Back to Journals » Journal of Pain Research » Volume 19
A Comprehensive Evidence-Based Review of Non-Pharmaceutical Interventions for Neonatal Pain
Received 29 September 2025
Accepted for publication 7 January 2026
Published 8 April 2026 Volume 2026:19 571070
DOI https://doi.org/10.2147/JPR.S571070
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Ferry Efendi
Yongxue Cai,1 Shanghui Sun,2 Chunli Chen2
1Department of Neonatology, The Second People’s Hospital of Hefei, Hefei, Anhui, 230011, People’s Republic of China; 2Department of Nursing, The Second People’s Hospital of Hefei, Hefei, Anhui, 230011, People’s Republic of China
Correspondence: Chunli Chen, Department of Nursing, The Second People’s Hospital of Hefei, Hefei, Anhui, 230011, People’s Republic of China, Email [email protected]; [email protected]
Abstract: This narrative evidence-based review examines current progress in non-pharmaceutical interventions (NPIs) for neonatal pain, a critical factor influencing neurodevelopment and long-term health. NPIs offer safer alternatives to pharmacologic treatments in this vulnerable population. This review summarises advances in auditory approaches (white noise, maternal voice), oral–tactile strategies (non-nutritive sucking, oral glucose/sucrose), tactile interventions (kangaroo care) Yongxue Cai and positional support. These methods alleviate pain by activating endogenous opioid pathways, reducing stress hormone responses and recreating intrauterine-like sensory environments that modulate nociception. Collectively, NPIs reduce behavioral and physiological indicators of pain, enhance sensory integration and promote autonomic stability. Despite their benefits, challenges remain, including heterogeneous study designs, limited sample sizes and clinical constraints such as inadequate provider training and resource limitations in neonatal intensive care units. Future work should focus on large, standardised trials to establish optimal intervention protocols. Integration of neuroimaging and molecular tools may clarify central mechanisms, while personalised approaches using real-time physiological data could support precision pain management. Strengthening the evidence base will enable NPIs to evolve from empirically used techniques into standardised, neuroprotective strategies that improve both immediate comfort and long-term outcomes for neonates.
Keywords: neonatal pain, non-pharmaceutical interventions, tactile stimulation, auditory interventions, neurodevelopmental outcomes, precision medicine
Introduction
Neonatal pain, particularly procedural pain from routine medical interventions such as heel lance, venipuncture and endotracheal suctioning, represents a significant clinical concern with both immediate and long-term implications for vulnerable infants.1–3 Up to 90% of neonates in intensive care units undergo repeated noxious procedures, which can disrupt physiological stability and influence neurodevelopmental outcomes. Unmanaged pain activates stress pathways, elevating cortisol and catecholamines, leading to autonomic instability, reduced oxygen saturation and altered metabolic balance.4,5 Early-life pain exposure may also induce synaptic changes in developing brain regions, potentially contributing to long-term alterations in pain sensitivity, emotional regulation and cognition.6–8 Clinically, these physiological disruptions manifest as altered sleep patterns, feeding difficulties and impaired growth, especially in preterm or critically ill infants.
Accurate assessment of neonatal pain is a critical prerequisite for effective pain management. Currently, pain assessment relies primarily on validated behavioral and physiological scales such as the Neonatal Infant Pain Scale (NIPS), the Premature Infant Pain Profile (PIPP and PIPP-R) and the COMFORT scale. These tools evaluate parameters including facial expressions, body movements, cry characteristics, heart rate and oxygen saturation. While widely used, they present several limitations: behavioral cues may be blunted in preterm or neurologically compromised infants; physiological indicators lack specificity and can be influenced by factors unrelated to pain; and inter-observer variability can compromise reliability. In addition, the absence of a universal gold standard, challenges in real-time assessment during rapid bedside procedures and the difficulty of interpreting pain in non-verbal patients highlight ongoing gaps in neonatal pain evaluation. These challenges underline the need for consistent, systematic assessment practices as recommended by international guidelines.
International guidelines, including those from the American Academy of Pediatrics (AAP), the Canadian Paediatric Society (CPS) and the European Society of Paediatric and Neonatal Intensive Care (ESPNIC), affirm that all neonates experience pain and recommend routine pain assessment alongside the systematic use of non-pharmacological strategies as first-line interventions. Despite these recommendations, pharmacological options present essential limitations.9 Opioids pose risks such as respiratory depression and neonatal abstinence syndrome, while non-steroidal anti-inflammatory drugs may adversely affect gastrointestinal and renal function in immature systems.10 These safety concerns have intensified interest in non-pharmaceutical interventions (NPIs), which modulate sensory or environmental factors to alleviate pain without systemic side effects. Approaches such as kangaroo care, non-nutritive sucking and oral sweet solutions consistently reduce behavioral and physiological indicators of pain, supporting their role in routine neonatal care.11–13
The objective of this review is to synthesise current evidence on NPIs for neonatal pain management, highlighting their mechanisms, clinical applicability and performance across different neonatal populations. The review also evaluates methodological issues such as variability in intervention protocols, small sample sizes and limited long-term follow-up to identify research gaps that constrain clinical translation. Additionally, emerging directions such as multimodal approaches, personalised interventions based on neonatal characteristics and advancements in real-time pain-monitoring technologies are discussed. A conceptual summary is provided to illustrate the major categories of non-pharmacological interventions (NPIs) and their underlying mechanisms (Figure 1). By integrating available evidence, this review aims to guide clinicians and researchers toward improving safe, effective and evidence-based pain management for neonates.
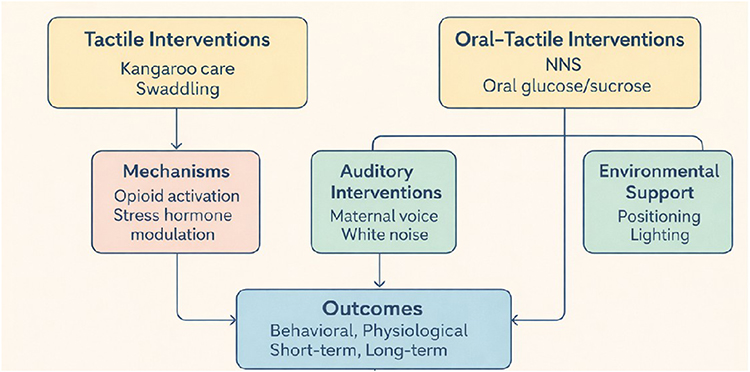 |
Figure 1 Conceptual Diagram of Non-Pharmaceutical Interventions for Neonatal Pain. |
Neonatal Pain: Concepts, Impacts and Assessment
Concepts of Neonatal Pain
According to the International Association for the Study of Pain, pain is “an unpleasant sensory and emotional experience associated with actual or potential tissue damage”, a definition that includes non-verbal individuals such as neonates.14 This recognition counters historical assumptions that newborns experience diminished pain due to neurological immaturity. Research shows that by 22–24 weeks of gestation, nociceptive pathways from peripheral receptors to central processing centers are functionally active, enabling neonates to detect and respond to noxious stimuli.15 Dense epidermal nociceptors and intact neural pathways allow newborns to exhibit behavioral (eg., facial grimacing, limb withdrawal) and physiological (eg., tachycardia, cortisol increase) responses indicative of accurate pain perception.16
Neonatal pain processing differs from that of adults due to underdeveloped inhibitory pathways, including descending serotonergic and noradrenergic systems.17,18 As a result, neonates often exhibit exaggerated and prolonged responses to painful stimuli. Even minor procedures may provoke sustained autonomic changes and increased sensitivity because of limited regulatory control.19 The high neuroplasticity of the neonatal brain further increases vulnerability: repeated early pain can modify synaptic organisation in regions such as the prefrontal cortex and amygdala, potentially influencing later stress reactivity and sensory processing.20
The consequences of untreated neonatal pain extend from immediate physiological disruption to long-term developmental effects. In the short term, unmanaged pain interferes with feeding, sleep regulation and immune function—critical factors for growth and recovery.9 Behaviorally, it may lead to irritability, prolonged crying and reduced stress tolerance.21 Over time, cumulative painful experiences during early development have been linked to altered hypothalamic–pituitary–adrenal axis function, structural brain changes, cognitive impairments and greater risk of emotional and behavioral issues in later childhood.22 These findings emphasise the importance of effective, early pain management strategies in neonatal care.
Impacts of Neonatal Pain
Neonatal pain has profound effects on both short-term physiological stability and long-term neurodevelopment, making it a significant threat to infant health. Acutely, unmanaged pain activates the sympathetic nervous system, leading to increased heart rate,23 elevated blood pressure24 and oxygen desaturation,25 all of which strain immature cardiovascular and respiratory systems. These responses signify disrupted homeostasis; even a single invasive procedure can raise cortisol levels by 20–30%, altering metabolic and immune functions essential for growth.26 Behaviorally, neonates may exhibit prolonged crying, disturbed sleep–wake patterns and feeding difficulties, which can reduce caloric intake and delay recovery.27 Such physiological and behavioral disruptions can amplify one another, diminishing the infant’s resilience to subsequent procedures.
These acute disturbances also contribute to long-term risks, as repeated pain exposure during critical developmental periods may affect brain organisation, stress regulation and later cognitive and behavioral outcomes. Recognising neonatal pain as a modifiable risk factor emphasises the need for timely, evidence-based management. Prioritising effective non-pharmacological strategies can help mitigate both immediate distress and potential lifelong consequences, ultimately supporting better short- and long-term health in this vulnerable population.
Assessment of Neonatal Pain
Neonatal pain assessment is crucial and several non-pharmacological instruments have been developed (Table 1). The Neonatal Facial Coding System (NFCS) evaluates nine facial action items, scoring 0–9 for full-term and 0–10 for preterm neonates and is used for procedural pain assessment with good reliability and validity.28 The Face, Legs, Activity, Cry, Consolability (FLACC) scale, designed to assess post-operative pain in preverbal/nonverbal children under 7 years old, evaluates 5 behavioral items with a score range of 0–10 and demonstrates high interrater reliability. COMFORTneo, used for prolonged pain and sedation assessment in neonates (24–42 weeks GA), has 7 items and a score range of 6–30, with acceptable reliability and concurrent validity.29 The Neonatal Infant Pain Scale (NIPS) combines 5 behavioral and 1 physiological item, scoring 0–7, suitable for procedural and post-operative pain in neonates (26–47 weeks GA). It demonstrates high reliability and moderate concurrent validity. The Neonatal Pain, Agitation and Sedation Scale (NPASS) include 4 behavioral and 1 physiological item, scoring 0–10, applicable for various pain types in neonates (23–40 weeks GA), with strong reliability.30 The Premature Infant Pain Profile (PIPP/PIPPR), covering 3 behavioral, 2 physiological and 2 contextual items, scores 0–18 for full-term and 0–21 for preterm neonates, used for procedural/postoperative pain in neonates (28–42 weeks GA) and is highly reliable and valid, especially in research.31 Each instrument has its specific application scenarios, item compositions and reliability-validity characteristics, providing diverse options for neonatal pain assessment.
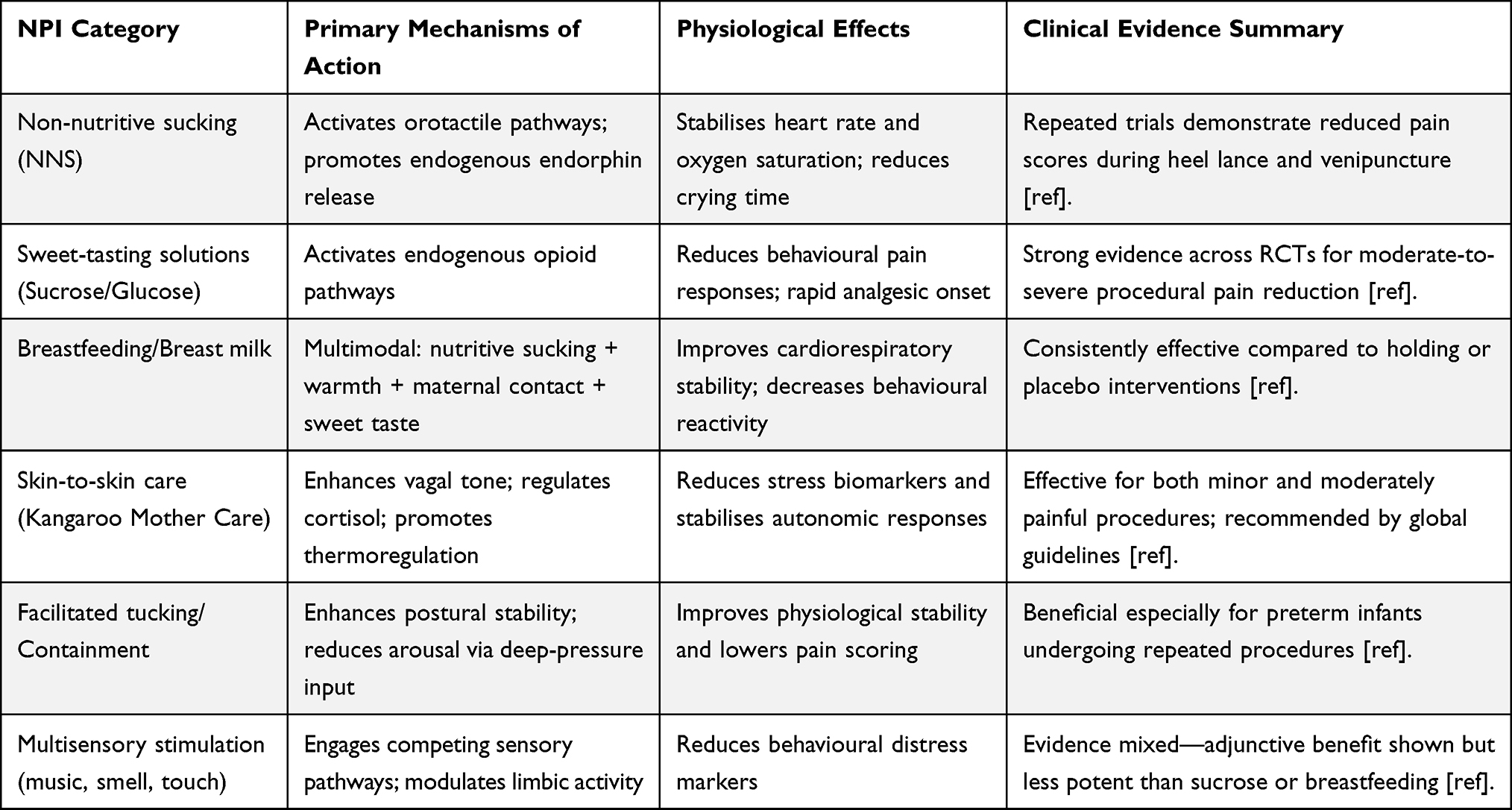 |
Table 1 Comparative Overview of Major Non-Pharmacological Interventions, Their Mechanisms, Physiological Effects, and Supporting Evidence |
These scales each possess unique characteristics. In terms of advantages, the Neonatal Facial Coding System (NFCS) is highly sensitive to the subtle facial movements of neonates, allowing for a practical assessment of procedural pain. The Face, Legs, Activity, Cry, Consolability (FLACC) scale encompasses multiple behavioral dimensions, facilitating the scoring of pain in young children after surgery. COMFORTneo offers a comprehensive evaluation of prolonged pain and sedation in neonates. The Neonatal Infant Pain Scale (NIPS) integrates behavioral and physiological indicators, making it suitable for assessing pain during neonatal surgeries and procedures. The Neonatal Pain, Agitation and Sedation Scale (NPASS) applies across various pain scenarios and demonstrates high reliability and validity. In contrast, the Premature Infant Pain Profile (PIPP/PIPPR) combines multiple factors and is widely used in research. However, they also have limitations. NFCS has a single-item focus, restricting its application; FLACC is not suitable for children who can communicate verbally; COMFORTneo has relatively lower reliability and validity; the physiological indicators of NIPS are easily affected by external factors; NPASS has an imprecise assessment of vital signs; and PIPP/PIPPR is time-consuming, which can be inconvenient in busy clinical settings.
AI-Based Neonatal Pain Assessment
With advances in biomedical engineering and machine learning, artificial intelligence (AI) has emerged as a promising tool to address the limitations of manual, observer-dependent pain scales. AI-based systems aim to provide objective, continuous and automated pain assessment by analysing multimodal neonatal data.
Recent studies have reported successful applications of machine-learning and deep-learning models using:
- Physiological signals, such as heart rate variability, oxygen saturation patterns and EEG/near-infrared spectroscopy data
- Cry analysis, where acoustic features (eg., pitch, intensity, spectral entropy) are used to classify pain states
- Facial expression recognition, using convolutional neural networks (CNNs) to detect brow bulge, eye squeeze and nasolabial furrow
- Video-based behavioural analysis, integrating limb movement, body tension and facial cues
- Multimodal fusion algorithms combining physiological, behavioral and contextual data for improved accuracy
Some systems—such as automated facial recognition platforms and cry-analysis devices—have already undergone prospective evaluation in real-world NICUs, demonstrating feasibility for real-time pain monitoring, reduced inter-observer variability and more timely detection of distress.
Despite these advances, challenges remain, including the need for large annotated datasets, variations across NICUs, ethical considerations, data privacy and the integration of AI outputs into clinical workflows. Nonetheless, AI-based assessment represents an important future direction that can complement traditional scales, enhance early pain detection and support personalised pain management strategies.
Non-Pharmaceutical Intervention Measures for Neonatal Pain
Auditory Interventions
White Noise
White noise, which mimics the low-frequency ambient sounds of the intrauterine environment—such as maternal blood flow and gastrointestinal motility—activates the neonatal auditory system and modulates central nervous system activity, promoting the release of neurotransmitters like dopamine and serotonin while inhibiting stress responses to alleviate anxiety and pain.32 This auditory intervention is hypothesised to create a familiar, soothing environment that recreates the sensory conditions of prenatal life, thereby reducing the neonatal stress response to painful procedures.33 White noise has a relaxing property and is similar to the sounds that a fetus hears in the mother’s womb. It can provide a familiar growth environment for newborns and has a soothing effect on them.34 Akca et al35 divided 127 newborns into two groups. Within one hour after birth, the newborns in the experimental group received a white noise intervention, while the control group received no intervention. The research results showed that white noise could increase the sucking success rate of newborns after birth. Liao et al36 randomly divided 103 preterm infants into three groups: the white noise intervention group, the mother’s voice intervention group and the routine nursing group. The interventions were provided to the newborns three times a day, each time for 20 minutes, over four consecutive days. The research results showed that the newborns in the white noise intervention group had the fastest weight gain. Sezici et al37 designed a randomized controlled trial with a two-stage crossover design. They provided 40 colicky infants with either a one-week white noise intervention or a swinging intervention. The results showed that the white noise intervention could reduce the daily crying time of colicky infants and increase their daily sleep time.37 In addition, white noise suppresses interfering sounds from the external environment through resonance, enhances the processing of information in the nervous system and serves as a regulator of cognition.
In conclusion, white noise, by simulating the sounds in the uterus, activates the auditory system of newborns, regulates the central nervous system, promotes the release of neurotransmitters and inhibits stress responses. It has shown positive effects in improving the success rate of sucking in newborns, accelerating the weight gain of premature infants and alleviating the symptoms of intestinal colic in infants. At the same time, it also has the functions of suppressing external interference and enhancing cognitive regulation. Based on existing research results, white noise has significant application potential in the field of neonatal care, offering a new direction for optimizing the growth environment and care strategies for newborns. However, research on the optimal duration, intensity and long-term effects of white noise intervention is still relatively limited at present. Future studies can further explore personalised application schemes of white noise in different neonatal groups, assess its potential risks and improve the relevant theoretical system, thereby applying white noise more safely and effectively in neonatal clinical care and family upbringing practices.
Maternal Voice
The maternal voice, serving as the earliest familiar auditory signal for neonates, exerts analgesic effects through neuroemotional bonding and physiological stabilization. Prenatally, fetal exposure to the maternal voice, transmitted through amniotic fluid, imprints a sensory memory that activates the limbic system post-birth, triggering the release of oxytocin, known for its calming and stress-reducing properties and suppressing cortisol, a key marker of the stress response. This neurobiological pathway creates a soothing effect that mitigates the autonomic arousal associated with painful procedures, as evidenced by reduced heart rate variability, stabilized respiratory patterns and dampened sympathetic nervous system activation.
Neonatal intensive care unit (NICU) patients are frequently exposed to repetitive and multiple painful stimuli due to diagnostic and therapeutic procedures. In China, intravenous puncture alone accounts for 14.86% of all pain-inducing interventions during NICU hospitalization.38 Neonatal pain can trigger a cascade of abnormal physiological and behavioral responses, leading to significant short - and long-term adverse outcomes.39,40 Another study has consistently demonstrated a positive correlation between gestational age and pain sensitivity in preterm infants.41
The efficacy of maternal voice intervention in mitigating procedural pain among preterm infants remains a subject of debate in international research, with conflicting findings regarding its effectiveness.42 Despite this, maternal voice and light music have been increasingly adopted in clinical practice as potential facilitators of preterm infant development, sparking numerous research initiatives.43
Furthermore, mother-infant contact, often initiated through admission education and subsequent interactions, has proven effective in alleviating parental anxiety and promoting early neonatal development, highlighting its crucial role in NICU care.
Music Therapy
Music therapy mitigates neonatal pain by stimulating the auditory cortex, engaging central nervous system mechanisms that modulate nociceptive processing and emotional states.44 The proposed mechanisms include enhancing endogenous endorphin release to inhibit pain pathways and diverting attentional resources via rhythmic or melodic patterns, thereby reducing the perception of noxious stimuli. Soft classical music or recordings of intrauterine sounds—characterized by low-frequency vibrations akin to those found in maternal uterine environments—have demonstrated efficacy in lowering heart rate increases by 10–15 beats per minute and reducing NIPS scores by 1–2 points during heel lance or venipuncture, reflecting a balance between stress reduction and pain modulation.
Music therapy operates on the principle that the auditory system, upon exposure to rhythmic music, modulates cellular excitability through neural synapses, effectively diverting patients’ attention to yield therapeutic benefits.45 Widely adopted as an adjuvant in clinical pain management across numerous countries, its efficacy in neonatal care has been substantiated by multiple studies. Kurdahi et al46 demonstrated that music therapy significantly reduced pain manifestations and stabilized physiological parameters during neonatal heel blood collection. Butt et al47 confirmed its analgesic effect by reducing heart rate in pediatric patients. Additionally, a study on the combined use of breastfeeding and music therapy48 revealed that this approach not only lowered pain scores but also minimized fluctuations in physiological indicators such as heart rate and oxygen saturation, while enhancing the effectiveness of breastfeeding interventions.
These findings highlight the nuanced effects of music therapy, which depend on matching acoustic properties to neonatal sensory preferences and procedural contexts. While consistent evidence supports its use as an adjunctive non-pharmacological strategy, challenges remain in standardizing intervention protocols—such as determining the optimal tempo, volume and music selection—and understanding the long-term impacts on auditory and neural development. Nonetheless, music therapy offers a versatile, low-risk approach that can be integrated with other sensory interventions, holding promise for enhancing neonatal comfort during painful procedures through targeted auditory stimulation.
Oral Interventions
Non-Nutritive Sucking (NNS)
Non-nutritive sucking (NNS) mitigates procedural pain in neonates by stimulating oral tactile receptors, thereby activating trigeminal afferent pathways and promoting the release of neurotransmitters, such as 5-hydroxytryptamine (serotonin), which elevates pain thresholds and diverts attention from noxious stimuli.49,50 Studies have demonstrated that non-nutritive sucking can mitigate the elevation of heart rate during and after intravenous puncture, reduce the decline in oxygen saturation during the recovery phase, shorten the crying time of neonates and lower the duration of pain expressions and neonatal pain scores. A meta-analysis of 23 RCTs involving 1461 preterm infants found that non-nutritive sucking (NNS) significantly shortened the time to exclusive oral feeding, length of hospital stay, time to start oral feeding and time to return to birth weight, increased weight gain at discharge and full oral feeding in the control group, reduced feeding intolerance incidence in preterm infants, though limited by small sample sizes, unaccounted confounding factors, heterogeneity and bias, it still provides valuable insights. It updates evidence on NNS for promoting oral feeding and evidence-based practices in preterm infants.51 Clinically, non-nutritive sucking can be combined with sweeteners52 and music therapy53 to enhance pain relief. While it is a practical strategy for alleviating neonatal procedural pain, concerns remain, such as the potential for oral aversion with prolonged use of reusable pacifiers that can be sterilized after high-pressure steam. Additionally, clinical implementation risks include vomiting, choking, iatrogenic skin damage from tape fixation and pressure injuries if a dislodged pacifier is not promptly retrieved. Although its analgesic benefits are well-established, key questions regarding the optimal duration of intervention to balance pain relief and avoid adverse effects still require further investigation.
Future research should focus on multicenter trials to define evidence-based parameters for NNS, including optimal pacifier specifications and timing protocols, with subgroup analyses to address preterm-neonate-specific efficacy and safety. Exploring combinations of NNS with auditory interventions—such as white noise or maternal voice—to create multimodal strategies holds promise, as integrated sensory stimulation may amplify pain relief through parallel activation of oral-tactile and auditory soothing pathways. Such approaches could leverage NNS’s established safety and accessibility to develop personalized protocols that balance pain management with developmental needs, ensuring that this simple yet powerful intervention is used effectively across diverse clinical contexts.
Oral Glucose/Sucrose
Oral sweet solutions, primarily glucose and sucrose, alleviate neonatal pain by activating taste receptors to engage endogenous opioid pathways, inhibiting nociceptive signal transmission in the spinal dorsal horn and dampening pain perception.13 Oral administration of sucrose or glucose solution is one of the standard non-pharmacological methods for pain intervention, which can relieve pain-induced crying and abnormal behaviors caused by invasive procedures.54 The mechanism of action of oral glucose for analgesia in neonates is not yet fully understood. Animal experimental studies have shown that the oral administration of sweet solutions can be used to activate brainstem structures involved in the descending modulation of pain, such as the periaqueductal gray matter of the midbrain or the nucleus raphe magnus, but does not involve the forebrain.55 Most studies suggest that children can experience an analgesic effect within a few minutes after consuming the glucose solution.56,57 This may be because the glucose solution, acting as a “sweetener”, activates the release of endogenous opioid receptor-like substances through the gustatory system and plays a role in the brainstem pathway of descending pain modulation.
Harrison et al58 conducted a Meta-analysis of previous studies. They pointed out that oral administration of sucrose or glucose solution can reduce the duration of crying and the comprehensive pain score during neonatal blood collection. However, due to the limitations of the database, differences in evaluation methods, inclusion criteria and quality control among the various research protocols, further research is needed. Tanyeri et al59 believed in their study that the minimum effective dose of 24% sucrose at 0.2 mL/kg can relieve the pain of preterm infants during procedural pain. However, long-term oral administration of sucrose may cause short-term or long-term risks, including asphyxia, coughing, vomiting, persistent tachycardia or bradycardia, hyperglycemia or reactive hypoglycemia and even necrotizing enterocolitis. Schneider et al60 believed that long-term exposure to a high dose of sucrose may affect the development of the basal ganglia of the brain in neonates, especially female infants.
Currently, there have been new advancements in the concentration and dosage of orally administered glucose or sucrose solutions. Previous studies suggested that administering 2 mL of 30% glucose/sucrose orally could effectively reduce the pain score in neonates. Increasingly, scholars have recently believed55,61,62 that administering 2 mL of 20% glucose orally to neonates before heel blood collection can weaken or even prevent the pain response of the cerebral cortex.
Future research on oral sweet solutions must prioritize three key areas to advance evidence-based practice: developing personalized dosing algorithms that integrate gestational age, body weight and gastrointestinal function (eg., feeding tolerance) to optimize safety and efficacy—potentially using machine learning to tailor concentrations in real time and reduce risks like NEC and hyperglycemia; conducting longitudinal studies to clarify long-term neurodevelopmental impacts, such as programming of taste pathways and associations with childhood metabolic outcomes, which remain understudied beyond short-term safety; and using neuroimaging tools (NIRS, EEG) to mechanistically explore how combined oral-tactile stimulation enhances central inhibitory pathways, such as whether concurrent taste and tactile activation amplifies opioid/serotonin release in pain-modulating brain regions. Addressing these gaps will transition these interventions from empirical use to precision strategies, ensuring guidelines balance short-term analgesia with long-term developmental safety, particularly in vulnerable neonates.
Kangaroo Care (KC)/Skin-to-Skin Contact
Kangaroo care (KC), also known as skin-to-skin contact, alleviates neonatal pain through multisensory integration, engaging tactile, auditory and olfactory pathways to promote physiological and emotional regulation.63 Through the stimulation of the skin, including tactile, auditory, olfactory and thermal sensations, it can effectively inhibit the activity of the hypothalamic-pituitary-adrenal axis, thereby reducing procedural pain in neonates.22,64,65 Animal experiments have confirmed66 that experiencing repeated pain stimuli and maternal-infant separation in the early stage of life can lead to tactile hypersensitivity and enhance the fear conditioning reflex effect during adolescence. Foreign clinical controlled studies have confirmed64,67 that when neonates experience pain stimuli, comforting care, such as being held in the arms of their mother or father, can effectively relieve their pain, improve physiological indicators and is beneficial for their healthy development.
Gao et al68 noted in their study that, compared with conventional incubator care, kangaroo mother care can alleviate the irritable state of preterm infants, reduce the fluctuation range of heart rate and oxygen saturation and is conducive to maintaining the stability of preterm infants’ vital signs. A study has found that performing kangaroo mother care twice a day for 1 hour each time during the hospitalization of neonates can reduce the pain experienced by neonates during procedural stimuli, shorten crying time and improve their neurobehavioral abilities.69 Although studies have shown that kangaroo mother care is an effective method for pain relief, issues such as the optimal duration, frequency, long-term effects and the gestational age of neonates in relation to kangaroo mother care remain controversial.
Non-pharmacologic pain interventions for neonates, including sweet-tasting solutions (sucrose and glucose) that reduce heart rate changes, crying time and pain scores; Kangaroo Care, which stabilizes physiological parameters, improves behavioral states and lowers cortisol levels; Nonnutritive Sucking that modulates physiological and behavioral responses; formula, breast milk and breastfeeding with comparable pain - relieving effects to sucrose (Table 2).
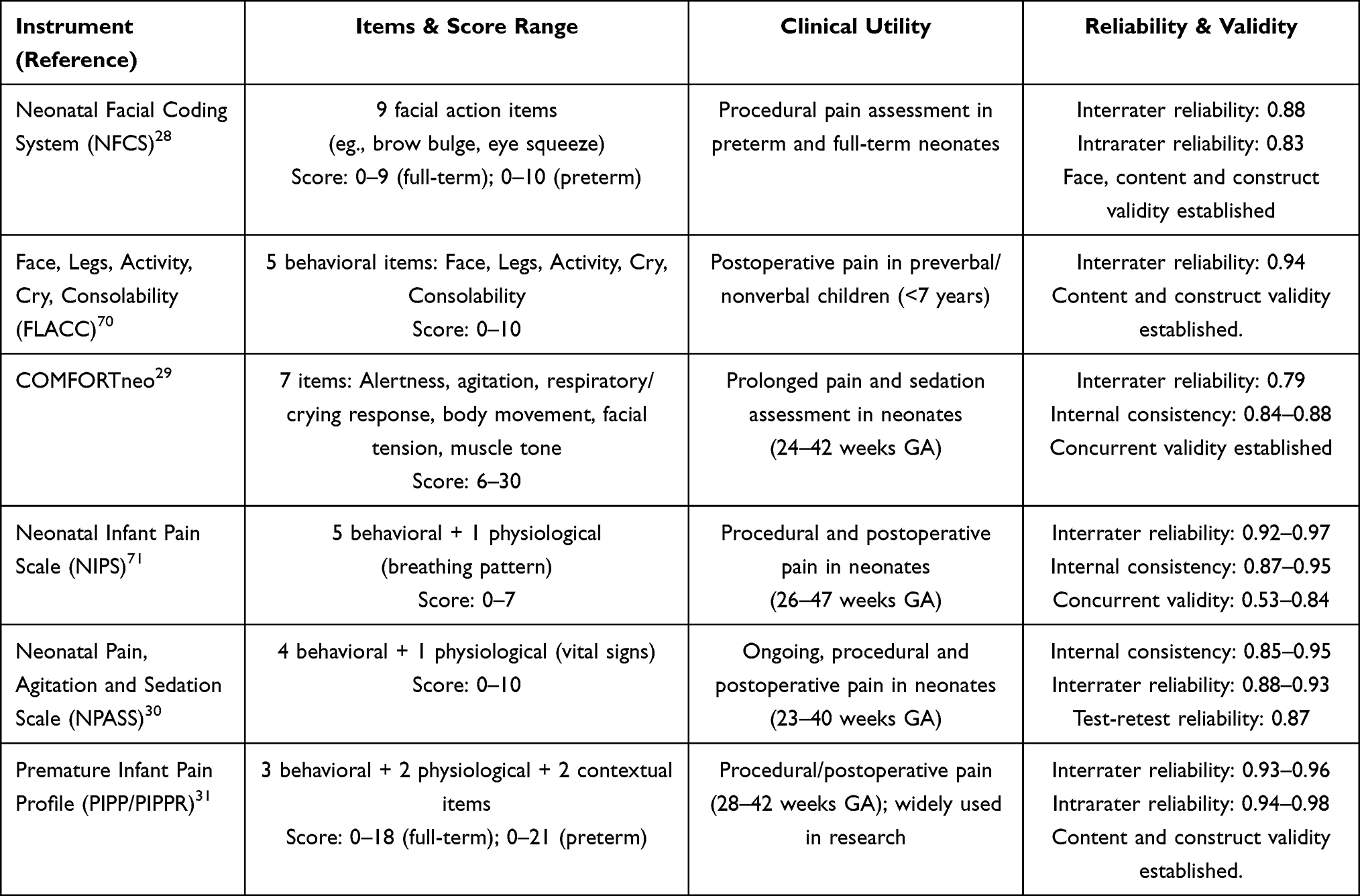 |
Table 2 Summary of Non-Pharmacologic Interventions for Neonatal Pain |
Comparative Overview of Non-Pharmaceutical Interventions
To provide a clearer synthesis of the diverse non-pharmaceutical interventions (NPIs) evaluated in this review, a comparative table was developed summarizing their efficacy, safety and clinical feasibility. These interventions function through distinct neurobiological pathways—such as orotactile stimulation, endogenous opioid activation, vagal modulation and multisensory engagement—and vary in their impact on physiological stability and behavioural pain responses. Given the differences across study populations and procedural contexts, this table offers a structured comparison of the major NPIs and the strength of supporting evidence. Table 3 provides an integrated overview of these intervention categories to facilitate clinical decision-making and highlight their relative strengths and limitations. Although most interventions demonstrate consistent analgesic effects, several modalities show variability across studies. For example, research on maternal voice has produced mixed results, with some trials reporting meaningful reductions in behavioural distress, while others observe minimal benefit. These inconsistencies may reflect differences in sound intensity, timing, maternal proximity, or infant maturity. Highlighting such conflicting findings reinforces the need for standardised methodologies and helps contextualise the relative strengths of the interventions summarised in Table 3.
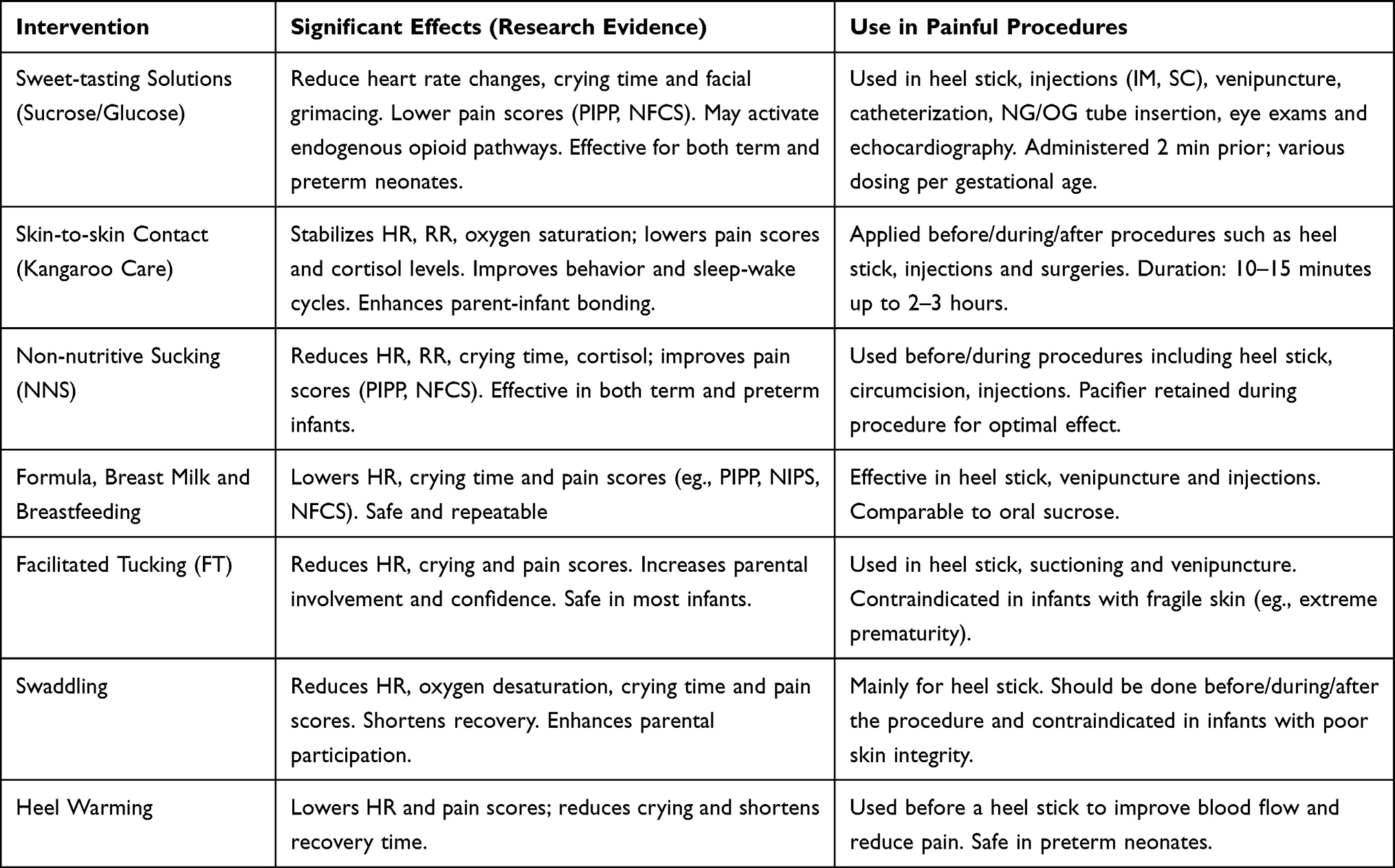 |
Table 3 Non-Pharmacologic Pain Interventions and Major Effects |
Challenges and Limitations of Non-Pharmaceutical Intervention Measures
Heterogeneity in Research Design
Current studies on non-pharmaceutical pain interventions in neonates exhibit substantial heterogeneity in intervention protocols, study populations and outcome measures, severely complicating evidence synthesis and clinical translation. Intervention protocols vary widely in terms of timing, dosage and frequency.72 For example, white noise interventions range from 45 to 65 dB in volume and from 1-minute pre-procedure exposure to continuous post-procedure playback.73 At the same time, oral sweet solutions differ in concentration (10%-30%) and single-dose volume (0.2 mL/kg to 2 mL), making it impossible to identify optimal parameters.74 Such disparities hinder the establishment of standardised guidelines, as results from one study are rarely comparable to those of another.
The diversity of study populations adds further complexity: preterm and term infants respond differently to tactile interventions, such as swaddling, with preterm neonates showing weaker analgesic effects due to immature motor control. However, research focusing on critically ill infants or those with congenital conditions remains scarce, limiting generalizability to real-world clinical scenarios.75 Outcome measures are also inconsistently reported, with some studies relying solely on behavioral scales (eg., NIPS, PIPP-R). In contrast, others prioritise physiological parameters (such as heart rate and oxygen saturation), while only a fraction incorporates neurobiological markers (including cortisol levels and cerebral oxygen saturation). A 2021 review of kangaroo care, for instance, found that just 30% of studies reported both pain scores and physiological stability data, creating a fragmented evidence base that undermines the scientific validity of cross-study comparisons.76
Inconsistencies in Research Findings
The efficacy of NPIs in neonatal pain management often yields conflicting results due to sample size limitations, heterogeneous study environments and individual neonatal variability. Most studies are underpowered, with 70% of white noise research enrolling fewer than 100 infants, which may mask actual effects or inflate statistical noise.77 For instance, a small trial with 50 participants failed to detect the impact of 50 dB white noise on regional cerebral oxygen saturation. In contrast, larger subsequent studies demonstrated its ability to stabilise physiological parameters in preterm infants.78
Study environment disparities further contribute to inconsistency, as baseline NICU noise levels (40–70 dB), nursing practice variations (eg., clustered vs. fragmented procedures) and differing conditions can modulate intervention outcomes. Kangaroo care, for example, reduces pain scores by 30% in quiet NICUs but shows diminished efficacy in noisier settings, illustrating how environmental context influences results.79 Individual differences in gestational age, neurological maturity and genetics also play key roles. Preterm infants respond less to oral sucrose due to immature taste receptors, while term infants exhibit greater sensitivity. Genetic variations in pain thresholds mean that some neonates experience significantly smaller reductions in crying than the average, even with identical exposure to white noise.
These factors create wide-ranging outcomes—for example, the reported pain score reductions from combining non-nutritive sucking with oral glucose vary by 15%–40% across studies, reflecting the complex interplay between individual and environmental factors. Such inconsistencies hinder clinical translation and highlight the need for methodologically robust research. Future studies should employ multicenter, large-sample designs to control for environmental variables and conduct stratified analyses by neonatal characteristics (such as gestational age and health status), enabling the accurate determination of intervention efficacy and the identification of applicable populations to advance evidence-based practice.
Future Research Directions
Optimisation of Intervention Protocols
The significant heterogeneity and inconsistent findings in current non-pharmaceutical intervention research necessitate large-scale, multicenter randomised controlled trials (RCTs) to strengthen the quality of the evidence. These studies should enrol diverse populations, including preterm and term infants, as well as healthy and critically ill neonates, with sample sizes exceeding 500 to ensure generalizable results across clinical contexts. For intervention parameter optimization, dose-gradient designs are essential: for example, in white noise studies, comparing 45 dB, 50 dB and 55 dB volumes initiated 1, 3 and 5 minutes before procedures and sustained for 2 minutes afterward, while measuring differences in pain scores, physiological markers (heart rate, oxygen saturation) and behavioral responses (crying duration, facial grimacing) to establish “dose-response” relationships. Similarly, oral glucose interventions require a systematic exploration of 20%, 25% and 30% concentrations at doses of 0.2 mL/kg, 0.5 mL/kg and 1 mL/kg, with a particular focus on gastrointestinal tolerance in preterm infants to define safe and effective dosage boundaries.
Cost-benefit analysis is equally critical for clinical translation, requiring the quantification of resource inputs—such as white noise device procurement, nursing time for kangaroo care, or materials for positional support—and outcomes, including reduced stress-related complications (eg., stress ulcers), shortened NICU stays and lower parental anxiety scores. For instance, decision-tree modelling might demonstrate that although kangaroo care adds 15 minutes of nursing time per procedure, it reduces pain-induced oxygen desaturation by 20% in preterm infants, potentially decreasing ventilator use and saving approximately 3000 yuan per case in cumulative medical costs. Such analyses will guide healthcare systems in prioritising high-value interventions that balance efficacy, feasibility and economic sustainability, bridging the gap between research evidence and bedside implementation in neonatal pain management.
In-Depth Mechanistic Insights into Interventions
Unravelling the central nervous system mechanisms of NPIs through neuroimaging and molecular biology represents a critical frontier in understanding these interventions. Near-infrared spectroscopy (NIRS) enables real-time monitoring of oxyhemoglobin changes in pain-related brain regions, such as the prefrontal cortex and insula, revealing whether interventions like white noise reduce pain perception by enhancing prefrontal blood flow (attenuating cognitive processing of pain) or dampening insular activation (blunting emotional pain responses). Functional magnetic resonance imaging (fMRI) can dynamically map how kangaroo care modulates limbic structures, such as the amygdala and hippocampus, potentially via maternal odor recognition, to activate oxytocin pathways and inhibit the hypothalamic-pituitary-adrenal (HPA) axis stress response. This provides a neurobiological basis for its calming effects. Electroencephalography (EEG) measures changes in brainwave patterns (eg., δ waves during sleep, β waves during wakefulness) to elucidate how auditory interventions, such as maternal voice, enhance pain tolerance by regulating neural oscillations associated with stress and attention.
Long-term studies on neural plasticity aim to track structural brain changes induced by early interventions, such as whether frequent kangaroo care in preterm infants promotes prefrontal cortex thickness, linked to improved later cognitive function, or if oral sucrose alters synaptic connections in the gustatory cortex, potentially shaping childhood taste preferences. By integrating animal models (eg., neonatal rat pain models) with human cohort studies, researchers can explore epigenetic mechanisms—such as DNA methylation and histone modifications-that underlie NPIs’ influence on neurodevelopmental trajectories. These investigations seek to establish causal links between early pain management and long-term neural health, providing a scientific foundation for developing “neuroprotective analgesia” strategies that not only relieve acute pain but also safeguard long-term brain development in vulnerable neonates.
Development of Individualised Intervention Systems
Constructing personalised intervention strategies based on neonatal characteristics- including gestational age, birth weight, genetic susceptibility and pain phenotype is crucial for overcoming the limitations of “one-size-fits-all” approaches. This requires first establishing a multidimensional assessment framework that integrates genetic testing (eg., identifying OPRM1 gene A118G polymorphism associated with pain sensitivity), physiological metrics (baseline heart rate variability, cortisol levels) and behavioral observations (intensity of limb movement, crying duration during pain) to classify neonates into “high-reactant” or “low-reactant” pain subgroups. For example, extremely preterm infants (<28 weeks gestation, often high-reactant) might receive a tailored protocol combining 30 minutes of kangaroo care, 0.3 mL/kg of 25% glucose and moderate limb swaddling, with intervention intensity dynamically adjusted using real-time cerebral oxygen saturation (rScO2) feedback—automatically increasing white noise volume to 55 dB if rScO2 drops by >15% to maintain neural stability.
Technological integration plays a pivotal role in realising this vision, with machine-learning-driven intelligent systems capable of analysing real-time sensor data (such as heart rate, oxygen saturation and body movement) to generate personalised intervention recommendations. These systems could autonomously suggest optimal combinations—such as non-nutritive sucking, maternal voice and curled positioning—and remotely control connected devices (eg., adjusting white noise generators in incubators or adjusting the tightness of smart swaddling) through IoT platforms. For complex procedures like endotracheal suctioning, closed-loop systems that integrate pre-procedure risk prediction (using NIRS to anticipate cerebral oxygen desaturation), real-time intervention modulation and post-procedure efficacy assessment would ensure synchronised activation of tactile, gustatory and auditory stimuli at the moment of noxious stimulation, maximising inhibition of pain signal transmission. By aligning interventions with each neonate’s unique biological and behavioral profiles, this individualised approach promises to transform neonatal pain management from empirical practice to precision care, enhancing both acute pain relief and long-term neurodevelopmental outcomes.
Conclusion
Non-pharmacological interventions (NPIs) are a cornerstone of modern neonatal pain management, providing safe and developmentally appropriate strategies to mitigate both immediate and long-term consequences of procedural pain in vulnerable infants. By engaging multisensory pathways, including auditory, oral-tactile, tactile and positional mechanisms, these interventions effectively reduce pain perception, stabilise physiological stress responses and support neurodevelopment, often showing synergistic benefits when combined. Despite their promise, clinical implementation is challenged by methodological inconsistencies, limited long-term outcome data and variability in intervention protocols. To advance NPIs from empirical use to precision strategies, specific clinical recommendations include standardising protocols for widely used interventions (such as oral sucrose/glucose dosing, kangaroo care duration and auditory stimulation) and integrating multimodal approaches tailored to gestational age and neonatal condition. Research priorities should focus on large-scale multicenter RCTs to determine optimal intervention parameters, long-term neurodevelopmental outcomes and mechanistic studies using neuroimaging and molecular tools to guide individualised care. The development of intelligent, sensor-driven systems to personalise interventions in real time could further enhance efficacy and safety. By addressing these gaps, NPIs can be optimised not only to alleviate acute procedural pain but also to safeguard neurodevelopment, ultimately promoting evidence-based, precision and neuroprotective care that improves comfort and clinical outcomes in this most vulnerable population.
Use of Artificial Intelligence
No artificial intelligence tools were used in the conduct of this study.
Data Sharing Statement
The data used to support this study are available from the corresponding author upon request.
Ethical Statement
As this study is a review article, ethical approval was not required.
Acknowledgments
The authors would like to thank the medical staff of the Departments of Neonatology and Nursing at The Second People’s Hospital of Hefei for their support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for this study.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Yamada J, Bueno M, Santos L, et al. Sucrose analgesia for heel-lance procedures in neonates. Cochrane Database Syst Rev. 2023;8(8):CD014806. doi:10.1002/14651858.CD014806
2. Queirós I, Moreira T, Pissarra R, Soares H, Guimarães H. Non-pharmacological management of neonatal pain: a systematic review. Minerva Pediatr. 2023;75(2):282–15. doi:10.23736/S2724-5276.22.06871-9
3. Fatollahzade M, Parvizi S, Kashaki M, et al. The effect of gentle human touch during endotracheal suctioning on procedural pain response in preterm infants admitted to neonatal intensive care units: a randomized controlled crossover study. J Matern Fetal Neonatal Med. 2022;35(7):1370–1376. doi:10.1080/14767058.2020.1755649
4. McLean MA, Niknafs N, Scoten OC, et al. Sensory processing and cortisol at age 4 years: procedural pain-related stress in children born very preterm. Dev Psychobiol. 2021;63(5):915–930. doi:10.1002/dev.22079
5. Hannibal KE, Bishop MD. Chronic stress, cortisol dysfunction and pain: a psychoneuroendocrine rationale for stress management in pain rehabilitation. Phys Ther. 2014;94(12):1816–1825. doi:10.2522/ptj.20130597
6. Meesters NJ, Dilles T, van Rosmalen J, et al. COMFORTneo scale: a reliable and valid instrument to measure prolonged pain in neonates? J Perinatol. 2023;43(5):595–600. doi:10.1038/s41372-023-01628-1
7. Gianni ML, Bettinelli ME, Manfra P, et al. Breastfeeding difficulties and risk for early breastfeeding cessation. Nutrients. 2019;11(10):2266. doi:10.3390/nu11102266
8. Min C, Ling R, Chen M, et al. Enriched environment rescues neonatal pain induced cognitive deficits and the impaired hippocampal synaptic plasticity later in life. Dev Neurobiol. 2022;82(6):545–561. doi:10.1002/dneu.22898
9. Shah PS, Torgalkar R, Shah VS. Breastfeeding or breast milk for procedural pain in neonates. Cochrane Database Syst Rev. 2023;8(8):CD004950. doi:10.1002/14651858.CD004950.pub4
10. Baldo BA, Rose MA. Mechanisms of opioid-induced respiratory depression. Arch Toxicol. 2022;96(8):2247–2260. doi:10.1007/s00204-022-03300-7
11. Pavlyshyn H, Sarapuk I. Skin-to-skin contact-an effective intervention on pain and stress reduction in preterm infants. Front Pediatr. 2023;11:1148946. doi:10.3389/fped.2023.1148946
12. Akbari N, Mutlu B, Nadali J. Effect of non-nutritive sucking during heel-stick procedure in pain management of term infants in the neonatal intensive care unit: a systematic review and meta-analysis. Curr Pediatr Rev. 2022;19(1):90–98. doi:10.2174/1573396318666220410225908
13. Olsson E, Pettersson M, Eriksson M, et al. Oral sweet solution to prevent pain during neonatal Hip examination: a randomised controlled trial. Acta Paediatr. 2019;108(4):626–629. doi:10.1111/apa.14588
14. Stevens BJ, Gibbins S, Yamada J, et al. The premature infant pain profile-revised (PIPP-R): initial validation and feasibility. Clin J Pain. 2014;30(3):238–243. doi:10.1097/AJP.0b013e3182906aed
15. Lagercrantz H. The emergence of consciousness: science and ethics. Semin Fetal Neonatal Med. 2014;19(5):300–305. doi:10.1016/j.siny.2014.08.003
16. Olsson E, Ahl H, Bengtsson K, et al. The use and reporting of neonatal pain scales: a systematic review of randomized trials. Pain. 2021;162(2):353–360. doi:10.1097/j.pain.0000000000002046
17. Timmerman BM, Mooney-Leber SM, Brummelte S. The effects of neonatal procedural pain and maternal isolation on hippocampal cell proliferation and reelin concentration in neonatal and adult male and female rats. Dev Psychobiol. 2021;63(8):e22212. doi:10.1002/dev.22212
18. Hassanein EHM, Althagafy HS, Baraka MA, et al. Pharmacological update of mirtazapine: a narrative literature review. Naunyn Schmiedebergs Arch Pharmacol. 2024;397(5):2603–2619. doi:10.1007/s00210-023-02818-6
19. Liu J, Fang S, Wang Y, et al. The effectiveness of massage interventions on procedural pain in neonates: a systematic review and meta-analysis. Medicine. 2022;101(41):e30939. doi:10.1097/MD.0000000000030939
20. Beltrán-Campos V, Silva-Vera M, García-Campos ML, et al. Effects of morphine on brain plasticity. Neurologia. 2015;30(3):176–180. doi:10.1016/j.nrl.2014.08.004
21. Geerling I, Roberts RM, Sved Williams A. Impact of infant crying on mothers with a diagnosis of borderline personality disorder: a qualitative study. Infant Ment Health J. 2019;40(3):405–421. doi:10.1002/imhj.21776
22. Mooney-Leber SM, Brummelte S. Neonatal pain and reduced maternal care alter adult behavior and hypothalamic-pituitary-adrenal axis reactivity in a sex-specific manner. Dev Psychobiol. 2020;62(5):631–643. doi:10.1002/dev.21941
23. Sevivas C, Ibáñez R, Fontalvo M, et al. Pain and heart rate variability in neonates receiving dexmedetomidine. J Perinatol. 2024;44(11):1669–1674. doi:10.1038/s41372-024-02053-8
24. Eriksson M, Campbell-Yeo M. Assessment of pain in newborn infants. Semin Fetal Neonatal Med. 2019;24(4):101003. doi:10.1016/j.siny.2019.04.003
25. Pirlotte S, Beeckman K, Ooms I, et al. Non-pharmacological interventions for the prevention of pain during endotracheal suctioning in ventilated neonates. Cochrane Database Syst Rev. 2024;1(1):CD013353. doi:10.1002/14651858.CD013353.pub2
26. Hartl L, Simbrunner B, Jachs M, et al. An impaired pituitary-adrenal signalling axis in stable cirrhosis is linked to worse prognosis. JHEP Rep. 2023;5(8):100789. doi:10.1016/j.jhepr.2023.100789
27. Kawashima N. Kambakutaisoto treatment for children with night crying and arousal parasomnias developed during prolonged hospitalization for hematological and oncological diseases. J Child Neurol. 2021;36(7):568–574. doi:10.1177/0883073820984062
28. Kappesser J, de Laffolie J, Faas D, et al. Comparison of two neonatal pain assessment tools (children and infant’s postoperative pain scale and the neonatal facial coding system-revised) and their relations to clinicians’ intuitive pain estimates. Eur J Pain. 2019;23(4):708–718. doi:10.1002/ejp.1338
29. Campbell-Yeo M, Carrier L, Benoit B, et al. Evaluation of the Premature Infant Pain Profile-Revised (PIPP-R) e-Learning module: immediate and sustained competency. Adv Neonatal Care. 2022;22(3):246–252. doi:10.1097/ANC.0000000000000922
30. Benbrook K, Manworren RCB, Zuravel R, et al. Agreement of the Neonatal Pain, Agitation and Sedation Scale (N-PASS) with NICU nurses’ assessments. Adv Neonatal Care. 2023;23(2):173–181. doi:10.1097/ANC.0000000000000968
31. Weng Y, Zhang J, Chen Z. Effect of non-pharmacological interventions on pain in preterm infants in the neonatal intensive care unit: a network meta-analysis of randomized controlled trials. BMC Pediatr. 2024;24:1–9. doi:10.1186/s12887-023-04488-y
32. Kadiroğlu T, Yalçın R, Güven M. Effect of Yakson touch and white noise on pain in neonatal heel blood collection: a randomized controlled study. Altern Ther Health Med. 2024;30(7):28–33.
33. Liu X, Iwanaga K, Shimomura Y, et al. Comparison of stress responses between mental tasks and white noise exposure. J Physiol Anthropol. 2007;26(2):165–171. doi:10.2114/jpa2.26.165
34. Garcia-Argibay M, Santed MA, Reales JM. Efficacy of binaural auditory beats in cognition, anxiety and pain perception: a meta-analysis. Psychol Res. 2019;83(2):357–372. doi:10.1007/s00426-018-1066-8
35. Akca K, Aytekin A. Effect of soothing noise on sucking success of newborns. Breastfeed Med. 2014;9(10):538–542. doi:10.1089/bfm.2014.0131
36. Liao J, Liu G, Xie N, et al. Mothers’ voices and white noise on premature infants’ physiological reactions in a neonatal intensive care unit: a multi-arm randomized controlled trial. Int J Nurs Stud. 2021;119:103934. doi:10.1016/j.ijnurstu.2021.103934
37. Sezici E, Yigit D. Comparison between swinging and playing of white noise among colicky babies: a paired randomised controlled trial. J Clin Nurs. 2018;27(3–4):593–600. doi:10.1111/jocn.13928
38. Bucsea O, Pillai Riddell R. Non-pharmacological pain management in the neonatal intensive care unit: managing neonatal pain without drugs. Semin Fetal Neonatal Med. 2019;24(4):101017. doi:10.1016/j.siny.2019.05.009
39. Buglione A, Saccone G, Mas M, et al. Effect of music on labor and delivery in nulliparous singleton pregnancies: a randomized clinical trial. Arch Gynecol Obstet. 2020;301(3):693–698. doi:10.1007/s00404-020-05475-9
40. Ou Y, Chen L, Zhu X, et al. The effect of music on pain management in preterm infants during daily painful procedures: a systematic review and meta-analysis. Front Pediatr. 2024;12:1351401. doi:10.3389/fped.2024.1351401
41. Gibbins S, Stevens B, McGrath PJ, et al. Comparison of pain responses in infants of different gestational ages. Neonatology. 2008;93(1):10–18. doi:10.1159/000105520
42. Provenzi L, Broso S, Montirosso R. Do mothers sound good? A systematic review of the effects of maternal voice exposure on preterm infants’ development. Neurosci Biobehav Rev. 2018;88:42–50. doi:10.1016/j.neubiorev.2018.03.009
43. Grunau RE, Holsti L, Peters JW. Long-term consequences of pain in human neonates. Semin Fetal Neonatal Med. 2006;11(4):268–275. doi:10.1016/j.siny.2006.02.007
44. Lee JH. The effects of music on pain: a meta-analysis. J Music Ther. 2016;53(4):430–477. doi:10.1093/jmt/thw012
45. de Witte M, Pinho ADS, Stams GJ, et al. Music therapy for stress reduction: a systematic review and meta-analysis. Health Psychol Rev. 2022;16(1):134–159. doi:10.1080/17437199.2020.1846580
46. Kurdahi Badr L, Demerjian T, Daaboul T, et al. Preterm infants exhibited less pain during a heel stick when they were played the same music their mothers listened to during pregnancy. Acta Paediatr. 2017;106(3):438–445. doi:10.1111/apa.13666
47. Butt ML, Kisilevsky BS. Music modulates behaviour of premature infants following heel lance. Can J Nurs Res. 2000;31(4):17–39.
48. Johnston C, Campbell-Yeo M, Disher T, et al. Skin-to-skin care for procedural pain in neonates. Cochrane Database Syst Rev. 2017;2(2):CD008435. doi:10.1002/14651858.CD008435.pub3
49. Pillai Riddell RR, Bucsea O, Shiff I, et al. Non-pharmacological management of infant and young child procedural pain. Cochrane Database Syst Rev. 2023;6(6):CD006275. doi:10.1002/14651858.CD006275.pub4
50. de Kort AR, Joosten EA, Patijn J, et al. Selective targeting of Serotonin 5-HT1a and 5-HT3 Receptors attenuates acute and long-term hypersensitivity associated with neonatal procedural pain. Front Pain Res. 2022;3:872587. doi:10.3389/fpain.2022.872587
51. Zhao S, Jiang H, Miao Y, et al. Effects of implementing non-nutritive sucking on oral feeding progression and outcomes in preterm infants: a systematic review and meta-analysis. PLoS One. 2024;19(4):e0302267. doi:10.1371/journal.pone.0302267
52. Lima AG, Santos VS, Nunes MS, et al. Glucose solution is more effective in relieving pain in neonates than non-nutritive sucking: a randomized clinical trial. Eur J Pain. 2017;21(1):159–165. doi:10.1002/ejp.912
53. Kjeldsen CP, Emery L, Simsic J, et al. Contingent Mother’s Voice Intervention Targeting Feeding in Hospitalized Infants with Critical Congenital Heart Defects. Children. 2023;10(10):1642. doi:10.3390/children10101642
54. Alves Cde O, Duarte ED, Azevedo VM, et al. Emprego de soluções adocicadas no alívio da dor neonatal em recém-nascido prematuro: uma revisão integrativa [Use of sweet solutions for neonatal pain relief in premature newborns: an integrative review]. Rev Gaucha Enferm. 2011;32(4):788–796. doi:10.1590/S1983-14472011000400021
55. Bembich S, Cont G, Causin E, et al. Infant analgesia with a combination of breast milk, glucose, or maternal holding. Pediatrics. 2018;142(3):e20173416. doi:10.1542/peds.2017-3416
56. Small C, Laycock H. Acute postoperative pain management. Br J Surg. 2020;107(2):e70–e80. doi:10.1002/bjs.11477
57. Squillaro A, Mahdi EM, Tran N, et al. Managing procedural pain in the neonate using an opioid-sparing approach. Clin Ther. 2019;41(9):1701–1713. doi:10.1016/j.clinthera.2019.07.014
58. Harrison D, Larocque C, Bueno M, et al. Sweet solutions to reduce procedural pain in neonates: a meta-analysis. Pediatrics. 2017;139(1):e20160955. doi:10.1542/peds.2016-0955
59. Tanyeri-Bayraktar B, Bayraktar S, Hepokur M, et al. Comparison of two different doses of sucrose in pain relief. Pediatr Int. 2019;61(8):797–801. doi:10.1111/ped.13914
60. Schneider J, Duerden EG, Guo T, et al. Procedural pain and oral glucose in preterm neonates: brain development and sex-specific effects. Pain. 2018;159(3):515–525. doi:10.1097/j.pain.0000000000001123
61. Carbajal R, Chauvet X, Couderc S, et al. Randomised trial of analgesic effects of sucrose, glucose and pacifiers in term neonates. BMJ. 1999;319(7222):1393–1397. doi:10.1136/bmj.319.7222.1393
62. Bembich S, Cont G, Baldassi G, et al. Maternal holding vs oral glucose administration as nonpharmacologic analgesia in newborns: a functional neuroimaging study. JAMA Pediatr. 2015;169(3):284–285. doi:10.1001/jamapediatrics.2014.3052
63. Sen E, Manav G. Effect of Kangaroo care and oral sucrose on pain in premature infants: a randomized controlled trial. Pain Manag Nurs. 2020;21(6):556–564. doi:10.1016/j.pmn.2020.05.003
64. Roshanray A, Rayyani M, Dehghan M, et al. Comparative effect of mother’s hug and massage on neonatal pain behaviors caused by blood sampling: a randomized clinical trial. J Trop Pediatr. 2020;66(5):479–486. doi:10.1093/tropej/fmaa001
65. Mooney-Leber SM, Spielmann SS, Brummelte S. Repetitive neonatal pain and reduced maternal care alter brain neurochemistry. Dev Psychobiol. 2018;60(8):963–974. doi:10.1002/dev.21777
66. Davis SM, Burman MA. Maternal separation with neonatal pain influences later-life fear conditioning and somatosenation in male and female rats. Stress. 2021;24(5):504–513. doi:10.1080/10253890.2020.1825674
67. Shukla VV, Chaudhari AJ, Nimbalkar SM, et al. Skin-to-skin care by mother vs father for preterm neonatal pain: a randomized control trial (ENVIRON Trial). Int J Pediatr. 2021;2021:8886887. doi:10.1155/2021/8886887
68. Gao H, Xu G, Gao H, et al. Effect of repeated Kangaroo Mother Care on repeated procedural pain in preterm infants: a randomized controlled trial. Int J Nurs Stud. 2015;52(7):1157–1165. doi:10.1016/j.ijnurstu.2015.04.006
69. Qiu J, Jiang YF, Li F, et al. Effect of combined music and touch intervention on pain response and β-endorphin and cortisol concentrations in late preterm infants. BMC Pediatr. 2017;17(1):38. doi:10.1186/s12887-016-0755-y
70. Matsuishi Y, Hoshino H, Shimojo N, et al. Verifying the validity and reliability of the Japanese version of the Face, Legs, Activity, Cry, Consolability (FLACC) behavioral scale. PLoS One. 2018;13(3):e0194094. doi:10.1371/journal.pone.0194094
71. Kanbur BN, Mutlu B, Salihoğlu Ö. Validity and reliability of the Neonatal Infant Acute Pain Assessment Scale (NIAPAS) in Turkish: prospective study. Sao Paulo Med J. 2021;139(4):305–311. doi:10.1590/1516-3180.2020.0721.r1.23122020
72. Nanji JA, Carvalho B. Pain management during labor and vaginal birth. Best Pract Res Clin Obstet Gynaecol. 2020;67:100–112. doi:10.1016/j.bpobgyn.2020.03.002
73. Zhang Q, Huo Q, Chen P, et al. Effects of white noise on preterm infants in the neonatal intensive care unit: a meta-analysis of randomised controlled trials. Nurs Open. 2024;11(1):e2094. doi:10.1002/nop2.2094
74. Harrison D, Stevens B, Bueno M, et al. Efficacy of sweet solutions for analgesia in infants between 1 and 12 months of age: a systematic review. Arch Dis Child. 2010;95(6):406–413. doi:10.1136/adc.2009.174227
75. Brandt JS, Ananth CV. Placental abruption at near-term and term gestations: pathophysiology, epidemiology, diagnosis and management. Am J Obstet Gynecol. 2023;228(5S):S1313–S1329. doi:10.1016/j.ajog.2022.06.059
76. Narciso LM, Beleza LO, Imoto AM. The effectiveness of Kangaroo Mother Care in hospitalization period of preterm and low birth weight infants: systematic review and meta-analysis. J Pediatr. 2022;98(2):117–125. doi:10.1016/j.jped.2021.06.004
77. Cetinkaya S, Yavas Celik M, Ozdemir S. Effect of white noise on alleviating the pain of new-born during invasive procedures. J Matern Fetal Neonatal Med. 2022;35(8):1426–1432. doi:10.1080/14767058.2020.1755652
78. Baijot S, Slama H, Söderlund G, et al. Neuropsychological and neurophysiological benefits from white noise in children with and without ADHD. Behav Brain Funct. 2016;12(1):1–11. doi:10.1186/s12993-016-0095-y
79. Kirbaş ZÖ, OdabaşI Aktaş E, Bayraktar B, et al. Effect of kangaroo mother care and white noise on physiological-stress parameters in heel lancing: randomized controlled study. BMC Pediatr. 2024;24(1):568. doi:10.1186/s12887-024-05033-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Awareness and Predictors of the Use of Bioinformatics in Genome Research in Saudi Arabia
Alomair L, Abolfotouh MA
International Journal of General Medicine 2023, 16:3413-3425
Published Date: 11 August 2023