")
Back to Journals » Advances in Medical Education and Practice » Volume 14
What are the Attitudes of Medical Students at Jazan University Toward Professionalism?
Authors Mustafa M , Terair S , Al Ageeli E , Gohal G , Salih S
Received 14 January 2023
Accepted for publication 24 March 2023
Published 7 April 2023 Volume 2023:14 Pages 343—354
DOI https://doi.org/10.2147/AMEP.S399888
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Mai Mustafa,1,2 Salaheldin Terair,2 Essam Al Ageeli,3 Gassem Gohal,1 Sarah Salih4
1Pediatric Department, Faculty of Medicine, Jazan University, Jazan, Jazan, Kingdom of Saudi Arabia; 2Medical Education Department, Faculty of Medicine, Jazan University, Jazan, Jazan, Kingdom of Saudi Arabia; 3Cinical Biochemistry Department, Faculty of Medicine, Jazan University, Jazan, Jazan, Kingdom of Saudi Arabia; 4Family and Community Medicine Department, Faculty of Medicine, Jazan University, Jazan, Jazan, Kingdom of Saudi Arabia
Correspondence: Mai Mustafa, Pediatric Department, Faculty of Medicine, Jazan University, Jazan, Jazan, Kingdom of Saudi Arabia, Email [email protected]
Purpose: We assessed the attitudes of Jazan University medical students toward professionalism and evaluated the associations of those attitudes with demographic factors.
Materials and Methods: Seven hundred ninety-seven respondents (88.85% response rate) out of 898 students who were invited to this study (50.7% were men and 49.3% were women) were studied by their response to the Learner’s Attitude of Medical Professionalism Scale (LAMPS) that assess their level of agreement with 28 items, each reflecting a single professionalism competency within the subscales of Altruism, Excellence, Duty/Accountability, Honor/Integrity, and Respect for Others.
Results: Of 797 respondents (88.85% response rate), 50.7% were men and 49.3% were women. Subscales with high agreement scores were Excellence (median, 21.0; range, 6– 30) and Duty/Accountability (median, 21.0; range, 7– 35). Subscales with slightly lower agreement scores were Respect for Others (median, 15.0; range, 5– 25), Altruism (median, 15.0; range, 5– 25), and Honor/Integrity (median, 12.0; range, 5– 25). No sex differences were observed for most subscales; however, men gave higher agreement scores on the Excellence subscale, and compared with year 3 respondents (preclinical phase), year 6 respondents (clinical phase) gave higher agreement scores on the Excellence, Altruism, and Respect for Others subscales.
Conclusion: Overall, medical students at Jazan University indicated high agreement with all attitudes to professionalism subscales on the LAMPS.
Keywords: professionalism, medical students, Jazan University, students’ attitudes, students’ perception
Introduction
Medical professionalism is neither an unexplored concept nor a recent idea; the Hippocratic Oath taken by physicians embodies it.1,2 A doctor’s commitment to optimum clinical care, personal integrity, and maintenance of good relationships with patients and colleagues constitute an acceptable medical approach.3 A patient’s trust in the doctor is well understood to be key to an effective doctor–patient relationship; to successful diagnosis, treatment, and prevention of illnesses,2 to enhancement of healthcare outcomes; and to overall patient satisfaction.4 Clinical excellence cannot be achieved unless physicians master indefectible personal values such as integrity, empathy, altruism, and respect for human life.5 Trust in the doctors and healthcare system is crucial to delivering good healthcare and achieving desirable health outcomes; It is a perspective formed around specific attributes of those who provide care and the dimensions of one’s relationship with them within the healthcare system. It could be in the form of interpersonal trust that is defined by acceptance of one own vulnerable condition with a related belief that one’s interests will be cared for by physicians or could be impersonal, institutional trust reflecting trust in healthcare institutions or the whole system. It has numerous dimensions: fidelity, honesty, confidentiality, and competence.6
The definitions of medical professionalism are many and varied. Some describe it as a combination of adequate clinical care, learning and teaching, communicating with patients, and interacting with colleagues. Others define it as adherence to ethics, committed performance of professional responsibilities, and sensitivity to various patient populations; still others emphasize excellence, integrity, and altruism.7,8 The American Board of Medical Specialties defines professionalism as a system for the reliable transfer of competency standards and ethics. The six domains for physician professionalism as outlined by the Board are:9,10
Excellence in performance, by achieving or exceeding ordinary expectations and the goal of lifelong learning.
Altruism, by prioritizing the wellbeing of patients above self-interest.
Accountability, by taking responsibility for reactions to patients, the community, and the health profession.
Honor and integrity, by being honest, fair, and credible.
Duty of care, by ensuring patient safety and health through high-quality care
Respect for others, by dealing equitably with patients, families, and other healthcare professionals.
Unprofessional conduct could be an underlying causality of medical malpractice and can sometimes contribute to patient mortality and morbidity.5,11
Medical professionalism is a central competency for medical students as trainees and practicing doctors as life-long learners. Despite the increased value of this competence among healthcare stakeholders, there’s still a need to emphasize it in the healthcare environment. 10 Teaching professionalism is not about instructing individuals how to do the right things or do things well, but rather about enhancing the individual’s intellect to shape appropriate future actions.11 Numerous factors affect the perception of what constitutes professional or unprofessional conduct, and in medical education, the design of a professionalism curriculum should reflect the core attributes of a professional doctor in a particular culture.12–14
Geographical background and culture must be considered when describing professionalism, and they should also be considered when designing the curriculum for professionalism.14,15 Examples of inadequate medical professionalism include using social media applications during working hours, smoking cigarettes in the office, absence of collaboration with the other health care professionals within the team, referrals of complex cases to other hospitals, and freeing up beds before holidays.5
Methods of teaching professionalism can include lectures, simulations, group discussions, and role modeling.1,16 Standards for implementing professionalism into undergraduate training remain undetermined but merging professionalism into the curriculum can positively affect the quality of healthcare delivered.11
With an increasing emphasis by universities and national accreditation commissions on professionalism in medical practice, measuring the attitudes of medical students toward professionalism has become essential. However, measures for evaluating whether appropriate attitudes being imparted are challenging to generalize, both because the strategies used to teach professionalism vary widely and because no universally agreed-upon definition of professionalism has been reached.11
Western frameworks of medical professionalism often fail to accommodate the cultural values of non-Western countries. The Arabian context describes the culture, beliefs, traditions, and behaviors practiced by nations of Arabian countries in the Middle East, where Arabic is the official language, and Islam is the religion of most of the population. Those behaviors and habits are some common values that have been accepted as the norm among the people of these countries.12 Literature that addresses the concept of medical professionalism in an Arabian context emphasizes that cultural differences require the addition of domains addressing faith and values to the six domains articulated by the American Board of Internal Medicine.17,18 Arabian educators and students believe that professionalism is a major contributor to the hidden curriculum rather than to formal teaching.19
The 2016 Saudi MED framework, created as a national standard for Saudi medical graduates, was designed to ensure acquisition of the competencies needed to be a successful physician. Its six competencies include a scientific approach, patient care, community-oriented practice, communication and collaboration, professionalism, and research and scholarship.20,21
The National Commission for Academic Accreditation and Assessment of Saudi Arabia mandates that the following domains be integrated into all medical programs of study: knowledge, cognitive skills, communication, interpersonal skills and responsibility, psychomotor skills, collaboration, professionalism, research, and scholarship.19 Program graduates must be able to collaborate with other health professionals to optimize patient care and should be active voices in their communities on global health concerns.20
In Saudi Arabia, studies to assess the attitudes of medical students toward professionalism have been limited. We therefore set out to assess the attitudes of Jazan University medical students toward professionalism and to compare those attitudes by age, sex, and academic year.
Materials and Methods
This descriptive cross-sectional study was conducted at the Faculty of Medicine, Jazan University, Jazan province (southwestern Saudi Arabia), during 2021–2022.
The six academic years of the university’s Medicine program are divided into three phases. During the first phase (year 1), students learn basic concepts in chemistry, physics, biology, and more of the English and Arabic languages. During the second phase (years 2–3), students study organ systems (structure and function). In the third phase (years 4–6), students take up clinical clerkships, where they practice the skills, attitudes, and behaviors specific to each discipline and to the practice of medicine.
During 2021–2022, 898 students (442 men, 459 women) were enrolled in years 2–6 of the program. An electronic self-administered Arabic questionnaire that collected demographic information and responses to the Learner’s Attitude of Medical Professionalism Scale (LAMPS) was offered to those students. Data was collected through an electronic questionnaire called Learners’ Attitudes on Medical Professionalism Scale (LAMPS), an assessment tool developed and validated by Al-Eraky et al to assess professionalism in the Arab context. It was developed and validated with different statements/items; each one is responsible for reflecting single competency professionalism that will be scored and interpreted.13 LAMPS has high internal consistency and is useful both to identify learning gaps in professionalism and to track changes in attitude to professionalism over time or after an intervention.13 The invitation was done by students from different years who sent the electronic survey to their colleagues’ email and followed their responses.
LAMPS covers the six ABIM-described domains of professionalism in five subscales: Altruism, Duty/Accountability (combined), Excellence, Honor/Integrity, and Respect for Others.13 Each individual item in a subscale reflects a single professionalism competency. Respondents rate the items using a five-point Likert scheme (1, strongly disagree; 2, disagree; 3, neutral; 4, agree; 5, strongly agree).
Questionnaire responses were analyzed using the IBM SPSS Statistics software application (version 22: IBM, Armonk, NY, USA). For the analysis, responses 1 and 2 (strongly disagree, disagree) were grouped, and responses 4 and 5 (agree, strongly agree) were also grouped.
Variables are reported as frequencies and percentages. Mann–Whitney U-tests and linear regression analyses were used to compare groups and to identify significant factors. P < 0.05 was considered statistically significant.
The ethics clearance for the study was obtained from the Institutional Review Board of Jazan University (no. REC-43/03/037). Informed consent was obtained from all participants, and data privacy and confidentiality were ensured.
Results
Demographics
Of the 898 medical students enrolled in years 2–6, 797 completed the questionnaire, for a response rate of 89%. Responses by sex were 50.7% men, 49.3% women: (Table 1). Responses by academic year were almost equal, with a slightly greater proportion coming from year 6 students. About 50.3% were 18–20 years of age. Residency was distributed between rural (50.1%) and urban (49.9%). 48.2% of respondents’ mothers had a high school education, and 47.4% had a family member working in the health field. 68.1% of students had a grade point average greater than 3.5.
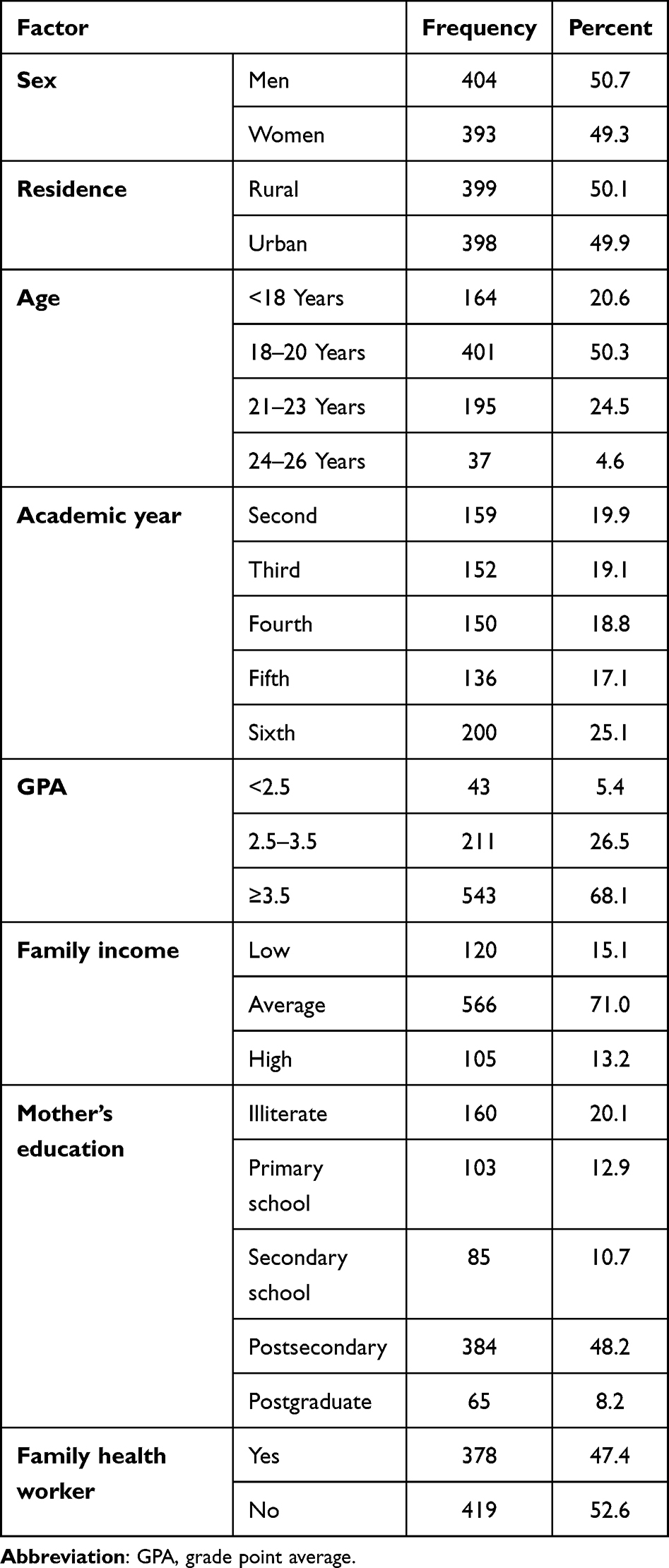 |
Table 1 Demographics of the Respondents |
Professionalism Subscale Scores
Altruism
Overall, questionnaire respondents demonstrated a high attitude of altruism on the Altruism subscale (Table 2).
 |
Table 2 Responses to Items in the Altruism Subscale |
Analysis of individual items in the Altruism subscale revealed that about 65% agreed with the attitudes that doctors stop a sports activity to answer an emergency call or cancel a family appointment for an urgent patient 57.5% of the respondents disagreed with the attitudes that doctors frequently skipping clinical teaching to prepare for conferences 0.50.7% of the respondents disagreed with the attitudes that doctor not witnessing against a hospital in favor of a patient before the court, but notably, 31.2% gave a neutral response to this item. Only 21.4% of respondents agreed with a doctor turning down a home visit to a disabled patient because of a busy clinic; the remaining responses were split between disagree (41.2%) and neutral (37.5%).
Duty/Accountability
Table 3 presents the responses in the Duty/Accountability subscale. For the statement ‘Do you agree when the doctor calls the insurance company to follow up on a valid patient claim, 42.3% were neutral with 39.2% indicating agreement, and 18.2%, disagreement. 45.7% of respondents indicated agreement with the attitudes that doctors decline an invitation to an infection control committee meeting; only 18.2% disagreed. About 72% of respondents agreed with the attitudes that doctors encourage patients to contribute to decision-making and actively participate in orientation for new residents; 8.6% disagreed. 50% agreed with the attitudes that doctors admit the wrong diagnosis before a patient, with 25.5% disagreeing, and 24.8% being neutral. However, 67.7% of respondents agreed with the attitudes that doctors leave before handing over patients to the next colleague, and 68.4% agreed with the attitudes that doctors discuss cases with colleagues in a crowded elevator.
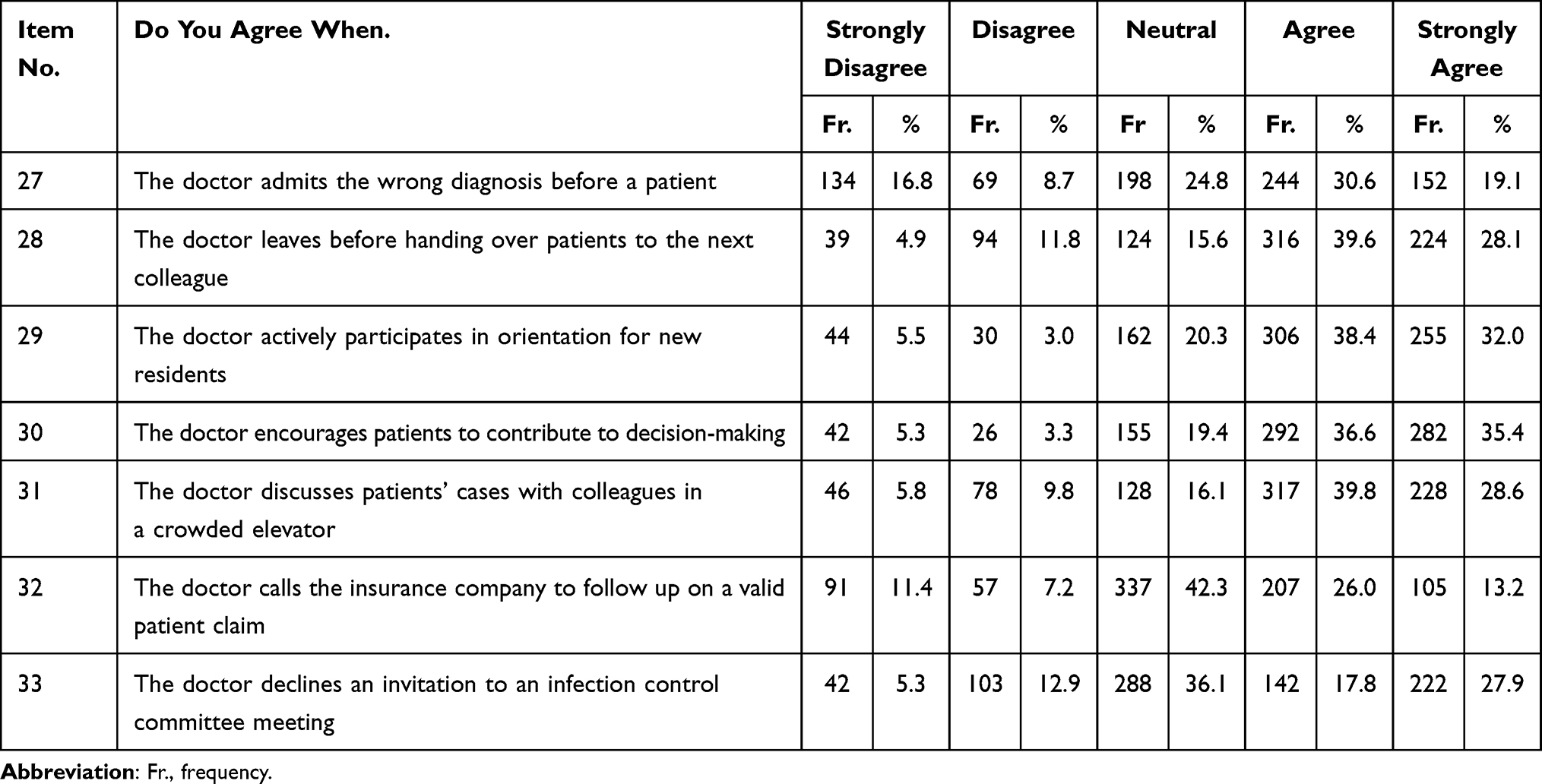 |
Table 3 Responses to Items in the Duty/Accountability Subscale |
The final analysis of this subscale showed a tendency of a positive attitude toward Duty/Accountability by respondents.
Excellence
All results for this subscale indicated that respondents had a highly positive attitude toward Excellence (Table 4), with 60.4% indicating agreement when the doctor reflects on clinical cases to discover unmet learning needs; just 13.3% indicated disagreement.
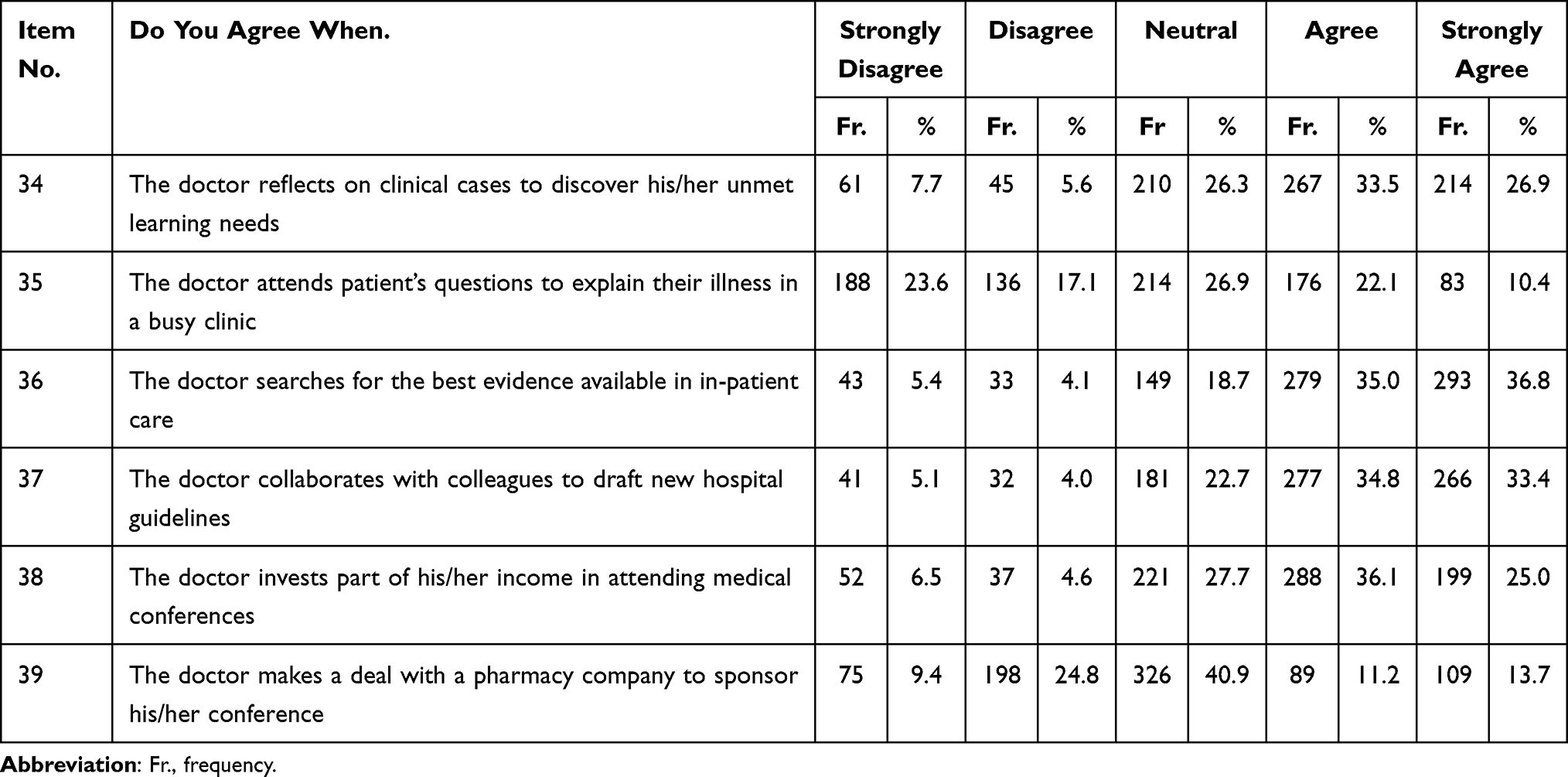 |
Table 4 Responses to Items in the Excellence Subscale |
When respondents were asked “Do you agree when the doctor attends a patient’s questions to explain their illness in a busy clinic”, 40.7% disagreed; 26.9% were neutral; and 32.5% agreed. About 70% of the respondents agreed with the attitudes that doctors search for the best evidence in-patient care and with the attitudes that doctors collaborate with colleagues to draft new hospital guidelines. Also, 61.6% of the respondents agreed with the attitudes that doctors invest part of their income in attending medical conferences. Only 34.2% agreed when the doctor made a deal with a pharmacy company to sponsor their conference; 40.9% were neutral, and 24.9% disagreed.
Honor/Integrity
Analysis of the Honor/Integrity subscale (Table 5) revealed that 66.2% disagreed with the attitude that doctors give wrong information to a patient to protect a colleague; only 16.3% agreed. 57.4% of the respondents disagreed with the statement that a doctor issues false sick leave for a friend’s child to study at home. Neutrality about when the doctor changes actual data in their research based on the supervisor’s advice was indicated by 29.7% of respondents. Only 19.7% disagreed; half the respondents (50.5%) agreed. Most respondents (59.7%) disagreed when the doctor hides information about a fatal diagnosis to avoid patient disturbance; 17.9% disagreed, and 22.9% were neutral. The item “Do you agree when the doctor introduces medical students as doctors to patients” drew 42.8% agreement, 25.6% neutrality, and 31.7% disagreement.
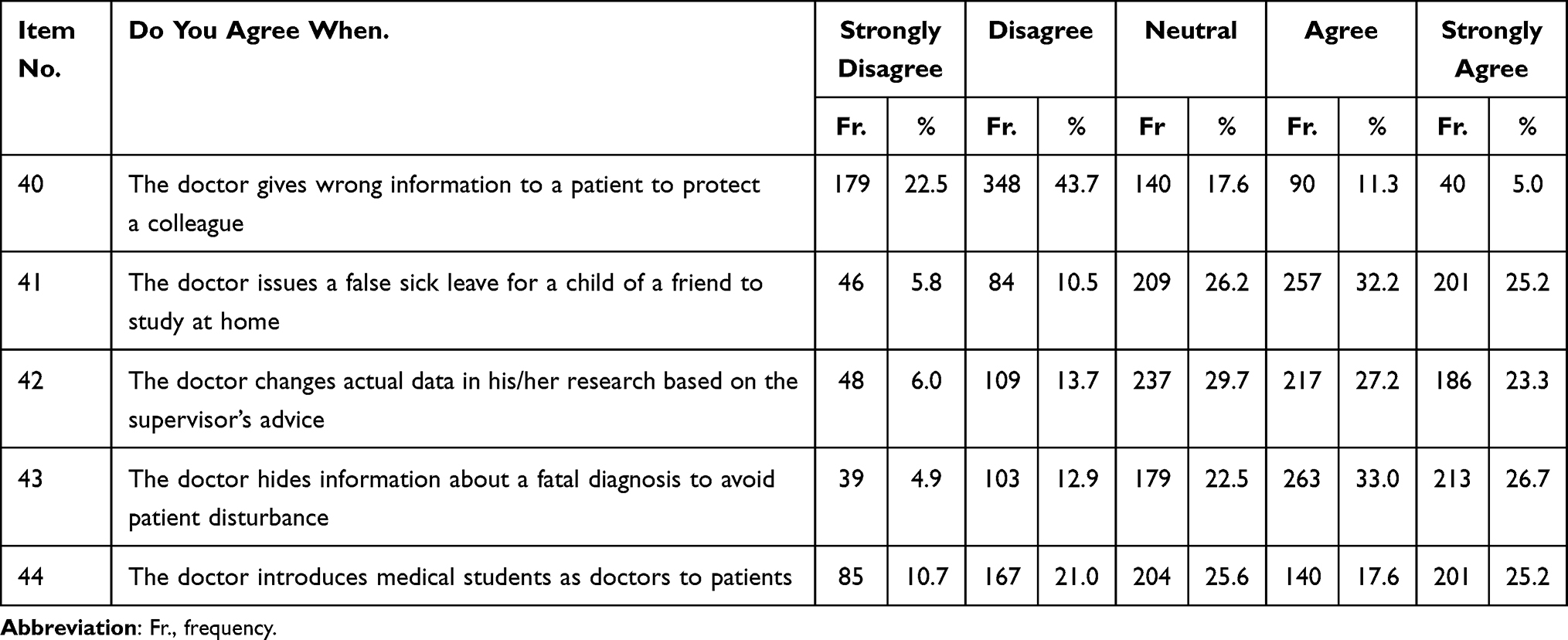 |
Table 5 Responses to Items in the Honor/Integrity Subscale |
Although most items on the Honor/Integrity subscale drew responses revealing positive attitudes toward professionalism, exceptions were the items about changing research data (only half the respondents disagreed) and about introducing medical students as doctors (less than half the respondents disagreed).
Respect for Others
Respect for Others drew highly positive scores from the respondents (Table 6), with 70.8% agreeing when the doctor respects the roles of all members of the healthcare team in the department, and 64.5% agreeing when the doctor considers a patient’s background when explaining their illness. About 70% of the respondents disagreed with the attitude that doctors keep patients waiting in their clinic without apology or gives priority to some patients based on social status or nationality. Similarly, respondents disagreed with the attitude that doctors criticize a prescription written by a colleague in front of patients.
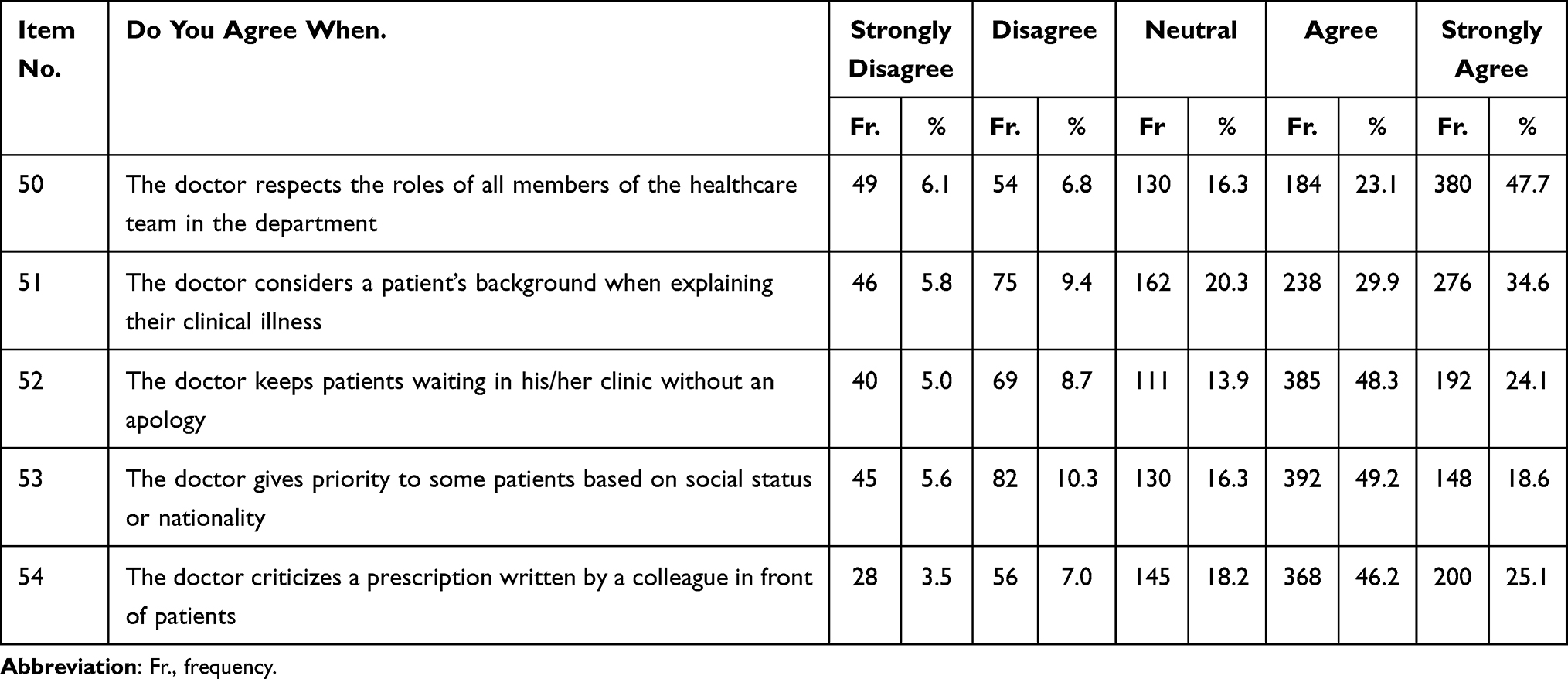 |
Table 6 Responses to Items in the Respect for Others Subscale |
Correlations Between the Subscales and Demographics
In linear regression analysis, associations between the five professionalism subscales and respondent sex, age, and academic year were tested.
● No significant correlations were observed between Altruism and respondent age, sex, or academic year.
● No significant correlations were observed between Duty/Accountability and respondent sex, age, or academic year.
● A significant correlation was observed between Excellence and respondent sex, but not between Excellence and age or academic year (Table 7).
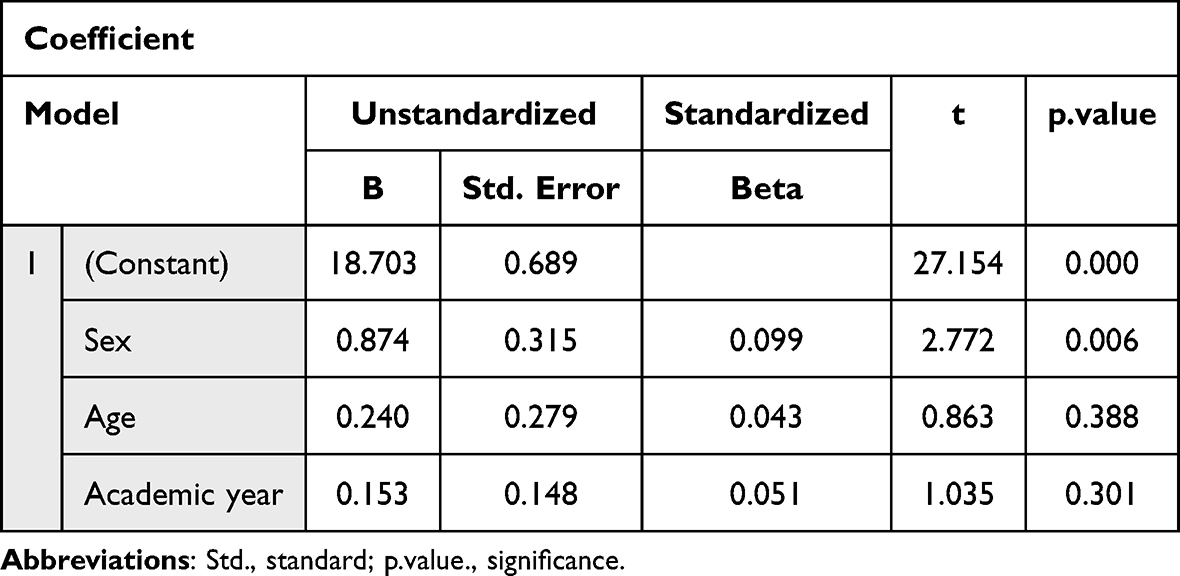 |
Table 7 Association of Excellence (Dependent Variable) with Three Demographic Variables |
● No significant correlations were observed between Honor/Integrity and respondent sex, age, or academic year.
● No significant correlations were observed between Respect for Others and respondent sex, age, or academic year.
The subscales of Excellence (median, 21.0; range, 6–30) and Duty/Accountability (median, 21.0; range, 7–35) drew especially high agreement across all age groups and academic years (Table 8). Agreement was slightly less for the subscales of Respect for Others (median, 15.0; range, 5–25), Altruism (median, 15.0; range, 5–25), and Honor/Integrity (median, 12.0; range, 5–25). No sex differences were observed for most subscales; the exception was Excellence, for which men indicated higher agreement. The Excellence, Altruism, and Respect for Others subscales drew higher agreement from year 6 than from year 3 respondents (Table 9 and Table 10).
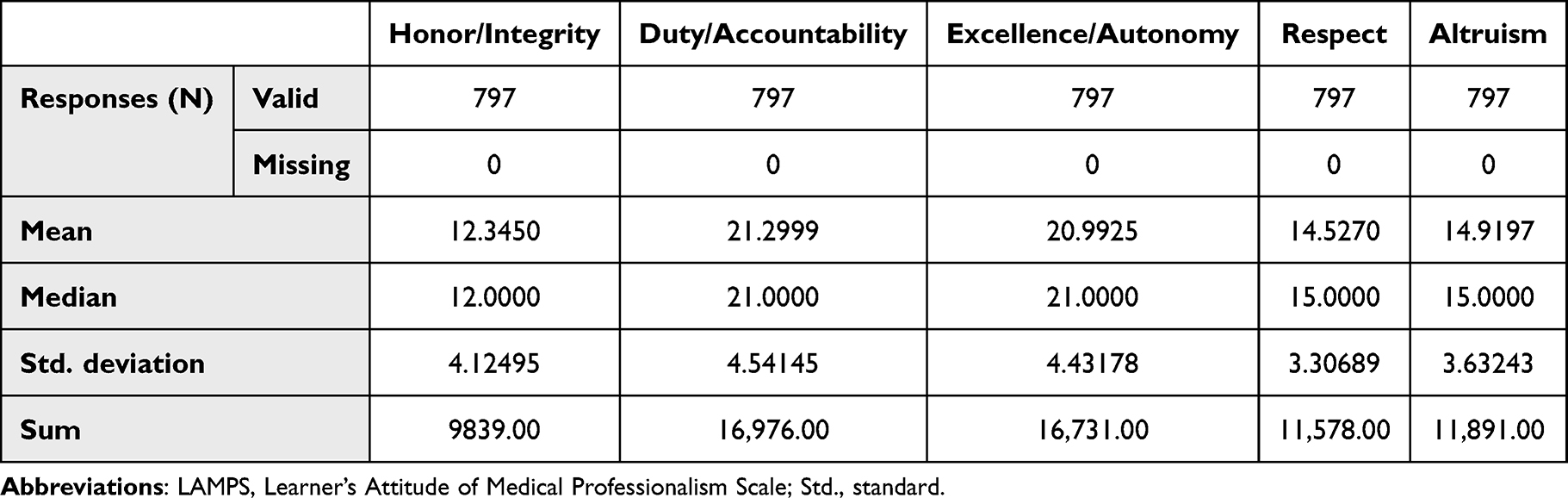 |
Table 8 Agreement Scores by LAMPS Subscale, 797 Respondents |
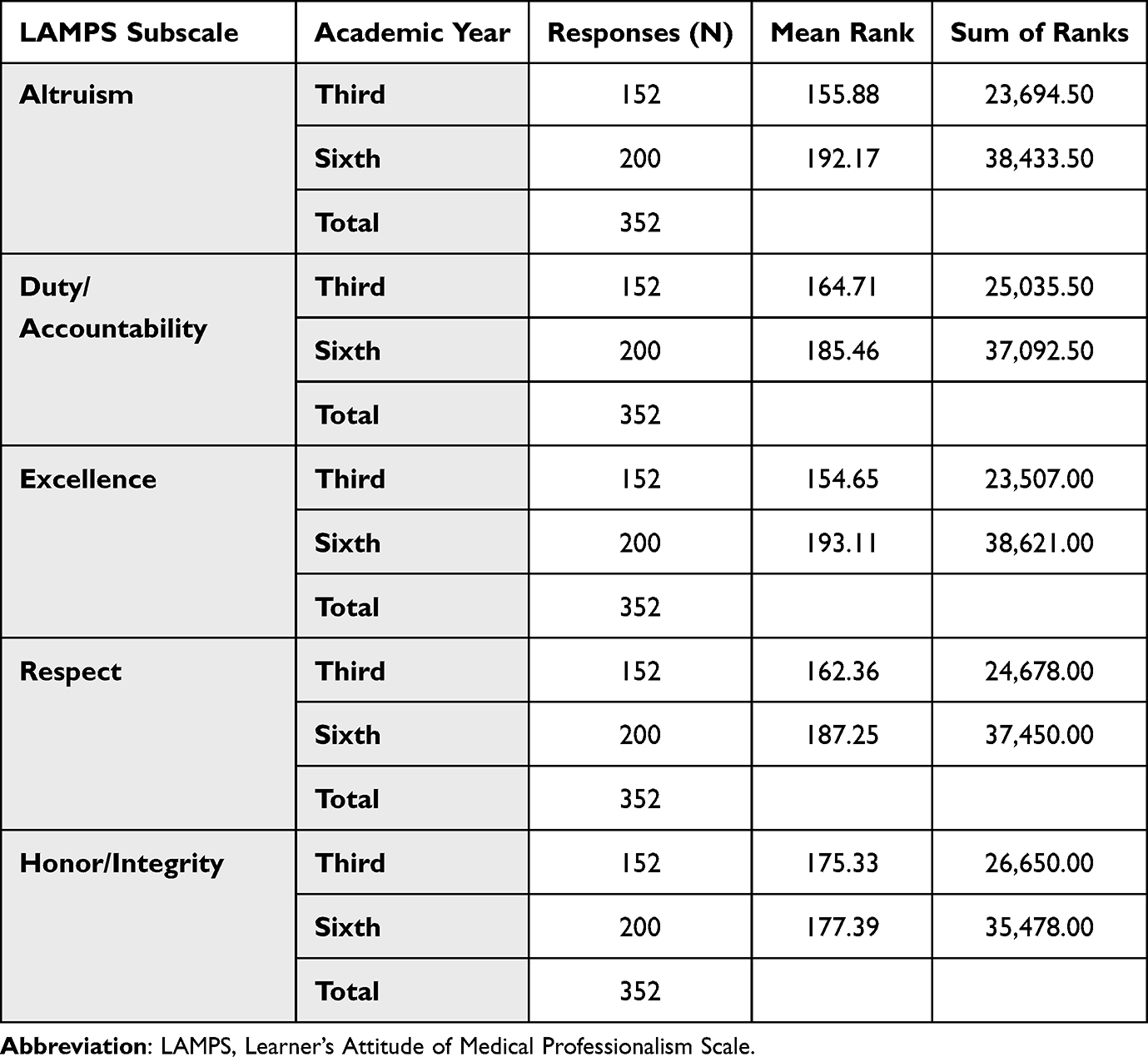 |
Table 9 Ranking of LAMPS Subscales by Respondents’ Academic Year |
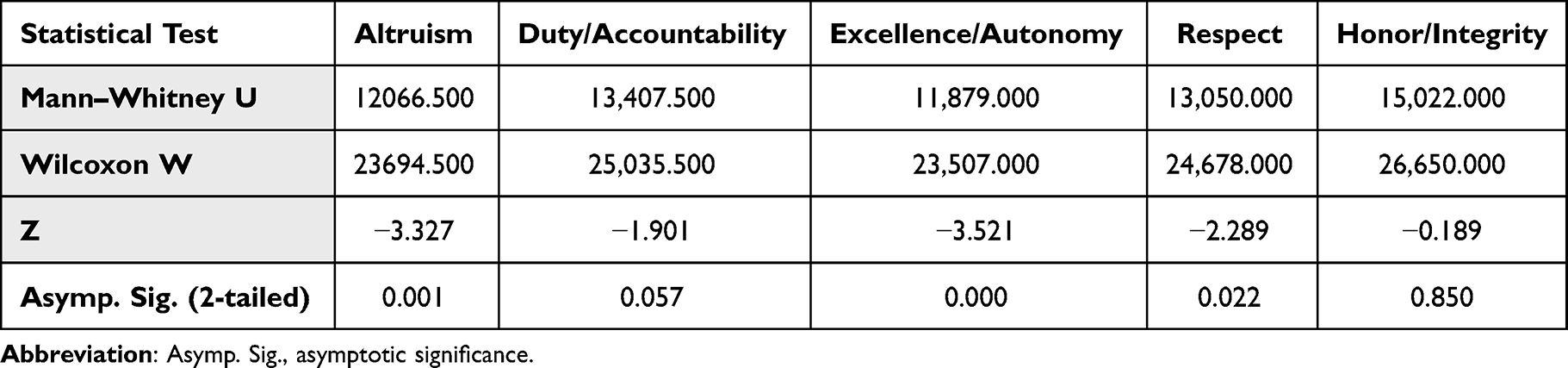 |
Table 10 Statistical Tests of LAMPS Subscales with Academic Level as the Grouping Variable |
Discussion
The development of professionalism in medical students is becoming increasingly crucial; however, debate about how to identify and measure it continues.21,22
This study is one of few research exploring professionalism among medical students in Saudi Arabia using a questionnaire with a high internal consistency that has been validated to be used in the Arabian context.
The present study revealed that students in all academic years had positive attitudes toward most items assessing professionalism (Tables 2–6), a finding compatible with results from many previous studies showing above-average professionalism scores for medical students5,8,23,24 and differing from results of a study concluding that medical students seemed to have a less than adequate understanding of professionalism.23 No differences by academic year or age group were observed, which contrasts with other studies that observed a considerable decline in attitudes toward professionalism as medical education advanced.22,26 Some studies reported that positive attitudes were more often expressed by ethnic minorities, primary care practitioners, and women, especially with respect to doctor–patient communication, persons with disabilities, and communication skills.22,26 Other studies concluded that the professional attitudes of medical students improved most when curriculum and community-based learning were committed to social accountability.22,26 Another study revealed that, in medical residents, a good attitude toward professionalism declined as residency advanced, matching observations made during medical school.27 Another study found that students described their peers and faculty as more professional than the residents.28
A unique and strange finding in this study, only half disagreed with the items about changing research data and about introducing medical students as doctors, although most responses showed positive attitude on the Honor/Integrity subscale. Another study among final year medical students and PhD students has found a significant number reported research misconduct and questionable research practices.29 However, given the nature of this study, there is lack of evidence on the causes of this observation and further studies are needed to better address it.
In the present study, the only professionalism subscale that showed a sex difference was the Excellence subscale, which drew higher scores from men. Other studies have reported that sex and academic year are significant factors affecting scores.22
In the present study, all professionalism subscales drew mostly similar scores from respondents in all academic years. In the one exception, professionalism scores from year 6 respondents were higher than those from their year 3 counterparts (Table 10), thus agreeing with studies that observed higher accountability and excellence scores from final-year students.7,8,30 By contrast, another study found that, compared with year 6 students, year 2 students scored significantly higher on the Excellence subscale. The authors suggested that this finding was explained by the year 2 students making efforts to exceed ordinary expectations, while the year 6 students tended to be overwhelmed with the stress of clinical clerkships.23
Of the five professionalism subscales, Excellence, Altruism, and Respect for Others were scored more highly by year 6 than by year 3 respondents in the present study, which differs from other studies that explained the lack of statistically significant differences between those academic years by the fact that medical professionalism was not being formally taught.25 Declines in a positive professionalism attitude have been suggested to relate to initial positive attitudes that cannot be further elevated, loss of idealism and adoption of a more realistic view of medicine, and the impact of unplanned curriculum and role modeling.22,26
Limitations
Although this study used a validated survey to evaluate attitudes toward professionalism in medical students, some limitations remain. This single assessment of attitudes toward professionalism does not assure that the expressed attitudes will translate into future conduct. The study results cannot be generalized because the study was conducted at a single institution in one region. Some principles of medical professionalism can differ depending on regional customs and culture. Future national and cross-cultural studies should be conducted, as should studies that assess attitudes toward professionalism among graduate Saudi doctors working in Western countries.
Conclusions
Overall, medical students at Jazan University demonstrated good professionalism through high scores on all LAMPS professionalism subscales, particularly Excellence and Duty/Accountability.
The results of this study could be used to emphasize professionalism by bringing clinical modules into the curriculum earlier. Prospective studies are needed to assess how the curriculum influences professionalism over time, with consideration of the effects of sociodemographic and cultural factors. Contextual factors that might influence subscale scores for professionalism by sex and academic year should also be investigated.
Acknowledgments
The research group appreciates everyone who assisted and supported this research study. We thank the students who participated in the study and Dr. Hisham Hanfi for his valuable assistance with the data analysis. The authors would also like to thank Enago (www.enago.com) for the English language review.
Disclosure
The authors report no conflicts of interest in this work. This research was self-funded.
References
1. Seif-Farshad M, Bazmi S, Amiri F, Fattahi F, Kiani M. Knowledge of medical professionalism in medical students and physicians at Shahid Beheshti University of Medical Sciences and affiliated hospitals-Iran. Medicine. 2016;95(45):e5380. doi:10.1097/MD.0000000000005380
2. Lynch DC, Surdyk PM, Eiser AR. Assessing professionalism: a review of the literature. Med Teach. 2004;26(4):366–373. doi:10.1080/01421590410001696434
3. Passi V, Doug M, Peile E, Thistlethwaite J, Johnson N. Developing medical professionalism in future doctors: a systematic review. Int J Med Educ. 2010;1:19–29. doi:10.5116/ijme.4bda.ca2a
4. Tay KT, Ng S, Hee JM, et al. Assessing professionalism in medicine - A scoping review of assessment tools from 1990 to 2018. J Med Educ Curric Dev. 2020;7:2382120520955159. doi:10.1177/2382120520955159
5. Jalil A, Mahmood QK, Fischer F. Young medical doctors’ perspectives on professionalism: a qualitative study conducted in public hospitals in Pakistan. BMC Health Serv Res. 2020;20:847. doi:10.1186/s12913-020-05681-w
6. Nikodem K, Ćurković M, Borovečki A. Trust in the healthcare system and physicians in Croatia: a survey of the general population. Int J Environ Res Public Health. 2022;19(2):993. doi:10.3390/ijerph19020993
7. Sobani ZU, Mohyuddin MM, Farooq F, et al. Professionalism in medical students at a private medical college in Karachi, Pakistan. J Pak Med Assoc. 2013;63(7):935–939.
8. Bhutto SN, Asif M, Jawaid M. Professionalism among medical students at two public sector universities””a comparative study. J Postgrad Med Inst. 2015;29(1):3–8.
9. Blackall GF, Melnick SA, Shoop GH, et al. Professionalism in medical education: the development and validation of a survey instrument to assess attitudes toward professionalism. Med Teach. 2007;29(2–3):e58–e62. doi:10.1080/01421590601044984
10. Sattar K, Akram A, Ahmad T, Bashir U. Professionalism development of undergraduate medical students: effect of time and transition. Medicine. 2021;100(9):e23580. doi:10.1097/MD.0000000000023580
11. Birden H, Glass N, Wilson I, Harrison M, Usherwood T, Nass D. Defining professionalism in medical education: a systematic review. Med Teach. 2014;36(1):47–61. doi:10.3109/0142159X.2014.850154
12. Spiwak R, Mullins M, Isaak C, Barakat S, Chateau D, Sareen J. Assessing perceptions of professionalism in medical learners by the level of training and sex. Educ Health. 2020;33(1):13–19. doi:10.4103/efh.EfH_316_15
13. Al-Eraky MM, Chandratilake M, Wajid G, Donkers J, van Merrienboer J. Medical professionalism: development and validation of the Arabian LAMPS. Med Teach. 2013;35(Suppl 1):S56–S62. doi:10.3109/0142159X.2013.765553
14. Parthiban N, Boland F, Fadil Azim DH, et al. Asian medical students’ attitudes towards professionalism. Med Educ Online. 2021;26(1):1927466. doi:10.1080/10872981.2021.1927466
15. Ćurković M, Farag M. Professionalism and medical practice-cultural perspectives. In: Ćurković M, Borovečki A, editors. The Bridge Between Bioethics and Medical Practice: Medical Professionalism. New York: Springer Cham; 2022:425–450. doi:10.1007/978-3-031-09733-1_18
16. Sethi A, Schofield S, McAleer S, Ajjawi R. The influence of postgraduate qualifications on educational identity formation of healthcare professionals. Adv Health Sci Educ Theory Pract. 2018;23(3):567–585. doi:10.1007/s10459-018-9814-5
17. Al-Eraky MM. Twelve Tips for teaching medical professionalism at all levels of medical education. Med Teach. 2015;37(11):1018–1025. doi:10.3109/0142159X.2015.1020288
18. Abdel-Razig S, Ibrahim H, Alameri H, et al. Creating a framework for medical professionalism: an initial consensus statement from an Arab Nation. J Grad Med Educ. 2016;8(2):165–172. doi:10.4300/JGME-D-15-00310.1
19. Sattar K, Roff S. Comparison of recommended sanctions for lapses in professionalism of undergraduate medical students in a Saudi Arabian and a Scottish medical school. Med Teach. 2016;38(12):1262–1266. doi:10.1080/0142159X.2016.1230190
20. Tekian AS, Al Ahwal MSA. Aligning the SaudiMED framework with the National Commission for Academic Accreditation and Assessment domains. Saudi Med J. 2015;36(12):1496–1497. doi:10.15537/smj.2015.12.12916
21. Shadid AM, Bin Abdulrahman AK, Bin Dahmash A, et al. SaudiMEDs and CanMEDs frameworks: similarities and differences. Adv Med Educ Pract. 2019;10:273–278. doi:10.2147/AMEP.S191705
22. Woloschuk W, Harasym PH, Temple W. Attitude change during medical school: a cohort study. Med Educ. 2004;38(5):522–534. doi:10.1046/j.1365-2929.2004.01820.x
23. AlKhater SA. Perception of Saudi Undergraduate students towards professionalism in medicine. Sultan Qaboos Univ Med J. 2021;21(3):378–385. doi:10.18295/squmj.4.2021.019
24. Tashiya EH, Daniels ER, Karera A. Perceived level of professionalism among radiography students at the University of Namibia. S Afr Radiogr. 2021;59(1):9–15.
25. Aleem S, Raja AK, Iqbal M, Naveed T, Yousaf I, Gul F. Knowledge of medical professionalism among the undergraduate students of army medical college, Rawalpindi. Pak Armed Forces Med J. 2020;70(5):1396–1401.
26. Leaune E, Rey-Cadilhac V, Oufker S, et al. Medical students attitudes toward and intention to work with the underserved: a systematic review and meta-analysis. BMC Med Educ. 2021;21(1):129. doi:10.1186/s12909-021-02517-x
27. García-Estañ J, Cabrera-Maqueda JM, González-Lozano E, Fernández-Pardo J, Atucha NM. Perception of medical professionalism among medical residents in Spain. Healthcare. 2021;9(11):1580. doi:10.3390/healthcare9111580
28. Hoobehfekr S, Asghari F, Sayarifard A, Kadivar M, Kashefinejad S. Medical students’ perception of professionalism climate in clinical settings. J Med Ethics Hist Med. 2021;14:10. doi:10.18502/jmehm.v14i10.7238
29. Ljubenković AM, Borovečki A, Ćurković M, Hofmann B, Holm S. Survey on the research misconduct and questionable research practices of medical students, PhD students, and supervisors at the Zagreb school of medicine in Croatia. J Empir Res Hum Res Ethics. 2021;16(4):435–449. doi:10.1177/15562646211033727
30. Wagner P, Hendrich J, Moseley G, Hudson V. Defining medical professionalism: a qualitative study. Med Educ. 2007;41(3):288–294. doi:10.1111/j.1365-2929.2006.02695.x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.