Back to Archived Journals » Adolescent Health, Medicine and Therapeutics » Volume 11
Young People’s Response to Parental Neurological Disorder: A Structured Review
Authors Hartman L ![]() , Jenkinson C, Morley D
, Jenkinson C, Morley D ![]()
Received 8 November 2019
Accepted for publication 8 February 2020
Published 26 March 2020 Volume 2020:11 Pages 39—51
DOI https://doi.org/10.2147/AHMT.S237807
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Alastair Sutcliffe
Lilian Hartman,1 Crispin Jenkinson,2 David Morley2
1Lincoln College, University of Oxford, Oxford OX1 3DR, UK; 2Nuffield Department of Population Health, University of Oxford, Oxford OX3 7LF, UK
Correspondence: David Morley Tel +44 1865 289432
Email [email protected]
Introduction: A significant paucity of literature exists relating to the impact on children of parental neurological disorder, with the exception of multiple sclerosis. The wider literature in this field (parental cancer, depression, alcoholism, HIV/AIDS) exhibits the many potential challenges young people might experience during serious parental illness. Given this, a literature review of parental neurological disorder is long overdue.
Methods: This review is structured around the World Health Organisation (WHO) classification of neurological disorders. The WHO identifies 10 common neurological disorders; dementia, epilepsy, headache, multiple sclerosis, neuroinfections, neurological disorders associated with malnutrition, pain associated with neurological disorders, Parkinson’s disease, stroke, and traumatic brain injury. A comprehensive search of the MEDLINE database was performed using key terms for each of the 10 conditions. Results for each condition were divided in to “negative”, “positive and/or neutral” and “other” child responses.
Results: The search yielded a total of 6247 titles, of which 184 underwent a full-text assessment. Sixty-five met all eligibility criteria and were thus included in the review. A number of negative issues emerged across parental conditions including the prevalence of child mood disorders, parent-child role reversal, children’s need for information on the parental condition, the importance of family cohesion, the negative effect of parental psychopathology and differences between male and female children. A limited number of positive outcomes were evident in a minority of parental conditions. Outcomes measured and methodologies employed were highly heterogeneous.
Conclusion: Children generally respond negatively to parental neurological disorder. Responses varied between neurological disorders, suggesting the need for parental disease-specific guidance and clinical management where required.
Keywords: parental illness, neurological disorder, young people, children, parent, World Health Organisation, outcomes, review
Introduction
It has often been overlooked that illness has a wider reaching impact than being confined to the individuals affected themselves.1,2 Partners and close relatives also experience difficulties resulting from an illness, but the effects on the offspring of those diagnosed has, until recently, been largely neglected. Approximately 10% of children have a chronically ill parent3 and these children can potentially experience unique and complex challenges when faced with their parent’s condition. Current research emphasises the importance of specific variables such as the child’s family environment, their age, gender,4 and the specific nature and course of the parental condition.5 These challenges can lead to a variety of child responses, both positive, such as coping and independence,6 and negative, such as psychosocial maladjustment.4
In 2005, neurological disorders contributed to 10.9% and 4.5% of the global burden of disease in high- and low-income countries, respectively. Ultimately, they were responsible for 6.39% of the total disability-adjusted life years in 2015.7 Neurological conditions are often immensely debilitating, with many disorders showing a chronic progression that is lifelong, but not ultimately fatal.7 The disorders affect a diverse range of ages, with diseases classically associated with ageing, such as dementia, also occurring in a minority of younger patients. Many of those affected are, therefore, of child-rearing age. Over twenty years ago, the World Health Organisation’s (WHO) global initiative on neurology and public health8 identified a general lack of information on the burden of neurological disorders. Specifically, a great paucity of literature still exists relating to the impact on children of parental neurological illness. The wider literature in this field (parental cancer, depression, alcoholism, HIV/AIDS9–11) exhibits the many potential challenges young people are faced with during serious parental illness. Given this, a literature review of parental neurological illness is long overdue.
Aim
The purpose of this review is to scope the existing literature using a structured approach in order to determine the characteristics of children’s experiences of a range of parental neurological illnesses. It is intended that results will highlight current knowledge and research needs, as well as provide valuable information for clinicians and service providers. This review focuses on all children of affected parents, regardless of their caring status. A much wider literature is available regarding the specific impact of fulfilling the role of carer as a child12 and this is not addressed here.
World Health Organisation Classification of Neurological Disorders
This review is structured around the World Health Organisation’s (WHO) classification of neurological disorders. A 2006 report published by the WHO identified 10 neurological disorders that were said to “represent a substantial component of the global burden of neurological disorders”: dementia, epilepsy, headache disorders, neurological disorders associated with malnutrition, multiple sclerosis, neuroinfections, pain associated with neurological disorders, Parkinson’s disease, stroke, and traumatic brain injury.7 These conditions will be briefly introduced, in order to provide some context for the relevant child responses.
Dementia is an umbrella term used to describe a decline in multiple higher cortical functions such as memory, learning and comprehension,7 as well as behavioural changes.13 A minor proportion of patients are diagnosed before the age of 65, and are thus classified as “early onset” cases.14
Epilepsy describes conditions involving recurrent seizures, defined as “transient occurrences of signs and/or symptoms due to abnormal or excessive synchronous neuronal activity in the brain”.15 Epilepsy affects all ages and both sexes, including those of child-bearing age.
Headache disorders include cluster headache, tension-type headache, and medication-overuse headache. Those affected tend to be in the 20–40 year age group; often young families are particularly vulnerable. Migraine is the most extensively studied disorder, although not the most common, and affects women (and consequently mothers) far more than men.16
Neurological disorders associated with malnutrition are a largely preventable global problem resulting from the inadequate availability of food in many areas of the world.7 Malnutrition disturbs many aspects of health including the nervous system and cognitive development, can affect people of all ages, and ultimately lead to death. Specific neurological disorders include polyneuropathy, progressive myelopathy, and pellagra including dementia and depression.7,18
Multiple sclerosis (MS) is an autoimmune condition responsible for gradual and progressive physical disability, often accompanied by cognitive decline. Additional symptoms can include chronic fatigue and depression. Women are affected significantly more than men, where its onset tends to occur at childbearing age between 20 and 40 years.7,17
Neuroinfections is a term used to denote infectious diseases affecting the nervous system. In this category, the WHO includes: HIV/AIDS, viral encephalitis, poliomyelitis, tuberculosis, leprosy neuropathy, bacterial meningitis, tetanus, neurocysticercosis, cerebral malaria, toxoplasmosis, American/African trypanosomiasis, schistosomiasis and hydatidosis.7 Parental HIV/AIDs is not included here due to the number of recent reviews conducted,19–22 which readers may wish to refer to.
Pain associated with neurological disorders can be either direct neuropathic pain, or nervous system disorders that indirectly cause pain, where pain is defined as “an unpleasant sensory and emotional experience associated with actual or potential tissue damage”.23 Direct neuropathic pain is the consequence of neurological conditions that damage pathways that transmit information about painful stimuli in the peripheral or central nervous system. Alternatively, indirectly caused pain is a result of a condition that causes secondary activation of pain pathways, eg, musculoskeletal pain in Parkinson’s disease.7
Parkinson’s disease (PD) is a chronic progressive condition characterised by motor symptoms such as tremor and rigidity.7 Between 5% and 10% of those affected will develop PD before the age of 40 (although many will remain undiagnosed), and one in seven is diagnosed before the age of 50. Consequently, a number of those affected are likely to be raising young and/or adolescent children.24,25
Stroke can be defined as a rapid loss of neurological function as a result of haemorrhage or ischaemia. It is the third most common cause of death behind heart disease and cancer in most developed countries.7 Stroke can occur at any age with resultant features varying in severity, from mild weakness or tingling in the limbs, to major paralysis. The majority of stroke survivors show a degree of recovery over time, but only a minority return to their pre-stroke health state.26
Traumatic brain injury (TBI) is the leading cause of disability worldwide in those under the age of 40.7 Many young families are thus burdened considerably.27 The severity of TBI ranges greatly, leading to a diversity of patient outcomes with an often unpredictable recovery course.
Methods
Literature Search
A preliminary search indicated that the earliest relevant paper was published in 1984 and consequently the review searched the period from 1984 to October 2018. The PubMed interface was used to search the MEDLINE database. Each of the 10 aforementioned disorders was individually searched, with the search terms taking the general format of: “children AND parent AND condition”. Where the WHO classification sub-divided a single condition in to smaller categories, these sub-conditions were also searched in the database. The Web of Knowledge database was additionally searched for “children AND parent AND Parkinson’s disease” and results were then compared to those obtained from MEDLINE. This enabled validation of the original findings, and the assurance that no new studies were identified for inclusion.
Where relevant, methodologically sound systematic reviews of any of the ten disorders published within the last 5 years were summarised. The review process, as outlined above, was subsequently commenced 1 year prior to the submission date of the previous systematic review.
Eligibility Criteria
Peer-reviewed, full-text published studies were included where they met the following criteria: (1) children or youths aged 24 or below (in accordance with the United Nations’ definition of “youth”)28 were included or referenced by proxy as part of the study; (2) results were reported in either a qualitative or quantitative analysis; (3) at least one parent was diagnosed with at least one of the aforementioned 10 neurological conditions, or a condition mentioned as a sub-section within one of the 10 categories; and (4) the study was published in English. Due to the limited literature in this field, the inclusion criteria was designed to include a wide variety of methodologies including less reliable proxy reports (where the respondent is an individual other than the specific child in question). Data such as comments, conference abstracts, and opinion pieces were not included.
Data Extraction and Analysis
The utilisation of a data extraction form (see Figure 1) enabled the selection of relevant information from included studies, and an easier cross-comparison upon analysis. This was based on, and adapted from, a previously published review included in this report.29 All potentially eligible studies were then reviewed in a full-text analysis. In this instance, meta-analysis was not possible due to the diverse range of methodologies, both qualitative and quantitative, incorporated in the included studies. Outcomes measured were also highly heterogeneous. Consequently, narrative analyses were performed, where results from each condition were divided in to “negative”, “positive and/or neutral” and “other” child responses, thus facilitating an easier cross-comparison between results.
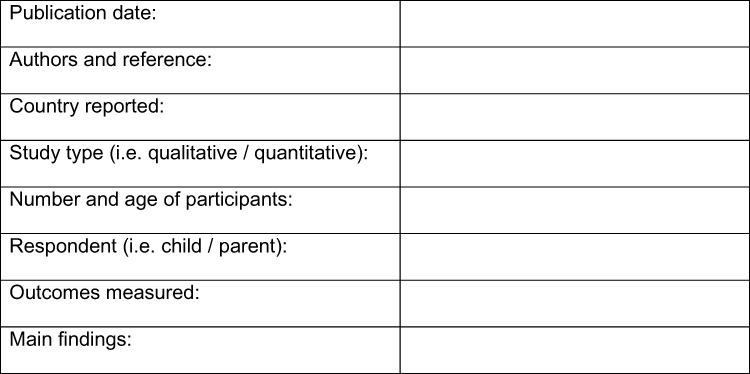 |
Figure 1 Data extraction form used for review process. Data from Razaz et al.29 |
Results
Literature Search
The numbers of studies returned by the initial searches of each condition, and the numbers undergoing subsequent exclusion and inclusion from the study, are summarised in Table 1. From the individual searches of all 10 conditions, a total of 6247 citations were returned. These citations underwent a title (and, where necessary, abstract) screening stage; here, 6064 were excluded, as they were not relevant to this review based of the previously outlined inclusion criteria. The remaining 183 underwent a full-text assessment for eligibility using the criteria, of which 118 were excluded. Reasons for their exclusion are given in Table 2. Sixty-five studies were thus deemed eligible, and included in this review.
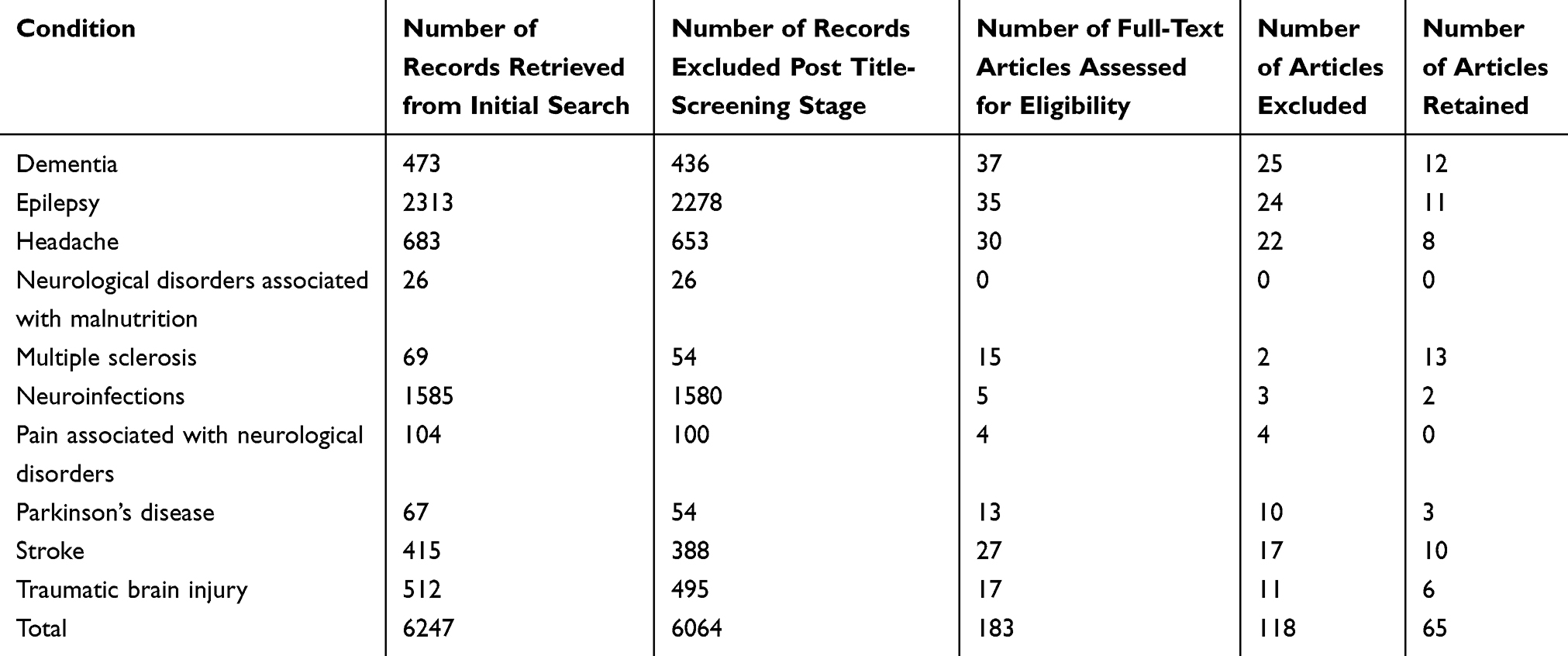 |
Table 1 Numbers of Records Retrieved, Excluded and Included Across All Conditions |
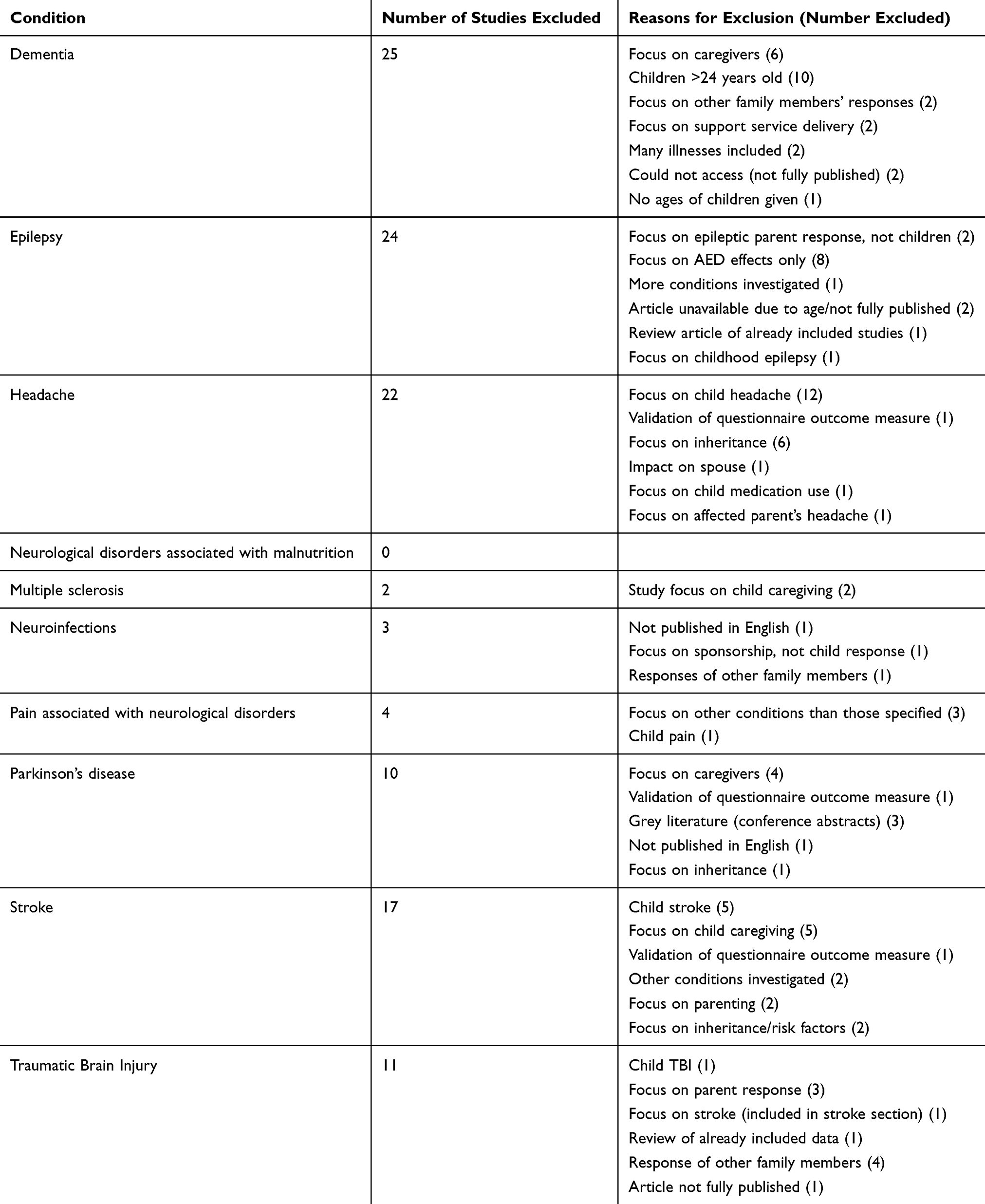 |
Table 2 Articles Excluded at Full-Text Screening Stage |
Outcomes Measured
Outcomes measured between studies varied greatly, for example, from parental psychopathology and child educational outcomes, to parental marital satisfaction and child behaviour. Some included studies did not focus on any particular outcomes at all, instead facilitating an “open” interview where the children were simply able to recount their experiences in their preferred manner.
Overview of results
The complete findings from all included studies are presented in Table 3. Child mood and anxiety disorders were common, with studies from the dementia,39 headache,55,58 multiple sclerosis,64–66 neuroinfections,74 Parkinson’s disease76,77 and traumatic brain injury89,92 searches all identifying an increased risk. Three of the 10 conditions also observed significant parent-child role reversal.30,33,38,39,53,57,76 Furthermore, many children sought to be well-informed regarding their parent’s condition and communicated with relevant services. This communication was evident in six conditions,34,41,49,52,71,73,78,82,85,94 but satisfaction with the information and services received was variable.33,37,50 Family cohesion, including the parental marital relationship, was also a significant factor in child responses for half of the 10 conditions.48,51,58,68,78,79,81,88 Parental psychopathology was also associated with poor child responses and stress.60,65,66,70,79-81,83,91,93 Female children were seen to be at an increased risk of psychiatric disorders, stress, or behavioural problems compared to males in four conditions.78–80,83,89 Multiple sclerosis was the only condition with a recent systematic review,33 concluding that affected children had generally negative psychosocial experiences.
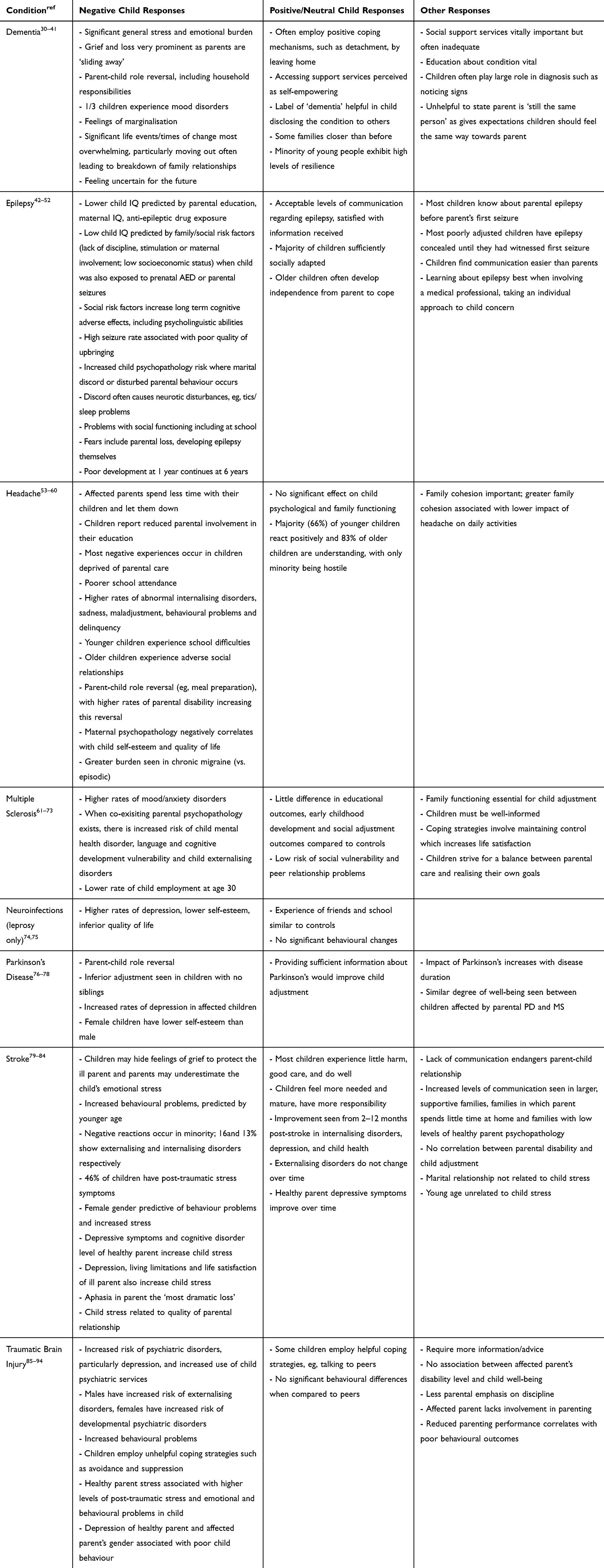 |
Table 3 Overview of Results for All Included Studies |
There were, however, some positive responses noted. These were limited but most evident in children of parental stroke, multiple sclerosis and dementia. Many of the children affected by parental stroke were seen to “do well long term”, with some responses even improving over time from 2 to 12 months.81–83 For parental multiple sclerosis, children seemed to show lower risks of social vulnerability.62,66,72 Positive responses tended to focus around the employment of useful coping mechanisms34,39,40 and the development of resilience in parental dementia.39
Discussion
Discussion by Parental Neurological Condition
The following commences with a summary of the potential implications of each parental condition for children, followed by a more general discussion of the results. Some limitations of the review process are subsequently highlighted, concluding with implications and recommendations based on the review results.
Dementia
The unique feeling of grief in children with dementia-affected parents was not seen in the other nine included neurological conditions.32,33,38,39 Whilst other conditions may be chronic and debilitating, no other condition causes such a profound behavioural change in the parent as dementia does. Parents are said to “slide away”.37 The availability of support services for parental loss whilst the parent is still alive may aid children through this grieving process. It may also be important to provide support to those children who are going through important life changes such as leaving the parental home or going to university, as such changes can cause significant disruption to the family unit.30,31
Epilepsy
The effects of in utero exposure to antiepileptic drugs (AEDs) accounted for most of the epilepsy research, of which most was excluded from this review. In the few-included studies that had a component exploring this, there was no clear distinction between the effects of AEDs on children, and child responses occurring as a result of solely social and psychological factors.43–47 It thus remains difficult to conclude the cause of specific child responses. Moreover, higher parental seizure frequency appears to be associated with greater impact on child outcomes.46 Responses could consequently change, dependent on the epilepsy severity. Additionally, epilepsy results from a diverse range of aetiologies, and the correlation between the aetiology/cause of epilepsy and the child response has so far been neglected.
Headache Disorders
Extrapolation of the results to include all headache disorders is inappropriate, as five of the seven included studies examined only parental migraine. It is most evident from included studies that headache can lead to a lack of parental care.53–55 There may be potential for this to be a causative factor in other observed outcomes such as school interference, internalising disorders, and parent-child role reversal. More support with parenting skills may thus improve child outcomes. Furthermore, the lone study that observed little effect on child functioning56 noted that their participants were recruited from the community (rather than clinics), where disability rates and child burden are less common.
Neurological Disorders Associated with Malnutrition
With no studies identified in this review, the lack of literature is most likely a result of the nature of malnutrition, which remains a problem in the developing world. Scarce resources are unlikely to be utilised in research relating to child responses to parental malnutrition when the problem of malnutrition itself has yet to be fully tackled.
Multiple Sclerosis
A diverse range of child responses to parental MS were observed, which may be a result of the variable nature of the condition. It is striking that recent evidence suggests more positive social outcomes for children than previously suggested.66,67,72 However, parental mental health appears to have a profound impact on children’s own emotional well-being, suggesting that parental mental health screening could be a useful tool to identify children most at risk themselves.
Neuroinfections
The virtual eradication of most neuroinfections in many first world nations has led to their effects being largely overlooked in the developing world. This is reflected in the paucity of literature reported here. Whilst negative psychosomatic experiences were found in children of parents with leprosy in one study,74 there were no behavioural changes observed in another.75 The participants in the latter study happened to be living in a care facility away from their parent, therefore their living situation, as opposed to the leprosy itself, may be the causative factor that facilitates behaviour similar to unaffected children.
Pain Associated with Neurological Disorders
A recent publication of Morley et al2 highlights the small field of literature concerning child response to more general chronic pain, something reflected in the results reported here, with no studies identified relating to parental neurological disorders associated with pain. Future research is required in this area in order to identify its potential impact on the offspring of affected parents.
Parkinson’s Disease
A unique finding in parental PD is the negative impact of a reduced number of siblings on adjustment.76 One study also observed that children of different ages perceived different problems78 which would be useful to follow up using longitudinal study designs. Furthermore, the impact of parental PD on children tends to increase with disease duration,78 perhaps due to its progressive nature.
Stroke
A largely positive response of children to parental stroke is apparent when compared to other parental conditions. This may be due to the nature of the condition itself; unlike other neurological disorders such as dementia, stroke rehabilitation is generally not degenerative, thus enabling children to adjust to the parental condition over time. The greatest risk factors of child maladjustment identified were female gender and parental status/stress, with this highlighting the need for a holistic family-orientated approach, when assessing the effect of parental stroke.
Traumatic Brain Injury
Parental TBI represented a negative picture of child responses. This was contrary to stroke. This could be due to the cause of the disorder: in TBI, “accidents” such as road collisions are a major cause,7 leading children to become angry and blame others. TBI may also be more severe, acute and restricting for the parent than other neurological disorders. By contrast, stroke may be deemed as more of an illness, and thus its causes seem more elusive. This may instead facilitate acceptance over time. One study of parental TBI did, however, find there to be no significant difference in child behavioural problems compared to controls.92 This study observed that affected parents often reported a lack of emphasis on discipline, perhaps leading them to believe lower standards of child behaviour are deemed as acceptable.
General Discussion
The review identified the use of predominantly cross-sectional study designs, which have particular limitations given that child responses are often reported to differ between age groups.60,78,80 There may also be natural variations at different stages of a child’s development, and cross-sectional studies might not account for a response that may not be wholly down to parental illness, but due to the more commonplace challenges of growing up.
Furthermore, a total of eight studies included in this review were fully proxy, with many more having a proxy element. Dementia was the only condition to have no proxy studies included in its results. It has been found that there is a greater degree of agreement between parent and child ratings of health-related quality of life (HRQoL) when they refer to observable functioning such as physical health, as opposed to non-observable functioning such as emotional/social HRQoL.95,96 This may significantly influence results obtained across the included studies, as most contained social or emotional elements. One study reported that children often hid their negative feelings to protect their affected parent;86 this could also occur in the context of study participation if a parent is taking part alongside their child.
The larger cohorts used in the studies assessing parental headache, as opposed to the smaller cohorts in dementia and stroke, may reflect a number of factors. Headache is far more prevalent than young-onset dementia or stroke, and its associated lack of mortality may result in children experiencing their entire youth with an affected parent whose condition does not become fatal. Both of these factors simply produce a larger pool of potential participants.
Studies focusing on parental dementia used exclusively qualitative methods. Whilst these methods can be useful in identifying themes and concepts in the early stages of research,97 they do not provide accurate, objective assessment of responses and cannot be generalised to the wider population in question. In a similar vein, the use of control groups was not common. These were seen most often within the MS category. This may simply be due to the more advanced stages of research in this parental condition. Such a study design enables a more objective comparison of child responses to unaffected control children. It is also notable that many studies did not control for variables such as socioeconomic status that are likely to play a role in determining overall child outcomes.
Epilepsy studies were markedly older than all other conditions, with the first published in 1984. It is important to consider the differences in society and in pressures on young people today, when compared with over 30 years ago,98 and the implications for changes in child responses. These differences may, in turn, influence child responses to parental illness. They may include factors such as the widespread use of technology facilitating improved access to information, and the opportunity to connect with other young people experiencing similar issues, and the destigmatisation of mental health issues enabling more open conversations regarding child psychopathology. Furthermore, only 10 of the 65 studies were carried out in the UK; this is vital to consider when informing guidelines intended for a particular population.
Limitations of the Structured Review Process
The structured review process itself does come with some inherent limitations. For example, it is difficult to account for publication bias. Furthermore, the process of study inclusion may have an element of subjectivity. The use of a data extraction form aimed to make this selection process as objective as possible. Additionally, the large range of outcome measures used did not lend itself to a simple and objective cross-comparison of results across different conditions. Interpretation of the results gleaned by the review is also somewhat limited due to the varying methodological quality of included studies. Objective quality appraisal of studies was challenging, as there is no standard for quality appraisal of observational studies in a systematic review.99 Instead, the use of more general variables (cohort size, the use of controls, proxy respondents, quantitative measurements and longitudinal design) enabled a surface quality assessment.
Implications and Future Recommendations
The varying child responses across parental disorders suggest that the production of broad, sweeping guidelines produced for children experiencing parental illness may be inappropriate. Instead, clinicians and service providers should recognise the differing nature of responses across conditions and produce individualised recommendations accordingly. The association between parental psychopathology and negative child responses highlights the need to produce family-focused guidelines.
Recommendations for future research include longitudinal and population-based studies. Quantitative measures would also provide a more objective approach, where standardised measures can be used to fit varying experiences of children into a limited set of categories, thereby enabling easier comparison. Outcome measures may thus need to be developed and validated for this purpose, as well as to identify children most at risk of adverse outcomes. Furthermore, conditions such as parental neurological pain and neuroinfections require research to begin. For the latter, child responses to widespread tropical neuroinfections, such as malaria, would be a useful start due to their high prevalence.
Conclusions
The comparison of child responses to a range of parental neurological disorders is challenging. The range of outcome measures, and methodological study designs, used across all 10 conditions varied greatly and thus only tentative conclusions can be drawn. This variation highlights the need for an individualised approach to children from a clinical perspective. From this review, it is evident that children generally respond negatively to parental neurological disorder. This is particularly apparent in the areas of child psychopathology, parent-child role reversal and behavioural problems, where parental psychopathology, female gender, and disrupted family cohesion were common risk factors. There were, however, some positive responses, which were most evident in parental stroke, multiple sclerosis and dementia. The quality of included studies varied greatly, with many containing significant methodological limitations. Future research should aim to clarify these findings, by employing more robust methods of longitudinal and population-based study design to identify those children most at risk of adverse responses.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
This review was internally funded in fulfilment of the University of Oxford Final Honours School Medical Sciences, Cell and Systems Biology and Neuroscience research project.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Firth P. Patients and their families. In: Stiefel F, editor. Communication in Cancer Care. Recent Results in Cancer Research. Vol. 168. Berlin, Heidelberg: Springer; 2006:61–71.
2. Morley D, Li X, Jenkinson C. Children and Young People’s Response to Parental Illness: A Handbook of Assessment & Practice. Boca Raton, FL: CRC Press; 2017.
3. Sieh DS, Visser-Meily JMA, Meijer AM. Differential outcomes of adolescents with chronically ill and healthy parents. J Child Fam Stud. 2013;22(2):209–218. doi:10.1007/s10826-012-9570-8
4. Barkmann C, Romer G, Watson M, Schulte-markwort M. Parental physical illness as a risk for psychosocial maladjustment in children and adolescents: epidemiological findings from a National Survey in Germany. Psychosomatics. 2007;48(6):476–481. doi:10.1176/appi.psy.48.6.476
5. Armistead L, Klein K, Forehand R. Parental physical illness and child functioning. Clin Psychol Rev. 1995;15(5):409–422. doi:10.1016/0272-7358(95)00023-I
6. Helseth S, Ulfsaet N. Having a parent with cancer: coping and quality of life of children during serious illness in the family. Cancer Nurs. 2003;26(5):355–362. doi:10.1097/00002820-200310000-00003
7. World Health Organization. Neurological Disorders: Public Health Challenges; 2006.
8. Janca A, Prilipko L, Costa e Silva JA. The World Health Organization’s global initiative on neurology and public health. J Neurol Sci. 1997;145(1):1–2. doi:10.1016/s0022-510x(96)00228-6
9. Grabiak BR, Bender CM, Puskar KR. The impact of parental cancer on the adolescent: an analysis of the literature. Psychooncology. 2007;16(2):127–137. doi:10.1002/(ISSN)1099-1611
10. Barker ED, Jaffee SR, Uher R, Maughan B. The contribution of prenatal and postnatal maternal anxiety and depression to child maladjustment. Depress Anxiety. 2011;28(8):696–702. doi:10.1002/da.20856
11. Betancourt TS, Meyers-Ohki SE, Charrow A, Hansen N. Annual research review: mental health and resilience in hiv/aids-affected children - a review of the literature and recommendations for future research. J Child Psychol Psychiatry. 2013;54(4):423–444. doi:10.1111/j.1469-7610.2012.02613.x
12. Aldridge J, Becker S. Children as carers: the impact of parental illness and disability on children’s caring roles. J Fam Ther. 1999;21(3):303–320. doi:10.1111/1467-6427.00121
13. Stewart JT. The frontal/subcortical dementias: common dementing illnesses associated with prominent and disturbing behavioral changes. Geriatrics. 2006;61(8):23–27.
14. Draper B, Withall A. Young onset dementia. Intern Med J. 2016;46(7):779–786. doi:10.1111/imj.2016.46.issue-7
15. Fisher RS, Van Emde Boas W, Blume W, et al. Epileptic seizures and epilepsy: definitions proposed by the International League Against Epilepsy (ILAE) and the International Bureau for Epilepsy (IBE). Epilepsia. 2005;46(4):470–472. doi:10.1111/epi.2005.46.issue-4
16. Lipton RB, Stewart WF, Scher AI. Epidemiology and economic impact of migraine. Curr Med Res Opin. 2001;17(Suppl 1):s4–s12. doi:10.1185/0300799039117005
17. Noseworthy J, Lucchinetti M, Rodriguez M, Weinshenker B. Multiple sclerosis. N Engl J Med. 2000;343(13):938–952. doi:10.1056/NEJM200009283431307
18. Grantham-McGregor S, Baker-Henningham H. Review of the evidence linking protein and energy to mental development. Public Health Nutri. 2005;8(7A):1191–1201. doi:10.1079/PHN2005805
19. Conserve DF, Teti M, Shin G, Iwelunmor J, Handler L, Maman S. A systematic review and narrative synthesis of interventions for parental human immunodeficiency virus disclosure. Front Public Health. 2017;5:187. doi:10.3389/fpubh.2017.00187
20. Rochat T, Netsi E, Redinger S, Stein A. Parenting and HIV. Curr Opin Psychol. 2017;15:155–161. doi:10.1016/j.copsyc.2017.02.019
21. Chi P, Li X. Parental HIV/AIDS: from psychopathology to resilience. In: Morley D, Li X, Jenkinson C, editors. Children’s & Young People’s Response to Parental Illness: A Handbook of Assessment & Practice. Boca Raton, FL: CRC Press; 2017:130–152.
22. Qiao S, Li X. Disclosure of parental illness to children: examples from HIV/AIDS. In: Morley D, Li X, Jenkinson C, editors. Children’s & Young People’s Response to Parental Illness: A Handbook of Assessment & Practice. Boca Raton, FL: CRC Press; 2017:171–204.
23. IASP Group. Pain terms: a list with definitions and notes on usage. Recommended by the IASP subcommittee on taxonomy. Pain. 1979;6(3):249.
24. Clarke CE, Moore AP. Parkinson’s disease. Am Fam Physician. 2007;75(7):1045–1048.
25. Grimshaw R. Children of Parents with Parkinson’s Disease. A Research Report for the Parkinson’s Disease Society. London, UK: National Children’s Bureau; 1991.
26. Cramer S, Chopp M. Recovery recapitulates ontogeny. Trends Neurosci. 2000;23(6):265–271. doi:10.1016/S0166-2236(00)01562-9
27. Fleminger S, Ponsford J. Long term outcome after traumatic brain injury. BMJ. 2005;331(7530):1419–1420. doi:10.1136/bmj.331.7530.1419
28. United Nations Educational, Scientific and Cultural Organisation. What do we mean by “youth”? Available from: http://www.unesco.org/new/en/social-and-human-sciences/themes/youth/youth-definition/.
29. Razaz N, Nourian R, Marrie RA, Boyce WT, Tremlett H. Children and adolescents adjustment to parental multiple sclerosis: a systematic review. BMC Neurol. 2014;14(1):107. doi:10.1186/1471-2377-14-107
30. Millenaar JK, Van Vliet D, Bakker C, et al. The experiences and needs of children living with a parent with young onset dementia: results from the NeedYD study. Int Psychogeriatr. 2014;26(12):2001–2010. doi:10.1017/S1041610213001890
31. Hall M, Sikes P. From “What the Hell Is Going on?” to the “Mushy Middle Ground” to “Getting Used to a New Normal”: young people’s biographical narratives around navigating parental dementia. Illn Crises Loss. 2018;26(2):124–144. doi:10.1177/1054137316651384
32. Hall M, Sikes P. “It Would Be Easier if She’d Died”: young people with parents with dementia articulating inadmissible stories. Qual Health Res. 2017;27(8):1203–1214. doi:10.1177/1049732317697079
33. Gelman CR, Rhames K. In their own words: the experience and needs of children in younger-onset Alzheimer’s disease and other dementias families. Dementia. 2018;17(3):337–358. doi:10.1177/1471301216647097
34. Johannessen A, Engedal K, Thorsen K. Coping efforts and resilience among adult children who grew up with a parent with young-onset dementia: a qualitative follow-up study. Int J Qual Stud Health Well-Being. 2016;11(1):30535. doi:10.3402/qhw.v11.30535
35. Sikes P, Hall M. “It was then that I thought ‘whaat? This is not my Dad”: the implications of the ‘still the same person’ narrative for children and young people who have a parent with dementia. Dementia. 2018;17(2):180–198. doi:10.1177/1471301216637204
36. Hutchinson K, Roberts C, Daly M, Bulsara C, Kurrle S. Empowerment of young people who have a parent living with dementia: a social model perspective. Int Psychogeriatr. 2016;28(4):657–668. doi:10.1017/S1041610215001714
37. Johannessen A, Engedal K, Thorsen K. Adult children of parents with young-onset dementia narrate the experiences of their youth through metaphors. J Multidiscip Healthc. 2015;8:245–254. doi:10.2147/JMDH.S84069
38. Hutchinson K, Roberts C, Kurrle S, Daly M. The emotional well-being of young people having a parent with younger onset dementia. Dementia. 2016;15(4):609–628. doi:10.1177/1471301214532111
39. Svanberg E, Stott J, Spector A. Just helping: children living with a parent with young onset dementia. Aging Ment Health. 2010;14(6):740–751. doi:10.1080/13607861003713174
40. Allen J, Oyebode JR, Allen J. Having a father with young onset dementia: the impact on well-being of young people. Dementia. 2009;8(4):455–480. doi:10.1177/1471301209349106
41. Denny SS, Morhardt D, Gaul JE, et al. Caring for children of parents with frontotemporal degeneration: a report of the AFTD task force on families with children. Am J Alzheimers Dis Other Demen. 2012;27(8):568–578. doi:10.1177/1533317512459791
42. Gopinath N, Muneer AK, Unnikrishnan S, Varma RP, Thomas SV. Children (10–12 years age) of women with epilepsy have lower intelligence, attention and memory: observations from a prospective cohort case control study. Epilepsy Res. 2015;117:58–62. doi:10.1016/j.eplepsyres.2015.09.003
43. Titze K, Koch S, Helge H, Lehmkuhl U, Rauh H, Steinhausen HC. Prenatal and family risks of children born to mothers with epilepsy: effects on cognitive development. Dev Med Child Neurol. 2008;50(2):117–122. doi:10.1111/j.1469-8749.2007.02020.x
44. Thomas SV, Sukumaran S, Lukose N, George A, Sarma PS. Intellectual and language functions in children of mothers with epilepsy. Epilepsia. 2007;48(12):2234–2240. doi:10.1111/j.1528-1167.2007.01376.x
45. Øyen N, Vollset SE, Eide MG, Bjerkedal T, Skjaerven R. Maternal epilepsy and offsprings’ adult intelligence: a population-based study from Norway. Epilepsia. 2007;48(9):1731–1738. doi:10.1111/j.1528-1167.2007.01130.x
46. Lösche G, Steinhausen HC, Koch S, Helge H. The psychological development of children of epileptic parents. II. The differential impact of intrauterine exposure to anticonvulsant drugs and further influential factors. Acta Paediatr. 1994;83(9):961–966. doi:10.1111/j.1651-2227.1994.tb13181.x
47. Steinhausen HC, Lösche G, Koch S, Helge H. The psychological development of children of epileptic parent I. Study design and comparative findings. Acta Paediatr. 1994;83(9):955–960. doi:10.1111/j.1651-2227.1994.tb13180.x
48. Thiels C, Steinhausen HC. Psychopathology and family functioning in mothers with epilepsy. Acta Psychiatr Scand. 1994;89(1):29–34. doi:10.1111/j.1600-0447.1994.tb01481.x
49. Lannon SL. Meeting the needs of children whose parents have epilepsy. J Neurosci Nurs. 1992;24(1):14–18. doi:10.1097/01376517-199202000-00005
50. Aldenkamp AP, Suurmeijer TPBM, Bijvoet ME, Heisen TWM. Emotional and social reactions of children to epilepsy in a parent. Fam Pract. 1990;7(2):110–115. doi:10.1093/fampra/7.2.110
51. Rogacheva TA, Boldyrev AI. Neurotic states in children whose parents suffer from epilepsy. Neurosci Behav Physiol. 1987;17(3):259–261. doi:10.1007/BF01191260
52. Lechtenberg R, Akner L. Psychologic adaptation of children to epilepsy in a parent. Epilepsia. 1984;25(1):40–45. doi:10.1111/epi.1984.25.issue-1
53. Buse DC, Powers SW, Gelfand AA, et al. Adolescent perspectives on the burden of a parent’s migraine: results from the CaMEO Study. Headache. 2018;58(4):512–524. doi:10.1111/head.2018.58.issue-4
54. Lipton RB, Bigal ME, Kolodner K, Stewart WF, Liberman JN, Steiner TJ. The family impact of migraine: population-based studies in the USA and UK. Cephalalgia. 2003;23(6):429–440. doi:10.1046/j.1468-2982.2003.00543.x
55. Arruda MA, Bigal ME. Migraine and behavior in children: influence of maternal headache frequency. J Headache Pain. 2012;13(5):385–400. doi:10.1007/s10194-012-0441-x
56. Smith KB, Chambers CT. Psychological and family functioning among children of parents with recurrent headaches. J Pain. 2006;7(9):635–643. doi:10.1016/j.jpain.2006.02.010
57. Fagan MA. Exploring the relationship between maternal migraine and child functioning. Headache. 2003;43(1):1042–1048. doi:10.1046/j.1526-4610.2003.03205.x
58. Mikail SF, von Baeyer CL. Pain, somatic focus, and emotional adjustment in children of chronic headache sufferers and controls. Soc Sci Med. 1990;31(1):51–59. doi:10.1016/0277-9536(90)90009-H
59. Smith R. Impact of migraine on the family. Headache. 1998;38(6):423–426. doi:10.1046/j.1526-4610.1998.3806423.x
60. Güngen BD, Aras YG, Gül SS, et al. The effect of maternal migraine headache on their children’s quality of life. Acta Neurol Belg. 2017;117(3):687–694. doi:10.1007/s13760-017-0790-y
61. Moberg JY, Larsen D, Brødsgaard A. Striving for balance between caring and restraint: young adults’ experiences with parental multiple sclerosis. J Clin Nurs. 2017;26(9–10):1363–1374. doi:10.1111/jocn.2017.26.issue-9pt10
62. Moberg JY, Magyari M, Koch-Henriksen N, Thygesen LC, Laursen B, Soelberg Sørensen P. Educational achievements of children of parents with multiple sclerosis: a nationwide register-based cohort study. J Neurol. 2016;263(11):2229–2237. doi:10.1007/s00415-016-8255-4
63. Moberg JY, Laursen B, Koch-Henriksen N, et al. Employment, disability pension and income for children with parental multiple sclerosis. Mult Scler. 2017;23(8):1148–1156. doi:10.1177/1352458516672016
64. Razaz N, Tremlett H, Boyce T, Guhn M, Marrie RA, Joseph KS. Incidence of mood or anxiety disorders in children of parents with multiple sclerosis. Paediatr Perinat Epidemiol. 2016;30(4):356–366. doi:10.1111/ppe.2016.30.issue-4
65. Razaz N, Tremlett H, Marrie RA, Joseph KS. Peripartum depression in parents with multiple sclerosis and psychiatric disorders in children. Mult Scler. 2016;22(14):1830–1840. doi:10.1177/1352458516631037
66. Razaz N, Joseph KS, Boyce WT, et al. Children of chronically ill parents: relationship between parental multiple sclerosis and childhood developmental health. Mult Scler. 2016;22(11):1452–1462. doi:10.1177/1352458515621624
67. Razaz N, Tremlett H, Boyce WT, Guhn M, Joseph KS, Marrie RA. Impact of parental multiple sclerosis on early childhood development: a retrospective cohort study. Mult Scler. 2015;21(9):1172–1183. doi:10.1177/1352458514559298
68. Boström K, Nilsagård Y. A family matter - when a parent is diagnosed with multiple sclerosis. a qualitative study. J Clin Nurs. 2016;25(7–8):1053–1061. doi:10.1111/jocn.2016.25.issue-7pt8
69. Mauseth T, Hjälmhult E. Adolescents’ experiences on coping with parental multiple sclerosis: a grounded theory study. J Clin Nurs. 2016;25(5–6):856–865. doi:10.1111/jocn.2016.25.issue-5pt6
70. Bogosian A, Hadwin J, Hankins M, Moss-morris R. Parents’ expressed emotion and mood, rather than their physical disability are associated with adolescent adjustment: a longitudinal study of families with a parent with multiple sclerosis. Clin Rehabil. 2016;30(3):303–311. doi:10.1177/0269215515580600
71. Nilsagård Y, Boström K. Informing the children when a parent is diagnosed as having multiple sclerosis. Int J MS Care. 2015;17(1):42–48. doi:10.7224/1537-2073.2013-047
72. Pakenham KI, Cox S. Comparisons between youth of a parent with MS and a control group on adjustment, caregiving, attachment and family functioning. Psychol Health. 2013;29(1):1–15. doi:10.1080/08870446.2013.813944
73. Horner R. Interventions for children coping with parental multiple sclerosis: a systematic review. J Am Assoc Nurse Pract. 2013;25(6):309–313. doi:10.1111/j.1745-7599.2012.00795.x
74. Yamaguchi N, Poudel KC, Jimba M. Health-related quality of life, depression, and self-esteem in adolescents with leprosy-affected parents: results of a cross-sectional study in Nepal. BMC Public Health. 2013;13(1):22. doi:10.1186/1471-2458-13-22
75. Mahajan BB, Garg G, Gupta RR. A study of behavioural changes and clinical evaluation of leprosy in school going children of leprosy parents. Indian J Dermatol Venereol Leprol. 2002;68(5):279–280.
76. Morley D, Jenkinson C. Furthering our understanding of the needs of adolescent children of parents with parkinson’s disease. Adolesc Health Med Ther. 2013;4:74–77.
77. Morley D, Selai C, Schrag A, Jahanshahi M, Thompson A. Adolescent and adult children of parents with parkinson’s disease: incorporating their needs in clinical guidelines. Parkinsons Dis. 2011;2011:951874. doi:10.4061/2011/153979
78. Schrag A, Morley D, Quinn N, Jahanshahi M. Impact of parkinson’s disease on patients’ adolescent and adult children. Parkinsonism Relat Disord. 2004;10(7):391–397. doi:10.1016/j.parkreldis.2004.03.011
79. Sieh DS, Meijer AM, Visser-Meily JMA. Risk factors for stress in children after parental stroke. Rehabil Psychol. 2010;55(4):391–397. doi:10.1037/a0020918
80. Visser-Meily A, Post M, Meijer AM, Maas C, Ketelaar M, Lindeman E. Children’s adjustment to a parent’s stroke: determinants of health status and psychological problems, and the role of support from the rehabilitation team. J Rehabil Med. 2005;37(4):236–241. doi:10.1080/16501970510025990
81. Visser-Meily A, Post M, Meijer AM, van de Port I, Maas C, Lindeman E. When a parent has a stroke: clinical course and prediction of mood, behavior problems, and health status of their young children. Stroke. 2005;36(11):2436, 2440. doi:10.1161/01.STR.0000185681.33790.0a
82. Kitzmüller GK, Asplund K, Häggströ T. The long-term experience of family life after stroke. J Neurosci Nurs. 2012;44(1):E1–E13. doi:10.1097/JNN.0b013e31823ae4a1
83. van de Port IGL, Visser-meily AMA, Post MWM, Lindeman E. Long-term outcome in children of patients after stroke. J Rehabil Med. 2007;39(9):703–707. doi:10.2340/16501977-0109
84. Harlow A, Murray LL. Addressing the needs of adolescent children when a parent becomes aphasic: one family’s experiences. Top Stroke Rehabil. 2001;7(4):46–51. doi:10.1310/3V28-6BQ5-CWPG-V3UF
85. Takanashi S, Sakka M, Sato I, et al. Factors influencing mother–child communication about fathers with neurobehavioural sequelae after brain injury. Brain Inj. 2017;31(3):312–318. doi:10.1080/02699052.2016.1225986
86. Kieffer-Kristensen R, Johansen KLG. Hidden loss: a qualitative explorative study of children living with a parent with acquired brain injury. Brain Inj. 2013;27(13–14):1562–1569. doi:10.3109/02699052.2013.841995
87. Kieffer-Kristensen R, Teasdale TW, Bilenberg N. Post-traumatic stress symptoms and psychological functioning in children of parents with acquired brain injury. Brain Inj. 2011;25(7–8):752–760. doi:10.3109/02699052.2011.579933
88. Redolfi A, Bartolini G, Gugliotta M, et al. When a parent suffers ABI: investigation of emotional distress in children. Brain Inj. 2017;31(8):1050–1060. doi:10.1080/02699052.2017.1297486
89. Kinnunen L, Niemelä M, Hakko H, et al. Psychiatric diagnoses of children affected by their parents’ traumatic brain injury: the 1987 Finnish Birth Cohort study. Brain Inj. 2018;32(7):933–940. doi:10.1080/02699052.2018.1470331
90. Niemelä M, Kinnunen L, Paananen R, et al. Parents’ traumatic brain injury increases their children’s risk for use of psychiatric care: the 1987 Finnish Birth Cohort study. Gen Hosp Psychiatry. 2014;36(3):337–341. doi:10.1016/j.genhosppsych.2013.12.012
91. Kieffer-Kristensen R, Siersma VD, Teasdale TW. Family matters: parental-acquired brain injury and child functioning. NeuroRehabilitation. 2013;32(1):59–68. doi:10.3233/NRE-130823
92. Uysal S, Hibbard MR, Robillard D, Pappadopulos E, Jaffe M. The effect of parental traumatic brain injury on parenting and child behavior. J Head Trauma Rehabil. 1998;13(6):57–71. doi:10.1097/00001199-199812000-00007
93. Pessar LF, Coad ML, Linn RT, Willer BS. The effects of parental traumatic brain injury on the behaviour of parents and children. Brain Inj. 1993;7(3):231–240. doi:10.3109/02699059309029675
94. Rohleder P, Lambie J, Hale E. A qualitative study of the emotional coping and support needs of children living with a parent with a brain injury. Brain Inj. 2017;31(2):199–207. doi:10.1080/02699052.2016.1225985
95. Eiser C, Morse R. Can parents rate their child’s health-related quality of life? Results of a systematic review. Qual Life Res. 2001;10(4):347–357. doi:10.1023/A:1012253723272
96. Galloway H, Newman E. Is there a difference between child self-ratings and parent proxy-ratings of the quality of life of children with a diagnosis of attention-deficit hyperactivity disorder (ADHD)? A systematic review of the literature. Atten Defic Hyperact Disord. 2017;9(11):11–29. doi:10.1007/s12402-016-0210-9
97. Golafshani N. Understanding reliability and validity in qualitative research. Qual Rep. 2003;8(4):597–606.
98. Scott J. Is it a different world to when you were growing up? Generational effects on social representations and child-rearing values. Br J Sociol. 2000;51(2):355–376. doi:10.1080/00071310050030226
99. Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. PRISMA 2009 flow diagram. PLoS Med. 2009;6(7):e1000097. doi:10.1371/journal.pmed.1000097
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.