Back to Journals » Neuropsychiatric Disease and Treatment » Volume 22
White Matter Integrity in General Paresis: An Exploratory Tract-Based Spatial Statistical Analysis
Authors Chen H, Li S, Xing YX, Xie RM, Xue M, Li JJ
Received 13 October 2025
Accepted for publication 28 January 2026
Published 19 February 2026 Volume 2026:22 569932
DOI https://doi.org/10.2147/NDT.S569932
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Hui Chen,1,* Shuo Li,1,* Yu-Xue Xing,1 Ru-Ming Xie,1 Ming Xue,1 Jing-Jing Li2,3
1Department of Radiology, Beijing Ditan Hospital, Capital Medical University, National Center for Infectious Diseases(Beijing), Beijing, People’s Republic of China; 2Department of Radiology, Beijing Ditan Hospital, Xuzhou Hospital, Capital Medical University, Xuzhou, People’s Republic of China; 3Department of Radiology, Xuzhou Infectious Diseases Hospital, Xuzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jing-Jing Li, Email [email protected]
Purpose: The white matter integrity and fine structure changes were rarely reported in General Paresis (GP). We discussed white matter (WM) integrity in GP patients which was analyzed by Diffusion Tensor Imaging (DTI) Tract-Based Spatial Statistical Analysis (TBSS).
Patients and Methods: This was a prospective cross-sectional study. We recruited 18 GP patients and 24 age-sex-matched healthy controls (HC). DTI for WM of whole-brain was analyzed by TBSS and got of fractional anisotropy (FA), mean diffusivity (MD), axial diffusivity (AD) and radial diffusivity (RD), local diffusion homogeneity (Spearman) (LDHs), and local diffusion homogeneity (Kendall) (LDHk). The results of WM tracts with statistical difference between GP and HC groups were analyzed with Mini-Mental State Examination (MMSE) using Pearson correlation. All correlations were statistically tested with a significant p-value < 0.05.
Results: GP patients had significantly reduced FA and increased AD, RD, and MD in a wide range of WM. On DTI-TBSS comparison the mean FA decreased in forceps minor (FCP), inferior fronto-occipital fasciculus R (IFOF_R), superior longitudinal fasciculus (temporal part) L (SLFTP_L). MD increased in cingulum (hippocampus) R (Ch_R), FCPm, IFOF_L, IFOF_R, inferior longitudinal fasciculus L (ILF_L), ILF_R, superior longitudinal fasciculus_L (SLF_L), SLF_R, uncinate fasciculus L (UF_L), UF_R and SLFTP_R. AD increased in Ch_R, ILF_L, UF_L. RD increased in FCPm, IFOF_L, IFOF_R, ILF_L, ILF_R, UF_L, UF_R, SLFTP_R. LDHs decreased in anterior thalamic radiation L (ATR_L), cingulum (cingulate gyrus) L (CCG_L). LDHk decreased in ATR_L, CCG_L. The MMSE score correlated with FA (positive correlation) and MD (negative correlation) in FCPm and IFOF_R. The MMSE score correlated with LDHs (positive correlation) and LDHk (positive correlation) in ART_L.
Conclusion: These findings suggest that DTI-TBSS is a sensitive tool for detecting widespread white matter impairment in GP, and that the identified microstructural damage is closely associated with core cognitive deficits in memory and speech, which may inform early diagnosis and monitoring of disease progression.
Keywords: neurosyphilis, dementia, general paresis, magnetic resonance imaging, diffusion tensor imaging
Introduction
With the incidence of syphilis more than doubling over the last decade, understanding of its clinical and imaging manifestations has become increasingly important.1 Neurosyphilis can occur at any time in the course of syphilis, even in the earliest primary stage.2 General paresis (GP) is a late stage of neurosyphilis with rapid progressive dementia and personality changes.2,3 Unfortunately, GP has a wide variety of central nervous system manifestations, both clinical or neuroimaging findings,4 which makes the diagnosis challenging.1 Dementia related to GP is one of the dementia that can be cured at present. Therefore, early diagnosis and early treatment are crucial for its prognosis.
It is reported that the most common imaging manifestation of GP is brain atrophy, especially frontal temporal lobe and hippocampus.4–6 But can these brain atrophy explain severe dementia and mental disorders? Is cognitive impairment associated with the destruction of white matter (WM) integrity? Tract-based spatial statistics (TBSS) was used to observe whether WM integrity was related with underlying cognitive impairment by analyzing diffusion tensor imaging (DTI). Several prior studies have employed DTI to investigate brain microstructural changes in neurosyphilis and HIV-dementia. Studies revealed that disrupted white matter microstructural integrity and spontaneous brain activity were observed in early neurosyphilis using DTI-TBSS.7 DTI-TBSS was helpful to explore the WM microstructure abnormalities and provide a new perspective for the investigation of the pathomechanism of HIV-associated WM injury.8 DTI is recommended as a sensitive method to explore the changes of brain WM. TBSS is a reliable and optimized method, which is unbiased and automatic, which can be used to comprehensively understand WM fiber damage across the entire brain. The extent of the changes in the microstructure of major WM tracts was investigated by TBSS. We got the diffusion metrics fractional anisotropy (FA), mean diffusivity (MD), axial diffusivity (AD), radial diffusivity (RD), local diffusion homogeneity (Spearman) (LDHs) and local diffusion homogeneity (Kendall) (LDHk). Mini-Mental State Examination (MMSE) analysis by Pearson correlation was performed for WM regions with statistically significant difference between GP group and HC group. LDHs and LDHk are as advanced techniques that provide more specific estimates of axonal density and myelination, respectively. We state that their application in GP could offer deeper mechanistic insights beyond standard DTI. How white matter microstructural signature relate to cognitive profiles remains largely unexplored in GP. This directly sets up the rationale for our study. However, white matter integrity in GP may be influenced by concurrent factors such as age, vascular risk burden, or treatment history, which must be considered when interpreting the results. We will increase the sample size for group discussions in the future.
Materials and Methods
Participants
This was a prospective cross-sectional study. The study was approved by the ethics committee (2018(044)-01 and DTEK-KY2025-139-01), and all the included patients had signed informed consent.
Eighteen male patients with GP (age 50.95±12.76 years, range = 21~68 years) and 24 male age-matched healthy controls (age 52.42±9.22 years, range = 28~67 years) were involved in this study. All of the participants were right-handed and were voluntarily and consecutively recruited from Mar 2018 to Sep 2019.
Clinical symptoms and signs in GP group include memory impairment (11/18), emotion disorder (11/18), speech impairment (5/18), hallucination (4/18), unstable gait (4/18), dizziness (3/18) and Numbness of limbs (2/18).
All participants were given MMSE score. GP group scores were 20.61±7.51, while HC group scores were 29.58±0.65.
The inclusion and exclusion criteria of GP groups refer to the 2015 Center for Disease Control (CDC) states neurosyphilis guidelines:9 (1) Treponema pallidum particle assay (TPPA) was positive, or rapid plasma reagent (RPR) was positive, and Toluidine red un-hoated serum test (TRUST) were positive. (2) There were neurological symptoms and signs; (3) Cerebrospinal fluid (CSF) TRUST test was positive, white blood cells >5/μL or CSF protein > 45mg/dl. (4) CSF ink staining, cryptococcal antigen, acid fast staining, toxoplasma antibody were all negative, excluding diseases caused by other pathogenic microorganisms.
The inclusion and exclusion criteria of HC group refer to no neurological symptoms and disease.
Imaging Examination
General Electric Company (GE) Discovery MR750W 3.0 T was used for MR examination. Multidirectional (axial, sagittal, coronal) scanning and multiparameter scanning were performed, including conventional MR T1WI, T2WI, DTI and T1-weighted 3D axial IR-prepped FSPGR (BRAVO). The DTI sequence parameters were: TR 7000ms, TE 97.9ms, b=1000, matrix 128 × 128, FOV 240 mm × 240mm, Directions 15. BRAVO T1WI in axis orientation yielding contiguous slices with thickness of 1.0 mm. The in-plane spatial resolution of the contiguous coronal slices was 0.5×0.5×1mm /pixel. Field of view = 256 mm × 256 mm and matrix size = 512 × 512, flip angle = 15◦, TR = 7.472 ms, and TE = 2.796ms, TI=450ms.
Image Analysis
DTI data were processed using the FMRIB Software Library (https://fsl.fmrib.ox.ac.uk/fsl/fslwiki) software.
- Diffusion Tensor Imaging Data Processing. Data Conversion and Preprocessing: Raw DICOM images were converted to the NIFTI format. Preprocessing included correction for susceptibility-induced distortions, followed by correction for eddy currents and head motion. A brain mask was generated from the non-diffusion weighted (b0) image of each participant using the Brain Extraction Tool (BET). Tensor Fitting and Scalar Maps: A diffusion tensor model was fitted at each voxel within the brain mask using FSL’s tool. This generated individual maps of FA, MD, AD, RD, LDHs and LDHk.
- TBSS Analysis. Registration and Skeleton Creation: All participants’ FA images were nonlinearly registered to the standard FMRIB58_FA template in Montreal Neurological Institute (MNI) space using FNIRT. The registered FA images were averaged and thinned to create a mean FA skeleton, representing the centers of common white matter tracts. The skeleton was thresholded at FA ≥ 0.2 to exclude peripheral areas with high inter-subject variability or partial volume effects. Projection of Diffusion Metrics: Each participant’s aligned FA data were projected onto this common skeleton. The voxelwise group comparisons were performed using FSL’s randomise tool with 5000 permutations. Threshold-Free Cluster Enhancement (TFCE) was applied to address the multiple comparisons problem across the white matter skeleton. Results are reported as statistically significant at a family-wise error (FWE) corrected p value <0.05. The identical nonlinear warps and projection parameters were then applied to the FA, MD, AD, RD creating analogous skeletonized data for subsequent group analysis.
Local Diffusion Homogeneity (Spearman-based), LDHs: This index was calculated by evaluating the similarity of diffusion-weighted signal profiles within a local neighborhood using Spearman’s rank correlation coefficient. For each voxel, the signal intensities of its adjacent voxels were ranked, and the Spearman correlation between the central voxel’s rank vector and each neighbor’s was computed. The LDHs value was defined as the average of these correlation coefficients within the neighborhood. Local Diffusion Homogeneity (Kendall-based). LDHk: This index was derived following an identical spatial process but using Kendall’s tau coefficient as the similarity metric. The LDHk value represents the average Kendall’s tau correlation within the neighborhood. Both LDHs and LDHk range from −1 to 1, with higher positive values indicating greater local pattern uniformity. A 6-mm spherical kernel was used to define the neighborhood for all calculations.
Statistical Analysis
Independent samples t-test was performed for age and MMSE. TBSS analyses were performed using TBSS Statistics, as previously mentioned. The results of WM tracts with statistical difference between GP and HC groups were analyzed with MMSE by Pearson correlation coefficient (IBM SPSS Statistics 22.0 for Windows). p value<0.05 was regarded as statistical significance.
Result
Clinical Data
There was no significant difference in age and gender between GP and HC groups, but MMSE was statistically significant (P < 0.05).
DTI-TBSS Comparison
Widespread whiter matter disruption in GP, as shown in Table 1 and Figures 1–6.
- FA value in GP group was significant decreased than HC group in forceps minor (FCPm) (p=0.03), inferior fronto-occipital fasciculus R (IFOF_R) (p=0.04), and superior longitudinal fasciculus (temporal part) L (SLFTP_L) (p=0.04) regions.
- MD increased in cingulum (hippocampus) R (Ch_R) (p=0.04), FCPm (p=0.01), IFOF_L (p=0.01), IFOF_R (p=0.03), inferior longitudinal fasciculus L (ILF_L) (p=0.02), ILF_R (p=0.04), superior longitudinal fasciculus_L (SLF_L) (p=0.03), SLF_R (p=0.03), uncinate fasciculus L (UF_L) (p<0.01), UF_R (p=0.04) and SLFTP_R (p=0.02) regions.
- AD increased in Ch_R(p=0.01), ILF_L(p=0.04), UF_L(p<0.01) regions.
- RD increased in FCPm (p=0.01), IFOF_L (p=0.041), IFOF_R (p=0.01), ILF_L (p=0.01), ILF_R(p=0.02), UF_L (p=0.048), UF_R (p=0.04), SLFTP_R(p=0.02) regions.
- LDHs decreased in anterior thalamic radiation L(ATR_L)(p=0.045) and cingulum (cingulate gyrus) L (CCG_L) (p<0.01) regions.
- LDHk decreased in ATR_L (p=0.048), CCG_L (p<0.01) regions.
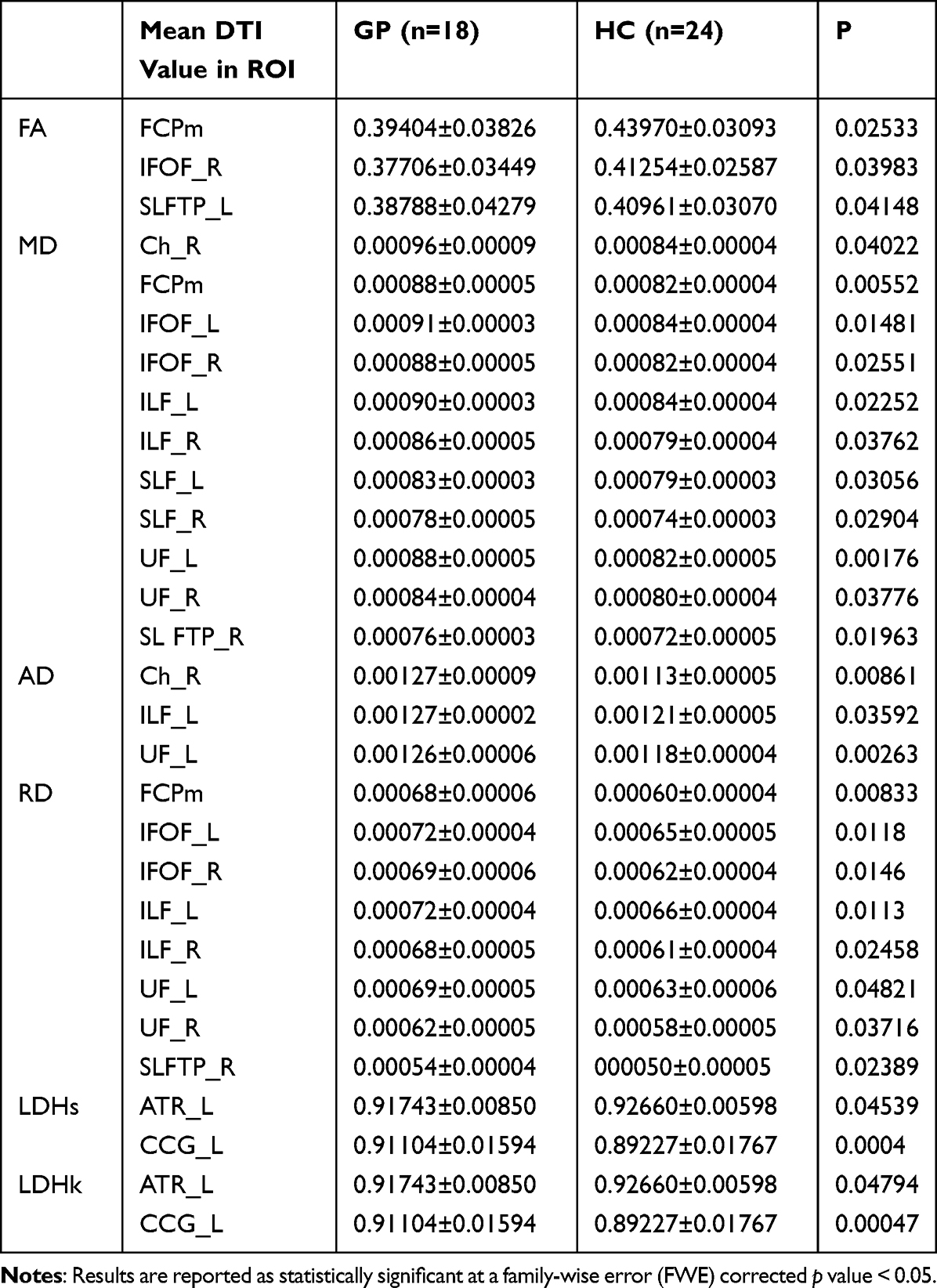 |
Table 1 The Difference Between the GP and HC Group in Mean DTI Value |
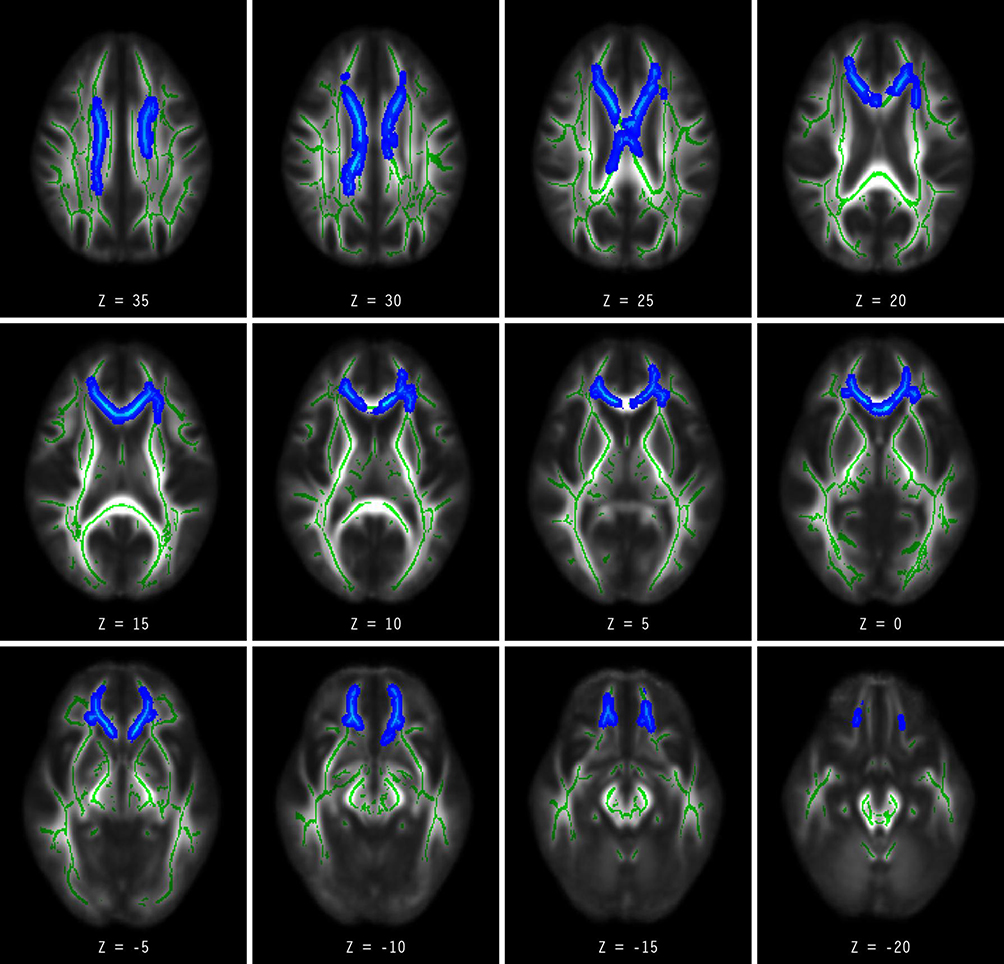 |
Figure 1 Showed FA value in GP group was significant decreased than HC group in FCPm, IFOF_R, and SLFTP_L regions. Notes: The statistical maps are overlaid on the mean FA skeleton. The color coding indicates the direction of group differences: blue denotes voxels with decreased values. The Threshold-Free Cluster Enhancement (TFCE) method was employed. Results for all metrics are reported as statistically significant at a family-wise error (FWE) corrected threshold of p value <0.05. |
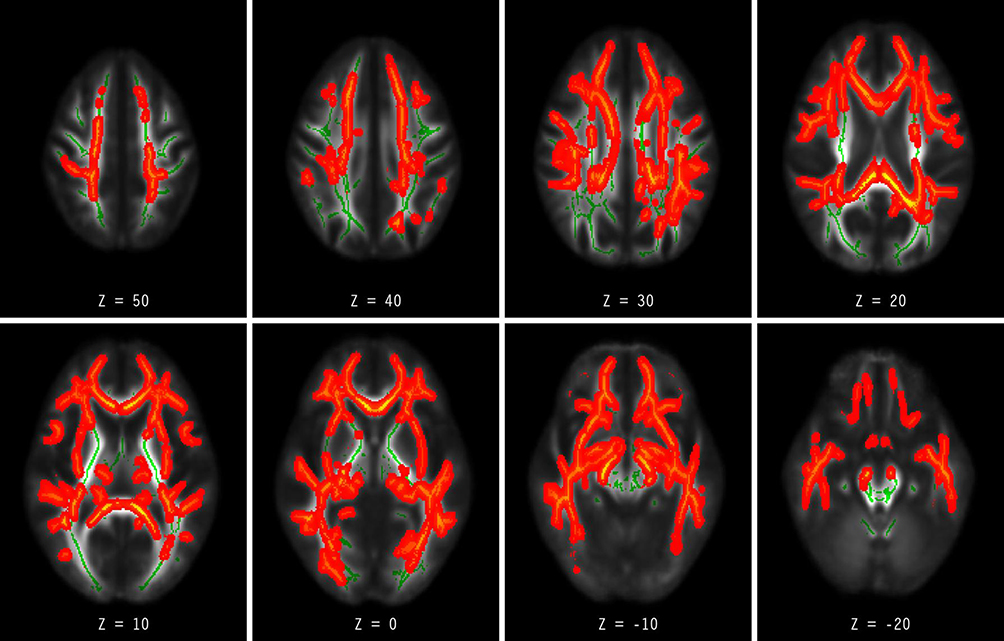 |
Figure 2 Showed MD increased in Ch_R, FCPm, IFOF_L, IFOF_R, ILF_L, ILF_R, SLF_L, SLF_R, UF_L, UF_R and SLFTP_R regions. Notes: The statistical maps are overlaid on the mean FA skeleton. The color coding indicates the direction of group differences: red denotes voxels with increased values in the GP group relative to controls. The Threshold-Free Cluster Enhancement (TFCE) method was employed. Results for all metrics are reported as statistically significant at a family-wise error (FWE) corrected threshold of p value <0.05. |
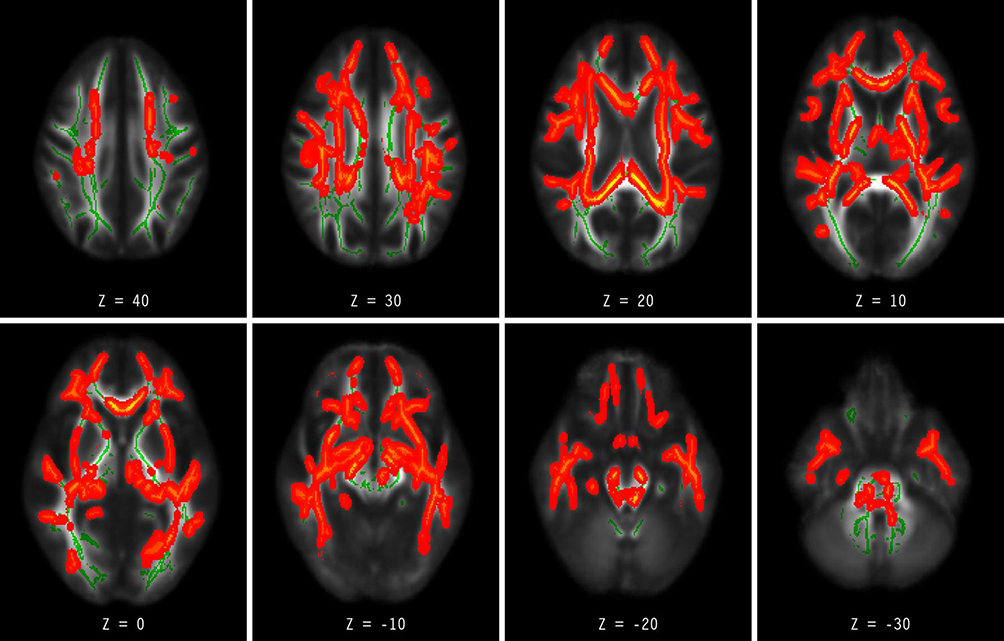 |
Figure 3 Showed AD increased in Ch_R, ILF_L, UF_L regions. The statistical maps are overlaid on the mean FA skeleton. Notes: The statistical maps are overlaid on the mean FA skeleton. The color coding indicates the direction of group differences: red denotes voxels with increased values in the GP group relative to controls. The Threshold-Free Cluster Enhancement (TFCE) method was employed. Results for all metrics are reported as statistically significant at a family-wise error (FWE) corrected threshold of p value <0.05. |
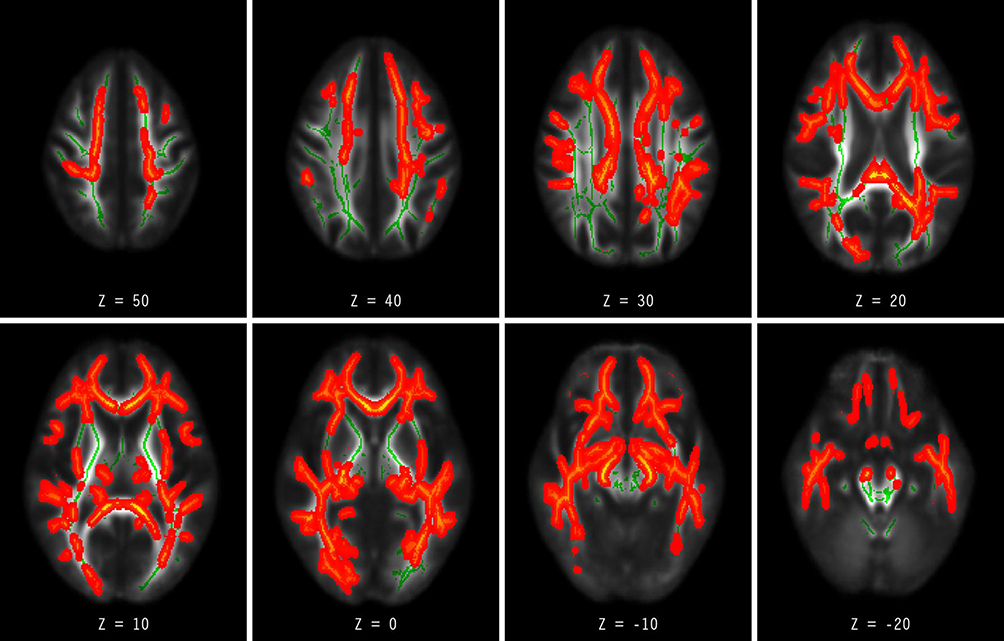 |
Figure 4 Showed RD increased in FCPm, IFOF_L, IFOF_R, ILF_L, ILF_R, UF_L, UF_R, SLFTP_R regions. Notes: The statistical maps are overlaid on the mean FA skeleton. The color coding indicates the direction of group differences: red denotes voxels with increased values in the GP group relative to controls. The Threshold-Free Cluster Enhancement (TFCE) method was employed. Results for all metrics are reported as statistically significant at a family-wise error (FWE) corrected threshold of p value <0.05. |
 |
Figure 5 Showed LDHs decreased in ATR_L, CCG_L regions. Notes: The statistical maps are overlaid on the mean FA skeleton. The color coding indicates the direction of group differences: blue denotes voxels with decreased values. The Threshold-Free Cluster Enhancement (TFCE) method was employed. Results for all metrics are reported as statistically significant at a family-wise error (FWE) corrected threshold of p value <0.05. |
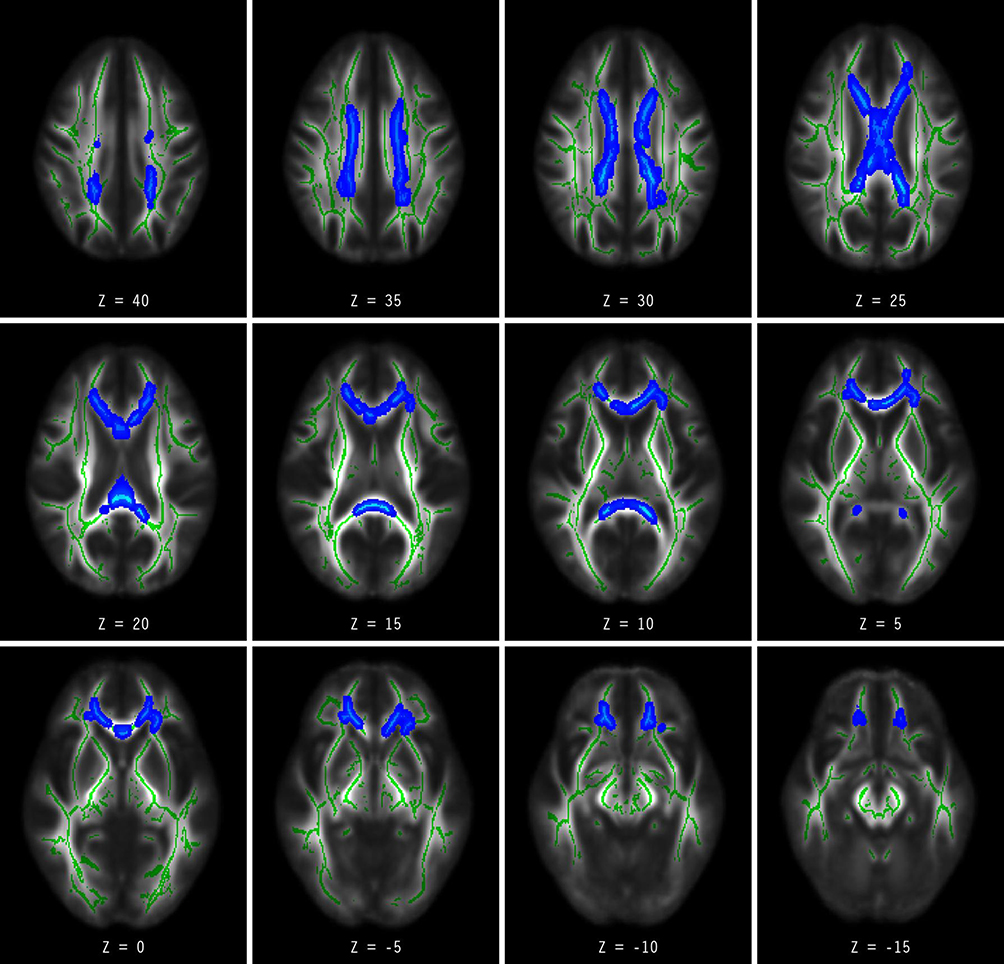 |
Figure 6 Showed LDHk decreased in ATR_L, CCG_L regions. Notes: The statistical maps are overlaid on the mean FA skeleton. The color coding indicates the direction of group differences: blue denotes voxels with decreased values. The Threshold-Free Cluster Enhancement (TFCE) method was employed. Results for all metrics are reported as statistically significant at a family-wise error (FWE) corrected threshold of p value <0.05. |
Table 1, Comparison of Mean DTI Values between Groups.
Correlations Between WM and MMSE Scores
The difference between the two groups of diffusion metric and MMSE correlation was analyzed by Pension correlation, as shown in Table 2.
- FA was positively correlated with MMSE in FCPm region (p<0.01, r=0.52).
- MD was a negative correlation between MMSE in FCPm (p=0.03, r=−0.51), IFOF_R (p=0.047, r=−0.47). There was no significant difference between GP group and HC group in ART_L region, but it was negatively correlated with MMSE (p=0.01, r=−0.58).
- LDHs in ART_ L region (p=0.01, r=0.57) was correlated with MMSE.
- LDHk in ART_ L region (p=0.01, r=0.57) was correlated with MMSE.
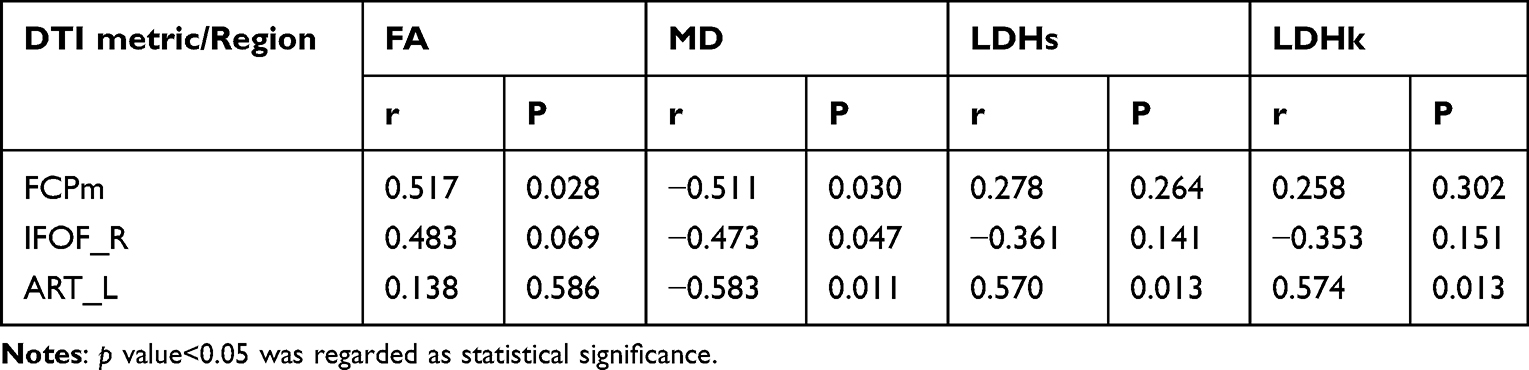 |
Table 2 The Difference Between the Two Groups of Diffusion Metric and MMSE Correlation Analyzed by Pearson Correlation Coefficient |
Discussion
In our study, DTI analysis by TBSS was used in GP and NC groups. It demonstrated preliminary results of altered widespread microstructural WM abnormalities in GP. DTI can detect microstructural integrity of white matter fiber by quantitative assessment in brain disorders. We used the voxel-wise TBSS to find that decreased FA/LDHs/LDHk values and increased MD/RD/AD values throughout almost the whole WM skeleton of GP patients. This is consistent with the research conducted by scholar Ma WT,7 in early neurosyphilis DTI-TBSS revealed that decreased FA and increased MD values in the FCPm, Ch_R and Ch_L, IFOF_R, ILF, corticospinal tract, CCG_R, and anterior thalamic radiation. Increased MD or AD values in multiple white matter structures showed significant associations with many cognitive domain tests. Research showed increased MD or AD values in multiple white matter structures and associated with many cognitive domain tests in HIV patients8,10. Currently, the mechanisms underlying WM pathology in GP are unclear. The clinical symptom of GP was progressive dementia with or without psychological and behavior disorders.2,11 Therefore, the author discussed the DTI results of other cognitive disorders (Alzheimer’s disease). FA represented the integrity of nerve fibers and reflected WM tract damage and MD represented reduced barriers to free water diffusion. The combination of reduced FA and increased MD may reflect the progressive loss of intensity of WM. There was a wide alteration of WM microstructure in early Alzheimer’s disease12 and Parkinson’s disease.13 Some scholars found that increased AD and RD in WM tracts, suggesting lesion-related axonal damage and demyelination contributing to WM impairment.14 Gong proposed LDH as an additional marker for evaluating the WM microstructural properties of the brain.15 This metric quantifies the local coherence of water molecule diffusion in a model-free manner. LDH is used to characterize the local coherence of water molecule diffusion in a model-free manner. It may provide additional insights into inter-subject WM variability. In calculation, the LDH parameter uses Spearman correlation coefficient (LDHs) or Kendall harmony coefficient (LDHk) to quantify the overall coherence of diffusion series. In GP LDHs and LDHk decreased in ART_L and CCG_L. That was consistent with other studies that decreased FA and LDH in patients correlate with vascular cognitive impairment.16,17
Some scholars found that WM damage may occur secondarily to grey matter atrophy by Wallerian degeneration, but additional WM alterations may also occur independent.18 Neuropathology also indicated that perivascular inflammation was present in the leptomeninges, cortex, and white matter in GP. We hypothesized that this progressive dementia in GP is not only because of damage of cortical architecture and neuron loss, but also related to the alterations of white matter integrity. We speculated that the decrease of FA/LDHs/LDHk and the increase of MD/AD and RD in GP patients may be related to the loss of myelin and axon damage from microvascular pathology.19 It is currently unknown whether microstructural changes with WM can be detected earlier than GM volumetric changes. Thus, future work should focus on both grey and WM of GP.
GP has a wide range of WM tracts integrity in the whole brain. Including ATR in project fibers. In this group, two cases of limb numbness may be related to the damage of white matter integrity. Commissural fibers: Corpus callosum (CC) (FCPm). The CC has the greatest volume of white matter in the brain, and it connects both brain hemispheres. Damage to the anterior portion (FCPm) caused frontal symptomatology, including disinhibition, impulsivity, memory issues, inertness, and decreased motivation.20 In our study, GP patients who had memory and emotional disorders and hallucinations may be related to the abnormal WM of corpus callosum. Cognition Association fibers: IFOF, ILF, SLF, UF were damaged in our study. The damage of those WM may cause speech and memory impairment. In our study, five patients had speech impairment, 11 patients had memory impairment.
We also found these WM tract abnormalities were associated with cognitive function in GP. MMSE score was correlated significantly with FA (positive correlation) in FCPm, as well as MD in FCPm, IFOF_R (negative correlation) in the WM tracts. LDHs and LDHk in ART_ L region were also correlated with MMSE. This is similar with the results of AD, MCI and vascular cognitive impairment,20 which confirmed that FA and LDH was positive correlation and MD was negative correlation with MMSE or Montreal Cognitive Assessment (MoCA).
Researchers from Japan detected T. pallidum in the CSF of 28.6% patients with primary and secondary syphilis.2,3,21 Parenchymatous neurosyphilis (NS) is characterized by general paresis and tabes dorsalis. In early neurosyphilis DTI-TBSS revealed that decreased FA and increased MD in WM and associated with many cognitive domain tests.7 GP is a late stage NS caused by the direct invasion of brain parenchyma by spirochetes. Selective atrophy of the frontal and mesial temporal structures has been recognized as a feature of the GP. But GP had no specificity in clinic and MRI. Diagnosis and differential diagnosis of GP is a big clinical challenge.4,22 Our study found that WM tracts integrity was widely abnormal in GP patients and correlated with MMSE. When MMSE score was high, FA value was high and MD value was low for FCPm area, which indicated that fiber bundle integrity was good in this region. It was consistent with mild clinical symptoms. When MMSE score was high, MD value was low in IFOF region, and LDHs and LDHk values in the region were high, which indicated that WM traces were not damaged in the regions. And those were supported by clinical manifestations. The extensive alterations of WM tracts can better explain the clinical symptoms of GP. Noting that the discussion focuses on significant results to generate hypotheses, but that alterations in tracts without cognitive correlations may also be biologically important and require future study. The conclusions imply that white matter damage may explain clinical symptoms. But the relationships may be bidirectional or influenced by shared underlying factors. Expanding cognitive assessment beyond global screening (eg, MMSE) to include tests like the MoCA, AVLT, and WMS are necessary to clarify associations with specific cognitive domains. Will DTI-TBSS change before and after the treatment of syphilis? Early diagnosis and treatment of NS can delay the progression of the disease. Can DTI-TBSS be used to assess the severity of the disease and the therapeutic effect? Further research is needed.
Limitations: The number of cases and the sample size were relatively small, so more cases are needed to continue the discussion. At the same time, the abnormal gray matter volume and WM tracts may reveal the pathological process of the disease. The next step we should study on asymptomatic neurosyphilis and perform long-term follow-up on patients with NS to find DTI-TBSS whether it would help with earlier diagnosis or monitoring treatment response.
Conclusion
GP had extensive alterations in WM integrity. The damage to the WM tracts may explain the clinical features, such as neuropsychological symptoms, impulsivity, language and memory disorders. DTI might be a potential biomarker for identifying the underlying mechanisms of GP. A larger sample size needs to be studied further.
Highlights
- We discussed white matter (WM) integrity in GP patients which was analyzed by Diffusion Tensor Imaging (DTI) Tract-Based Spatial Statistical Analysis (TBSS).
- GP patients had significantly reduced FA, and increased AD, RD, and MD in a wide range of WM.
- DTI could be established as a potentially biomarker to detect underlying mechanisms of GP.
Abbreviations
DTI, Diffusion Tensor Imaging; TBSS, Tract-Based Spatial Statistical Analysis; GP, General Paresis; HC, Healthy Controls; MRI, Magnetic Resonance Imaging; WM, White Matter; FA, Fractional Anisotropy; MD, Mean Diffusivity; AD, Axial Diffusivity; RD, Radial Diffusivity; LDHs, Local Diffusion Homogeneity; LDHk, Local Diffusion Homogeneity; MMSE, Mini-Mental State Examination; TPPA, Treponema Pallidum Particle Asset; RPR, Rapid Plasma Reagent; TRUST, Toluidine Red Unheated Serum Test; CSF, Cerebrospinal Fluid; FCPm, Forceps Minor; IFOF_R, Inferior Fronto-occipital Fasciculus R; SLFTP_L, Superior Longitudinal Fasciculus; Ch_R, Cingulum (hippocampus) R; ILF_L, Inferior Longitudinal Fasciculus L; SLF_L, Superior Longitudinal Fasciculus_L; UF_L, Uncinate Fasciculus L; ATR_L, Anterior Thalamic Radiation L; CCG_L, Cingulum (cingulate gyrus) L.
Data Sharing Statement
The datasets used during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
All procedures of this study were performed in accordance with the Declaration of Helsinki and were approved by Ethics Committee of Beijing Ditan Hospital (approval No. 2018-No.0044-01 and No. DTEC-KY2025-139-01). All participants gave written informed consent prior to taking part in this study.
Acknowledgments
We appreciate the help on English Language editing by AJE. An unauthorized version of the Chinese MMSE was used by the study team without permission, however this has now been rectified with PAR. The MMSE is a copyrighted instrument and may not be used or reproduced in whole or in part, in any form or language, or by any means without written permission of PAR (www.parinc.com).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work is supported by Beijing Ditan Hospital, Xuzhou Hospital, Capital Medical University, Special Program for Clinical Research and Scientific Innovation Transformation (KCZL202504).
Disclosure
Hui Chen and Shuo Li are co-first authors for this study. The authors declare that they have no conflicts of interest in this work.
References
1. Ropper AH. Neurosyphilis. N Engl J Med. 2019;381(14):1358–13. doi:10.1056/NEJMra1906228
2. Hamill MM, Ghanem KG, Tuddenham S. State-of-the-art review: neurosyphilis. Clin Infect Dis. 2024;78(5):e57–e68. doi:10.1093/cid/ciad437
3. Ha T, Tadi P, Leslie SW, Dubensky L. Neurosyphilis. In: StatPearls. StatPearls Publishing; 2024.
4. Faraut E, Wallon D, Gueit E, et al. MRI findings in a case of Lissauer form of neurosyphilis. Acta Neurol Belg. 2018;118(1):113–114. doi:10.1007/s13760-017-0833-4
5. Chen H, Li JJ, Guan CS, et al. Investigation of gray matter changes using voxel-based morphometry in HIV-negative patients with general paresis of the insane. Neuropsychiatr Dis Treat. 2024;20:2529–2539. doi:10.2147/NDT.S484214
6. Liu H, Dong D. MRI of neurosyphilis with mesiotemporal lobe lesions of “knife-cut sign” on MRI: a case report and literature review. Heliyon. 2023;9(4):e14787. doi:10.1016/j.heliyon.2023.e14787
7. Ma WT, Yao SJ, Cao Y, et al. Altered white matter microstructure and cerebral spontaneous activity in early neurosyphilis without human immunodeficiency virus infection. J Comput Assist Tomogr. 2025;49(5):825–832. doi:10.1097/RCT.0000000000001743
8. Li RL, Sun J, Tang ZC, Zhang JJ, Li HJ. Axonal chronic injury in treatment-naïve HIV+ adults with asymptomatic neurocognitive impairment and its relationship with clinical variables and cognitive status. BMC Neurol. 2018;18(1):66. doi:10.1186/s12883-018-1069-5
9. Tuddenham S, Ghanem KG. Management of Adult Syphilis: key Questions to Inform the 2021 Centers for Disease Control and Prevention Sexually Transmitted Infections Treatment Guidelines. Clin Infect Dis. 2022;74(suppl 2):S127–S133. doi:10.1093/cid/ciac060
10. Su T, Caan MW, Wit FW, et al. AGEhIV Cohort Study. White matter structure alterations in HIV-1-infected men with sustained suppression of viraemia on treatment. AIDS. 2016;30(2):311–322. doi:10.1097/QAD.0000000000000945
11. Gao JH, Li WR, Xu DM, et al. Clinical manifestations, fluid changes and neuroimaging alterations in patients with general paresis of the insane. Neuropsychiatr Dis Treat. 2021;17:69–78. doi:10.2147/NDT.S279265
12. Tranfa M, Lorenzini L, Collij LE, et al. Alzheimer’s disease and small vessel disease differentially affect white matter microstructure. Ann Clin Transl Neurol. 2024;11(6):1541–1556.13. doi:10.1002/acn3.52071
13. Sang T, He J, Wang J, et al. Alterations in white matter fiber in Parkinson disease across different cognitive stages. Neurosci Lett. 2022;769:136424. doi:10.1016/j.neulet.2021.136424
14. Mascalchi M, Salvadori E, Toschi N, et al. VMCI-Tuscany study group. DTI-derived indexes of brain WM correlate with cognitive performance in vascular MCI and small-vessel disease. A TBSS study. Brain Imaging Behav. 2019;13(3):594–602.
15. Zhang Y, Zhan F. Diffusion tensor imaging (DTI) analysis based on tract-based spatial statistics (TBSS) and classification using multi-metric in Alzheimer’s disease. J Integr Neurosci. 2023;22(4):101
16. Tang X, Chen Y, Tan H, et al. Micro- and macro-changes in early-stage type 2 diabetes mellitus without cognitive impairment: a diffusion tensor imaging (DTI) and surface-based morphometry (SBM) study. Front Neurol. 2023;14:1115634. doi:10.3389/fneur.2023.1115634
17. Liu L, Huang Q, Yang S, et al. Micro-structural white matter abnormalities and cognitive impairment in asymptomatic carotid plaque patients: a DTI study using TBSS analysis. Clin Neurol Neurosurg. 2020;197:106096. doi:10.1016/j.clineuro.2020.106096
18. Nagai Y, Fujimura T, Uchida W, et al. Gray matter microstructure alterations with excess extra-cellular free water contribute to cognitive dysfunction in bipolar disorder: a comparative analysis with white matter pathology. Neuroimage. 2025;317:121342. doi:10.1016/j.neuroimage.2025.121342
19. Li L, Yang W, Wan Y, et al. White matter alterations in mild cognitive impairment revealed by meta-analysis of diffusion tensor imaging using tract-based spatial statistics. Brain Imaging Behav. 2023;17(6):639–651. doi:10.1007/s11682-023-00791-5
20. Bertrand E, van Duinkerken E, Laks J, et al. Structural gray and white matter correlates of awareness in Alzheimer’s disease. J Alzheimers Dis. 2021;81(3):1321–1330. doi:10.3233/JAD-201246
21. Wang RZ, Chen SF, Fei CJ, et al. Clinical, radiological, pathological and prognostic features of general paresis: a cohort study. Brain. 2025;148(8):2763–2771. doi:10.1093/brain/awae389
22. Pastuszak M, Kwaśny A, Czarnowska-Cubała M, Kwaśna J. Comment on:”Imaging features of neurosyphilis”. J Neuroradio. 2023;50(5):502. doi:10.1016/j.neurad.2023.05.003
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Gut Microbiota Alternation in Disease Progression of Neurosyphilis
Wang G, Zou D, Lu X, Gu X, Cheng Y, Qi T, Cheng Y, Yu J, Ye M, Zhou P
Infection and Drug Resistance 2022, 15:6603-6612
Published Date: 14 November 2022
Clinical and Laboratory Characteristics, Neuroimaging Alternations and Treatment Response of 25 HIV-Negative General Paresis Patients
Liu M, Tong M, Zhou J, Lan Y, Wu M, Zhang H, Leng L, Zheng H, Li Y, Li M, Li J
Infection and Drug Resistance 2023, 16:6931-6939
Published Date: 30 October 2023
Investigation of Gray Matter Changes Using Voxel-Based Morphometry in HIV-Negative Patients with General Paresis of the Insane
Chen H, Li JJ, Guan CS, Xue M, Xing YX, Xie RM
Neuropsychiatric Disease and Treatment 2024, 20:2529-2539
Published Date: 14 December 2024
Multimodal Magnetic Resonance Findings in Parkinson’s Disease With “Antecedent Essential Tremor”: A Case Series of a Large Kindred
Kong Y, Yao L, Xiao X, Chen A, Wang K, Yan H, Sun R, Liu R, Kong Q
Neuropsychiatric Disease and Treatment 2025, 21:79-92
Published Date: 22 January 2025