Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Where Do Chronic Obstructive Pulmonary Disease Patients Die? 8-Year Trend, with Special Focus on Sex-Related Differences
Authors Fernández-García A, Pérez-Ríos M, Candal-Pedreira C, Represas-Represas C, Fernández-Villar A ![]() , Santiago-Pérez MI, Rey-Brandariz J, Naveira-Barbeito G, Malvar-Pintos A, Ruano-Ravina A
, Santiago-Pérez MI, Rey-Brandariz J, Naveira-Barbeito G, Malvar-Pintos A, Ruano-Ravina A ![]()
Received 12 January 2022
Accepted for publication 3 April 2022
Published 6 May 2022 Volume 2022:17 Pages 1081—1087
DOI https://doi.org/10.2147/COPD.S351259
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Richard Russell
Alberto Fernández-García,1 Mónica Pérez-Ríos,1– 3 Cristina Candal-Pedreira,1,3 Cristina Represas-Represas,4,5 Alberto Fernández-Villar,4,5 María Isolina Santiago-Pérez,1,6 Julia Rey-Brandariz,1 Gael Naveira-Barbeito,6 Alberto Malvar-Pintos,6 Alberto Ruano-Ravina1– 3
1Department of Preventive Medicine and Public Health, University of Santiago de Compostela, Santiago de Compostela, Spain; 2Consortium for Biomedical Research in Epidemiology and Public Health (Ciber en Epidemiología y Salud Pública/CIBERESP), Madrid, Spain; 3Health Research Institute of Santiago de Compostela (IDIS), Santiago de Compostela, Spain; 4Respiratory Medicine, Alvaro Cunqueiro University Teaching Hospital, Vigo, Spain; 5Grupo NeumoVigo I+i, Instituto de Investigación Sanitaria Galicia Sur (IISGS), Vigo, Spain; 6Epidemiology Unit, Galician Health Authority, Xunta de Galicia, Santiago de Compostela, Spain
Correspondence: Mónica Pérez-Ríos, Department of Preventive Medicine and Public Health, University of Santiago de Compostela, C/ San Francisco s/n, Santiago de Compostela, 15782, Spain, Tel +34-981-581237, Fax +34-981-572282, Email [email protected]
Background: To plan end-of-life care it is essential to ascertain where patients die. There is very little information on the place of death of chronic obstructive pulmonary disease (COPD) patients. Accordingly, this study set out to describe the place of death of all COPD-related deaths in a Spanish region across the period 2009– 2017, taking into account the sex and age of the deceased.
Methods: We analyzed COPD deaths, codes J41-44 of the International Classification of Diseases-10th revision, in the Galician Autonomous Region from 2009 to 2017. Using death certificate data furnished by the Galician Mortality Registry, information was extracted on place of death, categorized as “hospital”, “nursing home”, “patient’s home”, “other” or “not shown”.
Results: There were 10,274 deaths, with a male:female ratio of 2.52; 39.0% of deaths occurred in hospital and 41.4% at home, with these data varying according to sex and age. Across the study period, no reduction was observed in the number of deaths that occurred in hospital. For all the period analyzed, deaths among women occurred mostly at home, with an increase being seen in the number of deaths in nursing homes over the course of the study. Patients aged under 70 years tended to die more frequently in hospital, and those over this age died more frequently at home or in nursing homes.
Conclusion: A very high percentage of COPD patients still die in hospital, a trend that has shown no decline in recent years. Even so, there are important variations by sex and age on the place of death of these patients.
Keywords: pulmonary disease, chronic obstructive, death, hospital
Introduction
Chronic obstructive pulmonary disease (COPD) is currently one of the most common diseases and, due to aging, its impact on the population is expected to increase in the coming years.1,2 COPD is defined as a preventable and treatable disease, characterized by the presence of persistent symptoms and limitation of airflow due to anomalies in the respiratory tract or at an alveolar level. It is a leading cause of death at a global level, being estimated to account for approximately 3 million deaths annually.3 Each year around 18,000 persons die due to COPD4 in Spain, which ranks it as the fifth leading cause of death in men and the seventh in women.5,6 While the World Health Organization estimates in the early part of this century indicated an increase in COPD mortality, recent studies based on official records have reported a downward trend since the mid-1990s.7–9 However, it is not clear if there is an actual reduction in COPD mortality or if this decrease is related to methodological problems of these studies.10
Although it is a frequent disease, little is known about the place of death of COPD patients. In many cases, the disease’s characteristics, essentially its chronicity and prognostic uncertainty, make palliative care necessary, as a way of improving the symptomatology, and of halting and treating the frequent exacerbations that such patients experience. To be able to plan appropriate healthcare and end-of-life focused strategies, it is essential to have updated information on where COPD patients die. Place of death is a basic standard of quality of care, which has a marked impact on the patient and involves what is understood as a dignified death.11–13 In the case of COPD, however, very few studies have analyzed place of death. One study on the place of death of these patients, which was undertaken in 14 countries, including Spain, and published in 2017, yielded highly heterogeneous results, reporting that 10% to 70% of patients die in hospital.14 In the case of Spain, there is no detailed information on the place of death of COPD patients. Furthermore, it is to be expected that in recent years, with the implementation of home hospitalization services and palliative care, the percentage of COPD patients dying in a hospital setting should have declined.
The main aim of this study was therefore to describe the place of death of all COPD-related deaths in a Spanish region across the period 2009–2017, by reference to sex and age group.
Methods
Study Design and Setting
Galicia is a region situated in northwest Spain with a population of 2,701,819. It has universal health coverage, and approximately half of the population lives in a rural setting. It was one of the first European regions to implement electronic medical records. According to EPISCAN II study data, COPD prevalence stands at 10.2% in women and 22.8% in men, with 72.8% of all COPD sufferers being undiagnosed. Based on these prevalences, it is estimated that in Galicia should be 232,000 patients with COPD among the population aged 40 years and over.15
Data Source
We obtained from the Galician Mortality Registry all medical death certificate-statistical deaths bulletin with COPD coded as basic cause of mortality (codes J41-J44) under the International Classification of Diseases-10th revision (ICD-10). Deaths occurred among residents of the Galician Autonomous Region aged 35 years and over, across the period 2009–2017. Data on place of death, categorized as “hospital”, “nursing home”, “patient’s home”, “other” or “not shown”, were extracted from the medical death certificate-statistical deaths bulletin. Under the “not shown” category, we included unknown options and registrations left blank in this respect.
Statistical Analysis
We conducted a descriptive analysis of COPD-related deaths in Galicia, calculating the crude rates by year, sex, and age group (35–69, 70–79, and 80 years and over). To calculate these rates, annual population data were obtained from the Annual Electoral Roll Update, as sourced from the Galician Statistics Institute. The annual percentages of deaths were calculated by place of death, both overall and by sex and age group, using the following age categories: 35–69 years; 70–79 years; and 80 years and over.
Results
In Galicia, there were 10,274 deaths due to COPD across the period 2009 through 2017, which amounted to an annual mean rate of 62.2 cases per 100,000 inhabitants. The breakdown by year showed that the maximum rate was observed in 2012 (70.3 deaths per 100,000) and the minimum in 2014 (53.7). In terms of sex, 71.6% of all COPD deaths occurred in men (7361) and 28.4% in women (2913), with rates of 95.1 and 33.2 cases per 100,000, respectively, and a rates ratio of 2.9. During the study period, COPD mortality rates rose with age, going from 6.5 cases per 100,000 in the 35–69 age group to 397.0 per 100,000 in the 80-and-over age group (Table 1). Under the age of 45 years, mortality was incidental, with only 7 deaths recorded.
 |
Table 1 Number of Deaths and Mortality Rate Due to Chronic Obstructive Pulmonary Disease (COPD) Mortality Rate, Number of Deaths by Place Where Death Occurred, and Number of Certificates Containing No Information About Place of Death, Plus the Percentage That These Deaths Represent with Respect to Total COPD-Related Deaths |
Of the total number of COPD deaths registered in Galicia between 2009 and 2017, 9158 (89.1%) showed the place of death and 1116 (10.9%) did not show this information. The percentage of certificates without a recorded place of death was 63.3% in 2009, when these data started being shown on the death certificate, and fell to 14.0% in 2010. Thereafter, the “not shown” percentage varied from 5.2% in 2011 to 0.9% in 2013. Overall, there was no difference in compliance with place-of-death registration between men and women, while a breakdown by age group indicated that the “not shown” percentage was higher in the youngest age group, ie, 35–69 years (Table 1).
For analysis purposes, deaths in which the place of death was not shown were excluded. In all, 46.4% of COPD-related deaths in the period 2009–2017 occurred at home, 43.8% in hospital, and 9.3% in nursing homes; only 0.5% died elsewhere (Table 1). Place of death varied according to sex and age group, as can be seen in Figure 1, which shows the percentage distribution of deaths according to place of death, for each year across the period 2010–2017. In the calculation, 2009 was excluded for having a very high “not shown” percentage. In any given year of the study period, hospital was the place where deaths among men mainly occurred; among women however, it was home where deaths mainly occurred, though the percentage of deaths at home across the study period decreased, with a rise of 9.9 percentage points being observed in nursing home mortality. This increase of 3.8 percentage points was likewise seen in men. In terms of age, while the population aged 35 to 69 years was most likely to die in hospital, the population aged 70 years and over was most likely to die at home, though the differences were smaller.
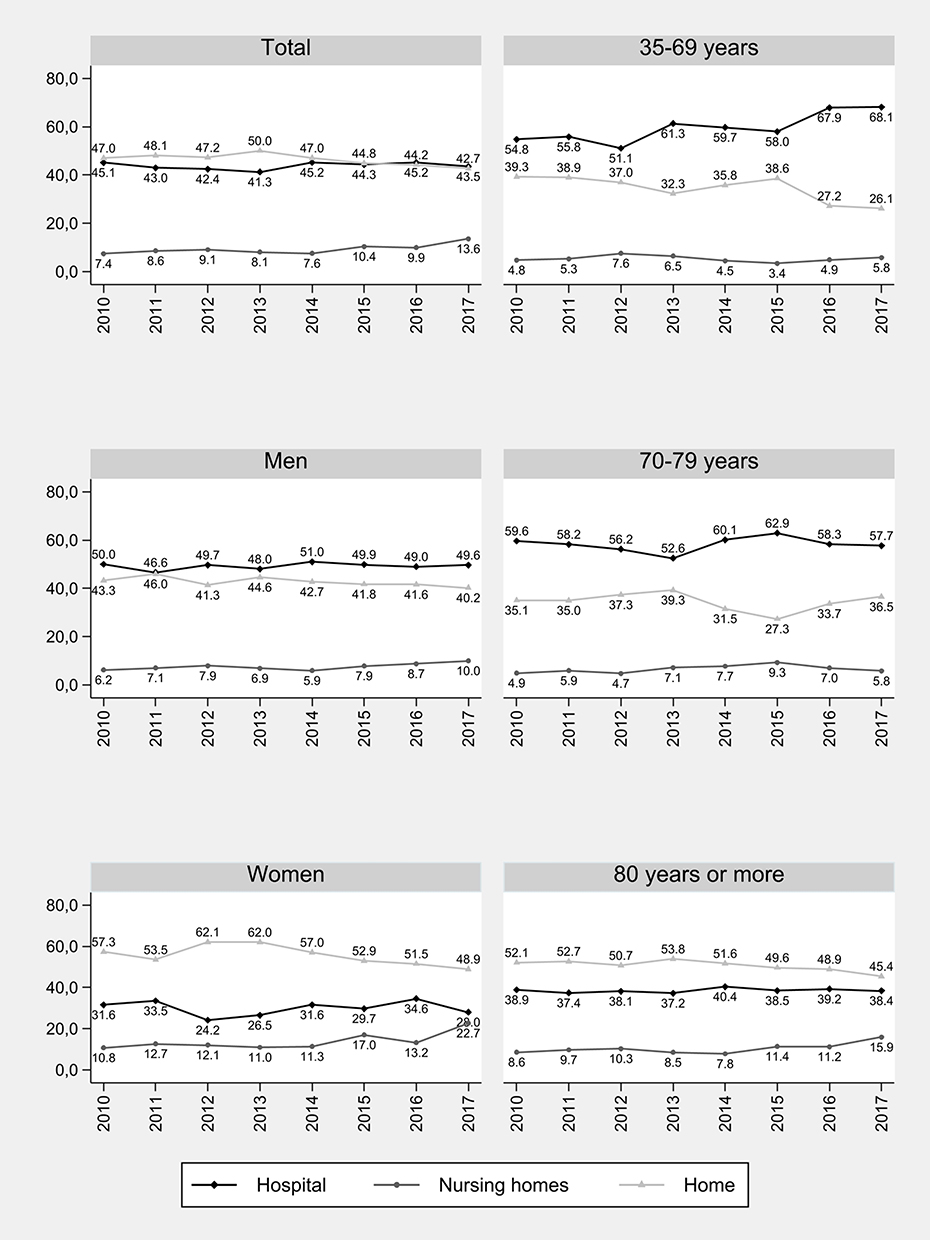 |
Figure 1 Percentage of deaths according to place of death, by sex and age group: 2010–2017. |
Discussion
This is one of the few European studies to analyze place of death in COPD patients, and the first to analyze this aspect in Spain, along with changes that have taken place over time. More than 40% of all COPD-related deaths occur in the hospital setting, with this percentage rising to 50% in men, without any appreciable change in the trend to die in hospital in the last 9 years. There is a difference between the sexes in the percentage of deaths which occur at home, with these being more frequent among women. In some of the years analyzed, the percentage of men who died in hospital was double that of women. As age of death rises, the likelihood of dying outside the hospital setting also rises. Moreover, the study period showed an increase in the number of COPD-related deaths in nursing homes. Since 2009, the year in which place of death was included on the death certificate, there has been an improvement in the collection of this information, to the extent that in the last year of study it was available in 97% of certificates.
Dying at home would seem to be the most frequent preference among patients with advanced disease status, among carers, and among the general population, being regarded as an indicator of quality of end-of-life care.16,17 While the Spanish Society for Palliative Care (Sociedad Española de Cuidados Paliativos/SECPAL) has no specific guideline that makes provision for evaluating place of death in the case of chronic patients, it does address certain aspects relating to this. Patients have a right to healthcare, even where curative care goals are replaced by comfort goals, as well as a right to exercise a decision-making capacity in respect of matters such as the place where they choose to die. Regardless of whether a person is staying in his/her own home, an institution (long-stay centers, nursing homes) or an acute-care hospital, there are situations where decisions must be taken pertaining to the level of intervention and end-of-life stage. Hence, the principle of autonomy is important, and implies respecting the considerations of autonomous persons and favoring situations in which such persons can express their opinions, so that these can then be taken into account when they are no longer able to exercise their own decision-making capacity. In this regard, informed consent and advance directive documents (the so-called “living will”) are really useful. The patient or, in default, his/her family has the capacity to take decisions involving the type of clinical approach to be adopted (palliative or curative), the intensity of interventions, the patient’s location for care purposes, and the place where his/her life can draw to a close.18 Yet, unlike what happens in English-speaking countries, the implementation of such advance directive documents or prior orders, albeit available in most Spanish regions, is generally very low, with an overall incidence of 4.52 per 1000 inhabitants, though implementation has been observed to rise with increasing age.19
In this study, approximately 40% of men and 50% of women, a figure that exceeded 60% in 2012 and 2013, died in their homes. This percentage is higher than that reported in the studies reviewed (which included patients of different ages and with different diseases), and in no case exceeded 30%.20–23 However, a study conducted in Andalusia in 2011 and not focused on COPD, concluded that the higher the age, the higher the number of deaths at home and in nursing homes, as opposed to hospitals, with both results agreeing with those of our study.24 Furthermore, a study on all-cause deaths in Belgium shows that, though palliative care increased from 18.3% in 1998 to 22.6% in 2007, hospital deaths decreased, going from 55.1% in 1998 to 51.7% in 2007.25 This result is not in line with those of our study, in which deaths in the hospital setting remain stable, both when analyzed by sex and by age group.
In the USA, a study which, in addition to COPD mortality, included deaths due to other respiratory causes, concluded that in recent years the number of deaths in hospital had decreased (44.4% in 2003 versus 28.3% in 2017), leading to an increase in deaths at home (23.3% in 2003 versus 34.7% in 2017).14 This may perhaps relate to the healthcare model in that country, which is different to European models. In our study, however, no increase in mortality at home was observed, which may possibly reflect a lack of information and adequate infrastructure, and which, in turn, often leads to families being “conditioned” to decide that the death will take place at the hospital, inasmuch as care tends to be provided in a hospital context. The palliative care guidelines recommended by Spanish societies for chronic diseases, COPD among them, lay down that, where possible, the home is the ideal place to treat patients with advanced chronicity until the end of their lives, including death.26 A Canadian study observed that palliative care was far less frequent in patients with COPD than in patients with lung cancer (20% in COPD versus 57% in cancer).27 In that study, 53% of patients with COPD died in acute care, 7.4% in sub-acute care, 18.2% in long-term care, and 20.8% in the community. A Spanish study which was undertaken in the hospital setting and included 66 patients registered in a home-based palliative care program, observed that 85% of these patients died at home or in a palliative care unit.28
A recent study which analyzes the place of death of patients dependent on palliative care and differentiates between oncological and non-oncological diseases, concludes that in the latter case, deaths largely tend to occur in the hospital setting, increasing the likelihood of dying at home in the case of oncological diseases.29
In another study, however, which included data on 14 countries, including Spain, and analyzed place of death due to COPD and lung cancer, the results obtained for COPD in Spain are in great measure comparable with those of this study. Nonetheless, it should be noted that the proportion of home-based deaths is slightly lower in cancer, a finding that contradicts what has been stated above. This may be due to the fact that the study was conducted in 2008, and that the trend toward the use of palliative care and the occurrence of death in the home setting is a measure which began to be implemented relatively recently.14
Analysis of place of death due to COPD highlights the fact that actions are needed to foster the home hospitalization of patients with COPD, along with better briefing and preparation of families for when the moment of death arrives. Unlike oncological diseases, it should be borne in mind that in patients with advanced or end-stage COPD, the disease course is complex, heterogeneous, and in certain cases somewhat unpredictable, which implies difficulties in establishing an accurate prognosis and indicating the point at which palliative needs should progressively replace conventional treatment.17
This study describes differences by sex and age, such that women with COPD and from a lower age tend to die more frequently outside the hospital setting. This finding is in line with O’Dowd’s conclusion to the effect that the trend to die in hospital increases with age and among males.18
In Galicia, the number of residential places in social service providers in 2018 was 22,123, which amounts to a percentage occupation of 95.7%. A total of 59.7% of residential places are occupied by persons aged over 80 years (67.4% women and 47.1% men).30 This might account for the differences observed in the percentage of women who die in nursing homes.
Among the advantages of our study, it should be noted that all deaths coded as COPD were comprehensively analyzed in a region that has a population of close on 3 million. The period analyzed spanned almost 10 years and the data were sourced from a registry with universal coverage: this ensures the representativeness of the study, since in reality there was no sampling, with the study instead including all COPD-related deaths recorded during the period analyzed.
Our study is not free of limitations. Although specific information on place of death was obtained from the death certificate, there was a lack of other data, such as the treatments applied, disease exacerbations, related admissions and re-admissions, number of days at place of death, and/or whether these patients had received palliative care from the relevant home hospitalization service. The impact of “not shown place” in the mortality registration is negligible from 2012 onwards but it is unknown in 2010 and 2011.
In conclusion, no important changes were observed in the place of death of COPD patients in the last 10 years, something that may reflect inadequate implementation of end-of-life care among these patients. Changes in the place of death by sex and age should be borne in mind. The improvement in the recording of place of death on death certificates is evident, though there is still room for improvement, particularly in the case of the population aged under 70 years. Further studies are required to reinforce these results, and make health decision-makers aware of the need to introduce the changes required to enable COPD patients to die in their own homes with the best possible care available.
Ethics Statement
Based on Article 1 in the “Decreto 63/2013, de 11 de abril, por el que se regulan los comités de ética de la investigación en Galicia”, we do not need formal ethics approval since this study is not research on human participants including identifiable human material or identifiable data.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Working group of the GesEPOC. Clinical practice guideline for the diagnosis and treatment of patients with Chronic Obstructive Pulmonary disease (COPD)-The Spanish COPD Guideline (GesEPOC). Arch Bronconeumol. 2017;53(Supl 1):1–64.
2. 2020 GOLD Report. Global strategy for prevention, diagnosis and management of COPD. Available from: https://goldcopd.org.
3. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: global burden of disease study. Lancet. 1997;349(9064):1498–1550. doi:10.1016/S0140-6736(96)07492-2
4. Centro Nacional de Epidemiología. Instituto de Salud Carlos III. Mortalidad España y Comunidades Autónomas. Mortalidad por causas y sexo (1989–1998) [Mortality by cause and gender (1989-1998)]. Available from: http://cne.isciii.es/mortal/mortal98/Cau8098.html.
5. INE. Defunciones por enfermedades respiratorias de vías bajas [Deaths due to lower respiratory tract diseases]; 2016. Available from: http://www.ine.es/jaxiT3/Tabla.htm?t=9936.
6. Fernández-García S, Represas-Represas C, Ruano-Raviña A, et al. Dependence IN performing activities as a predictor of mortality following hospitalization for Chronic Obstructive Pulmonary Disease exacerbation. Arch Bronconeumol. 2020;56(5):291–297. doi:10.1016/j.arbres.2019.10.005
7. López-Campos JL, Ruiz-Ramos M, Soriano JB. Mortality trends in chronic obstructive pulmonary disease in Europe, 1994–2010: a joinpoint regression analysis. Lancet Respir Med. 2014;2(1):54–62. doi:10.1016/S2213-2600(13)70232-7
8. Lortet-Tieulent J, Soerjomataram I, López-Campos JL, et al. International trends in COPD mortality, 1995–2017. Eur Respir J. 2019;54(6):1901791. doi:10.1183/13993003.01791-2019
9. Fernández-García A, Pérez-Rios M, Fernández-Villar A, et al. Four decades of COPD mortality trends: analysis of trends and multiple causes of death. J Clin Med. 2021;10(5):1117. doi:10.3390/jcm10051117
10. Represas-Represas C, Ruano-Raviña A, Fernández-Villar A. Changes in Chronic Obstructive Pulmonary Disease mortality trends: fact or fiction? Arch Bronconeumol. 2014;50(8):311–312. doi:10.1016/j.arbr.2014.06.008
11. Harding R, Marchetti S, Onwuteaka-Philipsen BD, et al. Place of death for people with HIV: a population-level comparison of eleven countries across three continents using death certificate data. BMC Infect Dis. 2018;18(1):55. doi:10.1186/s12879-018-2951-x
12. Badrakalimuthu V, Barclay S. Do people with dementia die at their preferred location of death? A systematic literature review and narrative synthesis. Age Ageing. 2014;43(1):13–19. doi:10.1093/ageing/aft151
13. Teno JM, Gozalo PL, Bynum JP, et al. Change in end-of-life care for Medicare beneficiaries: site of death, place of care, and health care transitions in 2000, 2005 and 2009. JAMA. 2013;309(5):470–477. doi:10.1001/jama.2012.207624
14. Cohen J, Beernaert K, Van den Block L, et al. Differences in place of death between lung cancer and COPD patients: a 14-country study using death certificate data. NPJ Prim Care Respir Med. 2017;27(1):14. doi:10.1038/s41533-017-0017-y
15. Soriano JB, Alfageme I, Miravitlles M, et al. Prevalence and Determinants of COPD in Spain: EPISCAN II. Arch Bronconeumol. 2020;57(1):61–69.
16. Gomes B, Calanzani N, Gysels M, et al. Heterogeneity and changes in preferences for dying at home: a systematic review. BMC Palliat Care. 2013;12(1):7. doi:10.1186/1472-684X-12-7
17. Cross SH, Ely EW, Kavalieratos D, et al. Place of death for individuals with chronic lung disease. trends and associated factors from 2003 to 2017 in the United States. Chest. 2020;158(2):670–680. doi:10.1016/j.chest.2020.02.062
18. SECPAL. Problemas éticos al final de la vida [Ethical issues at the end of life]. Available from: https://www.secpal.com/problemas-eticos-al-final-de-la-vida.
19. Arimany J, Aragonés L, Gómez E, et al. El testamento vital o documento de Voluntades Anticipadas. Consideraciones médico-legales y análisis de la situación de implantación en España [The living will or advance directives. Medical-legal considerations and analysis of the status of implementation in Spain]. Rev Esp Med Legal. 2017;43(1):35–40. Spanish.
20. Ohlén J, Cohen J, Hakanson C. Determinants in the place of death for people with different cancer types: a national population-based study. Acta Oncol. 2017;56(3):455–461. doi:10.1080/0284186X.2016.1250946
21. Dasch B, Blum K, Gude P, et al. Place of death: trends over the course of a decade: a population-based study of death certificates from the year 2001 and 2011. Dtsch Arztebl Int. 2015;112(29–30):496–504. doi:10.3238/arztebl.2015.0496
22. MacNeil Vroomen JL, Kjellstadli C, Allore HG, et al. Reform influences location of death: interrupted time-series analysis on older adults and persons with dementia. PLoS One. 2020;15(11):e0241132. doi:10.1371/journal.pone.0241132
23. O´Dowd EL, McKeever T, Baldwin DR, et al. Place of death in patients with lung cancer: a retrospective cohort study from 2004–2013. PLoS One. 2016;11(8):e0161399.
24. Ruiz-Ramos M, García-León FJ, Méndez-Martínez C. El lugar de muerte en Andalucía: influencia de la edad, sexo y causa de defunción [Place of death in Andalusia: influence of age, gender and cause of death]. Rev Clin Esp. 2011;211(3):127–132. Spanish. doi:10.1016/j.rce.2010.10.006
25. Houttekier D, Cohen J, Surkyn J, et al. Study of recent and future trends in place of death in Belgium using death certificate data: a shift from hospital to care homes. BMC Public Health. 2011;11(1):228. doi:10.1186/1471-2458-11-228
26. SECPAL. Monografía SECPAL de cronicidad Avanzada [Monograph SECPAL on Advance Chronicity]. Available from: http://www.secpal.com//Documentos/Blog/Monografia%20Cronicidad.pdf.
27. Kendzerska T, Nickerson JW, Hsu AT, et al. End-of-life care in individuals with respiratory diseases: a population study comparing the dying experience between those with chronic obstructive pulmonary disease and lung cancer. Int J Chron Obstruct Pulmon Dis. 2019;14:1691–1701. doi:10.2147/COPD.S210916
28. Gainza-Miranda D, Sanz-Peces EM, Alonso-Babarro A, et al. Breaking barriers: prospective study of a cohort of advanced Chronic Obstructive Pulmonary Disease patients to describe their survival and end-of-life palliative care requirements. J Palliat Med. 2019;22(3):290–296. doi:10.1089/jpm.2018.0363
29. Cabañero-Martínez MJ, Nolasco A, Melchor I, et al. Place of death of people with conditions needing palliative care in the different autonomous communities (regions) of Spain. An Sist Sanit Navar. 2020;43:1.
30. Instituto Galego de Estadística. Enquisa a entidades prestadoras de servizos sociais [Survey of social service providers]; 2021. Available from: http://www.ige.eu/estatico/html/gl/OperacionsEstruturais/Resumo_resultados_Enquisa_Entidades_Servizos_Sociais.html.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.