Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Zero-Balance Ultrafiltration Reduces Postoperative Delirium After Cardiac Surgery with Cardiopulmonary Bypass: A Randomized Controlled Trial
Authors Lan X, Tang S, Lu J, Tang G, Shao Y, Zhu Z ![]() , Zhou K, Xiong X, Chen D, Shi J
, Zhou K, Xiong X, Chen D, Shi J ![]()
Received 25 September 2025
Accepted for publication 11 December 2025
Published 23 December 2025 Volume 2025:21 Pages 1807—1819
DOI https://doi.org/10.2147/TCRM.S570006
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sandeep Ajoy Saha
Xin Lan,1,2,* Sijie Tang,1,* Jun Lu,1 Guangling Tang,1 Yi Shao,1 Zhenyan Zhu,1 Kun Zhou,1 Xinglong Xiong,1 Dongxu Chen,3,4,* Jing Shi1,*
1Department of Anesthesiology, The Affiliated Hospital of Guizhou Medical University, Guiyang, People’s Republic of China; 2Department of Anesthesiology, The Second Affiliated Hospital of Guizhou University of Traditional Chinese Medicine, Guiyang, People’s Republic of China; 3Department of Anesthesiology, West China Second Hospital, Chengdu, People’s Republic of China; 4Key Laboratory of Birth Defects and Related Diseases of Women and Children, Sichuan University, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Shi, Department of Anesthesiology, The Affiliated Hospital of Guizhou Medical University, Guiyang, People’s Republic of China, Tel +86-18685034016, Email [email protected] Dongxu Chen, Department of Anesthesiology, West China Second Hospital, Sichuan University, Chengdu, People’s Republic of China, Tel +86-15881730901, Email [email protected]
Purpose: To assess the effects of conventional ultrafiltration and conventional plus zero-balanced ultrafiltration on delirium and cognition in patients undergoing cardiac surgery with cardiopulmonary bypass (CPB).
Methods: A total of 116 adults who were scheduled for cardiac surgery with CPB were randomly assigned to the conventional ultrafiltration group or the conventional plus zero-balanced ultrafiltration group. CPB was managed with standard protocols. In the conventional ultrafiltration group, ultrafiltration began during the rewarming phase and was performed until the CPB was terminated. In another group, perfusionists conducted zero-balance ultrafiltration after aortic cross-clamping and began conventional ultrafiltration during the rewarming phase. The primary outcome was the incidence of postoperative delirium (POD) within 7 days; the secondary outcome was postoperative cognitive dysfunction (POCD) at 1 and 3 months. In addition, the patients’ vital signs and postoperative complications at different points during the operation were also recorded.
Results: During the first 7 postoperative days, POD was observed in 12 patients in the zero-balance ultrafiltration group and 27 patients in the conventional ultrafiltration group (12/53 [22.64%] vs 27/53 [50.94%]; RR 0.45, 95% CI 0.25 to 0.78; P = 0.005). At 1 month after surgery, POCD occurred in 12 patients in the zero-balance ultrafiltration group versus 18 patients in the conventional ultrafiltration group (12/53 [22.64%] vs 18/53 [33.96%]; RR = 0.67; 95% CI 0.36– 1.24; P = 0.281). By 3 months postoperatively, postoperative cognitive dysfunction occurred in 4 patients in the zero-balance ultrafiltration group and 7 patients in the conventional ultrafiltration group (4/53 [7.55%] vs 7/53 [13.21%]; RR = 0.57; 95% CI 0.18– 1.84; P = 0.524).
Conclusion: In patients who underwent cardiac surgery with CPB, zero-balance ultrafiltration significantly reduced the incidence of delirium compared with conventional ultrafiltration alone within the first 7 postoperative days. In contrast, the incidence of cognitive dysfunction did not differ significantly between the two groups at 1 or 3 months postoperatively.
Keywords: ultrafiltration, cardiopulmonary bypass, cardiac surgery, delirium, cognitive function
Introduction
Cognitive impairment occurring after cardiac surgery is mainly manifested as two distinct clinical phenomena whose mechanisms partially overlap: post-operative delirium (POD) and post-operative cognitive dysfunction (POCD).1 POD is associated with an increased risk prolonged hospitalization, compromised rehabilitation, and diminished quality of life, thereby imposing a greater burden on healthcare systems and raising mortality.2 The incidence of POD is closely related to the type of surgery, with cardiac surgery often having a greater incidence of POD than noncardiac surgery. POD occurs in up to one-third of elderly patients undergoing complex cardiac surgery.3,4 Although POD was identified more than half a century ago in cardiac surgery, strategies to prevent and control this condition have remained very limited until now.
Although the specific mechanism underlying POD in cardiac surgery has not been clarified, an increasing number of studies have suggested that the neuroinflammatory response is a key factor in its occurrence and development.5,6 On the one hand, inflammation can directly or indirectly stimulate glial cells to release inflammatory factors, resulting in inflammation of the central nervous system. Additionally, inflammation can increase the permeability of the blood–brain barrier, consequently inducing postoperative cognitive dysfunction.7–9 Cardiopulmonary bypass (CPB), a nonphysiological blood circulation method, involves the circulation of blood through a pipeline, membrane oxygenator, and other materials that come into contact with human blood. This process leads to the release of many inflammatory factors, including TNF-α, IL-6, IL-1β, and C-reactive protein (CRP). These factors disrupt the blood‒brain barrier and contribute to neuroinflammation. Therefore, CPB may be among the most closely associated risk factors for POD.10–12
Ultrafiltration is a technique commonly used during CPB for volume management and the filtration of blood to reduce harmful components. Ultrafiltration techniques that are commonly employed include conventional, modified, and zero-balanced ultrafiltration.13 Conventional ultrafiltration is primarily utilized to remove excess water from the circulating blood after blood dilution for CPB, concentrate the blood, and increase hematocrit levels. However, it has an extremely weak ability to filter out inflammatory factors. Compared with conventional ultrafiltration, modified ultrafiltration is superior because it yields higher hematocrit levels and mean arterial blood pressures, but it is performed after the termination of CPB. Modified ultrafiltration may prolong the duration of surgery; high blood flow rates through the ultrafilter are often used to decrease the duration of modified ultrafiltration, but the resulting rapid withdrawal of blood from the aortic cannula at high flow rates has negative consequences. Therefore, this strategy is used mainly for pediatric cardiac surgery in clinical practice.14,15 Zero-balance ultrafiltration enables continuous ultrafiltration throughout the CPB process, with its primary focus on the effective filtration of inflammatory mediators rather than mere fluid removal. Its core mechanism for reducing inflammatory mediators relies on a dynamic cycle of “continuous filtration-separation plus equal-volume replacement”, enabling the selective clearance of small-molecule inflammatory mediators without compromising hemodynamic stability.16 Existing studies have confirmed the effectiveness of Z-BUF in clearing inflammatory mediators. Among them, studies in the pediatric population have demonstrated that it can reduce the risk of postoperative organ dysfunction by clearing inflammatory factors.17 Although Z-BUF is widely applied for volume control in pediatric CPB, its use in adults remains limited to select centers. To our knowledge, no adult randomized trial has examined the effect of Z-BUF on delirium incidence: current research has only focused on the effects of Z-BUF on inflammatory cytokine removal or protective effects on organ functions such as respiratory function.18,19
We therefore formulated the following primary hypothesis: Among patients undergoing cardiac surgery with CPB, combining zero-balance ultrafiltration with conventional ultrafiltration decreases the occurrence of delirium within the first 7 postoperative days compared with conventional ultrafiltration alone. Our study, which employed a single-blinded randomized controlled design, aimed to compare the effects of two extracorporeal circulation protocols—conventional ultrafiltration versus conventional ultrafiltration combined with zero-balance ultrafiltration—on the incidence of delirium within 7 days post-operatively and on the incidence of cognitive function at 1 and 3 months post-operatively in patients undergoing cardiac surgery to explore the specific role of zero-balance ultrafiltration in postoperative cognition-related outcomes.
Materials and Methods
Study Design
This study was conducted in accordance with the principles of the World Medical Association Declaration of Helsinki. It was approved by the Medical Science Ethics Committee of the Affiliated Hospital of Guizhou Medical University [No. 2022(476)] and registered with the Chinese Clinical Trial Registry (www.chictr.org.cn; identifier: ChiCTR2200061269). The study was reported following the Consolidated Standards of Reporting Trials guidelines. All participants provided written informed consent.
Patients
We enrolled patients who fulfilled specific criteria based on their medical history and examination instructions. The inclusion criteria were as follows: age ≥ 18 years, undergoing cardiac surgery with CPB, American Society of Anesthesiologists (ASA) III or IV, New York Heart Association (NYHA) classification II or III, and ability to participate in neuropsychological tests and follow-up.
Patients were excluded if they had the following conditions: a history of neurological or psychiatric disorders, such as dementia or language disorders; the use of extracorporeal membrane oxygenation before or after surgery for any reason; poor cardiac repolarization or the need for a second surgery; severe intraoperative hemodynamic disorders or malignant arrhythmia; death within 24 h.
Randomization and Masking
After the designated anesthesiologist completed the preoperative screening and baseline evaluation, the researcher responsible for grouping used a random number table to randomly divide the patients into two groups at a 1:1 ratio: the conventional ultrafiltration group or the zero-balance ultrafiltration combined with conventional ultrafiltration group. When the patient arrived in the operating room, the researcher handed the sealed envelope containing the patient’s random number and corresponding ultrafiltration protocol to the perfusionist. The perfusionist was solely responsible for implementing the assigned ultrafiltration strategy and was instructed not to disclose the group information to other members of the surgical team. The researchers responsible for grouping were not involved in anesthesia management, surgical procedures, or data collection. Patients, researchers responsible for data recording, postoperative follow-up personnel, and statisticians remained unaware of the grouping throughout the study. In addition, the perfusionists, anesthesiologists or surgeons were not involved in the postoperative follow-up of the patients.
CPB Management
Cardiopulmonary bypass was performed using a Sorin Stockert S5 heart-lung machine (Sorin Stockert Instrument GMBH, Germany) equipped with a centrifugal blood pump and a heater-cooler unit. A nonpulsatile CPB technique was adopted. The priming volume was 2000 mL of solution with a crystalloid-colloid ratio of 0.6:1; the crystalloid was lactated Ringer’s solution and the colloid was hydroxyethyl starch 130/0.4. During CPB, heparin was initially administered intravenously at 300–400 U/kg to maintain an activated clotting time (ACT) above 480 s. The ACT was monitored every 30 minutes, and an additional 50–100 U/kg heparin was given if it was below 480 s. Myocardial protection was achieved by antegrade perfusion of 4 °C Del Nido solution through the aortic root, with an initial perfusion dose of 10–20 mL/kg. A half dose was added when the aortic cross-clamp time exceeded 60 minutes.
During CPB, the body temperature was maintained at mild to moderate hypothermia (28–35 °C). During the rewarming phase, the temperature was increased at a rate of 0.5–1 °C/min until the nasopharyngeal temperature exceeded 36 °C. The initial pump flow was calculated based on the patient’s body surface area (formula: 2.4–2.8 L/(min·m2)) and adjusted according to circulatory indicators: When the mean arterial pressure (MAP) was below 60 mmHg, norepinephrine was intravenously pumped at a dose of 0.05–0.2 μg/kg/min; when the MAP was above 80 mmHg, 0.5–2 μg/kg/min nitroglycerin was administered to maintain the MAP between 60–80 mmHg. Moreover, the regional cerebral oxygen saturation (rcSO2) was maintained above 50%, the urine output was between 1 and 2 mL/(kg·h) (0.5–1 mg/kg furosemide was given when the urine output was insufficient), and the base excess was between −3 and 3 mmol/L (managed by the α-stat method; 1–2 mmol/kg sodium bicarbonate was intravenously infused when the base excess was < −3 mmol/L).
Ultrafiltration [Sorin Ultrafiltration Module: Hemoconcentrator, DHF06, Polyethersulfone (PES) Fiber Membrane, Italy] was conducted with a blood flow rate of 100–200 mL/min and a transmembrane pressure maintained at 100–200 mmHg. After the patient was weaned off CPB, protamine was intravenously infused at a ratio of 1:1 to the total heparin dose, and 2 g of tranexamic acid was administered to restore the ACT to the preoperative baseline value of ±20 s.
Interventions
In the conventional ultrafiltration group, ultrafiltration began during the rewarming phase and was performed until the CPB was terminated. In the zero-balance group, perfusionists conducted zero-balance ultrafiltration after aortic cross-clamping and began conventional ultrafiltration during the rewarming phase. To ensure the effectiveness of the zero-balance ultrafiltration volume, a dosage of 35 mL/kg was selected. This approach successfully reduced the presence of postoperative inflammatory factors and procalcitonin levels while preventing severe water and electrolyte imbalances and the destruction of red blood cells.20
Perioperative Management
Routine vital signs were monitored upon the patients arriving in the operating room. Left radial artery puncture and catheterization were performed under local anesthesia to monitor invasive arterial pressure before anesthesia induction. The induction medications used were midazolam (0.03 mg/kg), etomidate (0.3 mg/kg), sufentanil (0.5–1 µg/kg), and rocuronium (0.6 mg/kg). Following induction, mechanical ventilation was initiated through tracheal intubation, followed by central venous puncture and catheterization. The maintenance medications used were sevoflurane (0.7–1.0 MAC), remifentanil (0.2–0.3 μg·kg·min−1), propofol (4–6 mg·kg·min−1), and dexmedetomidine (0.3–0.5 μg·kg·h−1).
The depth of anesthesia was adjusted based on the intensity of surgical stimulation. Intraoperative routine monitoring included the following: maintaining the MAP between 60 and 80 mmHg, maintaining the SPO2 level above 95%, and maintaining the rcSO2 above 50%. Regular blood gas analysis was conducted to ensure proper adjustment of the internal environment. All patients received autologous blood transfusions. Red blood cell transfusions were considered for patients with a hematocrit of less than 21% during CPB or less than 24% during surgery.
Study Outcomes
The primary outcome was the incidence of POD, as indicated by a positive evaluation using either the Confusion Assessment Method (CAM) or the Confusion Assessment Method for intensive care units (CAM-ICU). Delirium was assessed twice daily, specifically between 8 and 10 am and again between 8 and 10 pm, during the first 7 postoperative days, until hospital discharge or death, whichever occurred first. Patients with delirium were classified into three subtypes: hyperactive (Richmond Agitation Sedation Scale score consistently positive, from +1 to +4), hypoactive (Richmond Agitation Sedation Scale score consistently neutral or negative, from –3 to 0), and mixed.21
The secondary outcomes included the evaluation of cognitive function using the Mini-Mental State Examination, with scores ranging from 0 to 30. Higher scores indicate better cognitive function.22 The MMSE was conducted in consulting rooms with a quiet environment, appropriate lighting, and freedom from distractions. Notably, all CAM/MMSE assessments were performed by 3 trained physicians who were blinded to group assignments and had completed professional operational training at the Department of Psychology.
We recorded the occurrence of postoperative complications, including postoperative pneumonia, pleural effusion, and acute kidney injury, according to the European Perioperative Clinical Outcome (EPCO) Definitions.23 Details of these definitions are provided in the Supplementary materials. In addition, we recorded the duration of mechanical ventilation, the length of intensive care unit stay, and the length of postoperative hospital stay.
Statistical Analyses
Based on the results of preliminary pilot study conducted by our team, the baseline incidence of POD in patients who underwent cardiac surgery was 45%. Considering clinical relevance, the minimum clinically significant difference in POD incidence between the two groups was 25%. The statistical parameters were defined as follows: type I error probability (α) = 0.05 and statistical power (1-β) = 0.80. With the use of PASS software, the required sample size was calculated to be 53 patients per group. Accounting for a 10% dropout rate, the final sample size was determined to be 58 patients per group.
The normality of the distribution of continuous variables was tested by visually inspecting histograms and quantile‒quantile (Q‒Q) plots, combined with the Shapiro‒Wilk test. Data with a normal distribution are presented as the mean (standard deviation), whereas data with a skewed distribution are presented as the median (interquartile range, IQR). Intergroup differences in baseline characteristics were compared using the absolute standardized difference, and differences >1.96  were considered imbalanced.24 In this study, absolute standardized differences >0.38 were considered imbalanced.
were considered imbalanced.24 In this study, absolute standardized differences >0.38 were considered imbalanced.
Our primary outcome was the incidence of POD within 7 days, defined as a patient experiencing at least one episode of delirium during this period (regardless of the number of episodes). Comparisons of this binary outcome between groups were performed using the chi-square test. Patients whose data were missing because of early hospital discharge or death (N=1) were excluded from the final analyses. The effects of zero-balance ultrafiltration on the incidence of POD are presented as relative risk (RR) and 95% confidence intervals (CIs). The same methodology was applied to analyze other categorical outcomes. Exploratory analyses were performed to assess differences in the primary outcome in predefined subgroups, including age (≤60 years or >60 years), sex (female or male), ASA physical status (III or IV), NYHA class (II or III), duration of surgery (≤4 hours or >4 hours), and CPB duration (≤2 hours or >2 hours). Treatment-by-covariate interactions were assessed separately for each subgroup factor using logistic regression. We did not use the Bonferroni correction for the subgroup analyses.
The MMSE was administered at 1 month and 3 months post-operatively to evaluate both short-term and medium-term cognitive function, as these time points align with key stages of postoperative recovery and are clinically meaningful for assessing cognitive trajectory. For the MMSE scores at 1 and 3 months after surgery, group comparisons were performed using a generalized estimating equation (GEE) approach, with the intervention group and time (1 and 3 months after surgery) included as fixed effects. An unstructured working correlation matrix was specified to account for within-participant correlations over time. Aggregated MMSE scores across all time points were reported separately by group, with contrasts for between-group differences and 95% confidence intervals (CIs) provided. To mitigate the risk of inflating Type I error associated with multiple assessments, a Bonferroni correction was implemented, with the significance level adjusted to α = 0.025 for all MMSE-related analyses.
Intergroup differences in the length of stay in the intensive care unit and hospital stay were assessed using the Mann‒Whitney U-test and by calculating the Hodges–Lehman median difference with 95% CI.
Results
Baseline Characteristics
Between July 2022 and November 2022, a total of 183 patients were screened for inclusion. Of these, 116 were eligible, enrolled and randomly assigned to either the zero-balance ultrafiltration group (n = 58) or the conventional ultrafiltration group (n = 58). Among the enrolled patients, 6 were excluded because surgery was cancelled, and 4 patients were excluded because of missing data (n = 1) or because they withdrew consent (n = 3); thus, 106 patients were included in the analyses (Figure 1b). The demographic and baseline variables were well balanced between the two groups (Table 1). In addition, surgery type, duration of surgery, duration of CPB, transfusion therapy, heart recovery, or Dexmedetomidine dosage did not significantly differ between the two groups (supplemental Table 1). The total amount of liquid filtered out by ultrafiltration in the zero-balance ultrafiltration group was significantly greater than that in the conventional ultrafiltration group (2158 mL vs 1122 mL), and the total amount of crystal liquid used during CPB in the zero-balance ultrafiltration group was significantly greater than that in the conventional ultrafiltration group (3300 mL vs 2200 mL); the amount of component blood transfusion volume, autologous blood transfusion volume, or urine volume did not significantly differ between the two groups. In addition, there was no significant difference in the comparison of vital signs at each intraoperative time point between the two groups (Supplemental Figure 1).
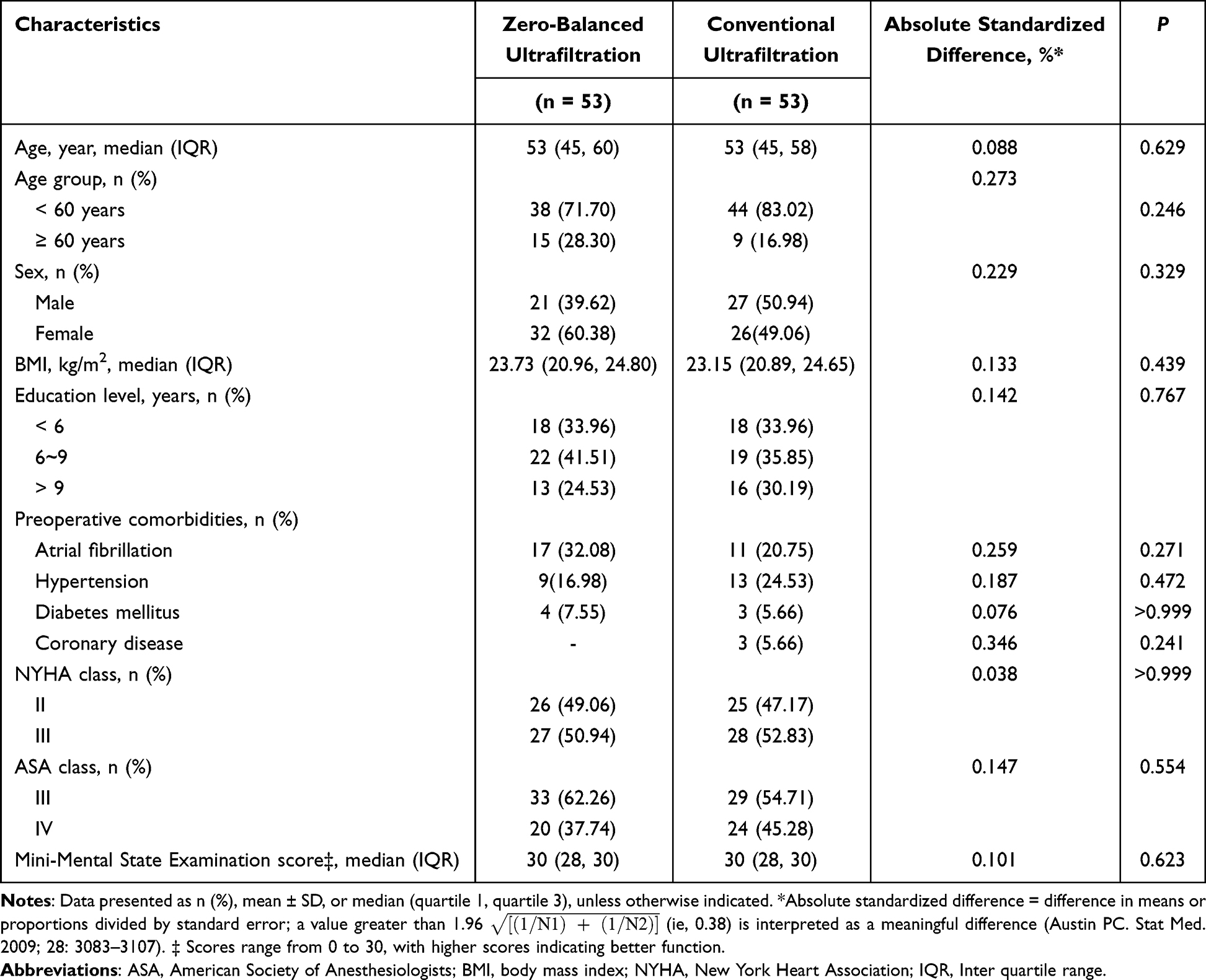 |
Table 1 Baseline Characteristics |
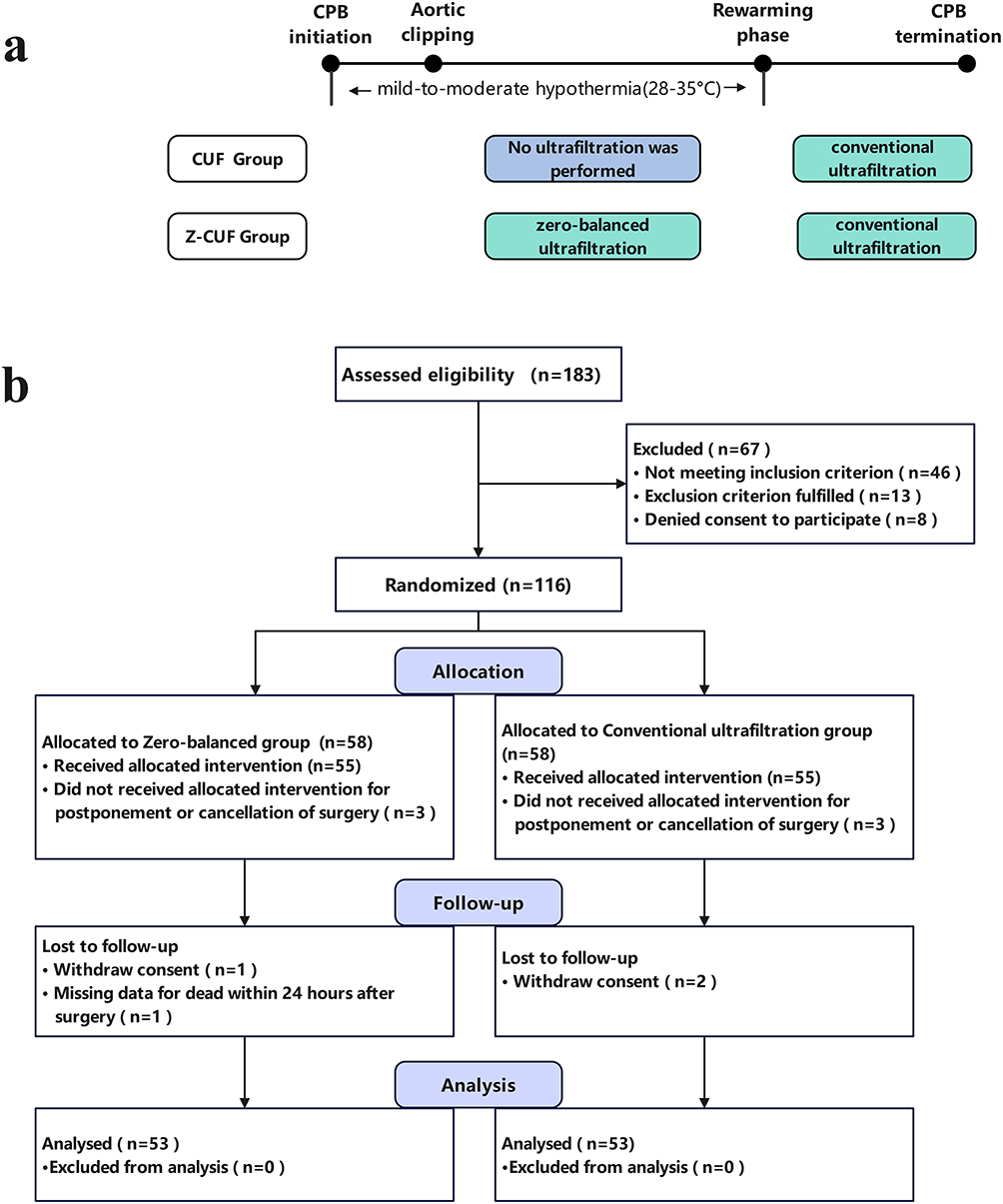 |
Figure 1 Flow chart. (a) Time frame; (b) Enrollment. Abbreviations: CPB, Cardiopulmonary bypass; CUF, conventional ultrafiltration; Z-CUF, zero-balance ultrafiltration combined with conventional ultrafiltration. |
Primary Outcome
The incidence of POD was significantly lower in patients who received zero-balance ultrafiltration than in those who received conventional ultrafiltration (12/53 [22.64%] vs 27/53 [50.94%]; RR 0.45, 95% CI 0.25 to 0.78; P = 0.005; Table 2). The absolute risk reduction with zero-balance ultrafiltration was 28%, corresponding to a number needed to treat of 4. All three subtypes of delirium were significantly less common in the zero-balance ultrafiltration group (Table 2). No significant interactions were identified between the treatment group and predefined factors (Figure 2). Additionally, among patients in the zero-balance ultrafiltration group, 6 (11.32%) experienced two or more episodes of delirium. In contrast, in the conventional ultrafiltration group, 19 out of 53 patients (35.84%) had two or more episodes of delirium (RR 0.32, 95% CI 0.14 to 0.73; P = 0.006). In terms of medication usage for controlling delirium, 7 out of 53 patients (13.21%) in the zero-balance ultrafiltration group received treatment, whereas 12 out of 53 patients (22.64%) in the conventional ultrafiltration group received treatment (RR 0.58, 95% CI 0.25 to 1.37; P = 0.311).
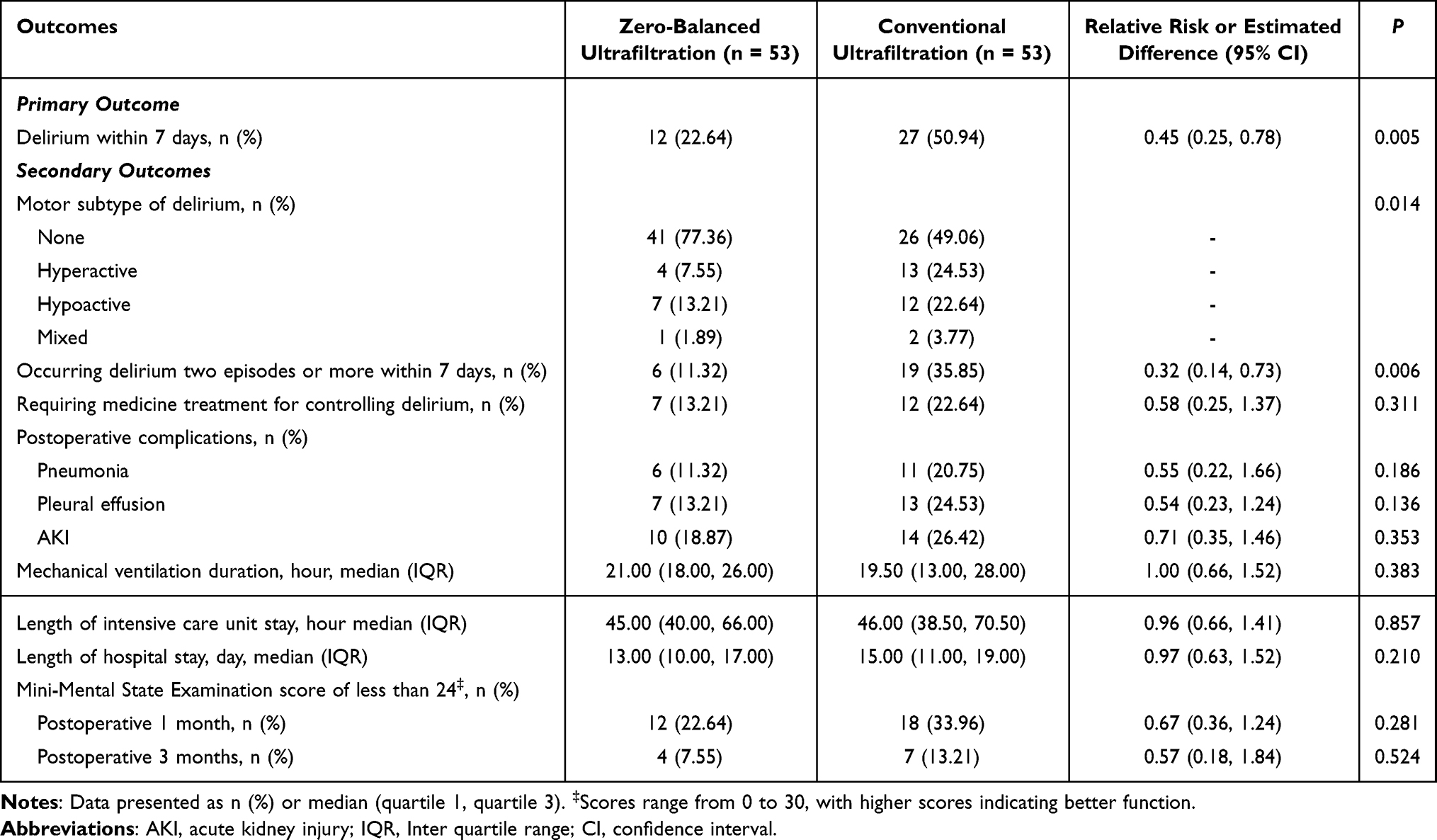 |
Table 2 Primary and Secondary Outcome |
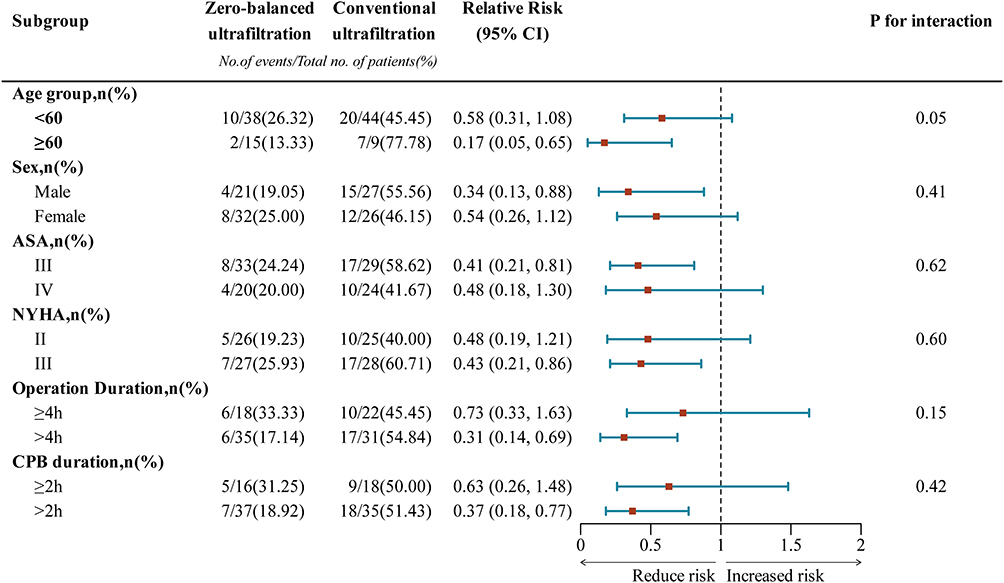 |
Figure 2 Estimated effect of the ultrafiltration mode on POD by prespecified subgroups. Abbreviations: NYHA, New York Heart Association; ASA, American Society of Anesthesiologists. |
Long-Term Cognition Follow-Up
No significant differences in MMSE scores were observed between the two groups at 1 month (differences in means = 0.99, 95% CI −0.57 to 2.56; P = 0.214; Supplemental Table 2) or 3 months (differences in means = 0.57, 95% CI −4.03 to 1.56; P = 0.248) after surgery. Similarly, no significant difference was found in the incidence of MMSE scores less than 24 at 1 month (P = 0.281) or 3 months (P = 0.524) after surgery.
Postoperative Complications
The incidences of postoperative pneumonia (6/53 [11.32%] vs 11/53 [20.75%]; RR 0.55; 95% CI 0.22 to 1.66; P = 0.186; Table 2), pleural effusion (7/53 [13.21%] vs 13/53 [24.53%]; RR 0.54; 95% CI 0.23 to 1.24; P = 0.136), and acute kidney injury (10/53 [18.87%] vs 14/53 [26.42%]; RR 0.71; 95% CI 0.35 to 1.46; P = 0.353) did not significantly differ between the two groups. The duration of mechanical ventilation, length of intensive care unit stay, and length of hospital stay did not differ between the two groups (Table 2).
Discussion
Our study investigated the effect of the ultrafiltration mode on postoperative cognitive function in patients who underwent cardiac surgery with CPB. Our findings revealed that the combination of zero-balance ultrafiltration and conventional ultrafiltration significantly reduced the risk of POD in these patients. This reduction was consistent across all three motoric subtypes of delirium, and was similar in all pre-defined subgroups, except for the POD subgroup that required drug treatment. Importantly, the observed treatment effect was substantial and highly statistically significant, with the incidence of POD among those treated with combined ultrafiltration being only approximately half that of patients treated with conventional ultrafiltration. However, we noted that combined ultrafiltration did not significantly affect the MMSE score at 1 month or 3 months after surgery.
The incidence of POD in cardiac surgery can range from 16%~73%, and POD severely affects the postoperative rehabilitation of patients undergoing cardiac surgery. Increasing evidence suggests that central nervous system inflammation and the peripheral inflammatory response may play a role in the development of POD during cardiac surgery with CPB.25 Peripheral inflammatory factors disrupt the blood‒brain barrier, leading to increased concentrations of central inflammatory factors and ultimately resulting in central nervous system inflammation, which has been linked to an increased incidence of POD.26,27 Some scholars have pointed out that dexmedetomidine has a neuroprotective effect and can reduce the incidence of POD in patients undergoing cardiac surgery.28 Therefore, dexmedetomidine was incorporated as one of the standard anesthetic agents in our study, and no statistically significant difference was observed in its dosage between the two groups. In terms of the ultrafiltration strategy of CPB, zero-balance ultrafiltration seems to be better at decreasing inflammatory responses to prevent pulmonary injury and bypass circuit; however, few studies have investigated the effects of different ultrafiltration methods on postoperative cognitive function. M. de Baar’s research revealed that zero-balance ultrafiltration did not reduce the incidence of early neurocognitive disorder, but the methodological shortcomings of existing investigations include small sample sizes or restrictions to patients with certain surgery types (eg, elective coronary artery bypass grafting surgery)19 and insufficient efforts to identify the effect of zero-balance ultrafiltration on the development of POD. In our study, the overall incidence of POD after cardiac surgery with CPB was 36.79%, which was consistent with the incidence of POD reported in previous studies of cardiac surgery with CPB. Our study included different types of patients who underwent cardiac surgery with CPB, and the sample size was also larger than those in previous studies, which may explain our positive results. Specifically, we found that zero-balance ultrafiltration reduced the incidence of POD compared with conventional ultrafiltration. Additionally, we assessed the difference in the motor subtypes of delirium, and our results revealed that the incidences of hyperactive delirium and two or more episodes of delirium were significantly lower in the zero-balance ultrafiltration group than in the conventional ultrafiltration group.
Embolization and cerebral hypoperfusion may be related to cognitive dysfunction in patients who underwent cardiac surgery with CPB.29–31 Moreover, the systemic inflammatory response (SIRS) caused by the CPB procedure may play an important role in the etiology of postoperative cognitive dysfunction. The inflammatory response results from the exposure of blood to foreign surfaces of the CPB circuit.32 Therefore, improving CPB techniques can suppress the inflammatory response, which may be of clinical value for reducing the incidence of brain dysfunction. Ultrafiltration is a technique commonly used during CPB for volume management and/or the filtration of blood to reduce deleterious components.33 Compared with efforts to reduce bleeding and remove fluid, conventional ultrafiltration appeared to result in superior cardiac function.13 Zero-balance ultrafiltration seems to decrease inflammatory responses to prevent acute pulmonary injury and the bypass circuit.17 However, its postoperative clinical benefits have not been consistently reported. In a prospective study of pediatric cardiac surgery, counterfactual analysis confirmed that continuous ultrafiltration can only significantly remove the complement fragment C3a, with an overall weak anti-inflammatory effect,34 which is contrary to previous studies. This discrepancy may be related to differences in study populations, combined ultrafiltration strategies, and sample sizes. Furthermore, the type of ultrafiltration that might yield optimal postoperative outcomes is unclear. In our study, zero-balance ultrafiltration combined with conventional ultrafiltration reduced the incidence of POD, and various mechanisms may contribute to this effect. First, zero-balance ultrafiltration combined conventional ultrafiltration can more effectively remove excess fluid more optimally and maintain cerebral perfusion during CPB, thereby reducing adverse clinical events. Second, zero-balance ultrafiltration and conventional ultrafiltration during CPB could reduce the concentration of serum inflammatory mediators and stabilize vascular endothelium, which is an important cause of neuroinflammation, an underlying mechanism of POD in cardiac surgery.
In the subgroup of patients with POD requiring medication treatment, the zero-balance ultrafiltration group showed a downward trend compared to the conventional ultrafiltration group, but this difference was not statistically significant (7/53 [13.21%] vs 12/53 [22.64%]; RR 0.58; 95% CI 0.25 to 1.37; P = 0.311). Based on our current clinical observations, most patients developed the symptoms within 1–2 days postoperatively. While some patients achieved spontaneous recovery, only those with severe symptoms and prolonged duration were referred to the psychology department for consultative evaluation and medication guidance. Consequently, although the incidence of POD in the zero-balance ultrafiltration group exhibited a decreasing trend, the total number of clinical interventions was relatively limited, resulting in no statistically significant difference between the groups.
Prior studies have demonstrated an association between POD and the subsequent risk of POCD in elderly patients undergoing cardiac surgery.35,36 However, a recent study revealed that POD is independently associated with cognitive decline 1 month after surgery, but such an association was not observed at postoperative year 1.37 Therefore, whether POD increases the risk of POCD is unclear. Although the MMSE scores or the incidences of an MMSE scores of less than 24 at 1 month (P = 0.281) or 3 months (P = 0.524) after surgery did not significantly differ between the two groups in our study, the MMSE scores were lower in the zero-balance ultrafiltration group than in the conventional ultrafiltration group at 1 month (12/53 [22.64%] vs 18/53 [33.96%]; RR 0.67; 95% CI 0.36 to 1.24; P = 0.281) and 3 months (4/53 [7.55%] vs 7/53 [13.21%]; RR 0.57; 95% CI 0.18 to 1.84; P = 0.524). The above results were attributed to several reasons. On the one hand, we calculated the sample size based on the incidence of POD, which may have led to an insufficient sample size for the evaluation of the MMSE scores; although differences and decreases in incidence were observed, these changes were not significant. On the other hand, cognitive function gradually recovered as the follow-up time was extended, leading to a decrease in the incidence of an MMSE score of less than 24 in both groups. Additionally, although the MMSE is widely used in clinical settings to rapidly screen global cognitive status, it is not designed to assess specific cognitive domains (such as memory, attention, and executive function) in detail. Because our study focused on short-term POD prevention and included only MMSE assessments at 1 and 3 months post-operatively, without concurrent delirium evaluations using tools such as the CAM, our ability to link long-term cognitive trends with early delirium outcomes is limited. Therefore, the findings regarding postoperative cognitive changes should be interpreted with caution. Future research should employ comprehensive psychometric assessments alongside synchronized delirium evaluations to better characterize the nature and extent of postoperative cognitive changes, thereby strengthening the connection between short-term preventive strategies and long-term cognitive outcomes.
This study was subject to several limitations. First, this work was a single-center study, and the results may not be generalizable. Second, our study included only patients aged 18 to 65 years, and the reference values for individuals who exceeded this range were limited. Third, the bispectral index was used in this study only as a reference indicator and was not included in the statistical analysis because its monitoring range lacks exact guidelines for the cardiac surgery population. Moreover, the degree of brain edema in the two groups was not determined by MRI and other means in this study, which may also be the potential mechanism of POD in patients with CPB. In addition, the subgroup analyses in this study, including those of the delirium subgroups, were not prespecified in the trial registration and should therefore be regarded as exploratory. Moreover, owing to multiple comparisons, the results may be susceptible to Type I error. Consequently, the findings from these subgroup analyses should be interpreted with caution, and their validity needs to be confirmed in future studies with predefined subgroup hypotheses.
Conclusion
In summary, the addition of zero-balance ultrafiltration to conventional ultrafiltration during CPB significantly reduced the incidence of POD. Although no significant differences were observed in the risk of postoperative delirium requiring treatment and short-term cognitive scores, these results highlight the potential of perfusion-based strategies to improve neurocognition after cardiac surgery. Larger, multicenter trials with longer follow-up are warranted to confirm these findings and evaluate their impact on long-term cognitive outcomes.
Data Sharing Statement
The corresponding author will provide the data on reasonable request.
Ethics Approval and Informed Consent
This study was conducted in accordance with the principles of the World Medical Association Declaration of Helsinki. This study was approved by the Medical Science Ethics Committee of the Affiliated Hospital of Guizhou Medical University [No. 2022(476)] and registered with the Chinese Clinical Trial Registry (www.chictr.org.cn; identifier: ChiCTR2200061269). The study was reported following the Consolidated Standards of Reporting Trials guidelines. All participants provided written informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China [grant number 82560234], the outstanding reserve talents in the discipline of Affiliated Hospital of Guizhou Medical University in 2023 (gyfyxkrc-2023-15), the science and technology plan project of Guizhou province (ZK (2022) General 414) and the science and technology plan project of Guizhou province [ZK (2023)- General 390].
Disclosure
Jing Shi is the first correspondence author for this study. The authors report no conflicts of interest in this work. An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
References
1. Majewski P, Zegan-Baranska M, Karolak I, et al. Current evidence regarding biomarkers used to aid postoperative delirium diagnosis in the field of cardiac surgery-review. Medicina. 2020;56(10):493. doi:10.3390/medicina56100493
2. O’Gara BP, Mueller A, Gasangwa DVI, et al. Prevention of early postoperative decline: a randomized, controlled feasibility trial of perioperative cognitive training. Anesth Analg. 2020;130(3):586–595. doi:10.1213/ane.0000000000004469
3. Djaiani G, Silverton N, Fedorko L, et al. Dexmedetomidine versus propofol sedation reduces delirium after cardiac surgery: a randomized controlled trial. Anesthesiology. 2016;124(2):362–368. doi:10.1097/aln.0000000000000951
4. Lei L, Katznelson R, Fedorko L, et al. Cerebral oximetry and postoperative delirium after cardiac surgery: a randomised, controlled trial. Anaesthesia. 2017;72(12):1456–1466. doi:10.1111/anae.14056
5. Alam A, Hana Z, Jin Z, Suen KC, Ma D. Surgery, neuroinflammation and cognitive impairment. EBioMedicine. 2018;37:547–556. doi:10.1016/j.ebiom.2018.10.021
6. Kawano T, Yamanaka D, Aoyama B, et al. Involvement of acute neuroinflammation in postoperative delirium-like cognitive deficits in rats. J Anesth. 2018;32(4):506–517. doi:10.1007/s00540-018-2504-x
7. Zhang XP, Liu YR, Chai M, et al. High‑fat treatment prevents postoperative cognitive dysfunction in a hyperlipidemia model by protecting the blood‑brain barrier via Mfsd2a‑related signaling. Mol Med Rep. 2019;20(5):4226–4234. doi:10.3892/mmr.2019.10675
8. Steinmetz J, Christensen KB, Lund T, Lohse N, Rasmussen LS. Long-term consequences of postoperative cognitive dysfunction. Anesthesiology. 2009;110(3):548–555. doi:10.1097/ALN.0b013e318195b569
9. Chu JMT, Abulimiti A, Wong BSH, et al. Sigesbeckia orientalis L. derived active fraction ameliorates perioperative neurocognitive disorders through alleviating hippocampal neuroinflammation. Front Pharmacol. 2022;13:846631. doi:10.3389/fphar.2022.846631
10. Evora PR, Bottura C, Arcencio L, et al. Key points for curbing cardiopulmonary bypass inflammation. Acta Cir Bras. 2016;31(Suppl 1):45–52. doi:10.1590/s0102-86502016001300010
11. Poli EC, Alberio L, Bauer-Doerries A, et al. Cytokine clearance with CytoSorb(R) during cardiac surgery: a pilot randomized controlled trial. Crit Care. 2019;23(1):108. doi:10.1186/s13054-019-2399-4
12. Farag M, Patil NP, Sabashnikov A, et al. Comparison of two miniaturized cardiopulmonary bypass systems regarding inflammatory response. Artif Organs. 2017;41(2):139–145. doi:10.1111/aor.12750
13. Wang S, Palanzo D, Ündar A. Current ultrafiltration techniques before, during and after pediatric cardiopulmonary bypass procedures. Perfusion. 2012;27(5):438–446. doi:10.1177/0267659112450061
14. Kuratani N, Bunsangjaroen P, Srimueang T, et al. Modified versus conventional ultrafiltration in pediatric cardiac surgery: a meta-analysis of randomized controlled trials comparing clinical outcome parameters. J Thorac Cardiovasc Surg. 2011;142(4):861–867. doi:10.1016/j.jtcvs.2011.04.001
15. Hu J, Li P, Chen X, et al. Effects of modified ultrafiltration and conventional ultrafiltration combination on perioperative clinical outcomes in pediatric cardiac surgery: a meta-analysis. Medicine. 2021;100(3):e24221. doi:10.1097/md.0000000000024221
16. Gholampour Dehaki M, Niknam S, Azarfarin R, Bakhshandeh H, Mahdavi M. Zero-balance ultrafiltration of priming blood attenuates procalcitonin and improves the respiratory function in infants after cardiopulmonary bypass: a randomized controlled trial. Artif Organs. 2019;43(2):167–172. doi:10.1111/aor.13325
17. Song LO, Yinglong LI, Jinping LI. Effects of zero-balanced ultrafiltration on procalcitonin and respiratory function after cardiopulmonary bypass. Perfusion. 2007;22(5):339–343. doi:10.1177/0267659107086726
18. Bierer J, Horne D, Stanzel R, et al. Continuous ultrafiltration enhances recovery after adult cardiac surgery with cardiopulmonary bypass: a systematic review and meta-analysis. CJC Open. 2023;5(7):494–507. doi:10.1016/j.cjco.2023.03.009
19. de Baar M, Diephuis JC, Moons KG, et al. The effect of zero-balanced ultrafiltration during cardiopulmonary bypass on S100b release and cognitive function. Perfusion. 2003;18(1):9–14. doi:10.1191/0267659103pf621oa
20. Wang J, Wu JJ, Ren XY, et al. Application of low-volume zero-balanced ultrafiltration and its effect on blood propofol concentration: a randomized controlled trial. J Cardiovasc Surg. 2010;51(2):257–263.
21. Han JH, Wilson A, Graves AJ, et al. Validation of the confusion assessment method for the intensive care unit in older emergency department patients. Acad Emerg Med. 2014;21(2):180–187. doi:10.1111/acem.12309
22. Creavin ST, Wisniewski S, Noel-Storr AH, et al. Mini-Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Cochrane Database Syst Rev. 2016;2016(1):Cd011145. doi:10.1002/14651858.CD011145.pub2
23. Jammer I, Wickboldt N, Sander M, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: european Perioperative Clinical Outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol. 2015;32(2):88–105. doi:10.1097/eja.0000000000000118
24. Austin PC. Balance diagnostics for comparing the distribution of baseline covariates between treatment groups in propensity-score matched samples. Stat Med. 2009;28(25):3083–3107. doi:10.1002/sim.3697
25. Cerejeira J, Firmino H, Vaz-Serra A, Mukaetova-Ladinska EB. The neuroinflammatory hypothesis of delirium. Acta Neuropathol. 2010;119(6):737–754. doi:10.1007/s00401-010-0674-1
26. Terrando N, Eriksson LI, Ryu JK, et al. Resolving postoperative neuroinflammation and cognitive decline. Ann Neurol. 2011;70(6):986–995. doi:10.1002/ana.22664
27. Ni P, Dong H, Wang Y, et al. IL-17A contributes to perioperative neurocognitive disorders through blood-brain barrier disruption in aged mice. J Neuroinflammation. 2018;15(1):332. doi:10.1186/s12974-018-1374-3
28. Zhuang X, Fu L, Luo L, et al. The effect of perioperative dexmedetomidine on postoperative delirium in adult patients undergoing cardiac surgery with cardiopulmonary bypass: a systematic review and meta-analysis of randomized controlled trials. BMC Anesthesiol. 2024;24(1):332. doi:10.1186/s12871-024-02715-2
29. Croughwell ND, Newman MF, Blumenthal JA, et al. Jugular bulb saturation and cognitive dysfunction after cardiopulmonary bypass. Ann Thorac Surg. 1994;58(6):1702–1708. doi:10.1016/0003-4975(94)91666-7
30. Barbut D, Hinton RB, Szatrowski TP, et al. Cerebral emboli detected during bypass surgery are associated with clamp removal. Stroke. 1994;25(12):2398–2402. doi:10.1161/01.str.25.12.2398
31. Lu J, Shi Y, Lan X, et al. Effect of ciprofol on postoperative cognitive function in patients undergoing cardiac surgery with cardiopulmonary bypass: a prospective, randomized, controlled trial. Drug Des Devel Ther. 2025;19:7541–7552. doi:10.2147/dddt.S536225
32. Hall RI, Smith MS, Rocker G. The systemic inflammatory response to cardiopulmonary bypass: pathophysiological, therapeutic, and pharmacological considerations. Anesth Analg. 1997;85(4):766–782. doi:10.1097/00000539-199710000-00011
33. Bierer J, Stanzel R, Henderson M, Sett S, Horne D. Ultrafiltration in pediatric cardiac surgery review. World J Pediatr Congenit Heart Surg. 2019;10(6):778–788. doi:10.1177/2150135119870176
34. Bierer JD, Stanzel R, Henderson M, et al. The immunomodulatory effect of continuous ultrafiltration during pediatric cardiac surgery. Perfusion. 2025:2676591251374252. doi: 10.1177/02676591251374252
35. Huang H, Li H, Zhang X, et al. Association of postoperative delirium with cognitive outcomes: a meta-analysis. J Clin Anesth. 2021;75:110496. doi:10.1016/j.jclinane.2021.110496
36. Crocker E, Beggs T, Hassan A, et al. Long-term effects of postoperative delirium in patients undergoing cardiac operation: a systematic review. Ann Thorac Surg. 2016;102(4):1391–1399. doi:10.1016/j.athoracsur.2016.04.071
37. Sauer AC, Veldhuijzen DS, Ottens TH, et al. Association between delirium and cognitive change after cardiac surgery. Br J Anaesth. 2017;119(2):308–315. doi:10.1093/bja/aex053
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors and Short-Term Outcomes of Postoperative Pulmonary Complications in Elderly Patients After Cardiopulmonary Bypass
Liu J, Li X, Xie W, Wang Y, Xu Z, Bai YX, Zhou Q, Wu Q
Clinical Interventions in Aging 2024, 19:31-39
Published Date: 6 January 2024
Effect of Ciprofol on Postoperative Cognitive Function in Patients Undergoing Cardiac Surgery with Cardiopulmonary Bypass: A Prospective, Randomized, Controlled Trial
Lu J, Shi Y, Lan X, Tang G, Shao Y, Chen C, Xiong X, Chen D, Shi J
Drug Design, Development and Therapy 2025, 19:7541-7552
Published Date: 29 August 2025