Back to Journals » International Journal of General Medicine » Volume 17
Willingness to Pay for Telemedicine Services Among Uninsured Individuals in Saudi Arabia: A Cross-Sectional Survey
Authors Almalki ZS ![]() , Alrashdi AM
, Alrashdi AM ![]() , AlHuzaimi DE
, AlHuzaimi DE ![]() , Alotaibi JO, Alqahtani MM, Alzahrani RD, Alajmi SA, AlOsaimi RR, Majrashi SM, Alahmari AK, Alshehri AM
, Alotaibi JO, Alqahtani MM, Alzahrani RD, Alajmi SA, AlOsaimi RR, Majrashi SM, Alahmari AK, Alshehri AM ![]() , Alzarea AI
, Alzarea AI ![]() , Imam MT, Alshlowi AA
, Imam MT, Alshlowi AA
Received 9 April 2024
Accepted for publication 29 August 2024
Published 6 September 2024 Volume 2024:17 Pages 3879—3891
DOI https://doi.org/10.2147/IJGM.S472926
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Satish Nair
Ziyad S Almalki,1 Abdullah M Alrashdi,1 Dalal E AlHuzaimi,2 Joud O Alotaibi,2 Malek M Alqahtani,1 Ruba D Alzahrani,2 Shahad A Alajmi,2 Rami R AlOsaimi,2 Salman M Majrashi,1 Abdullah K Alahmari,1 Ahmed M Alshehri,1 Abdulaziz I Alzarea,3 Mohammad Tarique Imam,1 Areej A Alshlowi2
1Department of Clinical Pharmacy, College of Pharmacy, Prince Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia; 2College of Pharmacy, Almaarefa University, Riyadh, Saudi Arabia; 3Department of Clinical Pharmacy, College of Pharmacy, Jouf University, Sakaka, Aljouf, Saudi Arabia
Correspondence: Ziyad S Almalki, Department of Clinical Pharmacy, College of Pharmacy, Prince Sattam Bin Abdulaziz University, Al-Kharj, Saudi Arabia, Tel +966 11 588 6059, Email [email protected]
Purpose: This study aimed to explore the Willingness To Pay (WTP) of uninsured individuals in Saudi Arabia and the factors influencing their decisions regarding telemedicine services.
Patients and Methods: This study used a cross-sectional survey design and convenience sampling to gather data from respondents aged 18 years or older who had visited healthcare facilities at least once in the past year and were uninsured. WTP was determined using the contingent valuation method, and a two-part regression model was applied to analyze the factors influencing WTP.
Results: The study included 4232 participants and discovered that approximately 17.41% were willing to pay for telemedicine services. Those aged 60 and older, employed in the government or private sector, in higher socioeconomic quintiles, and experiencing chronic health issues showed a positive association with their WTP value. Conversely, individuals aged between 30 and 44 years, married, and unemployed exhibited a negative association with a lower WTP value.
Conclusion: The findings indicate that most respondents hesitated to pay for telemedicine services, with a significant influence from sociodemographic characteristics, underscoring the need to promote telemedicine use among underserved populations and address health disparities.
Keywords: healthcare, sociodemographic, questionnaire, contingent valuation method
Introduction
Telemedicine has gained significant importance in recent years due to its capacity to offer healthcare services remotely through telecommunications technology.1 In Saudi Arabia, the Vision 2030 initiative strives to provide affordable and high-quality healthcare to all citizens, with telemedicine playing a critical role in accomplishing this goal.2 The integration of telemedicine services offers several advantages, including easing the strain on hospitals and clinics. By decreasing overcrowding and waiting times for immediate care, telemedicine allows for more efficient healthcare delivery, enhanced patient satisfaction, and improved overall health outcomes.3
The healthcare system in Saudi Arabia operates through a dual system encompassing both public and private sectors. The government provides free access to healthcare services for all Saudi citizens through a network of public hospitals and clinics. In addition to the public sector, a robust private healthcare sector caters to those seeking private insurance or willing to pay out-of-pocket for specialized or expedited care.4 Within the healthcare system in Saudi Arabia, telemedicine services are available in both public and private facilities.5 However, the level of telemedicine services offered can vary significantly between the two. Public facilities may offer limited telemedicine services for certain conditions or consultations, such as general medical advice and follow-up appointments.6 By contrast, private healthcare facilities provide a broader range of telemedicine services, including virtual consultations with specialized professionals across different fields, remote monitoring of patients outside hospital settings, and online access to comprehensive medical records for efficient patient management, which often requiring out-of-pocket payments or private insurance.7
In Saudi Arabia, nearly 37.5% of the population has private health insurance, and insurance plans increasingly cover telemedicine services.8,9 However, many people, particularly those who are uninsured, still struggle to access these services due to the cost.10 Lack of insurance support worsens healthcare disparities and puts individuals who cannot afford private healthcare at a further disadvantage. This results in an unjust situation in which the financial status or lack of insurance becomes a barrier to essential medical care access.11
In this context, Willingness to Pay (WTP) is a useful metric for evaluating the financial preferences of uninsured individuals regarding telemedicine services. It employs economic techniques to determine the maximum price that an individual is willing to spend on a specific telemedicine service, providing valuable insights into affordability and incentivizing the utilization of these services. Therefore, this study aims to fill this research gap by comprehensively assessing the WTP and its factors in the context of Saudi Arabia. These insights can guide healthcare providers and policymakers in developing programs and policies that ensure affordable access to telemedicine services, with a specific focus on reducing disparities in healthcare access while ensuring universal access, regardless of insurance coverage.
Materials and Methods
Study Design and Population
An anonymous cross-sectional survey design was used to determine Saudi citizens’ WTP for telemedicine services. The survey was made accessible through various channels, including WhatsApp, other social media platforms, and Email in the Google document format. Data collection took place over six months, from September 2023 to March 2024. Participants were recruited using a convenience sampling method. Eligible individuals were at least 18 years old, resided in Saudi Arabia, had at least one in-person visit to a healthcare facility in Saudi Arabia within the past year, and were uninsured. Uninsured individuals was defined as those without any form of third-party health insurance coverage, including both public and private insurance schemes, at the time of the study.
This study followed the ethical guidelines outlined in the Declaration of Helsinki and was approved by the Institutional Review Board of the MOH (IRB Log Number 22–490). Before providing consent, participants were informed about the study’s objectives, data usage, anonymization to protect privacy, survey duration, and data retention period. Our study design assumed that participants had a general understanding of the costs associated with comparable in-person healthcare services. Data collection was performed without personally identifiable information to ensure anonymity and confidentiality.
Data Collection
Data were gathered using a structured, self-administered questionnaire, drawing upon items from a published study exploring factors affecting WTP, and implemented in several previous studies. The questionnaire, consisting of four parts: respondent characteristics, clinical profile, healthcare utilization, and WTP, was designed for completion in five minutes. Originally in English, the survey was translated into Arabic by a bilingual translator using a comprehensive back-translation protocol. To ensure data quality, we focused on respondents familiar with both telemedicine and internet use. Potential participants were asked two screening questions: “Are you familiar with the concept of telemedicine?” and “Have you used the internet in the past three months?” Only individuals who answered “yes” to both questions were eligible to participate in the study.
Variables and Measurements
Dependent Variable
WTP was defined as the maximum value that patients were willing to pay for telemedicine services. The WTP value is determined using the contingent valuation method. The questions were divided into two parts to determine WTP values. The first question was,’ Considering all the effects and benefits of telemedicine services, will you be willing to pay for telemedicine services? (No; Yes)”. The second question asked, “If yes, the first question, how much will you be willing to pay per visit for telemedicine services?”. Only respondents who were willing to pay for telemedicine answered the second question. Respondents stated their WTP in Saudi Riyal, which was later converted to US dollars using an exchange rate of 1 USD = 3.75 SAR. Saudi Arabian policy defines telemedicine as the use of information technology and electronic communication for various healthcare services. This includes diagnosis, examination, medical assessments, and facilitating communication between healthcare practitioners and with their patients.12 Our study focuses on online consultations and examinations by medical specialists, aligning with the MOH’s objective of leveraging telemedicine to improve healthcare access and quality. For the purpose of this study, the scope of the consultation service was defined to include potential additional services such as basic assessments or follow-up scheduling. However, medication costs were explicitly excluded from this definition.
Independent Variables
Previous research investigating WTP for telemedicine services guided our inclusion of various independent variables, including gender, age (18–29, 30–44, 45–59), marital status (unmarried or married), educational attainment (high school or less, higher education), employment status (self-employed, the government employed, privately employed, unemployed), and geographic location (urban or rural). To evaluate the socioeconomic status (SES) of each respondent, the questionnaire sought information regarding the presence of household assets, including the type of housing and ownership of items such as automobiles, televisions, Internet access, satellite devices, and video games. SES was subsequently categorized into quartiles based on the information obtained.
The third section aimed to collect data on clinical characteristics such as chronic conditions and perceived general health. To identify the presence of chronic conditions, respondents were asked, “Have you ever been diagnosed by a healthcare professional with any chronic conditions?”. The participants’ general health was assessed using the question, “How would you rank your overall health?” Responses included 1 = very good, 2 = good, 3 = fair, 4 = poor, and 5 = very poor. The final part gathered information on the number of healthcare visits during the past year, and the type of healthcare facilities visited.
Questionnaire Validation
Pre-tests and pilot tests were conducted to assess the accuracy of the questionnaire. The first draft of the questionnaire was given to ten knowledgeable individuals for face-to-face interviews, resulting in feedback used to create a second draft. This second draft was reviewed by five experts, who ensured its clarity and simplicity. A pilot test with 30 participants from the target population with relevant online healthcare experience was then conducted to gather feedback on unclear sections and suggestions for improvements, leading to further refinement of the questionnaire.
Statistical Analysis
A formal analysis was conducted to assess the distribution and attributes of respondents’ WTP for telemedicine. The chi-square test was used to determine the correlation between the independent variables and WTP. A two-part regression model was used to examine the factors affecting WTP. The initial part of the model used logistic regression to evaluate the probability of having a positive WTP. The subsequent part employed a general linear model that used the same explanatory variables with a gamma distribution and log link function to determine the anticipated individual WTP levels, given their positively skewed nature. All analyses were performed using SAS Studio version 9.4 (SAS Institute Inc., Cary, NC, USA). Results were considered statistically significant if the p-value was less than 0.05.
Results
Four thousand two hundred thirty-two individuals participated in this study. There was no incomplete data, as all questions were compulsory. As shown in Table 1, the sample comprised 52.24% male participants, predominantly within the age brackets of 18–29 and 30–44. Of the participants, 50.24% were married, and 67.16% had completed higher education. Most participants had either a governmental or a private sector job (38.8% and 38.11%, respectively). Almost all participants (96%) resided in urban areas, and the majority (52.65%) belonged to the fourth quintile of the SES category. Approximately 65.05% of the patients had no chronic conditions. Most participants rated their health status as “Very good” or “good” (39.3% and 39.2%, respectively), and 40.97% had four or more healthcare visits in the last 12 months. Finally, 56.5% of the participants received treatment in public facilities. Approximately 17.41% of the participants expressed a WTP for telemedicine, as shown by the findings.
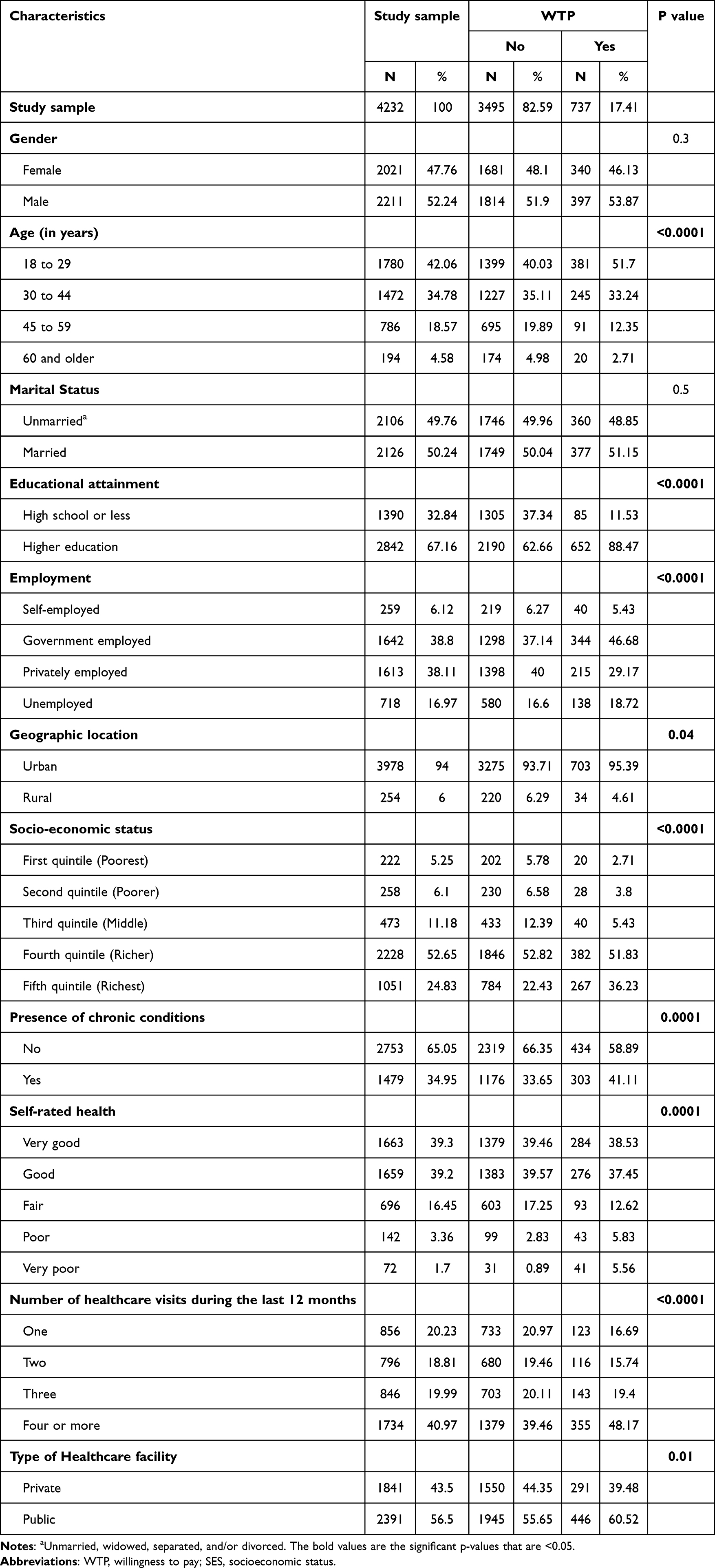 |
Table 1 Sample Characteristics Stratified by Their WTP |
Table 2 provides essential information on the mean WTP and its 95% confidence interval. For respondents willing to pay for telemedicine services, the average value was $107.74 per visit (95% CI: 95.38–120.09). We also observed significant differences across the socioeconomic characteristics of the respondents regarding the value they were willing to pay for telemedicine services. Gender disparity is evident in the mean WTP, with male respondents exhibiting a higher mean WTP value of $116.90 (95% CI: 98.72–135.07), in comparison to their female counterparts who displayed a mean WTP value of $97.05 (95% CI: 80.69–113.41). The mean WTP for telemedicine services appeared to increase with age, and married respondents demonstrated a higher WTP. Furthermore, the findings reveal a significant increase in the mean WTP from the unemployed to the self-employed categories. In addition, a positive correlation exists between the SES of the respondents and their WTP. The average WTP for the first quintile of SES is $26.40 (95% CI: 0.67–53.47), which gradually increases to $118.18 (95% CI: 105.03–131.33) for the fifth quintile. Finally, the study indicates that the mean WTP for respondents with chronic conditions is higher, with a value of $132.86 (95% CI: 109.59–156.13), compared to respondents without chronic conditions who had a mean WTP value of $90.20 (95% CI: 77.09–103.31).
 |
Table 2 The Average Value of WTP for Each Telemedicine Service per Visit |
Table 3 presents the results of a statistical analysis using a two-part model to examine the relationship between WTP and respondents’ sociodemographic characteristics. The first part of the logistic regression model showed that factors such as age, marital status, education, employment, geographic location, SES, chronic conditions, general health perception, healthcare visits in the last 12 months, and type of healthcare facility were statistically significant predictors of a positive WTP (P < 0.05). Specifically: older age and unemployment were linked to lower odds of reporting positive WTP (P < 0.05), while being married; having higher education; residing in rural areas; falling within third to fifth quintiles of SES; experiencing chronic conditions or rating health as “poor” or “very poor”; having four or more healthcare visits in the preceding year; and receiving treatment at a public health facility were associated with higher odds of positive WTP (P < 0.05).
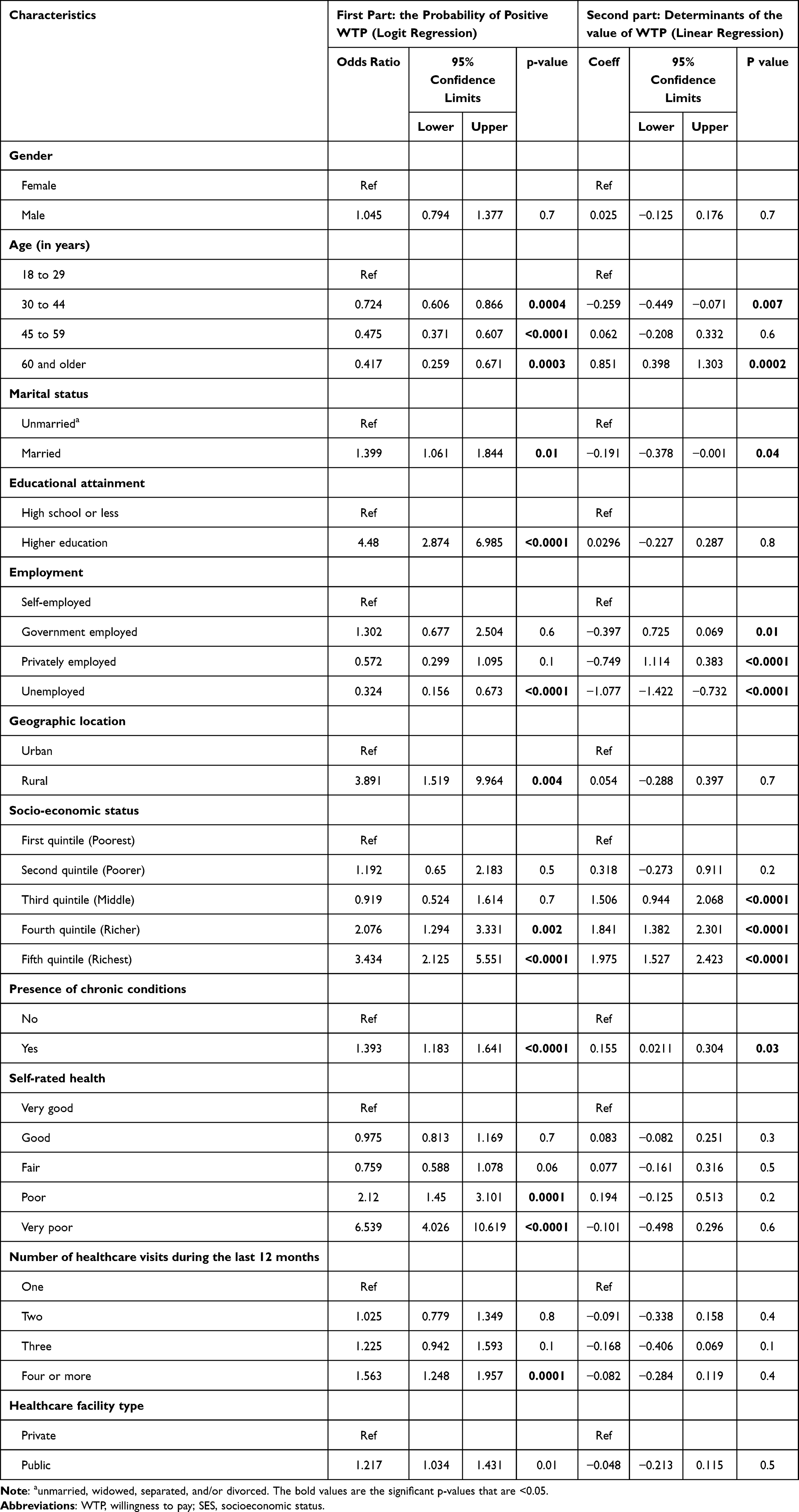 |
Table 3 Two-Part Model Estimates Showing the Factors Affecting WTP |
In the second part of the analysis, we employed a GLM with a log link and discovered that elderly individuals, aged 60 and above, employed in the government or private sector, belonging to the third, fourth, and fifth quintiles of SES, and experiencing chronic health issues displayed a positive association with their WTP value for telemedicine services (P < 0.05). In contrast, those aged between 30 and 44 years, married, and unemployed exhibited a negative association with a lower WTP value (P < 0.05).
Discussion
This study aimed to explore the willingness of uninsured individuals in Saudi Arabia to pay for telemedicine services and the factors influencing their decision-making process. A large sample size was used for this study to reveal that only a small percentage of respondents were willing to pay for such services. This finding is significant given the increasing popularity of telemedicine due to its convenience and accessibility. The findings of this study are consistent with those of previous studies,13,14 but lower than those of other studies.15,16
The mean value that respondents were willing to pay for telemedicine services was higher than the average WTP reported in previous studies,17 indicating a high value placed on these services by patients. Furthermore, WTP values varied significantly based on participant characteristics, highlighting the importance of considering patient characteristics when setting prices for telemedicine services to ensure accessibility for all patients at affordable prices.
In addition, this study adds to the existing knowledge on telemedicine in Saudi Arabia by identifying various factors that affect WTP for telemedicine services. The results indicated that WTP was influenced by age, marital status, educational level, employment status, location, SES, presence of chronic conditions, perceived general health, number of healthcare visits in the last 12 months, and type of healthcare facility.
The findings revealed a significant negative correlation between age and WTP for telemedicine. This aligns with previous research indicating that older adults are less likely to embrace technology-based interventions than younger individuals.17 Older patients may resist new technologies and prefer traditional personal interactions with healthcare providers rather than distance-based services such as telemedicine.18
Marriage was found to be associated with a higher likelihood of being willing to pay for telemedicine services and a lower WTP value. These findings are consistent with previous research.13 The reasons for this difference in WTP, based on marital status, remain unclear. It is possible that married individuals have better access to traditional healthcare services, such as in-person doctor visits, which could make them less likely to recognize the value of telemedicine.19
The present study revealed important information about the relationship between educational level and WTP for telemedicine services. Specifically, individuals with higher education levels are more likely to pay for telemedicine services than those with lower education levels. This finding is supported by a comprehensive Systematic Review and Meta-analysis study.20 One possible explanation for this trend is that well-educated individuals are generally more informed and better understand the benefits of telemedicine.3
Our research indicated a positive correlation between individuals’ employment status and their WTP for telemedicine services. We found that unemployed patients are less likely to be willing to pay, but when they do, they are willing to pay less than employed individuals. This aligns with a previous study in Malaysia,21 suggesting that employed patients are generally more inclined to invest greater value in telemedicine services than unemployed patients.
For the variable geographic location, our findings indicate a statistically significant positive correlation between rural areas and WTP for telemedicine intervention. This observation aligns with that of a previous study.22 WTP for telemedicine services in rural areas may be explained by the convenience afforded by remote consultations conducted in individuals’ homes.
The finding from this study found that WTP is dependent on SES is in line with the study that economic status is a factor that affects WTP.15 Regarding the WTP value, the fourth and fifth quintiles of SES association with their WTP value for telemedicine services imply that people experiencing poverty may not be able to pay for telemedicine and may need a government subsidy to be able to benefit from such services.
It is crucial to consider the complex interplay between employment, income, insurance coverage, and WTP for telemedicine. While our study found a general trend of higher WTP among employed individuals. This aligns with prior research that has explored relationship between socioeconomic factors and WTP in the context of telemedicine.15 The research emphasizes that socioeconomic factors, including employment status, income level, and insurance coverage, can significantly influence an individual’s WTP for telemedicine.
Necessity is communicated in several ways. Our study revealed that individuals with chronic conditions and lower self-rated health were more likely to show an inclination toward paying for telemedicine services. This indicates that chronic conditions and poor health have a significant impact on individuals’ willingness to invest in this level of convenience and accessibility in managing their health. This finding is consistent with previous research that demonstrated a positive correlation between chronic conditions and the perceived value of telemedicine services.23 These results indicate that telemedicine services may provide a valuable solution for patients who face difficulties in attending medical appointments because of their health conditions.
Additionally, patients who lack confidence in their health may be more inclined to seek convenient healthcare options such as telemedicine. Furthermore, patients who had more healthcare visits in the past 12 months demonstrated a stronger inclination to pay for telemedicine services. Notably, frequent healthcare visits often suggest the presence of chronic conditions, as patients with ongoing illnesses typically require regular check-ups and consultations.
It is important to consider that a high proportion of participants (78.5%) rated their health as “good” or “very good”, which might raise questions about their actual need for teleconsultations and the potential for biased WTP responses. However, it’s crucial to recognize that healthcare utilization encompasses a wide range of services, including preventive care, chronic disease management, and minor ailments. The fact that 41% of participants made four or more healthcare visits in the preceding year could indicate a pattern of proactive health-seeking behavior or the management of ongoing health conditions, even among those who perceive their overall health favorably. This suggests that WTP for telemedicine might be driven not solely by acute healthcare needs but also by factors such as convenience, accessibility, and preferences for managing certain aspects of healthcare remotely. Further research could explore the motivations behind healthcare utilization patterns among individuals reporting good health status to better understand their potential receptivity to telemedicine services.
In contrast, patients who regularly visit public healthcare facilities show a greater propensity to pay for telemedicine services. This is primarily because of the convenience it offers, such as not having to travel to the medical facility, avoiding long wait times, and the ability to schedule appointments more quickly.24 Additionally, patients who have difficulty traveling or have mobility issues find telemedicine a more accessible and convenient healthcare option. As a result, telemedicine has proven to be a viable and cost-effective solution for many patients who require healthcare services.
The study results have important implications for improving the accessibility and affordability of telemedicine services. Two promising strategies are to make telemedicine more accessible to people on a tight budget and to ensure that everyone has the opportunity to receive essential healthcare services. One effective strategy is to set affordable prices using sliding-scale discounts based on the patient’s ability to pay. Another approach is to offer multi-tiered packages tailored to the needs of disadvantaged populations, ensuring that everyone can access telemedicine, regardless of their financial situation. Additionally, the government could subsidize telemedicine costs through targeted programs for the uninsured or underinsured populations. This could involve allocating funds to private healthcare facilities that offer high-quality telemedicine services or partnering with telemedicine providers to offer discounted rates to disadvantaged populations without health insurance coverage.
Future researchers should conduct qualitative research to explore the reasons behind the hesitancy to pay for telemedicine. This research could involve interviews or focus groups with individuals of older age, lower education levels, residing in urban areas, and having lower SES. Understanding these perceptions will help design effective strategies to increase uptake. Additionally, it is essential to design studies that consider WTP for affordable packages, matching consumers’ ability to ensure that cost is not a barrier for those in need.
This study has certain limitations that should be considered. First, it is important to note that the study may have been affected by sampling bias. This means that certain groups of the population may not actively participate in social networks, which may have affected the results of the study. Second, it is worth noting that a service can be overvalued before it has to be paid for. This can occur either because the good is unknown, such as telemedicine, or because there is a belief that telemedicine services will not have to be paid for.16,25 Third, our study did not investigate the potential impact of specific diseases on the sample population’s WTP for telemedicine services. Future research would benefit from examining this aspect to gain a deeper understanding of how various medical conditions may influence patients’ perceptions of the value of telemedicine. Fourth, our study assumed participants’ familiarity with in-person healthcare costs, which could have influenced their WTP for telemedicine. Future research could address this by providing participants with standardized cost information or comparing WTP across groups with varying levels of cost awareness. Fifth, notably, while the questionnaire provided participants with a description of telemedicine services, it did not explicitly compare the cost of telemedicine to in-person care or no care at all. This lack of cost comparison could have influenced participants’ WTP responses, potentially leading to an overestimation or underestimation of their actual WTP when presented with real-world cost differentials. Future research should incorporate cost comparisons to provide a more nuanced understanding of WTP for telemedicine services within the context of existing healthcare alternatives. Sixth, it is important to acknowledge that the WTP values elicited in this study represent only one piece of the complex cost equation surrounding healthcare delivery. A comprehensive analysis would require accounting for the full range of expenses associated with traditional, in-person consultations. This includes not only direct medical costs but also indirect costs such as transportation, time spent traveling and waiting, and potential lost wages for both patients and accompanying individuals. Unfortunately, we were unable to locate published data on these specific costs within the Saudi Arabian context. Seventh, it is important to note that our study focused specifically on uninsured individuals, and the findings may not be directly generalizable to the insured population. While there is a growing trend of insurance plans covering telemedicine services, the extent of coverage and reimbursement policies can vary widely. Some plans may offer full reimbursement for teleconsultations, while others might have co-pays, deductibles, or restrictions on eligible services or providers. Moreover, this specific population is likely to exhibit differences compared to the overall Saudi population. They may be less inclined to actively pursue healthcare services and have lower incomes, which may prevent them from being able to purchase private insurance. The distinct characteristics of our study restrict the generalization of our results to a wider population. Finally, while our study establishes a benchmark for WTP for telemedicine consultations, the lack of publicly available data on private healthcare pricing in Saudi Arabia limits our ability to directly compare this figure to typical face-to-face consultation fees in private clinics.
Conclusion
This study provides valuable insights into the factors influencing WTP for telemedicine services. Our findings suggest that a considerable proportion of respondents were hesitant to pay for these services, and their WTP was significantly influenced by sociodemographic characteristics. Notably, we observed variations in WTP across different population groups, raising important considerations for equitable access. While this study highlights potential areas for intervention, such as addressing cost concerns and promoting awareness among specific population groups, further research is needed to confirm these findings in larger, more diverse populations and to explore the underlying reasons behind the observed WTP patterns. Such research will be crucial for informing the development of effective policies and strategies aimed at promoting equitable access to telemedicine services.
Funding
This study is supported via funding from Prince Sattam bin Abdulaziz University project number (PSAU/2023/R/1444).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jin MX, Kim SY, Miller LJ, Behari G, Correa R. Telemedicine: current impact on the future. Cureus. 2020;12(8). doi:10.7759/CUREUS.9891
2. Alasiri AA, Mohammed V. Healthcare transformation in Saudi Arabia: an overview since the launch of vision 2030. Heal Serv Insights. 2022;15. doi:10.1177/11786329221121214
3. Haleem A, Javaid M, Singh RP, Suman R. Telemedicine for healthcare: capabilities, features, barriers, and applications. Sensors Int. 2021;2:100117. doi:10.1016/J.SINTL.2021.100117
4. Gurajala S. Healthcare system in the Kingdom of Saudi Arabia: an expat doctor’s perspective. Cureus. 2023;15(5). doi:10.7759/CUREUS.38806
5. Al MA, Saha C, Alhuqbani W, et al. Utilization of Telemedicine during COVID-19 in Saudi Arabia: a multicenter study. Cureus. 2023;15(7). doi:10.7759/CUREUS.41541
6. Alharbi A, Alzuwaed J, Qasem H. Evaluation of e-health (Seha) application: a cross-sectional study in Saudi Arabia. BMC Med Inform Decis Mak. 2021;21(1):1–9. doi:10.1186/S12911-021-01437-6/TABLES/5
7. Alshahrani H, Al-Matrafi N, Al-Qahtani N, Taliby R, Hassanein M, Al-Rowilly I. Mapping the private healthcare sector in Riyadh Region: size, services, and alignment with the Saudi ministry of health priorities. Mater Sociomed. 2023;35(3):172. doi:10.5455/MSM.2023.35.172-177
8. Healthcare Statistics. The General Authority for Statistics. Healthcare Statistics; 2023.
9. Gajarawala SN, Pelkowski JN. Telehealth benefits and barriers. J Nurse Pract. 2021;17(2):218. doi:10.1016/J.NURPRA.2020.09.013
10. Shrank WH, Deparle NA, Gottlieb S, et al. Health costs and financing: challenges and strategies for a new administration. Health Affairs. 2021;40(2):235–242. doi:10.1377/HLTHAFF.2020.01560
11. Soltani S, Takian A, Akbari Sari A, Majdzadeh R, Kamali M. Financial barriers to access to health Services for Adult People with disability in Iran: the challenges for universal health coverage. Iran J Public Health. 2019;48(3):508. doi:10.18502/ijph.v48i3.895
12. Telemedicine. Available from: https://www.moh.gov.sa/en/Ministry/Information-and-services/Pages/Telemedicine.aspx.
13. Bradford WD, Kleit AN, Krousel-Wood MA, Re RM. Willingness to pay for telemedicine assessed by the double-bounded dichotomous choice method. J Telemed Telecare. 2004;10(6):325–330. doi:10.1258/1357633042601991
14. Qureshi AA, Brandling-Bennett HA, Wittenberg E, Chen SC, Sober AJ, Kvedar JC. Willingness-to-pay stated preferences for telemedicine versus in-person visits in patients with a history of psoriasis or melanoma. Telemed J E Health. 2007;12(6):639–643. doi:10.1089/TMJ.2006.12.639
15. Arize I, Onwujekwe O. Acceptability and willingness to pay for telemedicine services in Enugu state, southeast Nigeria. Digit Heal. 2017;3:205520761771552. doi:10.1177/2055207617715524
16. Bergmo TS, Wangberg SC. Patients’ willingness to pay for electronic communication with their general practitioner. Eur J Health Econ. 2007;8(2):105–110. doi:10.1007/S10198-006-0014-5
17. Chua V, Koh JH, Koh CHG, Tyagi S. The willingness to pay for telemedicine among patients with chronic diseases: systematic review. J Med Internet Res. 2022;24(4):e33372. doi:10.2196/33372
18. Jiang Y, Sun P, Chen Z, et al. Patients’ and healthcare providers’ perceptions and experiences of telehealth use and online health information use in chronic disease management for older patients with chronic obstructive pulmonary disease: a qualitative study. BMC Geriatr. 2022;22(1). doi:10.1186/S12877-021-02702-Z
19. Kemp MT, Liesman DR, Brown CS, et al. Factors associated with increased risk of patient no-show in telehealth and traditional surgery clinics. J Am Coll Surg. 2020;231(6):695. doi:10.1016/J.JAMCOLLSURG.2020.08.760
20. Xie Z, Chen J, Or CK. Consumers’ willingness to pay for eHealth and its influencing factors: systematic review and meta-analysis. J Med Internet Res. 2022;24(9):e25959. doi:10.2196/25959
21. Mey TM, Ogasawara K. Telehealth consultation for Malaysian citizens’ willingness to pay assessed by the double-bounded dichotomous choice method. Malays J Med Sci. 2024;31(1):91. doi:10.21315/MJMS2024.31.1.8
22. Bradford WD, Kleit A, Krousel-Wood MA, Re RM. Comparing willingness to pay for telemedicine across a chronic heart failure and hypertension population. Telemed J E Health. 2005;11(4):430–438. doi:10.1089/TMJ.2005.11.430
23. Yang K, Li Y, Qi H. Determinants of and willingness to use and pay for digital health technologies among the urban elderly in Hangzhou, China. Risk Manag Healthc Policy. 2023;16:463–478. doi:10.2147/RMHP.S393767
24. Cantor J, Schuler MS, Matthews S, Kofner A, Breslau J, McBain RK. Availability of mental telehealth services in the US. JAMA Heal Forum. 2024;5(2):e235142–e235142. doi:10.1001/JAMAHEALTHFORUM.2023.5142
25. Klose T. The contingent valuation method in health care. Health Policy. 1999;47(2):97–123. doi:10.1016/S0168-8510(99)00010-X
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Development and Validation of Questionnaires to Assess Workplace Violence Risk Factors (QAWRF): A Tripartite Perspective of Worksite-Specific Determinants in Healthcare Settings
Mohd Hatta FH, Samsudin EZ, Aimran N, Ismail Z
Risk Management and Healthcare Policy 2023, 16:1229-1240
Published Date: 5 July 2023