14651858.CD002068
19. Hughes DE, Wright KR, Uy HL, et al. Bisphosphonates promote apoptosis in murine osteoclasts in vitro and in vivo. J Bone Miner Res. 2009;10(10):1478–1487. doi:10.1002/jbmr.5650101008
20. Fleisch H. Bisphosphonates: mechanisms of action. Endocr Rev. 1998;19(1):80–100. doi:10.1210/edrv.19.1.0325
21. Lacey DL, Boyle WJ, Simonet WS, et al. Bench to bedside: elucidation of the OPG–RANK–RANKL pathway and the development of denosumab. Nat Rev Drug Discov. 2012;11(5):401–419. doi:10.1038/nrd3705
22. Rosen LS, Gordon D, Tchekmedyian NS, et al. Long-term efficacy and safety of zoledronic acid in the treatment of skeletal metastases in patients with nonsmall cell lung carcinoma and other solid tumors: a randomized, Phase III, double-blind, placebo-controlled trial. Cancer. 2004;100(12):2613–2621. doi:10.1002/cncr.20308
23. Rosen LS, Gordon D, Tchekmedyian S, et al. Zoledronic acid versus placebo in the treatment of skeletal metastases in patients with lung cancer and other solid tumors: a phase III, double-blind, randomized trial—the zoledronic acid lung cancer and other solid tumors study group. J Clin Oncol. 2003;21(16):3150–3157. doi:10.1200/JCO.2003.04.105
24. Fizazi K, Carducci M, Smith M, et al. Denosumab versus zoledronic acid for treatment of bone metastases in men with castration-resistant prostate cancer: a randomised, double-blind study. Lancet. 2011;377(9768):813–822. doi:10.1016/S0140-6736(10)62344-6
25. Stopeck AT, Lipton A, Body -J-J, et al. Denosumab compared with zoledronic acid for the treatment of bone metastases in patients with advanced breast cancer: a randomized, double-blind study. J Clin Oncol. 2010;28(35):5132–5139. doi:10.1200/JCO.2010.29.7101
26. Henry DH, Costa L, Goldwasser F, et al. Randomized, double-blind study of denosumab versus zoledronic acid in the treatment of bone metastases in patients with advanced cancer (excluding breast and prostate cancer) or multiple myeloma. J Clin Oncol. 2011;29(9):1125–1132. doi:10.1200/JCO.2010.31.3304
27. Gnant M, Pfeiler G, Steger GG, et al. Adjuvant denosumab in postmenopausal patients with hormone receptor-positive breast cancer (ABCSG-18): disease-free survival results from a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2019;20(3):339–351. doi:10.1016/S1470-2045(18)30862-3
28. Gnant M, Pfeiler G, Dubsky PC, et al. Adjuvant denosumab in breast cancer (ABCSG-18): a multicentre, randomised, double-blind, placebo-controlled trial. Lancet. 2015;386(9992):433–443. doi:10.1016/S0140-6736(15)60995-3
29. Tsourdi E, Langdahl B, Cohen-Solal M, et al. Discontinuation of denosumab therapy for osteoporosis: a systematic review and position statement by ECTS. Bone. 2017;105:11–17. doi:10.1016/j.bone.2017.08.003
30. Smith MR, Egerdie B, Toriz NH, et al. Denosumab in men receiving androgen-deprivation therapy for prostate cancer. N Engl J Med. 2009;361(8):745–755. doi:10.1056/NEJMoa0809003
31. Smith MR, Saad F, Coleman R, et al. Denosumab and bone-metastasis-free survival in men with castration-resistant prostate cancer: results of a phase 3, randomised, placebo-controlled trial. Lancet. 2012;379(9810):39–46. doi:10.1016/S0140-6736(11)61226-9
32. Scagliotti GV, Hirsh V, Siena S, et al. Overall survival improvement in patients with lung cancer and bone metastases treated with denosumab versus zoledronic acid: subgroup analysis from a randomized phase 3 study. J Thorac Oncol. 2012;7(12):1823–1829. doi:10.1097/JTO.0b013e31826aec2b
33. Michael Gnant MD, Frantal S, Pfeiler G, et al. Long-term outcomes of adjuvant denosumab in breast cancer. NEJM. 2022;12(1):EVIDoa2200162.
34. von Moos R, Lewis K, Massey L, et al. Initiation of bone-targeted agents in patients with bone metastases and breast or castrate-resistant prostate cancer actively treated in routine clinical practice in Europe. Bone. 2022;154:116243. doi:10.1016/j.bone.2021.116243
35. Coleman R, Hadji P, Body -J-J, et al. Bone health in cancer: ESMO clinical practice guidelines. Ann Oncol. 2020;31(12):1650–1663. doi:10.1016/j.annonc.2020.07.019
36. Goblirsch MJ, Zwolak PP, Clohisy DR. Biology of bone cancer pain. Clin Cancer Res. 2006;12(20):6231s–6235s. doi:10.1158/1078-0432.CCR-06-0682
37. Rich SE, Chow R, Raman S, et al. Update of the systematic review of palliative radiation therapy fractionation for bone metastases. Radiother Oncol. 2018;126(3):547–557. doi:10.1016/j.radonc.2018.01.003
38. Hoskin PJ, Hopkins K, Misra V, et al. Effect of single-fraction vs multifraction radiotherapy on ambulatory status among patients with spinal canal compression from metastatic cancer: the SCORAD randomized clinical trial. JAMA. 2019;322(21):2084–2094. doi:10.1001/jama.2019.17913
39. Nilsson S, Larsen RH, Fossa SD, et al. First clinical experience with α-emitting radium-223 in the treatment of skeletal metastases. Clin Cancer Res. 2005;11(12):4451–4459. doi:10.1158/1078-0432.CCR-04-2244
40. Coleman R. Treatment of metastatic bone disease and the emerging role of radium-223. Semin Nucl Med. 2016;46(2):99–104. doi:10.1053/j.semnuclmed.2015.10.012
41. Sousa S, Clezardin P. Bone-targeted therapies in cancer-induced bone disease. Calcif Tissue Int. 2018;102(2):227–250. doi:10.1007/s00223-017-0353-5
42. Parker C, Lewington V, Shore N, et al. Targeted alpha therapy, an emerging class of cancer agents: a review. JAMA Oncol. 2018;4(12):1765–1772. doi:10.1001/jamaoncol.2018.4044
43. Finlay IG, Mason MD, Shelley M. Radioisotopes for the palliation of metastatic bone cancer: a systematic review. Lancet Oncol. 2005;6(6):392–400. doi:10.1016/S1470-2045(05)70206-0
44. Garg AK, Shiu AS, Yang J, et al. Phase 1/2 trial of single-session stereotactic body radiotherapy for previously unirradiated spinal metastases. Cancer. 2012;118(20):5069–5077. doi:10.1002/cncr.27530
45. Gerszten PC, Burton SA, Ozhasoglu C, et al. Radiosurgery for spinal metastases: clinical experience in 500 cases from a single institution. Spine. 2007;32(2):193–199. doi:10.1097/01.brs.0000251863.76595.a2
46. Bishop AJ, Tao R, Guadagnolo BA, et al. Spine stereotactic radiosurgery for metastatic sarcoma: patterns of failure and radiation treatment volume considerations. J Neurosurg Spine. 2017;27(3):303–311. doi:10.3171/2017.1.SPINE161045
47. Yamada Y, Katsoulakis E, Laufer I, et al. The impact of histology and delivered dose on local control of spinal metastases treated with stereotactic radiosurgery. Neurosurg Focus. 2017;42(1):E6. doi:10.3171/2016.9.FOCUS16369
48. Jhaveri PM, Teh BS, Paulino AC, et al. A dose-response relationship for time to bone pain resolution after stereotactic body radiotherapy (SBRT) for renal cell carcinoma (RCC) bony metastases. Acta Oncol. 2012;51(5):584–588. doi:10.3109/0284186X.2011.652741
49. Bedard PL, Hyman DM, Davids MS, et al. Small molecules, big impact: 20 years of targeted therapy in oncology. Lancet. 2020;395(10229):1078–1088. doi:10.1016/S0140-6736(20)30164-1
50. Carducci MA, Saad F, Abrahamsson P-A, et al. A phase 3 randomized controlled trial of the efficacy and safety of atrasentan in men with metastatic hormone-refractory prostate cancer. Cancer. 2007;110(9):1959–1966. doi:10.1002/cncr.22996
51. Nelson JB, Fizazi K, Miller K, et al. Phase 3, randomized, placebo-controlled study of zibotentan (ZD4054) in patients with castration-resistant prostate cancer metastatic to bone. Cancer. 2012;118(22):5709–5718. doi:10.1002/cncr.27674
52. Gnant M, Baselga J, Rugo HS, et al. Effect of everolimus on bone marker levels and progressive disease in bone in BOLERO-2. J Natl Cancer Inst. 2013;105(9):654–663. doi:10.1093/jnci/djt026
53. Hortobagyi GN. Everolimus plus exemestane for the treatment of advanced breast cancer: a review of subanalyses from BOLERO-2. Neoplasia. 2015;17(3):279–288. doi:10.1016/j.neo.2015.01.005
54. Bertoldo F, Silvestris F, Ibrahim T, et al. Targeting bone metastatic cancer: role of the mTOR pathway. Biochim Biophys Acta. 2014;1845(2):248–254. doi:10.1016/j.bbcan.2014.01.009
55. Escudier B, Powles T, Motzer RJ, et al. Cabozantinib, a new standard of care for patients with advanced renal cell carcinoma and bone metastases? Subgroup analysis of the METEOR trial. J Clin Oncol. 2018;36(8):765–772. doi:10.1200/JCO.2017.74.7352
56. Bone HG, Dempster DW, Eisman JA, et al. Odanacatib for the treatment of postmenopausal osteoporosis: development history and design and participant characteristics of LOFT, the long-term odanacatib fracture trial. Osteoporos Int. 2015;26(2):699–712. doi:10.1007/s00198-014-2944-6
57. Bukowska B, Gajek A, Marczak A. Two drugs are better than one. A short history of combined therapy of ovarian cancer. Contemp Oncol. 2015;19(5):350–353.
58. Palmer AC, Chidley C, Sorger PK. A curative combination cancer therapy achieves high fractional cell killing through low cross-resistance and drug additivity. Elife. 2019;8:e50036.
59. Cursano MC, Iuliani M, Casadei C, et al. Combination radium-223 therapies in patients with bone metastases from castration-resistant prostate cancer: a review. Crit Rev Oncol Hematol. 2020;146:102864. doi:10.1016/j.critrevonc.2020.102864
60. Tanaka H, Makita C, Manabe Y, et al. Radiation therapy combined with bone-modifying agents ameliorates local control of osteolytic bone metastases in breast cancer. J Radiat Res. 2020;61(3):494–498. doi:10.1093/jrr/rraa020
61. Turashvili G, Brogi E. Tumor heterogeneity in breast cancer. Front Med. 2017;4:227. doi:10.3389/fmed.2017.00227
62. Haffner MC, Zwart W, Roudier MP, et al. Genomic and phenotypic heterogeneity in prostate cancer. Nat Rev Urol. 2021;18(2):79–92. doi:10.1038/s41585-020-00400-w
63. Chmielik E, Rusinek D, Oczko-Wojciechowska M, et al. Heterogeneity of thyroid cancer. Pathobiology. 2018;85(1–2):117–129. doi:10.1159/000486422
64. Beksac AT, Paulucci DJ, Blum KA, et al. Heterogeneity in renal cell carcinoma. Urol Oncol. 2017;35(8):507–515. doi:10.1016/j.urolonc.2017.05.006
65. Futakuchi M, Fukamachi K, Suzui M. Heterogeneity of tumor cells in the bone microenvironment: mechanisms and therapeutic targets for bone metastasis of prostate or breast cancer. Adv Drug Deliv Rev. 2016;99(20):206–211. doi:10.1016/j.addr.2015.11.017
66. Xu X, Hou Y, Yin X, et al. Single-cell exome sequencing reveals single-nucleotide mutation characteristics of a kidney tumor. Cell. 2012;148(5):886–895. doi:10.1016/j.cell.2012.02.025
67. Navin N, Kendall J, Troge J, et al. Tumour evolution inferred by single-cell sequencing. Nature. 2011;472(7341):90–94. doi:10.1038/nature09807
68. Francis JM, Zhang C-Z, Maire CL, et al. EGFR variant heterogeneity in glioblastoma resolved through single-nucleus sequencing. Cancer Discov. 2014;4(8):956–971. doi:10.1158/2159-8290.CD-13-0879
69. Han Y, Wang D, Peng L, et al. Single-cell sequencing: a promising approach for uncovering the mechanisms of tumor metastasis. J Hematol Oncol. 2022;15(1):59. doi:10.1186/s13045-022-01280-w
70. Ling A, Gruener RF, Fessler J, et al. More than fishing for a cure: the promises and pitfalls of high throughput cancer cell line screens. Pharmacol Ther. 2018;191:178–189. doi:10.1016/j.pharmthera.2018.06.014
71. Holbeck SL, Camalier R, Crowell JA, et al. The national cancer institute ALMANAC: a comprehensive screening resource for the detection of anticancer drug pairs with enhanced therapeutic activity. Cancer Res. 2017;77(13):3564–3576. doi:10.1158/0008-5472.CAN-17-0489
72. Jaaks P, Coker EA, Vis DJ, et al. Effective drug combinations in breast, colon and pancreatic cancer cells. Nature. 2022;603(7899):166–173. doi:10.1038/s41586-022-04437-2
73. Zagidullin B, Aldahdooh J, Zheng S, et al. DrugComb: an integrative cancer drug combination data portal. Nucleic Acids Res. 2019;47(W1):W43–W51. doi:10.1093/nar/gkz337
74. Yu C, Mannan AM, Yvone GM, et al. High-throughput identification of genotype-specific cancer vulnerabilities in mixtures of barcoded tumor cell lines. Nat Biotechnol. 2016;34(4):419–423. doi:10.1038/nbt.3460
75. Hirt CK, Booij TH, Grob L, et al. Drug screening and genome editing in human pancreatic cancer organoids identifies drug-gene interactions and candidates for off-label therapy. Cell Genom. 2022;2(2):100095. doi:10.1016/j.xgen.2022.100095
76. Jinek M, Chylinski K, Fonfara I, et al. A programmable dual-RNA–guided DNA endonuclease in adaptive bacterial immunity. Science. 2012;337(6096):816–821. doi:10.1126/science.1225829
77. Adli M. The CRISPR tool kit for genome editing and beyond. Nat Commun. 2018;9(1):1911. doi:10.1038/s41467-018-04252-2
78. Qi LS, Larson M, Gilbert L, et al. Repurposing CRISPR as an RNA-guided platform for sequence-specific control of gene expression. Cell. 2013;152(5):1173–1183. doi:10.1016/j.cell.2013.02.022
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.