Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Why Do Community-Dwelling Persons with Spinal Cord Injury Visit General Practitioners: A Cross-Sectional Study of Reasons for Encounter in Swiss General Practice
Authors Touhami D ![]() , Essig S, Scheel-Sailer A
, Essig S, Scheel-Sailer A ![]() , Gemperli A
, Gemperli A ![]()
Received 12 July 2022
Accepted for publication 6 September 2022
Published 12 September 2022 Volume 2022:15 Pages 2041—2052
DOI https://doi.org/10.2147/JMDH.S382087
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Dima Touhami,1,2 Stefan Essig,1,3 Anke Scheel-Sailer,1,4 Armin Gemperli1– 3
1Department of Health Sciences and Medicine, University of Lucerne, Lucerne, 6002, Switzerland; 2Swiss Paraplegic Research, Nottwil, 6207, Switzerland; 3Center of Primary and Community Care, University of Lucerne, Lucerne, 6002, Switzerland; 4Swiss Paraplegic Center, Nottwil, 6207, Switzerland
Correspondence: Dima Touhami, Swiss Paraplegic Research, Guido A. Zäch Strasse 4, Nottwil, 6207, Switzerland, Tel +41 41 939 65 65, Email [email protected]
Purpose: In a country of free selection of providers, general practitioners (GPs) remain the most visited health-care professionals by the vast majority of persons with spinal cord injury (SCI) in Switzerland; yet, little is known about these contacts. The study aims to explore reasons for encounters (RFEs) in general practice, and their relationships to first-contact of care (GP or specialist) and GP’s competence in managing SCI-specific problems.
Patients and Methods: Cross-sectional study from baseline data of non-randomized controlled trial. Persons with SCI in the chronic phase and living in Swiss rural communities were invited. Participants were asked about RFEs (reasons and health problems) of their last visit to a GP. RFEs were coded according to the International Classification of Primary Care (ICPC-2), and analyzed according to first-contact and participants’ ratings of GPs’ competence in managing SCI-specific problems.
Results: Out of 395, 226 (57%) persons participated, of which 89% have reported 2.1 (SD ± 1.4) RFEs and 2.4 (± 1.7) health problems per GP visit, on average. Participants visited GPs for medications (49%), urgent medical problems (33%) and follow-up (30%). Most RFEs were related to general/unspecified problems (65%). Persons whose first contact was a specialist were more likely to visit GPs for medications (Specialist = 60% vs GP = 42%). There were no associations between RFEs and the perceived GP’s competence at P < 0.05.
Conclusion: Irrespective of first contact of care, persons with SCI visit GPs for medication, urgent issues, and follow-up care, and more often for general problems than for secondary health conditions. Strengthening collaboration between GPs in rural communities and specialized centers is recommended; promoting such a connection potentially aids GPs in meeting their information needs for managing secondary health conditions and improving the quality of SCI care for this population.
Keywords: general practitioners, spinal cord injury, specialists, health problems, competence
Introduction
Spinal cord injury (SCI) is a potentially fatal medical condition, and has far-reaching effects on the physical, mental, social, and financial well-being of those affected.1,2 Depending on the location and severity of the injury, persons with SCI face a life-long increased risk of secondary health conditions, functional loss, and increased dependence, prompting the use of health-care services at a higher rate than the general population.3–5 To meet their complex needs, highly specialized multidisciplinary care is desired for the treatment, rehabilitation, and life-long care of persons with SCI.2,6 However, this institutes a challenge for those living in rural areas. The lack of local SCI expertise, problems with long-distance transportation, and unmet information needs are commonly cited the further they reside from specialized centers.7,8 To compensate, persons with SCI tend to become considerably higher users of primary care services.9–12
Primary care is defined by its comprehensiveness, continuity, centeredness, and coordination of care.3,13 In that respect, general practitioners (GPs) play an essential role in promoting health and in preventing life-threatening illnesses, hospital admissions, and secondary complications.3,13 However, due to the low prevalence and sporadic encounters with persons with SCI, GP care may fall behind acute and specialized rehabilitation services, as GPs experience doubt about their skills in providing SCI-specific care.3,4 Similarly, persons with SCI often report that GPs lack the up-to-date knowledge to deliver optimal care, and prefer to receive SCI-specific care from specialists.3,10,13 Several studies investigated GP visits of persons with SCI.10,12,14,15 A cross-sectional study of Donnelly et al examined the utilization of and access to primary care for persons with SCI in the United States, Canada, and the United Kingdom.10 The majority considered their GP the most appropriate provider of care for new conditions or problems such as fatigue, pain, and bowel or bladder issues.10 GPs were also cited as the main contact for preventive care, such as physical check-ups, blood and urinary specimens, and personal problems.10
There is no standard model of care in Switzerland that outlines care and services for persons with SCI across the SCI care continuum. Health-care services are decentralized; all people have direct access to primary and specialized care through the standard mandatory health insurance. Alternative plans with lower premiums are available but restrict the choice of provider.16 While specialized SCI care is the recommended choice in Switzerland, GPs remained the most visited health-care professionals by the vast majority of persons with SCI and the first point of contact for SCI-specific problems in 44% of cases.11,14 Most reported contacting a GP for acute problems at an average of 4.5 visits per year.11,14 Conversely, SCI specialists were predominately visited for check-ups by almost half of the participants at an average of 1.5 visits per year and were further pronounced as the first contact of care for 56% of cases.11,14 However, specialists’ support and availability of SCI outreach teams were foreseen as central to meeting the SCI-specific needs of the SCI population.2,12,14
So far, little is known about why persons with SCI contact GPs in Swiss rural regions and for which health problems. In the absence of defined roles and responsibilities in SCI care, understanding the perspectives of persons with SCI on GP care seems imperative for future roles clarification, planning of health services and training programs, and sensitizing GPs to the complex health needs of this population.16 With this study, we aim to explore the reasons for encounters (RFEs) in general practice, the extent to which RFEs are linked to the first contact of care (GP or specialist), and the perceived competence of GPs in managing SCI health problems.
Materials and Methods
Study Design
This is a cross-sectional study based on baseline data of an intervention study that aimed to enhance scientific collaboration between highly specialized SCI centers and GPs practicing in rural Swiss communities through medical education on SCI-specific topics.17 Details on the design, recruitment, and methodology of the study were described by Tomaschek et al.17 Persons with SCI were eligible to participate if they were above 16 years of age; living with SCI for more than two years at that time of data collection; residing further than a 60-minute vehicle driving distance to any of the four centers for persons with SCI in Switzerland (Swiss Paraplegic Center in Nottwil, REHAB in Basel, Clinique Romande de Réadaptation in Sion, University Hospital Balgrist in Zurich), and two SCI outpatient clinics in Lausanne and Bellinzona; and had previously participated in the Swiss Spinal Cord Injury Cohort Study (SwisSCI) community survey of 2017.18 Out of 1530 persons, 395 were eligible to participate. Paper-based questionnaires were sent by post with pre-stamped return envelopes in February 2020. Participants had the option to complete the questionnaire either online or on paper. Within eight weeks, non-respondents received two reminders: by post and telephonically.
Measures
Explanatory Variables
Participants’ characteristics included sex, age, civil status, country of birth, living arrangement, years in formal education, employment status, and language of the questionnaire (German, French, or Italian). Participants were also asked if they had a personal GP and to report the travel distance in minutes. Participants were asked about their first contact for SCI-specific health problems; options included (1) GP, (2) specialist with own practice, (3) specialist at one of the four SCI centers, or (4) other. Participants who indicated a GP or specialist were included in the analysis. Health status was assessed using a 5-point scale (1 = excellent; 5 = poor). Injury-related information included time since injury in years, cause of injury (traumatic or non-traumatic), SCI lesion type (complete versus incomplete), and injury level (paraplegia or tetraplegia). The modified Spinal Cord Injury Secondary Conditions Scale (SCI-SCS) was used to assess the occurrence of secondary health conditions (n = 15) in the previous 12 months.19 Responses were rated along a 4-point ordinal scale (0 = not experienced/insignificant problem to 3=significant/chronic problem). Participants were asked to rate how they perceived the competence of their GP in managing SCI health problems on a 5-point Likert scale rating (1 = excellent to 5 = very bad).
Outcome Measures
The structure of the International Classification for Primary Care 2 (ICPC-2) was used to design the RFE question. Participants were instructed to indicate the reason/s for their last GP visit and provide details for each selected response in a free text box. Components included routine exam/annual check-up; an urgent disease problem; new medical problem; follow-up on existing health condition or test results; diagnostic testing, screening, or vaccination; medication supply (refills or prescription renewal); referral (specialist, hospital, or diagnostics); administrative work (forms, certificates, etc.); other reason, or I do not remember. Only participants who completed the RFE question were included in the analysis.
Based on participants’ input in the free text box, health problems were coded according to the ICPC-2 chapters, which included general and unspecified, blood/blood forming organs, digestive, eye, ear, circulatory, musculoskeletal, neurological, psychological, respiratory, skin, endocrine, metabolic and nutritional, urological, pregnancy, child bearing and family planning, female genital, male genital, and social problems. Only chapters with observations are presented in the tables. The ATC classification system was followed to categorize reported medications according to their therapeutic group and indications; they were then coded under the ICPC-2 chapters.20
Statistical Methods
Descriptive statistics were employed to describe the participants’ characteristics, the number and distribution of RFEs, and health problems and were reported as absolute and relative frequencies, means, and standard deviations. A t-test was used to compare the differences in the mean number of RFEs or health problems per visit according to first contact of care. Pearson’s chi-square test was used to measure the association between RFEs or health problems and the first contact of care. It was also used to measure the association between the perceived competence level of GPs in managing SCI health problems and first contact of care. The Mann–Whitney U-test was used to measure the association between RFEs or health problems and the perceived competence level of GPs, respectively. All statistical findings were compared at a significance level of P < 0.05, and all statistical analyses were performed using Stata® version 16.1 (Stata Corp LP, College Station, Texas, USA).
Results
Of the 226 participants (response rate 57%), 75% were males, and the mean age was 57.2±13.6 (ranging from 21 to 86) years. Most participants (79%) were German-speaking, and had an average of 14.1±3.2 years of formal education. The vast majority had a personal GP (96%), who they visited at an average of 4.1±4.5 visits per year, and more than half (53%) reported the GP as their first contact for SCI-specific care. Detailed information on the participants’ characteristics is presented in Table 1.
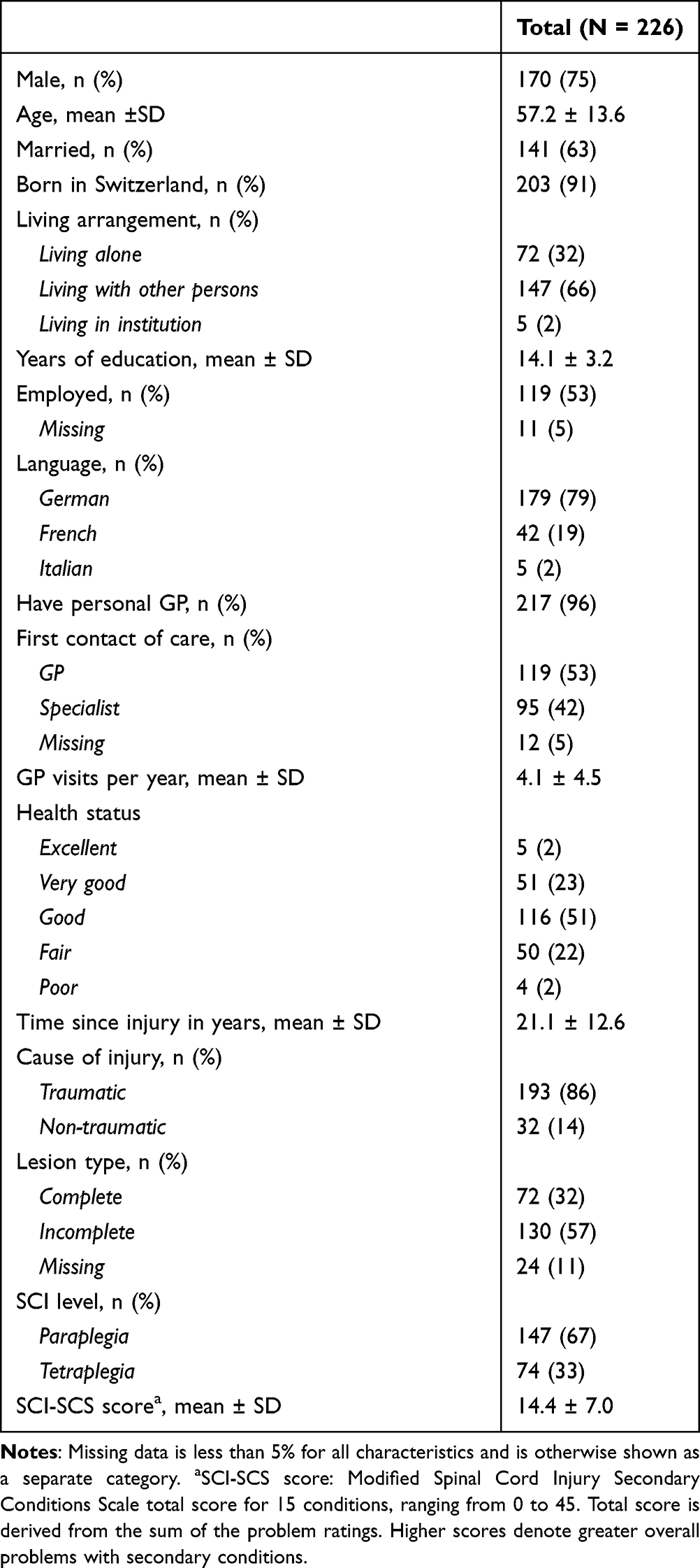 |
Table 1 Participants' Characteristics |
Table 2 presents the distribution of RFEs by health problems. Of the 226 questionnaires completed for the study, 210 participants had visited a GP within the last year, however only 202 (89%) participants filled out the RFE question, with an average of 2.1 (SD±1.4) RFEs and 2.4 (±1.7) health problems per GP visit, respectively.
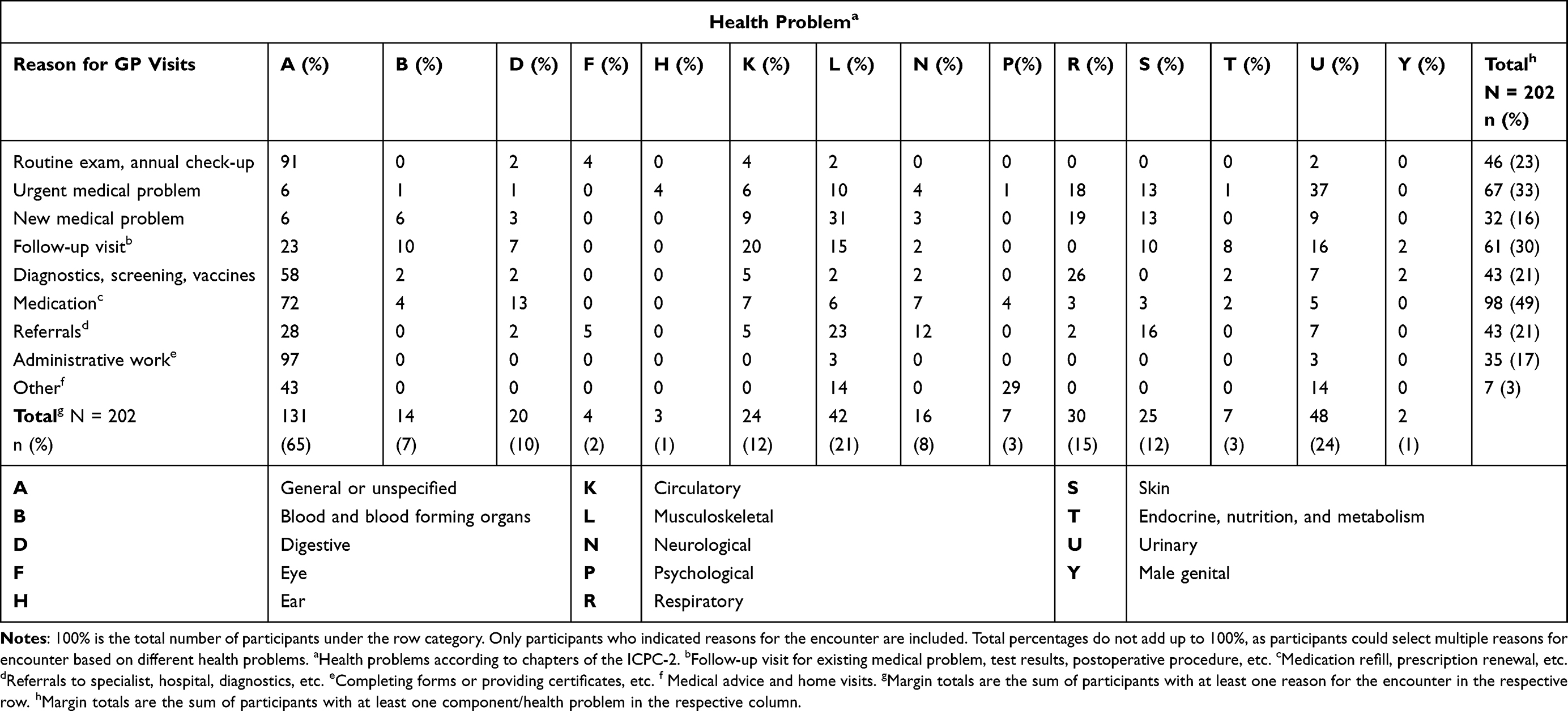 |
Table 2 Self-Reported Reasons for GP Visits by Health Problem |
Of the 202 participants, 39% reported one RFE, 32% two RFEs, 17% three RFEs, and 12% documented more than three RFEs per visit. Almost half of these participants (49%) visited GPs for medications, 33% for urgent medical problems, 30% for follow-up, and 23% for routine or annual check-ups. According to the ICPC2 chapter classification, seeking GP care was largely for general/unspecified problems (65%, n = 131), 24% for urinary (n = 48), 21% for musculoskeletal (n = 42), and 15% for respiratory-related issues (n = 30).
Urinary problems represented 37% of urgent medical problems. Musculoskeletal conditions and respiratory tract infections represented 31% and 19% of new problems, respectively. Similarly, cardiovascular (20%), urinary (16%), musculoskeletal problems (15%), and skin issues (10%) were among the top reasons for follow-up visits. Of the respondents who visited a GP for referrals (n = 43), almost 37% indicated it was for a specialist, 23% for physiotherapy and SCI specialized centers,14% for hospital admissions and 26% did not specify.
Table 3 presents the distribution of RFEs in GP visits according to the first contact of care. Out of the 202 participants, 191 (95%) indicated their first contact of care (GP or specialist). Persons with a GP as first contact (n = 109) had a lower mean number of RFEs (2.0±1.2) per visit, as compared to those in the specialist group (n = 82; 2.4±1.6), but this difference was not statistically significant.
 |
Table 3 Self-Reported Reasons for Encounter by First Contact of Care |
In both groups of participants, the common RFEs were for urgent medical problems (GP as first contact of care = 33% vs Specialist = 30%), follow-up (GP = 31% vs Specialist = 30%), and new medical problems (GP = 16% vs Specialist = 17%). Persons in the specialist group (60%) were statistically significantly more likely to visit GPs for medication than participants in the GP group (42%).
Table 4 provides an overview of the health problems managed by GPs according to first contact of care. Persons who had a GP as first contact demonstrated a lower mean number of health problems (2.2±1.4) per visit, as compared to those in the specialist group (2.6±1.9), and this difference was not statistically significant at P < 0.05. At comparable frequencies, participants in both groups visited GPs for urinary concerns (GP as first contact of care = 20% vs Specialist = 22%), musculoskeletal-related problems (GP = 18% vs Specialist = 23%), and respiratory issues (GP = 16% vs Specialist = 16%). Persons in the specialist group were twice as likely (16%) to visit GPs for circulatory conditions than those in the GP group (7%). We found no statistically significant association between any of the health problems and first contact of care.
 |
Table 4 Health Problems Managed by GPs by First Contact of Care |
In response to how participants generally rated their GP’s competence in managing SCI health problems, 23% reported it as “very good”, 44% as “good”, 25% as “average”, and 8% as “bad” to “very bad.” The relationship between RFEs and the perceived competence of GPs is presented in Figure 1. The majority of the participants who visited a GP for routine exam/annual check-up (favorable ratings = 70%); or follow-up (71%); regarded the competence of their GP in managing SCI health problems as “good” to “very good.” However, about 33% and 14% of persons who visited GPs for referrals rated their competence as “average” and “bad to very bad”, respectively. We found no statistically significant relationship between RFEs and the GPs’ competence ratings.
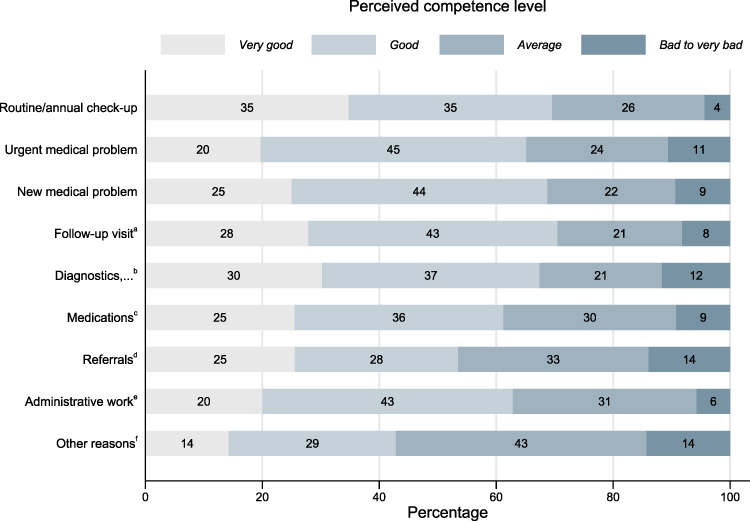 |
Figure 1 Perceived competence of GPs in managing SCI health problems by reasons for encounter. aFollow-up visit for existing medical problem, test results, etc. bDiagnostic, screening, and vaccination. cMedication refills, prescription renewal, etc. dReferrals to specialist, hospital, diagnostic, etc. eCompleting forms or providing certificates, etc. fMedical advice or home visits, etc. 100% is the total number of participants in each specific category responding to the competence level. Mann–Whitney-U test was used to measure the significant association between the reason for the encounter and the perceived competence of GPs, and no relation was found to be statistically significant at P < 0.05. |
Grouped by the perceived competence of GPs in managing SCI health problems, Figure 2 shows the top 7 health problems indicated by participants for visiting GPs. The majority of the participants who visited a GP for circulatory (favorable ratings = 75%), respiratory (74%), or skin problems (72%) rated their competence between “good” and “very good.” Almost half of the participants who visited a GP for musculoskeletal (49%) or digestive problems (45%) rated their competence between “average” and “bad to very bad.”
 |
Figure 2 Perceived competence of GPs in managing SCI health problems by top 7 health problems. Health problems according to chapters of the ICPC-2. 100% is the total number of participants in each specific category responding to the competence level. Mann–Whitney U-test was used to measure the significant association between health problem and the perceived competence of GPs, and no relation was found to be statistically significant at P < 0.05. |
The relationship between GPs’ perceived competence in managing SCI health problems and first contact of care is presented in Figure 3. Compared to a specialist, participants who had a GP as first contact of care were statistically significantly more likely to rate the GP’s competence as “very good” (GP as first contact of care = 35% vs Specialist = 10%) and less likely to rate it as “average” (GP = 18% vs Specialist = 35%) or “bad to very bad” (GP = 3% vs Specialist = 13%).
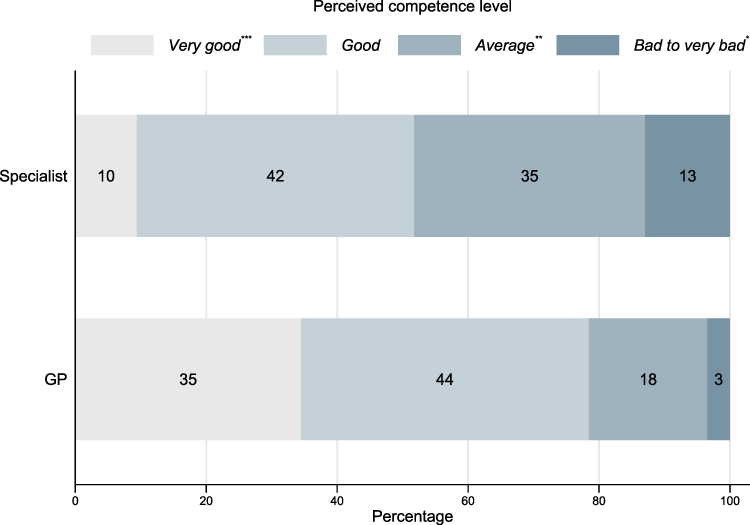 |
Figure 3 Perceived competence of GPs in managing SCI health problems by first contact of care. 100% is the total number of participants for each competence level. Pearson’s chi-square test was used to measure the significant association between the perceived competence level of GPs in managing SCI health problems and the first contact of care; *P < 0.05, **P < 0.01, ***P < 0.001. |
Discussion
This study examined the reasons persons with SCI visit GPs, the link between the RFEs and the perceived competence of GPs in managing SCI health problems, and the first contact of care. In this study, almost half of the participants visited a GP for medication. This finding is not surprising, as persons with SCI are at heightened risk of experiencing significant secondary health problems, such as spasticity, chronic pain, bowel and bladder problems, urinary tract infections, cardiovascular disease, and diabetes, which are commonly managed with pharmacotherapy.21,22 In view of the first contact of care, persons whose first contact was a specialist were likely to visit a GP for medication supply more often than those in the GP group. Apparently, this group tends to select providers and services according to their health situations, however both SCI specialists and GPs are needed together to fulfill their needs. Moreover, visiting GPs for medication is more convenient, given the proximity of GP practices and the far distance to specialists and SCI centers. Furthermore, GPs in Switzerland not only prescribe medications but are allowed to sell them directly to patients through their in-practice pharmacies.23 This “self-dispensing” practice is cantonal dependent, authorized in German-speaking cantons, and disapproved in the French-speaking regions. Currently, 14 of 26 cantons permit physicians to sell medications freely and another three offer dispensing licenses under specific conditions.23
In line with previous research on the same population, most visits to a GP were for acute problems.11 Whether as urgent or new medical problem, urinary tract infections, musculoskeletal pain, spasticity, and respiratory tract infections represented the top health problems to visit a GP in participants whose first contact of care was a GP or specialist. Similarly, no significant differences in frequency were found between the two groups when visiting a GP for follow-up care. Indeed, both groups reported visits for existing chronic conditions, such as hypertension, diabetes, or follow-up on blood test results or for suture removal or dressing change. These findings reflect the traditional scope of practice of GPs in Switzerland; they treat a wide range of illnesses and provide a broad set of services, including diagnosis and follow-up for chronic conditions.24 In addition, GPs are easily accessible, as their practices lied within 25 minutes of vehicle driving distance to almost 86% of the study participants.14
Comparable to Van Loo et al25, our study shows that 23% of the participants visited a GP for routine/annual check-ups, in contrast to 50% who reported receiving their check-up at one of the four specialized SCI centers.26 This finding may be interpreted by the complexity of SCI and the need for higher expertise and knowledge to manage their secondary health conditions.25,27 For this reason, the specialized centers in Switzerland routinely invite all persons with SCI for annual control visits, at which they receive multidisciplinary comprehensive care according to accepted clinical guidelines for various body systems, for which GPs may not have the needed skills and knowledge.11,27
Most participants rated the competence of their GP favorably in relation to SCI-specific care. Nonetheless, the frequency of documented RFEs for secondary health conditions remained low, despite the relatively higher SCI-SCS total mean score (14.4±7.0), which is opposed to previously reported.14 These findings possibly suggest response bias. As the participants were part of an interventional study,17 prior knowledge about the study may have resulted in more favorable ratings and fewer natural responses. In addition, participants were recruited based on their proximity to GPs participating in the interventional study;17 it may be possible that, because of the familiarity of participants with their GP, they had fears of having their responses linked to their data. Furthermore, the results on RFEs represented the last episode of care. Therefore, previous visits to GPs for other reasons or different health problems, including secondary conditions, were not captured in this study and could not be excluded. Alternatively, given the chronicity of certain secondary conditions, eg, pain and sexual dysfunction, persons with SCI may not necessarily seek GP care whenever experiencing these conditions. Nonetheless, former evidence on not receiving SCI-specific care in the same population was documented by Gemperli et al, and was linked to the unavailability of the service at the time of need or in the region, the lack of knowledge of whom to contact when medical care was needed, and the lack of SCI expertise among health-care providers.11 However, it is inconceivable to expect all GPs to be competent in managing secondary health conditions or trained on this topic.9 Instead, creating a connection between GPs in rural communities and specialized centers is far more feasible and attainable. Such an approach would enable GPs to meet their information needs on whom to contact and where to access knowledge about the management of SCI.6,28 In addition, promoting digital tools for information exchange among providers is recommended to optimize interprofessional collaboration along the patient pathway and for integrated care.29
The current study established a positive link between the choice of first contact and the perceived competence of GPs in the domain of SCI-specific care. This potentially reflects more complex medical needs in the specialist group and higher care expectations, leading to lower ratings. Former accounts of frustration among persons with SCI were documented by Stillman et al, and were attributed to the unfamiliarity of primary care physicians with the impact of SCI on their overall lives and their poor understanding of medical issues associated with disability.30 In addition, the continued doctor–patient relationship and positive personal interactions have possibly acted as a buffer against unfavorable ratings of technical expertise in the GP group.10
Despite the high prevalence of sexual dysfunction in persons with SCI,14,21 only two participants visited a GP for reproductive health issues. Nonetheless, this result is not surprising, as issues of sexual health are among the least addressed problems in general and in primary care for persons with SCI, and is viewed as a sensitive topic to address.10,21 Similarly, visiting a GP for psychological or social issues was almost non-existent among the participants, despite the higher prevalence of depression in this group than in the general population.31–33 This finding has already been highlighted previously,10,25 in which the majority cited unmet psychosocial care needs by GPs or specialists.10
Limitations and Strengths
The results of this study should be interpreted in light of its limitations. As noted, the study sample is not a random sample of all persons with SCI, and the results cannot be generalized to this population. Although a response rate of 57% is considered acceptable, non-response bias owing to differences in the individual characteristics between survey respondents and non-respondents cannot be excluded. In addition, participants were asked to retrospectively report their GP visits, which may have introduced recall bias. This survey took place during the COVID-19 pandemic lockdown. Hence, it is essential to account for potential variations in medical contacts and participants’ reports of RFEs owing to the physical distancing and reduced travel and transportation for this vulnerable population. In the present study, almost 22% of all RFEs were left without further details, which resulted in coding these RFEs under “unspecified.” Furthermore, the RFEs were solely based on the participants’ accounts. Therefore, further research is desired to find similarities between how persons with SCI express their demands for care and the actual diagnoses made by their GP.34 This study did not account for possible differences in RFEs, health problems or perceived competence of GPs across participants’ characteristics, but this could be considered in future research. Despite these limitations, this study represents an essential first step toward a better understanding of RFEs in a systematic and person-centered manner and of the GPs’ competence in managing SCI health problems from the perspective of persons with SCI.
Conclusion
Irrespective of first contact of care, persons with SCI living in rural communities visit GPs for medications, urgent issues, and follow-up care, and more often for health problems such as urinary tract infections, musculoskeletal pain, spasticity, and respiratory tract infections. The current care model for SCI, which unilaterally demands specialized rehabilitation care, seems unrealistic, and prevents adequate care for many patients. Strengthening collaboration and knowledge transfer between GPs in rural communities and specialized centers is recommended. Promoting such a connection potentially aids GPs in meeting their information needs for managing secondary health conditions and improving the quality of SCI care for this population.
Abbreviations
SCI, spinal cord injury; GP, general practitioner; RFE, reasons for encounter; SwiSCI, Swiss Spinal Cord Injury Cohort Study; SCI-SCS, Spinal Cord Injury Secondary Conditions Scale; ICPC-2, International Classification of Primary Care, 2nd edition.
Data Sharing Statement
Owing to our commitment to SwiSCI study participants and their privacy, datasets generated during the current study have not been made publicly available but can be provided by the SwiSCI Study Centre upon reasonable request ([email protected]).
Ethics Approval and Consent to Participate
This study is covered by the ethical approval awarded by Ethikkommission Nordwest-und Zentralschweiz (EKNZ, Project-ID: 2019-01527, approved in September 2019) to the SCI-Co study with the project title “Shared responsibility between general practitioners and highly specialized hospitals in complex chronic conditions: the case of spinal cord injury in a nationwide intervention study”. We confirm that this study complied with the ethical guidelines of the Helsinki Declaration and that all applicable institutional and governmental regulations relating to the ethical use of human volunteers were followed during the course of this research. All study participants have signed a document to provide their written informed consent.
Acknowledgments
We thank the SwiSCI Steering Committee with its members Xavier Jordan, Fabienne Reynard (Clinique Romande de Réadaptation, Sion); Michael Baumberger, Luca Jelmoni (Swiss Paraplegic Centre, Nottwil); Armin Curt, Martin Schubert (Balgrist University Hospital, Zürich); Margret Hund-Georgiadis, NN (REHAB Basel, Basel); Laurent Prince (Swiss Paraplegic Association, Nottwil); Heidi Hanselmann (Swiss Paraplegic Foundation, Nottwil); Daniel Joggi (Representative of persons with SCI); Mirjana Bosnjakovic (Parahelp, Nottwil); Mirjam Brach, Gerold Stucki (Swiss Paraplegic Research, Nottwil); Armin Gemperli (SwiSCI Coordination Group at Swiss Paraplegic Research, Nottwil).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Three of the authors (DT, AS, and AG) are salaried employees of organizations financially supported by the Swiss Paraplegic Foundation. The funding party had no role in the study design, collection, analysis, interpretation of data, or writing of the manuscript.
References
1. World Health Organization (WHO). Spinal cord injury; 2013. Available from: https://www.who.int/news-room/fact-sheets/detail/spinal-cord-injury.
2. European Spinal Cord Injury Federation. ESCIF Policy Statement on the treatment, rehabilitation and life-long care of persons with spinal cord injuries (SCI). Available from: http://www.escif.org/ESCIFpolicy_statement.htm.
3. McColl MA, Aiken A, McColl A, et al. Primary care of people with spinal cord injury: scoping review. Can Fam Physician. 2012;58(11):1207–e1635.
4. Beatty PW, Hagglund KJ, Neri MT, et al. Access to health care services among people with chronic or disabling conditions: patterns and predictors. Arch Phys Med Rehabil. 2003;84(10):1417–1425.
5. Harrington AL, Hirsch MA, Hammond FM, et al. Assessment of primary care services and perceived barriers to care in persons with disabilities. Am J Phys Med Rehabil. 2009;88(10):852–863.
6. Cox RJ, Amsters DI, Pershouse KJ. The need for a multidisciplinary outreach service for people with spinal cord injury living in the community. Clin Rehabil. 2001;15(6):600–606.
7. LaVela SL, Smith B, Weaver FM, et al. Geographical proximity and health care utilization in veterans with SCI&D in the USA. Soc Sci Med. 2004;59(11):2387–2399.
8. Ronca E, Brunkert T, Koch HG, et al. Residential location of people with chronic spinal cord injury: the importance of local health care infrastructure. BMC Health Serv Res. 2018;18(1):657.
9. Amsters D, Schuurs S, Kendall M, et al. General practice visits by people with traumatic spinal cord injury: a Queensland longitudinal study. Aust J Prim Health. 2014;20(2):167–173.
10. Donnelly C, McColl MA, Charlifue S, et al. Utilization, access and satisfaction with primary care among people with spinal cord injuries: a comparison of three countries. Spinal Cord. 2007;45(1):25–36. doi:10.1038/sj.sc.3101933
11. Gemperli A, Ronca E, Scheel-Sailer A, et al. Health care utilization in persons with spinal cord injury: part 1-outpatient services. Spinal Cord. 2017;55(9):823–827. doi:10.1038/sc.2017.44
12. Ronca E, Scheel-Sailer A, Koch HG, et al. Satisfaction with access and quality of healthcare services for people with spinal cord injury living in the community. J Spinal Cord Med. 2020;43(1):111–121. doi:10.1080/10790268.2018.1486623
13. Rosano A, Loha CA, Falvo R, et al. The relationship between avoidable hospitalization and accessibility to primary care: a systematic review. Eur J Public Health. 2013;23(3):356–360.
14. Touhami D, Brach M, Essig S, et al. First contact of care for persons with spinal cord injury: a general practitioner or a spinal cord injury specialist? BMC Fam Pract. 2021;22(1):195.
15. Ronca E, Scheel-Sailer A, Koch HG, et al. Health care utilization in persons with spinal cord injury: part 2-determinants, geographic variation and comparison with the general population. Spinal Cord. 2017;55(9):828–833.
16. Berchtold P, Peytremann-Bridevaux I. Integrated care organizations in Switzerland. Int J Integr Care. 2011;11 Spec Ed(Special 10th Anniversary Edition):e010.
17. Tomaschek R, Touhami D, Essig S, et al. Shared responsibility between general practitioners and highly specialized physicians in chronic spinal cord injury: study protocol for a nationwide pragmatic nonrandomized interventional study. Contemp Clin Trials Commun. 2021;24:100873.
18. Gross-Hemmi MH, Gemperli A, Fekete C, et al. Methodology and study population of the second Swiss national community survey of functioning after spinal cord injury. Spinal Cord. 2021;59(4):363–372.
19. Spinal Cord Injury Research Evidence. Spinal Cord Injury Secondary Conditions Scale (SCI-SCS); 2020. Available from: https://scireproject.com/outcome-measures/outcome-measure-tool/spinal-cord-injury-secondary-conditions-scale-sci-scs/#1467983894080-2c29ca8d-88af.
20. WHO Collaborating Centre for Drug Statistics Methodology. Guidelines for ATC classification and DDD assignment 2021. Oslo, Norway; 2020. Available from: https://www.whocc.no/atc_ddd_index_and_guidelines/guidelines/.
21. Brinkhof MW, Al-Khodairy A, Eriks-Hoogland I, et al. Health conditions in people with spinal cord injury: contemporary evidence from a population-based community survey in Switzerland. J Rehabil Med. 2016;48(2):197–209.
22. Böthig R, Domurath B, Kutzenberger J, et al. The real daily need for incontinence aids and appliances in patients with neurogenic bladder dysfunction in a community setting in Germany. J Multidiscip Healthc. 2020;13:217.
23. De Pietro C, Camenzind P, Sturny I, et al. Switzerland: health System Review. Health Syst Transit. 2015;17(4):1–288.
24. Cartier T, Cornuz J. Switzerland. In: Kringos DS, Hutchinson A, editors. Building Primary Care in a Changing Europe: Case Studies. Copenhagen (Denmark): European Observatory on Health Systems and Policies; Vol. 40, 2015
25. van Loo MA, Post MW, Bloemen JH, et al. Care needs of persons with long-term spinal cord injury living at home in the Netherlands. Spinal Cord. 2010;48(5):423–428.
26. Ronca E, Scheel-Sailer A, Eriks-Hoogland I, et al. Factors influencing specialized health care utilization by individuals with spinal cord injury: a cross-sectional survey. Spinal Cord. 2021;59(4):381–388.
27. Spreyermann R, Lüthi H, Michel F, et al. Long-term follow-up of patients with spinal cord injury with a new ICF-based tool. Spinal Cord. 2011;49(2):230–235.
28. Mann L, Middleton JW, Leong G. Fitting disability into practice–focus on spinal cord injury. Aust Fam Physician. 2007;36(12):1039–1042.
29. Bundesamt für Gesundheit. Interprofessionelle Zusammenarbeit in der ambulanten Versorgung stärken—Policy Brief. Bern; 2021. Available from: https://www.bag.admin.ch/dam/bag/de/dokumente/berufe-gesundheitswesen/Interprofessionalitaet/policy-briefs/ambulante-versorgung.pdf.download.pdf/1_DE_Ambulante%20Versorgung.docx.pdf.
30. Stillman MD, Frost KL, Smalley C, et al. Health care utilization and barriers experienced by individuals with spinal cord injury. Arch Phys Med Rehabil. 2014;95(6):1114–1126.
31. Dryden DM, Rowe BH, May LA, et al. Utilization of health services following spinal cord injury: a 6-year follow-up study. Spinal Cord. 2004;42(9):513–525.
32. Kroll T, Neri MT, Ho P-S. Secondary conditions in spinal cord injury: results from a prospective survey. Disabil Rehabil. 2007;29(15):1229–1237.
33. Kalpakjian CZ, Albright KJ. An examination of depression through the lens of spinal cord injury: comparative prevalence rates and severity in women and men. Womens Health Issues. 2006;16(6):380–388.
34. Chmiel C, Bhend H, Senn O, et al. The FIRE project: a milestone for research in primary care in Switzerland. Swiss Med Wkly. 2011;140:w13142.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.