Back to Journals » Journal of Pain Research » Volume 16
Work Interventions Within Interdisciplinary Pain Rehabilitation Programs (IPRP) – Frequency, Patient Characteristics, and Association with Self-Rated Work Ability
Authors Svanholm F ![]() , Björk M, Löfgren M
, Björk M, Löfgren M ![]() , Gerdle B
, Gerdle B ![]() , Hedevik H
, Hedevik H ![]() , Molander P
, Molander P ![]()
Received 21 September 2022
Accepted for publication 17 January 2023
Published 14 February 2023 Volume 2023:16 Pages 421—436
DOI https://doi.org/10.2147/JPR.S390747
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Frida Svanholm,1 Mathilda Björk,1 Monika Löfgren,2,3 Björn Gerdle,1 Henrik Hedevik,4 Peter Molander1,5
1Pain and Rehabilitation Centre, and Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden; 2Department of Clinical Sciences, Karolinska Institutet, Stockholm, Sweden; 3Department of Rehabilitation Medicine, Danderyd Hospital, Stockholm, Sweden; 4Unit of Physiotherapy, Department of Health, Medicine and Caring Sciences, Linköping University, Linköping, Sweden; 5Department of Behavioural Sciences and Learning, Linköping University, Linköping, Sweden
Correspondence: Frida Svanholm, Pain and Rehabilitation Centre, County Council of Östergötland, Brigadgatan 22, Linköping, S-58185, Sweden, Tel +46 730-447785, Email [email protected]
Background: Interdisciplinary pain rehabilitation programs (IPRPs) help people with chronic pain improve their health and manage their work; however, the way IPRPs address sick leave could be improved. Although work interventions can be a part of IPRP, it is not well known how and to what extent.
Aim: This study explores the frequency of work interventions and the characteristics of patients who participate in work interventions as part of IPRP at specialist pain rehabilitation departments in Sweden. In addition, this study explores the association between participation in work interventions and change in patients’ self-rated work ability after IPRP.
Methods: Data from the Swedish quality registry for pain rehabilitation (SQRP), which includes 3809 patients between 2016 and 2018, were analysed with descriptive statistics and regression analyses.
Results: The results indicate a high participation rate in work interventions (90%). Some differences were evident concerning characteristics of patients who participated in different work interventions. The return-to-work (RTW) plan, the most frequently used work intervention, had the strongest association with change in self-rated work ability after IPRP. However, the effect sizes were small, and the initial score best explained the change. Furthermore, there were differences between employed and unemployed patients and employment had a positive association with change in self-rated work ability.
Conclusion: More research is needed to understand IPRP’s mechanisms and work interventions to support patients with chronic pain, reduce sick leave, and manage work. Employment status needs to be considered and interventions should be tailored to match the individual needs.
Keywords: chronic pain, work interventions, rehabilitation
Introduction
In Europe, around 20% of the population suffers from chronic pain (>6 months) of at least moderate intensity.1 Chronic pain reduces ability to perform daily, social, and work activities and results in stress, poor mental health, and decreased quality of life.1–3 People with chronic pain often report pain that decreases work ability and increases absence from work.4–6 Chronic pain is the second most common reason for sick leave in Sweden.7 Longer periods of sick leave are common – eg, about 9% of sickness absence due to back pain lasts for over a year.8 Similar to the general population, people with chronic pain view work as an important activity not only for economic security but also because it makes them feel normal, allowing them to feel as if they are in control of their lives and routines, especially when it comes to establishing and maintaining relationships. High work value may facilitate work activities, but support is needed to balance work participation and work ability.9–11
Bio-psycho-social interdisciplinary pain rehabilitation programs (IPRPs) are evidence-based rehabilitation programs offered to patients with chronic pain.12,13 IPRPs generally include education, physical activity, cognitive behavioural therapy (CBT), and/or interventions to support social and work activities delivered by different professionals. IPRPs in real-world settings reduce pain and improve health and quality of life.14 Furthermore, IPRP aims to improve work ability and reduce sick leave, but the results are inconsistent.15 However, recent Swedish studies have shown promising results concerning reduced sick leave, particularly two years after completing an IPRP.16,17 Nevertheless, chronic pain patients still describe a range of difficulties returning to work after completing an IPRP, a finding that suggests a need for further improvement of interventions and more tailored solutions in the return-to-work (RTW) rehabilitation process.18
The RTW process is complex as it involves a dynamic interaction between pain management, workplace adjustments, and management of work relationships ie, collaboration with and support from managers and colleagues.19 IPRP may be a part of the RTW process and work interventions may be a part of IPRP. IPRP – including work interventions with more focus on work demands and abilities including, for example, coordination, a RTW plan, workplace visits, functional capacity training, and/or ergonomic adjustments – have shown better effects on work participation than IPRP without work interventions.20,21 Furthermore, workplace integrated care programs delivered by allied health professionals can decrease pain and improve functional status for employees with chronic musculoskeletal disorders.22 Therefore, learning to cope with pain in relation to work and intertwining work interventions in medical rehabilitation seem to be important. However, although a study of functional restoration programs found that occupational issues often were assessed, only a few programs included work intervention or adapted the program to reflect assessments.23 In 2013, Wåhlin et al found that patients with mental disorders were more likely to be offered work interventions (40%) than patients with musculoskeletal disorders (25%) in a primary care and occupational health-care settings.24 Professionals working with IPRP in primary care tend to focus on health-related aspects during rehabilitation and consider RTW and work rehabilitation as outside the purview of IPRP – ie, issues for other stakeholders.25 However, qualitative evidence suggests that patients with chronic pain need support and improved collaboration from both healthcare and workplace settings.26
The extent work interventions are a part of IPRP in Sweden and worldwide probably differ. It is also unclear what patients within IPRP are offered work interventions and on what indications. No core set of predictors for RTW for chronic pain patients exists that can guide selection, neither independent of interventions27 nor in relation to IPRP.
To inform further studies and to develop more tailored interventions to improve RTW for patients with chronic pain who have participated in IPRP, more knowledge is needed on the extent of work interventions within IPRP today, what patients participate in these interventions, and whether there is an association with changes in self-rated work ability after IPRP. Studies on patients with chronic pain have repeatedly identified self-rated work ability as a predictor for work participation and for RTW.28,29
Here, we explore the frequency of participation in work interventions and the characteristics of patients who participate in work interventions within IPRP at specialist pain rehabilitation departments in Sweden. In addition, we explore the association between participation in work interventions and change in patients’ self-rated work ability after IPRP.
Method
Context
Pain Rehabilitation in Sweden
Interdisciplinary pain rehabilitation programs (IPRPs) are group-based bio-psycho-social interventions planned and delivered by a team of professions (ie, physical therapists, psychologists, occupational therapists, and/or physicians) that include education, physical training, CBT, and/or a social/work component. There is no golden standard for the content, extent and design of IPRP, rather the arrangement of IPRPs somewhat differs between departments.12 However, common general goals for IPRPs are reduced pain, improved mental health, improved health and quality of life, and increased participation in activities/work and social life. In addition, more specific individual goals are identified in relation to the patients’ specific problems.12 Between 2008 and 2020, the Swedish government financially supported IPRPs as an evidence-based intervention to help people with chronic pain improve their health and ability to RTW. IPRPs are offered both at the primary care level and the specialist care level when complex pain conditions are present that include, for example, psychiatric comorbidity. Specialist pain rehabilitation departments offer IPRP to some patients. Some general criteria are used to determine whether to offer IPRP – eg, living with complex chronic benign pain that does not improve using monodisciplinary interventions, the ability to cope with pain is negatively affected by co-morbidities and/or social/work strains, being motivated to behavioural and cognitive change.
Swedish Quality Registry for Pain Rehabilitation (SQRP)
All 41 specialist pain rehabilitation departments in Sweden send data to the Swedish Quality Registry for Pain Rehabilitation (SQRP). SQRP, a national quality registry for pain rehabilitation, collects data primarily from patient-reported data (PROM) and aims to be a base for structured follow-up, clinical development, and research. All patients are asked to participate before their first visit to the pain rehabilitation department. Patients who agree to participate complete questionnaires near the time for their first visit (questionnaire 1). Patients who participate in IPRP also complete the same questionnaires directly after IPRP (questionnaire 2). See Table 1 for description of instruments and questions in questionnaires 1 and 2 included in this study. One part of SQRP includes staff-reported data where, since August 2016, patient participation in different work interventions during IPRP is registered.
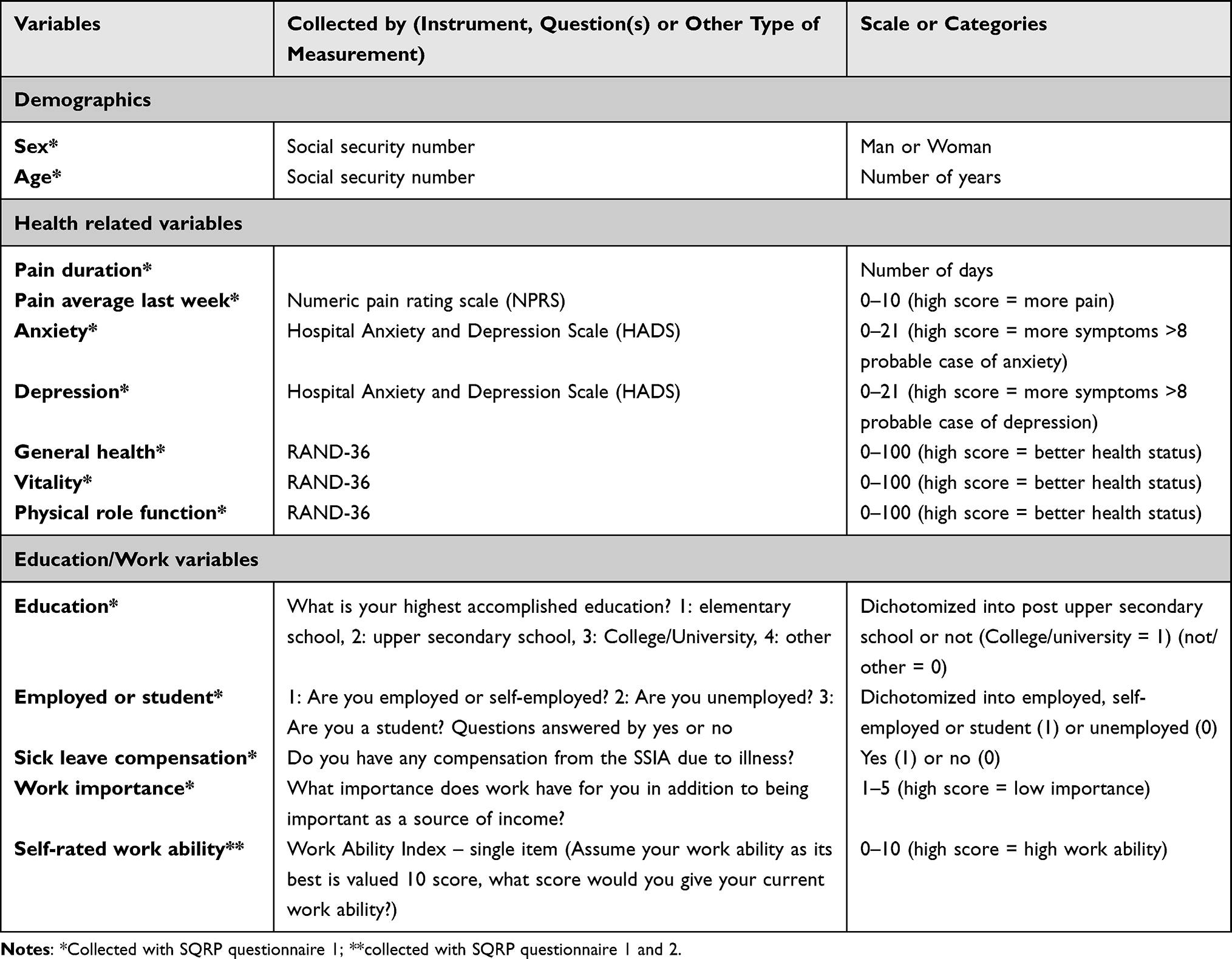 |
Table 1 Overview of Patient Characteristics Variables |
Swedish Sickness Insurance System
In Sweden, all citizens with an income are insured by the Swedish sickness insurance system. This provides economic security in the event of sickness, injury, or disability. The Swedish Social Insurance Agency (SSIA) assesses whether an applicant has the right to receive compensation. Day one of sickness is unpaid. The next 13 days are paid by the employer, and from day 14 as long as eligible (no time limit), the compensation is paid by SSIA.30 Although unemployed people are not eligible for sickness compensation, they can apply for benefits from the unemployment benefit office. People not eligible for sickness benefits or for unemployment benefits can apply for economic support from their municipality. All forms of benefits are time-bound and include specific demands on the individual to be active in rehabilitation and/or actively seeking employment or participating in some sort of educational program.
Participants
Inclusion criteria for the study were registered in SQRP as participants in an IPRP between August 2016 and January 2018. In addition, to ensure the participants were current for work or education, ie, self-supporting activities, they had to be between 18 and 65 years old. All benign pain diagnoses were included. Some of the most common diagnosis in SQRP are chronic low back pain, chronic neck pain, chronic wide-spread pain, ie, fibromyalgia and Ehlers Danlos syndrome.
Work Interventions
At the end of the IPRP, staff answer questions in the SQRP that address what work interventions each patient participated in. Four categories of work interventions can be reported by staff and each patient may have taken part in all, some, or none of these: ergonomic intervention, RTW plan, stakeholder meeting, and workplace visit. These categories have been identified and selected by clinicians and researchers within the SQRP network. There is no common definition in SQRP for these interventions or categories. However, ergonomic interventions can be described as a broad group of interventions that may include advice and practice working and using equipment as well as issues related to psychosocial and/or organizational aspects of work. The RTW plan aims to help patients and the stakeholders after the patients have completed an IPRP. Goals, strategies, and activities from different stakeholders may be a part of the written plan. Stakeholder meetings are interventions where at least one other stakeholder (other than IPRP) involved in the RTW rehabilitation process meets during the IPRP to discuss prerequisites and plan for RTW with the patient. Workplace visits may involve any interventions performed at the workplace – eg, assessment of the work environment, discussion with employer, and adjustment of workplace. Ergonomic intervention, RTW plan and stakeholder meeting can be actual for both employed and/or students and unemployed patients. All four work interventions may be applied for work or post upper secondary school context depending on the goal for each patient. The choice of work interventions are optional and not all pain departments offer all four work interventions. Some work interventions may be mandatory within IPRP at some departments, and others are individually chosen by the team and the patient in relation to the specific problems and goals for each specific patient within IPRP.
Patient Characteristics
Patient characteristic variables were mainly PROM measures gathered from the SQRP (questionnaire 1) and chosen to get a broad description of the patient group, covering a bio-psycho-social spectrum of variables (Table 1).
Demographics
Demographics included in the study were sex (woman or man) and age (years).
Health-Related Variables
Pain was measured by self-reported duration (date of pain onset) and pain intensity last week (numeric pain rating scale).31 Anxiety and depression were measured with the Hospital Anxiety and Depression Scale (HADS). HADS, a brief questionnaire developed to screen for emotional disturbances for non-psychiatric patients, contains 14 items evenly divided for anxiety and depression on two separate subscales ranging between 0 and 21 where a score >8 indicates a probable case and >11 indicates a definite case.32 General health, vitality, and physical role function were measured with RAND-36, a generic profile measure for health-related quality of life. RAND-36 includes 36 items that together assesses eight multi-item health concepts.33 Vitality was used as a proxy for energy/fatigue and physical role function as a proxy of activity performance and participation.
Education/Work Variables
Education was dichotomized into post upper secondary school or no post upper secondary school. Employment status and student status were merged into one variable and dichotomized into employed and/or student or not. Sick leave compensation was answered by the patients as either “yes” or “no”. Work importance besides value as economic income was reported on a Likert-type scale (1–5) where 1 = very high importance and 5 = no importance. Self-rated work ability was measured by work ability index (WAI) single item question concerning current work ability compared with the lifetime best, with a possible score of 0 (completely unable to work) to 10 (work ability at its best).34
Analysis
Statistical analyses were performed in IBM SPSS statistics 26, but Cohen’s d was calculated with the supplementary XLSX file in Lakens (2013).35 The data were extracted from the SQRP for the dates 1 August 2016 to 31 January 2018. Groups were identified within the cohort and dichotomized – ie, woman vs man and employed and/or student vs unemployed. Descriptive statistics for the variables were calculated for each subgroup separately based on SQRP questionnaire 1. Differences between groups were analysed with independent t-test for continuous variables and Fisher’s exact test for categorical/dichotomized variables. In addition, the cohort was dichotomized as either participation or no participation in the different work interventions (part 1). Differences between the group that had participated in an intervention and the group that had not participated in the same intervention were also analysed with independent t-test or Fisher’s exact test depending on variable level (part 2). Multiple comparisons in parts 1 and 2 were Bonferroni-corrected, and the significance level was calculated by dividing the primary significance level (0.05) with the number of comparisons (82), resulting in a critical p-value of 0.0006. Effect sizes were described with Cohen’s d for continuous variables, identifying 0.2–0.49 as low, 0.50–0.79 as medium, and >0.8 as large effect size.35 Effect sizes for categorical/dichotomized variables were described with odds ratio (OR).
The association between change in self-rated work ability from inclusion (SQRP questionnaire 1) to end of IPRP (SQRP questionnaire 2) and participation in work interventions were analysed with multiple regression analysis and adjusted for self-rated work ability at inclusion (SQRP questionnaire 1), sex and interaction between sex and intervention, and employment and interaction between employment and intervention (part 3). Between-subject effects were calculated for each intervention analysis and presented with partial eta squared (0.01–0.059 = small, 0.06–0.139 = medium, >0.14 = large effect size). In addition, the association between change in self-rated work ability and the combination of interventions were analysed with the same regression model. Change in self-rated work ability was defined as the absolute difference in self-rated work ability between questionnaire 2 and questionnaire 1 for each patient.
Results
Patient Characteristics at Inclusion to IPRP (Part 1)
In SQRP, there were 3809 patients registered as participants in an IPRP between 2016 and 2018. The mean age was 44.7 years (range 18–65) and 79.2% were women. The mean pain duration was 3237 days, and the pain intensity was on average 6.6 (SD = 1.9) at inclusion in IPRP, 86% were employed and/or students, and 61.8% were on sick leave compensation. The mean of their self-rated work ability was 3.4 (SD = 2.5) (Table 2).
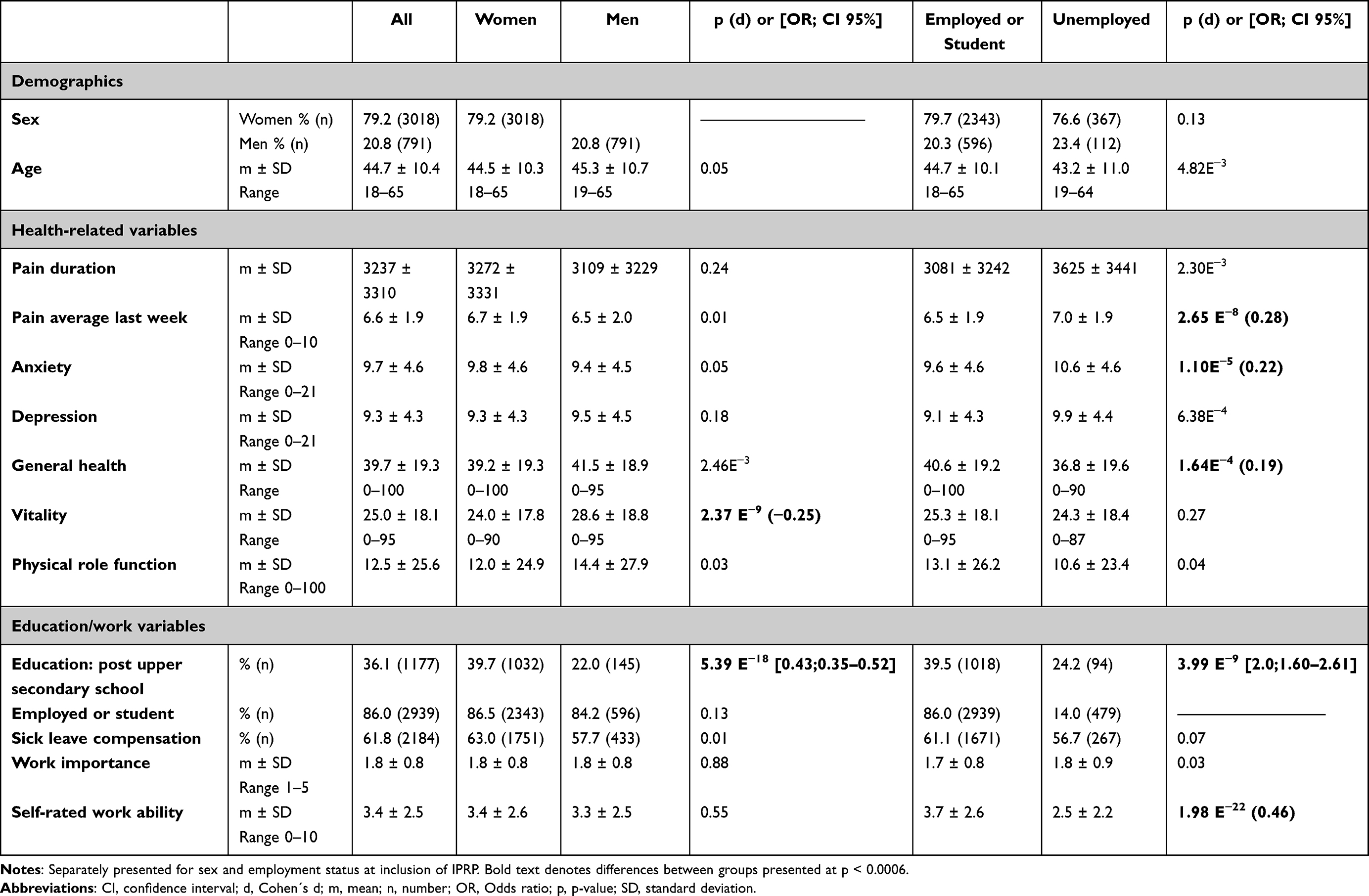 |
Table 2 Patient Characteristics for Patients Who Have Participated in IPRP |
At inclusion of IPRP, the mean ratings indicated a probability of both anxiety and depression (HADS mean ratings >8) for both women and men and significant higher rates concerning anxiety for the unemployed. General health (RAND-36) was significantly lower for unemployed patients. Vitality (RAND-36) was significantly lower for women than men, but there was no difference related to employment status. Pain intensity was higher for unemployed than for employed and/or students.
The proportion of post upper secondary school education was significantly higher in the group of women and for employed patients. There was no difference concerning self-rated work ability between women and men, but unemployed patients rated their work ability significantly lower than employed patients.
Overall, small effect sizes were found – ie, there were very small to small clinical important differences between the groups of men/women and employed/unemployed at inclusion to IPRP. One exception was self-rated work ability, where a medium effect size between employed and unemployed patients was found. See Table 2 for more details on patient characteristics at inclusion of IPRP.
Frequency of Work Interventions During IPRP (Part 2)
Most patients (n = 2822, 90.9%) participated in one or more work interventions during IPRP. Ergonomic interventions (n = 2229, 70.4%) and a RTW plan (n = 2748, 84.8%) were the most common work interventions. About a third (n = 1230, 32.3%) of the patients participated in stakeholder meetings, but only 4.2% (n = 136) participated in a workplace visit (Table 3). The most frequent combination of work interventions was ergonomic interventions together with a RTW plan (n = 1969). The second most frequent was a RTW plan together with stakeholder meeting (n = 1071). The least frequent was stakeholder meeting together with workplace visit (n = 90).
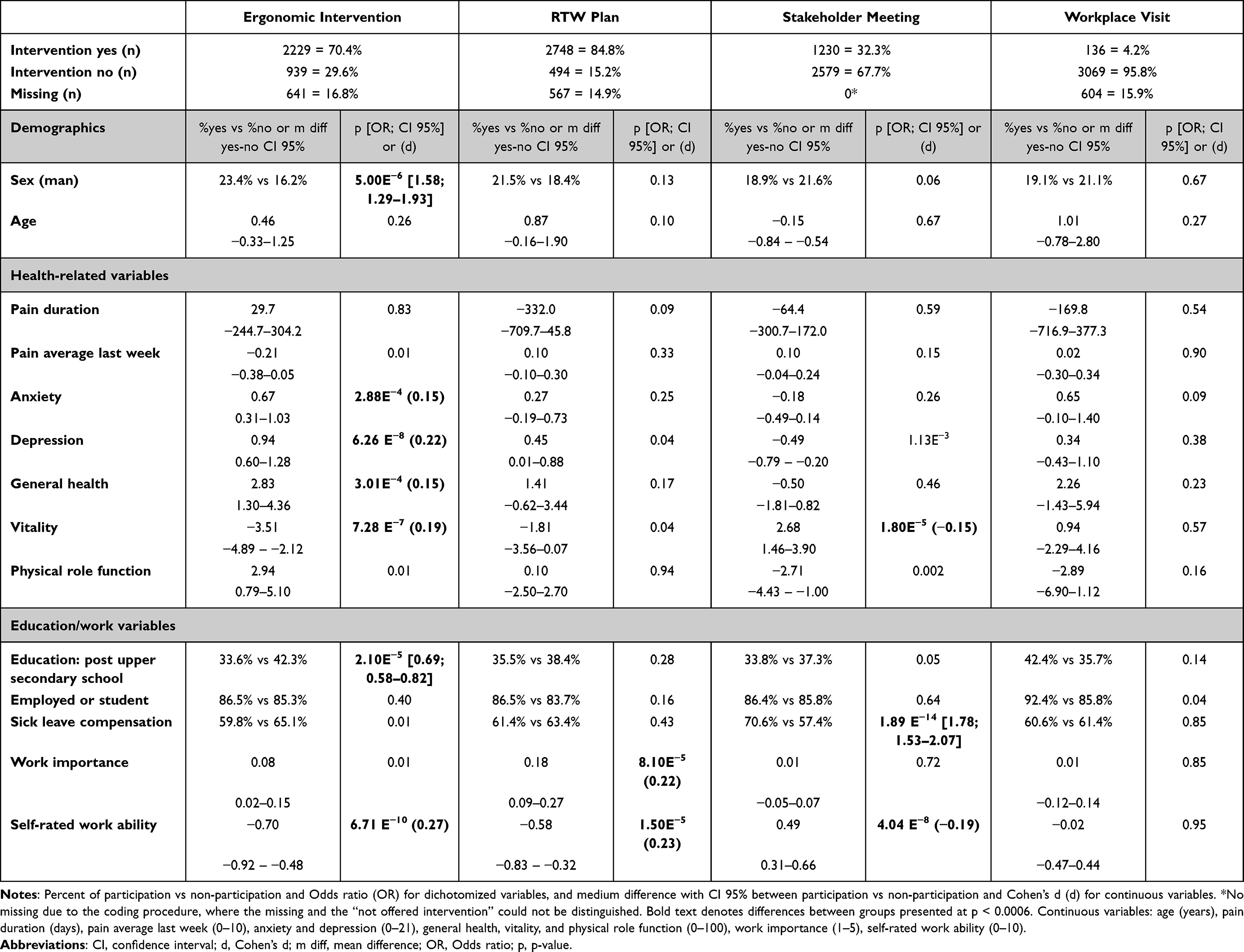 |
Table 3 Differences in Patient Characteristics at Inclusion of IPRP Between Patients Who Had or Had Not Participated in Different Work Interventions During IPRP |
Patient Characteristics for Participation in Work Interventions (Part 2)
Table 3 lists the frequencies of work interventions and patient characteristics in relation to participation in work interventions.
Ergonomic interventions were more common for men (OR = 1.58) and for patients with slightly better health concerning anxiety (d = 0.15), depression (d = 0.22), general health (d = 0.15), and vitality (d = 0.19) (Table 3). Patients participating in ergonomic interventions had lower education (OR = 0.69) and they rated their work ability higher (d = 0.27) than patients who did not participate in ergonomic interventions (Table 3).
Unlike ergonomic interventions, patients with lower vitality (d=−0.15) participated more frequently in stakeholder meetings. In addition, the patients more frequently relied on sick leave compensation (OR = 1.78) and they rated their work ability lower (d = −0.19) than patients who did not participate in stakeholder meetings (Table 3).
Patients who took part in a RTW plan rated importance of work (d = 0.22) and their work ability (d = 0.23) higher than patients who did not take part in a RTW plan. These groups had no significant differences concerning demographics or health-related variables (Table 3). In addition, there were no significant differences between patients who participated in a workplace visit and those who did not.
Association Between Work Intervention and Change in Self-Rated Work Ability (Part 3)
Table 4 presents the association between change in self-rated work ability from inclusion to end of IPRP and participation in work interventions. When controlling only for initial self-rated work ability, the ergonomic intervention (B = 0.36, p < 0.001) and the RTW plan (B = 0.67, p < 0.001) had a positive association with change in self-rated work ability. The stakeholder meeting had a negative association with self-rated work ability (B = −0.44, p < 0.001). No significant association was identified between workplace visit and change in self-rated work ability (Table 4).
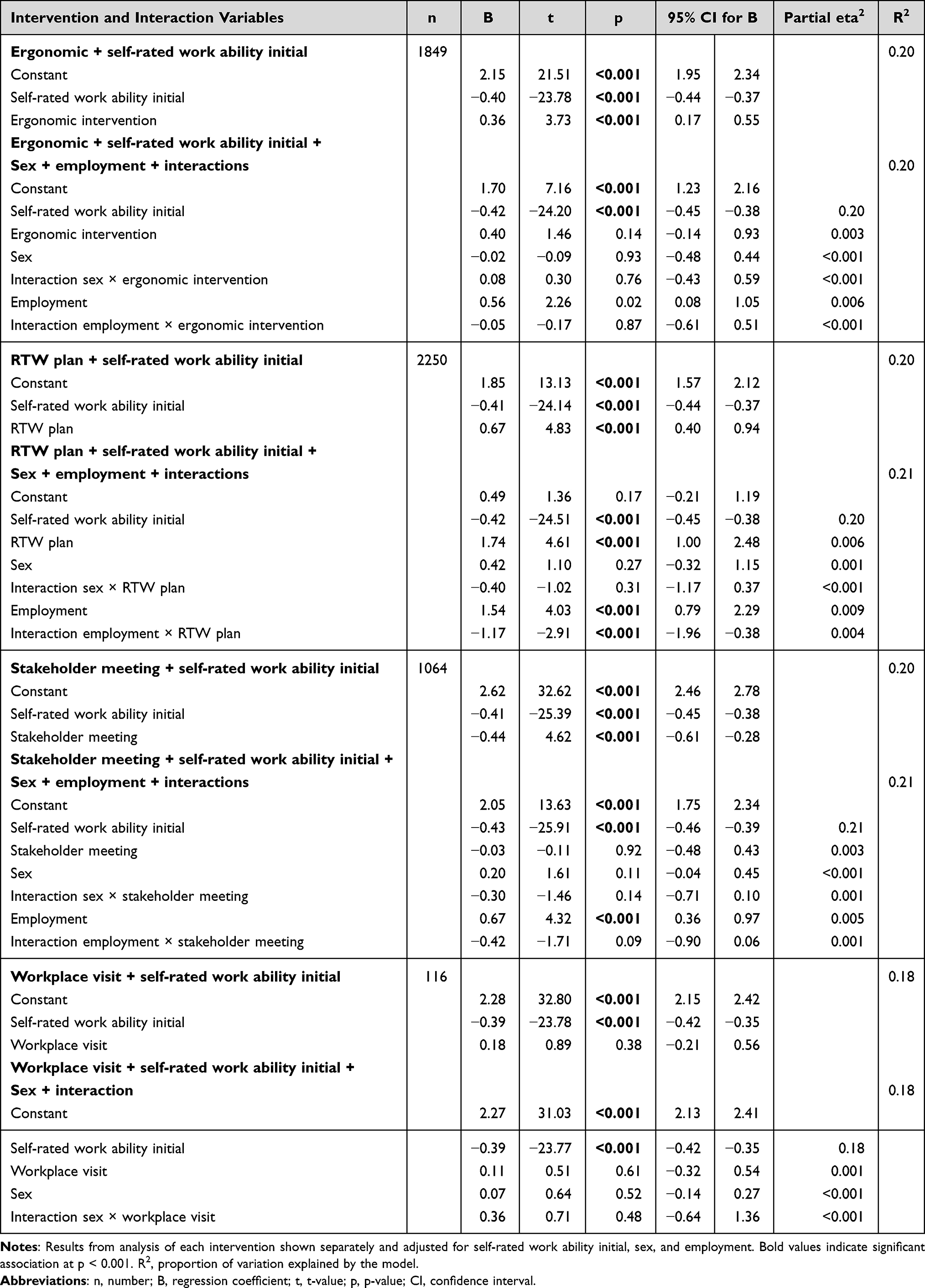 |
Table 4 Association Between Change in Self-Rated Work Ability from Inclusion to End of IPRP and Participation in Work Interventions |
With sex and employment added to the model, the initial score of self-rated work ability best explained the change in self-rated work ability (partial eta2 = 0.18–0.21) in relation to all interventions and other variables. Employment also showed significant associations, and the RTW plan was the only intervention that still had a significant association with change in self-rated work ability, both with effect sizes lower than what usually qualifies as small effects. Employment had a stronger association with change in self-rated work ability than the ergonomic intervention and the stakeholder meeting. Sex and the interaction variables did not add any significant information to the association with change in self-rated work ability for any of the interventions (Table 4).
The analysis of combination of interventions resulted in a significant association for the RTW plan with change in self-rated work ability in combination with the three other interventions separately. None of the other interventions had significant association with change in self-rated work ability in combination with the RTW plan. The ergonomic intervention had a significant association with change in self-rated work ability in combination with stakeholder meeting and workplace visit separately.
Discussion
This study explores work interventions within IPRP in Sweden between 2016 and 2018. The main results indicate a high participation rate in some work interventions (90.2%) although there were differences between different work interventions (RTW plan: 84.8%; Ergonomic intervention: 70.4%; Stakeholder meeting: 32.3%; Workplace visit: 4.2%). There were some differences concerning characteristics of patients who participated in different work interventions. That is, patients with better rates for health- and work-related variables participated in ergonomic intervention and RTW plan. The RTW plan had the strongest association with a change in self-rated work ability post IPRP, but the initial score of self-rated work ability best explained the change.
The interventions as well as the context and the patients involved in this study were characterised by complexity. Chronic pain is a complex condition that involves biological, psychological, and social aspects.3 Both IPRP and work interventions are complex interventions may have different dimensions of complexity – eg, a number of interactions between components, difficulty of behaviours associated with delivering and receiving the intervention, different groups and organizational levels targeted by the intervention, variability of outcomes, and degree of flexibility and tailoring of the intervention.36,37 Studying complex interventions for people with complex conditions such as pain is not straight forward work;12 rather, the different dimensions of complexity need consideration. Drawing on this, it would be considered as important with as much clarity as possible on the characteristics of the patients and the prerequisites of the interventions to be studied before moving on with studies on effects with more inferential approaches. Little research has been done on work interventions within IPRP and there is a need of deeper understanding. Therefore, to build an important foundation for future scientific endeavours, an explorative descriptive approach was used in the real-life setting of IPRP in Sweden.
The importance of intertwining work interventions with bio-psycho-social pain rehabilitation such as IPRP has been shown in earlier studies.20–22,38 However, little research has focused on how work interventions are included in IPRP. This study adds to this knowledge, as it found that about 90% of the patients in Sweden who are enrolled in an IPRP participate in some kind of work intervention. Interestingly, frequency of work interventions varies, from 84.8% for RTW plan to 4.2% for workplace visit. From these results, we cannot draw any conclusions regarding the underlying reasons or motives for the selection and the variance in frequency. One could argue that participation in work interventions occurs in relation to the patient’s needs. However, the selection is not always that easy and earlier research has raised the need for more tailored solutions in relation to the patient’s needs.18 Selecting patients for IPRP may be guided by the professionals’ preconceptions of who could benefit most, beliefs that could be based on diagnoses, sex, or culture.39 Michel et al found that although work issues may be a part of the assessment, they are not always addressed in the rehabilitation.23 Resource aspects such as economic costs and time consumption may also be reasons for using or not using an intervention, resulting in patients in need of a workplace visit not being offered the intervention. Some pain rehabilitation departments use work interventions such as workplace visits and others do not, depending on local priorities of resources. To better understand how and why patients are selected for the work interventions, future research should include more knowledge on patients’ characteristics and proportion of interventions in relation to the pain rehabilitation departments and indications for selection of interventions.
In this study, the RTW plan stood out from the other interventions in two ways: most patients (84.8%) participated in the RTW plan and it had the relatively strongest association with change in self-rated work ability. Earlier studies have raised the importance of a RTW plan for RTW outcomes.18,40 For example, patients have expressed a desire to be informed about steps in their rehabilitation, not only at the end of IPRP but also continually during their RTW rehabilitation process. Therefore, it could be seen as a positive result that the RTW plan is frequently offered to the patients within IPRP in Sweden. However, there is not a clear definition of a RTW plan in the context of IPRP and RTW plans are frequently used in combination with both ergonomic intervention and stakeholder reconciliation meetings. These facts need consideration when interpreting the results.
Qualitative evidence suggest the value of collaboration between stakeholders, clear communication, and transfer of knowledge and information.26 Surprisingly, in this study, the association between the stakeholder meeting and self-rated work ability indicated lower improvement for patients who were offered the intervention. One explanation may be that stakeholder meetings were offered to a rather vulnerable group of patients with lower vitality, lower self-rated work ability, and that were more frequently on sick leave. In addition, the stakeholder reconciliation meetings are often scheduled for the end of IPRP and could be perceived as stressful and demanding by the patients. The effects of the stakeholder reconciliation meeting may not be seen in association with self-rated work ability in the short perspective, as the meeting can be seen as a part of an ongoing stakeholder collaboration that needs continuity and may facilitate RTW in the long run. However, results from earlier studies18,41 as well as this study indicate that stakeholder collaboration and reconciliation meetings need improvements to be truly supportive and empowering for the patient.
According to the results of this study, unemployed patients are a vulnerable group with low ratings concerning both health- and work-related variables overall. Poorer health, lower education, and lower self-rated work ability indicate that patients are in a tough situation due to unemployment and therefore need support. These results agree with earlier studies that have identified higher levels of mental distress and lower quality of life for non-workers (sick leave and/or unemployed) compared to workers with chronic pain42 and more negative feelings, poorer self-esteem, and less acceptance for the pain and life situation.43 Still, Saunders et al found that work is meaningful and important to address for people who can no longer work due to chronic pain,44 indicating the importance of finding effective strategies and work interventions for this group. In this study, being employed had a positive association with change in self-rated work ability and a stronger association than the work interventions per se. In other words, the unemployed patients within IPRP received less benefit from work interventions when it came to change in self-rated work ability. In a qualitative study, Patel et al found that unemployed people with chronic pain perceived personal obstacles as well as barriers within health care and the benefit organisations that needs to be specifically addressed for the unemployed.45 As the prerequisites are rather different for the employed and the unemployed patients, further research should focus specifically on each group of patients so interventions can be tailored for employed and unemployed patients.
Some significant differences were evident between women and men upon inclusion to an IPRP. A higher proportion of women than men had a higher education and, in general, women compared to men rated their vitality lower. These results agree with an earlier study on the SQRP population.46 As there are differences between women and men regarding factors affecting the results of IPRP concerning sick leave,47 future studies should include gender analysis.
During the last decade, the Swedish government has pushed to include more work interventions within healthcare. For example, an agreement between the government and the Swedish association of local authorities and regions (SALAR)48 has been updated yearly between 2006 and 2020 for economic support to focus on strategies and interventions to decrease sick leave. As shown in this study, work interventions are a part of IPRP for many patients (90%). We have been able to explore and broadly describe the present situation based on real-life data. It is important to follow these data as well as to find ways to better understand the content and meaning of work interventions within IPRP. Future studies may focus on predictors for work interventions or examine the effect of work interventions concerning both work and health outcomes in a longer perspective. For example, a RCT study with well-defined work interventions added to the IPRP could better examine the effect of the work intervention component. However, work interventions also need to be considered as complex interventions in a complex context. However, it may be difficult and perhaps inappropriate to study the different parts of the intervention as the effect of the intervention may be the result of its holistic approach and the combination of interventions, individually tailored for each patient.
Strength and Limitations
The four work interventions included in this study are not fully distinguished as they overlap to some degree. A recently published review on interventions to promote work-focused care (ie, work interventions within healthcare) presented positive results concerning work-related outcomes overall.49 However, they highlighted the issue with a heterogeneity and variability in categorizing the work-focused interventions and concluded that the effectiveness of components could not be clarified. A common shared description of the content of work focused care would facilitate interpretation of results and comparison between studies. Xie et al presented six categories or elements of work-focused care: vocational advice/coaching or education, work-related assessment, involvement of the workplace stakeholders, regular communication with multidisciplinary team members, restoration of fitness for work, and training of work-related skills.49 The four categories of work interventions in our study – ie, ergonomic intervention, RTW plan, stakeholder reconciliation meeting, and workplace visit – can be found in the description of one or several of the categories devised by Xie et al Although categories are not well defined and there may be an overlap, the strength of our categories is that they were identified by clinicians in the national SQRP network to fit what is actually offered to the patients within IPRPs in Sweden.
In this study, self-rated work ability was chosen as the main outcome (ie, the dependent variable) in the regression analysis. It was considered the most robust work-related outcome variable in the SQRP. Self-rated work ability measured with WAI has been used in earlier studies.15,28,29,50 It has also been shown to be associated with and predictive values for RTW.50,51 By improving self-rated work ability in the short run, RTW may be facilitated in the long run. However, there are no known clinically significant values for the change on a single item of the WAI. With this knowledge, it would have been theoretically possible to have developed more conclusions about the findings. Other health-related outcome measures would have been possible, but this study has a narrower focus – ie, work-related outcomes after IPRP.
For part 1 and part 2 of the study, Bonferroni-corrections were made and 82 separate analyses were calculated, which resulted in a critical p-value of <0.0006. With this rather conservative p-value, there is a risk of type II error – ie, there may be differences between the groups concerning more variables than the ones below the critical p-value of 0.0006. In the results section, all p-values are presented to help the reader interpret the results. As most of the effect sizes are below the value for small effect sizes, it was considered reasonable to use a conservative p-value.
Conclusion
To slow the trend of increasing sick leave rates, there has been a recent push to include more work interventions within healthcare. At the same time, there is a need to tailor interventions and improve the work-related outcomes of IPRPs. This study adds to the knowledge that most patients within IPRPs in Sweden between 2016 and 2018 participated in one or more work interventions. The results indicated some differences in characteristics between patients who participated in certain work interventions and those who did not. The RTW plan was the most frequent work intervention, and it was also the intervention that had the strongest association with a positive change in self-rated work ability after the IPRP intervention. However, the initial score of self-rated work ability best explained the change, with higher scores at the start of IPRP resulting in less improvement. Furthermore, this study confirmed the vulnerable situation of unemployed patients. As the effect sizes were small, more knowledge is needed on how to select and tailor complex interventions to improve outcomes and decrease sick leave after completing an IPRP.
Ethics Approval
This study was approved by the national ethics committee in Sweden [EPN: 2018/036] and [EPM 2019 – 02167].
Acknowledgment
The authors would like to thank the DU/Pain group at Dalarna University for sharing data from their research database FRIDA. The database FRIDA was funded by Swedish Research Council [Vetenskapsrådet: 2015-02512] and by the Swedish Research Council for Health, Working Life and Welfare [FORTE: 2017-00177].
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was funded by the Swedish Research Council for Health, Working Life and Welfare [FORTE: 2016-07414].
Disclosure
The authors report no conflicts of interest in this work.
References
1. Breivik H, Collett B, Ventafridda V, Cohen R, Gallacher D. Survey of chronic pain in Europe: prevalence, impact on daily life, and treatment. Eur J Pain. 2006;10(4):287–333. doi:10.1016/j.ejpain.2005.06.009
2. Harker J, Reid KJ, Bekkering GE, et al. Epidemiology of chronic pain in Denmark and Sweden. Pain Res Treat. 2012;2012:371248. doi:10.1155/2012/371248
3. Mills SEE, Nicolson KP, Smith BH. Chronic pain: a review of its epidemiology and associated factors in population-based studies. Br J Anaesth. 2019;123(2):e273–e83. doi:10.1016/j.bja.2019.03.023
4. Fragoso ZL, McGonagle AK. Chronic pain in the workplace: a diary study of pain interference at work and worker strain. Stress Health. 2018;34(3):416–424. doi:10.1002/smi.2801
5. Lindegard A, Larsman P, Hadzibajramovic E, Ahlborg G
6. Wynne-Jones G, Buck R, Porteous C, et al. What happens to work if you’re unwell? Beliefs and attitudes of managers and employees with musculoskeletal pain in a public sector setting. J Occup Rehabil. 2011;21(1):31–42. doi:10.1007/s10926-010-9251-7
7. Försäkringskassan. Statistik. Pågående sjukfall efter diagnos. Secondary Statistik. Pågående sjukfall efter diagnos. [Ongoing illness after diagnosis. Secondary Statistics. Ongoing illness after diagnosis]. 2020. Swedish.
8. Ropponen A, Gémes K, Frumento P, et al. Predicting the duration of sickness absence spells due to back pain: a population-based study from Sweden. Occup Environ Med. 2020;77(2):115–121. doi:10.1136/oemed-2019-106129
9. Saunders SL, Nedelec B. What work means to people with work disability: a scoping review. J Occup Rehabil. 2014;24(1):100–110. doi:10.1007/s10926-013-9436-y
10. Lundberg T, Melander S. Key push and pull factors affecting return to work identified by patients with long-term pain and general practitioners in Sweden. Qual Health Res. 2019;29(11):1581–1594. doi:10.1177/1049732319837227
11. Kalsi P, Turkistani W, Sykes C, Lucas A, Zarnegar R. “Work is a beautiful thing.” Exploring attitudes towards employment in chronic pain (CP) patients attending a pain management programme (PMP). J Vocat Rehabil. 2016;44:97–107. doi:10.3233/JVR-150783
12. Gerdle BRFM, Ringqvist Å. Interdisciplinary pain rehabilitation programs - evidence and clinical real-world results. In: Pain Management - from Pain Mechanisms to Patient Care. London: IntechOpen; 2023.
13. Kamper SJ, Apeldoorn AT, Chiarotto A, et al. Multidisciplinary biopsychosocial rehabilitation for chronic low back pain: Cochrane systematic review and meta-analysis. BMJ. 2015;350:h444. doi:10.1136/bmj.h444
14. Ringqvist Å, Dragioti E, Björk M, Larsson B, Gerdle B. Moderate and stable pain reductions as a result of interdisciplinary pain rehabilitation – a cohort study from the Swedish Quality Registry for Pain Rehabilitation (SQRP). J Clin Med. 2019;8(6):905. doi:10.3390/jcm8060905
15. Saltychev M, Laimi K, Pentti J, Kivimäki M, Vahtera J. Short- and long-term changes in perceived work ability after interdisciplinary rehabilitation of chronic musculoskeletal disorders: prospective cohort study among 854 rehabilitants. Clin Rehabil. 2014;28(6):592–603. doi:10.1177/0269215513513602
16. LoMartire R, Dahlström Ö, Björk M, et al. predictors of sickness absence in a clinical population with chronic pain. J Pain. 2021;22(10):1180–1194. doi:10.1016/j.jpain.2021.03.145
17. Rivano Fischer M, Persson EB, Stalnacke BM, Schult ML, Lofgren M. Return to work after interdisciplinary pain rehabilitation: one- and two-year follow-up based on the Swedish quality registry for pain rehabilitation. J Rehabil Med. 2019;51(4):281–289. doi:10.2340/16501977-2544
18. Svanholm F, Liedberg GM, Löfgren M, Björk M. Factors of importance for return to work, experienced by patients with chronic pain that have completed a multimodal rehabilitation program - a focus group study. Disabil Rehabil. 2020;1–9. doi:10.1080/09638288.2020.1780479
19. Grant M, Froud R, Underwood M, Seers K, Seers K. The work of return to work. Challenges of returning to work when you have chronic pain: a meta-ethnography. BMJ Open. 2019;9(6):e025743. doi:10.1136/bmjopen-2018-025743
20. Beemster TT, van Bennekom CAM, van Velzen JM, Frings-Dresen MHW, Reneman MF. Vocational rehabilitation with or without work module for patients with chronic musculoskeletal pain and sick leave from work: longitudinal impact on work participation. J Occup Rehabil. 2020. doi:10.1007/s10926-020-09893-z
21. Streibelt M, Bethge M. Effects of intensified work-related multidisciplinary rehabilitation on occupational participation: a randomized-controlled trial in patients with chronic musculoskeletal disorders. Int J Rehabil Res. 2014;37(1):61–66. doi:10.1097/mrr.0000000000000031
22. Skamagki G, King A, Duncan M, Wåhlin C. A systematic review on workplace interventions to manage chronic musculoskeletal conditions. Physiother Res Int. 2018;23(4):e1738. doi:10.1002/pri.1738
23. Michel C, Guene V, Michon E, Roquelaure Y, Petit A. Return to work after rehabilitation in chronic low back pain workers. Does the interprofessional collaboration work? J Interprof Care. 2018;32(4):521–524. doi:10.1080/13561820.2018.1450231
24. Wåhlin C, Ekberg K, Persson J, Bernfort L, Öberg B. Evaluation of self-reported work ability and usefulness of interventions among sick-listed patients. J Occup Rehabil. 2013;23(1):32–43. doi:10.1007/s10926-012-9376-y
25. Hellman T, Jensen I, Bergstrom G, Busch H. Returning to work – a long-term process reaching beyond the time frames of multimodal non-specific back pain rehabilitation. Disabil Rehabil. 2015;37(6):499–505. doi:10.3109/09638288.2014.923531
26. Liedberg GM, Björk M, Dragioti E, Turesson C. Qualitative evidence from studies of interventions aimed at return to work and staying at work for persons with chronic musculoskeletal pain. J Clin Med. 2021;10(6):1247. doi:10.3390/jcm10061247
27. Steenstra IA, Munhall C, Irvin E, et al. Systematic review of prognostic factors for return to work in workers with sub acute and chronic low back pain. J Occup Rehabil. 2017;27(3):369–381. doi:10.1007/s10926-016-9666-x
28. Braathen TN, Veiersted KB, Heggenes J. Improved work ability and return to work following vocational multidisciplinary rehabilitation of subjects on long-term sick leave. J Rehabil Med. 2007;39(6):493–499. doi:10.2340/16501977-0081
29. Rashid M, Heiden M, Nilsson A, Kristofferzon ML. Do work ability and life satisfaction matter for return to work? Predictive ability of the work ability index and life satisfaction questionnaire among women with long-term musculoskeletal pain. BMC Public Health. 2021;21(1):584. doi:10.1186/s12889-021-10510-8
30. Socialdepartementet. Socialförsäkringsbalken (2010:110) [Social Insurance Code (2010:110)]; 2010. Swedish.
31. Dworkin RH, Turk DC, Farrar JT, et al. Core outcome measures for chronic pain clinical trials: IMMPACT recommendations. Pain. 2005;113(1–2):9–19. doi:10.1016/j.pain.2004.09.012
32. Lisspers J, Nygren A, Söderman E. Hospital Anxiety and Depression scale (HAD): some psychometric data for a Swedish sample. Acta Psychiatr Scand. 1997;96(4):281–286. doi:10.1111/j.1600-0447.1997.tb10164.x
33. Hays RD, Morales LS. The RAND-36 measure of health-related quality of life. Ann Med. 2001;33(5):350–357. doi:10.3109/07853890109002089
34. Ahlstrom L, Grimby-Ekman A, Hagberg M, Dellve L. The work ability index and single-item question: associations with sick leave, symptoms, and health--a prospective study of women on long-term sick leave. Scand J Work Environ Health. 2010;36(5):404–412. doi:10.5271/sjweh.2917
35. Lakens D. Calculating and reporting effect sizes to facilitate cumulative science: a practical primer for t-tests and ANOVAs. Front Psychol. 2013;4:863. doi:10.3389/fpsyg.2013.00863
36. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. Int J Nurs Stud. 2013;50(5):587–592. doi:10.1016/j.ijnurstu.2012.09.010
37. Skivington K, Matthews L, Simpson SA, et al. A new framework for developing and evaluating complex interventions: update of medical research council guidance. BMJ. 2021;374:n2061. doi:10.1136/bmj.n2061
38. Kuoppala J, Lamminpää A. Rehabilitation and work ability: a systematic literature review. J Rehabil Med. 2008;40(10):796–804. doi:10.2340/16501977-0270
39. Stenberg G, Pietilä Holmner E, Stålnacke BM, Enthoven P. Healthcare professional experiences with patients who participate in multimodal pain rehabilitation in primary care - a qualitative study. Disabil Rehabil. 2016;38(21):2085–2094. doi:10.3109/09638288.2015.1114156
40. van Vilsteren M, van Oostrom SH, de Vet HC, Franche RL, Boot CR, Anema JR. Workplace interventions to prevent work disability in workers on sick leave. Cochrane Database Syst Rev. 2015;10:Cd006955. doi:10.1002/14651858.CD006955.pub3
41. Seing I, Stahl C, Nordenfelt L, Bulow P, Ekberg K. Policy and practice of work ability: a negotiation of responsibility in organizing return to work. J Occup Rehabil. 2012;22(4):553–564. doi:10.1007/s10926-012-9371-3
42. Stedenfeldt M, Kvarstein G, Nilsen TIL, Schjødt B, Borchgrevink PC, Halsteinli V. Pre-consultation biopsychosocial data from patients admitted for management at pain centers in Norway. Scand J Pain. 2020;20(2):363–373. doi:10.1515/sjpain-2019-0076
43. Glavare M, Löfgren M, Schult ML. Between unemployment and employment: experience of unemployed long-term pain sufferers. Work. 2012;43(4):475–485. doi:10.3233/wor-2012-1394
44. Saunders S, Nedelec B, MacEachen E. Work remains meaningful despite time out of the workplace and chronic pain. Disabil Rehabil. 2018;40(18):2144–2151. doi:10.1080/09638288.2017.1327986
45. Patel S, Greasley K, Watson PJ. Barriers to rehabilitation and return to work for unemployed chronic pain patients: a qualitative study. Eur J Pain. 2007;11(8):831–840. doi:10.1016/j.ejpain.2006.12.011
46. Gerdle B, Boersma K, Åsenlöf P, Stålnacke BM, Larsson B, Ringqvist Å. Influences of sex, education, and country of birth on clinical presentations and overall outcomes of interdisciplinary pain rehabilitation in chronic pain patients: a cohort study from the Swedish quality registry for pain rehabilitation (SQRP). J Clin Med. 2020;9(8):2374. doi:10.3390/jcm9082374
47. Spinord L, Kassberg AC, Stålnacke BM, Stenberg G. Multivariate correlations between pain, life interference, health-related quality of life and full-time sick leave 1 year after multimodal rehabilitation, focus on gender and age. Scand J Occup Ther. 2021;1–15. doi:10.1080/11038128.2021.1903990
48. Regioner RoSko. En kvalitetssäker och effektiv sjukskrivnings- och rehabiliteringsprocess. Stockholm: Sveriges Kommuner och Regioner (SKR); 2020 [A quality-assured and efficient sick leave and rehabilitation process - Agreement between the state and SKR 2020. Stockholm: Swedish Municipalities and Regions (SKR); 2020]; 2020. Swedish.
49. Xie Y, Hutting N, Bartys S, Johnston V. Interventions to promote work-focused care by healthcare providers for individuals with musculoskeletal conditions a scoping review. J Occup Rehabil. 2021;31(4):840–865. doi:10.1007/s10926-021-09971-w
50. Wåhlin C, Ekberg K, Persson J, Bernfort L, Oberg B. Association between clinical and work-related interventions and return-to-work for patients with musculoskeletal or mental disorders. J Rehabil Med. 2012;44(4):355–362. doi:10.2340/16501977-0951
51. Ståhl C, Karlsson N, Gerdle B, Sandqvist J. Predictive validity of general work ability assessments in the context of sickness insurance. J Rehabil Med. 2021;53(4):jrm00177. doi:10.2340/16501977-2798
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.