Back to Journals » Drug Design, Development and Therapy » Volume 19
Effect of Ciprofol on Postoperative Cognitive Function in Patients Undergoing Cardiac Surgery with Cardiopulmonary Bypass: A Prospective, Randomized, Controlled Trial
Authors Lu J, Shi Y, Lan X, Tang G, Shao Y, Chen C, Xiong X, Chen D, Shi J ![]()
Received 28 May 2025
Accepted for publication 23 August 2025
Published 29 August 2025 Volume 2025:19 Pages 7541—7552
DOI https://doi.org/10.2147/DDDT.S536225
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Jun Lu,1,* Yewei Shi,1,* Xin Lan,1 Guangling Tang,1 Yi Shao,1 Chao Chen,1 Xinglong Xiong,1 Dongxu Chen,2,3 Jing Shi1
1Department of Anesthesiology, Affiliated Hospital of Guizhou Medical University, Guiyang, People’s Republic of China; 2Department of Anesthesiology, West China Second Hospital, Sichuan University, Chengdu, People’s Republic of China; 3Key Laboratory of Birth Defects and Related Diseases of Women and Children, Sichuan University, Chengdu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing Shi, Department of Anesthesiology, the Affiliated Hospital of Guizhou Medical University, Guiyang, People’s Republic of China, Tel +86-18685034016, Email [email protected] Dongxu Chen, Department of Anesthesiology, West China second Hospital, Sichuan University, Chengdu, People’s Republic of China, Tel +86-15881730901, Email [email protected]
Purpose: To investigate the effects of ciprofol on postoperative cognitive function in patients undergoing cardiac surgery with cardiopulmonary bypass (CPB).
Patients and Methods: A total of 138 patients who underwent cardiac surgery with cardiopulmonary bypass were included in this prospective, randomized, controlled study. Patients were randomized into two groups: the Ciprofol group (Group C) and the Propofol group (Group P). During anesthesia induction and maintenance, the patients in Group C received ciprofol, whereas those in Group P received propofol. The primary outcome measure was the incidence of postoperative delirium (POD), which was assessed twice daily for 7 days after surgery via either the Confusion Assessment Method (CAM) or the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU). Statistical analyses included chi-square tests for categorical outcomes and relative risk calculations for POD. Additionally, delirium subtypes were recorded. The incidence of postoperative cognitive dysfunction (POCD) was evaluated at 1 and 3 months after surgery using the Telephone Montreal Cognitive Assessment (T-MoCA). Furthermore, the occurrence of postinduction adverse events, including hypotension, bradycardia, and tachycardia, as well as the incidence of postoperative complications, were also documented.
Results: POD occurred in 19/64 (29.69%) patients in the Ciprofol group and 34/65 (52.31%) patients in the Propofol group (RR = 0.57; 95% confidence interval = 0.37 to 0.88; p = 0.009). There was no significant difference in the incidence of POCD at 1 month (22.03% vs 26.62%, p = 0.547) or 3 months (16.25% vs 16.00%; p = 0.771) after surgery between the two groups.
Conclusion: Ciprofol was found to decrease the incidence of POD in patients who underwent cardiac surgery with cardiopulmonary bypass. Nevertheless, no significant effect of this intervention on the incidence of POCD was demonstrated at either 1 or 3 months after surgery. A reduction in the incidence of delirium may be associated with improved postoperative recovery, shortened hospital stays, and a decrease in long-term cognitive impairments.
Registration: The study had been registered in the Chinese Clinical Trials Registry (www.chictr.org.cn; Trial Identifier: ChiCTR2200061712).
Keywords: ciprofol, cardiopulmonary bypass, cardiac surgery, delirium, cognitive function
Introduction
Perioperative neurocognitive disorder (PND) refers to a spectrum of behavioural, emotional, and cognitive alterations that may manifest during and after anesthesia and surgical interventions. PND encompasses acute postoperative delirium (POD) and postoperative cognitive dysfunction (POCD).1 The onset of PND can lead to longer hospital stays, higher costs, and a higher mortality rate.2 Reports indicate that postoperative delirium is the second most common perioperative organ injury, with a patient mortality rate of approximately 6.6% when it occurs alone. However, when it occurs in conjunction with other organ injuries, the mortality rate reaches 21.6%.3 Additionally, elderly patients with delirium face a greater risk of death.4,5
The incidence of POD is influenced by the type of surgical procedure. In patients undergoing noncardiac surgery, the incidence rate of POD is approximately 30%.6 Conversely, in patients undergoing cardiac surgery with cardiopulmonary bypass (CPB), the incidence of POD can be as high as 72%.7 Recent research has revealed that factors contributing to the onset of POD in this patient population include advanced age, prolonged CPB duration, embolization, hypoxemia, hypotension, and anesthetic, as well as inflammation and stress.8,9 Notably, anesthetic agents play a pivotal role in this context. Propofol is one of the most commonly used anesthetics in cardiac surgery with cardiopulmonary bypass because of its rapid metabolism and high safety. Nevertheless, propofol is not devoid of drawbacks; for example, it may significantly decrease the mean arterial pressure by suppressing sympathetic nerve activity, thereby affecting haemodynamics.10 In addition, in terms of cognitive function, the impact of propofol on postoperative cognitive function remains a subject of debate. A related study indicated that, compared with sevoflurane, propofol may result in a greater incidence of POD and POCD.11 Conversely, another study demonstrated that the effects of propofol on POD were not significantly different from those of sevoflurane or desflurane.12 Comparatively, studies on newer agents like remimazolam suggest potential benefits, but its performance relative to propofol for POD prevention in CPB surgery also shows mixed results.10
Ciprofol, a novel intravenous sedative agent, incorporates a cyclopropyl group into the chemical structure of propofol, thereby increasing its affinity for GABAA-R receptors.13 Compared with propofol, ciprofol has advantages such as more stable haemodynamic profiles, a reduced incidence of adverse reactions, and an increased safety margin.14 A recent study demonstrated that patients who received ciprofol for anesthesia induction and maintenance presented significantly lower Confusion Assessment Method (CAM) scores than did those who received propofol for anesthesia induction and maintenance.15 Therefore, we postulate that ciprofol therapy represents a potential strategy for mitigating the risk of cognitive impairment. Nevertheless, few studies have examined the impact of ciprofol on POD in patients undergoing cardiac surgery with CPB.
Consequently, the present study aimed to investigate the impact of ciprofol on postoperative cognitive function in patients undergoing cardiac surgery with CPB via a randomized, controlled, double-blind clinical trial design.
Materials and Methods
Study Design
This study was performed in accordance with the ethical standards of the Helsinki Declaration,16 which were developed by the World Medical Association. Moreover, this study was approved by the Medical Science Ethics Committee of the Affiliated Hospital of Guizhou Medical University (Approval No. 2022115K; Approval date, 2022/11/18) and was subsequently registered in the Chinese Clinical Trials Registry (www.chictr.org.cn; Trial Identifier: ChiCTR2200061712). The study was executed in accordance with the Consolidated Standards of Reporting Trials (CONSORT)17 guidelines, with all participants providing written informed consent.
Patients
Adult patients who had undergone cardiac surgery with CPB were included in the study. Eligible participants were at least 18 years of age, had an American Society of Anesthesiologists (ASA) classification of II–IV and a New York Heart Association (NYHA) functional class of II–IV, and were capable of participating in neuropsychological tests and follow-up assessments. Patients were excluded if they had a history of neurological or psychiatric disorders, such as dementia or speech impairment, were on long-term psychotropic medication, had severe hepatic or renal dysfunction. Additionally, patients who experienced severe hemodynamic instability or malignant arrhythmia during surgery, underwent secondary thoracotomy, or died within 24 hours after surgery were withdrawn. The definitions of severe hemodynamic instability and malignant arrhythmia can be found in the Supplementary Materials.
Randomization and Blinding
Following the completion of the preoperative screening and baseline assessment by the assigned investigator, the patients were randomly allocated to either the Ciprofol group (Group C) or the Propofol group (Group P) at a 1:1 ratio using a random number table (generated by SPSS 27.0 software) method developed by another investigator. Upon a patient’s arrival in the operating room, an envelope containing the patient’s random number and corresponding group assignment was provided to the anesthesiologist by the researchers. All anesthesiologists were excluded from the study, and the researchers who participated in the randomized allocation and intraoperative data collection did not participate in the postoperative follow-up. In addition, all patients and personnel involved in the preoperative assessment, intraoperative data collection, and postoperative follow-up and statisticians remained blinded to the group assignments.
Sample Size
The sample size was determined on the basis of preliminary experiments. The incidence of POD following cardiac surgery was approximately 52% in Group P and 28% in Group C. Our calculations indicated that a sample size of 62 patients per group would provide 80% power to detect a reduction of approximately half in POD incidence, at a two-sided significance level of 0.05. Consequently, we planned to enrol 138 patients (69 per group) to account for an expected dropout rate of 10%.
Intervention
The intervention process was divided into an anesthesia induction period and a maintenance period. During induction, after intravenous administration of 0.05 mg/kg midazolam and 0.5 µg/kg sufentanil in both groups, patients in groups C and P received intravenous injections of 0.4 mg/kg ciprofol and 2.0 mg/kg propofol, respectively. When the eyelash reflex had disappeared. All patients were given the muscle relaxant rocuronium 0.6 mg/kg intravenously. During the period of anesthesia maintenance and during off-cardiopulmonary circulation, patients in both groups were given a combined anesthesia regimen: Group C was given 0.4–0.8 mg·kg−1·h−1 intravenous ciprofol, and Group P was given 2–4 mg·kg−1·h−1 intravenous propofol. The dosing regimen for ciprofol in this study was selected based on its known relative potency (approximately 4–5 times that of propofol) and established effective dosing ranges from previous clinical studies aiming to achieve comparable anesthetic depth while leveraging its potentially favourable hemodynamic profile.13 In addition, the two groups of patients received the inhalation anesthetic sevoflurane (0.8–1 MAC) via a tracheal catheter and the analgesic sufentanil 0.5–1 µg·kg−1·h−1 intravenously. During extracorporeal circulation, sevoflurane was discontinued in both groups. The patients in Group C received an intravenous injection of 0.8–2.4 mg·kg−1·h−1 ciprofol, the patients in Group P received an intravenous injection of 4–12 mg·kg−1·h−1 propofol, and the patients in both groups continued to receive analgesic treatment with 0.5–1 µg·kg−1·h−1 sufentanil (Supplementary Figure S1). Patients in both groups were given intravenous rocuronium at 0.15–0.3 mg/kg per hour to ensure sustained muscle relaxation. All perioperative management procedures except for the interventions were consistent.
Perioperative Management
Upon entering the operating room, all patients first underwent peripheral intravenous cannulation. Standard monitoring protocols were then implemented, comprising five-lead electrocardiography (ECG), noninvasive blood pressure (NIBP) measurement, pulse oximetry (SpO2), and cerebral oxygen saturation (SctO2) monitoring. Moreover, arterial cannulation was established via radial artery access after passing Allen’s test for continuous mean arterial pressure (MAP) monitoring. A central venous catheter was subsequently inserted under ultrasound guidance through the right internal jugular vein for central venous pressure (CVP) monitoring and fluid administration. All patients underwent CPB via a cardiopulmonary machine (model: the Sorin Stockert S5, manufactured by Sorin Stockert Instruments GMBH, Germany). During CPB, the Bispectral Index (BIS) was controlled at 40–60, the MAP was maintained at 55–75 mmHg, the hematocrit (Hct) was maintained at 25–30%, the oxygenation index (OI = PO2/FiO2) was maintained at 300–400 mmHg, and the partial pressure of arterial blood carbon dioxide (PaCO2) was maintained at 35–45 mmHg. For SctO2, the target value was set at 60–80% (bilateral monitoring). If SctO2 dropped below 60% for more than 30 seconds, the following adjustments were made sequentially: 1) optimizing MAP within the target range (55–75 mmHg) by adjusting vasoactive drugs; 2) increasing hematocrit to 28–30% via autotransfusion; and 3) checking for mechanical obstruction in the CPB circuit or adjusting cerebral perfusion pressure by modifying pump flow rate. Furthermore, autotransfusion was administered to all patients.
Outcomes
The primary outcome of the study was the incidence of POD, as ascertained by a positive assessment utilizing the CAM or the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU), within the first 7 days following surgery or until the occurrence of discharge or death, whichever event preceded the others. CAM was used in patients who were awake or able to communicate verbally, and CAM-ICU was used in patients who were mechanically ventilated by endotracheal intubation and unable to communicate verbally.18 All CAM/CAM-ICU assessments were performed by a trained doctor (Chao Chen) who was blinded to group assignments and had completed certification in delirium assessment.
In addition, we evaluated the subtypes of POD and the incidence of two or more episodes of delirium. Drawing upon previous research, we categorized delirium into three distinct types: a low-activity type, a high-activity type, and a mixed type.19 A subgroup analysis was conducted to examine the occurrence of POD across preset subgroups.
Furthermore, the telephone version of the Montreal Cognitive Assessment (T-MoCA) was used to assess the patients’ cognitive function at 1 month and 3 months after surgery. The T-MoCA is a 22-point scale that briefly assesses a patient’s ability in the areas of auditory attention, mental dexterity, verbal fluency, sentence repetition, memory for lists of words, and orientation to time and place.20 A score less than 18 was considered to indicate POCD.
Baseline vital sign data for patients were collected five minutes after they had lain flat and rested upon entering the operating room. We documented various intraoperative adverse events, including postinduction (2 minutes after induction of anesthesia, T1) hypotension, bradycardia and tachycardia. Hypotension was defined as a MAP less than 65 mmHg. Tachycardia was defined as a heart rate (HR) exceeding 100 beats per minute, whereas a heart rate (HR) below 60 beats per minute was considered bradycardia. The observation time points were as follows: T0 (5 minutes after entering the operating room), T1 (2 minutes after induction of anesthesia), T2 (immediately after intubation), T3 (immediately before skin incision), T4 (10 minutes into the CPB), T5 (40 minutes into the CPB), T6 (immediately after the conclusion of the CPB), and T7 (immediately after surgery). The MAP, HR, SpO2, CVP, and SctO2 were recorded at these time points. To improve patient comfort and the safety of cardiac surgery, central venous puncture placement was performed after endotracheal intubation; therefore, central venous pressure was not monitored or recorded before the skin incision and during CPB.
We documented data pertaining to postoperative hospitalizations, including the duration of postoperative mechanical ventilation, the length of stay in the ICU, and the duration of the postoperative hospital stay. Additionally, we recorded the occurrence of postoperative complications, specifically postoperative pneumonia, postoperative pleural effusion, and postoperative acute kidney injury (AKI), in accordance with the European Perioperative Clinical Outcome (EPCO) definitions.21 Supplementary material that further elucidates these definitions is provided.
Statistical Analysis
The normality of the quantitative data was assessed using histograms. For normally distributed continuous variables, the means ± standard deviations (SDs) are reported, and group comparisons were performed via t tests. Otherwise, medians and quartiles are presented, with group comparisons carried out using the Mann‒Whitney U-test.
A chi-square test was used to compare the incidence of POD. The impact of ciprofol on POD incidence was quantified via the relative risk (RR) with a 95% confidence interval (CI). To investigate variations in the primary outcome, exploratory analyses were performed to assess differences among the predefined subgroups, which included subgroups classified by age, sex, ASA class, NYHA class, CABG status, CPB duration, and surgery duration. Logistic regression was used to analyze treatment-by-covariate interactions separately for each subgroup factor.
Multiple interpolation methods were employed to estimate the missing values in the postoperative neurocognitive function evaluation. An identical approach was used to verify the classification results. The detail approach of multiple-imputation can be found in Supplementary Materials. Additionally, the length of hospital stay and the duration of stay in the ICU were compared between the two groups using the Mann‒Whitney U-test, and the Hodges‒Lehman median difference (95% CI) was calculated. For multiple comparisons, we applied the Bonferroni correction to control the type I error rate in outcomes, and reported the adjusted p values.
All the statistical analyses were conducted using SPSS 27.0 software. Statistical significance was defined as a two-sided p value < 0.05.
Results
Baseline Characteristics
Between March 2023 and February 2024, a total of 171 patients were assessed in the study. Ultimately, 138 patients met the inclusion criteria and were subsequently randomized to either Group C (n = 69) or Group P (n = 69). However, six patients were excluded from the study because they underwent secondary thoracotomy within 24 hours (n = 3) or surgery postponement or cancellation (n = 3), and three other patients were excluded owing to missing data (n = 1) or withdrawal of consent (n = 2). Consequently, 129 patients were included in the final analysis (Figure 1). The baseline characteristics (Table 1) and intraoperative data (Supplementary Table S1) of the two groups were comparable, with no statistically significant differences observed.
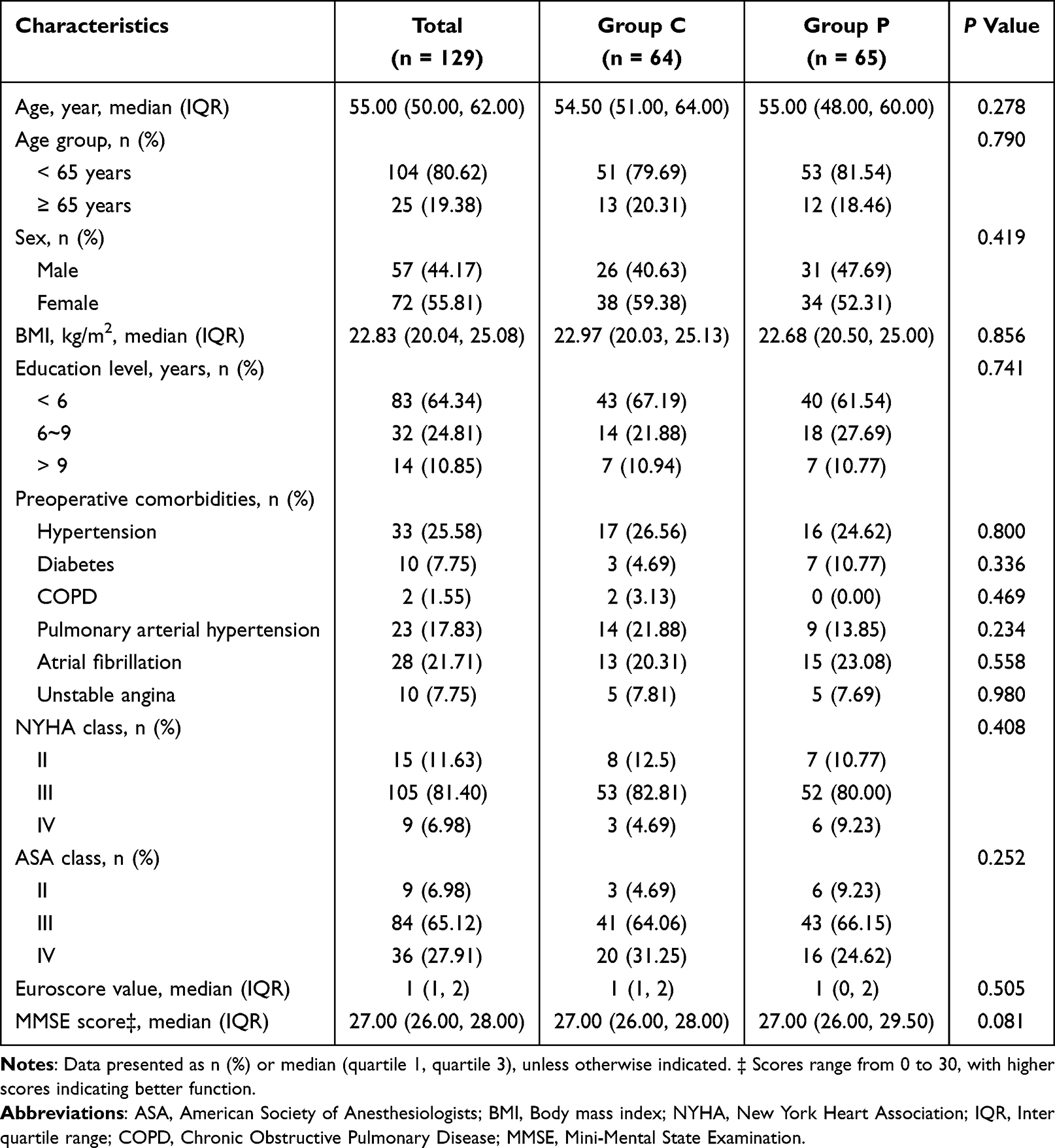 |
Table 1 Demographic Characteristics |
 |
Figure 1 Flow chart of patients enrollment. Abbreviations: CPB, cardiopulmonary bypass. |
Primary Outcome
The study revealed that the incidence of POD in Group C was significantly lower than that in Group P (29.69% vs 52.31%; RR 0.57, 95% CI 0.37–0.88; p = 0.009) (Table 2). No significant differences were observed in the three delirium subtypes between the two groups. Moreover, in Group C, 14 out of 64 patients (21.88%) experienced two or more delirium episodes, whereas 24 out of 65 patients (36.92%) experienced two or more delirium episodes in Group P; however, this difference did not reach statistical significance (RR 0.59, 95% CI 0.34–1.04; p = 0.061). Notably, the cumulative risk curve for POD indicated that the cumulative risk of delirium increased over time after surgery, with the peak incidence occurring on postoperative days 2 and 3 in both groups. Furthermore, the cumulative incidence of delirium in the control group was significantly greater than that in the intervention group (HR 2.791, 95% CI 1.352–5.763; p = 0.006) (Figure 2). Additionally, subgroup analysis of POD demonstrated no significant interaction effect between the intervention and the predefined factors (Supplementary Figure S2).
 |
Table 2 Primary and Secondary Outcomes |
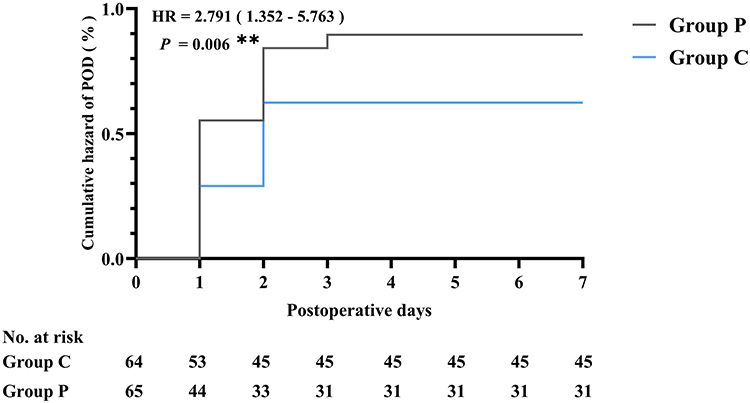 |
Figure 2 Cumulative hazard of postoperative delirium. Abbreviations: POD, postoperative delirium; HR, hazard ratio; P, P-value. Notes: **p < 0.01, the cumulative hazard of postoperative delirium between the two groups. |
Secondary Outcomes
One month after surgery, the incidence of POCD was 22.03% in Group C and 26.62% in Group P, with no statistically significant difference (p = 0.547). At the 3-month postsurgery follow-up, the incidence of POCD remained similar between the two groups (16.25% vs 16.00%; p = 0.771), again showing no significant difference.
Vital Signs
At all time points, no significant differences were observed in HR (Figure 3A), SpO2 (Figure 3C), CVP (Figure 3D), or bilateral SctO2 (Figure 3E and F) between the two groups. Notably, however, the postinduction (2 minutes after induction of anesthesia, T1) MAP in Group C was significantly greater than that in Group P (p = 0.021). In addition, the MAP in group C was greater than that in group P at other time points during anesthesia (T2 - T7), but the difference was not statistically significant (p > 0.05) (Figure 3B). Regarding cardiovascular adverse events during induction, there were no significant differences in the incidence rates of postinduction bradycardia and postinduction tachycardia between Groups C and P (Table 2). However, the incidence of postinduction hypotension was significantly greater in Group P than in Group C (44.62% vs 18.75%; p = 0.002).
 |
Figure 3 Intraoperative vital signs. Abbreviations: IQR, Inter quartile range, T0, 5 minutes after entering the operating room; T1, 2 minutes after induction of anesthesia; T2, immediately after intubation; T3, immediately before skin incision; T4, 10 minutes into CPB; T5, 40 minutes into CPB; T6, immediately after the conclusion of CPB; T7, immediately after surgery; HR, heart rate; MAP, mean arterial pressure; SpO2, pulse oxygen saturation; CVP, central venous pressure; SctO2, cerebral oxygen saturation; CPB, cardiopulmonary bypass; ns, no significant (p > 0.05). Notes: (A) HR, (B) MAP, (C) SpO2, (D) CVP, (E) SctO2-Left, and (F) SctO2-Right. Values are expressed as means or IQR. *p < 0.05 between the two groups at the same time point. |
Postoperative Hospitalization Data and Complications
No significant differences were observed between the two groups in terms of the duration of postoperative mechanical ventilation, length of stay in the ICU, or length of postoperative hospital stay. In addition, there was no statistically significant difference in the incidence of postoperative pneumonia, pleural effusion, or AKI between the two groups (Table 3).
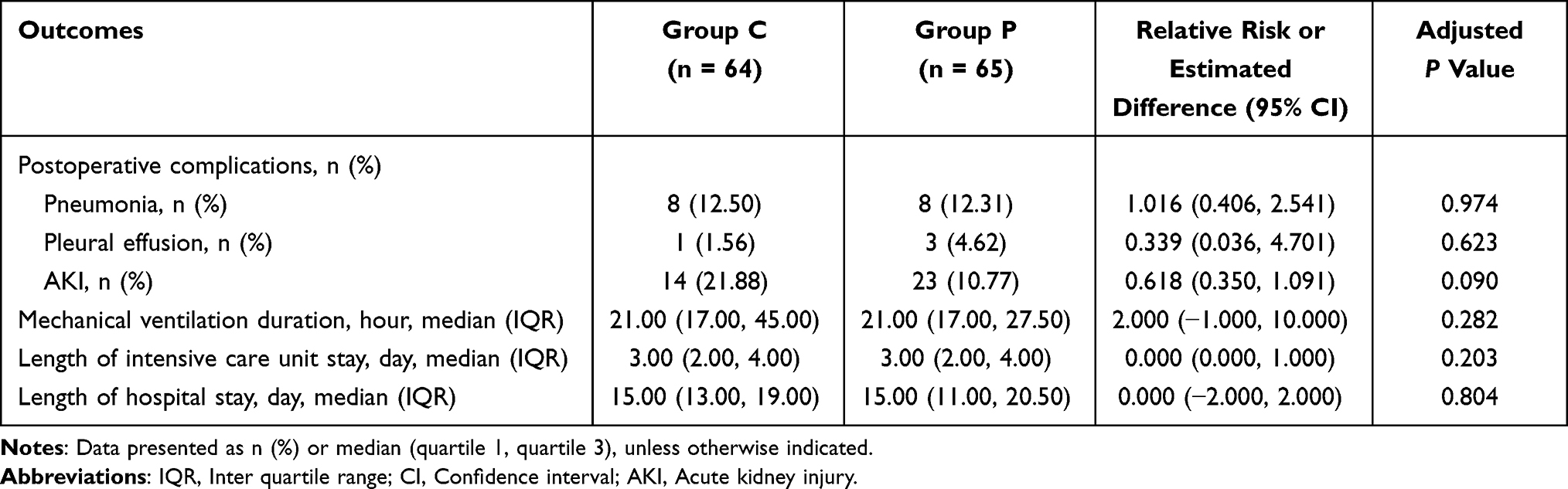 |
Table 3 Postoperative Complications and Hospitalization Data |
Discussion
This randomized controlled trial investigated the effects of ciprofol on postoperative cognitive function in patients who underwent cardiac surgery with CPB. The key findings are as follows:
First, compared with propofol, ciprofol significantly reduced the incidence of POD in patients who underwent cardiac surgery with CPB. Furthermore, ciprofol was associated with a lower cumulative risk of POD during the seven days after surgery. POD manifests clinically as altered consciousness, personality disorders, impaired attention and memory, and impaired spatial orientation, significantly impacting prognosis.22 The overall incidence of POD in our study was 41.09%, which aligns with the incidence of POD reported in previous studies of patients who underwent cardiac surgery with CPB.23,24 Notably, ciprofol significantly reduced the incidence of POD. Our findings offer novel insights into the prevention of POD in this patient population.
Another notable concern was that compared with propofol, ciprofol not only provided a greater postinduction mean arterial pressure but also significantly decreased the incidence of hypotension after induction. In addition, ciprofol also maintained a greater MAP than did propofol during the maintenance phase of anesthesia (T2-T7), although a comparison of the two data sets did not reveal statistical significance. These findings indicate that the ciprofol has a more favourable effect on sustaining more stable haemodynamics in patients undergoing cardiac surgery with CPB. Moreover, this may be associated with a lower incidence of POD in patients in group C undergoing cardiac surgery. Previous studies have shown that inadequate cerebral perfusion25 and low cerebral oxygen saturation26 due to hypotension may impair postoperative neurocognitive function in patients. Propofol not only causes circulatory depression but also induces cerebral vascular constriction, leading to a dose-dependent reduction in the cerebral oxygen metabolic rate, cerebral blood flow, and cerebral blood volume.27 The addition of cyclopropyl provides ciprofol with an asymmetric chemical structure that enhances its affinity for the GABAA-R receptor, thereby increasing its target selectivity and efficacy and increasing its target selectivity and potency.28 This specific mechanism enables the ciprofol to achieve an adequate depth of anesthesia while mitigating the risk of cerebral ischemia and hypoxia associated with circulatory depression. The results of this study revealed that patients in group C maintained higher brain tissue oxygen saturation during anesthesia than patients in group P did, although the difference was not statistically significant. These outcomes may be correlated with a lower incidence of POD in patients in group C who underwent cardiac surgery with CPB.
With respect to POCD, we employed the T-MoCA to assess mid- to long-term cognitive function. Unfortunately, despite performing multiple imputations for missing data, we did not observe significant differences in the incidence of POCD attributable to intervention factors. This lack of significance may be due to two factors. On the one hand, both ciprofol and propofol are short-acting intravenous anesthetics that are rapidly metabolized in vivo and thus do not significantly affect patients’ mid- to long-term cognitive function. On the other hand, as patients’ primary diseases improve, neurocognitive function is gradually restored.29 Therefore, the incidence of postoperative neurocognitive deficits did not significantly differ between the two groups of patients.
To investigate the effect of the ciprofol on patient prognosis, this study compared the incidence of different postoperative complications and hospitalization data between the two groups. We found that the incidence of each complication was similar between the two groups. One of the reasons for this may be that ciprofol and propofol are excreted from the body in a similar manner, being metabolized mainly by the liver and excreted by the kidneys.30 In addition, the metabolism of both drugs is largely unaffected in patients with mild to moderate hepatic and renal impairment.31 There were also no significant differences in the length of mechanical ventilation, ICU stay, or hospitalization between the two groups, which may be related to the similar and rapid elimination half-life of ciprofol and propofol,32,33 which would result in rapid clearance of both drugs from the patient’s body. Thus, there was no significant impact on patient prognosis.
This study has several limitations. First, as a single-center study, the generalizability of our findings may be limited. Second, our study recorded only vital signs and cognitive functions and did not investigate molecular markers related to PNDs in patients’ blood. Third, we lack direct data on cerebral perfusion (transcranial Doppler or cerebral blood flow measurements) to confirm the link between ciprofol-induced hemodynamic stability and reduced POD. These limitations may have biased our results. In addition, our study evaluated only cardiac surgery patients, which could not benefit a larger patient population. Therefore, in subsequent studies, we will further investigate the effect of ciprofol on POD in different patient populations and investigate PND-related biomarkers.
Conclusion
In summary, compared with propofol, ciprofol can reduce the incidence of POD in patients undergoing cardiac surgery with CPB. However, this intervention has not been shown to significantly impact the incidence of POCD at the first month or three months after surgery. Furthermore, ciprofol decreased the incidence of hypotension after induction.
Data Sharing Statement
The corresponding author (Jing Shi) will provide the data on reasonable request.
Ethics Approval and Informed Consent
This study was approved by the Medical Science Ethics Committee of the Affiliated Hospital of Guizhou Medical University (Approval No. 2022115K; Approval date, 2022/11/18) and was subsequently registered in the Chinese Clinical Trials Registry (www.chictr.org.cn; Trial Identifier: ChiCTR2200061712). The study was executed in accordance with the Consolidated Standards of Reporting Trials (CONSORT) guidelines, with all participants providing written informed consent.
Acknowledgments
We would like to acknowledge the support from Qin Shan for his invaluable assistance with the delirium and neurocognitive assessment.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China [grant number 82060220], the outstanding reserve talents in the discipline of Affiliated Hospital of Guizhou Medical University in 2023 [grant number gyfyxkrc-2023-15], the science and technology plan project of Guizhou province [grant number ZK (2023)-General 390], the National Natural Science Foundation Cultivation Program Project of Affiliated Hospital of Guizhou Medical University [grant number gyfynsfc (2023)-10].
Disclosure
Jing Shi is the first correspondence author for this study. The authors report no conflicts of interest in this work. An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
References
1. Evered L, Silbert B, Knopman DS, et al. Recommendations for the nomenclature of cognitive change associated with anesthesia and surgery—2018. Anesthesiology. 2018;129(5):872. doi:10.1097/ALN.0000000000002334
2. Dilmen OK, Meco BC, Evered LA, Radtke FM. Postoperative neurocognitive disorders: a clinical guide. J Clin Anesth. 2024;92:111320. doi:10.1016/j.jclinane.2023.111320
3. Kork F, Liang Y, Ginde AA, et al. Impact of perioperative organ injury on morbidity and mortality in 28 million surgical patients. Nat Commun. 2025;16(1):3366. doi:10.1038/s41467-025-58161-2
4. Fenta E, Teshome D, Kibret S, et al. Incidence and risk factors of postoperative delirium in elderly surgical patients 2023. Sci Rep. 2025;15(1):1400. doi:10.1038/s41598-024-84554-2
5. Wu H, Yan S, Cao H, Feng C, Zhang H. Unraveling the impact of frailty on postoperative delirium in elderly surgical patients: a systematic review and meta-analysis. BMC Anesthesiol. 2025;25(1):114. doi:10.1186/s12871-025-02994-3
6. Austin CA, O’Gorman T, Stern E, et al. Association between postoperative delirium and long-term cognitive function after major nonemergent surgery. JAMA Surg. 2019;154(4):328–334. doi:10.1001/jamasurg.2018.5093
7. Wang H, Guo X, Zhu X, et al. Gender differences and postoperative delirium in adult patients undergoing cardiac valve surgery. Front Cardiovasc Med. 2021;8:751421. doi:10.3389/fcvm.2021.751421
8. Steinmetz J, Rasmussen LS. Peri-operative cognitive dysfunction and protection. Anaesthesia. 2016;71 Suppl 1:58–63. doi:10.1111/anae.13308
9. Staicu RE, Vernic C, Ciurescu S, et al. Postoperative delirium and cognitive dysfunction after cardiac surgery: the role of inflammation and clinical risk factors. Diagnostics. 2025;15(7):844. doi:10.3390/diagnostics15070844
10. Suga M, Yasuhara J, Watanabe A, et al. Postoperative delirium under general anaesthesia by remimazolam versus propofol: a systematic review and meta-analysis of randomised controlled trials. J Clin Anesth. 2025;101:111735. doi:10.1016/j.jclinane.2024.111735
11. Varsha AV, Unnikrishnan KP, Saravana Babu MS, Raman SP, Koshy T. Comparison of propofol-based total intravenous anesthesia versus volatile anesthesia with sevoflurane for postoperative delirium in adult coronary artery bypass grafting surgery: a prospective randomized single-blinded study. J Cardiothorac Vasc Anesth. 2024;38(9):1932–1940. doi:10.1053/j.jvca.2024.05.027
12. Jiang JL, Zhang L, He LL, et al. Volatile versus total intravenous anesthesia on postoperative delirium in adult patients undergoing cardiac valve surgery: a randomized clinical trial. Anesth Analg. 2023;136(1):60–69. doi:10.1213/ANE.0000000000006257
13. Wu B, Zhu W, Wang Q, Ren C, Wang L, Xie G. Efficacy and safety of ciprofol-remifentanil versus propofol-remifentanil during fiberoptic bronchoscopy: a prospective, randomized, double-blind, non-inferiority trial. Front Pharmacol. 2022;13:1091579. doi:10.3389/fphar.2022.1091579
14. Qin K, Qin WY, Ming SP, Ma XF, Du XK. Effect of ciprofol on induction and maintenance of general anesthesia in patients undergoing kidney transplantation. Eur Rev Med Pharmacol Sci. 2022;26(14):5063–5071. doi:10.26355/eurrev_202207_29292
15. Liu Z, Jin Y, Wang L, Huang Z. The effect of ciprofol on postoperative delirium in elderly patients undergoing thoracoscopic surgery for lung cancer: a prospective, randomized, controlled trial. Drug Des Devel Ther. 2024;18:325–339. doi:10.2147/DDDT.S441950
16. Bulut B, Başcı AB, Olcay HE. Declaration of Helsinki: comparison of the 2024 version and the 2013 version. Infect Dis Clin Microbiol. 2025;7(1):112–113. doi:10.36519/idcm.2025.498
17. Schulz KF, Altman DG, Moher D, Group CONSORT. CONSORT 2010 statement: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c332. doi:10.1136/bmj.c332
18. Miranda F, Gonzalez F, Plana MN, Zamora J, Quinn TJ, Seron P. Confusion assessment method for the intensive care unit (CAM-ICU) for the diagnosis of delirium in adults in critical care settings. Cochrane Database Syst Rev. 2023;11(11):CD013126. doi:10.1002/14651858.CD013126.pub2
19. la Cour KN, Andersen-Ranberg NC, Weihe S, et al. Distribution of delirium motor subtypes in the intensive care unit: a systematic scoping review. Crit Care. 2022;26(1):53. doi:10.1186/s13054-022-03931-3
20. Chappelle SD, Gigliotti C, Léger GC, et al. Comparison of the telephone-montreal cognitive assessment (T-MoCA) and telephone interview for cognitive status (TICS) as screening tests for early Alzheimer’s disease. Alzheimers Dement. 2023;19(10):4599–4608. doi:10.1002/alz.13039
21. Jammer I, Wickboldt N, Sander M, et al. Standards for definitions and use of outcome measures for clinical effectiveness research in perioperative medicine: European Perioperative Clinical Outcome (EPCO) definitions: a statement from the ESA-ESICM joint taskforce on perioperative outcome measures. Eur J Anaesthesiol. 2015;32(2):88–105. doi:10.1097/EJA.0000000000000118
22. Pérez Palmer N, Trejo Ortega B, Joshi P. Cognitive impairment in older adults: epidemiology, diagnosis, and treatment. Psychiatr Clin North Am. 2022;45(4):639–661. doi:10.1016/j.psc.2022.07.010
23. Itting PT, Sadlonova M, Santander MJ, et al. Intra- and early postoperative predictors of delirium risk in cardiac surgery: results from the prospective observational FINDERI study. Int J Surg. 2025;111(4):2872–2885. doi:10.1097/JS9.0000000000002265
24. Mahmoudi H, Chalkias A, Moradi A, Moradian ST, Amouzegar SMR, Vahedian-Azimi A. Evaluation of postoperative delirium in cardiac surgery patients with the SDACS screening tool: a multicenter-multiphase study. Perioper Med. 2025;14(1):37. doi:10.1186/s13741-025-00518-8
25. Wang N, Ma J, Liu J, et al. Histamine H3 receptor antagonist enhances neurogenesis and improves chronic cerebral hypoperfusion-induced cognitive impairments. Front Pharmacol. 2019;10:1583. doi:10.3389/fphar.2019.01583
26. Li L, Gao Z, Zhang J, et al. Reduced regional cerebral oxygen saturation increases risk for emergence delirium in pediatric patients. Front Pediatr. 2023;11:1117455. doi:10.3389/fped.2023.1117455
27. Vimala S, Arulvelan A, Chandy Vilanilam G. Comparison of the effects of propofol and sevoflurane induced burst suppression on cerebral blood flow and oxygenation: a prospective, randomised, double-blinded study. World Neurosurg. 2020;135:e427–e434. doi:10.1016/j.wneu.2019.12.015
28. Liao J, Li M, Huang C, et al. Pharmacodynamics and pharmacokinetics of HSK3486, a novel 2,6-disubstituted phenol derivative as a general anesthetic. Front Pharmacol. 2022;13:830791. doi:10.3389/fphar.2022.830791
29. O’Gara BP, Mueller A, Gasangwa DVI, et al. Prevention of early postoperative decline: a randomized, controlled feasibility trial of perioperative cognitive training. Anesth Analg. 2020;130(3):586–595. doi:10.1213/ANE.0000000000004469
30. Hu Y, Li X, Liu J, et al. Safety, pharmacokinetics and pharmacodynamics of a novel γ-aminobutyric acid (GABA) receptor potentiator, HSK3486, in Chinese patients with hepatic impairment. Ann Med. 2022;54(1):2769–2780. doi:10.1080/07853890.2022.2129433
31. Tao J, Liu S, Zhao YY, et al. Pharmacokinetics, pharmacodynamics, and safety of ciprofol emulsion in Chinese subjects with normal or impaired renal function. Front Pharmacol. 2023;14:1260599. doi:10.3389/fphar.2023.1260599
32. Lu M, Liu J, Wu X, Zhang Z. Ciprofol: a novel alternative to propofol in clinical intravenous anesthesia? Biomed Res Int. 2023;2023:7443226. doi:10.1155/2023/7443226
33. Zhou J, Wang L, Zhong Z, et al. Pharmacological mechanism and clinical application of ciprofol. Front Pharmacol. 2025;16:1572112. doi:10.3389/fphar.2025.1572112
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Risk Factors and Short-Term Outcomes of Postoperative Pulmonary Complications in Elderly Patients After Cardiopulmonary Bypass
Liu J, Li X, Xie W, Wang Y, Xu Z, Bai YX, Zhou Q, Wu Q
Clinical Interventions in Aging 2024, 19:31-39
Published Date: 6 January 2024
Ciprofol in Children Undergoing Adenoidectomy and Adenotonsillectomy: A Retrospective Cohort Study
Zeng C, Li L, Wang M, Xiong J, Pang W, Yu H, He J, Wang X, Chen Y, Sun Y
Drug Design, Development and Therapy 2024, 18:4017-4027
Published Date: 6 September 2024
Zero-Balance Ultrafiltration Reduces Postoperative Delirium After Cardiac Surgery with Cardiopulmonary Bypass: A Randomized Controlled Trial
Lan X, Tang S, Lu J, Tang G, Shao Y, Zhu Z, Zhou K, Xiong X, Chen D, Shi J
Therapeutics and Clinical Risk Management 2025, 21:1807-1819
Published Date: 23 December 2025