")
Back to Journals » International Journal of Women's Health » Volume 14
Why Home Delivery After Full Antenatal Care Follow-Up in Southern Ethiopia? An Exploratory-Descriptive Qualitative Study
Authors Toja E, Abebe A , Mekonen N, Baza D
Received 6 March 2022
Accepted for publication 24 May 2022
Published 11 June 2022 Volume 2022:14 Pages 765—775
DOI https://doi.org/10.2147/IJWH.S365244
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Eshetu Toja,1 Amene Abebe,1 Niguse Mekonen,1 Daniel Baza2
1Department of Public Health, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 2Department of Nursing, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Correspondence: Amene Abebe, Email [email protected]
Background: Pregnant women who had full antenatal care follow-up are expected to give birth in health facilities. However, in Ethiopia, after full antenatal care booking, many women still prefer to give birth at home. Thus, the purpose of this study was to explore and describe why women give childbirth at home after full antenatal care follow-up in the study setting.
Methods: Exploratory-descriptive qualitative design was conducted in Humbo and Abala Abaya districts, Southern Ethiopia, from June to September 2020. Nine in-depth interviews and four focus group discussions were held with purposively selected participants. Women who gave birth at home after attending equal to or more than four antenatal care appointments in the last year were included. The collected data were majorly analyzed by inductive thematic analysis technique, but deductive analysis was also applied whenever the potential themes needed further enrichment. A thick description of the findings is done in the respective heading and sub-heading using participants’ verbatim quotations.
Results: A total of 9 in-depth interviews and four focus group discussions comprising 35 participants was conducted. Three major themes and nine sub-themes emerged from the data. Socio-cultural and community influences, socio-economic obstacles, and health system-related barriers are the major themes identified. Traditional practices, personal beliefs, social norms, knowledge, and attitude about institutional delivery, household economic capability, decision-making capacity of the women, delivery service quality, and service providers related barriers are the sub-themes defining the home delivery experience of women after full antenatal care follow-up in the study setting.
Conclusion: In this study, socio-economic, cultural, and health system-related barriers are major reasons for home delivery. Improvement of public awareness on the risk of home delivery and elimination of its facilitative social norms, empowerment of women’s economic, educational, and decision-making capability and healthcare workers’ and health facilities’ capacity are recommended.
Keywords: antenatal care, follow-up, full antenatal care, home delivery, institutional delivery
Introduction
Globally, in areas where maternal healthcare services are scarce or hardly accessible, maternal morbidity and mortality are among the top health and socio-economic problems.1 From the total maternal deaths which are occurring worldwide, two-thirds are happening during delivery or in the postnatal period immediately after childbirth.2
Evidence from around the world shows 90% of maternal deaths would have been prevented if immediate decisions and appropriate care had been provided during delivery and early postpartum period.3 Most of the maternal complications and deaths are attributable to easily preventable or manageable risk factors such as postpartum hemorrhage, postpartum sepsis, obstructed labor, and unsafe abortion.4,5
Skilled birth attendance during childbirth in a hygienic condition has a significant contribution to reducing adverse effects of childbirth.5 Contrary to the above fact, in Ethiopia, skilled birth attendance during delivery was 28% and it is 28.6% in the Southern Region where the current study was conducted.6
To promote institutional delivery service utilization, the Ethiopian government is implementing many strategies and programs. For instance, in Ethiopia, all maternal and child health-related services are provided free of any charge.7 The health extension program is another strategy that is designed to improve community health including maternal and neonatal health through home-to-home health problem identification, provision of basic healthcare services, and initiation of prompt referral system for complications.8
On contrary to this government’s ambition, from the general pregnant women, in Ethiopia, an unacceptably high proportion 73% nationally and 74% in the Southern Region give birth at their home.9,10 Home deliveries are either unattended or attended by Traditional Birth Attendants (TBAs) in an unhygienic and/or unconducive environment for delivery and newborn reception.11,12
A woman who had antenatal care (ANC) follow-up is anticipated to access health facility delivery that can smooth and reduce unfavorable maternal outcomes. Previous studies show that the magnitude of home delivery among pregnant women who had booked for ANC in the current study area ranges from 13.5% to 25.3%.13,14
These facts and figures show that either full or initiated ANC attendance has no guarantee for institutional delivery service utilization. Thus, this study aimed towards exploring why pregnant women still prefer to give birth at their home after being fully booked for ANC follow-up by analyzing the women’s explanations, understandings, how they perceive home delivery, how they interpret their home delivery experience, and their perspectives on the place of delivery.
Methods
Study Setting, Design, and Period
This study was conducted in Humbo and Abala Abaya districts, Wolaita Zone, Southern Ethiopia. According to the information obtained from the Wolaita Zone Health Department, the two study settings were purposely chosen because of the fact that the two districts had the lowest health facility deliveries relative to other districts in the Zone. Wolaita Zone is located 330 km south of Addis Ababa, the capital city of Ethiopia. According to the 2020 Central Statistical Agency of Ethiopia population projection, Wolaita Zone encompasses a total of 5,385,782 population. According to the information obtained from the Wolaita Zone administration office, the Zone constitutes about 16 rural districts and 7 town administrations. Based on Zonal Health Department information, there are about 400,844 women of childbearing age and has 11 Hospitals, 68 health centers, and 355 health posts. An exploratory-descriptive qualitative research design was conducted from June to September 2020.
Participant Recruitment Procedure
In-depth interviews and Focused Group Discussions (FGDs) were conducted with purposively selected women who gave birth at home in the last year after attending four or more ANC visits. Participants had been traced through their contact addresses from medical records of respective health centers and health posts. Health Extension Workers (HEWs) (health care providers in the health post level where delivery service is not given) working in the respective health posts guided to trace the participants. Women who gave birth in the last one year at their home and were able to inform well, knowledgeable, better articulated, reflective, and willing to talk at length with researchers were purposely selected.
Sample Size and Sampling Procedure
According to Miles and Huberman (1994), as cited in Perreault (2011), four major aspects of the purposive site and participants’ selection criteria were considered. The aspects used include where the study will take place (the natural setting of participants), who should be the participants (purposive sampling), appropriately identifying the issue to be interviewed and/or discussed, and contextual dimensions of the participants.15 Nine in-depth interview participants (IDIPs) who gave birth in the last year and 35 informants in four FGDs were selected. Humbo and Abala Abaya districts, Wolaita Zone, Southern Ethiopia were purposely selected. Maximum variation purposive sampling technique in terms of some important aspects of participants such age (aged and young), marriage type (monogamous and polygamous), and educational status (educated and uneducated) was considered during selection of IDIP. Seven to ten participants were included in each of the FGD sessions. FGD key informants included mothers group, fathers group, healthcare workers group (doctors, nurses, midwives, and health officers), and local community leaders group (health development army leaders, religious leaders, opinion leaders and non-professional health cadres). Homogeneity of the FGD participants in terms of important aspects such as age, educational status, occupation, parity, and marriage type was also considered to create comfortable group dynamics during the discussion. However, to improve the discussion of diversified ideas the familiarity of participants with each other was avoided by including participants from different residential distances, different working health facilities and asking the health extension workers on the familiarity status of the participants. The sample size required for the study was initially estimated by considering the experience of previous literature, the recommendation of qualitative research books, and the phenomena of interest. However, in In-depth Interview (IDI), both inclusion of new participants and further interview were terminated when new insights about the phenomenon being studied were stopped emerging. In FGDs, further continuation of probing and discussion was stopped when the participants repeated data which is already provided by their co-FGD discussants.16–18 HEWs were used as a community guide for tracing study participants in their residential addresses.
Data Collection Tools and Procedure
The required data were collected by the researchers. The researchers were trained, experienced, and certified in qualitative research methods. A semi-structured guide IDI with open-ended questions was used to explore rich data by participants’ language “Supplementary Materials Section 1”. To maintain the natural setting, interviews, and FGDs were conducted in a quiet place around the informants’ residential home with maximum privacy. A digital voice recorder was used to audio-tape the interviews and discussions. Probing was used to ensure the depth and clarification of the ideas during the interview and FGDs. All the interviews last on average 29 minutes and FGDs one hour to one hour and a half minutes.
Data Management and Analysis
After repeatedly listening to the audio-recorded data, audio transcripts were changed to the text transcripts in the language collected. The text transcripts were translated to the English language for analysis by the same person who is a native speaker of the local language (Wolaytattoo) and an expert in English. An inductive thematic analysis approach was followed to reach the final emerged themes and sub-themes. After converting the transcripts and field notes into a rich text file, the data were imported into Open Code Software Version 4.03.1 for coding. All the researchers have taken part in the data coding process. Reading and re-reading of the transcription and field notes were conducted to be familiarized with the data. Codes were repeatedly reviewed, and a cluster of potential themes was generated. The potential themes were critically reviewed whether they appropriately represent the codes and the data set the codes extracted. Then, those found to be too broad were split, too narrow were combined, some of them which were not sufficiently represented by the data set were discarded, and/or new themes were also created for unrepresented data set19 “Supplementary Materials Section 2”. Then, the themes that emerged are described in the respective heading and sub-heading. Besides this, the final manuscript quality was evaluated by using Consolidated Criteria for Reporting Qualitative Research (COREQ): A 32-Item Checklist for Interviews and Focus Groups were conducted.20
Trustworthiness of the Results
To maintain the rigor of the study, credibility, transferability, dependability and conformability aspects were maintained.
Credibility
Recorded audio data and field notes were kept safely and used as referencing materials. Validation of data was conducted by asking different questions, seeking different sources of data collection and using different methods. Peer-debriefing was done with a similar status colleague who is out of the context of the study. Copy of the transcribed text and distribution of preliminary findings to study participants was conducted to check for any inconsistencies if present and supplied with additional information. All the participants were responded that all themes and ideas listed in the preliminary finding were congruent with their views.
Transferability/Applicability
Purposive selection of the study area and participants was applied. A clear method and ways of participant recruitment were employed to assure utilization of the findings in other similar settings and contexts.
Dependability
In order to replicate the findings of the study from a similar respondent in a similar study setting, the texts included sections devoted to the research design and implementation, methods and approaches of data collection and reflective appraisal evaluating the effectiveness of the process was undertaken.
Confirmability
To provide readers with an accurate mental picture of the process of the research, copy of field notes and audio records are kept safely. An adequate audit trail was left for any third party to trace the sources of the research findings for confirmation.
Definition of Key Terms
Antenatal care: The care given to pregnant women to diagnose and treat diseases or complications during pregnancy.
Full antenatal care follow-up: documented ANC services of four and more than four visits.
Home delivery: childbirth which takes place in the pregnant women’s own home or other homes.
Institutional delivery: the delivery conducted at healthcare facilities and assisted by skilled healthcare workers.
Results
Socio-Demographic Profile of the Study Participants
A total of nine (9) IDIs with mothers who delivered at home after full ANC follow-up in the last year were done. Of those mothers, more than half (56%) categorized age as greater than thirty (30) years. Of the total participants, three had no formal education, while the other three were 10th grade completed. In addition to this, almost all women who participated in the study were married and Protestants in their religious affiliation (Table 1).
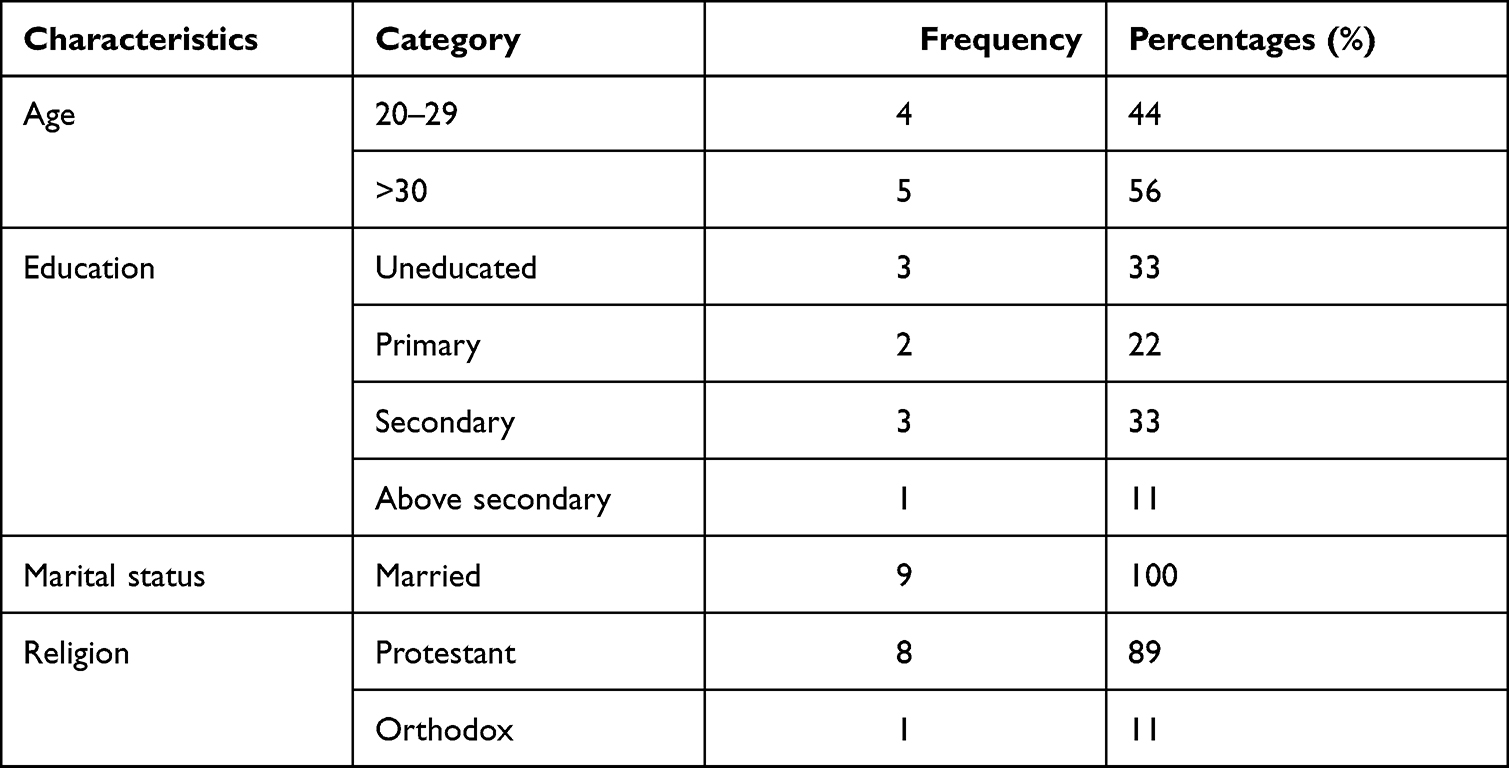 |
Table 1 Socio-Demographic Profile of in-Depth Interview Participants, Wolaita Zone, Ethiopia |
Thirty-five (35) different key informants have participated in four Focus Group Discussions (FGDs) which included mothers, fathers, healthcare providers (doctors, nurses, midwives, and health officers), and community leaders (Table 2).
 |
Table 2 Socio-Demographic Profile of FGD Participants |
The Emerged Themes and Sub-Themes from the Data
In the current study, three major themes and nine sub-themes emerged. Socio-cultural and community influences, socio-economic obstacles, and health system-related barriers are the major themes identified. Traditional practices, personal beliefs, social norms, knowledge, and attitude about institutional delivery, household economic capability, decision-making capacity of the women, delivery service quality, and service providers related barriers are the sub-themes that emerged from the data (Table 3).
 |
Table 3 Themes and Sub-Themes Emerged from the Data |
Theme One: Socio-Cultural and Community Influences
Socio-cultural and community influence is the first theme that emerged from the data which includes the sub-themes of traditional practices, personal beliefs, and social norms.
Sub-Theme One: Traditional Practices
This sub-theme is developed from the data analysis regarding who attended the birthing process. According to the study findings, TBAs and previously experienced women were among the traditional birth practitioners. Both the FGD and IDIP reported that the TBAs and the experienced women who are attending the birth at home were the reason for a break between institutional delivery service utilization and the community. A 42-year-mother of FGD discussant expressed this result as follows:
In our community, many deliveries after completing ANC follow-up are attended by TBAs and the rest by local elders, experienced women, and relatives. Because childbirth needs assistance from someone who is a trusted and well-known traditional delivery attendant in the community (TBAs) or who had previous experience in attending childbirth.
Sub-Theme Two: Personal Beliefs
As findings from this study show personal beliefs of the delivering women have a significant influence on the women’s preference of place of the delivery. The informants of the present study believe that the home is the correct place for delivery unless the pregnancy and labor are not complicated. A 35-year-old woman who participated in FGD expressed this notion as follows:
In our community; there is a continued social belief about the place of childbirth, giving childbirth in places other than the home is counted as a piece of bad luck.
The other participant from FGDs further strengthened the above result by saying:
When I was pregnant; my intimate community member advised me by saying please do not head to health institutions to give childbirth where you expose your private body to an unknown person, and that they insert their hand frequently which is not our culture.
Sub-Theme Three: The Social Norms
This study revealed that social norms such as considering giving birth at home as good luck, staying at home as the pregnancy advances to term as highly acceptable and expected behavior, and trusting in the capability of experienced women to attend the birth process were determining the home delivery experience of the women. This idea is well described by one of an IDIP as follows:
Home delivery is a common phenomenon in our community. However, currently delivering mothers head to health facilities for labor and childbirth. In our locality; giving birth at home is considered a social taboo which is still acceptable by many community members. Because of this reason, pregnant women stay at home when their pregnancy advances to term. Due to this social norm home delivery is common in our area.
Theme Two: Socio-Economic Obstacles
This theme comprises three sub-themes which are knowledge and attitude about institutional delivery, household economic capability, and decision-making capacity of the women.
Sub-Theme One: Knowledge and Attitude About Institutional Delivery
The study participants expressed that both lack of knowledge on institutional delivery and poor attitude is hindering health facility delivery service utilization. Low community awareness about institutional delivery and misunderstandings such as giving high emphasis to the ceremony of home delivery than the risk could occur in the delivery process, blaming health facility delivery setups. The above findings were explained by a 28-year-old IDIP in the following manner:
The community members do not support delivering women to go to health institutions for delivery. Whenever the delivery woman asks for support to go to institutional delivery, they say it is customary that we all gave birth at home safely with no problems and ask questions like “why you go there? What is new in your case?” Even once I asked my neighbor to accompany me to travel to the hospital during labor initiated, she refused to accompany me.
Sub-Theme Two: Household Economic Capability
According to this study household economic capability is one of the significant determinants of women’s home delivery experience. Women’s lack of money to cover the cost of transportation to health facilities and other costs pushes them to decide to give birth at their home after full ANC follow-up. This result is well described by a 30-year-old FGD discussant from husbands group as follows:
In our community, there are households with different economic statuses. Those who have better income and economic status take delivering women to health facilities for delivery service by covering all the accompanying costs. However, those who are from low economic status cannot afford to do so, in my opinion, this is one of the major causes of home delivery. The other thing which pushes women to make home delivery is the lack of important home remedies. Home remedies such as soup known as “Muk” and other locally prepared liquid and semi-liquid foods and drinks are facilitators of labor but these things are not available in the health facilities. If these things are made available in the health facilities, I think women prefer health facility delivery to the home.
Sub-Theme Three: Decision-Making Capacity of the Women
Relatives and close friends of the delivering women play a great role in the decision-making process of the place of delivery. Husbands, mothers-in-law, mothers of the women, and women who have a previous home delivery experience were among the significant others who influence women for home delivery. A 28-year-old mother expressed this finding in the following manner:
As my pregnancy advances to term, my mother-in-law said to me “please do not go other places than your home, such as hospitals for a delivery, I am here for you; because I have much experience for you to share. So there is no reason to go there, rather than exposing your body to a strange person”.
Theme Three: Health System-Related Barriers
This theme comprises three sub-themes which include quality of delivery service-related barriers, service providers-related barriers, and supply-related barriers.
Sub-Theme One: Delivery Service Quality-Related Barriers
In this study, poor quality of delivery service was among the frequently occurring issue in the data as a reason for home delivery. Participants’ experience of dissatisfaction with the quality of previous institutional delivery service affected their decision to give birth at home in the subsequent delivery. The participants of the study expressed that the health facilities are not providing delivery services fulfilling at least the minimum quality standard. Previous experience of unfriendly service provision, deliveries conducted by students with limited or absent supervision by seniors, poor infection prevention protocols, and lack of privacy during delivery were among the major dissatisfiers in the previous institutional delivery. This notion is well explained by a 34-year-old IDI mother as follows:
The delivery service in the health facilities is of poor quality. Most of the deliveries in the health facilities are attended by students. The students give priority to their learning than to the welfare of the mother and the baby. A woman whose delivery is attended by a senior gynecologist is a lucky person because it is too difficult to get them, particularly in the government health facilities. However, the senior professionals are available in the private clinics but the cost of delivery service in the private clinics is too much. Due to this fact, women who can pay will go to private clinics and get quality service while women who are unable to afford the cost are obliged to give birth at home.
Sub-Theme Two: Service Provider-Related Barriers
Knowledge, attitude, or skill gaps of the providers discouraged the delivering mothers from utilizing institutional delivery services. The providers’ early or late appointments based on miscalculated Expected Due Dates (EDD), poor counseling in ANC visits, inappropriate and inadequate examinations during ANC visits, poor and confusing recording of mothers’ data during ANC about Last Menstrual Period (LMP), and other necessary information are among the provider’s related reasons for home delivery after full ANC visits. This information is well grasped by one of the members of FGD discussant from healthcare providers:
Currently, we do not have an ultrasound in our health facility, due to this reason we cannot exactly verify the age of the fetus and tell the exact EDD. We recommend the mothers go to other advanced hospitals for the service. This is one of the major problems which discourages mothers from coming to health facilities for delivery services after full ANC follow-up. Whenever the health care workers attempt to calculate the EDD based on the LMP, the women miss the exact LMP and the health care providers miscalculate the EDD and appoint early or late for delivery services.
Congruent results are also obtained from FGDs of the mothers’ group. One of the FGD discussants described the above result in the same fashion as follows:
When we head to health centers for delivery services based on the EDDs told by HEWs; the physician who works in the health centers tells us to go back home reasoning the EDD is not yet completed. This is one of the major reasons that forced pregnant women to take a bad decision of home delivery after full ANC follow-up.
In addition to the above-mentioned findings, lack of health care workers’ readiness, long waiting times before getting the service, absence of service providers at the workplace, service delivery system complexity/bureaucracy, and giving selective service are reasons for home delivery after full ANC follow-up. This result is well described by a 34-year-old IDI mother as follows:
In the ANC visits the health extension workers and other health care workers tell us during delivery we would get in a compassionate, respectful, and friendly care approach. However, contrary to this, the health care workers discourage laboring mothers from the beginning to the end. They disturb laboring women psychologically and physically; they insult, abuse, blame the women if the labor is prolonged as an unlucky person.
Sub-Theme Three: Supply-Related Barriers
This study revealed that, contrary to the Ethiopian government’s effort to make every maternal service free of charge, both hospitals and health centers are not providing the necessary services up to the minimum standard free of charge. Lack of supplies and basic equipment is among the major drawbacks to giving standard service. At every ladder of the health system, there is a critical shortage of supplies for the diagnosis and treatment of pregnant and laboring women. Previous experience of shortage or absence of essential supplies such as basic drugs, laboratory reagents, and protective equipment is the reason for home delivery after full ANC follow-up. A 28-year-old mother who had a previous institutional delivery experience stated this fact as follows:
During my previous delivery, I was forced to buy examination gloves, anti-pain drugs, intravenous fluids, and every necessary thing for my delivery from a private pharmacy. Even they ordered me to buy extra materials, it was very costly and unexpected, and beyond my family capacity. Due to this reason, I am forced to decide to give birth at home for my recent delivery.
The other strong comment that had appeared frequently in the participants’ data and which had put negative pressure to decide for home delivery of pregnant women including infrastructure problems such as bad roads and inaccessibility of ambulance service as immediately as needed, poor delivery room set-up, lack of maternity waiting rooms and lack of ultrasound service at health centers level are among the major barriers after full ANC follow-up. This notion is explained by a verbatim quotation obtained from a 35-year-old mother in the following manner:
When I was pregnant for my recent child I planned to go to a health institution for delivery. When the labor started, my husband called to Ambulance service but the Ambulance was delayed to come; after a while, I deliver at my house. During the labor, the baby came in the wrong position choked by placenta fluid, and died.
Discussion
The current study identified three major themes and nine sub-themes. The three major themes are socio-cultural and community influence, socio-economic obstacles, and health system-related barriers. Traditional practices, personal beliefs, social norms, knowledge, and attitude about institutional delivery, household economic capability, decision-making capacity of the women, quality of delivery services, service providers, and supply-related barriers were the nine sub-themes that emerged from the data.
This study revealed that traditional practices such as attendance of deliveries by TBAs or previously experienced women during delivery were among the major reasons for home delivery after full ANC follow-up. A similar finding was found in a qualitative study conducted in Butajira, Ethiopia, where the study reported that reliance of the community on TBAs for delivery services was the major reason for home delivery.21 However, this finding is not consistent with the study finding of Zambia where the study revealed that TBAs could conduct home delivery only in emergencies to prevent the woman from delivering on the way to health institutions.22 The difference might be study setup, health policy, implementation strategy, coverage, or quality of institutional delivery services.
The current study also demonstrated that the women believe that home is the correct place for delivery unless the pregnancy and labor are not complicated. This belief accompanied by the community long-lived norms of considering home delivery as good luck, limiting the movement of the pregnant women at home to pave the way for home delivery, and trust in the capability of experienced women to attend the delivery are the additional barriers to institutional delivery service utilization after full ANC follow-up. This finding is reported similarly in a systematic review report in Ethiopia and rural Bangladesh.23,24 However, it is not in line with other studies conducted in North and North-West Ethiopia where lack of education is a major factor for not seeking institutional delivery service after full ANC.25,26 This reported difference might be explained in terms of the study approach and setting difference.
Findings from the current study indicate that there has been low community awareness regarding institutional delivery, misunderstandings such as giving high emphasis to the ceremony of home delivery than the risk could that occur in the delivery process and blaming health facility delivery setups are among the reported reasons for home delivery. This result is in line with the study report of Eritrea in which the major reason for home delivery was a lack of awareness on the advantages of institutional delivery.27
The current economic status of the women was among the major influencing factor which has a direct impact on the delivery place preference of the mother after fully attending ANC service. Cost of transportation and other direct and indirect costs are among the major reasons for home delivery in the study setting after full ANC follow-up. A similar finding was reported in other studies in Eritrea27 and Nepal.28
According to the present study, relatives and close friends of pregnant women play a significant role in the decision-making process of the place of delivery of the women after fully booked for ANC. Husbands, mothers-in-law, mothers of the women, and women who have a previous home delivery experience were the significant others who influence women’s decision-making. This finding is supported by similar studies in Ethiopia.24,29
Poor quality of delivery service is one of the barriers to institutional delivery service utilization. Previous institutional delivery experience of unfriendly service provision, delivery attendance by students with limited or absent supervision by seniors, poor infection prevention protocols, and lack of privacy were the major reasons for home delivery after full ANC service. This result is supported by a systematic review report done in Ethiopia where poor delivery service quality was among the main reasons for home delivery.24
Healthcare providers’ knowledge, attitude, or skill gaps were the other causes for home delivery after full ANC follow-up. Early or late appointments by miscalculated EDDs, poor counseling in ANC visits, inappropriate and inadequate examinations during ANC visits, and confusing recording of LMP are among the frequently mentioned healthcare providers related barriers. A similar finding was reported in other studies in Ethiopia and other African countries.24,29,30
This study demonstrated that supply-related barriers are also the major reasons for home delivery. Previous experience of shortage or absence of essential supplies such as basic drugs, laboratory reagents, and protective equipment is also an additionally raised reason for home delivery after a full ANC follow-up. The same finding was reported in other studies of Ethiopia and other African countries.13,30
Conclusions
In this study, home delivery experience after full antenatal care follow-up is explained by socio-economic, cultural, and health system-related barriers in the study setting. Therefore, banning or upgrading traditional birth attendant’s skills, awareness creation of pregnant women about institutional delivery, and community health education on the elimination of home delivery facilitative social norms are recommended. Moreover, empowerment of pregnant women’s economic and decision-making capability and healthcare workers’ and health facilities’ capacity should be improved.
Abbreviations
ANC, antenatal care; EDD, expected due date; FGDs, focused group discussions; IDI, in-depth interview; IDIPs, in-depth interview participants; LMP, last menstrual period; TBAs, traditional birth attendants.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and its Supplementary Materials.
Ethics Approval and Consent to Participate
The current study was conducted following the declaration of Helsinki for studies involving human participants. Ethics approval was obtained from the Institutional Review Board (IRB) of Wolaita Sodo University. Permission was secured from Wolaita Zone Health Department and District Health Offices sequentially. The purpose and procedure of the study were explained to study participants. Informed written consent was obtained from each participant. To maintain the privacy of study participants, a comfortable place for interviews and FGDs were chosen based on the participants’ recommendations. Items seeking personal information such as names and phone numbers were not included in the interview guide to keep privacy and confidentiality. Participants were assured that they have the right to continue with the interview or FGDs or to withdraw at any point if they want to do so. Code labels of participants were used to maintain the privacy, confidentiality and anonymity of the participants’. The study participants also voluntarily consented to publish their anonymized responses in scientific journals for better dissemination of the results “Supplementary Materials Section 3”.
Acknowledgments
Our gratitude goes to the research study participants, Wolaita Zone Health Department, District Health Offices, Health Center Administrators, the Kebele leaders and HEWs for their valuable contributions.
Author Contributions
All authors equally contributed to this work beginning from the conception, study design, execution, acquisition of data, analysis, and interpretation. All authors of this work took part in the drafting, revising, and/or critical reviewing of the article, agreed on the journal to which the article was submitted, reviewed and agreed on all versions of the article before submission, during revision, the final version accepted for publication and gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding
This study did not receive any funding.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Olonade O, Olawande TI, Alabi OJ, Imhonopi D. Maternal mortality and maternal health care in Nigeria: implications for socio-economic development. Open Access Maced J Med Sci. 2019;7(5):849–855. doi:10.3889/oamjms.2019.041
2. Merdad L, Ali MM, Yotebieng M. Timing of maternal death: levels, trends, and ecological correlates using sibling data from 34 sub-Saharan African countries. PLoS One. 2018;13(1):e0189416–e0189416. doi:10.1371/journal.pone.0189416
3. Bauserman M, Lokangaka A, Thorsten V, et al. Risk factors for maternal death and trends in maternal mortality in low- and middle-income countries: a prospective longitudinal cohort analysis. Reprod Health. 2015;12(Suppl2):S5. doi:10.1186/1742-4755-12-S2-S5
4. WHO U, UNFPA, World Bank Group, The United Nations Population Division. Trends in Maternal Mortality: 1990 to 2015; 2015.
5. Ayenew AA. Incidence, causes, and maternofetal outcomes of obstructed labor in Ethiopia: systematic review and meta-analysis. Reprod Health. 2021;18(1):61. doi:10.1186/s12978-021-01103-0
6. Agency CS. Demographic and health survey; 2016.
7. The Federal Democratic Republic of Ethiopia Ministry of Health. Health sector transformation plan; 2015.
8. Berhan Y, Berhan A. Antenatal care as a means of increasing birth in the health facility and reducing maternal mortality: a systematic review. Ethiop J Health Sci. 2014;24:93–104. doi:10.4314/ejhs.v24i0.9S
9. Berhe R, Nigusie A. Magnitude of home delivery and associated factors among child bearing age mothers in Sherkole District, Benishangul Gumuz regional state-Western-Ethiopia. BMC Public Health. 2020;20(1):796. doi:10.1186/s12889-020-08919-8
10. Delibo D, Damena M, Gobena T, Balcha B. Status of home delivery and its associated factors among women who gave birth within the last 12 months in East Badawacho District, Hadiya Zone, Southern Ethiopia. Biomed Res Int. 2020;2020:4916421. doi:10.1155/2020/4916421
11. Cheelo C, Nzala S, Zulu JM. Banning traditional birth attendants from conducting deliveries: experiences and effects of the ban in a rural district of Kazungula in Zambia. BMC Pregnancy Childbirth. 2016;16(1):323. doi:10.1186/s12884-016-1111-9
12. Paul BK, Rumsey DJ. Utilization of health facilities and trained birth attendants for childbirth in rural Bangladesh: an empirical study. Soc Sci Med. 2002;54(12):1755–1765. doi:10.1016/S0277-9536(01)00148-4
13. Kasaye HK, Endale ZM, Gudayu TW, Desta MS. Home delivery among antenatal care booked women in their last pregnancy and associated factors: community-based cross sectional study in Debremarkos town, North West Ethiopia, January 2016. BMC Pregnancy Childbirth. 2017;17(1):225. doi:10.1186/s12884-017-1409-2
14. Siyoum M, Astatkie A, Mekonnen S, et al. Home birth and its determinants among antenatal care-booked women in public hospitals in Wolayta Zone, southern Ethiopia. PLoS One. 2018;13(9):e0203609. doi:10.1371/journal.pone.0203609
15. Perreault K. Research design: qualitative, quantitative, and mixed methods approaches. Man Ther. 2011;16:103. doi:10.1016/j.math.2010.09.003
16. John W C. Research Design: Qualitative, Quantitative and Mixed Methods Approaches.
17. Polit DF, Beck CT. Nursing Research – Generating and Assessing Evidence for Nursing Practice.
18. Vasileiou K, Barnett J, Thorpe S, Young T. Characterising and justifying sample size sufficiency in interview-based studies: systematic analysis of qualitative health research over a 15-year period. BMC Med Res Methodol. 2018;18:148–166. doi:10.1186/s12874-018-0594-7
19. Kiger ME, Varpio L. Thematic analysis of qualitative data: AMEE guide no. 131. Med Teach. 2020;42(8):846–854. doi:10.1080/0142159X.2020.1755030
20. Tong A, Sainsbury P, Craig J. Consolidated Criteria for Reporting Qualitative Research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
21. Roro MA, Hassen EM, Lemma AM, Gebreyesus SH, Afework MF. Why do women not deliver in health facilities: a qualitative study of the community perspectives in south central Ethiopia? BMC Res Notes. 2014;7(1):556. doi:10.1186/1756-0500-7-556
22. Sialubanje C, Massar K, Hamer DH, Ruiter RAC. Reasons for home delivery and use of traditional birth attendants in rural Zambia: a qualitative study. BMC Pregnancy Childbirth. 2015;15(1):216. doi:10.1186/s12884-015-0652-7
23. Sarker BK, Rahman M, Rahman T, Hossain J, Reichenbach L, Mitra DK. Reasons for preference of home delivery with traditional birth attendants (TBAs) in rural Bangladesh: a qualitative exploration. PLoS One. 2016;11(1):e0146161. doi:10.1371/journal.pone.0146161
24. Weldegiorgis SK, Feyisa M. Why women in Ethiopia give birth at home? A systematic review of literature. Int J Womens Health. 2021;13:1065–1079. doi:10.2147/IJWH.S326293
25. Nigatu A, Gelaye K, Degefie DT, Birhanu A. Spatial variations of women’s home delivery after antenatal care visits at lay Gayint District, Northwest Ethiopia. BMC Public Health. 2019;19. doi:10.1186/s12889-019-7050-4
26. Abebe F, Berhane Y, Girma B. Factors associated with home delivery in Bahirdar, Ethiopia: a case control study. BMC Res Notes. 2012;5(1):653. doi:10.1186/1756-0500-5-653
27. Kifle MM, Kesete HF, Gaim HT, Angosom GS, Araya MB. Health facility or home delivery? Factors influencing the choice of delivery place among mothers living in rural communities of Eritrea. J Health Popul Nutr. 2018;37(1):22. doi:10.1186/s41043-018-0153-1
28. Dhakal PMS, Shrestha MMS, Baral DMS, Pathak SMD. Factors affecting the place of delivery among mothers residing in Jhorahat VDC, Morang, Nepal. Int J Community Based Nurs Midwifery. 2018;6(1):2–11.
29. Mehretie Adinew Y, Abera Assefa N, Mehretie Adinew Y. Why do some Ethiopian women give birth at home after receiving antenatal care? Phenomenological study. Biomed Res Int. 2018;2018:3249786. doi:10.1155/2018/3249786
30. Wilunda C, Quaglio G, Putoto G, et al. A qualitative study on barriers to utilization of institutional delivery services in Moroto and Napak districts, Uganda: implications for programming. BMC Pregnancy Childbirth. 2014;14(1):259. doi:10.1186/1471-2393-14-259
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.