Back to Journals » Breast Cancer: Targets and Therapy » Volume 14
Whole Genome Sequencing of Single-Circulating Tumor Cell Ameliorates Unraveling Breast Cancer Heterogeneity
Authors Li Y, Jiang X, Zhong M, Yu B, Yuan H
Received 3 September 2022
Accepted for publication 7 December 2022
Published 28 December 2022 Volume 2022:14 Pages 505—513
DOI https://doi.org/10.2147/BCTT.S388653
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Pranela Rameshwar
Yongping Li,1 Xiaofei Jiang,1 Ming Zhong,1 Bo Yu,2 Hao Yuan1
1Department of Breast Surgery, Shanghai Pudong Hospital, Fudan University Pudong Medical Center, Shanghai, 201399, People’s Republic of China; 2Department of Vascular Surgery, Shanghai Pudong Hospital, Fudan University Pudong Medical Center, Shanghai, 201399, People’s Republic of China
Correspondence: Hao Yuan, Department of Breast Surgery, Shanghai Pudong Hospital, Fudan University Pudong Medical Center, 2800 Gongwei Road, Pudong New Area, Shanghai, 201399, People’s Republic of China, Tel +86 18918790382, Email [email protected] Bo Yu, Department of Vascular Surgery, Shanghai Pudong Hospital, Fudan University Pudong Medical Center, 2800 Gongwei Road, Pudong New Area, Shanghai, 201399, People’s Republic of China, Tel +86 18918922698, Email [email protected]
Objective: Because tumor tissues are most frequently heterogeneous and hard to characterize, the resulting therapeutic strategy could be misled. The most active and invasive tumor cells are circulating tumor cells (CTCs). In this study, we investigated the feasibility of individualized treatment of breast cancer patients based on whole genome sequencing (WGS) of single cell CTC.
Methods: Twenty-four CTCs were identified in three breast cancer patients. For each patient, one polyploid CTC was captured, and on which the WGS was performed. WGS was considered due to its sequencing robustness compared to conventional sequencing approaches. Based on the histopathological Her-2 status in tumor tissue and the HER2 gene status in WGS results of CTC, we adjusted treatment strategies and monitored disease progression.
Results: Patients ID1 and ID2 are found to be Her-2 positive in primary tumors and HER2 gene amplification in the DNA of CTCs. In-patient ID3, histopathological examination of the primary tumor and liver metastases revealed Her-2 negative, but the WGS analysis of CTC showed HER2 gene amplification. After adjusting treatment by adding Her-2 inhibitors according to the results of CTC sequencing, liver metastases and pleural effusion were significantly reduced two months later, CTC number and ctDNA burden were decreased, and 18-months progression-free survival (PFS) was recorded. In addition, some potential therapeutic targets and mutations in drug-resistant genes were detected.
Conclusion: The results of CTC sequencing effectively guided the treatment of a patient with HER2 gene amplification in CTC but with Her-2 negative on tumor tissue. Therefore, CTC sequencing could help resolve the heterogeneity of tumors and provide precision medicine for patients.
Keywords: single circulating tumor cell, breast cancer, heterogeneity, whole genome sequencing, HER2 gene
Introduction
The incidence of women’s breast cancer is expanding quickly and ranks first, and morbidity trends are increasing, according to the most recent data on cancer in China and worldwide.1–4 The typical survival period after diagnosis of advanced breast cancer is two to three years. Only 5–10% of patients have a five-year survival rate.5
Various therapies are integrated based on the patient’s tumor condition to develop an efficient and comprehensive treatment approach.6 Targeted therapy is a widely used treatment option for patients who have significant immunohistochemical (3+) or immunofluorescence in situ hybridization (FISH)-confirmed expression of Her-2 (2+) in their tissue samples. Patients with HER2/Her-2 positive status have significantly improved results, potentially leading to currently available HER2-targeting medications.7 When selecting patients for targeted treatment, accurate and precise identification of this characteristic is essential. However, the IHC/FISH approach, primarily used to examine the Her-2 status on tissue, cannot indicate the precise gene status in the patient’s tumors since the HER2 gene status between primary and metastatic tumors may vary.
Highly active tumor cells called circulating tumor cells (CTCs), a liquid biopsy material, separate from solid tumors and enter the peripheral circulation. It has been reported that CTCs are linked to tumor metastasis and come from highly invasive malignancies.8 According to early research, CTCs are highly connected with the prognosis and survival of several solid tumors, including metastatic breast cancer,9 prostate cancer,10 and colorectal cancer.11 A recent study also demonstrated the use of CTC as a possible biomarker for patient classification and the selection of targeted therapies.12 Multiple tumor tissue samples are challenging to collect in advanced and metastasized malignancy. CTCs could be a good source of cancer cells for genetic research. The majority of genetic variations present in heterogeneous malignancies like breast cancer cannot be detected by tumor tissue sample analysis.13 There is evidence that molecular profiling of CTCs represents tumor variety more accurately than a single biopsy.14
Several gene variants in a single CTC may be studied using whole genome sequencing (WGS) technology.15,16 Our understanding of intra-tumor heterogeneity has dramatically increased with CTC separation and WGS technology, and the targeted and precise treatment of cancers has advanced.
In this current study, we compared the tumor pathologic outcomes of 3 breast cancer patients with the WGS data of CTCs obtained using CTC single-cell sequencing. We also examined the tumor heterogeneity, improved these patients’ therapy options, and achieved remarkable clinical outcomes.
Materials and Methods
Patients and Sample Collection
In this study, patients were enrolled and diagnosed at Shanghai Pudong Hospital. The Shanghai Pudong Hospital Ethics Committee was approved this study (No. W2001). We obtained written informed consent to allow the sample collection and data analysis for research purposes. Tumor tissue was collected after the surgery for the histopathological tests. For CTC analysis, 7.5 mL of peripheral blood was drawn from patients into the ACD anticoagulant tube. For ctDNA analysis, another 10 mL of peripheral blood was collected into an EDTA anticoagulant tube. Clinical characterizations of these patients are presented in Supplementary Table 1.
Immunohistochemistry and Fluorescence in-situ Hybridization
IHC staining of tumor tissues was performed on 4-μm sections using the standard procedure and VENTANA anti-HER2 /neu (4B5) Rabbit Monoclonal Primary Antibody (Roche Diagnostics, Basel, Switzerland). Standard protocols performed the experiments. At least three experienced pathologists independently evaluated all stained tumor section sits. Her-2 negative (IHC score equals 0 or 1+) and positive (IHC score equals 3+) were defined according to the IHC results. If the IHC score was 2+, then the FISH test was performed.
The HER2 gene amplification detection kit (Sinomdgene, Beijing, China) performed the FISH test following the corresponding manufacturer’s instructions. A 162 kb spectrum orange labeled fluorescent DNA probe specific for the HER2 gene and a 5.4 kb spectrum green-labeled chromosome enumeration probe (CEP17) were used. The results were generated according to the 2018 ASCO/CAP criteria.17
Investigation of CTCs
The CTC detection kit was used to perform the test (Majorbio, China). First, red blood cells were extracted using density gradient centrifugation after the plasma had been centrifuged. This technique combines immunofluorescence labeling, chromosomal in situ hybridization, and subtraction enrichment to separate and identify CTC.18
Antibody-coated magnetic beads were used to remove white blood cells with precision, and the remaining cells, including CTCs, were coated on a slide for further cell identification. Second, the multi-tumor immunofluorescence markers CD45 and Her-2 were used to label the cells on the slide. Fluorescence in situ hybridization was used to find the centromere of chromosome 8 (CEP8). Last but not least, CTCs were found using the criteria of CD45-, DAPI+, and CEP8 ≥3. The Her-2 expression was also recorded on the CTC surface.
Whole Genome Amplification and Sequencing of Single CTC
For subsequent CTC single cell WGS, a single CTC from each patient was microdissected using PALM MicroBeam equipment (Zeiss) and placed into a tube. Based on the multiple annealing and looping-based amplification cycles (MALBAC) technique, the single-cell whole genome sequencing kit (Yikon Genomics, China) was used to perform single-cell WGS.19 Followed by sequencing MALBAC at 25x mean sequencing depth, amplified DNA reaches 93% genome coverage ≥1x for a single CTC cell.19 The molecular weight of the amplified DNA product was examined using a Qubit® dsDNA HS Assay kit in a Qubit 3.0 Fluorometer (Life Technologies, USA), and the amplified DNA product’s genomic integrity was confirmed using quantitative PCR (qPCR) using eight randomly chosen loci. DNA samples were deemed to fulfill the further sequencing requirements if their overall mass was more than 2μg and their DNA fragment sizes ranging from 300 bp to 2000 bp.
Following the SureSelectXT Illumina Paired-End Sequencing Library procedure, the library was prepared. The 2100 Bioanalyzer and qPCR using TBS380 picogreen (Invitrogen, USA) were used to evaluate the quality of the library. Illumina’s Next Seq CN500 High-throughput Sequencer has been used to sequence the whole genomes of the captured single cells.
ctDNA Analysis of the Metastatic Patient
Using the QIAamp Circulating Nucleic Acid Kit (Qiagen, Germany), following the manufacturer’s instructions for ctDNA analysis, the plasma DNA of patient ID3 with metastatic breast cancer was collected for this investigation. The NGS technology investigated 67 cancer-related genes, including 57 drug-related genes, two endocrine therapy-related genes, and 9 chemotherapy-related genes. The complete list of alterations that were detected from the CTC and the ctDNA sequencing analysis is presented in Supplementary Tables S2–S5. We prepared the DNA libraries following the manufacturer’s suggested procedures. Typically, ctDNA fragments were hybridized with capture probes baits of the target areas, followed by hybrid selection using magnetic beads and 1% variant allelic frequency (VAF) for ctDNA of PCR amplification. Subsequently, 150 bp paired-end sequencing was performed on the Nextseq500 sequencer (Illumina, Inc., California, USA). Point mutations, small fragment insertions and deletions, copy number variants, and fusions of these genes were detected.
The human genome (hg19/GRCh37) was used to map the sequencing data. Variant calling and annotation were performed using MuTect, and VarScan. DNA Variants were filtered using the VarScan filter pipeline. Somatic variants were confirmed based on the Catalogue of Somatic Mutations in Cancer (COSMIC) database. The minimum confidence threshold for the variant was set to 0.05.
Results
CTC Enumeration of Breast Cancer Patients
All three patients had 24 enriched CTCs with chromosomal aneuploidy (Table 1 and Figure 1). For the three patients, there were 10, 7, and 7 CTCs in 7.5 mL of blood, respectively. The Her-2 expression on the membrane surface was not observed in any of these cells. Microdissection was used to isolate just one CTC per subject for the WGS analysis. Tetraploid cells came from patients ID2, whereas pentaploid cells came from patients ID1 and ID3. White blood cell pairs were employed as a control.
 |
Table 1 CTC Number Assessed for Each Patient Based on Chromosome Aneuploidy |
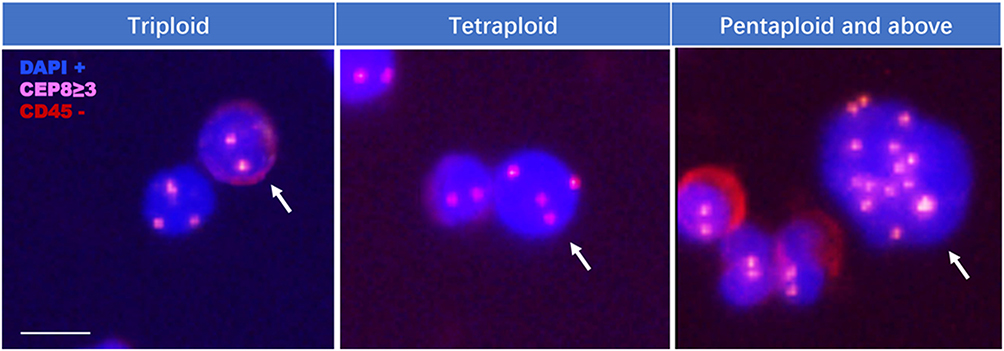 |
Figure 1 CTCs in patients with breast cancer. White arrows showed the identified CTCs. Scale bar is 10 μm. |
Somatic Mutation and CNV in CTCs
In the CTCs of the three patients, we found 2934, 497, and 2901 mutations, respectively. The COSMIC database documented around 20% of these mutations. In three patients, we also found 30, 8, and 39 breast cancer-related, and 174, 35, and 201 were found in chromosome 17, respectively (Table 2). In addition, TP53 R248W was found in-patient ID3, which was also found by the 57-panel in the patient’s ctDNA. In all three cases, there was HER2 amplification (Table 2). Additionally, patient ID3 had CNV increases of two additional drug-related genes (FGFR1 and FGFR2).
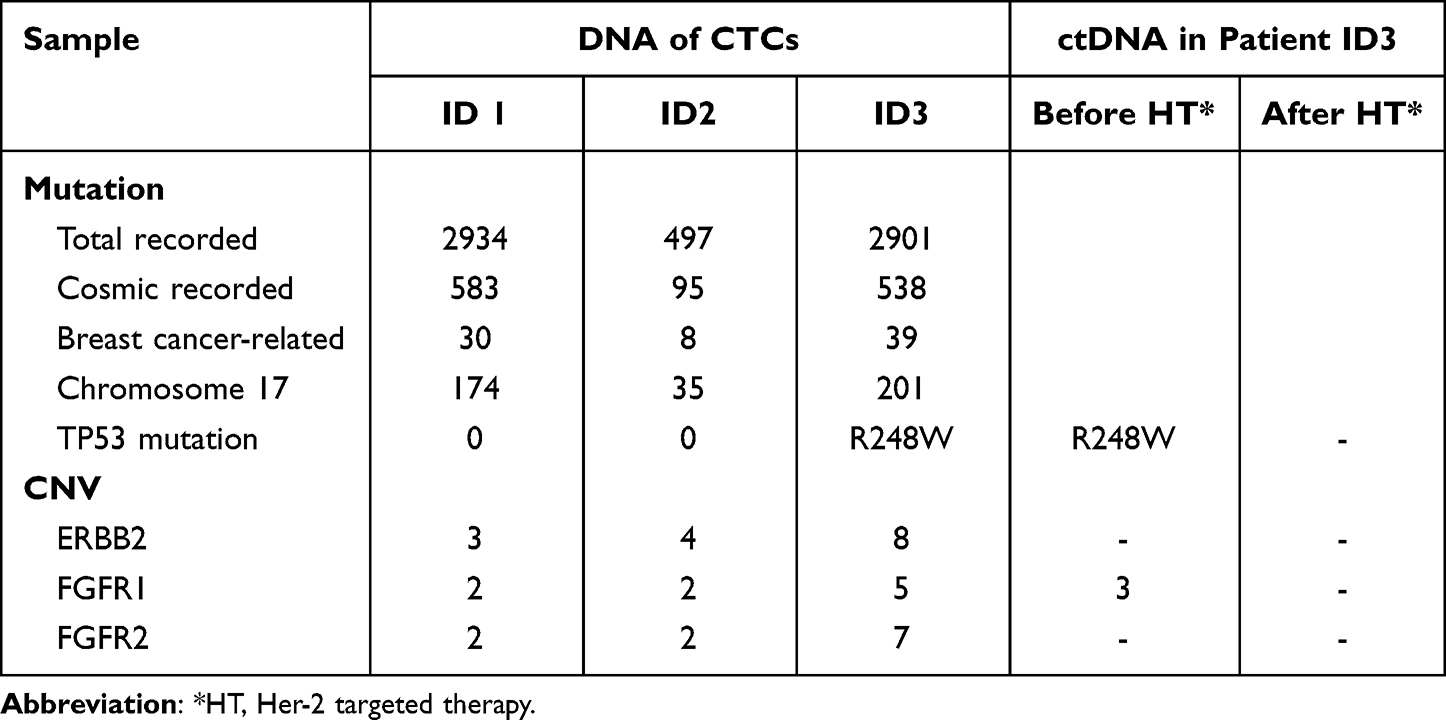 |
Table 2 DNA Status in CTCs and ctDNA of Patients with Breast Cancer |
Correlation Between HER2 Status and Patients’ Treatment
According to the WGS analysis of CTC, Patient ID1 with Her-2 protein expression in the tumor by IHC (Figure 2A) demonstrated HER2 gene amplification (Table 2). In October 2017, the first case of invasive breast cancer was identified. The patient received a mastectomy and six rounds of molecularly targeted chemotherapy called TCH (Paclitaxel-Carboplatin-Trastuzumab) every 21 days. Trastuzumab was used for a year. Hormone therapy is continuously used. Disease-free survival (DFS) has been attained for 18 months as of May 2019 (Figure 3).
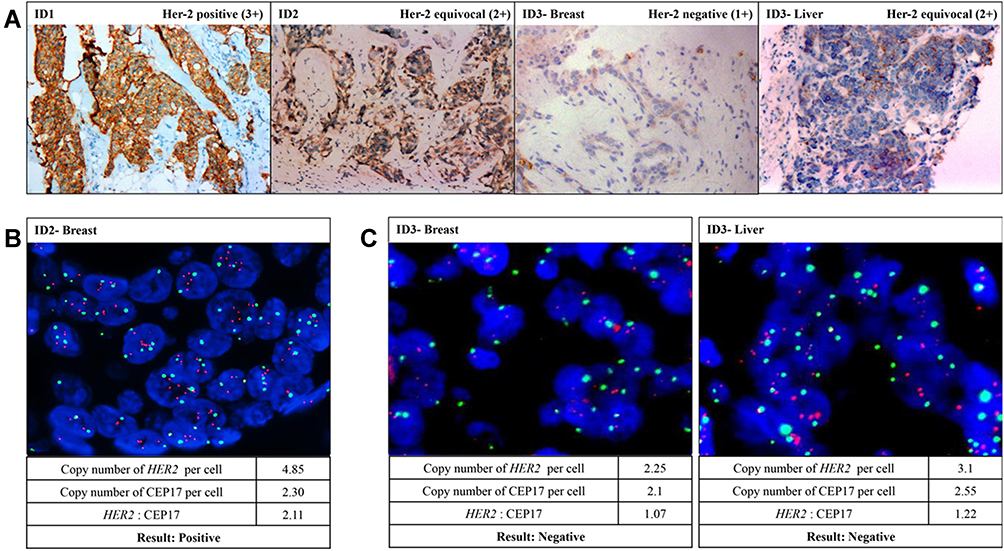 |
Figure 2 Her-2/HER2 status in the tissue of the 3 patients. (A) The Her-2 protein expression in the primary tissue of patient ID1, ID2, and ID3, and in the liver metastasis tissue of patient ID3 were detected by IHC test. (B) The copy number of HER2 gene in the tumor tissue of patient ID2 was detected by FISH test. (C) The copy number of HER2 gene in the primary and liver metastasis tissue of patient ID3 were detected by FISH test. |
 |
Figure 3 Clinical timelines of the 3 patients with breast cancer. The HER2 targeted drug trastuzumab were highlighted in bold type. DFS, disease-free survival; PFS, progression-free survival. |
Patient ID2 was found with Her-2 protein equivocal expression (2+) in the tumor by IHC (Figure 2A) and HER2 positive by FISH (Figure 2B). This patient also showed HER2 gene amplification in the WGS analysis of CTC (Table 2). In November 2017, invasive breast cancer was detected. Following a mastectomy, the patient underwent 4 cycles of an anthracycline with cyclophosphamide (AC) followed by 4 cycles of docetaxel coupled with trastuzumab (TH). Trastuzumab continued for a year. The continuously used endocrine therapy. Disease-free survival (DFS) reached 18 months after followed up to May 2019 (Figure 3).
IHC testing revealed that Patient ID3’s primary tumor had deficient (1+) Her-2 protein expression, making it Her-2 negative (Figure 2A). After that, a FISH test revealed that the initial tumor was Her-2 negative (Figure 2C). For the liver metastasis tumor of Patient ID3, equivocal expression (2+) of Her-2 protein was revealed by IHC test (Figure 2A) and Her-2 negative was reported by FISH test (Figure 2C), based on which this patient was evaluated as lack of benefit from the Her-2 targeted therapy. However, this patient’s WGS study of CTC revealed an amplification in the HER2 gene (Table 2). In November 2015, invasive breast cancer was identified. Before the mastectomy, docetaxel, epirubicin, and cyclophosphamide (TEC) neoadjuvant chemotherapy were carried out, and adjuvant chemotherapy and radiation were maintained following the operation. The patient then received endocrine treatment. Pleural effusion, peritoneal effusion, and numerous liver occupancies were noted in the patient in October 2017. The liver tissue biopsy revealed invasive adenocarcinoma, suggesting liver metastasis, although there were no cancer cells in the pleural effusion. The histological analysis indicated that the metastatic tissue lacked Her-2. The liver metastases decreased after paclitaxel and capecitabine therapy, and some tumor cells were found in the pleural effusion. Trastuzumab was added to the treatment plan in March 2018 when the pleural effusion dramatically increased. Compared to the effect of chemotherapy alone, partial tumor remission was significantly more clearly seen two months after the pleural effusion had dissipated. There is still endocrine treatment being used together with trastuzumab. An 18-month progression-free survival (PFS) was recorded for Patient ID3 until the manuscript was finished (Figures 3 and 4).
 |
Figure 4 Variations of imaging and molecular biomarker features in Patient ID3 during a series of medical treatments. Treatment process is showed in the top. Images of the lung (upper) and liver (lower) metastasis are listed in the middle. Variations of CTC (grey column) and ctDNA (black line for CNV of FGFR1; grey line for mutation of TP53 R248W) are presented in the bottom. |
Changes of CTC and ctDNA in Patient ID3 Before and After the Treatment
CTC test and ctDNA (57-gene panel) sequencing were performed at first diagnosis and after the trastuzumab-related treatment in-patient ID3 (Figure 4). At the first diagnosis, 7 CTCs/7.5 mL blood were identified, and a variation of TP53 R248W and amplification of FGFR1 was observed in the plasma. After the trastuzumab-related treatment, neither CTC in blood nor gene alteration in plasma was found in this patient (Table 2, Figures 3 and 4).
Discussion
Breast cancer is a disease that spreads rapidly, is exceedingly prevalent, and is also readily recurring. Accurate diagnosis and treatment of breast cancer is still a hot and challenging research point in recent years.20 Breast cancer tumors can be spatially and temporally heterogeneous, and distinct subpopulations of cancer cells can be found in various locations within a single patient’s tumors.21 CTCs are considered to have the same characteristics as primary or metastatic lesions.22 According to the previously reported studies,16,20,22 it is possible to undertake tumor medication based on the CTC genome’s features. The tumor genome heterogeneity and micrometastases may be discovered by whole genome sequencing of CTC. The results of the histological investigation (IHC and/or FISH tests) in our study were compatible with the genetic HER2 features of CTC in Patients ID1 and ID2, and the response to targeted treatment was as anticipated. The HER2 gene status of the CTC in Patient ID3 does not consistent with the tissue’s IHC or FISH test results. HER2-low, a new subtype classified as IHC 1+/2+ and FISH negative, coincides with patient ID3 in our study. The clinical benefits achieved by patient ID3 in this study could support the approval of HER2 inhibitors in this subgroup of patients, speculating that cancers may be treated using genetic characteristics of CTC.
TP53 and PIK3CA mutations, MYC, CCND1, and HER2 amplifications, as well as other essential leading mutations, are frequently seen in primary tumor cells.23,24 Some gene alterations identified by WGS analysis of CTC, like CNV gains of the HER2 gene in patients ID1 and ID2, are consistent with the result of IHC detection for tumor tissue. The results suggest that these modifications’ genesis might be the initial tumors. Further clonal diversity in primary or metastasizing cancers and treatment resistance may result from additional leading mutations or amplifications throughout the tumor evolution.25
Numerous investigations have revealed that the HER2 discordance rates between primary and metastatic or recurrent cancers are 8–16%, respectively.26–28 In our study, HER2 CNV gains were found in the DNA of CTC. Still, neither Her-2 protein expression nor HER2 gene amplification was observed in the primary tumor nor the liver metastasis tumor, demonstrating that HER2 CNV gains could be present in other metastatic tumors that had not yet been detected. Moreover, no HER2 alteration was detected in ctDNA, which implied that the potential metastasis was too tiny to be identified clinically. No tumor cell was discovered in the pleural effusion sample, even though increasing pleural effusion implied pulmonary metastasis. The heterogeneity of malignancies severely hampers the diagnosis and prognosis of illnesses. The heterogeneity of breast cancer mainly brings on many treatment failures. After treatment, patient ID3’s pleural effusion was continuously progressing. Trastuzumab is a potent target drug for HER2-positive breast cancer.29,30 However, this pleural abnormality was discharged, CTC was counted, and the mass of ctDNA in-patient ID3 was decreased after the first regimen combined with trastuzumab therapy. As a result, we speculatively assume that there may be lung micrometastases that have not been clinically identified. The possibility of lung metastasis in HER2-positive CTCs ultimately fails earlier treatment.
IHC and FISH assays, the examination of CTC membrane expression, or ctDNA sequencing did not reveal the presence of HER2-positive tumor tissues in the analysis of patient ID3. The HER2 gene amplification in CTC was only discovered by the WGS analysis. HER2 detection on tissues is commonly used as a criterion for targeting therapy in the clinic. However, the detection results are incorrect due to the heterogeneity of tumors and the defects of detection techniques.
The epithelial-mesenchymal transition makes detecting the expression of the Her-2 protein on CTC cell membranes difficult.31,32 The ctDNA test is constrained by the assay panel’s design, which makes the tumor signal dilution and eventual susceptibility to false-negative findings possible.33,34 Our results were consistent with other studies, suggesting that CTC sequencing can provide an alternative method for comprehensive genomic investigations to analyze tumor heterogeneity and identify the most effective therapy targets when conventional tissue samples are challenging to obtain.14,23
Compared to more traditional techniques like IHC and FISH, our findings demonstrate that WGS may be a reliable way to identify tumor heterogeneity. It may be used in place of IHC and FISH in standard clinical practice as a stand-alone diagnostic. As determined on unselected and heterogeneous patient groups and validated on additional external data, amplified DNA reaches 93% genome coverage ≥1x for a single CTC cell with a 25x mean sequencing depth, and we speculate that the technology is developed enough for prospective, multicenter, analytical, and clinical validation.
Limitation
A large sample of prospective control research will be required in the future because this is retrospective research with a small number of cases. Because single-cell sequencing was employed in this study, there is still room for improvement in whole genome sequencing, CTC identification, and single-cell separation. Single-cell technology has improved fast during the past two years. It can assess a large number of samples, improve clinical applications, improve detection precision, and cut expenses.
Conclusion
In this study, we have reported a patient with metastatic breast cancer with histopathologically negative tumor tissue but HER2 gene amplification in a single CTC by WGS. CTC sequencing helps us better understand the heterogeneity of breast cancer, enables non-invasive and repeated accurate monitoring of therapeutic response and tumor progression, and helps us in making therapeutic decisions and outcome prediction, which ultimately achieves personalized molecularly guided cancer treatment.
Data Sharing Statement
The datasets generated and/or analysed during the current study are available upon a reasonable request to the corresponding authors.
Ethical Statement
The Shanghai Pudong Hospital Ethics Committee was approved this study (No. W2001). The authors envisaged all standard protocols in accordance with the 1964 Declaration of Helsinki.
Acknowledgments
The study was supported by (1) Key specialty project of the Shanghai Pudong New Area Health and Family Planning Commission (PWZzk2017-32). (2) Funded by PDH-SPFDU Joint Research Fund (Project no. RHJJ2018-01). (3) Funded by Science and Technology Development Fund of Shanghai Pudong New Area (PKJ2019-Y28). (4) Funded by The construction project of the National Comprehensive Reform Pilot Zone for the Development of Traditional Chinese Medicine in Pudong New Area (PDZY-2021-0817). (5) The National Natural Science Foundation of China (No. 81672593, 81272899). We sincerely thank Dr. Ling Wang, Vascular and Endocrine Surgery Department, Xijing Hospital, Xi'an Fourth Military Medical University, China, for providing us with original samples, filling in clinical medical records and for his intellectual contributions during revising our manuscript.
Disclosure
All authors declare that they do not have conflicts of interest in this work.
References
1. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424. doi:10.3322/caac.21492
2. Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68:7–30. doi:10.3322/caac.21442
3. Chen W, Zheng R, Zhang S, et al. Cancer incidence and mortality in China, 2013. Cancer Lett. 2017;401:63–71. doi:10.1016/j.canlet.2017.04.024
4. Zheng R, Zeng H, Zhang S, Chen W. Estimates of cancer incidence and mortality in China, 2013. Chin J Cancer. 2017;36:66. doi:10.1186/s40880-017-0234-3
5. Huober J, Thurlimann B. The role of combination chemotherapy in the treatment of patients with metastatic breast cancer. Breast Care. 2009;4:367–372. doi:10.1159/000262808
6. Curigliano G, Burstein HJ, Winer EP, et al. De-escalating and escalating treatments for early-stage breast cancer: the St. Gallen international expert consensus conference on the primary therapy of early breast cancer 2017. Ann Oncol. 2017;28(8):1700–1712. doi:10.1093/annonc/mdx308
7. Bartsch R, Bergen E. ASCO 2018: highlights in HER2-positive metastatic breast cancer. Memo. 2018;11:280–283. doi:10.1007/s12254-018-0441-x
8. Lianidou ES, Strati A, Markou A. Circulating tumor cells as promising novel biomarkers in solid cancers. Critical Reviews in Clinical Laboratory Sciences. 2014;51:160–171. doi:10.3109/10408363.2014.896316
9. Cristofanilli M, Budd GT, Ellis MJ, et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N Engl J Med. 2004;351:781–791. doi:10.1056/NEJMoa040766
10. de Bono JS, Scher HI, Montgomery RB, et al. Circulating tumor cells predict survival benefit from treatment in metastatic castration-resistant prostate cancer. Clin Cancer Res. 2008;14:6302–6309. doi:10.1158/1078-0432.CCR-08-0872
11. Cohen SJ, Punt CJ, Iannotti N, et al. Relationship of circulating tumor cells to tumor response, progression-free survival, and overall survival in patients with metastatic colorectal cancer. J Clin Oncol. 2008;26:3213–3221. doi:10.1200/JCO.2007.15.8923
12. Lee JS, Magbanua MJM, Park JW. Circulating tumor cells in breast cancer: applications in personalized medicine. Breast Cancer Res Treat. 2016;160:411–424. doi:10.1007/s10549-016-4014-6
13. Kim C, Paik S. Gene-expression-based prognostic assays for breast cancer. Nat Rev Clin Oncol. 2010;7:340–347. doi:10.1038/nrclinonc.2010.61
14. Lohr JG, Adalsteinsson VA, Cibulskis K, et al. Whole-exome sequencing of circulating tumor cells provides a window into metastatic prostate cancer. Nat Biotechnol. 2014;32:479–484. doi:10.1038/nbt.2892
15. Katsios C, Roukos DH. Individual genomes and personalized medicine: life diversity and complexity. Per Med. 2010;7:347–350. doi:10.2217/pme.10.30
16. Gulbahce N, Magbanua MJM, Chin R, et al. Quantitative whole genome sequencing of circulating tumor cells enables personalized combination therapy of metastatic cancer. Cancer Res. 2017;77:4530–4541. doi:10.1158/0008-5472.CAN-17-0688
17. Wolff AC, Hammond MEH, Allison KH, et al. Human epidermal growth factor receptor 2 testing in breast cancer: American society of clinical oncology/college of American pathologists clinical practice guideline focused update. J Clin Oncol. 2018;36:2105–2122. doi:10.1200/JCO.2018.77.8738
18. Lin PP. Integrated EpCAM-independent subtraction enrichment and iFISH strategies to detect and classify disseminated and circulating tumors cells. Clin Transl Med. 2015;4:38. doi:10.1186/s40169-015-0081-2
19. Zong C, Lu S, Chapman AR, Xie XS. Genome-wide detection of single-nucleotide and copy-number variations of a single human cell. Science. 2012;338:1622–1626. doi:10.1126/science.1229164
20. Joseph C, Papadaki A, Althobiti M, Alsaleem M, Aleskandarany MA, Rakha EA. Breast cancer intratumour heterogeneity: current status and clinical implications. Histopathol. 2018;73:717–731. doi:10.1111/his.13642
21. Navin N, Krasnitz A, Rodgers L, et al. Inferring tumor progression from genomic heterogeneity. Genome Res. 2010;20:68–80. doi:10.1101/gr.099622.109
22. Brouwer A, De Laere B, Peeters D, et al. Evaluation and consequences of heterogeneity in the circulating tumor cell compartment. Oncotarget. 2016;7:48625–48643. doi:10.18632/oncotarget.8015
23. Stephens PJ, Tarpey PS, Davies H, et al. The landscape of cancer genes and mutational processes in breast cancer. Nature. 2012;486:400–404. doi:10.1038/nature11017
24. Nik-Zainal S, Van Loo P, Wedge DC, et al. The life history of 21 breast cancers. Cell. 2012;149:994–1007. doi:10.1016/j.cell.2012.04.023
25. Almendro V, Kim HJ, Cheng YK, et al. Genetic and phenotypic diversity in breast tumor metastases. Cancer Res. 2014;74:1338–1348. doi:10.1158/0008-5472.CAN-13-2357-T
26. Amir E, Miller N, Geddie W, et al. Prospective study evaluating the impact of tissue confirmation of metastatic disease in patients with breast cancer. J Clin Oncol. 2012;30:587–592. doi:10.1200/JCO.2010.33.5232
27. Niikura N, Liu J, Hayashi N, et al. Loss of human epidermal growth factor receptor 2 (HER2) expression in metastatic sites of HER2-overexpressing primary breast tumors. J Clin Oncol. 2012;30:593–599. doi:10.1200/JCO.2010.33.8889
28. Lindström LS, Karlsson E, Wilking UM, et al. Clinically used breast cancer markers such as estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2 are unstable throughout tumor progression. Journal of Clinical Oncology. 2012;30:2601–2608. doi:10.1200/JCO.2011.37.2482
29. Singer CF, Balmaña J, Bürki N, et al. Genetic counselling and testing of susceptibility genes for therapeutic decision-making in breast cancer-an European consensus statement and expert recommendations. European Journal of Cancer. 2019;106:54–60. doi:10.1016/j.ejca.2018.10.007
30. Howie LJ, Scher NS, Amiri-Kordestani L, et al. FDA approval summary: pertuzumab for adjuvant treatment of HER2-positive early breast cancer. Clinical Cancer Research. 2018;2018:3003.
31. Guan X, Ma F, Li C, et al. The prognostic and therapeutic implications of circulating tumor cell phenotype detection based on epithelial-mesenchymal transition markers in the first-line chemotherapy of HER2-negative metastatic breast cancer. Cancer Commun. 2019;39:1. doi:10.1186/s40880-018-0346-4
32. Papadaki MA, Stoupis G, Theodoropoulos PA, Mavroudis D, Georgoulias V, Agelaki S. Circulating tumor cells with stemness and epithelial-to-mesenchymal transition features are chemoresistant and predictive of poor outcome in metastatic breast cancer. Mol Cancer Ther. 2019;18(2):437–447. doi:10.1158/1535-7163.MCT-18-0584
33. Clark TA, Chung JH, Kennedy M, et al. Analytical validation of a hybrid capture-based next-generation sequencing clinical assay for genomic profiling of cell-free circulating tumor DNA. J Mol Diagn. 2018;20:686–702. doi:10.1016/j.jmoldx.2018.05.004
34. Lanman RB, Mortimer SA, Zill OA, et al. Analytical and clinical validation of a digital sequencing panel for quantitative, highly accurate evaluation of cell-free circulating tumor DNA. PLoS One. 2015;10:e0140712. doi:10.1371/journal.pone.0140712
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Heterogeneity Assessment of Breast Cancer Tumor Microenvironment: Multiparametric Quantitative Analysis with DCE-MRI and Discovery of Radiomics Biomarkers
Ma W, Yang L, Zhang Y, Gao Y, Jie H, Huang C
Breast Cancer: Targets and Therapy 2025, 17:573-581
Published Date: 8 July 2025