Back to Journals » Advances in Medical Education and Practice » Volume 14
3D-Printing-Based Fluoroscopic Coronary Angiography Simulator Improves Learning Capability Among Cardiology Trainees
Authors Wibowo G, Anggrahini DW, Rismawanti RI, Fatimah VAN, Hakim A, Hidayah RN ![]() , Gharini PPR
, Gharini PPR
Received 21 March 2023
Accepted for publication 23 June 2023
Published 13 July 2023 Volume 2023:14 Pages 763—771
DOI https://doi.org/10.2147/AMEP.S407629
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Ganda Wibowo,1,2 Dyah Wulan Anggrahini,1,2 Rochmi Isnaini Rismawanti,1 Vita Arfiana Nurul Fatimah,1 Alhadi Hakim,1 Rachmadya Nur Hidayah,3 Putrika Prastuti Ratna Gharini1,2
1Department of Cardiology and Vascular Medicine, Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia; 2Integrated Cardiovascular Center, Dr. Sardjito General Hospital, Yogyakarta, Indonesia; 3Department of Medical Education and Bioethics, Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada, Yogyakarta, Indonesia
Correspondence: Putrika Prastuti Ratna Gharini, Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada, Jalan Farmako Sekip Utara, Depok, Sleman, Daerah Istimewa, Yogyakarta, 55281, Indonesia, Tel +62 8180 4309 353, Fax +62 274 581 876, Email [email protected]
Aim: One of the essential competencies of cardiology trainees is the ability to perform coronary angiography with good projection.
Purpose: This study is a research and development study aimed at testing the effectiveness of 3D-printing-based fluoroscopic coronary angiography simulator as a learning medium for diagnostic coronary angiogram.
Methods: Thirty-four cardiology trainees randomly were divided into two groups. Both groups took a pretest before the intervention. The first group (group A) studied using conventional learning media and underwent the first post-test. Afterward, they switched to a 3D-printing-based fluoroscopic coronary angiography simulator and underwent a second post-test. The second group (group B) studied using a 3D-printing-based fluoroscopic coronary angiography simulator, underwent the first post-test, switched to the conventional learning media, and underwent a second post-test.
Results: The delta between the post-test I and the pretest of group B was 8.53, higher than the delta between the post-test I and the pretest of group A (5.21) with a significant difference (p = 0.003). In group A, the delta between post-test II and pretest was 9.65, higher than the delta between post-test I and pretest (5.21) with a significant difference (p < 0.001).
Conclusion: 3D-printing-based fluoroscopic coronary angiography simulator is effective as a learning medium for coronary angiogram diagnostics.
Keywords: 3D-printing-based fluoroscopic coronary angiography simulator, effectiveness, learning, cardiology, trainee, diagnostic, conventional
Graphical Abstract:

Introduction
The ability to perform and interpret cardiovascular examinations using invasive and non-invasive modalities is one of the key competencies of cardiology trainees. The learning objective is for students to be able to perform coronary angiography (CA) with good projection and evaluate normal and pathological coronary angiography.1 Coronary angiography is an X-ray procedure aiming to visualize the arteries in the heart.2 3D printing models created from real patient images have a great potential to reduce the misinterpretation of pathological structures.3 Research on medical students using 3D-printing found a significant improvement in the conceptualization of the heart structure.4 3D printing can improve the spatial orientation of medical students.5 Visuospatial ability is the ability to manipulate or rotate 3D objects as a cognitive process. This ability has an essential role in medical training or for participants in surgical technique training and basic anatomy education for medical students.6 Visuospatial ability influences the ability to learn anatomy, and accordingly, educators can develop learning methods to improve students’ visuospatial abilities in understanding anatomical structures and medical training7 On the other hand, simulation can improve technical skills, as found in the study where beginners who underwent simulations significantly developed technical skills in the first week. The improvement was more evident in participants with no experience than in more experienced participants.8
Traditional learning methods for studying anatomy mainly use images from anatomy atlases and textbooks.9 Visualizing where and how these structures run is critical to the complexity of the coronary arteries. Physical models are proven superior to other learning media used for anatomy learning.10 At the Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada, a new learning model for 3D-printing coronary arteries has been developed.11 A 3D-printing-based fluoroscopic coronary angiography simulator has been developed,12 and recently has been revised based on expert validation. The new state of using 3D-printing-based coronary artery learning models presents a dilemma of whether one should adopt the technology due to the lack of knowledge on its effectiveness. For a technology or method to be adopted, evidence is needed to show that the positive impacts outweigh the negative consequences.13 The effectiveness of the teaching method using a 3D-printing-based fluoroscopic coronary angiography simulator as a coronary angiogram diagnostic learning medium and its impact on the cardiology trainee’s understanding of coronary anatomy and its application in coronary angiography procedures have never been evaluated.
The contributions of this study area are described below:
- 3D-printing-based fluoroscopic coronary angiography simulator enhances the diagnostic ability of coronary angiograms for students.
- Students will increase their interest and motivation in learning coronary angiography using a 3D-printing-based fluoroscopic coronary angiography simulator.
Materials and Methods
Design and Subject
This research used a research and development (R&D) design to evaluate the effectiveness of a 3D-printing-based fluoroscopic coronary angiography simulator as a coronary angiogram diagnostic learning medium with quantitative and qualitative methods. The study was conducted at Dr. Sardjito General Hospital, Yogyakarta, Indonesia. Participants were taken from the entire affordable population using a purposive sampling method with 34 participants consisting of 28 cardiology residents and 6 internal medicine residents. Inclusion criteria include (1) Cardiology residents who have not undergone clinical rotation of the invasive division at Dr. Sardjito General Hospital, (2) Internal medicine residents who are undergoing clinical rotation in the Cardiology Department, and (3) Willing to sign the consent form to participate. Exclusion criteria include: (1) Having undergone training or simulation using 3D-printing coronary models or 3D-printing-based fluoroscopic coronary angiography simulator.
Instruments
This study uses three instruments: a 3D-printing-based fluoroscopic coronary angiography simulator, conventional learning media, and pretest and post-test questions. The first instrument is a 3D-printing-based fluoroscopic coronary angiography simulator owned by the Faculty of Medicine, Public Health and Nursing, Universitas Gadjah Mada, consisting of a 3D coronary model anatomically positioned and coupled with a light source to resemble the actual coronary angiography process as shown by Figure 1. The second instrument is conventional learning media, including material on basic coronary anatomy and identification of 2D fluoroscopy images from various standard projections used in coronary angiography, which refers to the textbook The Cardiac Catheterization Handbook delivered by an instructor using conventional learning media (textbooks presented in the form of slides and examples of 2D coronary angiogram images). The third instrument is the pretest and post-test questions. The questions are crafted referring to the competency standard provided by Indonesian Heart Association and have been validated by three cardiology experts. Aiken’s content validity of V=0.91 and Lawshe’s content validity of CVR = 1 was acquired, which shows that the questions are proven valid. The pretest and post-test questions are about basic coronary anatomy and identification of 2D fluoroscopy images from various projections, including 17 multiple choice questions and three essay questions in the form of reading normal coronary angiography videos.
 |
Figure 1 (a) Coronary angiography simulator equipped with light source and white screen. (b) 3D-printed transparent heart model with opaque coronary artery. (c) Result image of the coronary angiography simulator. |
Research Scheme
Participants underwent a pretest and were then randomized into two groups, each consisting of 17 participants (Figure 2).
 |
Figure 2 Research scheme. |
Data Analysis
The statistical analysis was conducted using the IBM SPSS version 26 software. The effectiveness of the 3D-printing-based fluoroscopic coronary angiography simulator as a coronary angiogram diagnostic learning medium is analyzed by calculating the difference (delta values) of the pretest, post-test I, and post-test II using the t-test.
Ethical Issues
This research was conducted with the approval of Medical and Health Research Ethics Committee, Faculty of Medicine, Public Health and Nursing Universitas Gadjah Mada, Yogyakarta, Indonesia with reference number KE/FK/0890/EC/2021. Subjects were explained about the research procedures and signed the informed consent forms before participating. This study complies with the Declaration of Helsinki.
Results
The research was carried out by collecting the data directly from the participants in July 2022. During the data collection period, all participants could take part in the study to completion.
Basic Characteristics of Participants
The mean age of the participants in this study was 29.7 years in both groups. Most participants were male in group A (64.7%) and group B (52.9%). The majority of the semester level is the semester I (35.3%) in group A and semester III (52.95%) in group B. There was no difference in the characteristics of the participants between the two groups based on age, gender, and semester (p > 0.05), while based on the department showed a significant difference (p = 0.018) (Table 1).
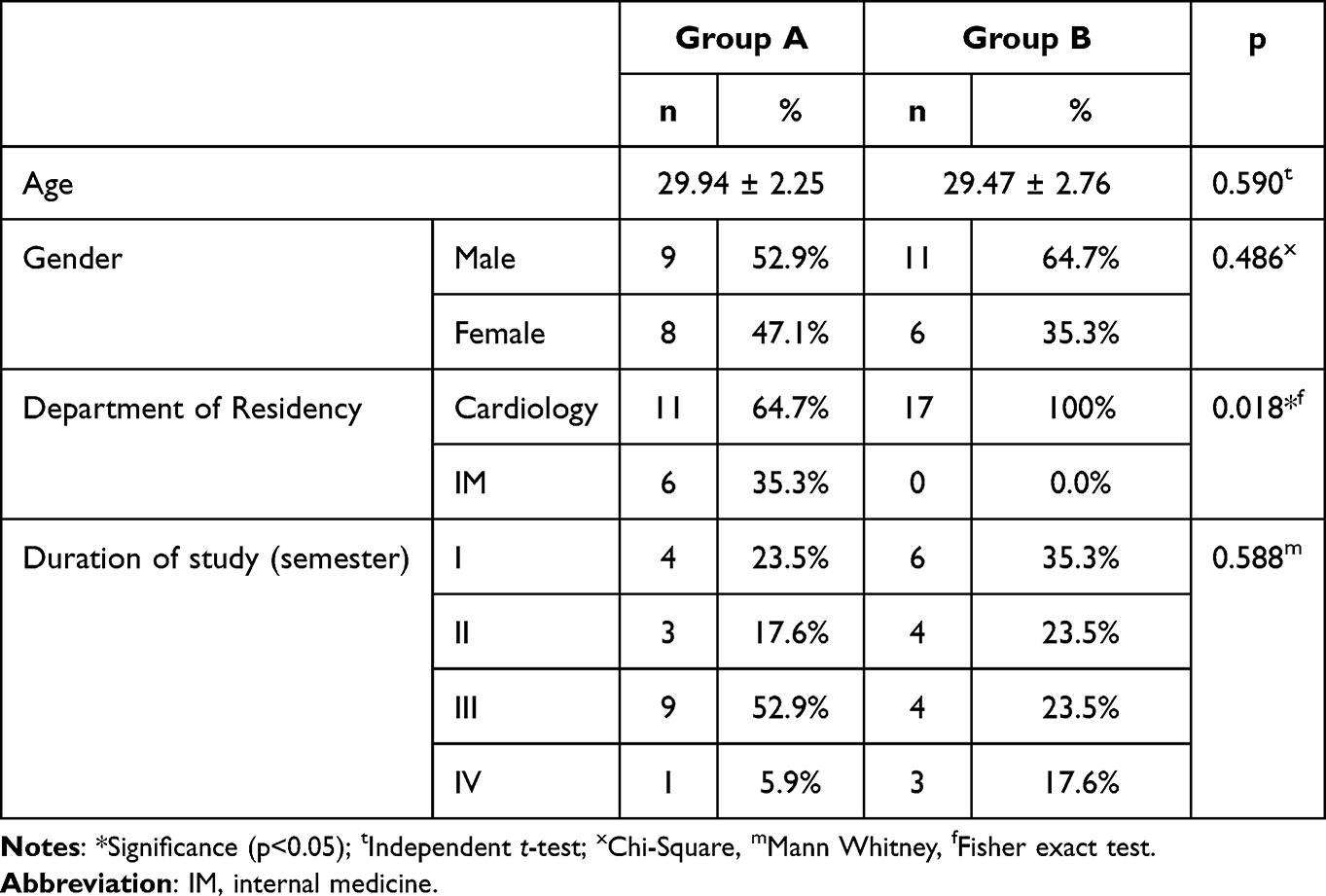 |
Table 1 Basic Characteristics of Participants |
Results of Pretest, Post-Test I, Post-Test II
The results of pretest, post-test I, and post-test II in both groups are presented in the following table (Table 2).
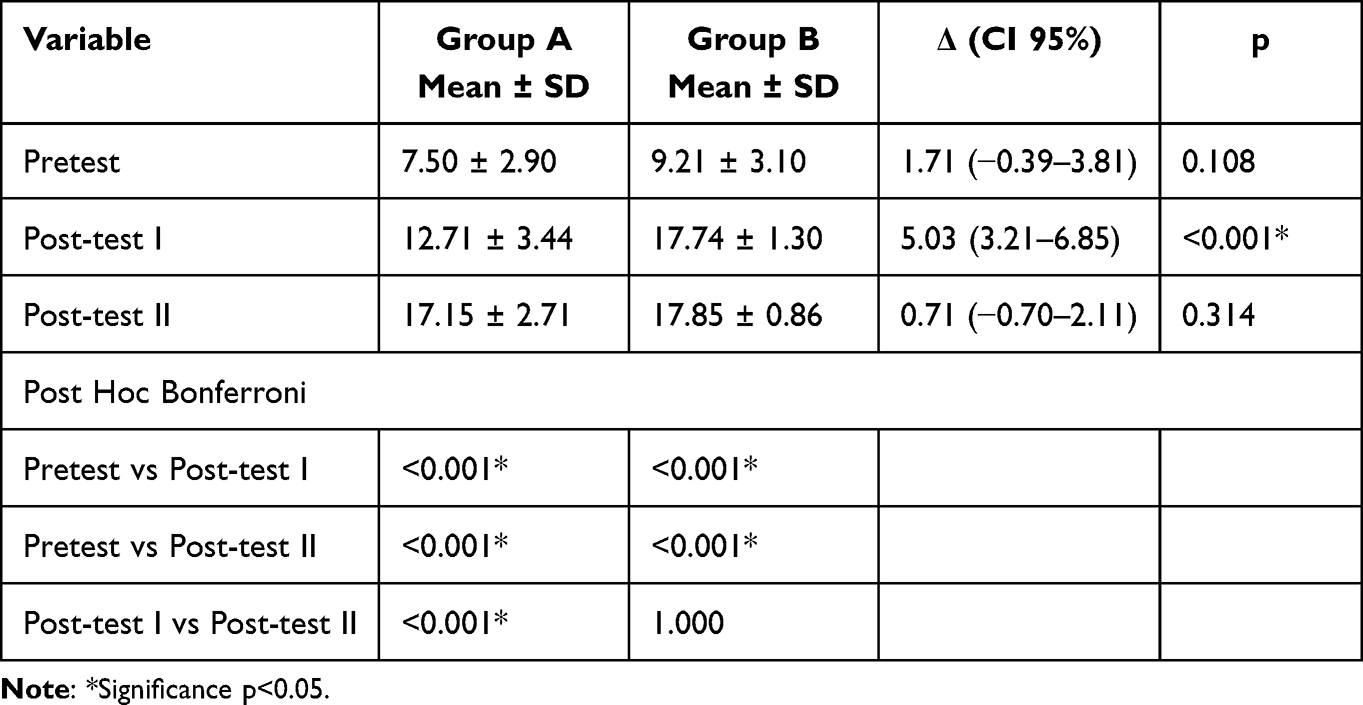 |
Table 2 Analysis of General Linear Model (GLM) with Repeated Measure ANOVA Test with Bonferroni Post Hoc |
The results of the normality test of pretest, post-test I, post-test II, delta post-test I – pretest, and delta post-test II – pretest data obtained p value >0.05 in each group. This shows that the data were normally distributed. To compare the measurement results from time to time between the two groups, the general linear model analysis was presented with the repeated measure ANOVA test with Bonferroni post hoc.
The difference scores between the two groups showed that the mean pretest score for group A was 7.50 and group B was 9.21, showing no significant difference (p = 0.108). This finding indicates that the pretest score between the two groups is homogeneous. The mean score of post-test I in group B was 17.74, higher than group A, which was 12.71, with a significant difference (p < 0.001). The post-test II score of group B was 17.85, higher than group A, which was 17.15 without a significant difference (p = 0.314). The results of the difference in values in one group (with post hoc Bonferroni), it was found that in group A, there was a significant increase in the value of the pretest to post-test I, from 7.50 to 12.71 (p < 0.001) and increased significantly again from the post-test I to post-test II, from 12.71 to 17.15 (p < 0.001).
Likewise, in group B, there was a significant increase in the value of the pretest to post-test I, from 9.21 to 17.74 (p < 0.001), but from post-test I to post-test II, there was a non-significant increase in scores from 17.74 to 17.85 (p = 1).
The mean pretest scores between the two groups showed no significant difference (p = 0.108). The mean score of post-test I in group B (17.74) was higher than group A (12.71), with a significant difference (p < 0.001). The post-test II score of group B (17.85) was higher than group A (17.15) but did not show a significant difference (p = 0.314). The results of the difference in values in one group (with post hoc Bonferroni), it was found that in group A, there was a significant increase in the value of the pretest to post-test I, from 7.50 to 12.71 (p < 0.001) and increased significantly again from the post-test I to post-test II, from 12.71 to 17.15 (p < 0.001). In group B there was a significant increase in the value of pretest to post-test I, from 9.21 to 17.74 (p < 0.001), but from post-test I to post-test II, there was a non-significant increase in scores from 17.74 to 17.85 (p = 1).
Effectiveness Analysis of 3D-Printing-Based Fluoroscopic Coronary Angiography Simulator
Effectiveness analysis of the 3D-printing-based fluoroscopic coronary angiography simulator as a coronary angiogram diagnostic learning medium was defined by calculating the value of the difference (delta) of pretest, post-test I, and post-test II. The analysis used the t-test with the following results (Figure 3).
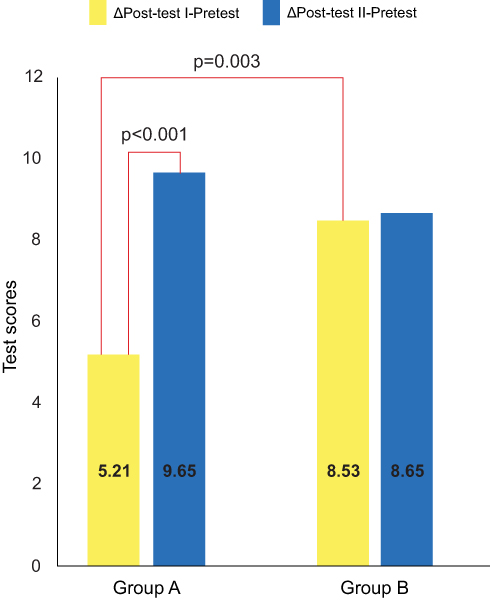 |
Figure 3 Effectiveness analysis of 3D-printing-based fluoroscopic coronary angiography simulator. |
The delta between post-test I and pretest in group B was 8.53. This was higher than the delta between post-test I and pretest group A, which was 5.21, with a significant difference (p = 0.003). The delta between post-test II and pretest in group A was 9.65. This was higher than the delta between post-test II and pretest group B, which was 8.65, with no significant difference (p = 0.368). In group A, the delta between post-test II and pretest was 9.65. This was higher than the delta between post-test I and pretest in group A, which was 5.21, with a significant difference (p < 0.001). In group B, the delta between post-test II and pretest was 8.65. This was higher than the delta between post-test I and pretest, which was 8.53, with no significant difference (p = 0.774). These results show that the 3D-printing-based fluoroscopic coronary angiography simulator is effective as a coronary angiogram diagnostic learning medium.
Discussion
The principal aim of our study was to determine the effectiveness of 3D-printing-based fluoroscopic as a coronary angiogram diagnostic learning method and address the potential of its application. This study showed that the simulator is an effective coronary angiogram teaching method. Increase of knowledge and CA interpretation skill was observed in simulator group showed by the significant increase of post-test score. Previous similar studies determined the effectiveness of incorporating simulator into clinical learning by the improvements of knowledge, skills and satisfaction.14 In the eleven studies comparing simulated training with no simulation, simulated training was associated with moderate improvements in skills and satisfaction compared to non-simulation training.14 The result of our study also supports previous study conducted by Wong and colleagues demonstrating the improvement in CA interpretation skills by virtual 3D CA simulator implementation to trainees.15 Another study held by Canty et al showed that an ultrasound simulator is a feasible and equivalent additional medium for studying cardiac anatomy compared to studying using a cadaver.16
When compared to existing conventional coronary angiogram learning media, our simulator learning model gain higher increase of knowledge. The delta between post-test I and pretest in group B (3D-printing-based fluoroscopic coronary angiography simulator) is higher and statistically significant than the delta between post-test I and pretest in group A (conventional learning media). Moreover, the study showed that the simulator learning model is also effective as complementary to the existing conventional learning method. The delta between post-test II and pretest in group A (conventional learning media followed by 3D-printing-based fluoroscopic coronary angiography simulator) was higher and statistically significant than the delta between post-test I and pretest group A (conventional learning media only).
There are several features that support our simulator learning model as an effective coronary angiogram diagnostic learning medium. This simulator is equipped with a 3D physical structure instead of a 2D. 3D technology has the advantage of presenting 2D images in a form that allows a more profound understanding of the human anatomy structure.3 3D rendering has shown an increased understanding by medical students and clinicians of complex anatomical structures.17 The rapid growth of 3D printing created a new way of medical education.18
3D-printing-based fluoroscopic coronary angiography simulator also has the potential to enhance visuospatial abilities. Vandenberg and Kuse define visuospatial ability as the ability to mentally manipulate or rotate 3D objects in the mind.19 This ability has an essential role in medical training or for participants in surgical technique training and basic anatomy education for medical students.6,20 High visuospatial ability is associated with a person’s excellence in science, technology, mathematics, chemistry, physics, anatomy, and psychology.21 In a fluoroscopy procedure, the coronary arteries can rotate relative to other structures making identification difficult. To understand the complexity of the condition being treated, a cardiologist or interventional specialist relies on mental abilities to compile the heart’s anatomical topology from 2D to 3D images.22,23 Using structures that can be studied from various points of view, such as cadavers, plastics, or computer models, a learning method can be developed to increase spatial ability.6 This is in line with the study by Lufler et al, which states that pedagogical techniques by incorporating a rotatable anatomical model or structure can improve visuospatial abilities.7
Another benefit of the simulator is that it improves comprehension and memory. Referring to Dale’s cone experience or learning pyramid, a higher level of understanding and memory can be achieved by simulating learning activities or doing something directly (learning by doing) because it involves more senses.24 Strong evidence shows that simulation is an effective educational strategy to help health profession learners acquire basic knowledge, clinical skills and acumen, and communication skills.25
Effectiveness analysis of the 3D-printing-based fluoroscopic coronary angiography simulator (Table 2) shows that the delta between post-test II and pretest group A (9.65), is higher than the delta between post-test II and pretest group B (8.65) with no significant difference (p = 0.368). This shows that the participants in group A who had been exposed to conventional learning media plus exposure to a 3D-printing fluoroscopic coronary angiography simulator had almost identical post-test scores as participants in group B who had been exposed to a 3D-printing-based fluoroscopic coronary angiography simulator plus exposure conventional learning media. This is possible because both groups have received the same exposure.26
Analysis of other data (Table 2), in group B, the delta between post-test II and pretest (8.65), was higher than the delta between post-test I and pretest (8.53) with no significant difference (p = 0.774). This shows that in group B, participants who only received exposure to 3D-printing-based fluoroscopic coronary angiography simulators had post-test scores almost the same as post-test scores of participants exposed to 3D-printing-based fluoroscopic coronary angiography simulators plus exposure to conventional learning media. This confirms the effectiveness of the 3D-printing-based fluoroscopic coronary angiography simulator as a coronary angiogram diagnostic learning medium. In group A, the delta between post-test II and pretest was higher and statistically significant (p < 0.001) than the delta between post-test I and pretest. This indicates that participants who received conventional learning plus 3D-printing-based fluoroscopic coronary angiography simulator exposure had higher post-test scores than those who only received exposure to conventional learning media, so this further supports the effectiveness of 3D-printing-based fluoroscopic coronary angiography simulators as a coronary angiogram diagnostic learning medium.26
There are, however, some limitations of this study. A larger number of participants could be included to further improve the study. The participants in this study were only from one institution, thus a wider variation within the population might not be reflected in this study.
Conclusion
A 3D-printing-based fluoroscopic coronary angiography simulator improves the learning capability of cardiology trainees, especially in coronary angiogram diagnostics. Subsequent trials of this simulator could be carried out in several educational institutions other than the Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada.
Abbreviations
CA, coronary angiography; GLM, general linear model.
Acknowledgments
The authors are grateful to all cardiologists: Budi Yuli Setianto, Hariadi Hariawan, Nahar Taufiq, Muhammad Taufik Ismail, Hendry Purnasidha Bagaswoto, Firandi Saputra; Prattama Santoso Utomo from Department of Medical Education and Bioethics, Faculty of Medicine, Public Health, and Nursing, Universitas Gadjah Mada; Execute 3D Printing Workshop (Yogyakarta, Indonesia) for simulator manufacturing, and all radiographers and nurses from the Catheterization Laboratory at Dr. Sardjito General Hospital, Yogyakarta for their effort to help in the research. The authors thank to all who support this study.
Funding
This research was funded by “Penelitian Pengembangan Unggulan Perguruan Tinggi (PPUPT)” number 7288/UN1/DITLIT/DIT-LIT/PT/2021 from the Ministry of Education, Culture, Research and Technology of Republic Indonesia and “Rekognisi Tugas Akhir (RTA)” Program Batch I number 3550/UN1.P.III/Dit-Lit/PT.01.05/2022 from Universitas Gadjah Mada, Yogyakarta, Indonesia.
Disclosure
Dr Ganda Wibowo reports grants from Ministry of Education, Culture, Research, and Technology of Republic Indonesia, grants from Gadjah Mada University, during the conduct of the study. Dr Dyah Wulan Anggrahini, Ms Vita Arfiana Nurul Fatimah and Dr Putrika Prastuti Ratna Gharini report a patent P00202205092 pending for 3D-printing-based fluoroscopic coronary angiography simulator issued by Indonesia Directorate General of Intellectual Property. Ms Vita Arfiana Nurul Fatimah reports grants from Ministry of Education, Culture, Research and Technology of Republic Indonesia, grants from Universitas Gadjah Mada, during the conduct of the study. The author reports no other conflicts of interest in this work.
References
1. Hariawan H. Teaching Design Book of Vascular Medicine and Cardiology Department. Universitas Gadjah Mada; 2014.
2. Johnson GT. Arteriograms, venograms are angiogram territory. Chicago Tribune; January 23, 1986. Available from: https://www.chicagotribune.com/.
3. Luo H, Meyer-Szary J, Wang Z, Sabiniewicz R, Liu Y. Three-dimensional printing in cardiology: current applications and future challenges. Cardiol J. 2017;24(4):436–444. doi:10.5603/CJ.a2017.0056
4. Costello JP, Olivieri LJ, Krieger A, et al. Utilizing three-dimensional printing technology to assess the feasibility of high-fidelity synthetic ventricular septal defect models for simulation in medical education. World J Pediatr Congenit Heart Surg. 2014;5(3):421–426. doi:10.1177/2150135114528721
5. Biglino G, Capelli C, Koniordou D, et al. Use of 3D models of congenital heart disease as an education tool for cardiac nurses. Congenit Heart Dis. 2017;12(1):113–118. doi:10.1111/chd.12414
6. Garg AX, Norman G, Sperotable L. How medical students learn spatial anatomy. Lancet. 2001;357(9253):9253. doi:10.1016/S0140-6736(00)03649-7
7. Lufler RS, Zumwalt AC, Romney CA, Hoagland TM. Effect of visual-spatial ability on medical students’ performance in a gross anatomy course. Anat Sci Educ. 2012;5(1):3–9. doi:10.1002/ase.264
8. Bagai A, O’Brien S, Al Lawati H, et al. Mentored simulation training improves procedural skills in cardiac catheterization: a randomized, controlled pilot study. Circ Cardiovasc Interv. 2012;5(5):672–679. doi:10.1161/CIRCINTERVENTIONS.112.970772
9. Alharbi Y, Al-Mansour M, Al-Saffar R, Garman A, Al-Radadi A. Three-dimensional virtual reality as an innovative teaching and learning tool for human anatomy courses in medical education: a mixed methods study. Cureus. 2020. doi:10.7759/cureus.7085
10. Wainman B, Wolak L, Pukas G, Zheng E, Norman GR. The superiority of three-dimensional physical models to two-dimensional computer presentations in anatomy learning. Med Educ. 2018;52(11):1138–1146. doi:10.1111/medu.13683
11. Gharini PPR, Herianto H, Arfian N, Satria FB, Amin N. 3 dimensional printing in cardiology: innovation for modern education and clinical implementation. ACI. 2018;4(2). doi:10.22146/aci.40855
12. Mawaris K. Manufacturing and Validation of 3D-Printing-Based Fluoroscopic Coronary Angiography as Coronary Angiogram Diagnostic Learning Media. Faculty of Medicine, Public Health, And Nursing, Universitas Gadjah Mada; 2021.
13. Ferdinandus KE. Student’s Perspective on the Effectiveness of 3-Dimensional Printed Coronary Artery Learning Model as an Educational Media. Faculty of Medicine, Public Health, And Nursing, Universitas Gadjah Mada; 2020.
14. Lorello GR, Cook DA, Johnson RL, Brydges R. Simulation-based training in anaesthesiology: a systematic review and meta-analysis. Br J Anaesth. 2014;112(2):231–245. doi:10.1093/bja/aet414
15. Wong WX, Natarajan B, Yousman W, et al. Coronary angiography simulation training improves image interpretation skills of trainees independent of their stage of training. J Am Coll Cardiol. 2017;69(11):2522. doi:10.1016/s0735-1097(17)35911-9
16. Canty DJ, Hayes JA, Story DA, Royse CF. Ultrasound simulator-assisted teaching of cardiac anatomy to preclinical anatomy students: a pilot randomized trial of a three-hour learning exposure. Anat Sci Educ. 2015;8(1):21–30. doi:10.1002/ase.1452
17. Peterson DC, Mlynarczyk GSA. Analysis of traditional versus three-dimensional augmented curriculum on anatomical learning outcome measures. Anat Sci Educ. 2016;9(6):529–536. doi:10.1002/ase.1612
18. Garcia J, Yang ZL, Mongrain R, Leask RL, Lachapelle K. 3D printing materials and their use in medical education: a review of current technology and trends for the future. BMJ Simul Technol Enhanc Learn. 2018;4(1):27–40. doi:10.1136/bmjstel-2017-000234
19. Vandenberg SG, Kuse AR. Mental rotations, a group test of three-dimensional spatial visualization. Percept Mot Skills. 1978;47(2):599–604. doi:10.2466/pms.1978.47.2.599
20. Wanzel KR, Hamstra SJ, Anastakis DJ, Matsumoto ED, Cusimano MD. Effect of visual-spatial ability on learning of spatially-complex surgical skills. Lancet. 2002;359(9302):9302. doi:10.1016/S0140-6736(02)07441-X
21. Uttal DH, Meadow NG, Tipton E, et al. The malleability of spatial skills: a meta-analysis of training studies. Psychol Bull. 2013;139(2):352–402. doi:10.1037/a0028446
22. Valverde I. Three-dimensional printed cardiac models: applications in the field of medical education, cardiovascular surgery, and structural heart interventions. Revista Española de Cardiología. 2017;70(4). doi:10.1016/j.rec.2017.01.012
23. Fernandez R, Dror IE, Smith C. Spatial abilities of expert clinical anatomists: comparison of abilities between novices, intermediates, and experts in anatomy. Anat Sci Educ. 2011;4(1):1–8. doi:10.1002/ase.196
24. Masters K. Edgar Dale’s pyramid of learning in medical education: a literature review. Med Teach. 2013;35(11):e1584–e1593. doi:10.3109/0142159X.2013.800636
25. Alinier G, Platt A. International overview of high-level simulation education initiatives in relation to critical care. Nurs Crit Care. 2014;19(1):42–49. doi:10.1111/nicc.12030
26. Wibowo G. Effectiveness of a 3D-Printing-Based Fluoroscopic Coronary Angiography Simulator as a Coronary Angiogram Diagnostic Learning Media. Faculty of Medicine, Public Health, And Nursing, Universitas Gadjah Mada; 2022.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.