Back to Journals » Clinical Interventions in Aging » Volume 17
White-Cell Derived Inflammatory Biomarkers in Prediction of Postoperative Delirium in Elderly Patients Undergoing Surgery for Lower Limb Fracture Under Non-General Anaesthesia
Authors Li X, Wang G, He Y, Wang Z, Zhang M ![]()
Received 30 October 2021
Accepted for publication 23 March 2022
Published 5 April 2022 Volume 2022:17 Pages 383—392
DOI https://doi.org/10.2147/CIA.S346954
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Xiaowei Li,1,2 Gongming Wang,2 Yingxue He,2 Zhun Wang,1 Mengyuan Zhang1,2
1Department of Anesthesiology, Shandong Provincial Hospital, Cheeloo College of Medicine, Shandong University, Jinan, Shandong, 250021, People’s Republic of China; 2Department of Anesthesiology, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan, Shandong, 250021, People’s Republic of China
Correspondence: Mengyuan Zhang, Department of Anesthesiology, Shandong Provincial Hospital, Cheeloo College of Medicine, Shandong University, Jinan, Shandong, 250021, People’s Republic of China, Tel +8668776472, Email [email protected]
Purpose: The aim of this study was to investigate whether white-cell derived biomarkers could serve as potential markers in prediction of postoperative delirium (POD) after lower limb fracture.
Patients and Methods: Elderly patients with surgery for lower limb fracture under non-general anaesthesia were included. Neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and platelet-to-white cell ratio (PWR), which were most recently measured preceding surgery and measured within 24h after surgery, were calculated. Delirium was measured with Confusion Assessment Method (CAM) once daily from preoperative day 1 to postoperative day 3 or hospital discharge.
Results: The incidence of POD was 32.6% (60/184). Between patients with and those without POD, there were significant differences in preoperative hematological biomarkers (neutrophil count, lymphocyte count, NLR and PWR) and postoperative hematological biomarkers (white cell count, neutrophil count, lymphocyte count, NLR, PLR and PWR). More obvious changes before and after operation for NLR, PLR and C-reactive protein (CRP) were found in patients with POD. Multivariate logistic regression showed that benzodiazepines (OR, 7.912; 95% CI, 1.884– 33.230; p = 0.005), change of CRP (OR, 1.017; 95% CI, 1.007– 1.027; p = 0.001) and postoperative NLR (OR, 1.358; 95% CI, 1.012– 1.823; p = 0.041) were associated with POD. When the changes of NLR, PLR and PWR entered multivariate logistic regression, older age (OR, 1.073; 95% CI, 1.001– 1.149; p = 0.046), benzodiazepines (OR, 6.811; 95% CI, 1.652– 28.081; p = 0.008), greater change of CRP (OR, 1.015; 95% CI, 1.006– 1.023; p = 0.001) and greater change of NLR (OR, 1.266; 95% CI, 1.035– 1.549; p = 0.022) were associated with increased risk of POD. Postoperative NLR had high accuracy to predict POD with area under curve (AUC) of 0.790 (95% CI 0.708 to 0.872).
Conclusion: Age, benzodiazepines, postoperative NLR, change of NLR and change of CRP were independent predictable markers for POD in elderly patients undergoing surgery for lower limb fracture under non-general anaesthesia. Early postoperative NLR may help to recognize POD as soon as possible.
Keywords: postoperative delirium, anaesthesia method, inflammation, neutrophil-to-lymphocyte ratio, lower limb fracture
Introduction
Postoperative delirium (POD) is a common complication after major surgery, especially in elderly patients and can cause significant short- or long-term adverse outcomes.1 There is a growing body of evidence suggesting that inflammation and oxidative stress may play critical roles in the pathophysiology of POD.2 Several inflammatory markers in serum or cerebrospinal fluid have been found to be associated with POD.3 However, it is expensive and time-consuming to conduct testing for these markers such as IL-6, IL-8, S-100β, which limits their clinical application. Markers of inflammation derived from white cell count, namely neutrophil-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and platelet-to-white cell ratio (PWR) are readily to obtain without additional financial burden. Some studies have shown their potential prognostic value in prediction of delirium after head and neck free-flap reconstruction, total hip arthroplasty, abdominal surgery, esophagectomy, carotid endarterectomy and cardiac Surgery.4–9
The incidence of POD in elderly patients undergoing operation of lower limb fracture is high.5,10 Although the effect of anaesthesia method on POD is controversial, general anesthesia is not the first choice for these patients in clinical practice due to high requirement for cardiopulmonary function, unstable haemodynamics, and complicated anaesthetic management.10–12 It is noteworthy that previous studies payed more attention to the relationship between markers of inflammation derived from the white cell count and POD after general anaesthesia.5 In this study, patients who accepted surgery for lower limb fracture under non-general anaesthesia were chosen. We performed this prospective observational study to investigate whether the panel of white-cell derived biomarkers before and after the operation could serve as potential markers in prediction of delirium.
Materials and Methods
Patients
Patients who underwent operation for lower limb fracture at Shandong Provincial Hospital from November 2020 to August 2021 were eligible for this study. The exclusion criteria were: 1) age<65 years old; 2) general anesthesia; 3) preoperative delirium; 4) a preoperative Mini-Mental State Examination (MMSE) score lower than 24;13 5) psychiatric disease; 6) patients managed in intensive care units after surgery; 7) patient refusal. This study was approved by the Institutional Review Board (SWYX: NO.2021–010) and conducted in accordance with the Helsinki Declaration. Informed consent was obtained from all study participants before surgery.
Data Collection
Patients’ details such as age, gender, body mass index, degree of education and comorbidity were obtained by preoperative visit. Severity of comorbidities was calculated using the age adjusted Charlson Comorbidity Index (ACCI).14 Laboratory data, including hematocrit, white cell count, neutrophil count, lymphocyte count, platelet, and C-reactive protein (CRP) level, most recently measured preceding surgery and measured within 24h after surgery were collected. Surgery information, including operative site, operation time, anesthesia method, intraoperative medication, and hemorrhage volume, were recorded. Application of anti-inflammatory agents within 24h before surgery, during surgery and within 24h after surgery was also collected. We also collected the application of benzodiazepines and anticholinergic drugs within 48h before and after surgery. NLR was calculated as the neutrophil count divided by the lymphocyte count. PLR was calculated as the platelet count divided by the lymphocyte count, and PWR was calculated as the platelet count divided by the total white cell count.
Outcomes
The primary outcome was the incidence of postoperative delirium. Delirium was measured with the Confusion Assessment Method (CAM) once daily from preoperative day 1 to postoperative day 3 or hospital discharge.15 Assessment contains four evaluation criteria: acute onset and fluctuating course, inattention, disorganized thinking, and altered level of consciousness. The CAM algorithm for diagnosis of delirium requires the presence of both the first and the second criteria and of either the third or the fourth criterion. The CAM is reliable and has been found to be consistent with the DSM-IV diagnostic criteria for delirium. CAM assessments were supplemented with medical record review, and family/nursing staff interview. All assessments were completed in the general ward.
Sample Size
When studying the relationship between white-cell derived inflammatory biomarkers and POD, NLR was most frequently mentioned, so we chose data of preoperative NLR, postoperative NLR, and change of NLR to calculate sample size. Sample size calculation of this study was based on the preliminary results for the first 100 patients. For elderly patients, incidence of delirium after surgery for lower limb fracture ever reported in the literature varied from 15% to 70%. During sample size calculation, we chose a relatively low incidence of 25%. With the ratio of patients being approximately 1:3, a total of 168, 84, or 88 patients was needed to have a power of 90% using a two-side proportion test with an alpha level of 0.05 for preoperative NLR, postoperative NLR, or change of NLR respectively.
Statistical Analysis
Continuous data were expressed as the mean ± SD and categorical data were expressed as the count. Student t-test or non-parametric test was used to compare continuous variables according to the normality test. Chi-squared test or Fisher’s exact test was used to compare the proportions of the categorical variables. We used tolerance and variance inflation factor to check for multicollinearity among the variables. Multivariate logistic regression analysis was used to assess independent predictors. Variables were selected for inclusion in multivariate logistic regression analyses based on a p value cut-off of 0.1 in univariate analyses. NLRs, PLRs and PWRs were included as explanatory variables regardless of their P value. Omnibus test of model coefficients was used to verify whether the regression analysis equation was meaningful. Hosmer and Lemeshow test was used to test the degree of fitting. Receiver operating characteristic (ROC) curve was used to evaluate the accuracy of POD prediction. Statistical analyses were performed using SPSS Statistics version 21.0 (IBM Corp., Armonk, NY, USA) and PASS 15.0 (NCSS, LLC. Kaysville, Utah, USA). P value<0.05 was regarded as statistically significant.
Results
Of 349 patients undergoing operation for lower limb fracture, 184 patients were finally included in this analysis. Exclusion criteria were outlined in Figure 1. The mean age was 76.15±7.94 (65–95) years and female accounted for 60.9% of the total. 80 (43.5%) participants had any education beyond primary school. The incidence of POD in our study was 32.6% (60/184).
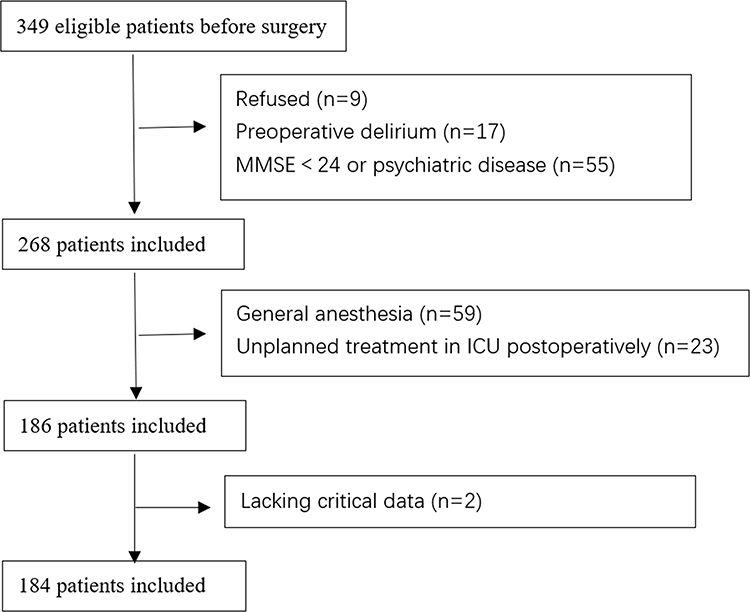 |
Figure 1 Study flowchart. |
Patients with POD showed significantly older age, higher percentage of stroke history and more blood loss than those without POD (Table 1). POD was more prevalent among patients with fracture of femur than other sites (femur vs tibiofibular, p= 0.030; femur vs others, p=0.001; tibiofibular vs others, p=0.256). Perioperative use of benzodiazepines was significantly associated with POD. Between patients with and those without POD, there were significant differences in preoperative hematological biomarkers (neutrophil count, lymphocyte count, NLR and PWR) and postoperative hematological biomarkers (white cell count, neutrophil count, lymphocyte count, NLR, PLR and PWR) (Table 2). More obvious changes before and after operation for NLR, PLR and CRP were found in patients with POD (Table 2).
 |
Table 1 Summary of Patient Characteristics and Perioperative Data, Stratified by Postoperative Delirium Status |
 |
Table 2 Laboratory Data for Patients with and without Postoperative Delirium |
Results of collinearity analyses showed serious collinearity among hematological biomarkers. Details were listed in Supplementary Tables 1 and 2. NLR, PLR and PWR were calculated using white cell count, neutrophil count, lymphocyte count and platelet count. Changes of NLR, PLR and PWR were calculated using preoperative and postoperative values of NLR, PLR and PWR. Considering the clinical practice and the purpose of this study, we eliminated perioperative values of white cell count, neutrophil count, lymphocyte count and platelet count in multivariate logistic regression analyses, and then included perioperative values of NLR, PLR and PWR, and their changes in separate multivariate logistic regression analyses. No obvious collinearity was found among variables in multivariate logistic regression analyses (Supplementary Table 3). Results from multivariate logistic regression (Model 1 adjusted for age, incidence of stroke, operation site, operation time, blood loss, benzodiazepines, change of CRP before and after operation, preoperative NLR, preoperative PLR, preoperative PWR, postoperative NLR, postoperative PLR and postoperative PWR) showed that benzodiazepines, change of CRP and postoperative NLR were associated with POD occurrence (Table 3). P value of Hosmer and Lemeshow test was 0.435. When the changes of NLR, PLR and PWR before and after operation entered multivariate logistic regression (Model 2 adjusted for age, incidence of stroke, operation site, operation time, blood loss, benzodiazepines, and change of CRP before and after operation), older age, benzodiazepines, greater change of CRP and greater change of NLR were associated with increased risk of POD (Table 3). P value of Hosmer and Lemeshow test was 0.392. Omnibus test of model coefficients showed both model 1 and model 2 regression analysis equations were meaningful.
 |
Table 3 Multivariate Logistic Regression Analysis for Selected Perioperative Parameters Predicting Delirium |
Table 4 showed the ROC analyses for age, the change of CRP, postoperative NLR, the change of NLR, model 1 and model 2. For a single variable, postoperative NLR had high accuracy to predict POD with Area Under Curve (AUC) of 0.790 (95% CI 0.708 to 0.872), followed closely by the change of NLR with AUC of 0.770 (95% CI 0.684 to 0.856). The AUCs of model 1 and model 2 were 0.846 (95% CI 0.781–0.911) and 0.849 (95% CI 0.787–0.911), respectively. The optimal cut-off values of age, the change of CRP, postoperative NLR, the change of NLR, model 1 and model 2 were found by Youden Index. Corresponding values of sensitivity and specificity were listed in Table 4. Sensitivity and specificity of benzodiazepines obtained by calculation were 0.217 and 0.952 respectively.
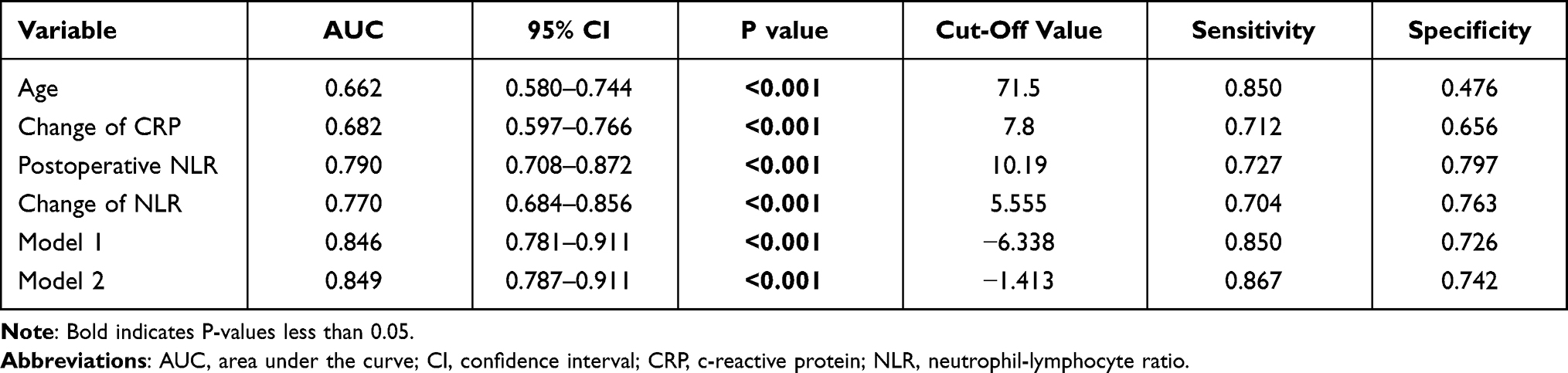 |
Table 4 Receiver Operating Characteristic Analysis of Associated Factors to Predict Postoperative Delirium |
Discussion
Chronic stress induced by trauma, surgery and anaesthesia often nonspecifically activates immune systems characterized by an increase in neutrophils count and a decrease in lymphocyte count, along with a decrease in platelet count in peripheral circulation.16–18 This activation may involve hypercortisolism, disruption of the blood-brain barrier, microglia activating and release of cerebral cytokines, which may contribute to the pathophysiology of delirium.18,19 Peripheral inflammatory markers have been found to significantly elevate in patients with delirium.17 Accumulating studies have proven the concentrations of CRP, IL-6, IL-8 and S-100β in peripheral circulation are indeed correlated with POD.3,20,21 However, their use in clinical practice is precluded by price and the difficulty of the diagnostic process. White-cell derived inflammatory biomarkers including NLR, PLR as well as PWR are easily available markers of generalized inflammation reported in different research settings.22–24 Recent studies found that preoperative NLR can be a predictive factor for POD after head and neck free-flap reconstruction, total hip arthroplasty, esophagectomy, and carotid endarterectomy.4,5,7,9 In this study, both preoperative NLR and postoperative NLR were higher in patients with POD after lower limb fracture than those in patients without POD. Multivariate analyses revealed that among the hematological biomarkers examined, postoperative NLR was still associated with the development of POD. Preoperative NLR was not an independent risk factor for POD in this study. Some of this can be attributed to the exclusion of patients with preoperative delirium, as some relative studies did not include this exclusion criteria.4,7,9 In addition, change of NLR (postoperative value− preoperative value) in the POD group was significantly higher than that in the non-POD group and was positive value, which meant that NLR in patients with POD increased significantly after surgery. This result may indicate more severe systemic inflammation and neuroinflammation caused by surgery and anaesthesia in patients with POD.
Lower preoperative PLR was ever reported to be associated with the development of POD after cardiac surgery and abdominal surgery,6,8 while another study reported high PLR values in patients with delirium in the intensive care unit.25 In our results, although patients with POD had higher postoperative PLR, perioperative PLR showed no statistically significant difference in multivariate analysis. Both platelet and lymphocyte decrease during nonspecific activation of the immune system. Influenced by various factors such as the amount of blood loss, infectious or aseptic inflammation, and so on, their magnitudes of decrease are different. This may be the reason that different studies did not get consistent results. Besides, previous studies reported lower PWR was an independent risk factor for delirium after acute ischemic stroke, cardiac surgery, and abdominal surgery.6,8,26,27 Our results also showed patients with POD had lower preoperative PWR and postoperative PWR, which was consistent with previous studies. No statistical difference in multivariate analyses may be due to the limitation of sample size.
CRP is a marker of nonspecific acute-phase response in inflammation, infection, and tissue damage.28 Recently, a meta-analysis summarized the relationship between CRP and POD.3 Results showed a high level of CRP, whether preoperative or postoperative, was a risk factor for the development of POD. However, the current study observed no statistically significant difference between patients with or those without POD in respect of preoperative or postoperative CRP level. It was noteworthy that postoperative CRP value in the delirium group was found to increase significantly compared to preoperative value, which was consistent with the change of NLR.
In addition, it is commonly recognized that incidence of POD increases with age, as pathophysiological changes induced by advanced age cause hypersensitivity to stimuli to which they are normally insensitive.29 Our study also showed similar results. We also assessed associations between commonly used perioperative medications and POD. The application of benzodiazepines was found to be an independent risk factor for POD as previous studies suggested.30,31 No application of anticholinergic drugs was found in this study. The probable reason may be that patients under non-general anaesthesia were chosen. Surgeons had different habits of prescribing for elderly patients may be another reason. Our results did not find significant associations between perioperative anti-inflammatory drugs and POD. Recent randomized controlled trials about the effects of glucocorticoids on POD also did not reach a consistent conclusion.32–34 More and more studies found glucocorticoids may increase inflammation of central nervous system.35,36 Several clinical trials revealed NSAIDs may help decrease the incidence of delirium.37,38 However, our study did not confirm this association. Inconsistent standards of dosage and duration of administration may be important reasons.
Although optimal cut-off value of age had the highest sensitivity of 0.850 and benzodiazepines had the highest specificity of 0.952, the specificity of age and the sensitivity of benzodiazepines were the lowest among the risk factors for POD. Postoperative NLR showed high accuracy to predict POD with AUC of 0.790. Optimal cut-off value of postoperative NLR also had the high specificity of 0.797 and sensitivity of 0.727. We must admit prediction of POD based only on one perioperative factor was difficult because POD occurrence was multifactorial. The AUC of the multivariate ROC was greater for model 1 (benzodiazepines + cCRP + postNLR) or model 2 (age + benzodiazepines + cCRP + cNLR) compared to postoperative NLR alone model.
The impact of anaesthetic technique on the risk of delirium remains controversial. A large retrospective study showed postoperative delirium for total knee and hip arthroplasty in older adults would occur at a higher rate among patients who received general anaesthesia, compared with those who underwent their procedures under neuraxial anaesthesia.10 One randomized controlled study with a small sample size also showed similar result.11 But recently, another large randomized controlled study got conflicting result. The authors reported spinal anesthesia for hip-fracture surgery in older adults was not superior to general anesthesia with respect to the incidence of POD.12 Previous studies investigating the association between white-cell derived biomarkers and POD seemed to focus more on patients receiving general anesthesia, while this was the first study selecting patients who accepted surgery for lower limb fracture under non-general anaesthesia. On the other hand, the effects of general anesthesia drugs on POD were eliminating.
Some limitations of this study were worth considering. Firstly, preoperative laboratory data were obtained at different point of time. Secondly, we did not evaluate the duration of delirium and ignored the difference between hyperactive and hypoactive delirium. Thirdly, some perioperative factors associated with the development of POD, such as pain control and sleep disturbance, were not included in our analysis.
Conclusion
In conclusion, our results indicated age, benzodiazepines, postoperative NLR, change of NLR and change of CRP may be independent predictable markers for POD in elderly patients undergoing surgery for lower limb fracture under non-general anaesthesia. These results added important evidence to the understanding of a causative relationship between delirium and perioperative inflammation. Early postoperative NLR may help to recognize POD as soon as possible. Further larger prospective trials are necessary to validate these findings.
Acknowledgment
This research was supported by Projects of Medical and Health Technology Development Program in Shandong Province (2019WS465) which had no financial support.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Seung-Taek O, Park JY. Postoperative delirium. Korean J Anesthesiol. 2019;72(1):4–12. doi:10.4097/kja.d.18.00073.1
2. Maldonado JR. Neuropathogenesis of delirium: review of current etiologic theories and common pathways. Am J Geriatr Psychiatry. 2013;21(12):1190–1222. doi:10.1016/j.jagp.2013.09.005
3. Liu X, Yang Y, Zhu S, Ma D. Inflammatory markers in postoperative delirium (POD) and cognitive dysfunction (POCD): a meta-analysis of observational studies. PLoS One. 2018;13(4):e0195659. doi:10.1371/journal.pone.0195659
4. Kinoshita H, Saito J, Takekawa D, Ohyama T, Kushikata T, Hirota K. Availability of preoperative neutrophil-lymphocyte ratio to predict postoperative delirium after head and neck free-flap reconstruction: a retrospective study. PLoS One. 2021;16(7):e0254654. doi:10.1371/journal.pone.0254654
5. Rui H, Wang F, Shen H, Zeng Y, Zhang L. Association between increased neutrophil-to-lymphocyte ratio and postoperative delirium in elderly patients with total hip arthroplasty for hip fracture. BMC Psychiatry. 2020;20(1):496. doi:10.1186/s12888-020-02908-2
6. Ida M, Takeshita Y, Kawaguchi M. Preoperative serum biomarkers in the prediction of postoperative delirium following abdominal surgery. Geriatr Gerontol Int. 2020;20(12):1208–1212. doi:10.1111/ggi.14066
7. Oyama T, Kinoshita H, Takekawa D, Saito J, Kushikata T, Hirota K. Higher neutrophil-to-lymphocyte ratio, mean platelet volume, and platelet distribution width are associated with postoperative delirium in patients undergoing esophagectomy: a retrospective observational study. J Anesth. 2022;36(1):58–67. doi:10.1007/s00540-021-03007-6
8. Kotfis K, Slozowska J, Safranow K, Szylinska A, Listewnik M. The practical use of white cell inflammatory biomarkers in prediction of postoperative delirium after cardiac surgery. Brain Sci. 2019;9(11):308. doi:10.3390/brainsci9110308
9. Halazun HJ, Mergeche JL, Mallon KA, Sander Connolly E, Heyer EJ. Neutrophil-lymphocyte ratio as a predictor of cognitive dysfunction in carotid endarterectomy patients. J Vasc Surg. 2014;59(3):768–773. doi:10.1016/j.jvs.2013.08.095
10. Weinstein SM, Poultsides L, Baaklini LR, et al. Postoperative delirium in total knee and hip arthroplasty patients: a study of perioperative modifiable risk factors. Br J Anaesth. 2018;120(5):999–1008. doi:10.1016/j.bja.2017.12.046
11. Song Y, Liu Y, Yuan Y, et al. Effects of general versus subarachnoid anaesthesia on circadian melatonin rhythm and postoperative delirium in elderly patients undergoing hip fracture surgery: a prospective cohort clinical trial. EBioMedicine. 2021;70:103490. doi:10.1016/j.ebiom.2021.103490
12. Neuman MD, Feng R, Carson JL, et al. Spinal anesthesia or general anesthesia for hip surgery in older adults. N Engl J Med. 2021;385(22):2025–2035. doi:10.1056/NEJMoa2113514
13. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”. A practical method for grading the cognitive state of patients for the clinician. J Psychiatr Res. 1975;12(3):189–198. doi:10.1016/0022-3956(75)90026-6
14. Charlson M, Szatrowski TP, Peterson J, Gold J. Validation of a combined comorbidity index. J Clin Epidemiol. 1994;47(11):1245–1251. doi:10.1016/0895-4356(94)90129-5
15. Inouye SK, van Dyck CH, Alessi CA, Balkin S, Siegal AP, Horwitz RI. Clarifying confusion: the confusion assessment method. A new method for detection of delirium. Ann Intern Med. 1990;113(12):941–948. doi:10.7326/0003-4819-113-12-941
16. Dhabhar FS, Malarkey WB, Neri E, McEwen BS. Stress-induced redistribution of immune cells–from barracks to boulevards to battlefields: a tale of three hormones–Curt Richter Award winner. Psychoneuroendocrinology. 2012;37(9):1345–1368. doi:10.1016/j.psyneuen.2012.05.008
17. Alam A, Hana Z, Jin Z, Suen KC, Ma D. Surgery, neuroinflammation and cognitive impairment. EBioMedicine. 2018;37:547–556. doi:10.1016/j.ebiom.2018.10.021
18. Murray C, Sanderson DJ, Barkus C, et al. Systemic inflammation induces acute working memory deficits in the primed brain: relevance for delirium. Neurobiol Aging. 2012;33(3):603–616.e603. doi:10.1016/j.neurobiolaging.2010.04.002
19. Hughes CG, Patel MB, Pandharipande PP. Pathophysiology of acute brain dysfunction: what’s the cause of all this confusion? Curr Opin Crit Care. 2012;18(5):518–526. doi:10.1097/MCC.0b013e328357effa
20. Cerejeira J, Lagarto L, Mukaetova-Ladinska EB. The immunology of delirium. Neuroimmunomodulation. 2014;21(2–3):72–78. doi:10.1159/000356526
21. Cerejeira J, Firmino H, Vaz-Serra A, Mukaetova-Ladinska EB. The neuroinflammatory hypothesis of delirium. Acta Neuropathol. 2010;119(6):737–754. doi:10.1007/s00401-010-0674-1
22. Kulaksizoglu B, Kulaksizoglu S. Relationship between neutrophil/lymphocyte ratio with oxidative stress and psychopathology in patients with schizophrenia. Neuropsychiatr Dis Treat. 2016;12:1999–2005. doi:10.2147/NDT.S110484
23. Gasparyan AY, Ayvazyan L, Mukanova U, Yessirkepov M, Kitas GD. The platelet-to-lymphocyte ratio as an inflammatory marker in rheumatic diseases. Ann Lab Med. 2019;39(4):345–357. doi:10.3343/alm.2019.39.4.345
24. Walzik D, Joisten N, Zacher J, Zimmer P. Transferring clinically established immune inflammation markers into exercise physiology: focus on neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio and systemic immune-inflammation index. Eur J Appl Physiol. 2021;121(7):1803–1814. doi:10.1007/s00421-021-04668-7
25. Jiang X, Shen Y, Fang Q, Zhang W, Cheng X. Platelet-to-lymphocyte ratio as a predictive index for delirium in critically ill patients: a retrospective observational study. Medicine. 2020;99(43):e22884. doi:10.1097/MD.0000000000022884
26. Kotfis K, Bott-Olejnik M, Szylińska A, Listewnik M, Rotter I. Characteristics, risk factors and outcome of early-onset delirium in elderly patients with first ever acute ischemic stroke - A prospective observational cohort study. Clin Interv Aging. 2019;14:1771–1782. doi:10.2147/CIA.S227755
27. Lechowicz K, Szylińska A, Listewnik M, et al. Cardiac delirium index for predicting the occurrence of postoperative delirium in adult patients after coronary artery bypass grafting. Clin Interv Aging. 2021;16:487–495. doi:10.2147/CIA.S302526
28. Pepys MB, Hirschfield GM. C-reactive protein: a critical update. J Clin Invest. 2003;111(12):1805–1812. doi:10.1172/JCI200318921
29. Jankowski CJ, Trenerry MR, Cook DJ, et al. Cognitive and functional predictors and sequelae of postoperative delirium in elderly patients undergoing elective joint arthroplasty. Anesth Analg. 2011;112(5):1186–1193. doi:10.1213/ANE.0b013e318211501b
30. Marcantonio ER, Juarez G, Goldman L, et al. The relationship of postoperative delirium with psychoactive medications. JAMA. 1994;272(19):1518–1522. doi:10.1001/jama.1994.03520190064036
31. Kassie GM, Nguyen TA, Kalisch Ellett LM, Pratt NL, Roughead EE. Preoperative medication use and postoperative delirium: a systematic review. BMC Geriatr. 2017;17(1):298. doi:10.1186/s12877-017-0695-x
32. Royse CF, Saager L, Whitlock R, et al. Impact of methylprednisolone on postoperative quality of recovery and delirium in the steroids in cardiac surgery trial: a randomized, double-blind, placebo-controlled substudy. Anesthesiology. 2017;126(2):223–233. doi:10.1097/ALN.0000000000001433
33. Kluger MT, Skarin M, Collier J, et al. Steroids to reduce the impact on delirium (STRIDE): a double-blind, randomised, placebo-controlled feasibility trial of pre-operative dexamethasone in people with hip fracture. Anaesthesia. 2021;76(8):1031–1041. doi:10.1111/anae.15465
34. Clemmesen CG, Lunn TH, Kristensen MT, Palm H, Foss NB. Effect of a single pre-operative 125 mg dose of methylprednisolone on postoperative delirium in hip fracture patients; a randomised, double-blind, placebo-controlled trial. Anaesthesia. 2018;73(11):1353–1360. doi:10.1111/anae.14406
35. Munhoz CD, Sorrells SF, Caso JR, Scavone C, Sapolsky RM. Glucocorticoids exacerbate lipopolysaccharide-induced signaling in the frontal cortex and hippocampus in a dose-dependent manner. J Neurosci. 2010;30(41):13690–13698. doi:10.1523/JNEUROSCI.0303-09.2010
36. Sorrells SF, Sapolsky RM. An inflammatory review of glucocorticoid actions in the CNS. Brain Behav Immun. 2007;21(3):259–272. doi:10.1016/j.bbi.2006.11.006
37. Wang X, Wang Y, Yanan H, et al. Effect of flurbiprofen axetil on postoperative delirium for elderly patients. Brain Behav. 2019;9(6):e01290. doi:10.1002/brb3.1290
38. Mu DL, Zhang DZ, Wang DX, et al. Parecoxib supplementation to morphine analgesia decreases incidence of delirium in elderly patients after hip or knee replacement surgery: a randomized controlled trial. Anesth Analg. 2017;124(6):1992–2000. doi:10.1213/ANE.0000000000002095
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.