Back to Journals » Journal of Pain Research » Volume 16
A Bibliometric and Scientific Knowledge Map Study of Migraine Treatment from 2013 to 2022
Authors Wang T, Li Y, Miao S, Yang C, Xie W, Yuan H, Bai W, Xiao H, Yu S ![]()
Received 12 March 2023
Accepted for publication 5 September 2023
Published 15 September 2023 Volume 2023:16 Pages 3169—3184
DOI https://doi.org/10.2147/JPR.S412158
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Alexandre F DaSilva
Tao Wang,1,2,* Yanan Li,2,* Shuai Miao,1,2 Chunxiao Yang,3 Wei Xie,1,2 Huijuan Yuan,3 Wenhao Bai,1,2 Han Xiao,1,2 Shengyuan Yu1,2
1Department of Neurology, the First Medical Centre, Chinese PLA General Hospital, Beijing, People’s Republic of China; 2Medical School of Chinese PLA, Beijing, People’s Republic of China; 3College of Medicine, Nankai University, Tianjin, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Shengyuan Yu, Email [email protected]
Background: Migraine treatment research has made much great progress over the past decade. However, there have been few bibliometric studies conducted so far. In this study, bibliometric analysis was used to explore the current status and future trends of migraine treatment research.
Methods: Migraine treatment-related articles were retrieved from the Web of Science Core Collection on December 7, 2022. Quantitative variables were analyzed by the R-tool bibliometrix and Excel 2020. VOS viewer and CiteSpace software were used to visualize citation, co-authorship, co-occurrence, and co-citation analysis of countries/regions, organizations, authors, references, and keywords.
Results: A total of 3294 articles were included with the global publication output showing a slow upward trend. The United States was the most productive country with 1116 papers and gained the most citations. Albert Einstein College of Medicine was the most active institution with 176 papers. Headache published the most articles in this domain, while Cephalalgia was the most commonly co-cited journal. Lipton, RB published the most articles and had the most citations. Tepper S, 2017, Lancet neurology and Silberstein S, 2004, Cephalalgia were defined as classic articles. The current research mainly focuses on CGRP-related therapeutics, such as fremanezumab, erenumab and ubrogepant.
Conclusion: Based on the analysis of bibliometric data on migraine treatment over the past decade, the trends and the knowledge graph of the country, organization, author, reference, and the keyword were identified, providing accurate and quick positioning of the critical information in the domain.
Keywords: migraine, treatment, bibliometric analysis, research trends, hot spots
Introduction
Migraine is a disabling neurological disorder caused by both genetic and environmental factors, which affects more than 1 billion people world-wide.1,2 The 1-year prevalence is about 15% worldwide and peaks in those aged 35–39 years.3 According to the Global Burden of Disease Study, migraine is ranked as the leading cause of disability worldwide in people younger than 50 years (particularly in women) and a major cause of tremendous losses to the global economy.3,4
The therapeutics of migraine include acute drug therapy, preventive drug therapy and non-pharmacological therapies. In the acute phase, nonopioid analgesics (such as nonsteroidal anti-inflammatory drugs [NSAIDs] and paracetamol) are primarily used, and if these drugs are not sufficient, triptans.5,6 Although the above-mentioned drugs have achieved positive effects, long-term use has more side effects. Such as inadequate drug treatment may cause medication-overuse headache or chronic migraine, and gastrointestinal reactions, bleeding risks, liver and kidney damage may be caused by long-term use of NSAIDs.7–10 And patients with severe migraine cannot control their disease in most cases and challenges with undertreatment remain.11 Therefore, the search for new therapeutics to treat migraine has never stopped. Especially over the past 5 years, a great deal of progress has been made in the treatment of migraine with the advance in the understanding of its pathophysiology, such as new therapeutics of migraine prevention including calcitonin gene-related peptide (CGRP) receptor antagonists and anti-pituitary adenylate cyclase-activating polypeptide (PACAP) monoclonal antibodies.11–15 And some other therapeutics have been also proved effective in treating migraine, such as acupuncture,16 transcranial magnetic stimulation (TMS),17 transcutaneous occipital nerve stimulation,18 Chinese medicine-tianshu capsule19 and toutongning capsule.20 However, there have been few bibliometric studies conducted to summarize the current research status so far.
As an effective and scientific method, bibliometric analysis, combining mathematical and statistical methods with data visualization, is used to analyze the overall knowledge structure and development trends in a specific research field.21 Researchers can create science mapping conveniently relying on visualization software and websites such as VOSviewer and CiteSpace.22,23 Our study aimed to conduct a comprehensive bibliometric analysis of migraine treatment research articles from 2013 to 2022, with concentration on publication outputs, citations, countries/regions, journals, authors, references, and keywords. The results may provide hotspots, new trends, and potential topics for future migraine treatment-related research works.
Methods
Data Source and Search Strategy
A systematic search of migraine treatment-related literatures from the Web of Science Core Collection (WoSCC) database was conducted using the followed retrieval strategy (Box 1). The search was completed on 7 December 2022 and indices included the Science Citation Index Expanded (SCI-Expanded). Two researchers reviewed and screened the title and abstract, and any discrepancies were resolved via consultation with a third researcher. A total of 5243 kinds of literature were retrieved, 3294 records were used for bibliometric analysis after Citespace deleted duplicates and manual verification (Figure 1).
 |
Box 1 Query Formulation |
 |
Figure 1 Flowchart for literature selection. |
Data Visualization and Analysis
An R-tool bibliometrix24 and Excel 2020 were used for preliminary bibliometric analysis and management of the data. Cooperation map of countries was analyzed by an online bibliometric analysis tool (https://bibliometric.com). Citation analysis, co-authorship analysis, and keyword co-occurrence analysis were performed by VOSviewer 1.6.18 in this study. The nodes in the VOSviewer maps represent elements such as countries, journals, organizations, authors, and keywords, and lines stand for co-authorship, co-occurrence, or citation relationships.22 VOSviewer parameters are set as follows: create a map based on bibliographic data (WOS files), type of analysis (co-authorship, co-occurrence, citation), unit of analysis (authors, organizations, countries, sources, all keywords), chose threshold (filter according to the output results, countries/regions: 500 citations; organizations: 20 articles; journals: 200 citations; authors: 20 articles; all keywords: 50 co-occurrences). CiteSpace 6.1 R321 was used to analyze co-citation relationship, journal dual-map. The setting of the CiteSpace was as follows: Time slicing from 2013-JAN to 2022-NOV, Years per slice 1, Term source including title, abstract, author keywords, and keywords plus, Node type select from author, country, journal, institution, and keyword, Selection criteria: top 20–50, Pruning: pathfinder plus pruning sliced networks.
Results
General Characteristics of the Retrieved Documents
From 2013-01-01 to 2022-11-30, a total of 3294 English articles on migraine treatment have been published. As shown in Figure 2A, global publication output shows a slow upward trend, with the greatest growth occurring in 2019, up by 78 papers than in 2018, and the majority of articles were published in 2021 (n = 496). With an average of 16.86 times per article, the mean total citation per year shows a slow increase in 2013–2018, while a decline trend in 2019–2021 (Figure 2B). Besides, publication growth in this field can be divided into two periods, a fluctuate period in 2013–2016 and a slow growth period in 2017–2021. The average number of publications in 2013–2016 is 250.5, and in 2017–2021 is 399.2. However, the growth rate calculated by the formula (growth rate = (present/past)1/n-1, n is the number of years)25 is 0.20% in 2013–2016, and 11.03% in 2017–2021.
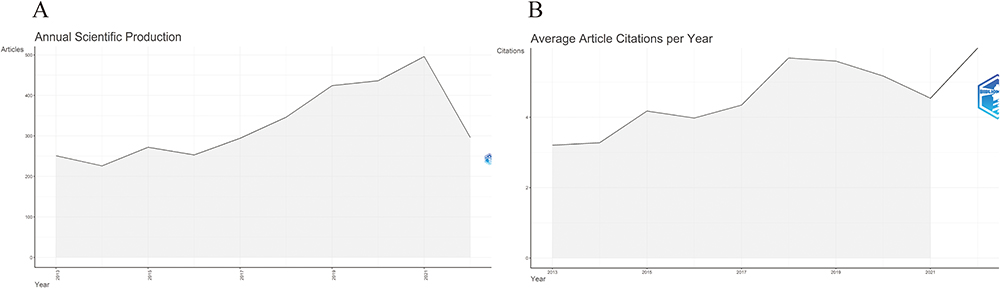 |
Figure 2 (A) The trend of publication outputs and (B) mean citations per year in the past 10 years. |
Analysis of Countries/Regions and Organizations
Researchers from 89 countries/regions and 3897 organizations have explored migraine treatment research during the past 10 years. As can been seen from Table 1, the United States was the most productive country with 1116 papers, next to Italy with 349 papers and China with 288 papers. There were 255 multiple-country articles in the United States, 81 in Italy, while only 38 in China, indicating that more international cooperation is needed in China. According to the total citations, The United States remains on top with 26,403 citations, while Italy is second with 5156 citations, and Germany is third. Among the top 10 institutions, Albert Einstein College of Medicine ranked the top with 176 papers, followed by Mayo Clinic with 143 papers and University of Copenhagen with 131 papers. Figure 3A shows the geographical distribution of global articles, from which can be seen that the most publications were from North America, Europe, and Asia.
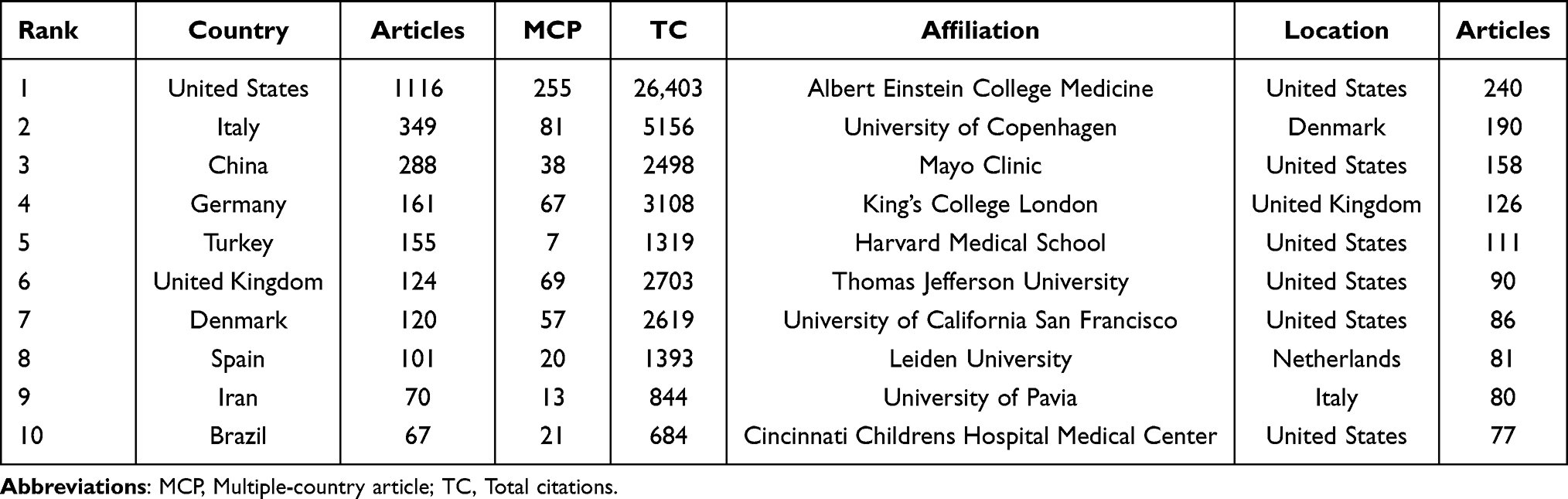 |
Table 1 The Top 10 Countries/Regions and Organizations Contributed to Publications About Migraine Treatment |
 |
Figure 3 (A) Geographical distribution of global articles of migraine treatment. The darker the national color block on the map, the more migraine treatment-related articles are published. (B) The collaboration of countries. Each country is represented by a color block, and larger blocks indicate a higher number of publications. The line between the blocks represents the cooperation between countries. (C) Citation relationships between countries. The United States, Italy and China are the major contributors to migraine treatment. |
We also analyzed the collaboration and co-citation relationship among countries or organizations. As shown in Figure 3B, the United States is located in the center of collaboration and collaborates with the United Kingdom and Germany closely. A map with 25 nodes with the minimum citation of 500 were created to reflect the citation relationships among countries using the VOSviewer (Figure 3C). The largest node in Figure 3C represents the United States, suggesting that researchers from the United States published the most articles on migraine treatment. Using “organizations” as node settings, the co-authorship analysis revealed that institutions collaborate closely, such as, Albert Einstein College of Medicine collaborated closely with Mayo Clinic, Montefiore Headache Center, etc., and University Copenhagen shows close cooperation with Mayo Clinic, Thomas Jefferson University, Amgen Inc, etc. (Supplementary Figure 1A). With 57 nodes and 1407 links of organizations, a network map was created to present the citation relationship (Supplementary Figure 1B). In terms of TLS, the top three organizations were: Albert Einstein college medicine (TLS = 5257), Mayo clinic (TLS = 4637) and Kings College London (TLS = 3509).
Analysis of Journals
In the past 10 years, therapeutics for migraine-related articles have been published in 619 journals, with Lancet (IF2021 = 202.731, JCR 2021 = Q1), a high-level medicine, general and internal journal, being the most influential journal among them. The top 10 journals ranked by number of publications are summarized in Table 2, from which can be concluded that Headache (IF2021 = 5.311, JCR 2021 = Q2) published most relevant publications with 486 articles, accounting for 14.84% of all therapeutics for migraine-related manuscripts, followed by Cephalalgia (IF2021 = 6.075, JCR 2021 = Q2) and Journal of headache and pain (IF2021 = 8.588, JCR 2021 = Q1). Figure 4A shows the dynamics of the number of articles in the top 5 journals during the past 10 years.
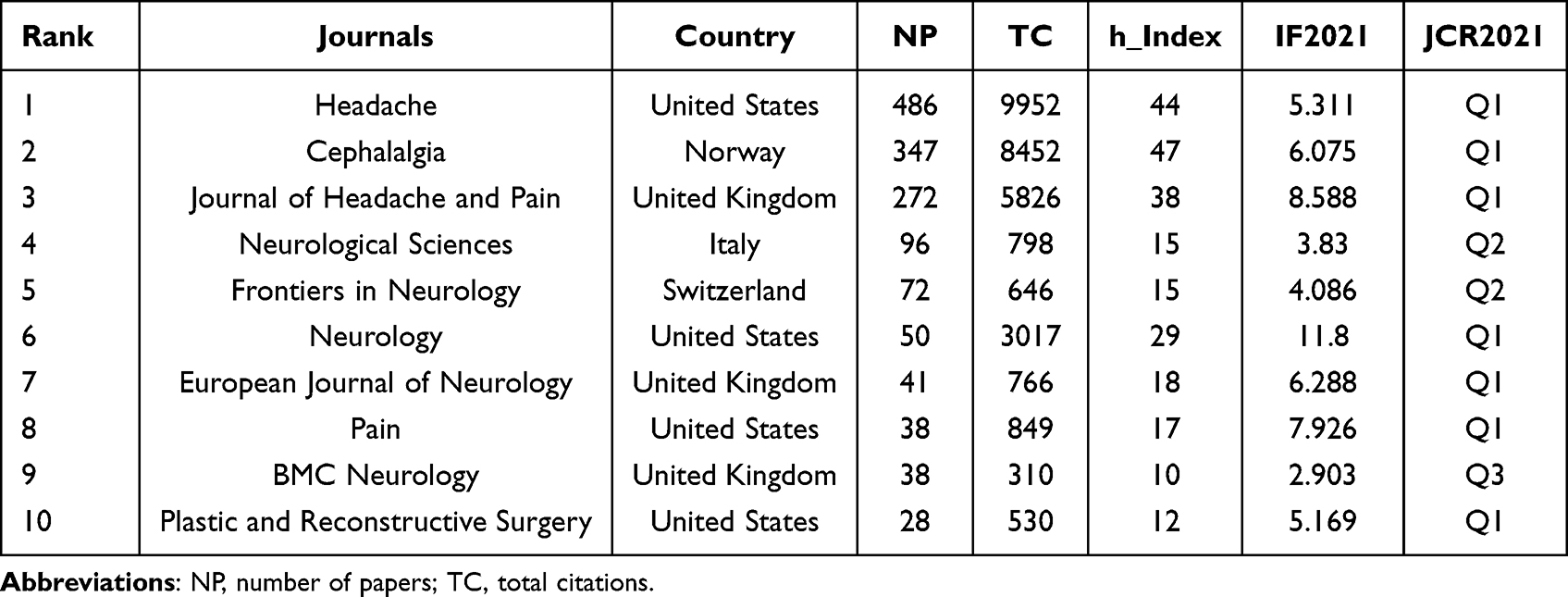 |
Table 2 The Top 10 Productive Journals Related to Migraine Treatment |
 |
Figure 4 (A) Articles dynamics of the top 5 journals. The number of articles published in the 5 journals in the figure is increasing year by year. (B) Co-Citation relationships between journals. As the largest node in the graph, Cephalalgia has the most co-citations and TLS. |
Figure 4B shows the co-citation relationship between journals, of which 67 journals gaining more than 200 citations were included in the VOSviewer map. And in terms of TLS, the top five journals were Cephalalgia (TLS = 466,419), Headache (TLS = 402,255), Neurology (TLS = 187,083), Journal of headache and pain (TLS = 173,362), Pain (TLS = 88,439). As shown in Figure 5, seven citation paths from the “Citating Journals” part flow to the “Cited Journals” part, which stand for the flow of research and the intersection of domains with their annotations at the beginning and end point of the path referring to the research field of related journals. Therefore, the research flow in the field can be summarized as follows: (i). Medicine, Medical, Clinical > Molecular, Biology, Genetics (Z = 2.0972595, F = 1753); (ii). Medicine, Medical, Clinical > Health, Nursing, Medicine (Z = 2.9023547, F = 1624); (iii). Medicine, Medical, Clinical > Psychology, Education, Social (Z = 2.7422707, F = 2223); (IV). Molecular, Biology, Immunology > Molecular, Biology, Genetics (Z = 3.562557, F = 2808); (V). Neurology, Sports, Ophthalmology > Molecular, Biology, Genetics (Z = 4.9030585, F = 3764); (VI). Neurology, Sports, Ophthalmology > Health, Nursing, Medicine (Z = 3.1447071, F = 2510); (VII). Neurology, Sports, Ophthalmology > Psychology, Education, Social (Z = 4.813318, F = 3700).
 |
Figure 5 Dual-map overlay of journals produced by CiteSpace. The color bar on the left side of the figure represents the field of the citing journals, the color bar on the right side speaks for the domain of the cited journals, and the connecting line between them represents the citation relationship. |
Analysis of Authors
The top ten most cited authors in the domain are presented in Table 3. Lipton, RB, with 153 publications and 6071 citations, ranked top among all authors; second place went to Goadsby PJ from Leiden University with 105 publications and 5985 citations. Dodick, David from the Mayo Clinic ranked third with 99 articles and 5200 citations. As shown in Figure 6A, Lipton, RB, Dodick, DW, Buse, DC with TLS values of 360, 260, and 179, respectively appear in the center of the collaboration map, demonstrating their contribution to this field. CiteSpace was used to analyze the co-citation relationships among authors (Figure 6B). Figure 6C shows the authors with the top 10 centralities, revealing that their researches may serve as bridges between different types of research.
 |
Table 3 The Top 10 High-Yield Authors Based on Total Citations |
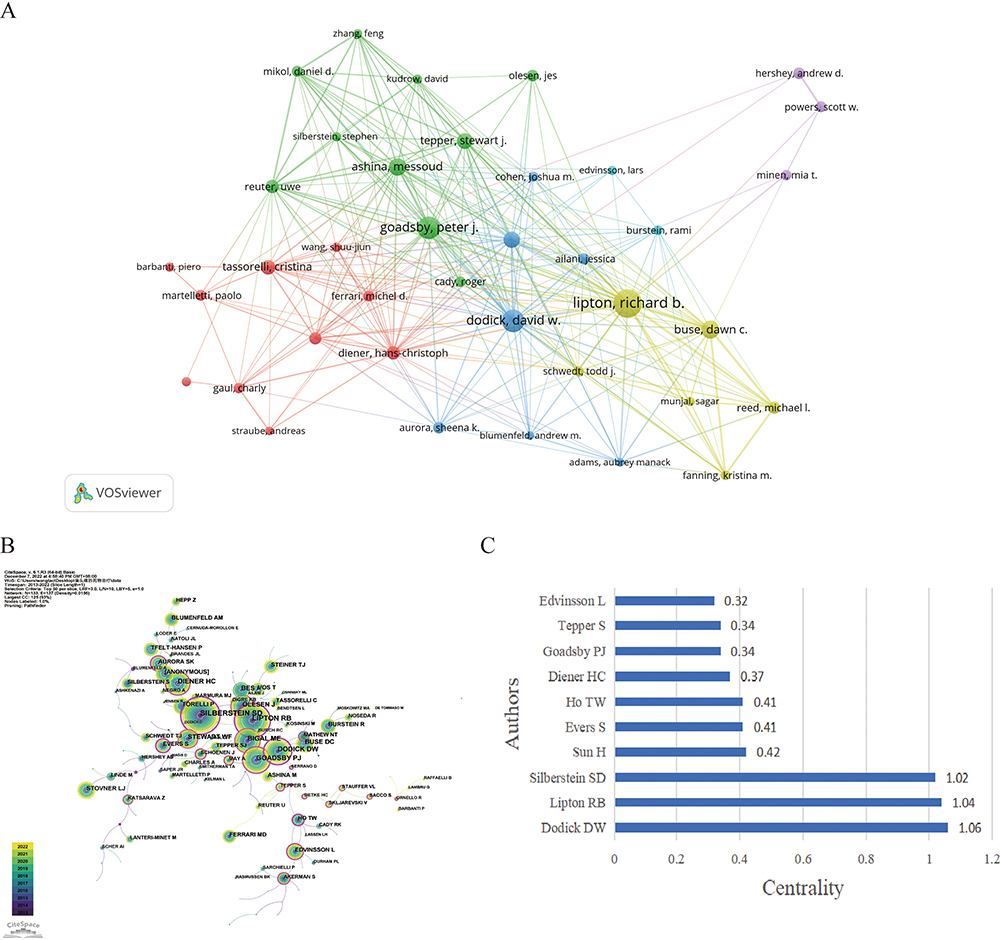 |
Figure 6 (A) Co-authorship relationships between authors. Top3 TLS was: Lipton, Richard B. (TLS=360), Dodick, David W. (TLS=260), and Buse, Dawn C. (TLS=179). (B) Co-Citation relationships between authors. (C) The top 10 authors of centrality in (B). |
Analysis of References
Supplementary Table 1 summarizes the top ten articles on migraine treatment with the most citations. Global citation is used to show global (In WoSCC) academic impact of the articles, whereas local citation reflects the regional (In this data set), and normalized citations can effectively reduce the effect of publication time censoring bias on citation measurements using a special algorithm.26 It found Tepper S, 2017, Lancet neurology27 ranked top with 392 global citations, next to Burstein R, 2015, J Neurosci28 with 385 global citations and Silberstein SD, 2017, New Engl Med29 with 366 global citations. According to normalized global citations, Tepper S, 2017, Lancet neurology27 (18.05 times), Silberstein SD, 2017, New Engl J Med29 (16.85 times), and Digre KB, 2019, Headache30 (16.68 times) were the top three articles.
Supplementary Table 2 summarizes the top 5 most cited references from 2013 to 2022. These references gained more than 174 citations, among which Silberstein S, 2004, Cephalalgia31 ranked first and were cited 762 times.
As illustrated in Figure 7, all the references could be divided into 11 clusters, including onabotulinumtoxina (#0), fremanezumab (#1), neurostimulation (#2), management (#3), erenumab (#4), prophylaxis (#5), trigeminovascular (#6), ubrogepant (#7), nitroglycerin (#8), frovatriptan (#9) and chronic migraine (#10). Generally, clusters with Q > 0.3 are considered significant and clusters with S > 0.5 are thought reasonable. The present study with Q value of 0.8190 and S value of 0.9522 indicates that the results are convincing. Figure 8 shows the development of the 11 clusters over 10 years, with the cluster #0 onabotulinumtoxina, cluster #2 neurostimulation, cluster #5 prophylaxis were the hotspots in the previous years but showed a decreasing trend year by year, indicating that the heat of these fields gradually decreased. However, the cluster #1 fremanezumab, cluster #4 erenumab, cluster #7 ubrogepant peaked in recent years and has been continuously studied. Based on these results, Tepper S, 2017, Lancet neurology27 and Silberstein S, 2004, Cephalalgia31 can be regarded as classic articles in this domain.
 |
Figure 7 Cluster diagrams of references. The figure shows 10 color blocks representing 10 clusters, each composed of articles on the same topic. |
 |
Figure 8 Timeline view of co-citation reference. The timeline from left to right represents the time evolution from 2012–2021. Nodes composed of different colors represent citations. The greater the node is, the larger the citations’ quantity is. The color of the node corresponds to the cited time for the time band. The timeline view visually shows the rise and fall of each area. |
Analysis of Keywords
As illustrated in Figure 9A, co-occurrence analysis of all keywords including 5241 keywords selected by authors and 3807 calculated keywords plus suggested that the keywords with the highest co-occurrence were migraine, headache, double-blind, prevalence, chronic migraine, efficacy, disability, episodic migraine, CGRP etc., which may be the foundation of migraine treatment research and the starting point of many researchers. Supplementary Table 3 displays the top 20 keywords that have the largest TLSs in the co-occurrence map. The overlay map shows the timeliness of the keywords’ co-occurrences (Figure 9B), where a yellow node represents the latest average appearing year (AAY), that could be research hotspot of the future, as shown in Figure 9B. “CGRP”, “safety”, “placebo”, “pathophysiology”, “galcanezumab” and “erenumab” exhibit the latest AAY, each of which is thought to be a potential frontier of migraine treatment research in the future.
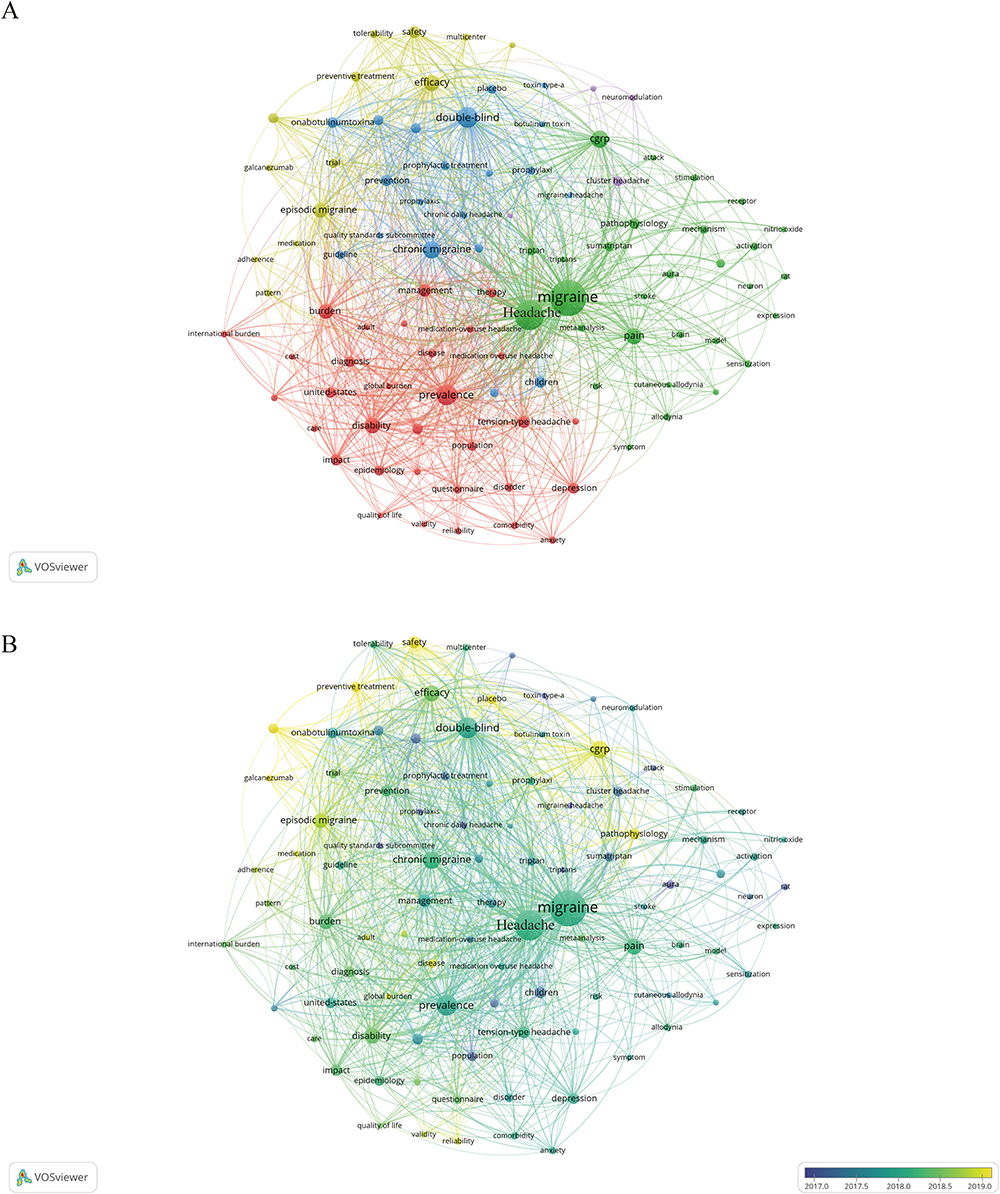 |
Figure 9 (A) Co-occurrence map of keywords on migraine treatment research generated by the VOS viewer. (B) Overlay map of co-occurrence keywords. The yellower node in the figure represents the latest time of appearance. That is, the future hotspots we are looking for. |
Citation bursts suggest an increase in research topics in a specific period and indicate future priorities for research. The top 25 keywords with the strongest citation bursts were identified by CiteSpace (Figure 10). Keywords such as pathophysiology (18.36, 2021–2022), erenumab (9.91, 2020–2022), monoclonal antibody (7,67, 2020–2022), subgroup analysis (6.14, 2021–2022) and ubrogepant (6.05, 2020–2022) were the focus of current research in the field.
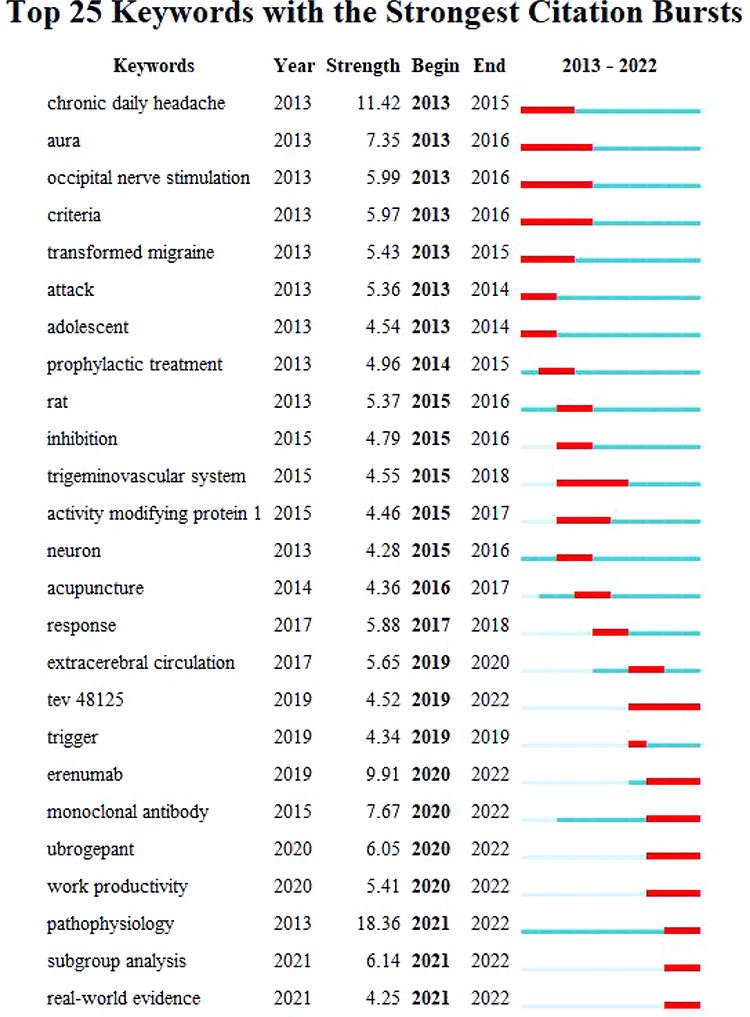 |
Figure 10 Top 25 keywords with the strongest citation bursts. Year: the first occurrence of the keyword; strength: the larger the value, the stronger the emergence of the keyword; begin: the start time of the keyword burst; end: the end time of the keyword burst. The blue line represents the time interval and the red line represents the time of the keyword burst. |
The R-tool bibliometrix was used to count the author keywords and keywords plus to draw a trend topic of the top 25 keywords in this area respectively. Supplementary Figure 2A shows the frequency of author keywords occurrence over time on migraine treatment and Supplementary Figure 2B shows that of keywords plus. Consistent with the results of keywords co-occurrence analysis via VOSviewer and citation bursts analysis by Citespace, migraine, headache, double-blind, prevalence, chronic migraine, efficacy, disability, episodic migraine, CGRP account for the highest frequency of the total keywords, while, ketamine, erenumab, lasmiditan, fremanezumab, subgroup analysis and of life questionnaire are new high-frequency keywords in the past 3 years.
Discussion
It is difficult for scholars to follow the progress of a field in this era of the information boom. As an effective and scientific tool, bibliometrics analysis allows researchers to take a broad view of a field’s past, present, and even future. This gives us succinct information about the trajectory of research in a given domain over the past few decades and serves as a valuable resource for researchers to direct future research. Rapid advancements in migraine treatment research necessitate the need for a bibliometric summary of this period’s research history.
Trends of Migraine Treatment Research Domain
According to 2013–2022 data from SCIE in WoSCC, a total of 3294 papers with 55,537 citations were published in 619 journals by 3897 organizations from 89 countries/regions. The publication outputs of migraine treatment research showed an overall rising trend from 2013 to 2022 and the greatest growth occurred in 2019. It indicates that there is growing concern and understanding about the disorder. While the number of mean article citations per year fluctuates, and the most average article citations occurred in 2018. This phenomenon reminds researchers to focus on high-impact studies rather than publishing as many papers as possible.
The United States holds the leading position in migraine treatment research, as it published the most articles and collaborated with United Kingdom, Germany and Denmark closely, followed by Italy and China. Among the top ten productive countries, 5 of which are European countries, such as Italy, Germany, United Kingdom, Denmark, Spain. This may be related to the high incidence of migraines in European countries, the level of treatment, and the resources invested by governments, like Italy with the highest age-standardized prevalence of migraine.32 While the prevalence in the United States and China was lower than many European countries, especially China with the lowest prevalence of the disorder.32,33 It indicates that the two countries pay attention to this disorder enough. As for organizations, Albert Einstein College of Medicine, University of Copenhagen, Mayo Clinic, Kings College London, and Harvard University are the most active institutions in the migraine treatment domain, most of which are located in the United States.
Regarding journals, Headache, Cephalalgia, Journal of Headache and Pain made significant contributions to this research and can be considered as core journals in the migraine treatment domain. For authors, this study indicates that several authors, including Lipton RB, Goadsby PJ, Dodick DW, Silberstein SD, and Buse DC deserve to be investigated. Lipton RB, Dodick DW, Buse Dawn collaborated more closely with other authors and were potential collaborators on relevant research. In bibliometric analysis, the number of papers, h-index, and citations can be used to evaluate an author’s research achievements.
Hotspots of the Migraine Treatment Research Domain
Among the top 10 cited articles, the latest was published in 2019, while the earliest was published in 2013, where Tepper S, 2017, Lancet neurology27 and Silberstein S, 2004, Cephalalgia31 were defined as classic articles by the bibliometric analysis, suggested their high research value. The efficacy and safety of erenumab, a human monoclonal antibody against the CGRP receptor, was assessed in patients with chronic migraine by Stewart Tepper et al.27 Besides, Migraine pathophysiology and its clinical implications were reviewed in Silberstein S, 2004, Cephalalgia.31 With normalized citations, Silberstein SD, 2017, New Engl J Med29 can also be defined as high-cited articles which may be cited more times in the future. Among the 10 papers with most citations listed in Supplementary Table 1, 5 papers concentrated on the efficacy and safety evaluation of CGRP-related therapeutics, such as fremanezumab, erenumab, galcanezumab where clinical trials related to monoclonal antibodies that target CGRP or its receptor particularly attracted considerable attention. As shown in Figure 8, #1 fremanezumab, #3 management, #4 erenumab, and #7 ubrogepant were still highly cited in 2022, which might be the representatives of the hot spots in current research. The 6 latest AAY keywords extracted in Figure 9B are “CGRP”, “safety”, “placebo”, “pathophysiology”, “galcanezumab” and “erenumab”, which can be thought of the direction of future migraine treatment research. As shown in Figure 10 keywords such as pathophysiology, erenumab, monoclonal antibody, subgroup analysis and ubrogepant had strong citation bursts. Based on these results, the current research hotspots mainly including studies on CGRP-related therapeutics, while future studies on migraine treatment will focus on: (I). In-depth understanding of the pathophysiological mechanisms of migraine; (II). Seeking new therapeutics for migraine based on pathophysiology, like CGRP-related therapeutics; (III). Conducting randomized controlled trials (RCTs) to verify the safety and efficacy of the new therapies.
Although migraine has been studied for decades and activation of the trigeminovascular system is recognized responsible for the characteristics of headache in migraine, its pathogenesis is incompletely understood so far. Advancement in understanding of migraine may provide new opportunities for more effective patient management. CGRP has been demonstrated as a mediator of migraine and patients with chronic migraine have persistently elevated CGRP concentrations.34–36 Based on these evidences, several treatment strategies target CGRP or its receptor have been discovered and verified efficacy as acute and prevention migraine therapies.37–39 PACAP is also reported as a mediator of migraine.40,41 Infusion of PACAP can also trigger migraine attack in susceptible individuals, and increased levels of PACAP have been reported in migraine patients during attacks, similar to CGRP.42 Therefore, PACAP, like CGRP, also could be a promising therapeutic target in migraine.
Besides, there is strong evidence that changes in thalamic and thalamo-cortical activity play a key role in the aberrant sensory processing related to migraines,43,44 and could be a therapeutic target for neuromodulatory methods such as TMS.45 And the association between gut microbiome and migraine that was demonstrated recently46,47 might also represent a potential therapeutic target in migraine. In a word, the list of potential targets for migraine treatment is long and will continue to grow with advancement in understanding of migraine.
Prospective, randomized, controlled clinical trials are the gold standard to assess the efficacy and safety of interventions for migraine. The International Headache Society guidelines for controlled trials of acute and preventive treatments for migraine have assured the continued viability of RCTs. Therefore, more standard clinical trials should be conducted to verify the safety and efficacy of these potential therapies and more, safer and more effective migraine therapies will be emerged in the future with advancement in understanding of migraine.
Limitation
There were some limitations in our study. First, we only included English papers that were indexed in the WoSCC database. Second, the included literature had varying degrees of quality, which could have caused some variation in the analysis.
Conclusions
Global research trends and hotspots in migraine treatment research are highlighted in this study. Migraine treatment has received much attention and made breakthroughs during the past 10 years. Most articles in this field were published in the United States, Italy and China. The current research hotspots mainly including studies on CGRP-related therapeutics, while future studies on migraine treatment will focus on understanding of the pathophysiological mechanisms of migraine, seeking new therapeutics for migraine based on pathophysiology, like CGRP-related therapeutics, and conducting randomized controlled trials (RCTs) to verify the safety and efficacy of the new therapies. It can aid researchers in swiftly grasping the present state and key areas of this field’s research.
Data Sharing Statement
The datasets generated or analyzed during the current study are available from the corresponding author on reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding was received for conducting this study.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders, 3rd edition. Cephalalgia. 2018;38(1):1–211. doi:10.1177/0333102417738202
2. Burch RC, Buse DC, Lipton RB. Migraine: epidemiology, Burden, and Comorbidity. Neurol Clin. 2019;37(4):631–649. doi:10.1016/j.ncl.2019.06.001
3. Feigin VL, Nichols E, Alam T. Global, regional, and national burden of neurological disorders, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2019;18(5):459–480. doi:10.1016/S1474-4422(18)30499-X
4. Vos T, Abajobir AA, Abate KH. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–1259. doi:10.1016/S0140-6736(17)32154-2
5. Steiner TJ, Jensen R, Katsarava Z, et al. Aids to management of headache disorders in primary care (2nd edition): on behalf of the European Headache Federation and Lifting The Burden: the Global Campaign against Headache. J Headache Pain. 2019;20(1):57. doi:10.1186/s10194-018-0899-2
6. Ashina M. Migraine. N Engl J Med. 2020;383(19):1866–1876. doi:10.1056/NEJMra1915327
7. González-Hernández A, Marichal-Cancino BA, MaassenVanDenBrink A, Villalón CM. Side effects associated with current and prospective antimigraine pharmacotherapies. Expert Opin Drug Metab Toxicol. 2018;14(1):25–41. doi:10.1080/17425255.2018.1416097
8. Munksgaard SB, Madsen SK, Wienecke T. Treatment of medication overuse headache-A review. Acta Neurol Scand. 2019;139(5):405–414. doi:10.1111/ane.13074
9. Kung D, Rodriguez G, Evans R. Chronic Migraine: diagnosis and Management. Neurol Clin. 2023;41(1):141–159. doi:10.1016/j.ncl.2022.05.005
10. Katsuki M, Yamagishi C, Matsumori Y, et al. Questionnaire-based survey on the prevalence of medication-overuse headache in Japanese one city-Itoigawa study. Neurol Sci. 2022;43(6):3811–3822. doi:10.1007/s10072-021-05831-w
11. Ashina M, Buse DC, Ashina H, et al. Migraine: integrated approaches to clinical management and emerging treatments. Lancet. 2021;397(10283):1505–1518. doi:10.1016/S0140-6736(20)32342-4
12. Goadsby PJ, Dodick DW, Ailani J, et al. Safety, tolerability, and efficacy of orally administered atogepant for the prevention of episodic migraine in adults: a double-blind, randomised Phase 2b/3 trial. Lancet Neurol. 2020;19(9):727–737. doi:10.1016/S1474-4422(20)30234-9
13. Lipton RB, Croop R, Stock EG, et al. Rimegepant, an Oral Calcitonin Gene-Related Peptide Receptor Antagonist, for Migraine. N Engl J Med. 2019;381(2):142–149. doi:10.1056/NEJMoa1811090
14. Croop R, Lipton RB, Kudrow D, et al. Oral rimegepant for preventive treatment of migraine: a phase 2/3, randomised, double-blind, placebo-controlled trial. Lancet. 2021;397(10268):51–60. doi:10.1016/S0140-6736(20)32544-7
15. Ashina M, Doležil D, Bonner JH, et al. A phase 2, randomized, double-blind, placebo-controlled trial of AMG 301, a pituitary adenylate cyclase-activating polypeptide PAC1 receptor monoclonal antibody for migraine prevention. Cephalalgia. 2021;41(1):33–44. doi:10.1177/0333102420970889
16. Xu S, Yu L, Luo X, et al. Manual acupuncture versus sham acupuncture and usual care for prophylaxis of episodic migraine without aura: multicentre, randomised clinical trial. BMJ. 2020;368:m697. doi:10.1136/bmj.m697
17. Stilling JM, Monchi O, Amoozegar F, Debert CT. Transcranial Magnetic and Direct Current Stimulation (TMS/tDCS) for the Treatment of Headache: a Systematic Review. Headache. 2019;59(3):339–357. doi:10.1111/head.13479
18. Liu Y, Dong Z, Wang R, et al. Migraine Prevention Using Different Frequencies of Transcutaneous Occipital Nerve Stimulation: a Randomized Controlled Trial. j Pain. 2017;18(8):1006–1015. doi:10.1016/j.jpain.2017.03.012
19. Yu S, Ran Y, Xiao W, et al. Treatment of migraines with Tianshu capsule: a multi-center, double-blind, randomized, placebo-controlled clinical trial. BMC Complement Altern Med. 2019;19(1):370. doi:10.1186/s12906-019-2775-2
20. Yu S, Ran Y, Wan Q, et al. Efficacy and Safety of Toutongning Capsule in Patients with Migraine: a Multicenter, Randomized, Double-Blind, Placebo-Controlled Trial. J Alternative Complementary Med. 2019;25(12):1215–1224. doi:10.1089/acm.2018.0500
21. Chen C, Song M. Visualizing a field of research: a methodology of systematic scientometric reviews. PLoS One. 2019;14(10):e0223994. doi:10.1371/journal.pone.0223994
22. van Eck NJ, Waltman L. Software survey: vOSviewer, a computer program for bibliometric mapping. Scientometrics. 2010;84(2):523–538. doi:10.1007/s11192-009-0146-3
23. Chen C, Hu Z, Liu S, Tseng H. Emerging trends in regenerative medicine: a scientometric analysis in CiteSpace. Expert Opin Biol Ther. 2012;12(5):593–608. doi:10.1517/14712598.2012.674507
24. Aria M, Cuccurullo C. bibliometrix: an R-tool for comprehensive science mapping analysis. J Informetr. 2017;11(4):959–975. doi:10.1016/j.joi.2017.08.007
25. Zhao Y, Huang L, Liu M, Gao H, Li W. Scientific Knowledge Graph of Acupuncture for Migraine: a Bibliometric Analysis from 2000 to 2019. J Pain Res. 2021;14:1985–2000. doi:10.2147/JPR.S314174
26. Bornmann L, Haunschild R. Citation score normalized by cited references (CSNCR): the introduction of a new citation impact indicator. J Informetr. 2016;10(3):875–887. doi:10.1016/j.joi.2016.07.002
27. Tepper S, Ashina M, Reuter U, et al. Safety and efficacy of erenumab for preventive treatment of chronic migraine: a randomised, double-blind, placebo-controlled phase 2 trial. Lancet Neurol. 2017;16(6):425–434. doi:10.1016/S1474-4422(17)30083-2
28. Burstein R, Noseda R, Borsook D. Migraine: multiple processes, complex pathophysiology. J Neurosci. 2015;35(17):6619–6629. doi:10.1523/JNEUROSCI.0373-15.2015
29. Silberstein SD, Dodick DW, Bigal ME, et al. Fremanezumab for the Preventive Treatment of Chronic Migraine. N Engl J Med. 2017;377(22):2113–2122. doi:10.1056/NEJMoa1709038
30. American Headache Society. The American Headache Society Position Statement On Integrating New Migraine Treatments Into Clinical Practice. Headache. 2019;59:1–18.
31. Silberstein SD. Migraine pathophysiology and its clinical implications. Cephalalgia. 2004;24 Suppl 2(2_suppl):2–7. doi:10.1111/j.1468-2982.2004.00892.x
32. Stovner LJ, Nichols E, Steiner TJ. Global, regional, and national burden of migraine and tension-type headache, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet Neurol. 2018;17(11):954–976. doi:10.1016/S1474-4422(18)30322-3
33. Yu S, Liu R, Zhao G, et al. The prevalence and burden of primary headaches in China: a population-based door-to-door survey. Headache. 2012;52(4):582–591. doi:10.1111/j.1526-4610.2011.02061.x
34. Cernuda-Morollón E, Larrosa D, Ramón C, Vega J, Martínez-Camblor P, Pascual J. Interictal increase of CGRP levels in peripheral blood as a biomarker for chronic migraine. Neurology. 2013;81(14):1191–1196. doi:10.1212/WNL.0b013e3182a6cb72
35. Zhang Q, Han X, Wu H, et al. Dynamic changes in CGRP, PACAP, and PACAP receptors in the trigeminovascular system of a novel repetitive electrical stimulation rat model: relevant to migraine. Mol Pain. 2019;15:1744806918820452. doi:10.1177/1744806918820452
36. Ashina M, Hansen JM, Olesen J. Pearls and pitfalls in human pharmacological models of migraine: 30 years’ experience. Cephalalgia. 2013;33(8):540–553. doi:10.1177/0333102412475234
37. Yu S, Kim BK, Wang H, et al. A Phase 3, randomised, placebo-controlled study of erenumab for the prevention of chronic migraine in patients from Asia: the DRAGON study. J Headache Pain. 2022;23(1):146. doi:10.1186/s10194-022-01514-9
38. Hu B, Li G, Li X, et al. Galcanezumab in episodic migraine: the phase 3, randomized, double-blind, placebo-controlled PERSIST study. J Headache Pain. 2022;23(1):90. doi:10.1186/s10194-022-01458-0
39. Marcus R, Goadsby PJ, Dodick D, Stock D, Manos G, Fischer TZ. BMS-927711 for the acute treatment of migraine: a double-blind, randomized, placebo controlled, dose-ranging trial. Cephalalgia. 2014;34(2):114–125. doi:10.1177/0333102413500727
40. Amin FM, Hougaard A, Schytz HW, et al. Investigation of the pathophysiological mechanisms of migraine attacks induced by pituitary adenylate cyclase-activating polypeptide-38. Brain. 2014;137(3):779–794. doi:10.1093/brain/awt369
41. Han X, Dong Z, Hou L, et al. Interictal plasma pituitary adenylate cyclase-activating polypeptide levels are decreased in migraineurs but remain unchanged in patients with tension-type headache. Clin Chim Acta. 2015;450:151–154. doi:10.1016/j.cca.2015.08.017
42. Hou L, Wan D, Dong Z, et al. Pituitary adenylate cyclase-activating polypeptide expression in peripheral blood mononuclear cells of migraineurs. Cell Biosci. 2016;6(1):40. doi:10.1186/s13578-016-0106-6
43. Coppola G, Di Renzo A, Tinelli E, et al. Thalamo-cortical network activity during spontaneous migraine attacks. Neurology. 2016;87(20):2154–2160. doi:10.1212/WNL.0000000000003327
44. Coppola G, Di Renzo A, Tinelli E, et al. Thalamo-cortical network activity between migraine attacks: insights from MRI-based microstructural and functional resting-state network correlation analysis. J Headache Pain. 2016;17(1):100. doi:10.1186/s10194-016-0693-y
45. Andreou AP, Holland PR, Akerman S, Summ O, Fredrick J, Goadsby PJ. Transcranial magnetic stimulation and potential cortical and trigeminothalamic mechanisms in migraine. Brain. 2016;139(7):2002–2014. doi:10.1093/brain/aww118
46. Kang L, Tang W, Zhang Y, et al. The gut microbiome modulates nitroglycerin-induced migraine-related hyperalgesia in mice. Cephalalgia. 2022;42(6):490–499. doi:10.1177/03331024211050036
47. Miao S, Tang W, Li H, et al. Repeated inflammatory dural stimulation-induced cephalic allodynia causes alteration of gut microbial composition in rats. J Headache Pain. 2022;23(1):71. doi:10.1186/s10194-022-01441-9
48. Burch RC, Loder S, Loder E, Smitherman TA. The prevalence and burden of migraine and severe headache in the United States: updated statistics from government health surveillance studies. Headache 2015;55:21–34. doi:10.1111/head.12482
49. Dodick DW, Goadsby PJ, Spierings EL, Scherer JC, Sweeney SP, Grayzel DS. Safety and efficacy of LY2951742, a monoclonal antibody to calcitonin gene-related peptide, for the prevention of migraine: a phase 2, randomised, double-blind, placebo-controlled study. The Lancet Neurology 2014;13(9):885–892. doi:10.1016/S1474-4422(14)70128-0
50. Marmura MJ, Silberstein SD, Schwedt TJ. The acute treatment of migraine in adults: the American headache society evidence assessment of migraine pharmacotherapies. Headache 2015;55(1):3–20. doi:10.1111/head.12499
51. Simpson DM, Hallett M, Ashman EJ, et al. Practice guideline update summary: botulinum neurotoxin for the treatment of blepharospasm, cervical dystonia, adult spasticity, and headache: report of the Guideline Development Subcommittee of the American Academy of Neurology. Neurology 2016;86(19):1818–1826. doi:10.1212/WNL.0000000000002560
52. Dodick DW, Ashina M, Brandes JL, et al. ARISE: a Phase 3 randomized trial of erenumab for episodic migraine. Cephalalgia: an International Journal of Headache 2018;38(6):1026–1037. doi:10.1177/0333102418759786
53. Stauffer VL, Dodick DW, Zhang Q, Carter JN, Ailani J, Conley RR. Evaluation of Galcanezumab for the Prevention of Episodic Migraine: the EVOLVE-1 Randomized Clinical Trial. JAMA Neurology 2018;75(9):1080–1088. doi:10.1001/jamaneurol.2018.1212
54. Zhang Y. The International Classification of Headache Disorders, 3rd edition (beta version). International Journal of Headache 2013;33(1):629–808. doi:10.1177/0333102413485658
55. Torelli P, Jensen R, Olesen J. Physiotherapy for tension-type headache: a controlled study. Cephalalgia: an International Journal of Headache 2004;24(1):29–36. doi:10.1111/j.1468-2982.2004.00633.x
56. Lipton RB, Bigal ME, Diamond M, Freitag F, Reed ML, Stewart WF. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology 2007;68(5):343–349. doi:10.1212/01.wnl.0000252808.97649.21
57. Diener HC, Barbanti P, Dahlöf C, Reuter U, Habeck J, Podhorna J. BI 44370 TA, an oral CGRP antagonist for the treatment of acute migraine attacks: results from a Phase II study. Cephalalgia: an International Journal of Headache 2011;31(5):573–584. doi:10.1177/0333102410388435
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Worldwide Bibliometric Analysis of Published Literature on Osteoporosis Vertebral Compression Fracture
Li Y, Tian J, Ge M, Ji L, Kang Y, Xia C, Zhang J, Huang Y, Feng F, Zhao T, Shao H
Journal of Pain Research 2022, 15:2373-2392
Published Date: 18 August 2022
Scientific Knowledge of Rheumatoid Arthritis: A Bibliometric Analysis from 2011 to 2020
Xu J, Yu J, Jiao W, Chen G, Liu L, Zhang M, Wu D
Journal of Pain Research 2022, 15:2761-2772
Published Date: 8 September 2022
A Bibliometric Analysis of Acupuncture Treatment of Tension-Type Headache from 2003 to 2022
Zhu D, Xu W, Mao Q, Zhong G, Chen R, Jiao L
Journal of Pain Research 2023, 16:1647-1662
Published Date: 18 May 2023
Bibliometric Analysis of Global Trends in Remimazolam-Related Research Over the Past 15 Years: Compared with Propofol
Hu X, Wang B, Hu L, Han D, Wu J
Drug Design, Development and Therapy 2023, 17:2119-2135
Published Date: 20 July 2023
Research Trends and Foci in Osteoarthritis Pain from 2012 to 2022: Bibliometric and Visualization Study

Zhao C, Yang G, Ji B, Jin H, Naranmandakh S, Li Y
Journal of Pain Research 2023, 16:2567-2585
Published Date: 26 July 2023