Back to Journals » Journal of Pain Research » Volume 16
What is “Opioid Stewardship”? An Overview of Current Definitions and Proposal for a Universally Acceptable Definition
Authors Shrestha S ![]() , Khatiwada AP, Sapkota B
, Khatiwada AP, Sapkota B ![]() , Sapkota S, Poudel P
, Sapkota S, Poudel P ![]() , KC B, Teoh SL, Blebil AQ, Paudyal V
, KC B, Teoh SL, Blebil AQ, Paudyal V ![]()
Received 9 September 2022
Accepted for publication 19 January 2023
Published 10 February 2023 Volume 2023:16 Pages 383—394
DOI https://doi.org/10.2147/JPR.S389358
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Twillman
Video abstract presented by Sunil Shrestha.
Views: 303
Sunil Shrestha,1 Asmita Priyadarshini Khatiwada,2 Binaya Sapkota,3 Simit Sapkota,4,5 Prabhat Poudel,6 Bhuvan KC,7,8 Siew Li Teoh,1 Ali Qais Blebil,1 Vibhu Paudyal9
1School of Pharmacy, Monash University Malaysia, Jalan Lagoon Selatan, Bandar Sunway, Selangor, 47500, Malaysia; 2Department of Health Outcomes Research and Policy, Harrison College of Pharmacy, Auburn University, Auburn, AL, USA; 3Department of Pharmaceutical Sciences, Nobel College, Kathmandu, Nepal; 4Department of Clinical Oncology, Civil Service Hospital, Minbhawan, Kathmandu, Bagmati Province, Nepal; 5Department of Clinical Oncology, Kathmandu Cancer Center, Tathali, Bagmati Province, Nepal; 6Nepal Medical College Hospital, Kathmandu, Province Bagmati, Nepal; 7College of Public Health, Medical & Veterinary Sciences, James Cook University, Townsville, QLD, Australia; 8Faculty of Pharmacy and Pharmaceutical Sciences Monash University Parkville Campus Parkville, Melbourne, VIC 3052, Australia; 9School of Pharmacy, College of Medical and Dental Sciences, University of Birmingham, Birmingham, UK
Correspondence: Sunil Shrestha; Vibhu Paudyal, Tel +60 102874113, Email [email protected]; [email protected]; [email protected]
Introduction: Opioid stewardship has been widely used to promote rational use, monitoring and discontinuation of opioid therapy; however, its definition and scope of practice remain unclear.
Objective: To synthesize definitions of opioid stewardship proposed by clinical practice guidelines and professional societies, and to offer a proposal for a universally acceptable definition.
Methods: Systematic literature searches were performed (earliest records to May 2022) in six databases (MEDLINE, EMBASE, APA PsycINFO, Scopus, and CENTRAL) and grey sources guidelines development bodies and professional societies through Google. The conventional but widely applied content analysis and word frequencies were used to analyze the definitions and scope of practice.
Results: After removing duplicates, 449 articles were retrieved (439 databases and registers and 11 from other sources), 19 of which included a definition of “opioids stewardship”. A total of 12 themes was identified in the definitions, including 1) improvement or appropriateness of prescribing opioids use, 2) mitigation of risk from opioids, 3) monitoring opioid use, 4) evaluation of opioid use, 5) judicious opioid use, 6) appropriateness of opioid disposal, 7) identification and treatment of opioid use disorder, 8) reduction in mortality associated with opioid overdoses, 9) appropriate procurement practices, 10) appropriate storage, 11) promoting better communications between patients and prescribers including education provision and 12) patient-centered decision-making.
Conclusion: Opioid stewardship is inconsistently defined across professional and research literature. While there is a greater focus on appropriateness and need for improvement of prescribing and monitoring of opioid use, the importance of communications between patients and prescribers, and patient involvement in both prescribing and deprescribing decision-making remains sparse. A comprehensive definition has been proposed as part of the work. There is a need to develop and validate the proposed definition and scope of practice to promote rationale for opioid prescribing, use and attainment of favourable outcomes through international consensus involving practitioners, researchers, and patients.
Keywords: opioid, opioid stewardship, opioid stewardship definition, stewardship
Background
Opioids are widely used for chronic pain management globally.1 However, suboptimal use can lead to unwanted economic, clinical, and humanistic outcomes. The opioid epidemic in the US has further prompted the need to promote rational prescribing and use.2,3 Internationally, the rising trend in opioid use has been reported, particularly in the UK, mainland Europe,4 Australia,5 and New Zealand.6 In addition, restriction measures around access to prescribed opioids which do not consider patient priorities, are also linked to the illicit use of non-prescribed opioids.7,8
The concept of opioid stewardship is based upon the principles of the antibiotic stewardship program that focuses on the right medication use for the right patient at the right time.9,10 Opioid dependence, misuse and deaths are key consequences of irrational use, with data globally suggesting the trend in adverse outcomes correlates with increasing use.11–13 Therefore, it is crucial to rationalize the use of opioids to prevent avoidable adverse events, dependency and addiction. An opioid stewardship program is one strategy to ensure the safe and effective utilization of opioids.10 Opioid stewardship, if defined uniformly, will help promote medicine optimization and risk-taking behaviours and reduce adverse outcomes, including associated morbidity and mortality.9
Various guidelines and policies have been developed and implemented across the globe to reduce opioid-related morbidity and mortality and to promote their better use in pain management.14 Some policies overlook opioid prescribing practices and opioid stewardship around the world, including tailored prescribers’ education.15 In addition, stewardship programs can incorporate the concept of shared decision-making to promote better utilization of the prescribed opioids among the patient population.16 However, there is a lack of an established definition and scope of practice referring to opioid stewardship.15 Considering the varying concept of opioid stewardship, this systematic review aimed to synthesize definitions of “opioid stewardship” proposed by clinical practice guidelines and professional societies and propose a universally acceptable definition.
Methods
Design
This review looked at definitions of opioid stewardship proposed by clinical practice guidelines and professional societies, and was performed following the principles outlined in the Cochrane Handbook for Systematic Reviews of Interventions.17 The reporting of this review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines (PRISMA 2020 Checklist is available in Supplement File).18
Search Strategy, Selection Criteria, and Data Sources
Electronic databases Medical Literature Analysis and Retrieval System Online [MEDLINE (Ovid)], Excerpta Medica (EMBASE), American Psychological Association (APA) PsycINFO, Scopus and Central Register of Controlled Trials (CENTRAL), were searched between 1 January 2000 and 30 May 2022 with the Medical Subject Headings or MESH and keywords related to “opioid stewardship”, ie, (opioid stewardship OR (opioid AND stewardship) OR (opioid adj3 stewardship)) AND (defin* OR explan* OR scope). The search included journal articles and grey literature sources, including Google and professional society webpages.
Resources using the term opioid stewardship anywhere in the text, including abstract, titles and full texts, guidelines or websites, and definitions proposed for the term “opioid stewardship” (as determined by two independent reviewers) were included in this study. Non‐English articles and the resources that used the term in the reference list were excluded. There were no specific interventions/exposures, as this was a review of definitions and scope of Opioid stewardship’ used by different research papers.
A grey literature search plan was developed to incorporate three different search strategies: 1) grey literature databases, 2) customized Google search engines, and 3) targeted websites.
Data Extraction
Studies were imported to the COVIDENCE online screening program, and study titles/abstracts were screened for inclusion by two reviewers SS and APK. Discrepancies were settled by discussion and consensus, with the mediation by other reviewers, VP and AQB. The study characteristics and definitions of “opioid stewardship” were extracted using a Microsoft Excel 365 spreadsheet as a proforma. The details of the PRISMA flow diagram results of the literature search are illustrated in Figure 1.
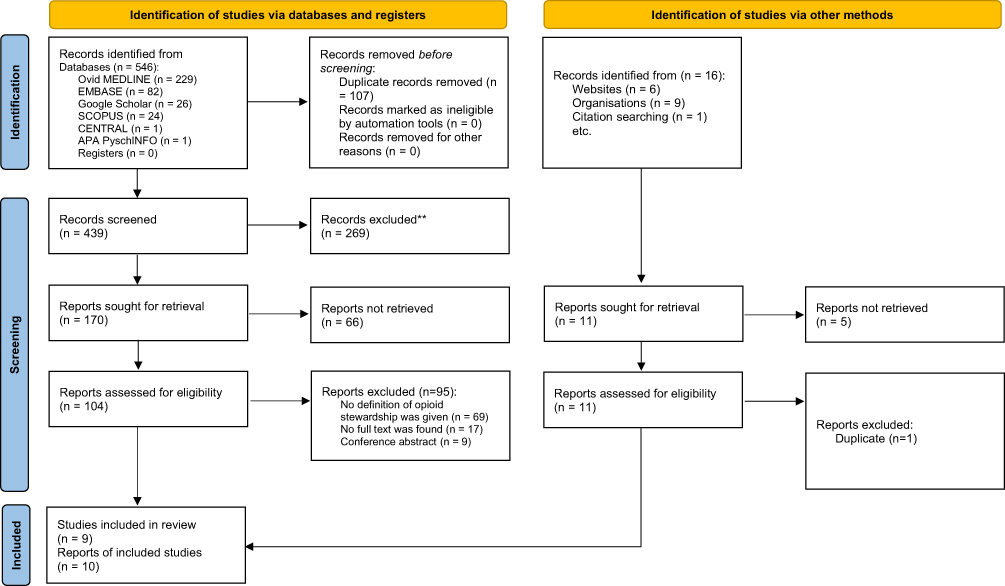 |
Figure 1 Preferred reporting items for systematic reviews and meta-analysis flow chart. Notes: Adapted from Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Annals of internal medicine. 2009;151(4):264–269. Creative Commons.18 |
Primary Outcome
The primary outcome of the current study is related to the scope of definitions of’ Opioid Stewardship’ as reported by the clinical practice guidelines and professional societies.
Conventional Content Analysis
All the study team members reviewed the extracted definitions from different resources, and characteristics were identified via conventional content analysis.19 Three research team members (SS, APK, VP) read the definition of opioid stewardship from the included sources and generated a list of codes. Differences in codes were reviewed for each definition of opioid stewardship, and any differences were resolved code-by-code. SS, APK and VP reviewed the remaining documents for the definition of opioid stewardship. The codebook was updated as new codes emerged via an agreement between all three researchers. SS and APK put the quotes into broader themes. BKC, SS and APK reviewed the themes generated. BKC and VP did the final analysis of the themes to provide a suitable context and background. Thematic saturation was reached when non-new codes were observed from the data.
Results
Identification and Selection of Studies
The details of the PRISMA flow diagram with the results of the literature search are illustrated in Figure 1. After removing duplicates, searching the published articles in various databases and registers yielded 439 articles within the study mentioned above. Additionally, 11 were identified by a manual search of the related websites, organizations, relevant review articles, and references. Nineteen definitions from different sources were included in this systematic review of qualitative data synthesis (Figure 1).
Included Sources
Out of 18 sources, 9 definitions were suggested by the researchers,9,20–27 and 10 definitions were identified from clinical practice guidelines and professional societies.13,28–34 The definition of opioid stewardship, “Coordinated interventions designed to improve, monitor, and evaluate the use of opioids in order to support and protect human health” is used by the researcher, Sandbrink25 and two organizations such as Queensland Opioid Stewardship Program (QOSP)33 and Institute for Safe Medication Practices (ISMP) Canada.31 Similarly, another definition of opioid stewardship, ie, “Opioid analgesic stewardship involves supervising or taking care of opioid analgesics and applies a systematic approach to optimising the use of opioid analgesics. This extends to appropriate and safe use of opioid analgesics, with effective monitoring and surveillance” was used by Uritsky9 and another two organizations and guidelines, Australian Commission on Safety and Quality in Health Care35 Safer Care Victoria.34 The definition “Opioid stewardship refers to a series of strategies and interventions involving the appropriate procurement, storage, prescribing and use of opioids, as well as the disposal of unused opioids when opioids are appropriately prescribed for the treatment and management of specific medical condition” was adopted by World Health Organization (WHO);30 and the Australian and New Zealand College of Anaesthetists including the Faculty of Pain Medicine32 used the same definitions. The definition suggested by Opioid Prescribing Toolkit. Metro North Hospital and Health Service: Brisbane referred to Opioid stewardship being a co-ordinated approach to ensuring the appropriate use of opioids – delivering adequate analgesia to patients whilst minimising harm by monitoring, evaluating, and improving practice.
The overview of definitions given by the researchers and societies is depicted in Table 1. Other websites use some definitions available here for pain or opioid-related societies.
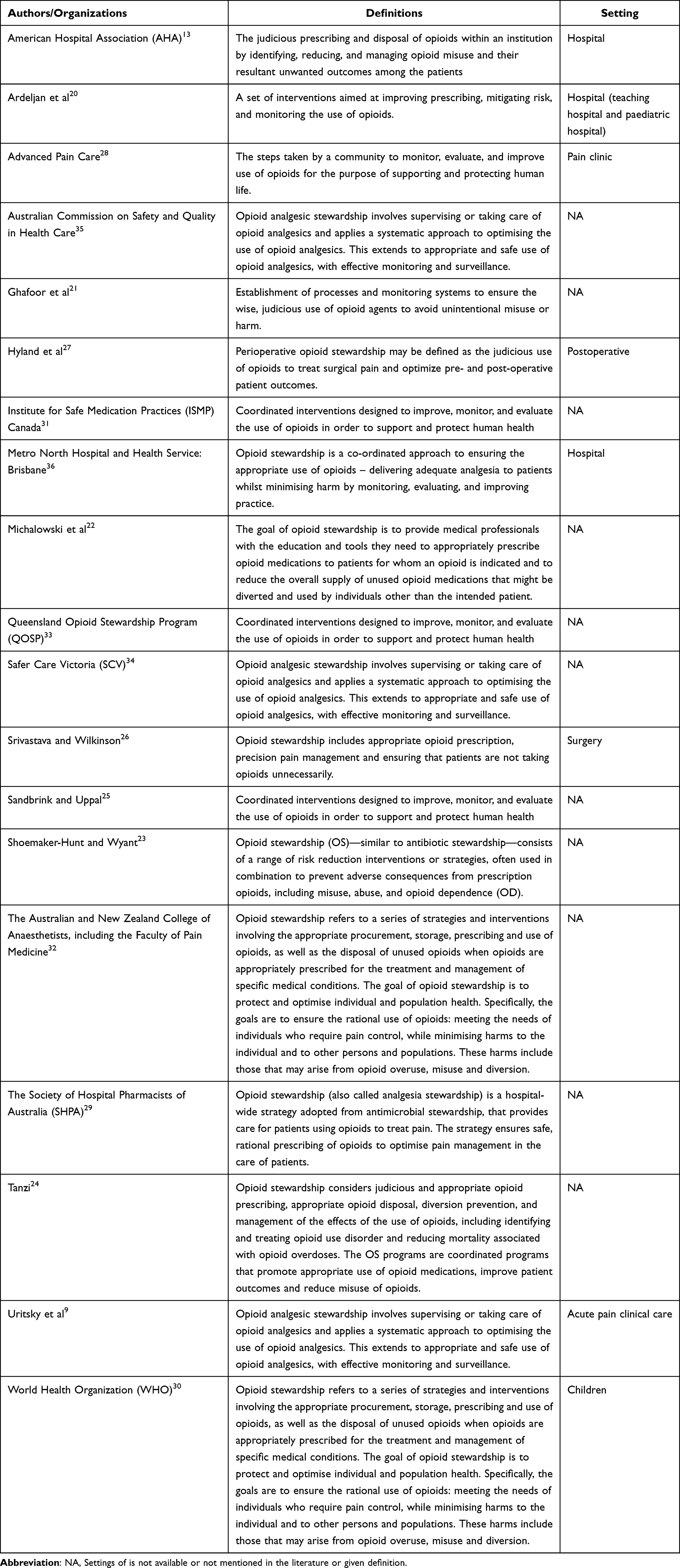 |
Table 1 Overview of Definitions of Opioid Stewardship |
Themes Extracted from the Definition of “Opioid Stewardship”
Definitions provided for “opioid stewardship” were divided into 12 different themes: 1) improvement or appropriateness of prescribing opioids use, 2) mitigation of risk from opioids, 3) monitoring opioid use, 4) evaluation of opioid use, 5) judicious opioid use, 6) appropriateness of opioid disposal, 7) identification and treatment of opioid use disorder, 8) reduction in mortality associated with opioid overdoses, 9) appropriate procurement practices, 10) appropriate storage of opioids, 11) promoting better communications between patients and prescribers including education provision and 12) patient-centered decision-making (Table 2).
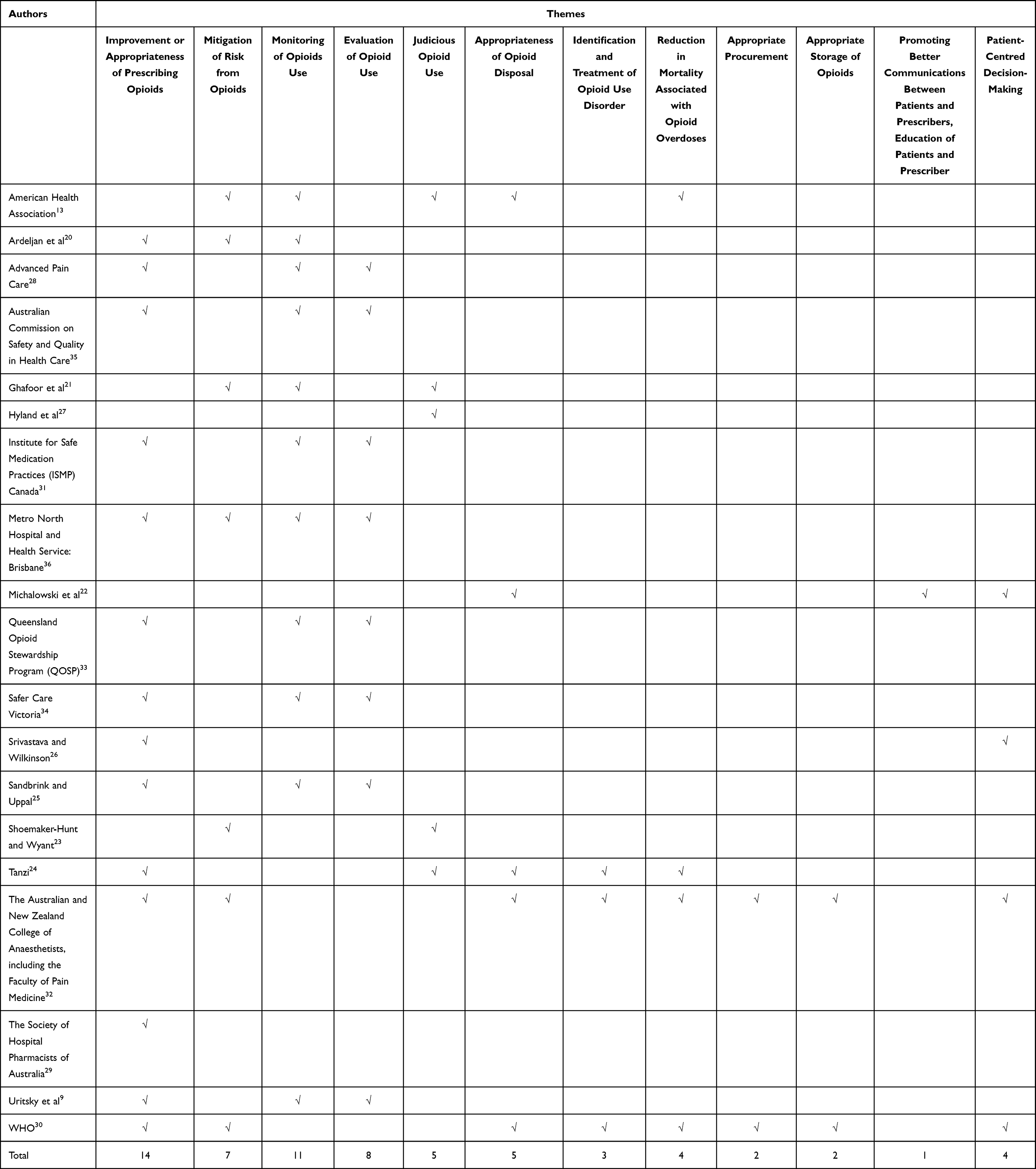 |
Table 2 Different Extracted Themes from the Definition of “Opioid Stewardship” |
The theme “Improvement or appropriateness of prescribing opioids” was found to be focused on in most of the definitions (14/19), which was followed by other themes “Monitoring opioids use” (11/19) and “Evaluation of opioids use” (8/19). The theme “Promoting better communications between patients and prescribers, education of patients and prescriber” was less focused (1/19).
Discussion
This systematic review aimed to review opioid stewardship definitions proposed by the clinical practice guidelines, professional societies, and researchers across healthcare settings. Opioids are mostly prescribed for patients with chronic and cancer pain management. Moreover, opioids are frequently used in acute pain management in in-patients and postsurgical interventions or post-emergency department discharge. Risks of adverse events from opioids are also prevalent in acute use.36,37 Opioids may lead to systemic adverse effects in the gastrointestinal, respiratory, cardiovascular, musculoskeletal, endocrine, and immune systems, and addiction and misuse in non-hospital and hospital practice.38–40 Prescribing opioids even during hospital discharge can lead to long-term opioid use by previously opioid-naive patients.39 There are also growing concerns about serious adverse events, including deaths with the increasing use of prescription opioids by the community.
In recent years, there has been increasing interest in implementing hospital-based opioid stewardship programs to improve safety and monitor opioid prescribing.41 There is currently a lack of consensus on defining “opioid stewardship” to help healthcare institutions successfully design and implement opioid stewardship.20 While implementation strategies of these programs can range from the audit-and-feedback mechanisms to multi-disciplinary consult services. Many programs mainly rely on medication and formulary restrictions.41 The opioid stewardship program inherently aims to restrict the use of opioid analgesics without consulting with healthcare providers skilled in pain management. This approach may disproportionately affect people who use illicit drugs and those with opioid use disorder.41 Therefore, most opioid stewardship programs currently focus on the judicious and appropriate use of opioids, looking primarily at the supply-side, ie, prescription issuance for preventing inappropriate use. Wider and holistic aspects of opioid access, use, safety and effectiveness must be considered.
Currently, most opioid stewardship programs emphasise reducing prescription numbers and doses of opioids. There is a lack of emphasis on patient-centred decision-making regarding tapering decisions. Opioid tapering is a recommended strategy to reduce risks associated with chronic opioid therapy by reducing doses to a lower level.42 In particular, patients with OUD can be disadvantaged, increasing the risk of illicit opioid use and overdose.
A crucial element that the current opioid stewardship guidelines and definition need to incorporate is patient perspectives in shared decision-makings. The blanket approach of curbing down opioids with outcomes solely focused on prescription numbers and doses without considering patient-reported outcomes is less likely to be successful. It is important to involve patients, carers and multi-disciplinary healthcare professionals involved in their care.32,43,44 A previous study demonstrated that patient-reported outcomes were positively linked to the opportunity to interact with healthcare professionals and wider opioid stewardship programs.45
While the current definitions of opioid stewardship mainly focus on “improvement or appropriateness of prescribing and monitoring the use of opioids”, emphasis on two essential themes, ie, “appropriate procurement, inventory management and storage” and “promoting better communications between patients and prescribers”, remain sparse. Also, the concept of perioperative opioid discharge planning is another essential component of stewardship, as all opioid-naive patients are counselled to avoid repeat/refill opioid prescriptions without physicians’ consultation.46 Most opioid stewardship interventions are multi-component, involving clinical interventions, care processes, and implementation strategies. Provisions of education, policies, dashboards, audit and feedback, monitoring and metrics, health information exchange, and electronic health record tools were some implementation strategies identified by the present review.23
When implementing an opioid stewardship programme, it is essential to ensure that access to opioids for patients with genuine needs is not affected.47 Early opioid stewardship programmes need to fine-balance the appropriate use of opioids, considering patient engagement and clinical outcomes.
The findings of this systematic review necessitate the importance of developing a valid and internationally acceptable definition and scope of practice with opioid stewardship programmes. While opioid stewardship is relevant to diverse practices and settings, the common goal should be to optimise treatment and outcomes through rationale and evidence-based prescribing practices. Given the scale of adverse events that have been reported internationally, promoting patient and prescriber education is vital. Evidence suggests that a lack of patient understanding regarding the potential for addiction, broken communications between prescribers and patients and a lack of continuity of care from the same provider are commonly reported barriers to treatment optimization. Therefore, future definitions and scope of practice should incorporate holistic initiatives to promote safe, evidence-based, rational use of prescribed and over-the-counter opioids.
Although the WHO (2020) definition of opioid stewardship seems to be the most comprehensive one offered to date as it encompasses most of the elements of appropriate use and disposal of unused opioids, an improved definition is needed to consider further the views of patients/carers and wider stakeholders. Considering the definitions included in the systematic review, we propose the following definition of opioid stewardship with wider scope, capturing the importance of safety, effectiveness, and patient/carer involvement.
Opioid stewardship programs include evidence-based guidelines, policies, person-centred practices and research to promote rational prescribing, use and deprescribing of opioids for managing pain and specified health conditions. Opioid stewardship programmes should aim to optimise treatment by maximising clinical benefits for the patients and the wider society and minimising adverse consequences, including overuse, misuse, and diversion. Effective patient-provider communications and involving patients and/or their carers in decision-making are key to implementing any opioid stewardship program by considering evidence-based outcomes that matter to patients. Stewardship programmes should also focus on safe procurement, storage, and disposal practices.
A larger consensus exercise involving patients, prescribers, researchers and wider stakeholders is needed further to validate the above definition and scope of practice.
Strengths and Limitations
A comprehensive search strategy of six large and reliable databases (MEDLINE, EMBASE, APA PsycINFO, Scopus and CENTRAL) was used to include all relevant articles within the study scope. Additionally, a grey literature search was also done. However, only publications in the English language and the resources defining the term “opioid stewardship” were considered. When the scope of practice was recommended without an overarching definition, such resources were not considered.
Conclusion
To the best of our knowledge, this is the first attempt to review and propose a comprehensive definition of “opioid stewardship” through the review of clinical practice guidelines and professional society domains. Despite the widespread and growing emphasis on opioid stewardship programmes, there is still a dearth of internationally accepted definition. Current definitions highlight the importance of appropriate opioid prescribing, procurement and inventory control of opioids and emphasize patient and prescriber education and communication. The definition proposed in this study is likely to be internationally acceptable, given the focus on the benefits to patients, healthcare professionals and wider society. The proposed definition highlights the importance of optimal communication between patients and providers, focusing on outcomes that patients value rather than solely on quantitative outcomes relevant to prescription items and dose quantities. All future opioid stewardship programmes involve patients and/or their carers at the heart of prescribing and deprescribing, including tapering decisions. There is a need for a larger consensus exercise involving patients, prescribers, researchers and wider stakeholders to validate the proposed definition of opioid stewardship programs.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There was no funding for this study. The authors acknowledge the support from the University of Birmingham to cover the open access fees for the article.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Cohen B, Ruth LJ, Preuss CV. Opioid analgesics. In: StatPearls. StatPearls Publishing; 2021.
2. Clark DJ, Schumacher MA. America’s opioid epidemic: supply and demand considerations. Anesth Analg. 2017;125:5. doi:10.1213/ANE.0000000000002388
3. Shipton EA, Shipton EE, Shipton AJ. A review of the opioid epidemic: what do we do about it? Pain Ther. 2018;7(1):23–36. doi:10.1007/s40122-018-0096-7
4. Alenezi A, Yahyouche A, Paudyal V. Current status of opioid epidemic in the United Kingdom and strategies for treatment optimisation in chronic pain. Int J Clin Pharm. 2021;43(2):318–322. doi:10.1007/s11096-020-01205-y
5. Australian Institute of Health and Welfare. Opioid Harm in Australia and Comparisons Between Australia and Canada. Australian Institute of Health and Welfare; 2019.
6. Gong J, Merry AF, Beyene KA, et al. Persistent opioid use and opioid-related harm after hospital admissions for surgery and trauma in New Zealand: a population-based cohort study. BMJ Open. 2021;11(1):e044493. doi:10.1136/bmjopen-2020-044493
7. Coffin PO, Rowe C, Oman N, et al. Illicit opioid use following changes in opioids prescribed for chronic non-cancer pain. PLoS One. 2020;15(5):e0232538. doi:10.1371/journal.pone.0232538
8. Hser YI, Mooney LJ, Saxon AJ, et al. High mortality among patients with opioid use disorder in a large healthcare system. J Addict Med. 2017;11(4):315–319. doi:10.1097/adm.0000000000000312
9. Uritsky TJ, Busch ME, Chae SG, Genord C. Opioid Stewardship: Building on Antibiotic Stewardship Principles. Taylor & Francis; 2021:181–183.
10. Phelps P, Achey TS, Mieure KD, et al. A survey of opioid medication stewardship practices at academic medical centers. Hosp Pharm. 2019;54(1):57–62. doi:10.1177/0018578718779005
11. Hall KK, Shoemaker-Hunt S, Hoffman L, et al. Making healthcare safer III: a critical analysis of existing and emerging patient safety practices. 2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK555526/.
12. Mayoral V. An overview of the use and misuse/abuse of opioid analgesics in different world regions and future perspectives. Pain Manag. 2022;12(4):535–555. doi:10.2217/pmt-2021-0094
13. American Hospital Association. Stem the tide: opioid stewardship measurement implementation guide. Chicago, IL; 2022. Available from: www.aha.org/opioids.
14. Degenhardt L, Grebely J, Stone J, et al. Global patterns of opioid use and dependence: harms to populations, interventions, and future action. Lancet. 2019;394(10208):1560–1579. doi:10.1016/s0140-6736(19)32229-9
15. Al-Samawy S, Varughese N, Vaillancourt R, Wang XYW, Penm J, Global A. Survey on opioid stewardship practices in hospitals: a cross-sectional pilot study. Pharmacy. 2021;9:3. doi:10.3390/pharmacy9030122
16. Xu K, Nolan S, Mihic T, Ti L. Improving opioid stewardship programs through shared decision-making. J Am Pharm Assoc. 2022;62(3):697–700. doi:10.1016/j.japh.2022.02.001
17. Higgins JP, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons; 2019.
18. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–269. doi:10.7326/0003-4819-151-4-200908180-00135
19. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005;15(9):1277–1288. doi:10.1177/1049732305276687
20. Ardeljan LD, Waldfogel JM, Bicket MC, et al. Current state of opioid stewardship. Am J Health Syst Pharm. 2020;77(8):636–643. doi:10.1093/ajhp/zxaa027
21. Ghafoor VL, Phelps PK, Pastor J, Meisel S. Transformation of hospital pharmacist opioid stewardship. Hosp Pharm. 2018;54(4):266–273. doi:10.1177/0018578718809267
22. Michalowski A, Boateng S, Fraser MR, Levine RL. 307C24Developing a culture of opioid stewardship: the pennsylvania example. In: Butler JC, Fraser MR, editors. A Public Health Guide to Ending the Opioid Epidemic. Oxford University Press; 2019.
23. Shoemaker-Hunt SJ, Wyant BE. The effect of opioid stewardship interventions on key outcomes: a systematic review. J Patient Saf. 2020;16(3SSuppl 1):S36–s41. doi:10.1097/pts.0000000000000710
24. Tanzi MG. Pharmacists have lead role in hospital-based opioid stewardship programs. Pharm Today. 2019;25(10):6.
25. Sandbrink F, Uppal R. The time for opioid stewardship is now. Jt Comm J Qual Patient Saf. 2019;45(1):1–2. doi:10.1016/j.jcjq.2018.10.004
26. Srivastava D, Wilkinson P. Surgery and opioids: some cracks in an enduring romance. Br J Anaesth. 2021;126(6):1088–1092. doi:10.1016/j.bja.2021.02.003
27. Hyland SJ, Brockhaus KK, Vincent WR, et al. Perioperative pain management and opioid stewardship: a practical guide. Healthcare. 2021;9:3. doi:10.3390/healthcare9030333
28. Advanced Pain Care. What is opioid stewardship?; 2022. Available from: https://austinpaindoctor.com/opioid-stewardship.
29. Society of Hospital Pharmacists of Australia (SHPA). Reducing opioid-related harm: a hospital pharmacy landscape paper for the medicines leadership forum; 2022. Available from: https://shpa.org.au/publicassets/d644d3eb-d783-ec11-80e0-005056be03d0/20-7-18_final_report_-_reducing_opioid-related_harm_-_shpa_landscape_paper.pdf.
30. World Health Organization. Guidelines on the management of chronic pain in children; 2020. Available from: https://www.who.int/publications/i/item/9789240017870
31. Institute for Safe Medication Practices (ISMP) Canada. Opioid Stewardship; 2022. Available from: https://www.ismp-canada.org/opioid_stewardship/.
32. Australian Commission on Safety and Quality in Health Care. 2021 national opioid analgesic stewardship program. Discussion paper for public consultation. 2022. Available from: https://www.safetyandquality.gov.au/sites/default/files/2021-05/opioid_analgesic_stewardship_discussion_paper_for_public_consultation_9-april-2021_acc_2.docx.
33. The State of Queensland (Queensland Health) 1996–2019, Queensland Government. Queensland Opioid Stewardship Program (QOSP); 2022. Available from: https://clinicalexcellence.qld.gov.au/improvement-exchange/queensland-opioid-stewardship-program-qosp.
34. Safe Care Victoria. Analgesic stewardship pilot program; 2022. Available from: https://www.safercare.vic.gov.au/sites/default/files/2021-09/Analgesic%20stewardship%20information%20pack.pdf.
35. ACSQHC. Opioid analgesic stewardship in acute pain clinical care standard. ACSQHC. 2022. Available from: https://www.safetyandquality.gov.au/standards/clinical-care-standards/opioid-analgesic-stewardship-acute-pain-clinical-care-standard.
36. Roughead EE, Lim R, Ramsay E, Moffat AK, Pratt NL. Persistence with opioids post discharge from hospitalisation for surgery in Australian adults: a retrospective cohort study. BMJ Open. 2019;9(4):e023990. doi:10.1136/bmjopen-2018-023990
37. Daoust R, Paquet J, Cournoyer A, et al. Side effects from opioids used for acute pain after emergency department discharge. Am J Emerg Med. 2020;38(4):695–701. doi:10.1016/j.ajem.2019.06.001
38. Baldini A, Von Korff M, Lin EH. A review of potential adverse effects of long-term opioid therapy: a practitioner’s guide. Prim Care Companion CNS Disord. 2012;14:3. doi:10.4088/PCC.11m01326
39. Schug SA, Palmer GM, Scott DA, Halliwell R, Trinca J. Acute pain management: scientific evidence, fourth edition, 2015. Med J Aust. 2016;204(8):315–317. doi:10.5694/mja16.00133
40. Webster LR. Risk factors for opioid-use disorder and overdose. Anesth Analg. 2017;125(5):1741–1748. doi:10.1213/ane.0000000000002496
41. Poteryko S, Nolan S, Mihic T, Ti L. Moving away from a “one size fits all” model: ensuring opioid stewardship includes people who use drugs. J Addict Med. 2021;2021:1. doi:10.1097/adm.0000000000000938
42. Berna C, Kulich RJ, Rathmell JP. Tapering Long-term Opioid Therapy in Chronic Noncancer Pain: evidence and Recommendations for Everyday Practice. Mayo Clin Proc. 2015;90(6):828–842. doi:10.1016/j.mayocp.2015.04.003
43. Palliative Care Australia. Reform in opioid regulation should not be at the expense of palliative care patients; 2021. Available from: https://palliativecare.org.au/mediarelease/reform-in-opioid-regulation-should-not-be-at-The-expense-of-palliative-care-patients/.
44. Australian Commission on Safety and Quality in Health Care. Opioid analgesic stewardship in acute pain clinical care standard – acute care edition; 2022. Available from: https://www.safetyandquality.gov.au/sites/default/files/2022-04/opioid-analgesic-stewardship-in-acute-pain-clinical-care-standard.pdf.
45. So WM. BC centre on substance use. St Paul’s hospital opioid stewardship program patient satisfaction report. Tamara, Nolan, Seonaid; 2021. Available from: http://www.providencehealthcare.org/sites/default/files/OSP_Patient_Satisfaction_Survey_Report_Nov2021.pdf.
46. Levy N, Lobo DN, Fawcett WJ, Ljungqvist O, Scott MJ. Opioid stewardship: a need for opioid discharge guidance. Comment on Br J Anaesth. 2019;122:e198–e208. doi:10.1016/j.bja.2019.01.028
47. Korownyk C, Perry D, Ton J, et al. Managing opioid use disorder in primary care: PEER simplified guideline. Can Fam Physician. 2019;65(5):321–330.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.