Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Words Matter: Content Analysis of Language Used When Documenting in the Medical Records of Patients in Mental Health
Authors Zolezzi M ![]() , Elamin SA
, Elamin SA ![]() , Abdallah O
, Abdallah O ![]() , Eltorki Y
, Eltorki Y ![]() , Alhathal T, Maklad E, Alkhuzaie N
, Alhathal T, Maklad E, Alkhuzaie N
Received 26 October 2025
Accepted for publication 19 February 2026
Published 21 March 2026 Volume 2026:19 576861
DOI https://doi.org/10.2147/JMDH.S576861
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Monica Zolezzi1 ,† Shahd Abubaker Elamin,1 Oraib Abdallah,2 Yassin Eltorki,2 Turfa Alhathal,3 Esraa Maklad,4 Noriya Alkhuzaie2
1College of Pharmacy, Qatar University, Doha, Qatar; 2Mental Health Services, Hamad Medical Corporation, Doha, Qatar; 3Aisha Bint Hamad Al-Attiyah Hospital, Hamad Medical Corporation, Doha, Qatar; 4Pharmacy Clinical Services Unit, Sidra Medicine, Doha, Qatar
†Prof Monica Zolezzi passed away on June 29th, 2025
Correspondence: Shahd Abubaker Elamin, College of Pharmacy, Qatar University, Doha, Qatar, Email [email protected]
Background: Biased healthcare documentation adversely impacts patient outcomes, by affecting providers’ perceptions. Identifying stigmatizing language is crucial for appropriate workforce training.
Purpose: To identify, describe, and compare language patterns used in medical records of individuals with mental illness.
Methods: Patient encounters within the sole Qatari mental health governmental provider were randomly selected. Rich-text notes documented by any of eight eligible healthcare fields, written October–December/2021, and taking place during outpatient, inpatient, or community-homecare encounters were analyzed qualitatively for positive and negative language, and quantitatively for the percentage of notes with language types/subtypes. Association between language and patient/provider characteristics was tested using Goodness-of-fit chi2 and Fisher’s exact test, as appropriate.
Results: Of 300 notes, most included potentially stigmatizing language (62.7%). Disability-first and inappropriate treatment-related language were the top isolated subtypes (33.22% and 31.31% of negative notes, respectively). Similarly, 66.67% of notes incorporated positive statements, mainly personalized language (44%). Positive language was statistically associated with specialty, age, diagnosis, discipline, setting, and patient’s first language. Stigmatizing language was statistically associated with setting, physician level, and discipline.
Conclusion: Content analysis of mental health notes highlighted comparable use of positive and negative language. These findings urge policymakers and educators to advocate for recovery-oriented mental health documentation.
Keywords: stigmatizing language, recovery-oriented practice, clinical documentation, healthcare communication, person-centered care
Introduction
Stigma against mental illness has been deep-rooted for millennia across societies around the world, and it is often perpetuated by the words used to describe mental illnesses and those experiencing them.1,2 Language is used to communicate, educate and inform, but if not used appropriately, it can also confuse, mislead and alienate.3 In healthcare, language is one of the main practice tools used to transfer information between patients and healthcare providers (HCPs) and plays a major role in shaping therapeutic relationships.2–4
Even when records are only accessed by providers, using stigmatizing language in patient medical records can foster negative attitudes and biases among the providers themselves. Such language might shape the perceptions and decisions of providers through reinforced stereotypes, sometimes without even meeting the patient. Patients who are stigmatized may encounter a self-fulfilling prophecy, where negative impressions from past clinicians influence their interactions with new ones, ultimately leading to health disparities and marginalization within the healthcare system.5 In fact, growing research in this field highlighted that stigmatizing language in medical narratives, both spoken and written, can perpetuate ingrained biases.6–8 For example, in studies using case vignettes, clinicians who assessed the vignette with stigmatizing language describing patients were more likely to have negative attitudes toward them and provided an overall lower quality of care.6–8
Recently, studies have been conducted to identify and analyze stigmatizing language used by HCPs during documentation in patients’ medical records.5,9,10 In a qualitative study evaluating the written language used by physicians in ambulatory internal medicine, both negative and positive statements were documented in patients’ medical records.5 Some examples of the positive language identified were complementary language when describing the patient and minimizing blame. Conversely, negative language contained stereotyping terms, implying disbelief about patients’ reports/symptoms or questioning credibility.5 Similarly, >5% of clinical notes in obstetrics included terms classified as stigmatizing through questioning credibility, conveying disapproval, or stereotyping patients.9 In another recently published study;10 Out of 48,651 hospital admission notes, 1197 contained stigmatizing language most frequently about diabetes (599, 6.9%), substance use disorder (209, 3.4%), and pain (37, 0.7%).10
Nonetheless, although preliminary work on language as part of documenting care exists,11 important gaps remain. Studies were often limited to specific medical conditions (eg, diabetes12,13 or opioid use disorder14) documentation settings/timepoints (eg, admission or discharge notes9,10,15), or disciplines (eg, physicians,5,16 nurses,16 or pharmacists17), rather than examining language within general mental health services or across multiple disciplines and care settings (inpatient, outpatient, and community). This may limit insight into how language varies across settings and disciplines.
Akin to global contexts, evidence on the use of stigmatizing language in clinical documentation within Middle eastern and Arab healthcare settings remains limited, with stigmatizing language examined in the context of media portrayal.18,19 In the region, literature supports the presence and negative impact of stigma on patients with mental health conditions and the initiatives to combat it.20–27 In Qatar, for example, the Qatar National Mental Health Strategy (2013–2018), and the Qatar National Mental Health & Wellbeing Strategic Framework (2019–2022) are part of ongoing efforts to enhance mental health care.27,28 Given that approximately 1 in 5 individuals in Qatar experience mental health conditions29–31 and that documentation language may influence provider attitude and patient experience, examining positive and negative language in clinical documentation not only addresses local needs and practice but also contributes to the global understanding of language use in mental healthcare documentation.
To address these gaps, this study aimed to identify and describe the patterns of language used by different mental HCPs when documenting in their patients’ Electronic Health Records (EHR) across inpatient, outpatient, and community mental health services. The secondary objectives of this project included assessing the: 1) extent of use of positive and negative language subtypes among HCPs working in mental health, 2) relationship between mental health HCPs (documenters) and stigmatizing or positive language when documenting care, and 3) relationship between patient sociodemographic characteristics and stigmatizing or positive language.5
Methods
Study Design and Setting
This was a retrospective EHR chart review undertaken at Mental Health Services (MHS) at Hamad Medical Corporation (HMC), which is the main provider of secondary/tertiary healthcare in Qatar.
Qatar’s national healthcare system is predominantly financed by the government and serves both citizens and expatriates. The system is administered by the Primary Health Care Corporation (PHCC) and Hamad Medical Corporation (HMC), alongside private healthcare options, offering comprehensive services frequently free or subsidized. Established in 1979, HMC oversees over 14 facilities, and stands as Qatar’s principal healthcare provider for >2 million residents. The Mental Health Services (MHS) division of HMC, is the sole public provider of mental health services in the country. It offers a full care continuum across inpatient, outpatient, community, and virtual settings. MHS uses Cerner®.32 This electronic medical record system allows for the use of sensitive notes where access to notes is only limited to MHS staff across HMC.
Within the corporation, documentation practices may vary by service or discipline, but rely on Cerner Electronic Health Record [Cerner EHR] through Oracle Health.32 This system allows healthcare providers to access patients’ health records, communicate with other providers, and deliver/document healthcare clinical operations in an automated matter. In MHS, specifically, most of the documentation is done through rich-text/free-text notes with integrated forms. Although Arabic is the official language in the State of Qatar, English is widely spoken and is the language used in communications within governmental health care (including documentation in electronic medical records, regardless of the language of consultation or interaction with the patient).
Sampling Procedure
Patient lists for those admitted to inpatient settings, attendees of outpatient clinics, and individuals who received home visits from the community team between October and December 2021 were sourced from the health information medical records departments. This three-month data collection period was selected to align with typical follow-up intervals in outpatient and community settings in the service, which average approximately three months. It also allowed for covering multiple inpatient admissions (average length of stay: 28 days) and several resident rotations (28-day blocks).
Subsequently, 300 unique patient records were randomly selected for review using a computer algorithm. This number was selected based on study objectives and previous literature to balance exploring meaningful patterns language use, adequate representation from multiple settings, and feasibility of coding and review by multiple researchers. From each of these 300 health record files, one random clinical note entry was chosen. The files were stratified to ensure the selection of 100 records from each of the three service settings: 1) inpatient care, 2) outpatient clinic appointments, and 3) community team home visits. Eligible notes could have been documented at any stage of the treatment process, including admission, follow-up, and discharge, and by any healthcare provider (eg, doctor/psychiatrist, pharmacist, nurse, psychologist, occupational therapist, physiotherapist, dietitian, social worker, case manager and students from all disciplines).
Data Collection
From the patient’s records, the following data were collected: patient demographics (eg, age, gender, ethnicity, mental health diagnosis), characteristics of the HCP documenting care, and the type of encounter (inpatient, outpatient clinic or home care visit) All text within the selected chart notes was retrieved and entered into a Microsoft Excel® spreadsheet along with patient, HCP/documenter, and encounter information.
Coding Framework
A pre-defined coding framework of positive and negative language and subtypes (see Appendix 1) was developed to characterize the linguistic content of the encounter notes, derived from a comprehensive literature review of previous literature and organizational guidelines.5,33–39 Definitions and further information about each subtype are detailed in Appendix 1. For negative language, the subtypes were Disability Language/Disorder-first Language, Disapproval/Questioning Credibility, Stereotyping, in addition to Inappropriate treatment and medication-related Language. Conversely, for positive language, the subtypes were Person-first Language/Non-disabling Language, Personalized Language, Minimizing blame, and Bilateral decision making. For example, a free-text notes may include a statement with negative language such as “a schizophrenic patient” which would be coded as disorder-first language, as opposed to “a patient with schizophrenia” (coded as patient-first language). Using this framework, encounter notes were classified as “positive” (potentially conducive of recovery), “negative” (potentially stigmatizing), or both. The classification was based on the presence of at least one instance of positive/negative language as per the guide (Positive yes/no, Negative yes/no). Notes were allowed to be labelled as both positive and negative simultaneously.
To ensure the methodological rigour of coding, independent double-coding and iterative consensus were used. A training session for all research members was conducted to ensure coding framework understanding. Then, three researchers worked independently classifying the encounter notes, which were then reviewed against the coding framework by another three researchers for triangulation. The six research team members met regularly to discuss all coding and resolve any coding discrepancies.
Data Analysis
Both qualitative and quantitative content analysis were used in this study. However, to maintain a clear distinction between linguistic choices on an individual level and predefined phrases used in departmental templates, phrases from standardized checklists/templates (both positive or negative) were excluded from the final quantitative and statistical analyses.
Qualitative Analysis
Deductive analysis was used to classify the extracted codes into subtypes of positive and negative language as per the coding framework. While free-text notes reflect documenters’ use of language, standardized templates may contain pre-set phrases that could unintentionally convey negative language (eg, smoker, compliant with her medications, dietary compliance). All coded statements from both free-text notes and standard forms were included in the qualitative analysis to capture all categories of positive or negative language present in the EHRs. Quotes were extracted from each category to illustrate the different types and subtypes of language.
Quantitative Analysis
Descriptive statistics (frequency and percentages) were used to report demographics and encounter characteristics. Then, using the categorized positive and negative statements, the number of notes in all subtypes/categories was quantified and tabulated against the sociodemographic characteristics of HCPs, patients, and settings where Pearson’s chi2 (goodness-of-fit chi2) and Fisher’s exact test were used as appropriate. Cramer’s V was calculated as a post-hoc test. Cohen’s omega was also used, and the effects were as follows: Small if w=0.10, medium if w=0.30, and large if w=0.50. Quantitative analyses were performed using STATA® statistical software version 17 for Windows and Microsoft Excel.
Results
Demographics and Clinical Characteristics
A total of 300 encounter notes were analyzed both quantitatively and qualitatively. As displayed in Table 1, those notes were written by HCPs from eight different professions, with physicians and nurses having written 111 (37%) and 69 (23%), respectively. More than half of the notes (157, 52%) were written for patients following with adult psychiatry, and similarly in relation to patients identifying as Arabs (202, 67%). Most patients spoke Arabic (163, 54%) or English (117, 39%). Patients were mostly male (179, 59%), ages 26–35 years old (101, 34%), and diagnosed with schizophrenia/schizoaffective disorder (88, 29.33%), bipolar affective disorder (52, 17%), or major depressive disorder (44, 15%).
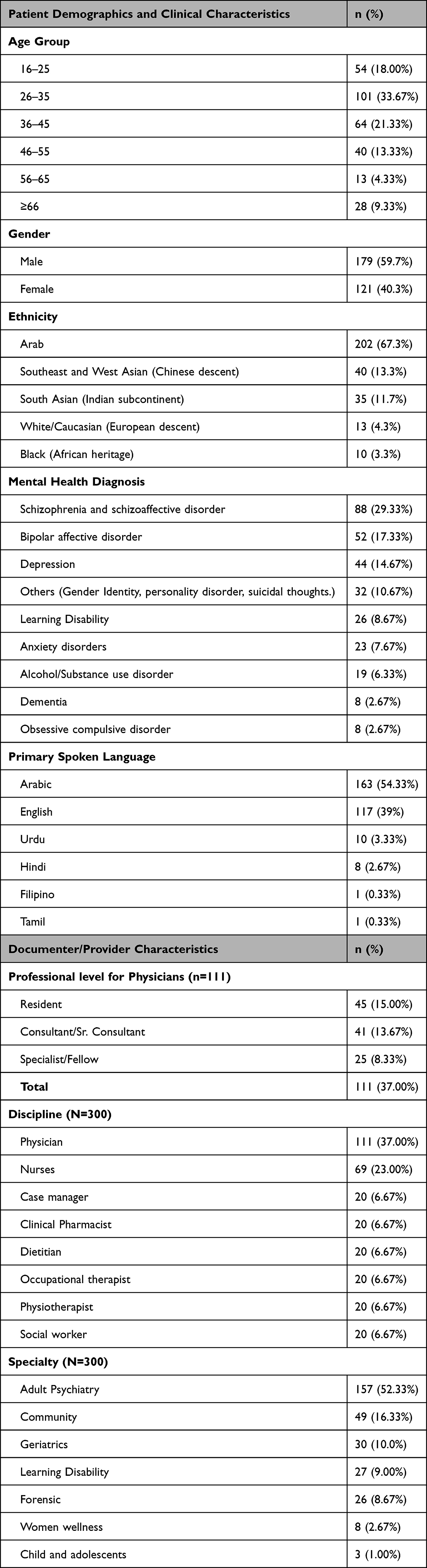 |
Table 1 Patient and Provider Characteristics (N=300) |
Use of Negative and Positive Language
Upon analysis of the 300 encounters, positive and negative language belonging to all the pre-defined subtypes were extracted. Qualitatively, free-notes (HCP-authored) and structured sections (filled templates/checklists) in documentations from all disciplines revealed examples from both language types. Structured lists or templates included patterns such as the use of “smoker” or “obese” (negative, disease-first language), “diet compliance” (negative, inappropriate treatment-related language), or “Patient understands and agrees to plan” (positive language conveying bilateral decision-making). Table 2 presents a selection of the extracted quotes.
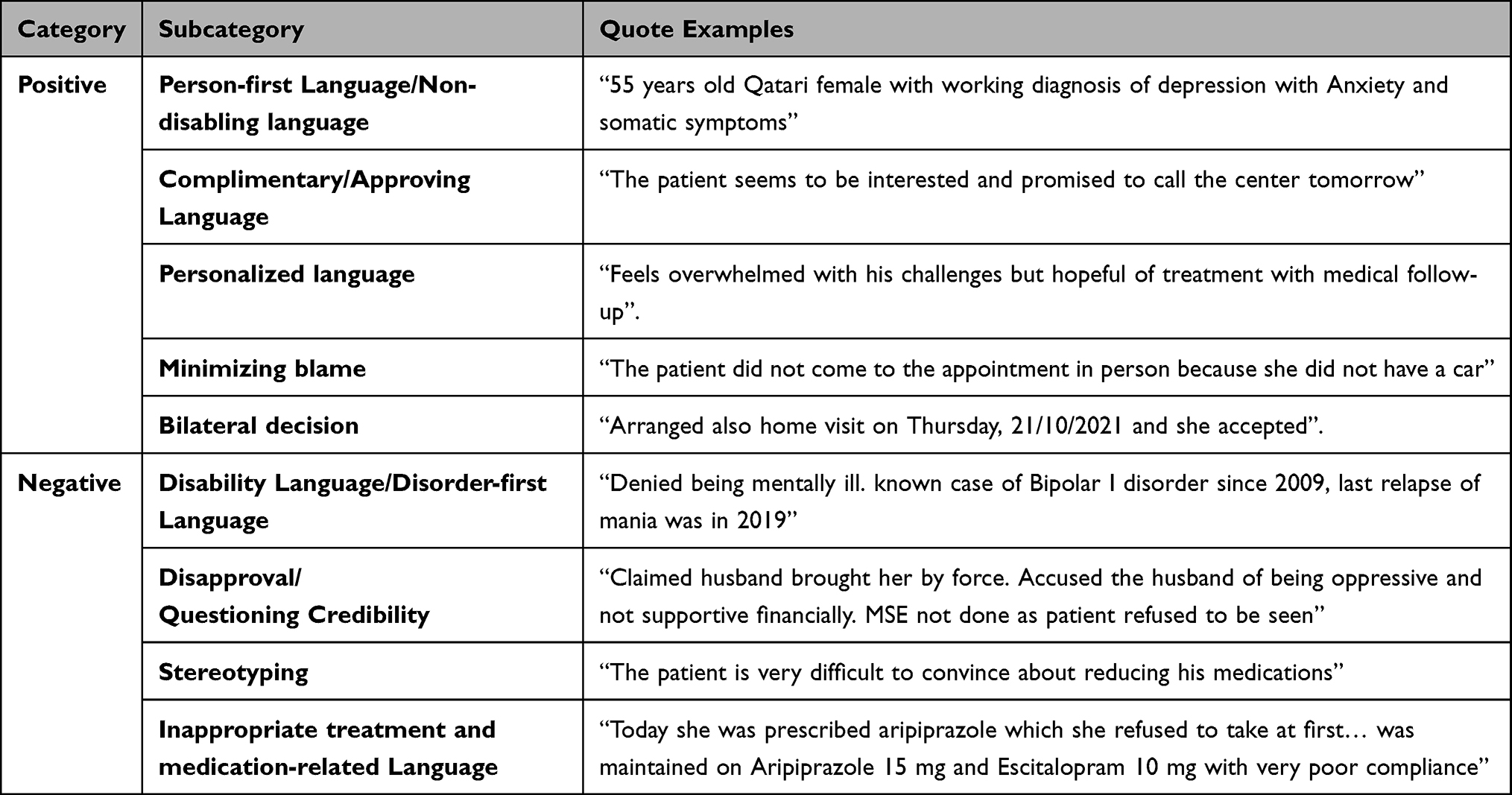 |
Table 2 Quote Examples of the Positive and Negative Language and Subtypes Extracted from the Clinical Notes |
On the other hand, findings from quantitative content analysis uncovered 201 notes (67%) incorporating positive language. Notes with negative language were closely numbered, as 188 notes (63%) had examples of stigmatizing language. Notes with either language types were further categorized into priori subtypes. Table 3 illustrates these subtypes along with the counts and percentages of notes using them.
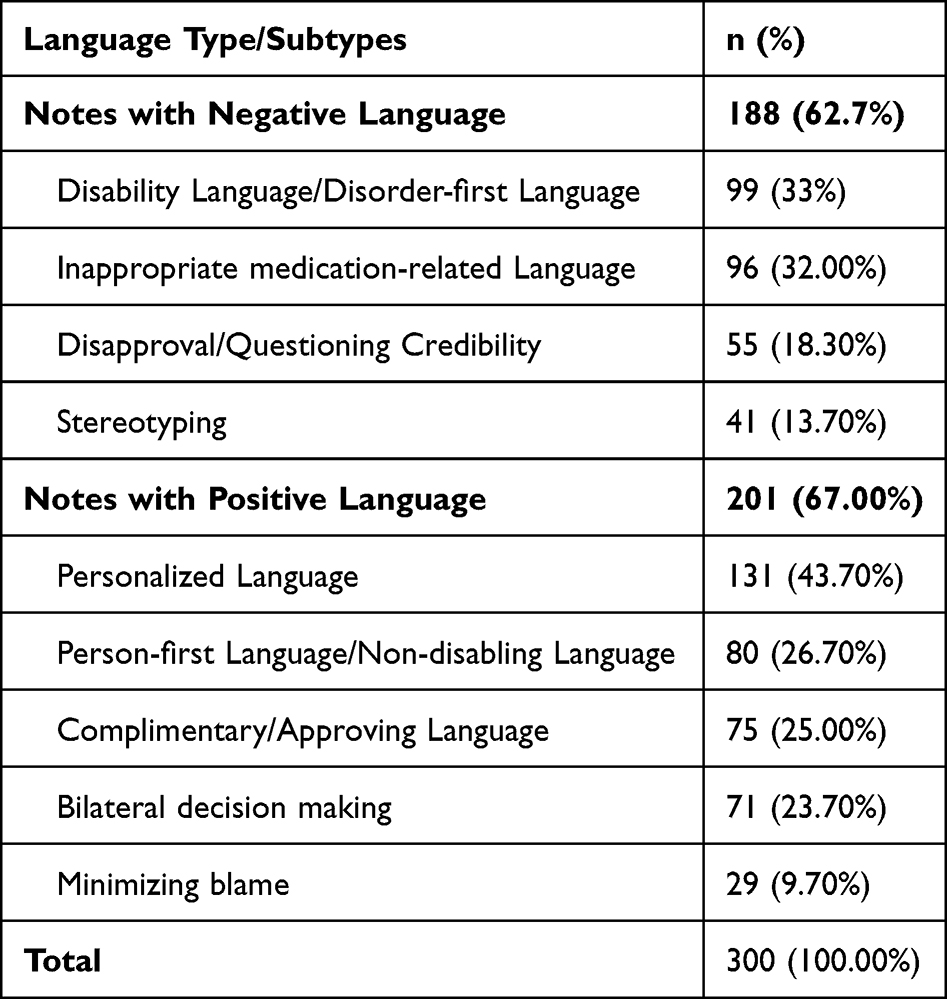 |
Table 3 Use of Negative and Positive Language |
Language Used in Context of Specific Notes’ Characteristics
Several documenter and patient characteristics were associated in a statistically significant manner with language types. Psychiatry specialty, documenter discipline, encounter setting, age group, diagnosis, and patient’s main language of communication, were all found to be associated with the use of positive language. On the other hand, discipline, care setting, and physician level (in notes written by physicians specifically) were associated with the use of stigmatizing language. Table 4 summarizes the calculated p-values and Cramér’s V for all the variables.
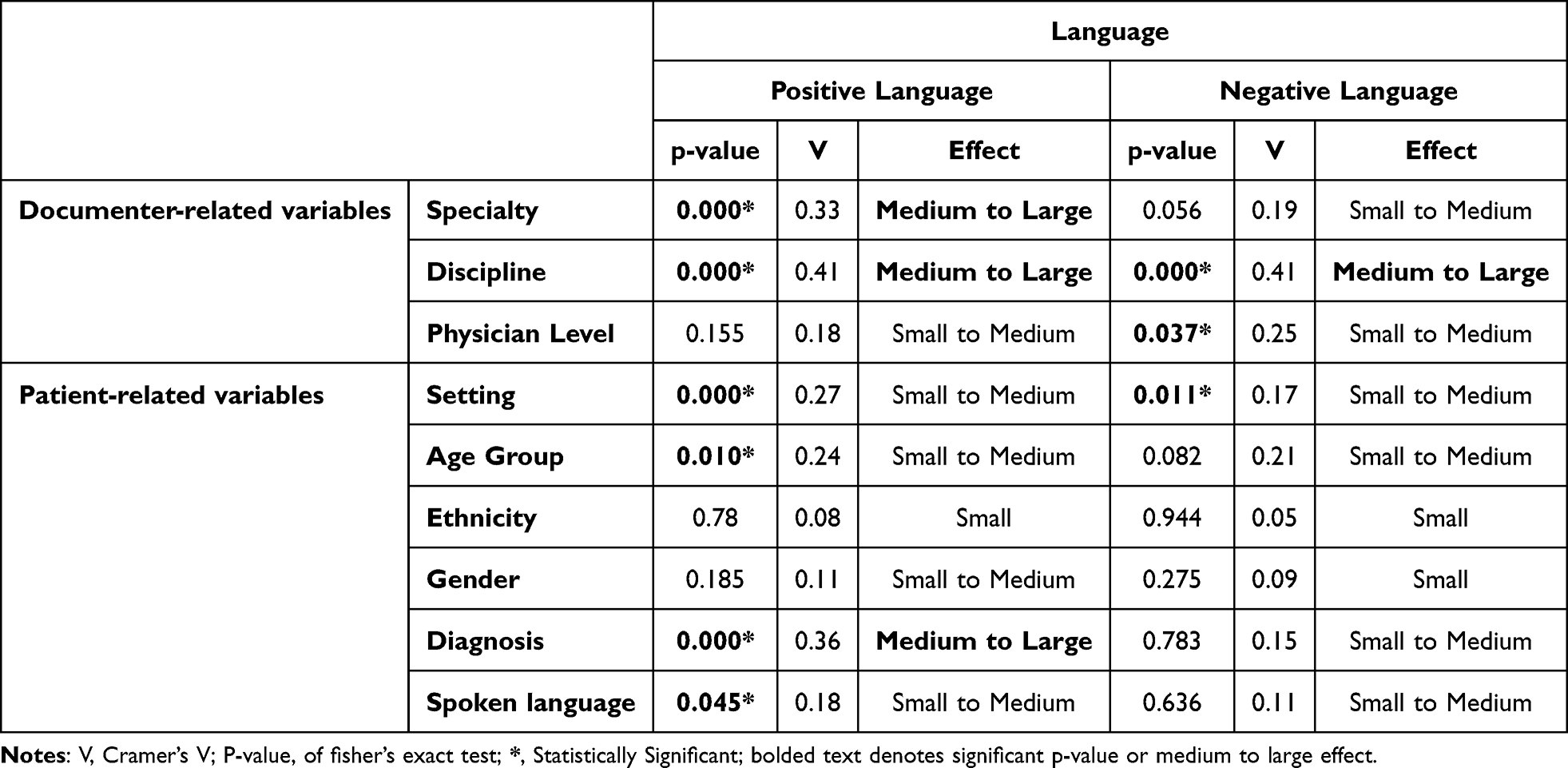 |
Table 4 Inferential Analysis of the Use of Language in Context of the Different Variables |
Further analysis of the presence of positive and negative language across the presented documenter and patient attributes is presented below. Table 5 provides a structured, visual representation of how the patterns of positive and negative language manifest in the distinct categories within the different attributes. These patterns are presented with the overall percentage of positive and negative language (67% and 62.7% in 300 notes, respectively) as reference. For instance, as seen in Table 5, 26/30 (87%) of notes written by the geriatrics team had positive language, a high percentage of positive language compared to the overall percentage of the 300 notes. On the other hand, notes written by members in the child and adolescent psychiatry had 2/3 (67%) include positive language (close to the overall percentage), while those written by adult psychiatry team members had a lower-than-overall percentage of positive language with 95/157 (61.21%).
 |
Table 5 Inferential Analysis of the Use of Language in Context of the Different Statistically or Non-Statistically Significant Variables |
Discussion
This study investigates positive (recovery-oriented) and negative (stigmatizing) language in EHRs in the setting of mental health services in Qatar. To the best of our knowledge, it represents the first study in this part of the world, and in mental health settings.
The results of this study revealed that HCPs in the mental health setting utilize a similar extent of positive and negative language when documenting patient care. Although this was a promising finding, the extent of negative language is still significantly higher than what other similar studies have reported (62.7% in our study vs. 3–20% in other studies).9,10,40–42 Such differences can be partly explained by the many determinants in each setting, sample, and methodology of assessment. For instance, most available literature investigates stigmatizing language only from the perspective of physicians and nurses, and in specific settings or types of notes (eg, neonatal/birth notes and admission/discharge, respectively). Since the present study focused on the setting of mental health, a setting that requires a multidisciplinary approach in its nature, several professions and note types were encountered. Hence, it can be expected that further differences would be observed in language patterns used in records due to this diversity. In any case, the presence of negative language in close to 70% of the notes regardless of past literature calls for attention to the causes and solutions to such prevalence.
Another interesting finding is that documenter profession and setting (outpatient, inpatient, or community) were the variables statistically associated with the use of both negative and positive language. Scarce literature exists comparing the use of language in notes among different professions. However, this can theoretically be attributed to inherent differences in documentation practices between professions due to training and work culture. When analyzing notes linguistically through a graph matching algorithm, Boyd et al suggested that physicians and nurses document records differently not only in terms of concepts but also terminology.43 Moreover, although the practice of documentation ideally starts during college education, documentation can be affected by practice and training in service. It is highly possible that many HCPs would mimic the language used by their supervisors and colleagues in their work setting, consequently picking up stigmatizing language, or even copy/pasting previously written notes with negative language embedded in them.44,45 Ultimately, due to the multidisciplinary nature of mental healthcare, professionals’ roles do not exist in isolation. Notes from one profession may influence others both through picking up on their writing practices and shaping team perspectives and decisions. Importantly, the associations identified in this study are exploratory in nature and should be interpreted as indicative of potential patterns rather than definitive differences.
On a similar note, qualitative analysis revealed templates and/or checklists using negative language within notes from several professions. As such templates are often obligatory from the respective departments as part of documentation and do not represent the individuals but rather the department, negative/positive language detected in them was not included in the final quantitative analysis. Additionally, in the present setting of health services in Qatar, HCPs are consulted when creating electronic forms or checklists, but they are primarily written and designed by the medical records section. Research supports that although literature on structured forms and data entry proposes the inclusion of HCPs as advisory sources when creating these forms,46,47 this involvement is primarily through advising for clinical content, process integration, and user experience, rather than appropriates of language.
When looking at positive language, several variables affected its use. For example, data in this study suggest that notes written by providers in more specialized areas included more positive language. The percentage of positive language in notes written by HCPs from the geriatrics, women wellness, and community teams was higher than the overall percentage. This might have also contributed to notes about patients of older ages, including more use of positive language. Of note, although the language spoken by the patient showed statistical significance in association with positive notes, the p-value was barely significant (p-value=0.045), which was supported by the small-to-medium effect (Cramer’s V = 0.1833). Additionally, as notes about patients speaking a language other than Arabic or English did not exceed 20, it was difficult to draw meaningful conclusions. Further research is needed to explore the relationship between the use of positive/negative language and the language spoken by patients, especially in cases where language barriers may be present.
Interestingly, while six variables in total were statistically associated with the use of positive language in notes, only three were associated with negative language. This might suggest that the use of positive language may be more deliberate and hence associated with more documenter- or patient-related factors. On the other hand, the use of stigmatizing language was observed in a wide range of negative expressions and descriptors with few variables affecting its use. This suggests that many HCPs may unknowingly include negative language in their documentation regardless of patient characteristics. One potential factor leading to that could be variations in HCPs’ English language fluency. A person’s language proficiency may inadvertently contribute to selecting bias-perpetuating terms, serving as an example of implicit bias—a more subtle form of stigmatizing practice that has been demonstrated to negatively impact the level of patient care.40,48 However, it is essential to highlight that the extent to which language proficiency influences the use of stigmatizing language remains uncertain, and further investigation is needed to establish such a connection.
Lastly, it is crucial to acknowledge the complex and ever-changing nature of language. The meaning and connotations of language, and stigmatizing language by extension, can be influenced by several factors including time, place, and culture. Additionally, phrases or words may shift from positive to negative and vice versa.49 Such is the case with terminology like “addiction” and “hysteria”, which evolved from clinical terminologies to stigmatizing language, and were replaced by more neutral or accurate terms.50,51 More recently, guidelines on language surrounding weight and obesity in the clinical setting started calling for person-first language and replacement of charged adjectives like “morbid/extreme” obesity with neutral severity stages “I, II, and III”.52 Conversely, the use of person-first language with autism for instance has become controversial.53–56 Identity-first language (eg, autistic individual, neurodivergent) has gained endorsement from several members of the community as autism is regarded as an integral part of one’s identity and encouraged to be treated with positivity and pride53 This, of course, still varies by community. In the Arab and Middle eastern communities, autism-related identity-first language is still highly stigmatized.19 Further studies are needed to investigate the intricacy of how cultural differences might affect the use of language in documentation.
Strength and Limitations
This study is not without limitations. For example, during analysis in context of characteristics, some subgroups had few notes. This might have been due to the short collection period or large number of characteristics. Nonetheless, although small numbers of notes might not have meaningful statistical significance, they could still have clinical significance and provide a baseline for possible future research. Additionally, as studies with large samples usually use computer science and language models, this study has the advantage of human analysis, providing opportunity for detecting stigmatizing and positive language through context rather than individual terms, keywords, or expressions. Additionally, as the collection of data was during the COVID-19 pandemic, this may have impacted generalizability due to potential disruptions in care delivery. Nevertheless, this period witnessed significant adaptations in mental health service delivery in Qatar. In response to the necessity for physical distancing, telepsychiatry was implemented through telephone/videoconferencing to ensure the continuity of outpatient psychiatric care, demonstrating a reduction in no-show rates.57 Consequently, rather than diminishing the study’s generalizability, the inclusion of data from this period represents an evolving model of care that may hold increasing relevance in both current and future psychiatric practice in Qatar and similar contexts. Lastly, existing literature and guidelines used for the guide were primarily designed by healthcare providers rather than patients. Patient and Public Involvement (PPI) could have offered valuable insight into additional types and/or examples of stigmatizing/positive language. Nonetheless, evidence on patient reactions to reading their medical records indeed supports several stigmatizing language categories identified in this study’s guide, including disease-first, credibility questioning or disapproval, and stereotyping language.58 Importantly, since the reviewed medical charts are primarily read by healthcare providers, the category guide appropriately fulfils the present study’s objectives.
In fact, many of this study’s strengths lie in its methodology. To achieve the study objectives, a meticulously created guide was used for data extraction and coding. Moreover, the research team used piloting, extensive training, guide edits, and regular meetings to ensure objectivity and consistency throughout the data collection and analysis process. Unlike most previous literature, which focused only on physicians and sometimes nurses, this study included notes from eight different professions in addition to students. It also analyzed different types of notes, rather than focusing on admission or discharge notes alone. To our knowledge, this is the first study to comprehensively investigate the patterns of both positive and negative language in the mental health setting and from a multidisciplinary lens. It is also the first to explore the relationship between language appropriateness and various documenter and patient characteristics.
Implications
All in all, findings from this research highlight the intricate nature of language patterns in EHR, and the vitality of needed efforts on an individual, organizational, and societal level. Healthcare providers should seek awareness about stigmatizing language, recovery-oriented language, and their different subtypes. Providers should be educated not only to constantly self-assess their own documentation but also raise awareness when noticing negative patterns in their colleagues’. Training to recognize and use appropriate language should also be integrated in curriculums as part of university education and residency programs. Of course, it is difficult to promote the use of appropriate language within records in isolation of society. In fact, stigmatizing language is also prevalent in scientific evidence, guidelines, mainstream media, and day-to-day conversations. This paper, hence, calls for policymakers in healthcare and society alike to provide guidance on negative and positive language overall.
Future Research
This research contributes to the body of literature related to stigma and stigmatizing language in the mental health setting and provides a baseline for a multitude of research opportunities. Future research can build and expand on this paper to evaluate language appropriateness in other settings, countries, or patient groups. Additionally, surveys or focus groups can be done with providers or patients to further explore individual characteristics affecting language appropriateness or appropriateness of language from other point of views. Engaging the public through Patient and Public Involvement (PPI) can present an essential opportunity to develop guidelines comprehensively reflecting perspectives of both healthcare providers and patients on the topic.
Conclusion
This project investigated the language patterns used in the medical health records within the multidisciplinary mental health services in Qatar. Despite the high prevalence of positive language used by HCPs in the sample, the similarly predominant stigmatizing language use stresses on the vital need for radical changes in education, policies, and societal awareness. Further research exploring patient and provider characteristics in relation to language appropriateness is vital to create a future with recovery-oriented, stigma-free mental health electronic health records.
Generative AI and AI-Assisted Technologies
During the preparation of this manuscript, the authors used artificial intelligence tools to assist with reviewing grammar and language of certain sections. The authors carefully revised and evaluated the content as necessary following this and assume complete responsibility for the published work.
Abbreviations
EHR, Electronic Health Records; HCP, Healthcare Provider; HMC, Hamad Medical Corporation; IRB, Institutional Review Board; MHS, Mental Health Services; NSS, Non-statistically Significant; PHCC, Primary Health Care Corporation; PPI, Patient and Public Involvement; V, Cramer’s V.
Data Sharing Statement
Study data are available upon request from the corresponding author.
Ethical Approval and Informed Consent
The study received ethical approval from HMC Institutional Review Board (IRB) (MRC-01-22-107). The study was conducted in accordance with the Helsinki Declaration. As this study did not include human participants with lived experiences but rather followed a retrospective design, informed consent was waived. The study was carried out following strict confidentiality measures in the data collection and extraction process, whereby only de-identified data was analyzed and reported.
Acknowledgments
In loving memory of Prof. Monica Zolezzi, whose guidance and dedication greatly influenced the foundation and progress of this work. Open Access funding provided by the Qatar National Library.
Author Contributions
This work represents Prof. Monica Zolezzi original concept and leadership.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research or authorship of this article. The article processing charges (APCs) were covered by the Qatar National Library (QNL).
Disclosure
The author(s) declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Rössler W. The stigma of mental disorders. EMBO Rep. 2016;17(9):1250–15. doi:10.15252/EMBR.201643041
2. Volkow ND, Gordon JA, Koob GF. Choosing appropriate language to reduce the stigma around mental illness and substance use disorders. Neuropsychopharmacology. 2021;46(13):2230. doi:10.1038/S41386-021-01069-4
3. Cayton H. The alienating language of health care. J R Soc Med. 2006;99(10):484. doi:10.1177/014107680609901002
4. Cox C, Fritz Z. Presenting complaint: use of language that disempowers patients. BMJ. 2022;377:e066720. doi:10.1136/BMJ-2021-066720
5. Park J, Saha S, Chee B, Taylor J, Beach MC. Physician use of stigmatizing language in patient medical records. JAMA Network Open. 2021;4(7):e2117052–e2117052. doi:10.1001/JAMANETWORKOPEN.2021.17052
6. Glassberg J, Tanabe P, Richardson L, Debaun M. Among emergency physicians, use of the term “Sickler” is associated with negative attitudes toward people with sickle cell disease. Am J Hematol. 2013;88(6):532–533. doi:10.1002/AJH.23441
7. Kelly JF, Westerhoff CM. Does it matter how we refer to individuals with substance-related conditions? A randomized study of two commonly used terms. Int J Drug Policy. 2010;21(3):202–207. doi:10.1016/J.DRUGPO.2009.10.010
8. Donnelly WJ. The language of medical case histories. Ann Intern Med. 1997;127(11):1045. doi:10.7326/0003-4819-127-11-199712010-00035
9. Barcelona V, Scharp D, Idnay BR, et al. A qualitative analysis of stigmatizing language in birth admission clinical notes. Nurs Inq. 2023;30(3):e12557. doi:10.1111/NIN.12557
10. Himmelstein G, Bates D, Zhou L. Examination of stigmatizing language in the electronic health record. JAMA Network Open. 2022;5(1):e2144967–e2144967. doi:10.1001/JAMANETWORKOPEN.2021.44967
11. Barcelona V, Scharp D, Idnay BR, Moen H, Cato K, Topaz M. Identifying stigmatizing language in clinical documentation: a scoping review of emerging literature. PLoS One. 2024;19(6):e0303653. doi:10.1371/journal.pone.0303653
12. Dickinson JK, Guzman SJ, Maryniuk MD, et al. The use of language in diabetes care and education. Diabetes Care. 2017;40(12):1790–1799. doi:10.2337/DCI17-0041
13. Beverly EA, Hughes AS, Saunders A. Examination of health care providers’ use of language in diabetes care: a secondary qualitative data analysis. Clin Diabetes. 2022;40(4):434. doi:10.2337/CD21-0108
14. Hirshman R, Hamilton S, Walker M, et al. Stigmatizing and affirming provider language in medical records on hospitalized patients with opioid use disorder. J Hosp Med. 2024;20(1):26–32. doi:10.1002/jhm.13472
15. Vick JB, Kelly M, McArthur A, Huang S, Beach MC. “He said he could take his own advice:” Stigmatizing language in notes documenting discharges against medical advice. J Hosp Med. 2025;21(3):273–283. doi:10.1002/jhm.70148
16. Apakama DU, Nguyen KAN, Hyppolite D, et al. Identifying bias at scale in clinical notes using large language models. Mayo Clin Proc. 2025;3(4):100296. doi:10.1016/j.mcpdig.2025.100296
17. Moore EL, Kuhn AK, Leung JG, Myhre LJ. Striving for health equity: stigmatizing language in inpatient pharmacy notes – a pilot study. Res Social Administrative Pharm. 2024;20(5):553–556. doi:10.1016/j.sapharm.2024.02.003
18. Alyousef SM, Alhamidi SA, Albloushi M, Eid TA. Perceptions of media’s contribution toward stigmatization of mental health by saudi arabian nurses. J Am Psychiatr Nurses Assoc. 2020;26(6):568–575. doi:10.1177/1078390319855771
19. Zolezzi M, Habib S, Saadia H, Elamin S. Portrayal of autism spectrum disorder and its treatments in Qatar’s leading newspapers: a content analysis study. Ment Health Prev. 2024;34(3):200327. doi:10.1016/j.mhp.2024.200327
20. Alshawwa Y, Caldwell-Harris C. A systematic review of mental health in the Arab Region. J Cross Cult Psychol. 2026. doi:10.1177/00220221251406572
21. Sharif L, Babhair R, Alzahrani D, et al. Unraveling the stigma: a qualitative descriptive exploration of the relationship between culture, religion, and mental disorders in Saudi Arabia. BMC Psychology. 2025;13(1):425. doi:10.1186/s40359-025-02733-w
22. Partovi Tabar P, Lloyd-Evans B, Low J, Scior K, Wood L. Stigma and health a systematic review and narrative synthesis of the stigma of psychosis in Middle Eastern populations. Stigma Health. 2025.doi:10.1037/sah0000616
23. Andrade G, Bedewy D, Elamin ABA, Abdelmonem KYA, Teir HJ, Alqaderi N. Attitudes towards mental health problems in a sample of United Arab Emirates’ residents. Middle East Curr Psy. 2022;29(1):88. doi:10.1186/s43045-022-00255-4
24. Stirling B, Hickey J, Omar H, Kehyayan V. Stigma towards mental disorders in Qatar: a qualitative study. QScience Connect. 2019;2019(1):2. doi:10.5339/connect.2019.2
25. Alageel S, Alsadhan NM, Alkhaldi G, AlKasabi R, Alomair N. Factors influencing decisions to seek mental healthcare in the Arab Gulf states: a qualitative thematic analysis. BMC Public Health. 2025;25(1):1438. doi:10.1186/s12889-025-21607-9
26. Sobhani M, Saeidi P, Naeim M, et al. Improving mental health infrastructure across the Middle East. Asian J Psychiatr. 2024;93:103908. doi:10.1016/j.ajp.2023.103908
27. Khaled SM, Al-Abdulla M, Tulley I, Al-Thani SM, Woodruff PW. Qatar’s national mental health study—the world mental health Qatar. Int J Methods Psychiatr Res. 2024;33(S1):e2008. doi:10.1002/mpr.2008
28. Summary national mental health & wellbeing strategic framework 2019–2022. Available from: https://andp.unescwa.org/sites/default/files/2020-10/National%20Mental%20Health%20Framework%202019_2022.pdf.
29. Ghuloum S, Bener A, Deafia E, Alyazidi T, Elamir Zakaria A, Elamin Mustafa A. Lifetime prevalence of common mental disorders in Qatar: using who composite international diagnostic interview (WHO-CIDI). International Journal of Clinical Psychiatry and Mental Health. 2014;2(1):HBOP0878. doi:10.5339/qfarc.2014.hbop0878
30. Bener A, Zirie M, Janahi IM, Al-Hamaq AOAA, Musallam M, Wareham NJ. Prevalence of diagnosed and undiagnosed diabetes mellitus and its risk factors in a population-based study of Qatar. Diabet Res Clin Pract. 2009;84(1):99–106. doi:10.1016/j.diabres.2009.02.003
31. Bener A, Abou-Saleh MT, Dafeeah EE, Bhugra D. The prevalence and burden of psychiatric disorders in primary health care visits in Qatar: too little time? J Family Med Prim Care. 2015;4(1):89. doi:10.4103/2249-4863.152262
32. Oracle health EHR | oracle health. Available from: https://www.oracle.com/health/clinical-suite/electronic-health-record/.
33. Person-first and destigmatizing language | National Institutes of Health (NIH). 2023. Available from: https://www.nih.gov/nih-style-guide/person-first-destigmatizing-language.
34. Raney J, Pal R, Lee T, et al. Words matter: an antibias workshop for health care professionals to reduce stigmatizing language. MedEdPORTAL. 2021;17:11115. doi:10.15766/MEP_2374-8265.11115
35. American Association of Psychiatric Pharmacists. Communication style guide. 2018.
36. Granello DH, Gibbs TA. The power of language and labels: “the mentally ill” versus “people with mental illnesses. J Couns Dev. 2016;94(1):31–40. doi:10.1002/JCAD.12059
37. Martinelli TF, Meerkerk GJ, Nagelhout GE, et al. Language and stigmatization of individuals with mental health problems or substance addiction in the Netherlands: an experimental vignette study. Health Soc Care Community. 2020;28(5):1504–1513. doi:10.1111/hsc.12973
38. Recovery oriented language guide - WORDS MATTER. 2022.
39. Jensen ME, Pease EA, Lambert K, et al. Championing person-first language: a call to psychiatric mental health nurses. J Am Psychiatr Nurses Assoc. 2013;19(3):146–151. doi:10.1177/1078390313489729
40. Sun M, Oliwa T, Peek ME, Tung EL. Negative patient descriptors: documenting racial bias in the electronic health record. Health Aff. 2022;41(2):203–211. doi:10.1377/HLTHAFF.2021.01423
41. Liu Y, Wang W, Gao GG, Agarwal R. Echoes of biases: how stigmatizing language affects AI performance. 2023. Available from: https://arxiv.org/abs/2305.10201v4.
42. Weiner SG, Lo YC, Carroll AD, et al. The incidence and disparities in use of stigmatizing language in clinical notes for patients with substance use disorder. J Addict Med. 2023;17(4):424–430. doi:10.1097/ADM.0000000000001145
43. Boyd AD, Dunn lopez K, Lugaresi C, et al. Physician nurse care: a new use of UMLS to measure professional contribution: are we talking about the same patient a new graph matching algorithm? Int J Med Inform. 2018;113:63–71. doi:10.1016/J.IJMEDINF.2018.02.002
44. Gagliardi JP, Turner DA. The electronic health record and education: rethinking optimization. J Grad Med Educ. 2016;8(3):325. doi:10.4300/JGME-D-15-00275.1
45. Tsou AY, Lehmann CU, Michel J, Solomon R, Possanza L, Gandhi T. Safe practices for copy and paste in the EHR: systematic review, recommendations, and novel model for health IT collaboration. Appl Clin Inform. 2017;8(1):12. doi:10.4338/ACI-2016-09-R-0150
46. Bush RA, Kuelbs C, Ryu J, Jiang W, Chiang G. Structured data entry in the electronic medical record: perspectives of pediatric specialty physicians and surgeons. J Med Syst. 2017;41(5):75. doi:10.1007/S10916-017-0716-5
47. Van Batavia JP, Weiss DA, Long CJ, et al. Using structured data entry systems in the electronic medical record to collect clinical data for quality and research: can we efficiently serve multiple needs for complex patients with spina bifida? J Pediatr Rehabil Med. 2018;11(4):303–309. doi:10.3233/PRM-170525
48. Merino Y, Adams L, Hall WJ. Implicit bias and mental health professionals: priorities and directions for research. Psychiatr Serv. 2018;69(6):723–725. doi:10.1176/APPI.PS.201700294
49. Altakhaineh ARM. The semantic change of positive vs. negative adjectives in modern english. Lingua Posnaniensis. 2018;60(2):25–38. doi:10.2478/LINPO-2018-00010
50. Alinsky RH, Hadland SE, Quigley J, et al. Recommended terminology for substance use disorders in the care of children, adolescents, young adults, and families. Pediatrics. 2022;149(6):e2022057529. doi:10.1542/PEDS.2022-057529
51. Shetty S, Chandini S, Fernandes S, Safeekh A. Hysteria: a historical perspective. Arch Med Health Sci. 2020;8(2):312. doi:10.4103/AMHS.AMHS_220_20
52. Bannuru RR, ElSayed NA, Aroda VR, et al. Weight stigma and bias: standards of care in overweight and obesity—2025. BMJ Open Diabetes Res Care. 2025;13(Suppl 1). doi:10.1136/BMJDRC-2025-004962
53. Botha M, Hanlon J, Williams GL. Does language matter? Identity-first versus person-first language use in autism research: a response to Vivanti. J Autism Dev Disord. 2023;53(2):870–878. doi:10.1007/S10803-020-04858-W/METRICS
54. Buijsman R, Begeer S, Scheeren AM. ‘Autistic person’ or ‘person with autism’? Person-first language preference in Dutch adults with autism and parents. Autism. 2023;27(3):788–795. doi:10.1177/13623613221117914
55. Dwyer P. Stigma, incommensurability, or both? Pathology-first, person-first, and identity-first language and the challenges of discourse in divided autism communities. J Dev Behav Pediatr. 2022;43(2):111–113. doi:10.1097/DBP.0000000000001054
56. Taboas A, Doepke K, Zimmerman C. Preferences for identity-first versus person-first language in a US sample of autism stakeholders. Autism. 2023;27(2):565–570. doi:10.1177/13623613221130845
57. Wadoo O, Khan F, Latoo J, et al. Telepsychiatry implementation in Qatar: a three-year analysis of no-show rates and its impact on mental health service delivery. Qatar Med J. 2024;2024(4):50. doi:10.5339/QMJ.2024.50
58. Fernández L, Fossa A, Dong Z, et al. Words matter: what do patients find judgmental or offensive in outpatient notes? J Gen Intern Med. 2021;36(9):2571. doi:10.1007/S11606-020-06432-7
 © 2026 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2026 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.