Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
Xietu Hemu Prescription Improves Metabolic Dysfunction-Associated Steatotic Liver Disease: A Real-World Cohort Study
Authors Xiang LL, Cao YT, Wang XX, Wang GX, Zhang YJ, Li RH, Qi F, Huai JX ![]() , Sun J, He XJ, Zhou XQ
, Sun J, He XJ, Zhou XQ ![]()
Received 20 March 2025
Accepted for publication 7 July 2025
Published 29 July 2025 Volume 2025:18 Pages 4377—4389
DOI https://doi.org/10.2147/JMDH.S522519
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Liu-lan Xiang,1,2,* Yu-tian Cao,1,2,* Xiao-xiao Wang,3,* Gao-xiang Wang,1,* Yu-juan Zhang,4 Rui-han Li,1,2 Fang Qi,5 Jia-xuan Huai,1,2 Jing Sun,1,2 Xiao-jin He,3 Xi-qiao Zhou1
1Department of Endocrinology, Affiliated Hospital of Nanjing University of Chinese Medicine, Jiangsu Province Hospital of Chinese Medicine, Nanjing, People’s Republic of China; 2The First Clinical Medical College of Nanjing University of Chinese Medicine, Nanjing, People’s Republic of China; 3Affiliated Hospital of Nanjing University of Chinese Medicine, Jiangsu Province Hospital of Chinese Medicine, Nanjing, People’s Republic of China; 4Department of Endocrinology, Seventh People’s Hospital of Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 5Department of Geriatrics, Panjin Liao-Oil Field Gem Flower Hospital, Liaoning, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xi-qiao Zhou, Email [email protected] Xiao-jin He, Email [email protected]
Purpose: This study aims to evaluate the efficacy of the Xietu Hemu prescription (XHP) in improving metabolic dysfunction-associated steatotic liver disease (MASLD) through a Real World Study approach.
Methods: This was a single-center, prospective, real-world cohort study of 262 patients with MASLD who met the inclusion and exclusion criteria from November 2021 to November 2023 at Jiangsu Provincial Hospital of Traditional Chinese Medicine. The exposure of this study was who took the XHP. We assessed the efficacy of the XHP on MASLD by comparing FibroScan parameters, body composition indicators, and liver serological indicators. The XHP was then evaluated for MASLD by inverse probability of treatment weighting (IPTW) as well as log-binomial analysis.
Results: We ended up collecting the exposure cohort (n=163) and the referent cohort (n=99). Patients were categorized into an exposure cohort (n=163, XHP + basic treatment) subdivided by treatment duration: 4 weeks (n=28), 8 weeks (n=60), 12 weeks (n=51), and ≥ 16 weeks (n=24), and a referent cohort (n=99, basic treatment alone). The results showed significant improvements in Liver stiffness measurement (LSM), controlled attenuation parameter (CAP), body mass index (BMI), waist-to-hip ratio (WHR), visceral fat area (VFA), the fatty liver index (FLI), and FibroScan-AST (FAST) in the exposure cohort after treatment compared to before treatment. After controlling confounding by IPTW, log-binomial analysis revealed that XHP administration was significantly more effective for MASLD in the exposure cohort than in the referent cohort (weighted risk ratio=2.99, 95% CI=1.86 to 4.89, p< 0.001). Subgroup analyses revealed a significantly greater efficacy of the XHP in the exposure cohort compared to the MASLD referent cohort, across various durations and dosages of XHP and varying degrees of hepatic steatosis and fibrosis. No serious adverse events occurred; occasional mild gastrointestinal reactions were self-limiting.
Conclusion: The results of our study suggest that XHP has a significant treatment effect on MASLD, which hopes to complement the current lack of treatment for MASLD.
Keywords: MASLD, Xietu Hemu prescription, efficacy, real-world study, Chinese medicine
Introduction
Metabolic dysfunction-associated steatotic liver disease (MASLD), formerly known as non-alcoholic fatty liver disease (NAFLD),1 affects the health of 1/3 of the world’s population.2 MASLD is defined as the presence of excess triglyceride storage in the liver in the presence of at least one cardiometabolic risk factor.3 MASLD is becoming the fastest-growing factor in the burden of disease associated with adverse liver outcomes, including cirrhosis, liver failure, and hepatocellular-cancer (HCC).4 It has also been shown that there is an association between MASLD and other disease processes,5 such as cardiovascular disease, peripheral vascular disease, chronic kidney disease, and some cancers, especially those of the gastrointestinal tract.6 Therefore, it is urgent to find more treatments for MASLD.
However, current therapeutic options for MASLD face significant limitations. Lifestyle modifications involving diet and exercise are the cornerstone of management, yet long-term adherence remains challenging.7 While numerous novel agents are under investigation, there remains an unmet need for effective, well-tolerated, and widely applicable treatments.8 This treatment gap highlights the potential value of complementary approaches such as TCM, which offers multi-targeted interventions that have been clinically validated.
Traditional Chinese medicine (TCM) has a long history of being commonly used in the treatment of MASLD due to its multi-target nature and clinical efficacy. The Xietu Hemu prescription (XHP) (national patent ZL 2022 1 0250245.4), developed at Jiangsu Province Hospital of Chinese Medicine, integrates two classical formulas: Shen Ling Baizhu San (SLBS) for spleen fortification and dampness resolution, and Chaihu Shugan San (CSS) for liver-soothing and qi-regulation. Pharmacological studies of key components, including Codonopsis extract9,10 and Nuciferine,11 demonstrate insulin resistance mitigation and hepatic inflammation reduction. Experimental research confirms SLBS improves lipid metabolism,12 while CSS modulates miRNA expression to reduce fatty acid biosynthesis.13 This prescription is specifically indicated for MASLD patients with TCM-diagnosed “spleen deficiency phlegm-dampness syndrome”.
In recent years, real word study (RWS) has been rapidly emerging worldwide. It has been widely used in the fields of studying the actual applicable population or syndrome of drugs, evaluating the modern application of ancient classics of traditional Chinese medicine, and the research and development and evaluation of new drugs and hospital preparations, courses of treatment, and follow-up outcomes14. To further clarify the effectiveness of XHP on MASLD, our team conducted an prospective RWS cohort study of patients with MASLD with “spleen deficiencyphlegm-dampness syndrome” in the last 2 years.
Methods
Study Design and Data Sources
This study was conducted to follow up on the cases of patients who were diagnosed with “MASLD (spleen deficiencyphlegm-dampness syndrome)” during November 2021 and November 2023 in the endocrine clinic of Jiangsu Province Hospital of Chinese Medicine, and to collect and organize the data of the patients’ medical records.Ethical review and approval for this study were obtained from the Jiangsu Province Hospital of Chinese Medicine under approval number 2022NL-122-02. Additionally, the study was registered with the International Traditional Medicine Clinical Trial Registry (ITMCTR2024000877). The study followed the recommended guidelines for observational studies using routinely collected health data (Additional File 1)15 and the Declaration of Helsinki. Patient characteristics, prescription drug use, covariate information, and outcome data were obtained from outpatient medical records of the Department of Endocrinology, Jiangsu Province Hospital of Chinese Medicine. Information on hospital admissions and diagnoses are coded by trained personnel using the International Classification of Diseases, 11th Revision (ICD-11) system code DB92, and diagnoses were simultaneously referenced to the multisociety Delphi consensus statement on new fatty liver disease nomenclature;1 definition of Chinese medicine diagnosis by professional Chinese medicine practitioners with senior qualifications.
Patients
The primary cohort consisted of patients aged 18–75 years with a diagnosis of MASLD and a TCM diagnosis of spleen deficiency phlegm-dampness syndrome. Patients were stratified based on disease severity using FibroScan CAP (steatosis grade: S0-3) and LSM (fibrosis stage: F0-4).16,17 The prescription fill date was the patient’s cohort entry date (the index date); patients could enter the cohort only once. The indicators used are all measurements taken within 7 days before and after the indicator date. Excluded were (1) those who were using medications associated with secondary MASLD (corticosteroids, estrogens, amiodarone, methotrexate), etc; (2) those who had a combination of alcoholic fatty liver disease, viral hepatitis, autoimmune liver disease, or liver tumors that resulted in impaired hepatic function; (3) women who were pregnant or breastfeeding.
Transient elastography (FibroScan) with CAP and LSM measurements was selected as the primary diagnostic tool due to its non-invasive nature, widespread clinical adoption for MASLD quantification, and validated accuracy in steatosis and fibrosis assessment.16,18 While liver biopsy remains the gold standard, FibroScan offers practical advantages including repeatability, cost-effectiveness, and avoidance of procedure-related risks, making it suitable for real-world longitudinal observation.19 Limitations include potential inaccuracy in severe obesity (BMI>35 kg/m²) and operator dependency, which were mitigated by using standardized protocols performed by trained technicians following manufacturer guidelines.
The Xietu Hemu prescription used by the patient was customized from Jiangsu Province Hospital of Chinese Medicine, with standardized specifications as a concentrated preparation. It is to be taken at a dosage of 10g, 30 minutes after breakfast and dinner daily (details of the prescription composition is Additional File 2). To ensure the standardized use of patients, the investigator will follow up with phone calls every 2 weeks.
Groups and Endpoint Event
In this study, XHP administration was used as the exposure factor, and 90 patients were needed for each of the exposure cohort and referent cohort calculated based on retrospective analysis of the previous clinical data (Additional File 3). Subgroup analyses by treatment duration were exploratory and not included in the sample size calculation due to statistical power considerations. The final sample size exceeded the minimum requirement (exposure cohort: n=163; referent cohort: n=99). All patients received standardized basic treatment including dietary counseling (calorie-restricted Mediterranean diet) and physical activity recommendations (≥150 mins/week moderate exercise). Concomitant medications for comorbidities were recorded and balanced through IPTW analysis.
This is a RWS with no special restrictions on the patient’s basic treatment, and the impact of errors arising from different medications and underlying diseases will be reduced by statistical methods to minimize the impact. To participate in this study, patients must take a stabilized dose of the medication every day and have their metabolic markers, and body composition tested on a periodic schedule. The following were the medication methods of the different groups:
- Exposure cohort: Patients with MASLD who fulfilled the inclusion and exclusion criteria and used XHP according to the dosing regimen.
- Referent cohort: Patients with MASLD who fulfilled the inclusion and exclusion criteria and did not used XHP.
This study was a RWS, and the diagnostic tool for MASLD in this study was Fibroscan, taking into account the economic pressure on patients and the preference for noninvasive diagnosis. Transient elastography (Fibroscan, TE) with liver stiffness measurement (LSM) and controlled attenuation parameter (CAP) has demonstrated good accuracy in quantifying the levels of liver steatosis and fibrosis in patients with MASLD.16,18 According to the references,17,20 when the absolute liver fat was reduced by 4.1%, there was a significant improvement in histologic steatosis and ballooning degeneration in patients with MASLD. Therefore, this study set an absolute CAP reduction of ≥4.1% as efficacious, which was the endpoint event of the cohort study.
Other covariates included: (1) Liver stiffness measurement (LSM); (2) body composition indicators: body mass index (BMI), waist-to-hip ratio (WHR), visceral fat area (VFA); (3) liver serum biomarkers: Fibrosis 4 Index (FIB-4),20 NAFLD Fibrosis Score (NFS),21 the FibroScan-AST (FAST) score,22 and the Fatty Liver Index (FLI).23 The serum biochemical indexes were measured by the automatic biochemical analyzer of the Laboratory Department of Jiangsu Province Hospital of Chinese Medicine. Body composition was determined by InBody 770 under constant conditions (proper hydration and the same time of day).
Adverse events are also closely monitored during follow-up visits and promptly documented. Gastrointestinal reactions were systematically evaluated using the Common Terminology Criteria for Adverse Events (CTCAE v5.0), specifically documenting nausea, epigastric discomfort, and diarrhea. Events were graded and managed according to protocol.
Statistical Analysis
For the statistical description in this study, continuous variables were reported as means ± standard deviation for normally distributed data and as medians (25th–75th percentiles) for data with skewed distribution. The normality of data distribution was assessed using the Shapiro–Wilk test. Independent and paired t-tests were used to assess between- and within-group differences in normally distributed data, and Wilcoxon’s rank-sum and paired rank-sum tests were used to evaluate between- and within-group differences in non-normally distributed data. Then Directed Acyclic Graph (DAG) model,24 Change-in-Effects method CIE (Change-in-Estimate)25 were used to find confounding factors and analyzed using inverse probability treatment weighting (IPTW)26 to control for confounding, while a log-binomial regression analysis was later performed to explore the relationship between XHP effective on MASLD. Data were analyzed statistically by applying SPSS 25.0 and R4.3.2. P<0.05 was considered statistically significant.
Results
Patient Characteristics
Between November 2021 and November 2023, 632 patients visited the Department of Endocrinology of Jiangsu Province Hospital of Chinese Medicine, and that these patients met the MASLD and TCM diagnoses. The final analyses included a total of 262 patients who fulfilled all the study inclusion and exclusion criteria. Among these, 163 and 99 patients were included in the exposure cohort (XHP+basic treatment) and referent cohort (basic treatment alone), respectively. Furthermore, the exposure cohort collected 28, 60, 51, and 24 patients based on the duration of XHP administration (4 weeks, 8 weeks, 12 weeks, and more than 16 weeks) (Figure 1).
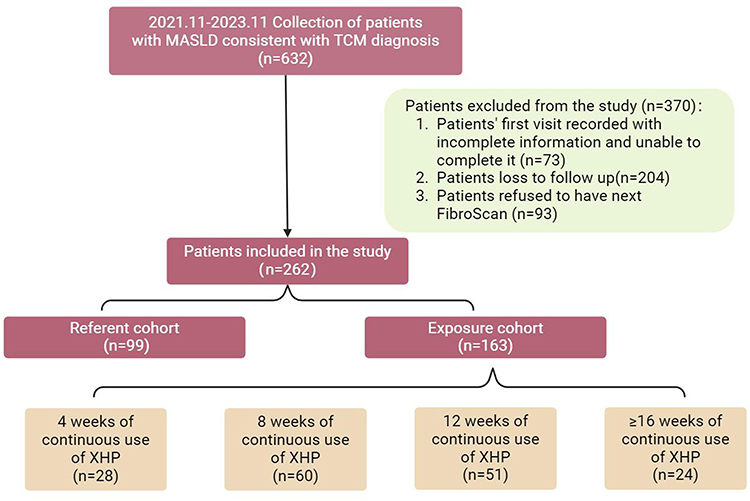 |
Figure 1 Flowchart of the selection process of the study population. |
According to the results of baseline analysis, clinical characteristics and metabolic profiles, concomitant therapy, and TCM syndrome score were analyzed at baseline (Table 1; Additional File 4). The results showed that in “whether combined hypertension”, “whether combined Hashimoto’s thyroiditis”, “whether using SGLT-2i”, “whether Euthyrox”, there was a difference between the two cohorts (p<0.05), and the rest of the exposure cohort and referent cohort were not significantly different.
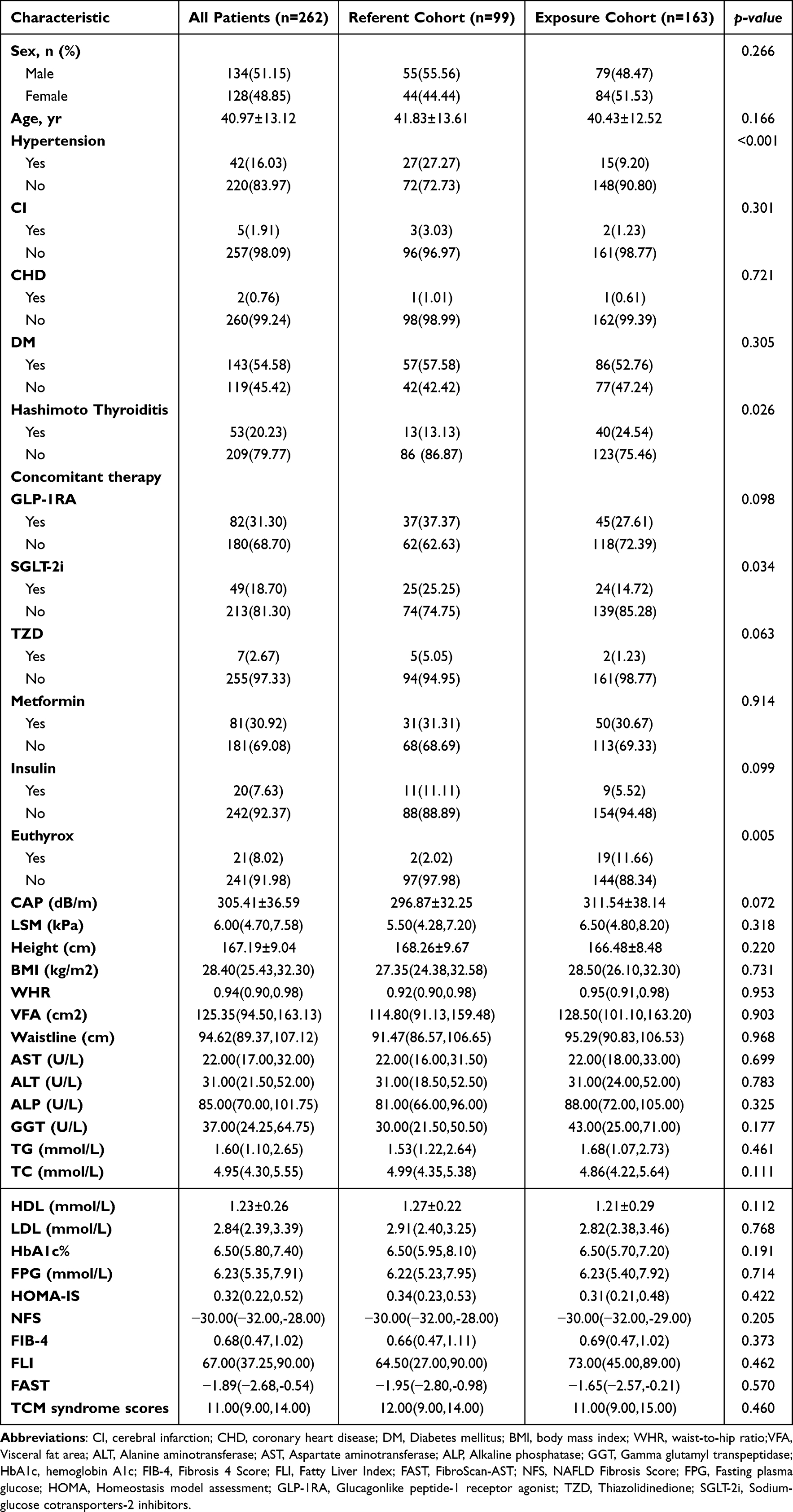 |
Table 1 Baseline Demographic and Clinical Characteristics of Exposure Cohort vs Referent Cohort |
Clinical Outcomes
Comparing the Efficacy of the Exposure Cohort and Referent Cohort
To better evaluate the therapeutic efficacy of XHP in patients with MASLD, we compared FibroScan, body composition, and serum biomarkers in the two cohorts of patients. For comparison of FibroScan parameters, the CAP pre-treatment compared to post-treatment for the exposure cohort (305.56±36.01 vs 286.24±36.63, p<0.001) (Figure 2A), and LSM before and after treatment [6.50 (4.80, 8.20) vs 5.40 (4.30, 7.10), p<0.001] (Figure 2B), all had significant efficacy. While there was no statistically significant difference between before and after referent cohort treatment. In addition, in the exposure cohort BMI before versus after treatment [27.30 (24.90, 29.90) vs 25.90 (24.00, 30.30), p<0.001] (Figure 2C), WHR before and after treatment (0.94±0.06 vs 0.93±0.06, p<0.001) (Figure 2D), and VFA before and after treatment [115.60 (89.70, 156.80) vs 100.00 (73.80, 125.20), p<0.001] (Figure 2E), with significant efficacy. Referent cohort’s BMI before and after treatment [26.60 (24.00, 31.95) vs 26.40 (23.70, 32.40), p=0.044] (Figure 2C), and the results were statistically significant, whereas the referent cohort’s other before and after treatments were not statistically significant compared to each other.
 |
Figure 2 Comparisons of body composition and serum biomarkers in the patient exposure cohort (MASLD who used XHP) with those in the referent cohort before and after treatment are shown. (A) Controlled attenuation parameter (CAP) values; (B) Liver stiffness measurement (LSM); (C) Body mass index (BMI); (D) Waist-to-Hip ratio (WHR); (E) visceral fat area (VFA); (F) NAFLD Fibrosis Score (NFS); (G) Fibrosis 4 Score (FIB-4); (H) Fatty Liver Index (FLI); (I) FibroScan + AST (FAST). Data presented as mean ± SD or median (IQR). *p<0.05, **p<0.01, ***p<0.001. Abbreviations: XHP, Xietu Hemu prescription; MASLD, Metabolic dysfunction-associated steatotic liver disease. |
In terms of MASLD diagnostic serum biomarkers, comparing before and after treatment (Figure 2F–I), the efficacy of FLI (66.20±14.84 vs 56.08±17.77, p<0.001), and FAST (0.48±2.39 vs −2.474±1.44, p<0.001) in the exposure cohort was compared before and after treatment. The efficacy was statistically significant when comparing FAST (−1.79±1.54 vs −2.26±1.52, p=0.019) in the referent cohort before and after treatment. NFS in the exposure cohort [−30 (−31.00, −28.00) vs −29.00 (−29.00, −28.00), p=0.001], and NFS in the referent cohort [- 31.00 (−32.50, −27.00) vs −29.00 (−31.00, −27.00), p=0.000], all showing a marked downward trend. Another aspect, FIB-4 in the exposure cohort, and FIB-4 and FLI in the referent cohort, were not statistically significant in the pre-treatment and post-treatment comparisons.
We further compared the FibroScan, body composition, and serum biomarkers between different XHP treatment duration cohorts and the referent cohort (Additional File 5). Within-group comparisons before and after treatment: In the referent cohort, both FAST and BMI decreased significantly after treatment compared to before treatment (P < 0.05), while NFS increased significantly (P < 0.05). In the cohort with 4 weeks of continuous XHP use, CAP, BMI, and VFA decreased significantly after treatment compared to before treatment (P < 0.05). In the cohort with 8 weeks of continuous XHP use, CAP, LSM, BMI, FIL, WHR, VFA, FLI, and FAST decreased significantly after treatment compared to before treatment (P < 0.05), while NFS increased significantly (P < 0.05). In the cohort with 12 weeks of continuous XHP use, CAP, LSM, BMI, WHR, and VFA decreased significantly after treatment compared to before treatment (P < 0.05). In the cohort with ≥16 weeks of continuous XHP use, CAP, LSM, BMI, VFA, and FAST decreased significantly after treatment compared to before treatment (P < 0.05), with no other significant differences observed. Between-group comparisons of treatment effects: Compared with the referent cohort, the cohort with 8 weeks of continuous XHP use showed significant decreases in CAP (291.34 ± 36.50 vs 287.50 ± 35.36, P = 0.041), WHR (0.94 ± 0.06 vs 0.92 ± 0.04, P < 0.05), VFA [109.70(80.50,151.90) vs 97.90(73.60,126.90), P = 0.012], and FIL [(60.00(28.00,87.00) vs 43.50(29.00,73.75), P = 0.011] after treatment compared to before treatment. The cohort with 12 weeks of continuous XHP use showed a significant decrease in BMI [26.80(24.80,32.70) vs 30.30(26.40,33.40), P = 0.012] after treatment compared to before treatment, with statistically significant results.
Analyzing the Effectiveness of XHP on MASLD Using IPTW
Based on the baseline analysis, the covariates found by combining the DAG analysis (Additional File 6) and the Change-in-Estimate CIE (Additional File 7): “Hypertension”, “CHD”, “Hashimoto Thyroiditis”, “INS”, “SGLT-2i”, “Euthyrox”, “HOMA-IS” and “NFS” were included in the propensity matching and analyzed using inverse probability of treatment weighting (Table 2). Before weighting, all P values for “Hypertension”, “Hashimoto Thyroiditis”, “SGLT-2i” and P values for “Euthyrox” were less than 0.05. After weighting, the two groups were balanced in these variables.
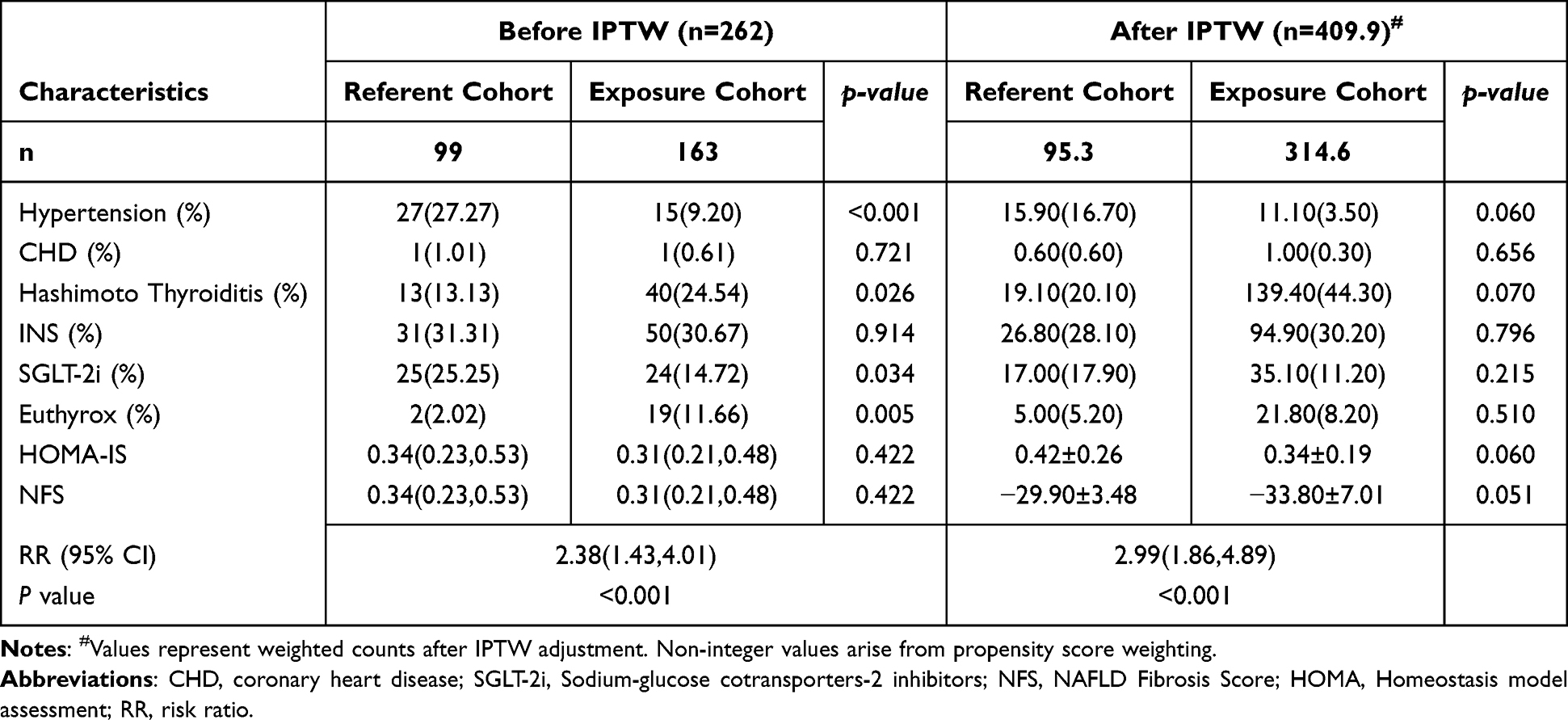 |
Table 2 Baseline Demographic and Clinical Characteristics Before and After Performing IPTW Analysis, and the Relationship Between Use of XTP and Improvement in MASLD |
Using an absolute value of CAP reduction of up to 4.1% as the endpoint event, whether performed before or after IPTW analysis, log-binomial regression analysis [risk ratio (RR)=2.38, 95% confidence interval (CI)=1.43 to 4.01 p<0.001]; weighted RR==2.99, 95% CI=1.86 to 4.89, p<0.001), which showed that the addition of XHP was effective in improving MASLD compared with basal treatment alone.
Subgroup and Sensitivity Analyses
When the outcome was defined as an absolute CAP reduction of ≥4.1% (Figure 3). (1) The results of the subgroup analyses according to the different dosing durations are shown in Figure 3A, and the weighted efficacy rates of MASLD (4 weeks weighted RR= 2.77, 95% CI=1.33 to 5.88, p=0.007; 8 weeks weighted RR=2.90, 95% CI=1.58 to 5.38, p=0.001; 12 weeks weighted RR=3.82, 95% CI=1.08 to 7.17, p=0.001; ≥16 weeks weighted RR=3.38, 95% CI=1.46 to 8.11, p=0.005) were statistically significant. (2) The results of the subgroup analyses according to the different degrees of steatosis and fibrosis in MASLD are shown in Figure 3B, with statistically significant weighted efficacy rates for steatosis S1≤S<S2 (weighted RR=1.11, 95% CI=0.33 to 4.04, p=0.022), S≥S3 (weighted RR=4.81, 95% CI=3.42 to 6.83], p=0.000), and fibrosis (F<F2 weighted RR=3.34, 95% CI=1.94 to 5.89, p=0.000; F2≤F<F3 weighted RR=17.36, 95% CI=7.67 to 36.47, p=0.001; F≥F3 weighted RR=9.25, 95% CI=1.82 to 70.49, p=0.013). However, the weighted effectiveness rate for steatosis S2≤S<S3 (weighted RR=1.62, 95% CI=0.73 to 3.89, p=0.134) was not statistically significant.
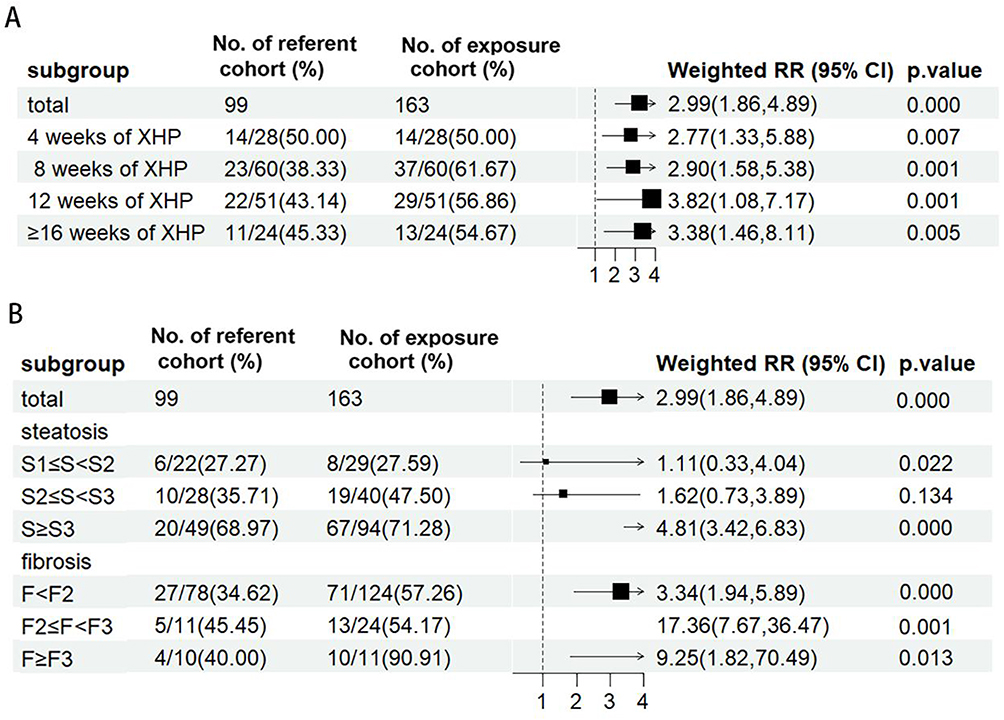 |
Figure 3 Stratified analysis of XHP efficacy by treatment duration and disease severity. (A) Forest plot of improvement in patients with MASLD using different durations of XTP; (B) Forest plot for subgroup analysis of liver with different degrees of steatosis and fibrosis. Weighted risk ratios (RR) with 95% CI calculated via inverse probability treatment weighting (IPTW). Statistical significance defined as p<0.05. A study from Prof. Jiangao Fan’s team on a Chinese population27 showed that: CAP<244dB/m, S<S1; 244dB/m≤CAP<269dB/m, S1≤S<S2; 269dB/m≤CAP<269dB/m, S2≤S<S3; 296dB/m ≤ CAP, S≥S3. LSM ≥ 5.5kPa, F≥F1; LSM≥7.85kPa, F≥F2,; LSM≥10kPa, F≥F3; LSM≥12.7kPa, F≥F4. |
Adverse Events
There were no obvious abnormalities in the blood routine, renal function, or vital signs of the patients included in this study that were tested before and after the administration of the drug. Occasionally, gastrointestinal reactions occurred during treatment, but the symptoms were mild and could be self-healed within a short period, and no significant adverse events occurred. Patients with hypertension, coronary heart disease, cerebral infarction, diabetes mellitus, and Hashimoto’s thyroiditis had stable conditions, and there was no significant progression of the disease during treatment.
Discussion
This study found that the exposure cohort (with XHP) was significantly more effective than the referent cohort (without XHP) for MASLD treatment. In the absence of statistically significant differences in baseline data, we compared CAP, LSM, body composition, and serum biomarkers before and after treatment in the two cohorts. Results showed significant improvements in hepatic steatosis, liver fibrosis and metabolic markers in MASLD patients after treatment in the exposure cohort. Additionally, we analyzed different XTP treatment duration cohorts and found that 8 weeks of continuous XTP use showed more significant effects on FibroScan, body composition, and serum biomarkers, while 12 weeks of continuous XTP use demonstrated significant effects on FibroScan and body composition. After performing IPTW analysis, we found significant improvement in MASLD in the exposure cohort compared to the referent cohort in subgroups with different dosing durations and different degrees of hepatic steatosis and fibrosis. In addition, no significant adverse effects were observed in this real-world study.
Contemporary Chinese medicine scholars28 mostly consider Phlegm unturbidity obstructing the middle jiao as a key factor in the development of MASLD disease. The previous treatment of MASLD with SLBS as the main efficacy to support the spleen and resolve dampness has been supported by the results of modern pharmacological studies. SLBS administration can effectively improve lipid metabolism in high-fat diet rats by regulating glycerophospholipid and glycerolipid metabolism.12 The beneficial effects of this prescription on hepatic lipid metabolism may be attributed, at least in part, to Sirtuin-1 (SIRT1) activation in the liver, which attenuates MASLD by suppressing hepatic inflammation.29 And another classic formula related to XHP, CSS, has the primary effect of soothing the liver and relieving depression. It has also been shown to significantly reduce hepatic lipid accumulation in high-fat diet-induced MASLD model rats by a mechanism that may be through the action of 15 MicroRNAs (miRNAs) including miR-34a-5p, miR-146a-5p, miR-20b-5p, and miR-142-3p, to reduce the gene and protein expression levels, thereby reducing fatty acid biosynthesis and thus treating MASLD.13 Furthermore, the anti-inflammatory effect of CSS in attenuating inflammation in MASLD is mediated, at least in part, by inhibition of the tumor necrosis factor-α/tumor necrosis factor receptor-1 (TNFα/TNFR1) signaling pathway.30 The Department of Endocrinology of Jiangsu Province Hospital of Chinese Medicine, in its long-term clinical practice, combined two classic recipe ideas, which were constantly adjusted by various TCM clinicians, and finally formulated the XHP. Despite the popularity of XHP in long-term clinical practice, there is still a lack of scientific research to demonstrate specific efficacy. Our team decided to study XHP in both clinical research and basic pharmacology, and this study answers the question of how clinically effective XHP is in the real world. Despite its popularity in clinical practice, XHP has remained relatively underexplored in rigorous scientific research until now. Our study directly addresses this gap by providing the first real-world evidence of XHP’s efficacy across multiple MASLD severity stages. Future research should prioritize: (1) Large-scale RCTs comparing XHP with first-line pharmacotherapies (eg, pioglitazone); (2) Mechanistic studies identifying active compounds and molecular targets; (3) Long-term outcomes tracking fibrosis progression.
A meta-analysis reported16 that Controlled Attenuation Parameters (CAP) and Liver Stiffness Measurements (LSM) performed with the Fibroscan device demonstrated high accuracy in quantifying steatosis and fibrosis in patients with MASLD. Recent studies have demonstrated the diagnostic and prognostic value of many serum biomarkers for steatosis.31 The Fibrosis 4 Index (FIB-4), and NAFLD Fibrosis Score (NFS) have been shown to be effective in the diagnosis of clinically significant fibrosis.20,21 FIB-4 and NFS have high diagnostic accuracy for advanced fibrosis (F3 or higher) but lower sensitivity and specificity in the early fibrosis stage (F0-F2), resulting in early disease that may be underestimated or with uncertain results.32 The FibroScan-AST (FAST)22 score, as a serologic predictor of high-risk Metabolic dysfunction-associated steatohepatitis (MASH), and the Fatty Liver Index (FLI), which assesses the degree of hepatic steatosis, have all been used as secondary outcome indicators inclusion. Studies have found that weight loss of more than 5 to 7% can reduce liver fat content and steatohepatitis, and weight loss of more than 10% can alleviate liver fibrosis.23 Therefore, improvements in body fat indicators such as BMI, WHR, and VFA can all prevent the emergence of comorbidities in patients with MASLD at an earlier stage and avoid further deterioration of MASLD disease. In balanced and comparable baseline data, our study found that XHP significantly improved CAP, LSM, BMI, WHR, VFA, FIL, and FAST in patients with MASLD. The NFS and FIB-4 results were not as favorable. It may be because similar blood measures such as FIB-4 have limitations in terms of sensitivity and positive predictive value, which makes them less reliable in identifying advanced fibrosis.33 And most of the MASLD patients included in this study had not yet reached the severe stage of fibrosis, which may be a possibility that led to the lack of meaningful results for several fibrosis serologic indices. In addition, our analysis of different XTP treatment duration cohorts revealed that 8 weeks of continuous use showed the most significant efficacy for MASLD. This finding will guide our upcoming large-scale multicenter cohort study and the design of randomized controlled trials.
In order to exclude the inevitable confounders of real-world situations, we used IPTW and validated its sensitivity using subgroup analyses. Log-binomial regression analysis showed that the efficacy of XHP was improved in MASLD patients with different duration of administration and different degrees of hepatic steatosis and fibrosis, with CAP decreased by more than 4.1% as the endpoint event. However, considering that this study was the first clinical study of XHP and that not many patients with cirrhosis and severe MASH above grade F3 were included, the efficacy of XHP in patients with severe MASLD still needs to be verified in more subsequent trials. This result suggests a wide range of effectiveness in the treatment of MASLD with XHP. The efficacy in patients with MASLD of different disease duration and different degrees of hepatic steatosis and fibrosis facilitates follow-up and translational studies of XHP.
The novelty of these findings lies in several key aspects: First, this is the first real-world evidence demonstrating that a TCM formula can achieve significant improvement in both hepatic steatosis (CAP reduction) and fibrosis (LSM reduction) within 8 weeks. Compared to conventional therapies like pioglitazone which typically require 24 weeks for similar effects,34 XHP offers a faster therapeutic response. Second, our subgroup analyses revealed that XHP maintains efficacy across all fibrosis stages, including advanced fibrosis (F≥3) where current pharmacotherapy options are extremely limited.35 The weighted RR of 9.25 for this subgroup suggests XHP may fill a critical therapeutic gap. Third, the unique multi-pathway mechanism of XHP, differs fundamentally from single-target Western medications. This explains its simultaneous improvements in both liver parameters (CAP/LSM) and metabolic indices (BMI/VFA). Recent evidence supports the antifibrotic potential of XHP: a study36 suggests that Paeonia lactiflora Pall. (present in XHP), a major component of XHP, may be able to counteract hepatic fibrosis by modulating the TGF-β/Smad signaling pathway and the TGF-β/PI3K-AKT signaling pathway. This mechanistic insight complements our clinical finding of a significant reduction in LSM.
The pathophysiology of MASLD is complex, and clinical treatments for the disease are lacking despite a solid biological basis.7 This study shares our team’s longstanding protocols for the effective treatment of MASLD in clinical practice and hopes to complement the current lack of treatment for MASLD. Traditional Chinese medicine is now gradually converging with contemporary medicine, and the emergence of more and more specialized formulas for specific diseases is believed to complement the treatment of various clinical diseases through a number of columns of research. Of course there are some shortcomings in this study. First, despite our sample size calculations, the sample size included in this study is still considered small in RWS and lacks consideration of a wider range of outcomes. Second, our setting of endpoint events focused on the reduction of hepatic steatosis, and we look forward to completing future studies targeting XHP for the treatment of hepatic fibrosis. In the future, we will conduct a further prospective, randomized, double-blind study on XHP to verify the results. Third, while our duration-stratified analysis provides novel insights, future studies should directly compare XHP with active comparators like pioglitazone. Additionally, the interaction between disease duration and treatment response warrants prospective validation.
Conclusion
In summary, this is the first RWS to evaluated the efficacy and safety of XHP for the treatment of MASLD. And the results of the study present that XHP has good treatment effect on MASLD. This study is a good attempt at real-world research on TCM in the field of MASLD. Future research should prioritize multicenter RCTs to confirm these findings, evaluate XHP in severe MASLD patients, and explore its underlying mechanisms.
Data Sharing Statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics Statement
The studies involving humans were approved by The Ethics Committee of Jiangsu Province Hospital of Chinese Medicine (2022NL-122-02). The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author Contributions
First author: Liu-lan Xiang. LX, XW and XZ contributed to the concept and design of this study. YC, JH and FQ carried out the clinical studies, collected data. LX and YZ completed statistical analyses, and drafted and revised the manuscript and JH participated in the data collection. YC, RL and JS validated data and gave some suggestions. XH, GW and XZ critically revised the manuscript and gave many suggestions. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by the Priority Academic Program Development of Jiangsu Higher Education Institutions (PAPD) and the 2023 Jiangsu Province Graduate Student Practice and Innovation Program (SJCX23_0787).
Disclosure
Dr Xi-qiao Zhou reports a patent ZL 2022 1 0250245.4 licensed to Xi-qiao Zhou. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Rinella ME, Lazarus JV, Ratziu V.; NAFLD Nomenclature consensus group, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Ann Hepatol. 2024;29(1):101133. doi:10.1016/j.aohep.2023.101133
2. Younossi Z, Anstee QM, Marietti M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15(1):11–20. doi:10.1038/nrgastro.2017.109
3. Rinella ME, Lazarus JV, Ratziu V, et al. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. J Hepatol. 2023;79(6):1542–1556. doi:10.1016/j.jhep.2023.06.003
4. Younossi ZM, Henry L. Epidemiology of non-alcoholic fatty liver disease and hepatocellular carcinoma. JHEP Rep. 2021;3(4):100305. doi:10.1016/j.jhepr.2021.100305
5. Niriella MA, Ediriweera DS, Kasturiratne A, et al. Outcomes of NAFLD and MAFLD: results from a community-based, prospective cohort study. PLoS One. 2021;16(2):e0245762. doi:10.1371/journal.pone.0245762
6. Gofton C, Upendran Y, Zheng MH, George J. MAFLD: how is it different from NAFLD? Clinical and molecular. Hepatology. 2023;29(Suppl):S17–S31.
7. Ali H, Shahzil M, Moond V, et al. Non-pharmacological approach to diet and exercise in metabolic-associated fatty liver disease: bridging the gap between research and clinical practice. J Personal Med. 2024;14(1):61. doi:10.3390/jpm14010061
8. Tincopa MA, Anstee QM, Loomba R. New and emerging treatments for metabolic dysfunction-associated steatohepatitis. Cell Metab. 2024;36(5):912–926. doi:10.1016/j.cmet.2024.03.011
9. Fan C, Wang G, Chen M, Li Y, Tang X, Dai Y. Therapeutic potential of alkaloid extract from Codonopsis Radix in alleviating hepatic lipid accumulation: insights into mitochondrial energy metabolism and endoplasmic reticulum stress regulation in NAFLD mice. Chin J Nat Med. 2023;21(6):411–422. doi:10.1016/S1875-5364(23)60403-0
10. Zhang Y, Wang H, Zhang L, Yuan Y, Yu D. Codonopsis lanceolata polysaccharide CLPS alleviates high fat/high sucrose diet-induced insulin resistance via anti-oxidative stress. Int J Biol Macromol. 2020;145:944–949. doi:10.1016/j.ijbiomac.2019.09.185
11. Cui H, Li Y, Cao M, et al. Untargeted metabolomic analysis of the effects and mechanism of nuciferine treatment on rats with nonalcoholic fatty liver disease. Front Pharmacol. 2020;11:858. doi:10.3389/fphar.2020.00858
12. Deng Y, Pan M, Nie H, et al. Lipidomic analysis of the protective effects of shenling baizhu san on non-alcoholic fatty liver disease in rats. Molecules. 2019;24(21):3943. doi:10.3390/molecules24213943
13. Zheng C, Nie H, Pan M, et al. Chaihu Shugan powder influences nonalcoholic fatty liver disease in rats in remodeling microRNAome and decreasing fatty acid synthesis. J Ethnopharmacol. 2024;318(Pt A):116967. doi:10.1016/j.jep.2023.116967
14. Lee Y, Park Y, Kim C, et al. Longitudinal outcomes of severe asthma: real-world evidence of multidimensional analyses. J Allergy Clin Immunol. 2021;9(3):1285–1294.e6. doi:10.1016/j.jaip.2020.09.055
15. Langan SM, Schmidt SA, Wing K, et al. The reporting of studies conducted using observational routinely collected health data statement for pharmacoepidemiology (RECORD-PE). BMJ. 2018;363:k3532. doi:10.1136/bmj.k3532
16. Cao YT, Xiang LL, Qi F, Zhang YJ, Chen Y, Zhou XQ. Accuracy of controlled attenuation parameter (CAP) and liver stiffness measurement (LSM) for assessing steatosis and fibrosis in non-alcoholic fatty liver disease: a systematic review and meta-analysis. EClinicalMedicine. 2022;51:101547. doi:10.1016/j.eclinm.2022.101547
17. Taheri H, Malek M, Ismail-Beigi F, et al. Effect of empagliflozin on liver steatosis and fibrosis in patients with non-alcoholic fatty liver disease without diabetes: a randomized, double-blind, placebo-controlled trial. Adv Ther. 2020;37(11):4697–4708. doi:10.1007/s12325-020-01498-5
18. Huwart L, Sempoux C, Vicaut E, et al. Magnetic resonance elastography for the noninvasive staging of liver fibrosis. Gastroenterology. 2008;135(1):32–40. doi:10.1053/j.gastro.2008.03.076
19. Vuppalanchi R, Siddiqui MS, Van Natta ML, et al. Performance characteristics of vibration-controlled transient elastography for evaluation of nonalcoholic fatty liver disease. Hepatology. 2018;67(1):134–144. doi:10.1002/hep.29489
20. Francque SM, Marchesini G, Kautz A, et al. Non-alcoholic fatty liver disease: a patient guideline. JHEP Rep. 2021;3(5):100322. doi:10.1016/j.jhepr.2021.100322
21. Wang S, Lin X, Zhu C, et al. Association between nonalcoholic fatty liver disease and increased glucose-to-albumin ratio in adults without diabetes. Front Endocrinol. 2024;14:1287916. doi:10.3389/fendo.2023.1287916
22. Fishman J, O’Connell T, Parrinello CM, Woolley JJ, Bercaw E, Charlton MR. Prevalence of nonalcoholic steatohepatitis and associated fibrosis stages among US adults using imaging-based vs biomarker-based noninvasive tests. J Health Econ Outcomes Res. 2024;11(1):32–43. doi:10.36469/001c.92223
23. Powell EE, Wong VW, Rinella M. Non-alcoholic fatty liver disease. Lancet. 2021;397(10290):2212–2224. doi:10.1016/S0140-6736(20)32511-3
24. Ma SX, Dhanaliwala AH, Rudie JD, et al. Bayesian networks in radiology. Radiol. 2023;5(6):e210187. doi:10.1148/ryai.210187
25. Greenland S, Daniel R, Pearce N. Outcome modelling strategies in epidemiology: traditional methods and basic alternatives. Int J Epidemiol. 2016;45(2):565–575. doi:10.1093/ije/dyw040
26. Tassistro E, Bernasconi DP, Valsecchi MG, Antolini L. Adverse events in single-arm clinical trials with non-fatal time-to-event efficacy endpoint: from clinical questions to methods for statistical analysis. BMC Med Res Method. 2024;24(1):3. doi:10.1186/s12874-023-02123-z
27. Qu Y, Song YY, Chen CW, et al. Diagnostic performance of fibrotouch ultrasound attenuation parameter and liver stiffness measurement in assessing hepatic steatosis and fibrosis in patients with nonalcoholic fatty liver disease. Clin Transl Gastroenterol. 2021;12(4):e00323. doi:10.14309/ctg.0000000000000323
28. Zhu K, Guo Y, Zhao C, et al. Etiology exploration of non-alcoholic fatty liver disease from traditional Chinese medicine constitution perspective: a cross-sectional study. Front Public Health. 2021;9:635818. doi:10.3389/fpubh.2021.635818
29. Pan MX, Zheng CY, Deng YJ, et al. Hepatic protective effects of Shenling Baizhu powder, a herbal compound, against inflammatory damage via TLR4/NLRP3 signalling pathway in rats with nonalcoholic fatty liver disease. J Integr Med. 2021;19(5):428–438. doi:10.1016/j.joim.2021.07.004
30. Lei S, Zhao S, Huang X, et al. Chaihu Shugan powder alleviates liver inflammation and hepatic steatosis in NAFLD mice: a network pharmacology study and in vivo experimental validation. Front Pharmacol. 2022;13:967623. doi:10.3389/fphar.2022.967623
31. Habibullah M, Jemmieh K, Ouda A, Haider MZ, Malki MI, Elzouki AN. Metabolic-associated fatty liver disease: a selective review of pathogenesis, diagnostic approaches, and therapeutic strategies. Front Med. 2024;11:1291501. doi:10.3389/fmed.2024.1291501
32. Han S, Choi M, Lee B, et al. Accuracy of noninvasive scoring systems in assessing liver fibrosis in patients with nonalcoholic fatty liver disease: a systematic review and meta-analysis. Gut Liver. 2022;16(6):952–963. doi:10.5009/gnl210391
33. Sinha RA, Bruinstroop E, Singh BK, Yen PM. Nonalcoholic fatty liver disease and hypercholesterolemia: roles of thyroid hormones, metabolites, and agonists. Thyroid. 2019;29(9):1173–1191. doi:10.1089/thy.2018.0664
34. Genua I, Cusi K. Pharmacological approaches to nonalcoholic fatty liver disease: current and future therapies. Diabetes Spectrum. 2024;37(1):48–58. doi:10.2337/dsi23-0012
35. Diaz LA, Arab JP, Idalsoaga F, et al. Updated recommendations for the management of metabolic dysfunction-associated steatotic liver disease (MASLD) by the Latin American working group. Ann Hepatol. 2025;30:101903. doi:10.1016/j.aohep.2025.101903
36. Zhang Q, Wu Y, Ge M, et al. Paeoniflorin-free subfraction of Paeonia lactiflora Pall. shows the potential of anti-hepatic fibrosis: an integrated analysis of network pharmacology and experimental validation. J Ethnopharmacol. 2022;299:115678. doi:10.1016/j.jep.2022.115678
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Real-World Efficacy and Safety of Adalimumab Biosimilar (HS016) in Biologic-Naïve Patients with Perianal Fistulizing Crohn’s Disease: A Prospective, Single-Arm, Observational Study
Yu Q, Cheng Y, Wang H, Fang L, Chen Y, Zhang X, Li J, Fu X, Li J, Zhu L
Drug Design, Development and Therapy 2026, 20:574904
Published Date: 30 March 2026