Back to Journals » Journal of Asthma and Allergy » Volume 16
Yellow Urticaria: A Systematic Review
Authors Kulthanan K ![]() , Tanwandee T
, Tanwandee T ![]() , Chularojanamontri L, Panjapakkul W, Saengthong-aram P
, Chularojanamontri L, Panjapakkul W, Saengthong-aram P ![]()
Received 6 June 2023
Accepted for publication 1 September 2023
Published 8 September 2023 Volume 2023:16 Pages 973—978
DOI https://doi.org/10.2147/JAA.S424360
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Luis Garcia-Marcos
Kanokvalai Kulthanan,1 Tawesak Tanwandee,2 Leena Chularojanamontri,1 Waratchaya Panjapakkul,1 Phuwakorn Saengthong-aram1
1Department of Dermatology, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; 2Division of Gastroenterology, Department of Internal Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Kanokvalai Kulthanan, Department of Dermatology, Faculty of Medicine Siriraj Hospital, Mahidol University, 2 Wanglang Road, Bangkok Noi, Bangkok, 10700, Thailand, Tel +66 2 419 4333, Fax +66 2 411 5031, Email [email protected]
Urticaria is defined as the development of wheals, angioedema or both. A wheal is characterized by a circumscribed superficial edema of the skin, often surrounded by a red erythema (flare) with association of itching or sometime burning sensation. With transient nature, the individual wheal resolves to normal skin within 30 minutes to 24 hours. Acute urticaria is considered as an appearance of wheals, angioedema or both with duration up to 6 weeks, while chronic urticaria is characterized by the recurrence of lesions over more than 6 weeks. Urticaria can be caused by various factors.1
“Yellow urticaria” does not represent a distinct disease; rather, it refers to the yellow-colored wheals that manifest in certain patients with hyperbilirubinemia. Yellow urticaria is a rare disease, with a scarcity of comprehensive studies investigating this phenomenon. The pathogenesis of yellow urticaria remains poorly understood, with limited available information on its underlying mechanisms.2 To address this knowledge gap, a systematic review was conducted to examine the pathogenesis, clinical characteristics and natural progression of patients presenting with yellow urticaria.
The systematic review was conducted per the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement guidelines. A systematic search in the PubMed, Embase, and Scopus databases to identify studies published up until March 2023 was performed. The search terms used were “hyperbilirubinemia”, “jaundice”, “cirrhosis”, “hepatitis”, “urticaria”, “yellow urticaria”, “allergic reaction”, “hypersensitivity”, and “anaphylaxis”. This search yielded 43 353 articles (PubMed 11 886, Embase 11 403, and Scopus 20 064). Duplicate articles and those deemed irrelevant were excluded from the review. Articles that included wheals, angioedema, or both, particularly those with yellow wheals, were prioritized. The inclusion criteria were (1) reports of patients with yellow wheals, with or without angioedema, and with hyperbilirubinemia or jaundice; and (2) information on patient characteristics or the natural course of the wheals. Titles and abstracts that met both criteria were independently screened by three investigators (KK, WP, PS), with disagreements resolved through consensus. The same investigators then independently reviewed the full-text versions of articles deemed relevant to determine their final eligibility (Figure 1).
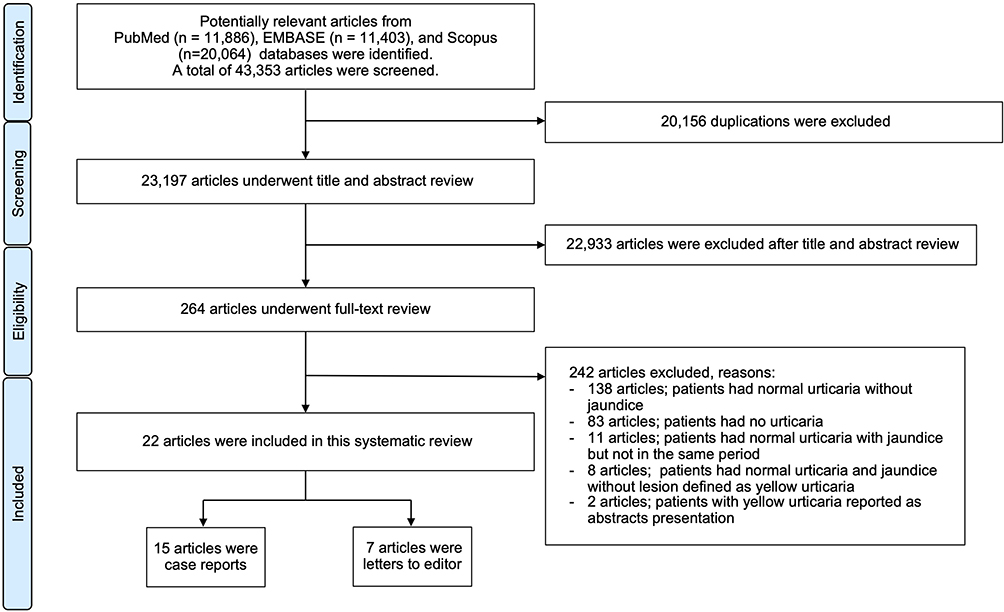 |
Figure 1 Flow chart of the study selection process. |
Upon applying the inclusion criteria, 22 publications were selected for analysis. The quality of the nonrandomized controlled trials (non-RCTs) and pre-post intervention studies we reviewed was assessed by the Methodological Index for Nonrandomized Studies (MINORS), with results shown in Table S1. The 15 case reports and 7 letters to the editor reported a total of 25 patients (Table S2).
The same investigators independently reviewed the following data from each article: (1) first author’s name and year of publication; (2) number of reported patients with yellow urticaria; (3) onset and cause of wheals; (4) cause of jaundice; (5) laboratory investigations, including complete blood count, liver function test, skin biopsy and bilirubin staining; (6) treatment of yellow urticaria; and (7) duration of wheal resolution and yellow pigmentation resolution. Descriptive statistics were performed (eg. percentage, mean, median, standard deviation, and range) to illustrate demographic data, cause of disease, investigations, and treatment.
Of the 25 patients, 68% (17) were male. Pre-existing hepatic and biliary diseases were found in 72% of patients (12 males and 6 females) (Table 1). The most common pre-existing condition was cirrhosis (61.1%), with alcoholic cirrhosis particularly prevalent. Liver cancer (16.7%) and viral hepatitis (5.6%) were the next most common.
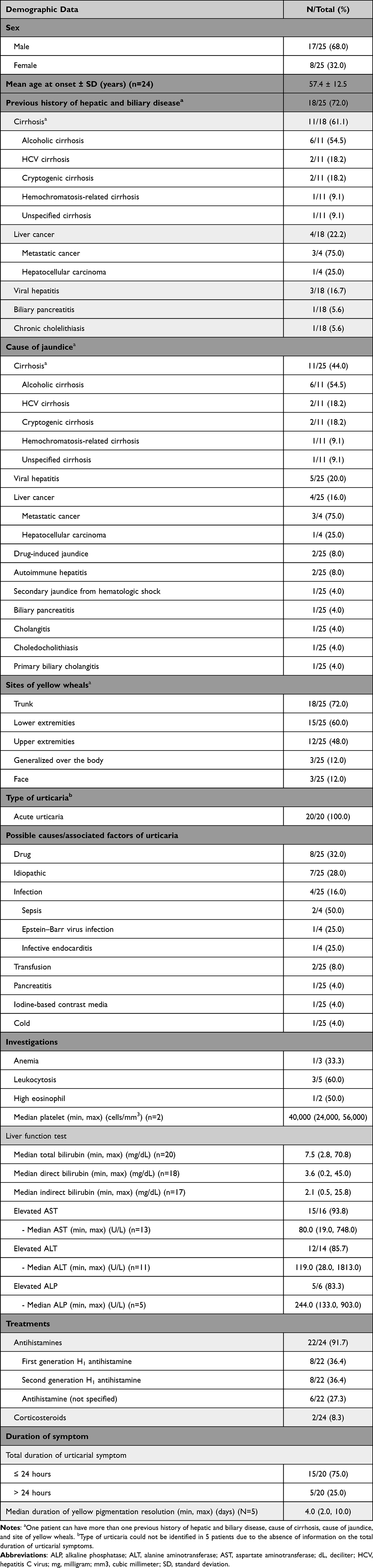 |
Table 1 Demographic Data, Clinical Manifestations, Investigations, and Treatments of Patients with Yellow Urticaria (n=25) |
All cases displayed hyperbilirubinemia (a total bilirubin level exceeding 2.0 mg/dL). The median bilirubin level was 7.5 mg/dL (range 2.8–70.8 mg/dL). The causes of jaundice varied among the patients, and an individual patient may have had multiple causes. Cirrhosis was the most prevalent cause (44.0%), followed by viral hepatitis (20.0%). The remaining patients had other pathological diseases leading to hyperbilirubinemia.
Jaundice types were reported for 18 patients, with 94.7% (17/18) exhibiting direct or conjugated hyperbilirubinemia. Only one patient presented with unconjugated hyperbilirubinemia, resulting from antiretroviral therapy. Among the 15 patients with sclera color data, 14 exhibited icteric sclera. The exception was one patient with a bilirubin level of 2.8 mg/dL, who displayed normal sclera color.
All 25 cases presented with yellow wheals as the first episode, without any non-yellowish ordinary wheals. Ordinary urticaria is characterized by skin-colored/erythematosus wheals surrounded by a red erythema (flare). Yellow urticaria is different from ordinary urticaria in that it presents with yellow-colored wheal (Figure S1). Each of the 20 patients with available data on urticarial symptom duration experienced acute urticaria. However, one patient had a history of chronic cold-induced urticaria for some months before developing acute yellow wheals, which were accompanied by hyperbilirubinemia resulting from infectious hepatitis.
Among the 25 cases, drugs (32.0%) and infections (16%) were frequently identified as possible causes or associated factors of urticaria; however, 28% of cases were idiopathic. The most common site of wheals was the trunk (18/25; 72.0%), followed by the lower extremities (15/25; 60.0%). Antihistamines were the most commonly prescribed medications (91.7%), with 8 cases treated using oral second-generation H1 antihistamines.
Most cases (75.0%) displayed resolution of urticarial symptoms within 24 hours, with a residual yellow pigmentation persisting for a median duration of 4 days (range 2–10 days). Skin biopsies from yellow wheals were conducted in 7 patients. Hall’s stain, which demonstrates bile staining in tissue, was applied in 4 of these cases. Olive-green crystals in the dermis tested positive in 2 cases, with bilirubin levels of 5.3 mg/dL and 8.4 mg/dL. It should be noted that biopsy and staining were not deemed obligatory for diagnosing yellow urticaria, as the primary basis for diagnosis was clinical.
The pathogenesis of yellow urticaria remains uncertain. Some authors have suggested that elevated serum bile acid levels may directly activate mast cell degranulation, triggering urticaria,3 while others have argued that bilirubin’s antioxidant and anti-inflammatory properties may alleviate urticaria.4 It has been proposed that the yellow coloration of the disease may result from the increased capillary permeability that cytokines and mediators, especially histamine, induce. These agents are released during the mast cell degranulation that occurs during wheal development. The increased capillary permeability may lead to bilirubin diffusing into the dermis and subsequently depositing in elastin.5 Bilirubin exhibits an affinity for binding with elastin in the dermis, resulting in a yellow hue similar to the cause of icteric sclera. Elastin is also abundant in the sclera, which typically becomes yellow when the bilirubin level reaches 3 mg/dL.6
The correlation between the development of yellow wheals and bilirubin levels remains unclear. Although most patients who develop yellow wheals exhibit hyperbilirubinemia and icteric sclera, there have been reported cases of non-yellowish ordinary wheals in individuals with bilirubin levels as high as 9.3 mg/dL, without any occurrence of yellow wheals.7
In conclusion, yellow-colored wheals, typically presenting as acute urticaria, can occur in association with hepatic and biliary diseases. Hyperbilirubinemia is consistently detected, and most patients display icteric sclera. Antihistamines are the mainstay treatment for yellow urticaria, as is the case for non-yellowish ordinary urticaria.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon request.
Funding
This research did not receive specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
All authors declare that there are no conflicts of interest related to this study.
References
1. Zuberbier T, Abdul Latiff AH, Abuzakouk M, et al. The international EAACI/GA²LEN/EuroGuiDerm/APAAACI guideline for the definition, classification, diagnosis, and management of urticaria. Allergy. 2022;77(3):734–766. doi:10.1111/all.15090
2. Mendes L, João GAP, Oliveira LM. Yellow urticaria in a patient on prophylactic antiretroviral therapy. An Bras Dermatol. 2018;93(4):618–619. doi:10.1590/abd1806-4841.20187573
3. Quist RG, Ton-Nu HT, Lillienau J, Hofmann AF, Barrett KE. Activation of mast cells by bile acids. Gastroenterology. 1991;101(2):446–456. doi:10.1016/0016-5085(91)90024-F
4. Ziberna L, Martelanc M, Franko M, Passamonti S. Bilirubin is an endogenous antioxidant in human vascular endothelial cells. Sci Rep. 2016;6(1):29240. doi:10.1038/srep29240
5. Hardy S, King R, Scholand S. Yellow urticaria in a patient with liver disease. Case Rep Clin Pract. 2022;11(04):101–105.
6. Joseph A, Samant H. Jaundice. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023. Available from: https://www.ncbi.nlm.nih.gov/books/NBK544252/.
7. Lockshin NA, Hurley H. Urticaria as a sign of viral hepatitis. Arch Dermatol. 1972;105(4):570–571. doi:10.1001/archderm.1972.01620070042014
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.