Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Which Aspect of Patient–Provider Relationship Affects Acceptance and Adherence of Insulin Therapy in Type 2 Diabetes Mellitus? A Qualitative Study in Primary Care
Authors Mathew BK, De Roza JG, Liu C, Goh LJ, Ooi CW, Chen E, Poon S, Tang WE
Received 21 October 2021
Accepted for publication 31 December 2021
Published 26 January 2022 Volume 2022:15 Pages 235—246
DOI https://doi.org/10.2147/DMSO.S344607
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ming-Hui Zou
Blessy Koottappal Mathew,1 Jacqueline Giovanna De Roza,2 Changwei Liu,2 Ling Jia Goh,3 Chai Wah Ooi,2 Elya Chen,4 Shixuan Poon,1 Wern Ee Tang4
1National Healthcare Group Polyclinics, Toa Payoh Polyclinic, National Healthcare Group, Singapore; 2National Healthcare Group Polyclinics, Geylang Polyclinic, National Healthcare Group, Singapore; 3National Healthcare Group Polyclinics, Hougang Polyclinic, National Healthcare Group, Singapore; 4National Healthcare Group Polyclinics, Clinical Research Unit, National Healthcare Group, Singapore
Correspondence: Blessy Koottappal Mathew, National Healthcare Group Polyclinic, 2003 Toa Payoh Polyclinic, Lorong 8, Toa Payoh, 319260, Singapore, Email [email protected]
Purpose: In type 2 diabetes mellitus (T2DM), insulin therapy is often recommended to achieve the optimal control of disease, thereby preventing the onset and progression of diabetes-related complications. Despite knowing about the benefits, it has been reported that 71% of patients refuse insulin and the adherence rate ranges from 30 to 80%. Patient–provider relationship (PPR) may affect such insulin-related behaviours, but little is known about which aspect of PPR affects this. This study aimed to explore the key aspect of the patient–provider relationship that affects the initial insulin acceptance and continued adherence.
Patients and Methods: We used the grounded theory approach in this qualitative research. The study was conducted at two primary care clinics between September 2019 and January 2021. Patients with T2DM on basal or premixed insulin were recruited using maximum variation sampling. Data were collected using semi-structured in-depth interviews and transcribed verbatim for analysis using constant comparison and synthesis.
Results: Twenty-one participants with different levels of diabetes control and adherence were recruited. Four themes that emerged were 1) patient–provider interaction, 2) addressing the psychological fears, 3) gaining confidence in handling insulin equipment and 4) follow-up after insulin initiation. Among the subthemes, trust in doctors, provider’s communication skills, patient-centred decision-making and continuity of care positively influenced insulin acceptance and adherence. Conversely, fear of being judged by the provider hindered open communication around non-adherence. Various aspects of interaction with nurses helped in alleviating patient’s fear of injection and gaining confidence with the insulin equipment.
Conclusion: Many aspects of PPR affect insulin acceptance and adherence. Among these, gaining patients’ trust, effective patient–provider communication, patient-centred decision-making, and ensuring continuity of care improve both insulin acceptance and treatment adherence. Various interactions with nurses help in addressing fears surrounding injection and gaining acceptance towards insulin therapy. Patients’ fear of being blamed or judged by the provider negatively affects open communication around non-adherence.
Keywords: insulin initiation, insulin adherence, insulin acceptance, healthcare provider, patient interactions, primary care
Introduction
The proportion of people with type 2 diabetes mellitus (DM) has been increasing worldwide. In Singapore, the prevalence of diabetes was 8.6% in 20181 with estimated 19,000 people being diagnosed each year.2 One out of 9 people aged 18 to 69 has diabetes, comprising 11.3% of our population.3
Many people with type 2 DM require insulin therapy to achieve the optimal goal of disease, thereby preventing the onset and progression of diabetes-related complications.4 Despite knowing the benefits of insulin, many people still refuse such treatment. In a local survey conducted in 2011, 70.6% of patients refused insulin when it was recommended.5 The refusal rate is similar in Malaysia, 74.2%6 but is comparatively lower in Korea, 35.7%7 and the United States, 40%.8 Once insulin is initiated, treatment adherence is another barrier that affects glycaemic control. The rate of insulin adherence varies between 30% and 80%.9,10
Refusal of insulin and non –adherence to treatment are caused by various patient –related and healthcare provider (HCP) related factors. Fear of needle, pain, side-effects, difficulty in administration, perceived punishment, social stigma and discrimination are some of the patient-related factors that hinder insulin initiation.11–13 Similarly, fear of injection, side effects, and complex regime were noted to be the reasons for non-adherence to insulin therapy.14 HCP plays an important role in addressing such multiple factors but is hindered due to various factors, such as lack of good doctor–patient relationship, poor communication and not engaging patients in decision-making.11,15 Similar findings were also noted in our local setting by Tan et al12 that the insulin initiation is hindered by the complex interaction between patients and healthcare providers. A 2-year prospective multinational observational study found that the various aspects of the patient–physician relationship affect adherence to insulin.16
The nature of patient–provider relationship may contribute either positively or negatively to insulin-related behaviours. To be able to develop/guide the improvement programs or trainings for HCP, it is vital to understand which aspect of the patient–provider relationship affects insulin acceptance and adherence. The increased local prevalence of insulin refusal and non-adherence makes it even more significant to look into strategies to tackle them. However, limited studies have explored the impact of patient–provider relationship in this area, and we are not aware of any such research in our local setting.
Aim
This study aims to explore the key aspects of patient–provider relationship that may be related to insulin acceptance and adherence.
The research questions were:
- Which aspects of patient – provider interaction influenced the patient’s initial acceptance of insulin?
- What were the initial fears associated with insulin use?
- How did the health care provider assist in overcoming the initial fears of insulin use?
- What was the patient’s struggle in ensuring adherence to insulin therapy?
- Which aspects of patient–provider relationship influenced patient’s adherence to insulin?
Methods
We used COREQ guidelines in reporting this study.
Study Design
We used the grounded theory approach to conceptualize this qualitative research. The grounded theory tries to account for peoples’ actions from the perspective of those involved.17
Setting and Participants
This study involved twenty-one patients with type 2 DM, who had been on basal or premixed insulin for at least 6 months. It was conducted in the primary care clinics under the National Healthcare Group Polyclinics, where participants received routine care.
We used purposive sampling to provide maximum variation in patients’ characteristics. This sampling method helps to maximize the diversity of data and obtain greater understandings of the phenomenon studied.17
Data Collection
Data collection took place from September 2019 to January 2021. The healthcare provider identified suitable participants during the routine clinic visits and referred them to the study team members for recruitment. Participants were not interviewed by their treating clinicians to avoid any potential bias.
Recruitment was ceased from February 2020 to June 2020 due to the COVID-19 pandemic and resumed in July 2020 with interviews conducted via a video conferencing zoom platform. We approached thirty-two patients in total, eleven of them refused participation due to lack of time, interest, knowledge or unavailability of online technology. Face-to-face interviews were conducted in a private room located at the clinic itself to ensure patients’ convenience and privacy. Four out of 21 patients were interviewed remotely. Patients were advised to find a private corner at home for the interview sessions.
Information on patient demographics and treatment regimens was collected at recruitment. The study used semi-structured in-depth interviews using a topic guide, and it was audio recorded by 3–4 interviewers. We allowed participants to converse in any of the locally preferred languages: English, Mandarin, Malay or Tamil. The topic guide comprised questions around the patient–provider relationship and its impact on insulin acceptance and adherence. It was revised based on the preliminary data analysis. We used probing, rephrasing and clarifying to facilitate in-depth exploration of the main responses.
Each interview was conducted over 15 minutes to an hour. Video conferencing has also worked well in this study with comparable duration and depth of the initial face-face interviews. The sample size was determined when the data saturation was reached.
Data Analysis
The audio recording of each in-depth-interview was professionally transcribed verbatim, and interviews conducted in Mandarin, Malay and Tamil were translated into English for coding. The transcripts were vetted against the audio recording to ensure accuracy.
Thematic analysis was performed by 3–4 coders using line-by-line NVivo coding to identify themes found in each transcript. Findings were shared and discussed during the regular meetings with all team members to organize and contextualize the evolved interpretations. Eventually, all themes were categorized into major themes followed by sub themes.
Trustworthiness
The key strategies to ensure trustworthiness and rigor in qualitative research include credibility, transferability, conformability and dependability.18 To ensure researcher credibility, the experienced research members in the team conducted training to ensure all investigators had the required skills and knowledge to carry out their role. To ensure credibility of the results, a semi-structured interview guide was designed to obtain accurate sharing from participants; interviews were audiotaped with verbatim transcription and vetted against audio recording. The study process and data collection methods are detailed to ensure dependability. Conformability was ensured through the development of a codebook and inter-coder checks between the research team. We used purposive sampling, providing a maximum variation in demographic and clinical characteristics to support transferability.17
Ethical Considerations
The study was approved by the National Healthcare Group (NHG) Domain Specific Review Board (DSRB), reference 2019/00096. The study was conducted in accordance with the declaration of Helsinki. Participation was voluntary, and the participants could withdraw at any time. Informed written consent was taken from all participants and it included consent for publication of anonymised responses. The collected data were anonymized before analysis to maintain confidentiality. Hard copy, electronic data and audio recordings were stored on secured computers and locked cabinets, accessible to study team members only.
Results
Participant Characteristics
The demographic data of the participants are outlined in Table 1. The median age of the participants was 63 years. The average duration of having diabetes was 14 years, and the average duration of insulin use was 6 years. 80% of them were on pen devices for the insulin therapy. 43% of participants self-reported as being not fully adherent to insulin therapy and the median HbA1c (glycosylated haemoglobin) was at 8.2%.
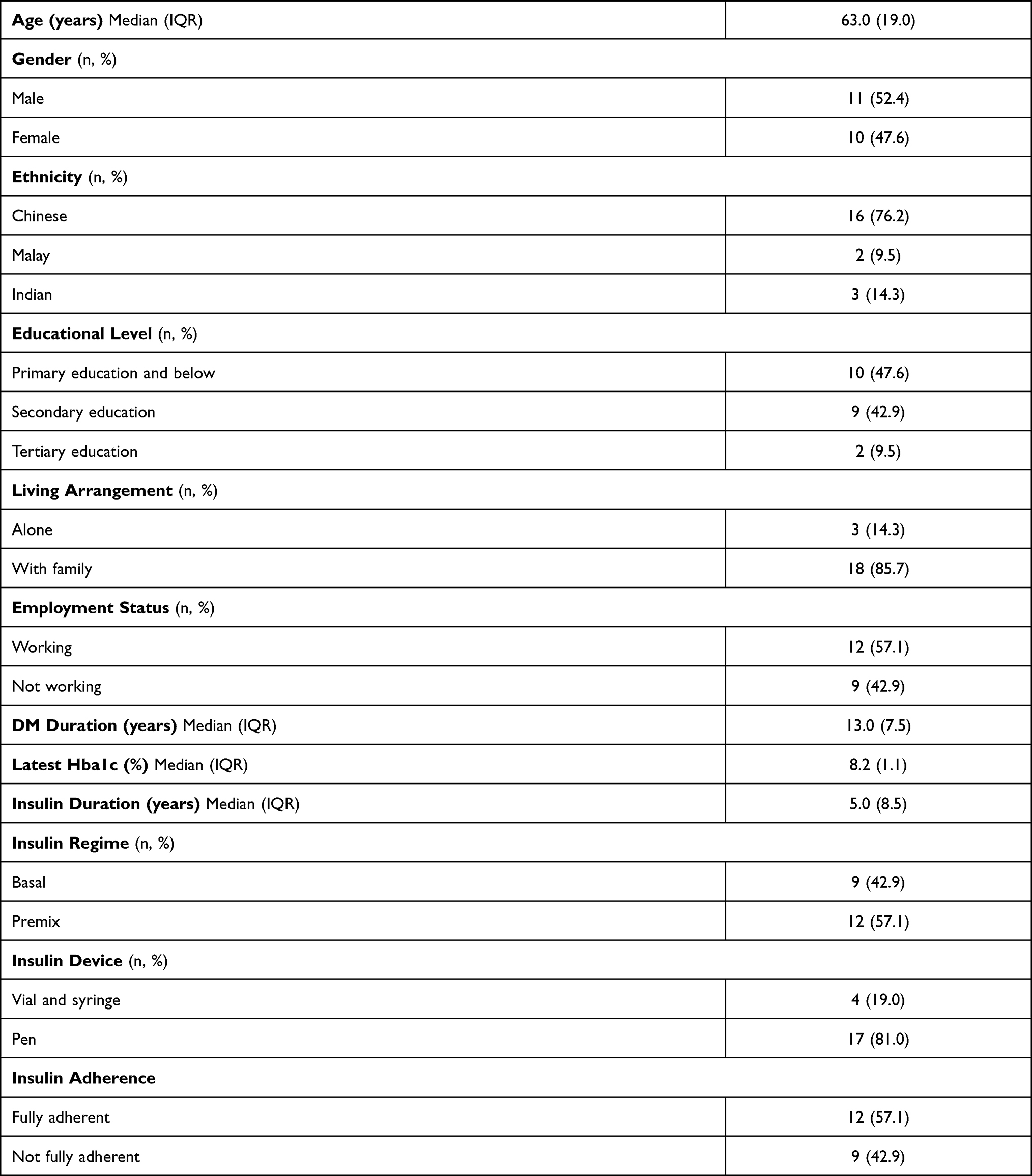 |
Table 1 Demographic and Clinical Information (n = 21) |
Themes and Subthemes
Four themes and eight subthemes were emerged and are outlined in Table 2.
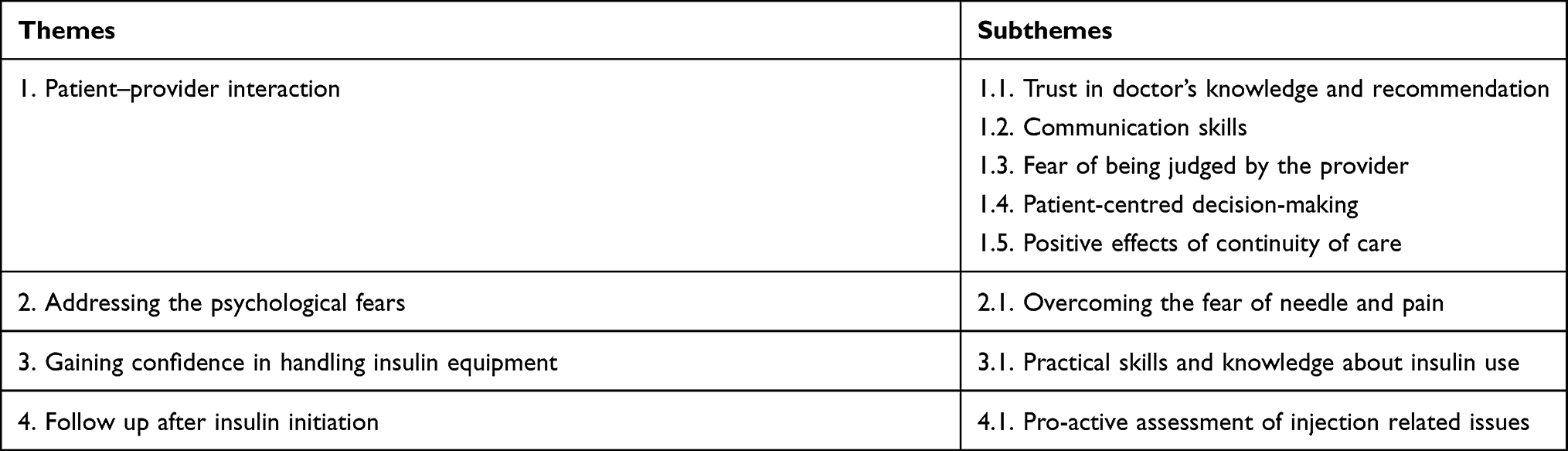 |
Table 2 Themes and Subthemes |
Theme 1: Patient–Provider Interaction
Subtheme 1.1: Trust in Doctor’s Knowledge and Recommendation
Trust in doctor’s knowledge and recommendation had a positive effect on accepting insulin therapy.
I listen to what the doctor says, you ask me to inject, then I will inject … I was never afraid. Because doctors want you to be healthy. Want you to control your diabetes. Because only doctors have such knowledge. – P11.
What doctor says, just follow his instructions. If I do not trust him, why do I still visit him? He is my lifeline leh. – P17.
Subtheme 1.2: Communication Skills
Participants shared about how the doctor’s explanation convinced them to start insulin.
At first, I was a bit hesitant and I said I do not want injections. But the doctor told me that your diabetes level is very high. He said that only by taking insulin injections, will I be able to manage and keep my diabetes under control – P08.
Participants found that encouragement from the doctor and nurses helped them in the initial acceptance of insulin.
He encouraged, he believes that it’s better to take the jabs than the medication. He encouraged me that way, that time I said ok lo, since he said that I will try it out lo. Then the nurse also encouraged me to take the jabs – P03.
I mean injection to your body … yah … and erm … but due to their persuasion from the doctor lah … so they say that it is much faster than the oral medication. That’s why I gave it a try. But the first … I mean the first starting is actually quite bad for me.- P21
Subtheme 1.3: Fear of Being Judged by the Provider
One of the participants shared that he felt being blamed for missing his injections and the poorly controlled sugars.
But he’s telling you off … he say that, “Your sugar is still very high”. I mean … why you never do your injection … you never … wah … then so you … he’s blame you …. P21.
However, he did not share his feeling with the doctor but wanted to finish off the consult as fast as he could.
I ….did not say anything lah. I just … I just want to quickly … finish- P21.
As a result, he wanted to skip the future visit to that particular doctor.
Sometimes he even make me want to skip the … to visit this doctor. So let us say, this doctor is my … let us say currently I am seeing this doctor … I will just miss the appointment … I will re-arrange to see another doctor -P21.
The same participant shared that he would not discuss his health issues with such doctor as the doctor would say that his condition is getting serious and would relate it to his behaviour of missing injections and the high sugars.
Sometimes even if you, let us say, your health got some issues but you do not want to tell the doctor because the doctor will tell you, “Eh eh, you are becoming more serious you know?” You just hide. Because you say that then say,’ Woah … you … because you never take the injection that’s why it comes back to you then woah … you come … straight come to you. That’s how I feel lah- P21.
Subtheme 1.4: Patient-Centred Decision-Making
Participants shared about their struggles in following the prescribed insulin regimen.
Like what I said, early in the morning if let us say you wake up late, I will not have the time to actually do that lah … [stammers] … first thing is to rush to work. Unless we are those. We are those very … I mean set through the timing. I mean let us say, you always have the time to set for doing the blood sugar, the time to do insulin … but I am not that kind of person- P21.
The difficulties were shared with the healthcare provider and the regimens were adjusted accordingly to suit the individual patient.
Previously I was taking at night … Shift duty missed … So that’s why change it to the morning. So easy for me – P03.
One of the participants shared the experience of hypoglycaemia while on insulin therapy.
I was saying how come I eat, eat and also take the insulin, also took medicine and breakfast why is it that when it’s 10 o’clock I will automatically start trembling badly -P04.
The doctor individualized the insulin regimen based on the diet pattern and it helped in preventing hypoglycaemia.
So they (healthcare provider) asked me about my lunch timing, my breakfast timing and my dinner time … Ah, then they started to arrange the, the amount of medicine, the amount of insulin. – P04.
Subtheme 1.5: Positive Effects of Continuity of Care
The participants found it beneficial to have continuous care provided by the same doctor as they knew about their issues regarding insulin therapy.
Because he every time sees me ah, then you see the result ah, then he knows what happen. Then you other … change other doctor, he thinking his one … he thinking his one. I tell you ah, he ask you huh, repeat again … repeat again, I very tired. –P20.
But I feel that the same doctor would be preferable because different doctor will have different approach and opinions ah. - P21.
Theme 2: Addressing the Psychological Fears
Subtheme 2.1: Overcoming the Fear of Needle and Pain
Needle phobia was identified as a barrier to insulin initiation. Participants reported that the healthcare provider explored on their fears and offered solutions by proposing the use of a pen device and shorter needles.
They asked me to try with a pen …. now I overcome already I now not scared already – P01.
The recommendation from HCP to use the smallest needle was also helpful in accepting the insulin therapy.
I very scared with the needle one. I dare not see also. Sister(nurse) told me to get the smallest (needle), for me not so painful – P01.
Theme 3: Gaining Confidence in Handling Insulin Equipment
Subtheme 3.1: Practical Skills and Knowledge About Insulin Use
The participants shared about their initial lack of confidence in managing insulin injection. The practical skills taught by the nurses and the return demonstration had helped them gain confidence in managing insulin injections.
Problem is what, that time we do not know the … the insulin how to poke- Then the nurse taught me-P20.
How to inject, near stomach. She taught everything (referring to nurse) – P12.
They taught me. In fact, the last time they taught me also go which way, how to go about, all these thing. The doctor also teach me how to go about it. So ok la. More or less I know the inject … injection, where to inject and all these thing.- P19.
Teaching me about the insulin, and just teaching me how to inject.- P14.
I was tested a few times previously. This side la … the nurse here tested me. Correct lor. I drew out, they said correct. – P15.
Theme 4: Follow Up After Insulin Initiation
Subtheme 4.1: Pro-Active Assessment of Injection Related Issues
Few participants shared that the doctor and nurses provided follow-up to tackle any coping issues with insulin and problems with the injection site.
… doctor, nurses will ask me “How is your insulin?”, uh … can … can you uh … can get … ask me to give her to take a look uh … my … uh … my … around the belly there, is it like swollen, blue black, this and that –P16.
So last time I used to inject in the same area … yah.yah. But they tell me is that I will have to actually shift around the area of the stomach- P21.
Discussion
Theme 1: Patient–Provider Interaction
Subtheme 1.1: Trust in Doctor’s Knowledge and Recommendation
Trust is an important aspect of the physician–patient relationship. In this study, several participants verbalized that they trusted their physicians and hence accepted insulin when it was offered. None of the studies was done examining the relationship between trust and insulin acceptance. However, trust in HCP is associated with increased adherence to insulin therapy19 and better glycaemic control.20,21
According to Rodriguez,22 when patients do not have confidence in their healthcare provider, they are less likely to implement care recommendations and be adherent to their prescribed treatment. A single approach might not work to build or maintain trust, as it requires effort from the patient, HCPs, and also the senior management in healthcare institutions. A work group of 17 health care leaders and patient advocates from the Forum of Building Trusts, American Medical Association, has published a summarised approach for increasing trust among patients and the health care team in an organisation.23 It recommends that the training and education should focus on communication and relationship skills to improve clinician’s behaviour. The stakeholders in healthcare institutions play a key role in crafting an environment that values trusting relationships with the patients.
Sub- Theme 1.2: Communication Skills
In the study, doctor’s explanations about the patient’s state of diabetes control, insulin being the most effective and the last resort of treatment have made the participants accept insulin.
Few studies have also noted that patients are more likely to accept insulin therapy if they perceive the importance of insulin in gaining glycaemic control and improving health.24,25 Patients who perceived they had no other choice than commencing insulin were noted to be more likely to start insulin.26
Interactions with healthcare provider create a great opportunity to influence the patient’s attitude toward insulin therapy. A significantly greater proportion of patients who failed to initiate prescribed insulin therapy reported that the risks and benefits of insulin treatment were not clearly explained during their physician interactions.27 Effective communication plays an integral role in such interactions to provide patients with the knowledge as well as a positive experience for them to adopt favourable decision towards insulin acceptance.28 Training the HCPs on communication skills can add benefit in building a strong patient–provider relationship and achieving long-term benefits.
Subtheme 1.3: Fear of Being Judged by the Provider
One of the participants shared that it has been difficult for him to fully comply with his insulin treatment. The direct questioning by the physician on his non-adherent behaviour and the resulting poor glycaemic control made him feel that he had been blamed for missing his injections. As a result, he decided not to communicate openly about his health condition and attempted to even avoid future visits to that particular physician.
The finding echoes with a survey conducted at the University of Utah Health. It found that a great proportion of people tend to lie to their doctors or fail to speak up about their health condition due to the fear of being judged or lectured.29 Withholding important information about health could result in significant negative implications for disease control and outcomes. It is also noted that dissatisfaction with the aspects of interactions with physicians contributes to poor insulin adherence.16 Therefore, it is vital to look into strategies to improve open communication between patients and providers.
In an article on how to work with noncompliant patients, Kleinsinger suggests raising the question of non-adherence in a non-judgmental and problem-solving manner.30 By staying non-judgmental, patients feel comfortable about discussing their health concerns, and continue with the conversation. Instead of using the traditional way of direct questioning, an open-ended, non-judgmental question can be effective in approaching non-adherence.
Subtheme 1. 4: Patient-Centred Decision-Making
In this study, participants identified work commitments and experiences of hypoglycaemia as barriers to insulin adherence. They further shared that the physician addressed it by making an individualized insulin regimen to better suit the lifestyle. Various studies have reported the positive impact of patient-centred decision-making on treatment adherence, clinical outcomes and cost-effectiveness.31,32
Adherence to insulin is affected by the interference of injections with daily activities, the complexity of insulin regimen, multiple daily dosing, cost, and side effects.33,34 Every patient is unique in terms of their lifestyle and health –related practices.
In an article on providing new approaches to individualized care, Powell et al encourages appreciation and frankness to the patient’s choices even if not the HCP’s primary choice.35 Sometimes, it can be hindered by factors like physician’s desire for autonomy and the lack of skill. Training the HCPs on motivational interviewing (MI) might be helpful in addressing it. MI provides an opportunity to help patients assess what might be important or possible and how they can incorporate changes to address the insulin adherence.36
Subtheme 1. 5: Positive Effects of Continuity of Care
Continuity of care is a hallmark of the primary healthcare system and is associated with better glycaemic control among people with diabetes.37 In the present study, participants shared the benefits of having a consistent doctor for better follow-up and continuity of care. In a local study conducted in the primary care setting, lack of continuity of care was reported as a barrier to insulin initiation.12
Diabetes management involving insulin initiation is a complex process requiring patient education, skills training and regular follow-up. Continuity of care ensures follow-up on patient’s individual issues and management accordingly. However, it might be impractical to ensure all aspects of care and continuity by a single provider even though having a consistent doctor would sound ideal. Moreover, Mainous et al found no difference in having a regular provider versus a regular site of care in terms of diabetes care.37
Continuity of care can also be facilitated by a physician-led, team-based approach to health care. The World Health Organization (WHO) recommends team –based care where there is a strategic distribution of work among nurses and other providers in caring for complex chronic diseases like diabetes.38 In our institution, a team-based care model has been implemented since 2015, and with more patients gaining access to such a model of care, we might be able to better address the issue with continuity of care.
Theme 2: Addressing the Psychological Fears
Subtheme 2.1: Overcoming the Fear of Needle and Pain
Fear of injection, needle and pain are the common barriers to insulin initiation and adherence.11–13
In this study, participants shared that the healthcare provider explored their fears with insulin therapy and offered a pen device and shorter needles to ease the fear of injection. A total of 80% of our participants are on insulin pen devices. A study conducted among Japanese patients also found that showing an insulin pen and reassurance concerning the pain of injection has helped them accept insulin.39 HCP may use the newer insulin device, shorter needles and provide a practical demonstration to address patient’s fears of injection.40 Another study found that pen devices are preferred by patients and are also associated with improved adherence.41
Theme 3: Gaining Confidence in Handling Insulin Equipment
Subtheme 3.1: Practical Skills and Knowledge About Insulin Use
Participants shared about the role of nurses in helping them achieve the knowledge and practical skills in using insulin therapy. None of them verbalized any lack of confidence in managing injections.
A systematic review found that patients perceive insulin administration as difficult and complex11 and that the practical demonstration of insulin injection facilitates insulin initiation.40 Limited self-management training has been associated with poor insulin acceptance.13,28 It is recommended to assign a designated team of HCP to provide education on insulin use.40
In our setting, we have a designated team of nurses to provide insulin education and skills training. The patients get to inject their first injection under supervision if required and it greatly benefits in alleviating fear and gaining self-confidence in managing injections.
Theme 4: Follow Up After Insulin Initiation
Subtheme 4.1: Pro-Active Assessment of Injection Related Issues
Participants mentioned the continued follow-up made by the nurses either via tele-phone or during clinic visits. Incorrect injection technique is a common problem faced by patients and is associated with injection site issues like lipohypertrophy, bleeding, pain, and bruises. Such issues may affect compliance and also glycaemic control.40 Therefore, it is important for the HCP to render continued support and follow-up to patients even after the initial initiation of insulin therapy.
Implication to Practice
The findings from this study suggest that the efforts to enhance patient–provider interactions such as building a trusting relationship, good communication skills and patient-centred decision-making promotes patients’ acceptance and adherence to insulin therapy. The results remind HCP on approaching non-adherence in a problem-solving manner30 to create a safe environment promoting open communication about patient’s barriers towards insulin adherence. Basic training on motivational interviewing can be considered to encourage patient-centred decision-making36 in terms of optimal use of insulin. Team-based care can be considered to ensure continuity of care, enhance communication and follow-up. Employing trained nurses in the team would be impactful as this study shows the beneficial role that they play in patient education, training on injection-related skills, addressing patients’ fears towards insulin and providing continued support even after the initiation of insulin.
Strength and Limitation
Our study included multi-cultural participants to capture the ethnic differences in perception towards patient–provider relationships. It included the views from both adherent and non-adherent participants. To our knowledge, this is the first local study exploring aspects of patient–provider relationship in both insulin acceptance and adherence. One of the unique findings from this study is about how patient perceives direct questioning on their non-adherent behaviour as “being blamed or judged” and its influence on open communication about insulin use. Overall, our study provided insights into the elements that positively and negatively affect insulin acceptance and adherence so that training and interventions can be planned accordingly.
One limitation of our study is that we did not include patients on the basal plus bolus insulin regimen, as it is not common in our setting. The duration of the interview was short for a few participants even though they provided valuable insights into the topic. Our study was limited to the primary care setting; hence, the findings should be used with caution in other settings. Future research on the provider’s view may be considered.
Conclusion
Our findings highlight that insulin initiation and adherence are greatly influenced by the various aspects of patient–provider relationship. Trust in providers, communication skills of provider, patient-centred decision-making and continuity of care have positive effects on gaining acceptance of insulin and ensuring adherence. Fear of being blamed or judged by the provider negatively affects open communication about insulin use and, therefore, treatment adherence. Nurses play an important role in addressing patient fears about injection. The findings from this study can be used to plan teachings, trainings or intervention programs to improve the rate of insulin acceptance and adherence. Future research may look into the HCP’s view on patient–provider relationship in insulin acceptance and adherence.
Acknowledgments
We thank the participants of the study, the institution’s clinical research unit, nursing services and the clinic staff for their support in this study.
Funding
This research was supported by the Singapore Ministry of Health’s National Medical Research Council under the Centre Grant Programme (Ref No: NMRC/CG/C019/2017).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ministry of Health. Executive Summary on National Population Health Survey 2016/17; 2018. Available from: https://www.moh.gov.sg/docs/librariesprovider5/resources-statistics/reports/executive-summary-nphs-2016_17.pdf.
2. Han GY. Parliament: 19,000 diagnosed with diabetes yearly, more expected to be diagnosed in short term, says MOHThe Straits Times; Feburary 26, 2020. Available from: https://www.straitstimes.com/politics/parliament-19000-diagnosed-with-diabetes-yearly-more-expected-to-be-diagnosed-in-short-term.
3. Khalik S. 3 key issues at National Day Rally 2017: singapore’s war on diabetes. The Straits Times; August 20, 2017. Available from: https://www.straitstimes.com/singapore/spores-war-on-diabetes.
4. American Diabetes Association. 9.Pharmacologic approaches to glycemic treatment: standards of Medical Care in Diabetes-2021. Diabetes Care. 2021;44(Supplement 1):111–124. doi:10.2337/dc21-S009.
5. Wong S, Lee J, Ko Y, Chong MF, Lam CK, Tang WE. Perceptions of insulin therapy amongst Asian patients with diabetes in Singapore. Diabetic Med. 2011;28(2):206–211. doi:10.1111/j.1464-5491.2010.03195.x
6. Tan WL, Asahar SF, Harun NL. Insulin therapy refusal among type II diabetes mellitus patients in Kubang Pasu district, Kedah, Malaysia. Singapore Med J. 2015;56(4):224–227. doi:10.11622/smedj.2014170
7. Song Y, Ku BJ, Cho J, Jun Y, Kim B, Nam S. The prevalence of insulin refusal and psychological insulin resistance among Korean patients with type 2 diabetes mellitus. Ann Transl Med. 2019;7(23):760. doi:10.21037/atm.2019.11.77
8. Turchin A, Hosomura N, Zhang H, Malmasi S, Shubina M. Predictors and consequences of declining insulin therapy by individuals with type 2 diabetes. Diabetic Med. 2020;37(5):814–821. doi:10.1111/dme.14260
9. Peyrot M, Barnett AH, Meneghini LF, Schumm-Draeger PM. Insulin adherence behaviours and barriers in the multinational global attitudes of patients and physicians in insulin therapy study. Diabetic Med. 2012;29(5):682–689. doi:10.1111/j.1464-5491.2012.03605.x
10. Weinger K, Beverly EA. Barriers to achieving glycemic targets: who omits insulin and why? Diabetes Care. 2010;33(2):450–452. doi:10.2337/dc09-2132
11. Ng CJ, Lai PSM, Lee YK, Azmi SA, Teo CH. Barriers and facilitators to starting insulin in patients with type 2 diabetes: a systematic review. Int J Clin Pract. 2015;69(10):1050–1070. doi:10.1111/ijcp.12691
12. Tan AM, Muthusamy L, Ng CC, Phoon KY, Ow JH, Tan NC. Initiation of insulin for type 2 diabetes mellitus patients: what are the issues? A qualitative study. Singapore Med J. 2011;52(11):801–809.
13. Lee YK, Ng CJ, Lee PY, et al. What are the barriers faced by patients using insulin? A qualitative study of Malaysian health care professionals’ views. Patient Prefer Adherence. 2013;(2013(7):103–109. doi:10.2147/PPA.S36791
14. Davies MJ, Gagliardino JJ, Gray LJ, Khunti K, Mohan V, Hughes R. Real-world factors affecting adherence to insulin therapy in patients with Type 1 or Type 2 diabetes mellitus: a systematic review. Diabetic Med. 2013;30(5):512–524. doi:10.1111/dme.12128
15. Ellis K, Mulnier H, Forbes A. Perceptions of insulin use in type 2 diabetes in primary care: a thematic synthesis. BMC Fam Pract. 2018;19(1):70. doi:10.1186/s12875-018-0753-2
16. Linetzky B, Jiang D, Funnell MF, Curtis BH, Polonsky WH. Exploring the role of the patient–physician relationship on insulin adherence and clinical outcomes in type 2 diabetes: insights from the MOSAIc study. J Diabetes. 2017;9(6):596–605. doi:10.1111/1753-0407.12443
17. Polit DF, Beck CT. Essentials of Nursing Research: Appraising Evidence for Nursing Practice.
18. Lincoln YS, Gubaman EG. Naturalistic Inquiry. Sage Publications; 1985.
19. Halepian L, Saleh MB, Hallit S, Khabbaz LR. Adherence to insulin, emotional distress, and trust in physician among patients with diabetes: a cross-sectional study. Diabetes Ther. 2018;9(2):713–726. doi:10.1007/s13300-018-0389-1
20. White RO, Osborn CY, Gebretsadik T, Kripalani S, Rothman RL. Health literacy, physician trust, and diabetes-related self-care activities in Hispanics with limited resources. J Health Care Poor Underserved. 2013;24(4):1756–1768. doi:10.1353/hpu.2013.0177
21. Alazri MH, Neal RD. The association between satisfaction with services provided in primary care and outcomes in type 2 diabetes mellitus. Diabetic Med. 2003;20(6):486–490. doi:10.1046/j.1464-5491.2003.00957.x
22. Rodriguez KM. Intrinsic and extrinsic factors affecting patient engagement in diabetes self-management: perspectives of a certified diabetes educator. Clin Ther. 2013;35(2):170–178. doi:10.1016/j.clinthera.2013.01.002
23. Lee T, McGlynn H, Safram D,G. A framework for increasing trust between patients and the organizations that care for them. J Am Med Assoc. 2019;321(6):539–540. doi:10.1001/jama.2018.19186
24. Morris JE, Povey RC, Street CG. Experiences of people with type 2 diabetes who have changed from oral medication to self-administered insulin injections. Pract Diabetes Int. 2005;22(7):239–243. doi:10.1002/pdi.829
25. Bogatean MP, Hancu N. People with type 2 diabetes facing the reality of starting insulin therapy: factors involved in psychological insulin resistance. Pract Diabetes Int. 2004;21(7):247–252. doi:10.1002/pdi.670
26. Nakar S, Yitzhaki G, Rosenberg R, Vinker S. Transition to insulin in type 2 diabetes: family physicians’ misconception of patients’ fears contributes to existing barriers. J Diabetes Complications. 2007;21(4):220–226. doi:10.1016/j.jdiacomp.2006.02.004
27. Karter AJ, Subramaniam U, Saha C, et al. Barriers to insulin initiation: the translating research into action for diabetes insulin starts project. Diabetes Care. 2010;33(4):733–735. doi:10.2337/dc09-1184
28. Hassan AH, Tohid H, Amin RM, Bidin MBL, Muthupalaniappen L, Omar K. Factors influencing insulin acceptance among type 2 diabetes mellitus patients in a primary care clinic: a qualitative exploration. BMC Fam Pract. 2013;14(1):164. doi:10.1186/1471-2296-14-164
29. Robertson S. Embarrassment and fear of being judged can mean patients lie to their doctors. News-Medical; November 30, 2018. https://imsva91-ctp.trendmicro.com:443/wis/clicktime/v1/query?url=https%3a%2f%2fwww.news%2dmedical.net%2fnews%2f20181130%2fEmbarrassment%2dand%2dfear%2dof%2dbeing%2djudged%2dcan%2dmean%2dpatients%2dlie%2dto%2dtheir%2ddoctors.aspx&umid=BD63F96C-BD3A-C205-BCE5-2947B0E73B41&auth=6e3fe59570831a389716849e93b5d483c90c3fe4-9b8e0a4b26f41b6b783a541a55273ca3302a4932.
30. Kleinsinger F. Working with the noncompliant patient. Perm J. 2010;14(1):54–60. doi:10.7812/TPP/09-064
31. Little P, Everitt H, Williamson I, et al. Observational study of effect of patient centeredness and positive approach on outcomes of general practice consultations. BMJ. 2001;323(7318):908–911. doi:10.1136/bmj.323.7318.908
32. Stewart M, Brown JB, Donner A, et al. The impact of patient-centered care on outcomes. J Fam Pract. 2000;49(9):796–804.
33. Peyrot M, Rubin RR, Kruger DF, Travis LB. Correlates of insulin injection omission. Diabetes Care. 2010;33(2):240–245. doi:10.2337/dc09-1348
34. Farsaei S, Radfar M, Heydari Z, Abbasi F, Qorbani M. Insulin adherence in patients with diabetes: risk factors for injection omission. Prim Care Diabetes. 2014;8(4):338–345. doi:10.1016/j.pcd.2014.03.001
35. Powell PW, Corathers SD, Raymond J, Streisand R. New approaches to providing individualized diabetes care in the 21st century. Curr Diabetes Rev. 2015;11(4):222–230. doi:10.2174/1573399811666150421110316
36. Welch G, Rose G, Ernst D. Motivational interviewing and diabetes: what is it, how is it used, and does it work? Diabetes Spectrum. 2006;19(1):5–11. doi:10.2337/diaspect.19.1.5
37. Mainous A, Koopman G, Gill RJ, Baker R, Pearson WS. Relationship between continuity of care and diabetes control: evidence from the third national health and nutrition examination survey. Am J Public Health. 2004;94(1):66–70. doi:10.2105/AJPH.94.1.66
38. World Health Organisation. Team –Based Care. WHO/NMH/NV1/18.4; 2018.
39. Okazaki K, Shingaki T, Cai Z, Perez-Nieves M, Fisher L. Successful healthcare provider strategies to overcome psychological insulin resistance in Japanese patients with Type 2 diabetes. Diabetes Ther. 2019;10(5):1823–1834. doi:10.1007/s13300-019-0664-9
40. Polonsky WH, Arsenault J, Fisher L, Kushner P, Miller EM, Pearson TL, Tracz M, Harris S, Hermanns N, Scholz BM, Pollom RK, Perez-Nieves M, Pollom RD, Hadjiyianni. (2017).Initiating insulin: How to help people with type 2 diabetes start and continue insulin successfully. Int J Clin Pract 2017 Aug; 71(8). doi: 10.1111/ijcp.12973. Epub 2017 Jul 23. https://www.ncbi.nlm.nih.gov/pubmed/28735508
41. Meece J. Effect of insulin pen devices on the management of diabetes mellitus. Am J Health Syst Pharm. 2008;65(11):1076–1082. doi:10.2146/ajhp070524
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.