Back to Journals » Journal of Pain Research » Volume 18
Wrist-Ankle Acupuncture Relieves Postoperative Pain After Milligan-Morgan Hemorrhoidectomy for Mixed Hemorrhoids: A Randomized Controlled Clinical Trial
Authors Xu M, Li W, Wang X, Gao Y, Qi L, Xu L, He Y, Dong C, Zhang J, Zhang H, Wang J ![]()
Received 22 May 2025
Accepted for publication 19 August 2025
Published 18 September 2025 Volume 2025:18 Pages 4875—4882
DOI https://doi.org/10.2147/JPR.S542202
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Min Xu,1,* Wenjuan Li,1,* Xiaoyan Wang,1 Yulei Gao,1 Lingyi Qi,1 Liping Xu,1 Yuhua He,1 Changsheng Dong,2 Jing Zhang,1 Huachun Zhang,1 Jiawen Wang3
1Nursing Department, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 2Cancer Institute/Department of Oncology, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China; 3Coloproctology Department, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, Shanghai, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jiawen Wang, Coloproctology Department, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, No. 725 South Wanping Road, Shanghai, 200032, People’s Republic of China, Email [email protected] Huachun Zhang, Nursing Department, Longhua Hospital, Shanghai University of Traditional Chinese Medicine, No. 725 South Wanping Road, Shanghai, 200032, People’s Republic of China, Email [email protected]
Purpose: To evaluate the efficacy of wrist-ankle acupuncture in alleviating postoperative pain in patients undergoing Milligan-Morgan hemorrhoidectomy for mixed hemorrhoids.
Patients and Methods: A total of 124 patients who underwent Milligan-Morgan hemorrhoidectomy for mixed hemorrhoids at our center between January 2024 and December 2024 were randomly assigned to two groups (62 patients in each group). The control group received postoperative patient-controlled intravenous analgesia (PCIA), whereas the treatment group received wrist-ankle acupuncture in addition to PCIA. Pain relief was assessed at 6 h, 12 h, 24 h, 48 h, and 72 h postoperatively. Additional outcomes included PCIA usage, frequency of rescue analgesia for pain, and the incidence of postoperative complications.
Results: The treatment group exhibited significantly lower Numerical Rating Scale (NRS) pain scores than the control group starting at 12 h postoperatively (P < 0.05). By 24 h, both PCIA usage and the frequency of rescue analgesia were significantly reduced in the treatment group compared with the control group (P < 0.05). The incidence of constipation and urinary retention was also lower in the treatment group (P < 0.05). No adverse events occurred in either group.
Conclusion: Wrist-ankle acupuncture is a safe and effective adjunct for postoperative analgesia following Milligan-Morgan hemorrhoidectomy. It significantly alleviates pain, lowers the incidence of constipation and urinary retention, and is not associated with any adverse effects.
Keywords: wrist-ankle acupuncture, mixed hemorrhoids, Milligan-Morgan hemorrhoidectomy, postoperative pain, randomized controlled trial
Introduction
Mixed hemorrhoids, which involve both internal and external components, are a common clinical condition resulting from degeneration of anal cushion tissues, vascular hyperplasia, varicose veins, and other factors. This term is commonly used in Chinese clinical practice to describe such combined presentations. Key symptoms include bleeding, pain, and anal discomfort, which often recur and significantly impair patients’ quality of life.1 Hemorrhoidal disease is the most common anorectal disease, with a prevalence of about 4.4% in the general population, peaking in individuals aged 45–65 years.2 Surgical intervention, particularly the Milligan-Morgan hemorrhoidectomy, is typically considered when conservative treatments fail. Although various pain management protocols have been developed and proven effective, postoperative pain remains the most common complication.3 This persistence of pain may be partly due to the inherent limitations and adverse effects of conventional analgesics, such as opioids and NSAIDs, which can cause nausea, drowsiness, gastrointestinal irritation, and, in some cases, drug dependence.4,5 Studies indicate that 65% of patients experience moderate to severe pain after surgery for hemorrhoidal disease.6 Postoperative pain may also lead to complications such as urinary retention, constipation, prolonged hospitalization, and increased medical costs.7 In severe cases, it may even trigger cardiovascular or cerebrovascular events, significantly worsening postoperative recovery.8
Wrist-ankle acupuncture, a characteristic therapy of traditional Chinese medicine, alleviates pain through subcutaneous superficial stimulation of specific acupoints around the ankle based on the theory of the Three Yin and Three Yang meridians.9 To further investigate the efficacy of wrist-ankle acupuncture in improving postoperative pain in patients with mixed hemorrhoids undergoing Milligan-Morgan hemorrhoidectomy, our research team applied this technique postoperatively. Results demonstrated that wrist-ankle acupuncture significantly reduced postoperative pain, decreased the usage of PCIA, minimized the need for rescue analgesics, and exhibited notable therapeutic benefits with a high safety profile.
Patients and Methods
This study was a randomized controlled clinical trial. A total of 124 patients undergoing Milligan-Morgan hemorrhoidectomy for mixed hemorrhoids at Longhua Hospital, Shanghai University of Traditional Chinese Medicine, between January 2024 and December 2024 were enrolled. Participants were randomized using a random number table method into two groups:
(1) Treatment group (n = 62): 31 males, 31 females; age range 24–67 years, mean age 41.32 ± 11.18 years.
(2) Control group (n = 62): 29 males, 33 females; age range 25–67 years, mean age 38.09 ± 19.97 years.
No statistically significant differences were observed in baseline characteristics (age, sex, disease duration) between the two groups (P > 0.05), ensuring comparability. All subjects have signed informed consent forms.
Diagnostic Criteria
The diagnostic criteria were based on the Chinese Clinical Practice Guidelines for Diagnosis and Treatment of Hemorrhoidal Disease (2020), issued by The Coloproctology Society of Chinese Association of Integrative Medicine.10
In Chinese clinical practice, mixed hemorrhoids refer to hemorrhoids with both internal and external components, presenting with symptoms such as bleeding, prolapse, anal distention, and pain. In this study, all cases met the criteria for Goligher grade III or IV hemorrhoidal disease, which are generally indicated for Milligan-Morgan hemorrhoidectomy:
Clinical Manifestations
Mixed hemorrhoids refer to hemorrhoids with both internal and external components, presenting with symptoms such as bleeding, prolapse, anal distention, and pain.
Diagnostic Basis
- Symptoms: Hematochezia, prolapsed hemorrhoids (spontaneous or requiring manual reduction), anal discomfort, pruritus, or pain.
- Visual inspection: Protruding masses at the anal verge or dentate line.
- Digital rectal examination: Soft masses palpable within the anal canal, with loss of the intersphincteric groove.
- Anoscopy confirmation.
Diagnosis required fulfillment of at least two criteria.
Inclusion Criteria
- Aged 18–60 years.
- Diagnosed with mixed hemorrhoids and experiencing postoperative anal pain after Milligan-Morgan hemorrhoidectomy.
- Voluntarily participated and provided written informed consent.
- Able to cooperate with nurses for Numerical Rating Scale (NRS) assessments.
- NRS score≥4.
- Intact skin at wrist-ankle acupuncture sites (no redness, scars, or lesions).
- Postoperative use of PCIA.
Exclusion Criteria
- Concurrent anorectal surgeries (eg, anal fissure, fistula, rectal polyp, perianal abscess, colonic polyp, or colorectal lesions).
- Severe comorbidities (cardiovascular, cerebrovascular, hepatic, renal, or hematopoietic disorders).
- Communication barriers or noncompliance.
- Use of additional analgesics beyond PCIA.
- Needle phobia.
- Psychiatric disorders impairing study participation.
- Pregnancy or suspected pregnancy.
Treatment
Type of Anesthesia
All surgeries were performed under spinal anesthesia.
Surgical Technique
All patients underwent conventional Milligan-Morgan hemorrhoidectomy performed by experienced colorectal surgeons. The hemorrhoidal tissue was grasped and excised using scissors, with care taken to preserve adequate mucocutaneous bridges between excision sites to prevent anal stenosis. The vascular pedicle was ligated with absorbable sutures, and the wound edges were trimmed to ensure hemostasis. No energy devices, laser, or diathermic techniques were used in this series.
Control Group
PCIA was initiated immediately postoperatively and discontinued at 48 h. The PCIA protocol consisted of sufentanil (2 μg/kg) and ondansetron (8 mg) diluted in 300 mL normal saline, administered via continuous infusion at 2 mL/h. Patients could self-administer a 0.5 mL bolus dose as needed, with a lockout interval of 15 minutes. Routine postoperative pain management included: active listening to patients’ concerns and providing reassurance; distraction techniques (eg, music therapy); encouraging self-reporting of pain and guided relaxation; and protecting the surgical incision during activity to avoid irritation.
Treatment Group
In addition to the control group’s interventions, wrist-ankle acupuncture was applied:Initial treatment: Administered at 6 h postoperatively (after anesthesia wore off and lower limb sensation returned). Subsequent treatments: Performed on postoperative days 1 and 2, with needles retained for 8 h each session.
Acupoint Selection: Lower Zone 6 was selected bilaterally based on the anatomical principles of wrist-ankle zoning. Anatomical boundaries: Below the transverse line defined by the xiphoid process and costal margins, approximating the diaphragm. Laterality: Followed the principle of “left disease treated on the left, right disease on the right”. Procedure: The patient was placed in the supine position. After skin disinfection, 30-gauge, 1.5 cun (approximately 40 mm) filiform needles were inserted at a 30° angle into the subcutaneous layer at bilateral Lower Zone 6 points to a depth of 1.4 cun (approximately 38 mm). No manipulation (lifting, thrusting, or rotating) was performed, in order to avoid the deqi sensation. (Figure 1)
 |
Figure 1 Clinical photograph of a patient undergoing wrist-ankle acupuncture treatment following Milligan-Morgan hemorrhoidectomy. |
Outcome Measures
Pain Assessment
Numerical Rating Scale (NRS) scores were evaluated at 6 h, 12 h, 24 h, 48 h, and 72 h postoperatively.
Baseline Assessment
Conducted at 6 h postoperatively (after anesthesia wore off and lower limb sensation returned) prior to wrist-ankle acupuncture.
PCIA Usage
Rescue analgesia doses (bolus attempts), onset time, and duration of analgesia were recorded during the first three assessments (6 h, 12 h, 24 h).Residual PCIA solution volume was measured at 48 h postoperatively to calculate total self-administered rescue doses.
Complications
Incidence of constipation, urinary retention, and nausea/vomiting within 6–72 h postoperatively.
Constipation
Defined as persistent difficulty in defecation, sensation of incomplete evacuation, or reduced bowel movement frequency. Difficulty in defecation: Characterized by small stool volume, hard stools, prolonged or straining defecation, sensation of incomplete evacuation, or requiring manual assistance. Reduced bowel movement frequency: Fewer than three bowel movements per week or prolonged absence of bowel urgency.
Urinary Retention
Defined as postoperative inability to spontaneously empty the bladder, manifested as frequent urination, oliguria (scanty urine output), delayed micturition, or incomplete bladder emptying.
Statistical Methods
Data analysis was performed using SPSS 23.0. Continuous variables are expressed as mean ± standard deviation (SD). The t-test was applied for normally distributed data, while the Mann-Whitney U-test (non-parametric rank-sum test) was used for non-normally distributed data. Categorical variables were analyzed with the chi-square (χ²) test. A P < 0.05 was considered statistically significant.
Results
Comparison of NRS Scores Between Two Groups of Patients
Wrist-ankle acupuncture could improve postoperative pain score (NRS). (Table 1)
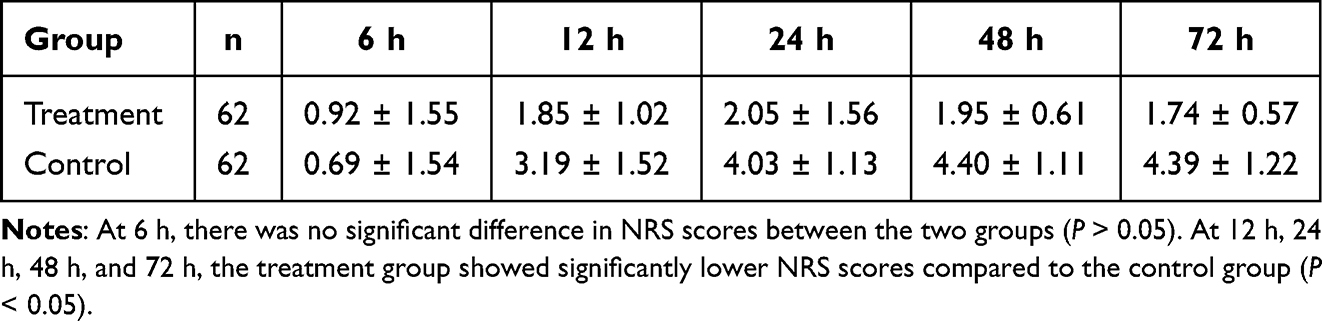 |
Table 1 Postoperative Pain Scores (NRS) |
Comparison of PCIA Usage Between Two Groups of Patients
Wrist-ankle acupuncture could decrease PCIA Usage. (Table 2)
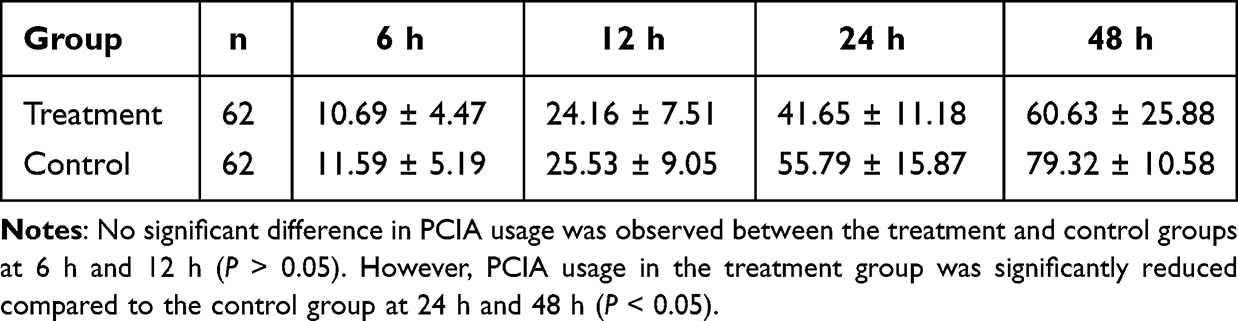 |
Table 2 PCIA Usage |
Comparison of Frequency of Rescue Analgesia Doses Between Two Groups of Patients
Wrist-ankle acupuncture could reduce frequency of rescue analgesia doses. (Table 3)
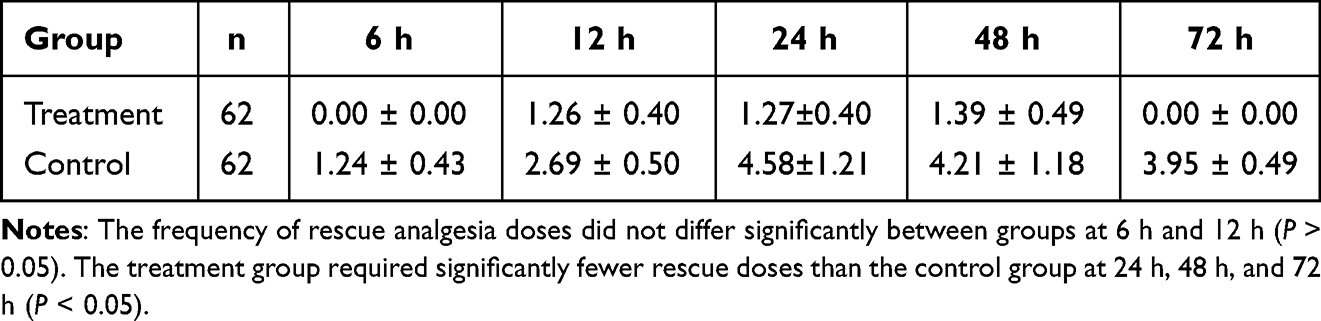 |
Table 3 Frequency of Rescue Analgesia Doses |
Comparison of Incidence of Postoperative Constipation and Urinary Retention Between Two Groups of Patients
Wrist-ankle acupuncture could lower incidence of postoperative constipation and urinary retention. (Table 4)
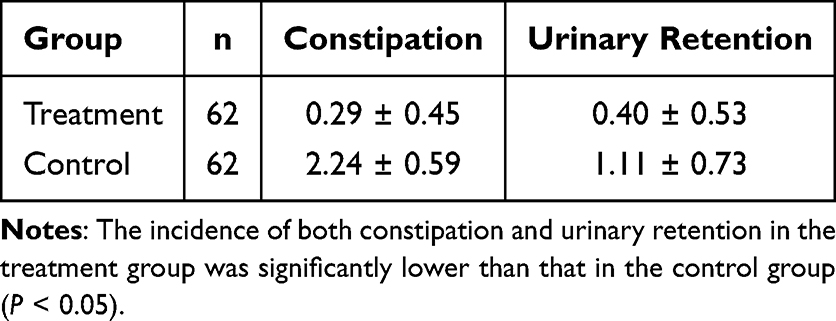 |
Table 4 Incidence of Postoperative Constipation and Urinary Retention |
Adverse Events
No postoperative complications, such as nausea and vomiting, occurred in either group during the treatment period.
Discussion
Hemorrhoidal disease is a common anorectal condition with a rising incidence across all age groups, and advanced cases frequently require surgical intervention for definitive treatment.2 Milligan-Morgan hemorrhoidectomy remains a widely used and effective procedure; however, postoperative pain continues to be a major and challenging complication.11 Even with timely administration of analgesics, complete pain relief is rarely achieved, which can hinder recovery, reduce patient satisfaction, and increase healthcare burden.12
Postoperative pain following Milligan-Morgan hemorrhoidectomy is multifactorial. (1) Surgical trauma from excision of diseased tissue leaves open wounds, resulting in localized nociceptive stimulation. (2) Defecation-related pain—often described as tearing or burning—can heighten patient anxiety, promote sustained anal sphincter contraction, and intensify discomfort after bowel movements. (3) Infection at the surgical site may trigger inflammatory nociceptive pathways, as supported by previous studies. (4) Edema related to intraoperative manipulation, stool characteristics, or premature physical activity can exacerbate pain and increase the risk of bleeding or delayed wound healing.3
Wrist-ankle acupuncture, based on traditional Chinese medicine theories of the Twelve Cutaneous Regions and the Three Yin and Three Yang meridians, involves subcutaneous stimulation of designated zones on the wrists and ankles to regulate visceral function, improve qi and blood circulation, and relieve pain.13–17 Proposed analgesic mechanisms include activation of cutaneous nerve endings to modulate central and peripheral neural pathways, promotion of β-endorphin release, and reduction of serum serotonin (5-HT) levels.18–20 This technique offers several advantages—minimal invasiveness, low cost, and good patient tolerance—that make it an attractive adjunct in postoperative pain management.9,14,21–24
Our study demonstrates that wrist-ankle acupuncture safely and effectively reduces postoperative pain (as measured by NRS scores), decreases PCIA usage and the frequency of rescue analgesia doses, and lowers the incidence of constipation and urinary retention without adverse events such as nausea or vomiting. These findings are consistent with prior evidence showing that acupuncture or acupuncture-point stimulation can improve postoperative pain control and reduce opioid consumption in surgical patients.25 A systematic review and meta-analysis confirmed the opioid-sparing effect of acupuncture across multiple surgical contexts, including hemorrhoidectomy, further supporting its role in multimodal pain management.9 In addition, broader non-pharmacological interventions—such as acupuncture, mind-body approaches, and patient education—have been shown to enhance recovery by reducing pain intensity, decreasing opioid reliance, and improving functional outcomes.26–28
Taken together, our findings add to the existing evidence by confirming the efficacy of wrist-ankle acupuncture in the context of Milligan-Morgan hemorrhoidectomy. However, as this was a single-center study, future research with standardized protocols and multicenter trials is warranted to improve reproducibility and facilitate cross-cultural applicability.
Conclusion
In conclusion, wrist-ankle acupuncture appears to be a safe, well-tolerated, and effective adjunct for postoperative pain management in patients undergoing conventional Milligan-Morgan hemorrhoidectomy performed with scissors. In our cohort, this technique not only alleviated pain intensity but also reduced the incidence of common postoperative complications—specifically constipation and urinary retention—without notable adverse effects. Given its simplicity, minimal invasiveness, and low cost, wrist-ankle acupuncture may represent a valuable complement to existing multimodal analgesia protocols. Nevertheless, differences in surgical practice, perioperative pathways, and cultural acceptance of acupuncture should be taken into account when extrapolating these findings. Future high-quality, multicenter randomized controlled trials in diverse populations are warranted to validate its efficacy, refine treatment protocols, and promote broader clinical adoption.
Ethics Approval and Informed Consent
This study was conducted in accordance with the principles of the Declaration of Helsinki. It was reviewed and approved by the Medical Ethics Committee of Longhua Hospital, Shanghai University of Traditional Chinese Medicine (Approval No. 2024LCSY028). The trial was registered in the Chinese Clinical Trial Registry (ChiCTR), WHO Primary Registry, with the registration number ChiCTR2400085599. Written informed consent was obtained from all participants prior to enrollment.
Consent for Publication
All the listed authors have carefully reviewed and approved this manuscript. We all agree to submit it to Journal of Pain Research for publication and are aware of and accept the journal’s publication policies.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was funded by Shanghai Nursing Association 2023 Research Project (Grant number: 2023MS-B06); National Development Program for Dominant Specialties of Traditional Chinese Medicine (Nursing) (Grant number: ZYZK011-001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Grimes WR, Stratton M. Pelvic floor dysfunction. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2020.
2. Gallo G, Martellucci J, Sturiale A, et al. Consensus statement of the Italian society of colorectal surgery (SICCR): management and treatment of hemorrhoidal disease. Tech Coloproctol. 2020;24(2):145–164. doi:10.1007/s10151-020-02149-1
3. Sun XW, Xu JY, Zhu CZ, Li SJ, Jin LJ, Zhu ZD. Analysis of factors impacting postoperative pain and quality of life in patients with mixed hemorrhoids: a retrospective study. World J Gastrointest Surg. 2024;16(3):731–739. doi:10.4240/wjgs.v16.i3.731
4. Wang T, Gao JQ, Chang M, et al. “Zhibian (BL54) to Shuidao (ST28)” acupuncture manipulation combined with analgesics in postoperative pain management for patients with mixed hemorrhoids: a randomized controlled trial protocol. J Pain Res. 2025;18:2163–2174. doi:10.2147/JPR.S519232
5. Rajan N, Joshi GP. Management of postoperative nausea and vomiting in adults: current controversies. Curr Opin Anaesthesiol. 2021;34(6):695–702. doi:10.1097/ACO.0000000000001063
6. Lohsiriwat D, Lohsiriwat V. Outpatient hemorrhoidectomy under perianal anesthetics infiltration. J Med Assoc Thai. 2005;88(12):1821–1824.
7. Romaguera VP, Sancho-Muriel J, Alvarez-Sarrdo E, Millan M, Garcia-Granero A, Frasson M. Postoperative complications in hemorrhoidal disease and special conditions. Rev Recent Clin Trials. 2021;16(1):67–74. doi:10.2174/1574887115666200406114218
8. Turan A, Leung S, Bajracharya GR, et al. Acute postoperative pain is associated with myocardial injury after noncardiac surgery. Anesth Analg. 2020;131(3):822–829. doi:10.1213/ANE.0000000000005033
9. Xu N, Liu LL, Rong W. Wrist-ankle acupuncture as additional therapy for postoperative multimodal analgesia in orthopedic surgery: systematic review and meta-analysis. Pain Med. 2022;23(10):1654–1669. doi:10.1093/pm/pnac065
10. The Coloproctology Society of Chinese Association of Integrative Medicine. Chinese clinical practice guidelines for diagnosis and treatment of hemorrhoidal disease (2020). J Colorect Anal Surg. 2020;26(05):519–533. doi:10.19668/j.cnki.issn1674-0491.2020.05.001
11. Amir A, Nazir A, Umair A, et al. Comparison of pedicle coagulation hemorrhoidectomy with LigaSure versus conventional Milligan Morgan hemorrhoidectomy in reducing post-operative pain: a randomized controlled trial. Cureus. 2023;15(9):e45015. doi:10.7759/cureus.45015
12. Tan VZZ, Peck EW, Sivarajah SS, et al. Systematic review and meta-analysis of postoperative pain and symptoms control following laser haemorrhoidoplasty versus Milligan-Morgan haemorrhoidectomy for symptomatic haemorrhoids: a new standard. Int J Colorectal Dis. 2022;37(8):1759–1771. doi:10.1007/s00384-022-04225-4
13. Zhao L, Shen XY. Tracing the origin of wrist-ankle acupuncture based on huan in bamboo slip and silk medical books, maikou and the theory of origin, junction, branch and trunk. Chin Acupunct Moxibust. 2021;41(3):339–341,353. doi:10.13703/j.0255-2930.20200124-0001
14. Chen HJ, Zheng YS, Chen LQ, Xiong GF, Xu JN. Evaluating the efficacy of wrist-ankle acupuncture combined with patient-controlled intravenous analgesia for managing post uvulopalatopharyngoplasty. J Craniofac Surg. 2024;35:2250–2253. doi:10.1097/SCS.0000000000010624
15. Wu JL, Su HT, Liang YH, Peng JJ, Hong WW. Auxiliary analgesic effect of wrist-ankle acupuncture on patients undergoing transforaminal endoscope surgery. Chin Acupunct Moxibust. 2020;40(2):147–151. doi:10.13703/j.0255-2930.20190125-k00034
16. Bi HJ, Wu GC, He YY, Chen HY, Zhou S, Zhou QH. Wrist-ankle acupuncture increases pain thresholds in healthy adults. Altern Ther Health Med. 2017;23(1):20–25.
17. Wu LM, Liu Q, Yin XH, et al. Wrist-ankle acupuncture combined with pain nursing for the treatment of urinary calculi with acute pain. World J Clin Cases. 2023;11(18):4287–4294. doi:10.12998/wjcc.v11.i18.4287
18. Cao HT, Zhang W, Luo C, Zhao HB, Liu JM. Effect of wrist-ankle acupuncture on postoperative analgesia after total knee arthroplasty. Chin J Integr Med. 2023;29(3):253–257. doi:10.1007/s11655-022-3463-5
19. Chen XM, Pang LN, Ke YC, et al. Exploring the mechanism of wrist-ankle acupuncture in treating chemotherapy-induced neuropathic pain in mice by regulating neuroinflammatory responses through ɑ7 nicotinic acetylcholine receptor in the spinal dorsal horn. Acupunct Res. 2025;50(7):735–742. doi:10.13702/j.1000-0607.20241267
20. Huo Y, Chen P, Zhu JN, Fu YQ, Xu GL. Curative effect of wrist-ankle acupuncture on postpartum abdominal pain and its influence on serum β-EP level in puerpera. Chin Acupunct Moxibust. 2023;43(11):1257–1260. doi:10.13703/j.0255-2930.20230228-k0006
21. Zhang Z, Liu Q, Chen R, et al. Effect of wrist-ankle acupuncture point stimulation on preventing postoperative nausea and vomiting in female patients undergoing orthopedic surgery. J Perianesth Nurs. 2025;40(3):634–639. doi:10.1016/j.jopan.2024.07.021
22. Guo S, Wang Y, Ai J, Zhao J, Huang S, Wang J. Wrist and ankle acupuncture relief moderate to severe postoperative pain after functional endoscopic sinus surgery: a randomized controlled study. Br J Pain. 2025;19(2):115–124. doi:10.1177/20494637241264941
23. Shi P, Liu J, Du J, Yu H, Fang F. Pain modulation induced by electronic wrist-ankle acupuncture: a functional near-infrared spectroscopy study. Pain Pract. 2022;22(2):182–190. doi:10.1111/papr.13076
24. Chen M, Xu Y, Fu X, Xie J, Cao X, Xu Y. Wrist-ankle acupuncture for the treatment of acute orthopedic pain after surgery: a meta-analysis. J Orthop Surg Res. 2023;18(1):106. doi:10.1186/s13018-023-03569-z
25. Yang K, Du YJ, Shi J, et al. Exploration of dominant diseases and clinical application characteristics of wrist-ankle acupuncture therapy based on data mining technology. Chin Acupunct Moxibust. 2019;39(6):673–678. doi:10.13703/j.0255-2930.2019.06.029
26. Du B, Xu Z, Zhong X. Electroacupuncture for postoperative pain in mixed hemorrhoids: a meta-analysis. Medicine. 2022;101(50):e32247. doi:10.1097/MD.0000000000032247
27. Wu MS, Chen KH, Chen IF, et al. The efficacy of acupuncture in post-operative pain management: a systematic review and meta-analysis. PLoS One. 2016;11(3):e0150367. doi:10.1371/journal.pone.0150367
28. Ye S, Zhou J, Guo X, Jiang X. Three acupuncture methods for postoperative pain in mixed hemorrhoids: a systematic review and network meta-analysis. Comput Math Methods Med. 2022;2022:5627550. doi:10.1155/2022/5627550
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.