")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
“We are Tired but Do Not Give Up” the Dilemma and Challenges of Primary Nurses Facing the Omicron Variant: Qualitative Research
Authors Aditya RS , Yusuf A , Alrazeeni DM , Almutairi RL, Solikhah FK , Rahmatika QT, Kotijah S
Received 26 January 2023
Accepted for publication 8 March 2023
Published 27 March 2023 Volume 2023:16 Pages 797—809
DOI https://doi.org/10.2147/JMDH.S404177
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ronal Surya Aditya,1 Ah Yusuf,2 Daifallah M Alrazeeni,3 Reem Lafi Almutairi,4 Fitriana Kurniasari Solikhah,5 Qory Tifani Rahmatika,1 Siti Kotijah6
1Department of Public Health, State University of Malang, Malang, Indonesia; 2Faculty of Nursing, Universitas Airlangga, Surabaya, Indonesia; 3Department of EMS, PSCEMS, King Saud University (KSU), Riyadh, Saudi Arabia; 4Department of Public Health, School of Public Health and Health Informatics, Hail University, Hail, Saudi Arabia; 5Department of Nursing, Poltekkes Kemenkes Malang, Malang, Indonesia; 6Department of Nursing, Universitas Bina Sehat PPNI, Mojokerto, Indonesia
Correspondence: Ah Yusuf, Email [email protected]
Background: Everyone becomes aware due to the epidemic, especially primary department nurses. The significance of their experiences teaches nurses how to take care of themselves and be successful in their caregiving.
Objective: The purpose of this study was to investigate the perceptions of nurses working in primary care settings in rural regions during the omicron variant pandemic.
Methods: On the basis of the Nvivo 12 analytic approach, extensive semi-structured interviews were used to perform this qualitative study. 20 interviews later, data saturation had been reached. Data collecting was place from February to March 2022 for a month. The following participant characteristics were discovered through semi-structured interviews with 20 nurse participants. Ages of the participants, who were split between eight men and twelve women, varied from 28 to 43 years (average age 36.4 years). The majority (75% of them) had a vocational education, and their years of experience ranged from five to fifteen (average 11 years).
Results: 4 topics and 7 sub-themes’ results. The results’ fundamental message is: The Nursing Clinical Practice Dilemma, school district, virus type uncertainty Indigenous peoples do not adhere to the concept of the afterlife. Must Be Excited and Alert; School Cluster; Virus Type Confusion; Non-Belief in Covid; and the Dilemma of Nursing in Clinical Practice are the Overarching Themes of This Study.
Conclusion: Making innovations to increase motivation thereby reducing mental and physical fatigue are the implications of the results of this study. Further exploration of the readiness of nurses to treat patients in the main department is believed to be beneficial for the results of this study.
Keywords: Indigenous peoples, pandemics, child, preschool, COVID-19
Introduction
There is an immediate threat to public health around the world due to the emergence of the Omicron version of the acute respiratory syndrome coronavirus 2 (SARS-CoV-2).1,2 In February of 2022, it was identified as the most recent VOC. Since December 2021, the Delta variety has been the most prevalent strain circulating globally, while Omicron is spreading faster. On January 7, 2020, in Wuhan City, Hubei Province, Chinese officials successfully isolated and identified COVID-19 virus. Both respiratory droplets and direct touch can spread the COVID-19 virus.3,4 Direct contact with an infected individual is the most reliable means of transmission, but indirect contact with infected surfaces or objects (like a thermometer or stethoscope) can also be a factor in the spread of infection.5,6 As of October 6, 2021, 4,223,095 people in Indonesia have positive test results for Covid-19. Four million, five hundred and two people have recovered completely from Covid-19, another 28,381 are undergoing medical care in hospitals or in isolation, and 142,413 have died from the virus. As of the 6th of October in 2021, the number of confirmed cases of Covid-19 in Indonesia was 4,223,092. 1 Out of the total number of people infected with Covid-19, 4,052,300 have recovered completely, 28,381 are still receiving medical care in hospitals or in isolation, and 142,413 have died. An isolation facility in a rural area will assist manage the anticipated influx of COVID-19 cases and keep hospitals from nearing capacity. This is supported by a number of studies.7
A Transmission of COVID-19 is more likely to occur at the primary departments in the healthcare sector. The primary care clinic is the initial point of contact between a patient and a healthcare provider, therefore the risk of infection for both the patients and the staff is significant.8 Nurses are particularly at risk for contracting COVID-19 because they deal directly with patients in the primary care setting.9,10 In the emergency room, nurses have a significant risk of contracting the COVID-19 virus.11
Inadequate protection, prolonged exposure to directly infected patients, job pressure, and the lack of personal protective equipment (PPE) are some of the variables previously found to contribute to the spread of COVID-19 among healthcare personnel.12–15 In spite of the widespread use of PPE, many healthcare workers remain at risk of getting COVID-19. In addition to the virus’s inherent ease of spread, the primary management structure put in place during the pandemic is largely to blame for the spread of COVID-19 among healthcare professionals. During the present pandemic, the health care system requires a suitable main management system.10,15–17
Primary care delivery in Indonesia is complicated by the country’s size and the widespread nature of its rural and remote regions. Behaviors linked to worse health outcomes18 are more common among those living in rural and remote areas of Indonesia. When patients are admitted to or while going to one of the numerous smaller hospitals in rural and non-existent distant locations, they are sometimes moved to larger hospitals because of a lack of medical staff. In both circumstances, patients in serious condition typically have to wait for medical help to arrive at the hospital.19 Nurses often make up the bulk of hospital staff at smaller facilities located in more distant areas. Often times, when doctors are not available, it’s up to registered nurses to provide primary care management on the front lines.20
The approach of health workers to the community to carry out tests and close contact tracing is often hampered by strong resistance from the community. There are also many people who are dishonest when they come to primary health care, so the risks we face are quite high.21 By exploring the perspectives of rural primary care nurses in Indonesia during the omicron variant pandemic, this study aims to fill in the gaps in the literature that does not specifically address this issue. This study specifically targets RNs working in a primary care setting because they will get the most out of it.
Methods
Study Design
Semi-structured interviews with primary nurses were conducted as part of the study’s qualitative explorative descriptive design. For investigating and comprehending the experiences of nurses working in primary care clinics in rural regions during the omicron variant pandemic, the qualitative technique is appropriate. In a way that the quantitative approach cannot do, the qualitative approach offers the most explanation possible.22 The completeness and validity of the analysis were assessed using the Consolidated Criteria for Qualitative Research Reporting (COREQ).23
Setting, Sampling, and Participant
To conduct this research, a purposive sample strategy was used. Unique instances are picked based on judgment for the special traits that these cases offer in solving a research topic, and purposeful sampling is most commonly utilized in exploratory research or field research.24 The nurses were gathered using a purposeful sample strategy from several public health institutions in the Malang area of East Java, Indonesia. Only nurses with extensive expertise in the field (ie, more than a year’s worth), who are actively receiving patients and caring for patients in main departments during the COVID-19 epidemic, and who are also willing to engage in this study, were considered for inclusion.
Data Collection
The researchers that performed the online interviews (using Zoom) were all equally skilled in carrying out qualitative research. master’s degrees, doctorates, and professorial credentials. includes one lady and four guys, As lecturers, they undertake research, Participants are aware of the study’s goal, and researchers and participants do not have any familial or other connections. This study does not interest the researcher in any way. The specifics of the interview procedure were provided to the participants after making contact with them and presenting the researcher to them. Participants were guaranteed that their identities would remain anonymous and that all personal information and interviews would be kept private. Data was gathered from February to March 2022 for a single month. Due of the tight constraints, the semi-structured interviews were conducted via Zoom on an individual basis. Digital voice recorders were used to capture every interview. Open-ended questions that let participant and interviewer to follow any fascinating or pertinent experience of inquiry directed the semi-structured interview. One broad inquiry regarding their experiences in the main department during the omicron variant pandemic was the first thing the researcher asked the interviewees. The probing questions for the co-construction of the following interview were amended in light of the findings of the interview data. To preserve data integrity and lessen researcher bias, the interview audio recordings were verbatim transcribed as soon as possible following each interview. Depending on the circumstances and the participants’ interests, experiences, and perspectives, the interview lasts anywhere between 30 and 65 minutes (on average 47 minutes). 20 interviews later, data saturation had been reached. No subjects withdraw from the study before the investigation is finished.
Interview Questions
Using guidelines, semi-structured interviews were done to promote conversation about the problems and emotions faced by nurses in rural areas during the delivery of care during a pandemic. Based on the Theory Base Rural Nursing, which consists of job beliefs and health beliefs; isolation and distance; independence; lack of anonymity; outsiders/insiders; and elderly people/newcomers, the question guideline was produced.
The primary concerns are as follows:
- How was your experience as a nurse at the village’s primary care facility?
- How do you feel about caring for this individual?
- What lessons can you learn from this experience?
- Which circumstances cannot be predicted?
- During the omicron variant epidemic, what challenges have you encountered in treating for rural patients?
Data Analysis
After verbatim transcription, the interview data were examined with a typical method to content analysis. Accordingly, data analysis begins with frequent reading of all transcripts in order to comprehend the entire and accomplish dyeing. Following this, the data were reviewed in their entirety, and a text expressing the nurse’s experience was gathered and included into the text, which served as the unit of analysis. Later on, condensed “meaning units” were developed. The writers summarized the “units of meaning” and took notes on initial thoughts, feelings, and early analyses (open coding). Then, using axial coding, the various codes are classified into subcategories based on their interconnections and relationships. To reach consensus across writers on how to divide code into subcategories, a procedure including debate and introspection was devised. Depending on the relationship between the subcategories that emerge, fewer categories are formed to arrange and organize the subcategories into meaningful categories in order to provide actual content. The category’s hidden meaning or latent content is defined as a single theme. Themes and categories of unprocessed data were thoroughly analyzed and amended using methods of continual comparison. For the purpose of reporting findings, examples for each category are extracted from the data. The author includes the following elements to enhance believability. The interview data were examined by the study team following transcription and codification. In addition, the whole text of the transcribed interview together with the Nvivo 12 code (words used by the patient in the interview) was made available to two participants so that they could assess the compatibility of the conversation transcript with their own experiences. Then, three specialists in qualitative research were requested to review the interviews, the codes, subcategories, categories, and themes were extracted, and if required, revisions were made to the synthesis and interpretation of the data based on their ideas.
Result
We conducted 20 semi-structured interviews with primary care nurses. Persons gave their written informed consent and participated in present study. The participants informed consent included publication of anonymized responses. As can be seen in Table 1, the participants’ ages ranged from 28 to 43 years old, with 8 (40%) being male and 12 (60%) being female (average age 36.4 years). The bulk (75%) had some sort of technical training, and they all had years of experience (5–15). (average 11 years).
 |
Table 1 Interviewees’ Socio-Demographic and Professional Characteristics |
Participants were asked to explain or describe their experiences working as a primary care nurse in a public health facility during the omicron variant pandemic in this semi-structured interview. Table 2 describes the findings of five themes and nineteen sub-themes. The five themes are: The Dilemma of Nursing Clinical Practice, School cluster, Virus Type Confusion, Indigenous peoples do not believe in covid, Must be Excited and Alert.
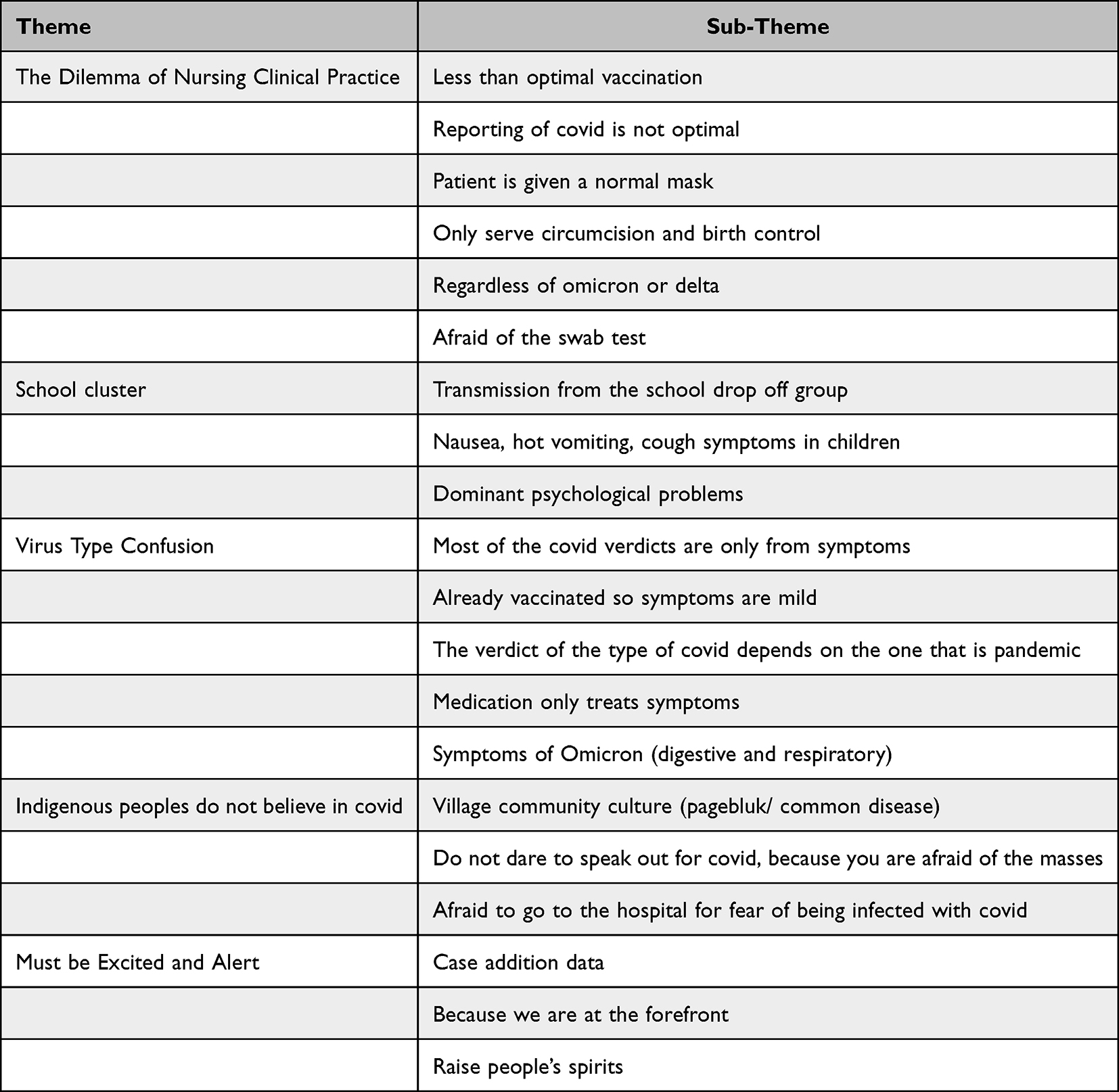 |
Table 2 Themes and Sub-Themes Derived from Analysis of Interviews |
Theme 1: The Dilemma of Nursing Clinical Practice
Nurses who care in the era of a pandemic have a big problem. One of them is the dilemma of how nurses deal with internal and external problems. Many things make them confused what they will do. Dilemma is always a problem in the field for many reasons.
Sub Theme: Less Than Optimal Vaccination
Primary care faced by Vaccination that is less than optimal due to the lack of operators, vaccinators and so on compared to the number of patients who are vaccinated. However, some people in rural area have bad mind about vaccinated. Optimally vaccination is the front line against covid, if this has problems then control will be hampered.
Vaccinator can’t handle people who have different mind about vaccinated (P4, P8)
Patients who are vaccinated more high than volunteer in primary care (P10, P12)
Sub Theme: Reporting of Covid is Not Optimal
Less than optimal was reporting vaccinated in primary health care how are problem in private data. However, other problem about technician in primary health care are bad signal, broken device, miscommunication with volunteer.
….we were working on network eror suddenly…(P2, P5, P6)
….The computer being used has an eror and lights are off so that administrators are hampered from collecting data(P8, P11, P12)
Sub Theme: Patient is Given a Normal Mask
Masks are very important, so all are required to wear masks, because the local government rules are very strict. But this is loose when in the country side, Because they are not usually used to wearing masks. Covid case reporting is the basis for determining policy.
…….We are actually afraid of the rules, but most people don’t wear masks….(P2, P5)
……we didn’t usually used to masks, so that important is we aren’t punished for not wearing masks….(P8, P11, P12)
Sub Theme: Only Serve Circumcision and Birth Control
Everyone is afraid to go to hospital, so that health worker who practice independently only serve circumcision, control pregnant women, prepare pregnant women for healthy and normal births. Only basic services are carried out, if the services are advanced, the nurses do not want to accept them because they are at risk.
….We have not been serve more patients because it is still a risk for to family and neighbor’s, especially the issue of stigma…(P1, P3, P12)
……We only serve circumcision and controlled pregnant women for their birth………(P13, P18, P19)
Sub Theme: Regardless of Omicron or Delta
Confusion between omicron or delta type is common in the countryside, due to we lack of equipment. We only rely on government regulation and patient symptoms. Whatever the type of covid, we still serve patients with wholeheartedly.
….When we were asked by our patient, we were confused, what the type of covid they had. So we advised them to refer for hospital in the city…(P3, P5)
….We recommend drugs that suit the symptoms, without knowing whether it is omicron type or delta type covid, we still serve them…(P9, P13, P17)
Sub Theme: Afraid of the Swab Test
Health workers are traumatized because they often do swab tests, sometimes they are also afraid when a swab test is done, not only because of pain when taking specimens, but afraid because they are afraid that the results will be positive and have an impact on their families.
I’m afraid to take a specimen in my nose, even though I’ve done swab tests many times (P5, P8)
We are afraid of the impact on the family, our swab test results (P9, P16, P20)
Theme 2: School Cluster
Schools are the initial place for the spread, because in shopping centers and government institutions there are already rules for restrictions on gathering, but in schools where the majority of children are less obedient to the rules, making it difficult to regulate in schools, besides traders, parents who take students increasingly creating clusters of covid 19 transmission.
Sub Theme: Transmission from the School Drop off Group
The transmission of covid from schools became dominant because students who were not controlled and introductory students crowded together waiting for students and snack vendors who were selling there.
…we can’t control the school cluster because most of the children and delivery students…(P6, P9)
the school’s dilemma is that they are allowed to teach offline, because they don’t fully control the spread of covid. (P10, P11, P12)
Sub Theme: Nausea, Hot Vomiting, Cough Symptoms in Children
Children have symptoms of vomiting, fever, and cough when they come to health services, so we immediately recommend symptomatic treatment. We do not dare to make a decision that their child has Covid, we only suggest increasing their immunity.
….We receive a lot of children with symptoms of vomiting, fever, accompanied by cough….(P1, P3, P15)
….Don’t dare if we make a decision that their child has covid….(P18)
….Good immunity is important for children….(P19, P20)
Sub Theme: Dominant Psychological Problems
Children have symptoms of vomiting, fever, and cough when they come to health services, so we immediately recommend symptomatic treatment. We do not dare to make a decision that their child has Covid, we only suggest increasing their immunity.
….We receive a lot of children with symptoms of vomiting, fever, accompanied by cough…(P3, P4, P7)
….Don’t dare if we make a decision that their child has covid…(P8, P11, P12)
….Good immunity is important for children.(P10, P14, P17)
Theme 3: Virus Type Confusion
Covid have some problem about type in Indonesia, because they are can not detection that minimal technology. So that health worker in rural area have problem about people who denial to covid spread.
Sub Theme: Most of the Covid Verdicts are Only from Symptoms
The different symptoms of each virus are the basis for health workers to conclude the type of virus. Because in rural areas there is a lack of tools to distinguish the types of viruses based on RNA.
We were confused when asked about the type of covid that attacked them (P5, P7)
inadequate tools so we differentiate by symptoms alone (P8, P16, P17)
Sub Theme: Have Been Vaccinated so Symptoms are Mild
People who have been vaccinated show a milder condition than those who have not been vaccinated. So, vaccines are the government’s way to fight the pandemic.
Incessantly carrying out vaccines because government programs must be carried out (P7, P10)
People often complain because it is mandatory to have vaccines (P11, P12)
Sub Theme: The Verdict of the Type of Covid Depends on the One That is Pandemic
The decision on the type of covid, when the patient’s symptoms are not clear, but the government has informed that the wave experienced by the country is omicron, then most types of covid virus are omicron. Sometimes there are also previous types of viruses.
When the patient has a cough and cold, but there is no typical sign of omicron, then we tend to suspect that the type of covid is omicron (P9, P14)
When we were asked by the patient, we only talked about being suspected of having the omicron virus type (P18)
Sub Theme: Medication Only Treats Symptoms
The focus of care in rural areas when there are people affected by Covid is to focus on treating and reducing symptoms. Most of them are only outpatient, and rarely hospitalized, because of many considerations.
Many people come to us asking for covid medicine, but we can only provide snacks to reduce it (P4, P7)
We already have a protocol for handling covid from the government that focuses on reducing patient symptoms (P8, P11, P12)
Sub Theme: Symptoms of Omicron (Digestive and Respiratory)
The symptom that distinguishes between the delta and omicron types of covid virus is that omicron has additional digestive symptoms in the form of diarrhea, cough, runny nose and shortness of breath. So that we can decide that the patient is suspected of being infected with the omicron type of covid.
dominant community with complaints of cough, cold and diarrhea (P1, P5)
What is typical is the presence of diarrhea (P12)
Theme 4: Indigenous Peoples Do Not Believe in Covid
The culture in the countryside is that the symptoms of COVID-19 are similar to previous outbreaks, so they do not think it’s a dangerous thing. So, they do not believe it and think it’s just an issue.
Sub Theme: Village Community Culture (Pagebluk/ Common Disease)
The countryside has a culture that is still strong, the signs and symptoms of covid have been there based on historical stories. So they consider it normal and do not obey the rules of the command. A culture that is still followed today.
they believe that this is a common thing that happened in the past (P11, P12)
We are having problems with public trust (P8, P11)
Sub Theme: Do Not Dare to Speak Out for Covid, Because You are Afraid of the Masses
People are already fed up with the Covid condition, because of restrictions on gathering so they cannot make a living, so if someone is exposed to Covid, they automatically cannot make a living and their needs. Misrepresentation about covid so that people are afraid and stigmatized. Because of this impact, people will be angry if one of their families is sentenced to covid and feels slandered.
They can’t believe their family has Covid (P12)
In fact we are a bit risky if we convict someone of covid, so we don’t say but still we recommend treatment (P8, P11, P12)
Sub Theme: Afraid to Go to the Hospital for Fear of Being Infected with Covid
The hospital is a place that villagers will never approach, because there is an issue that if you go to the hospital, even if you have a cold, you will be infected, so that when you are sick, people never go to the hospital.
They choose to be treated at home instead of having to go to the hospital (P3, P4)
They chose to call us home instead of taking the family to the hospital (P17, P19)
Theme 5: Must Be Excited and Alert
It’s been almost a year since this pandemic has haunted me, the fear has not gone away. As the front line fighters against Covid-19, these health workers are the most vulnerable group to get infected. It’s very hard to avoid. They can only take care and not infect other people or families. Nurses really have to be in good shape. They cannot be in a state of drop. If there are complaints of pain even though it is mild, it must be reported immediately.
Sub Theme: Case Addition Data
Since Covid-19 hit, every day there are always increasing positive cases. From dozens of cases, to a million cases. Some of the Covid-19 patients are in severe and critical condition. Nurses must be strong, and are required to reduce that number.
…we must fight with increasing positive case….(P9, P19, P20)
…people who have positive covid always increasing every day….(P8, P11, P12)
Sub Theme: Because We are at the Forefront
Community nurses are the first door in preventing covid 19. The failure of community nurses will have an impact on the number of patients in hospitals increasing and the government budget will also increase. Even though we work focused on prevention, we are very important in handling omicron cases.
Everything we have to face, because we are at the forefront (P1, P4, P7)
It has become our risk if we face more complex cases because we are at the forefront (P11, P12)
The government and hospitals really depend on us (P18, P19, P20)
Sub Theme: Raise People’s Spirits
Health workers, especially nurses, have to show and give their best, if they see us tired or giving up, they will become even more hopeless. No matter how tired the nursing staff are, they must always appear happy and enthusiastic in order to awaken the community.
We don’t want to look tired or tired in front of the community, so they can keep their spirits up (P8, P13, P15)
We humans feel tired and tired, but seeing people who are in a slumped condition doesn’t seem able to complain about it (P18, P20)
Discussion
The impact of the Covid-19 pandemic is felt in various aspects of human life, including for nurses who are the largest health profession in the world. The description of nurses’ experiences during the Covid-19 pandemic, especially for nurses who work in primary department in rural areas of Indonesia, is illustrated by 4 (four) themes which have answered the objectives of this study. The themes that emerged included the dilemma of nursing clinical practice, school clusters, confusion about the type of virus, and community leaders who do not believe in the Covid-19 virus.25
Nurses as the front line in handling patients in the midst of the Covid-19 pandemic are a vulnerable population to exposure to Covid-19, causing feelings of fear, stress, uncertainty, confusion, and difficulty.26 This finding is also reflected in the first theme in this study which describes the feelings of nurses’ dilemmas in conducting nursing clinical practice. This can be caused by heavy workloads, risk of infection, lack of Personal Protective Equipment (PPE), fears of transmitting the virus to family members, and long working hours.27 Nurses’ concerns in carrying out clinical practice described in this theme are also caused by low vaccination coverage and incomplete reporting of Covid-19 cases.28 stated that distrust of vaccine effectiveness and low perception of seriousness of Covid-19 infection were the main determinants of individuals reluctant to get vaccines. This situation triggers the emotional state of nurses who have close contact with Covid-19 patients prone to experiencing feelings of fear of being infected, falling sick, to fear of death.29,30 Encouragement and education from various elements including government, health professionals, and community leaders is needed to reduce public concerns and increase vaccine acceptance.
Another dilemma felt by nurses in conducting clinical practice is that the patient’s willingness to perform swab diagnostic tests is still low. Analyzed several obstacles why patients with symptoms that lead to COVID-19 were afraid to take a swab test, including the threat of stigma from the community, misinformation, to economic factors that required patients diagnosed with Covid-19 to be isolated so that they could be isolated. unable to work. Another concern that arises is related to the emergence of a new sub-variant of SARS-Cov-2, namely the Omicron variant which has different clinical features from the previous variant, namely the Delta variant. Although the delta variant has more severe clinical symptoms, longer disease duration, and higher hospitalization rates, the omicron variant is faster in terms of transmission. Some nurses in considering some of the things above decided not to do clinical practice and chose to provide limited services such as providing family planning and circumcision only. For this reason, it is important for nurses to have good knowledge and understanding of the clinical symptoms that arise so that they are able to treat patients with proper management.31
Another theme in this study reports about the majority of cases of Covid-19 transmission that occurred in school clusters. Although some research evidence suggests that school-age children are less likely to be infected with Covid-19,32,33 and a case study by34 also reports that no there is transmission from a child infected with Covid-19 despite contact with more than a hundred children at school, but the prognosis is different for children who are infected with Covid-19 and have a history of comorbid diseases. Children with comorbid diseases have an increased risk of admission to the PICU, increased mortality, and have more serious disease manifestations.35 This study also reported that nurses during the assessment found symptoms that they often complained about such as fever, nausea, vomiting, and coughing.36 The CDC (2019) states that fever and cough are the most common symptoms that child Covid-19 patients often complain about, but other symptoms may arise such as nausea and vomiting that are not specific to COVID-19 symptoms. This requires accurate diagnostic tests. However, this often encounters obstacles including inadequate diagnostic test facilities, especially in remote areas, limited costs, incompetent professional staff, so that many cases are suspected of leading to Covid-19 but are not diagnosed.37
In addition to the physical symptoms that arise, the dominant psychological problem is also a complaint that is often reported. Symptoms of anxiety, fear, uncertainty, social phobia due to stigmatization, to xenophobia are individual symptoms that need attention.38 For this reason, it is necessary to plan short-term interventions that specifically deal with psychological problems arising from the Covid-19 pandemic.
All viruses, including SARS-CoV-2, have characteristics that change over time. So far hundreds of variants of this virus have been identified worldwide.39 Nurses involved in this study expressed a sense of confusion regarding the type of virus that continues to mutate. In 2021, the delta and omicron variants are the most dominant. Detected for the first time in Botswana, the omicron variant was identified as having a higher infectivity rate than the previous variant. In contrast to omicron, which has a lower risk of infection in people who have received complete vaccination, the delta variant is actually capable of significantly infecting people even though they have been completely vaccinated or commonly known as breakthrough infections.21 In line with this, in this study it was also reported that from several cases handled by nurses in the primary department, most of the patients who received complete vaccinations complained of mild symptoms such as cough, runny nose, dizziness, and an increase in body temperature.40 Specific to the symptoms caused by the Omicron variant, in this study it was stated that the complaints did not only include the symptoms as previously mentioned, but also the presence of digestive complaints such as nausea and vomiting.
Most COVID-19 patients have mild to moderate symptoms, but about 15% develop severe pneumonia and about 5% develop acute respiratory distress syndrome (ARDS), septic shock, and/or multiple organ failure.41,42 The therapy given consisted of symptomatic management and oxygen therapy. Although several antiviral drugs are being actively tested, none are specifically aimed at treating COVID-19.43 This finding explains some of the statements that emerged in this qualitative study that the drugs given in the health care facility setting are only drugs to treat symptoms.44 Education and explanations are needed for the public to understand the type and purpose of therapy given for Covid-19 so that there are no misunderstandings that result in issues of trust in health professionals and the government, including awareness to get vaccines that are proven effective in overcoming the spread of Covid-19.
The final theme in this qualitative research describes one of the obstacles that are often found among health professionals, namely unscrupulous public figures who do not believe in Covid-19. This has an impact on people who have an incorrect understanding due to misinformation and disinformation. There are several statements obtained, one of which is the culture of the village community who believes in the existence of pagebluk from a mythical point of view. People believe that Covid-19 is a common disease and there is no need to be too vigilant. (Sahoo et al, 2020) mentions that in essence myths or inaccurate information are widely published, in a very short time, and people tend to follow them without questioning their authenticity or looking for evidence. This can increase the stigma of society in dealing with the Covid-19 pandemic. As is the case with the statement obtained in this study which states that there is a reluctance to access health services despite experiencing health complaints for fear of being diagnosed with Covid-19. This supports another statement which states that there is a fear of reporting Covid-19 cases because of the poor response from the public. Patients tend to be dishonest in reporting their medical history. This has resulted in difficulties for nurses in the primary department to obtain accurate data from patients and families during the Covid-19 screening. As a result of this, the diagnosis is inaccurate and there is a high risk of transmission for both nurses, patient families, and other patients. Therefore, WHO (2020) recommends accurate information, and the broadcasting sector has a big role in influencing the public so that people perceive that what is conveyed by the broadcasting sector is the truth. In addition, evidence-based information needs to be encouraged to change people’s perceptions that are not correct regarding Covid-19. The ultimate goal is for the public to understand and support various government programs in handling Covid-10 so as to reduce morbidity and mortality.
This research will become input for health services that are more alert, anticipatory, responsive and resilient in facing the threat of health problems that occur now and in the future. Nursing professional organizations always promote Nurses with the People, Towards a Healthy Nation, Free of Covid-19. Nurses as the front line always experience many problems but they will never give up. The implication of this research is that it becomes the basis for policy holders to give appreciation for their services, educational institutions must improve adaptation-based education so that they always make a contribution. As well as professional organizations that are always there for nurses.
Limitations of the Study
The sample included in this study may not represent the entire context of primary care nurses in Indonesia. In addition, the use of stratified random sampling, especially related to geographic areas, is needed to generalize the findings in future studies.
Conclusion
This research reveals that The Dilemma of Nursing Clinical Practice, School cluster, Virus Type Confusion, Indigenous peoples do not believe in covid, Must be Excited and Alert are the main theme identified in this study. Making innovations to increase motivation thereby reducing mental and physical fatigue are the implications of the results of this study. Further exploration of the readiness of nurses to treat patients in the main department is believed to be beneficial for the results of this study.
Declarations Ethics
Authorization and agreement to take part: All individuals gave written agreement to participate in the study, as did the guardians of each participant. This study has been approved by the regional review board for STIKes Kepanjen (211/S.Ket/KEPK/STIKesKPJ/VI/2020). The Declaration of Helsinki’s guidelines for ethical research were followed in this study.
Acknowledgments
The authors would like to acknowledge all nurses who participated in this study for the support in the research work. This work was supported by Airlangga University, State University of Malang, Indonesia and Deanship of Scientific Research, KSU, Riyadh, Saudi Arabia.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Singh JA, Upshur REG. Personal view the granting of emergency use designation to COVID-19 candidate vaccines: implications for COVID-19 vaccine trials. Lancet Infect Dis. 2020;3099(20). doi:10.1016/S1473-3099(20)30923-3
2. Bary D, Dei-tumi SD, Humura F, Aja GN. Public health in practice we need to start thinking about promoting the demand, uptake, and equitable distribution of COVID-19 vaccines NOW! Public Health Pract. 2020;1:100063. doi:10.1016/j.puhip.2020.100063
3. Sohrabi C, Alsafi Z, O’Neill N, et al. World Health Organization declares global emergency: a review of the 2019 novel coronavirus (COVID-19). Int J Surg. 2020;76:71–76. doi:10.1016/j.ijsu.2020.02.034
4. Ma Z-Q, Zhu -Y-Y. A tentative study on the evaluation of community health service quality*. Phys Procedia. 2012;24:1628–1634. doi:10.1016/j.phpro.2012.02.240
5. World Health Organization. Clinical Care Severe Acute Respiratory Infection: Toolkit. COVID-19 Adaptation. World Health Organization; 2020.
6. World Health Organization. Clinical Management for COVID-19. Vol. 1. World Health Organization; 2020.
7. Zhao S, Yin P, Xiao LD, et al. Nursing home staff perceptions of challenges and coping strategies during COVID-19 pandemic in China. Geriatr Nurs. 2021;42(4):887–893. doi:10.1016/j.gerinurse.2021.04.024
8. Rahmatika QT, Aditya RS, Yusuf A, et al. We are facing some barriers: a qualitative study on the implementation of kangaroo mother care from the perspectives of healthcare providers. J Public Health Africa. 2022;13(s2):59–63. doi:10.4081/jphia.2022.2412
9. Spina S, Marrazzo F, Migliari M, Stucchi R, Sforza A, Fumagalli R. The response of Milan’s emergency medical system to the COVID-19 outbreak in Italy. Lancet. 2020;395(10227):e49–e50. doi:10.1016/S0140-6736(20)30493-1
10. Amberson T, Wells C, Gossman S. Increasing disaster preparedness in emergency nurses: a quality improvement initiative. J Emerg Nurs. 2020;46(5):654–665.e21. doi:10.1016/j.jen.2020.05.001
11. Henriette I, Taylor F, Dihle A, Hofsø K, Alexander S. Intensive care nurses’ Experiences of withdrawal of life-sustaining treatments in intensive care patients: a qualitative study. Intens Critl Care Nurs. 2019;102768. doi:10.1016/j.iccn.2019.102768
12. Verbeek JH, Rajamaki B, Ijaz S, et al. Personal protective equipment for preventing highly infectious diseases due to exposure to contaminated body fluids in healthcare staff. Cochrane Database Syst Rev. 2020;2020(4). doi:10.1002/14651858.CD011621.pub4
13. Delgado D, Quintana FW, Perez G, et al. Personal safety during the covid-19 pandemic: realities and perspectives of healthcare workers in latin America. Int J Environ Res Public Health. 2020;17(8):1–8. doi:10.3390/ijerph17082798
14. Davey SL, Lee BJ, Robbins T, Randeva H, Thake CD. Heat stress and PPE during COVID-19: impact on healthcare workers’ performance, safety and well-being in NHS settings. J Hospital Infect. 2021;108:185–188. doi:10.1016/j.jhin.2020.11.027
15. Hou Y, Zhou Q, Li D, Guo Y, Fan J, Wang J. Preparedness of our emergency department during the coronavirus disease outbreak from the nurses’ perspectives: a qualitative research study. J Emerg Nurs. 2020;46(6):848–861.e1. doi:10.1016/j.jen.2020.07.008
16. Tunlind A, Granström J, Engström Å. Nursing care in a high-technological environment: experiences of critical care nurses. Intens Crit Care Nurs. 2015;31(2):116–123. doi:10.1016/j.iccn.2014.07.005
17. Aditya RS, Solikhah FK, Kurniawan SB. Teenager response to the conditions of basic level emergency: a phenomenology study. Indian J Public Health. 2019;10(1):170.
18. Aditya RS, Yusuf A, Solikhah FK, et al. The experience of nurses in handling business class patient in commercial medical escort in Indonesia. Syst Rev Pharm. 2020;11(7):119–124. doi:10.31838/srp.2020.7.19
19. Grant AW, Buckley DJ. Nurse experiences and confidence in treating critically ill and injured patients following the completion of the first line emergency care course. Australas Emerg Care. 2019;22(4):236–242. doi:10.1016/j.auec.2019.05.002
20. Bagherian B, Sabzevari S, Mirzaei T, Ravary A. Meaning of caring from critical care nurses’ perspective: a phenomenological study. J Intens Crit Care. 2017;3:1–9. doi:10.21767/2471-8505.100092
21. Duong BV, Larpruenrudee P, Fang T, et al. Is the SARS CoV-2 omicron variant deadlier and more transmissible than delta variant? Int J Environ Res Public Health. 2022;19(8). doi:10.3390/ijerph19084586
22. Yusuf A, Tristiana RD, Aditya RS. Qualitative Research in Nursing.
23. Lupieri G, Creatti C, Palese A. Cardio-thoracic surgical patients’ experience on bedside nursing handovers: findings from a qualitative study. Intens Crit Care Nurs. 2016;35:28–37. doi:10.1016/j.iccn.2015.12.001
24. Squires A, Dorsen C. Qualitative research in nursing and health professions regulation. J Nurs Regulat. 2018;9(3):15–26. doi:10.1016/S2155-8256(18)30150-9
25. Al Razeeni DM, Al-Wathinani A, Alhazmi R, et al. The preparedness of emergency medical services students for coronavirus disease 2019: a cross-sectional study among paramedic students. Indian J Pharm Sci. 2021;5:177–184.
26. American Nurses Association. NEW pulse on the nation’s nurses survey series: half of frontline nurses emotionally over-whelmed by COVID- 19. News Release; 2020.
27. Anlıtürk DS. Perceived and sources of occupational stress in intensive care nurses during the COVID-19 pandemic. Intens Critl Care Nurs. 2020;67. doi:10.1016/j.iccn.2021.103107
28. Gerretsen P, Kim J, Caravaggio F, et al. Individual determinants of COVID-19 vaccine hesitancy. PLoS One. 2021;16:1–14. doi:10.1371/journal.pone.0258462
29. Gao X, Jiang L, Hu Y, Li L, Hou L. Nurses’ experiences regarding shift patterns in isolation wards during the COVID-19 pandemic in China: a qualitative study. J Clin Nurs. 2020;29(21–22):4270–4280. doi:10.1111/jocn.15464
30. Liu Q, Luo D, Haase JE, et al. Articles The experiences of health-care providers during the COVID-19 crisis in China: a qualitative study. Lancet Global Health. 2020;8(6):e790–e798. doi:10.1016/S2214-109X(20)30204-7
31. Yunitasari E, Yusuf A, Aditya RS, Acob JRU, Solikhah FK, Alrazeeni DM. Nursing students facilitating the transition from suicidal ideation to action in the rural: a qualitative study. Neuropsychiatr Dis Treat. 2023;19:171–180. doi:10.2147/ndt.s387362
32. Jing QL, Liu MJ, Bin ZZ, et al. Household secondary attack rate of COVID-19 and associated determinants in Guangzhou, China: a retrospective cohort study. Lancet Infect Dis. 2020;20(10):1141–1150. doi:10.1016/S1473-3099(20)30471-0
33. Lavezzo E, Franchin E, Ciavarella C, et al. Suppression of COVID-19 outbreak in the municipality of Vo’, Italy. MedRxiv. 2020;2020. doi:10.1101/2020.04.17.20053157
34. Kostas D, Epaulard O, Benet T, et al. Cluster of coronavirus disease 2019 (Covid-19) in the French Alps, 2020. Clin Infect Dis. 2020;2019(1):825–832.
35. Tsankov BK, Allaire JM, Irvine MA, et al. Severe COVID-19 infection and pediatric comorbidities: a systematic review and meta-analysis. Int J Infect Dis. 2021;103:246–256. doi:10.1016/j.ijid.2020.11.163
36. Aditya RS, Yusuf A, Al Razeeni DM, Al-Sayaghi KM, Solikhah FK. “We are at the forefront of rural areas” emergency nurse’s experience during pandemic: a qualitative study. Health Equity. 2021;5(1):818–825. doi:10.1089/heq.2021.0080
37. Israfil SMH, Sarker MMR, Rashid PT, et al. Clinical characteristics and diagnostic challenges of COVID−19: an update from the global perspective. Front Public Health. 2021;8:1–17. doi:10.3389/fpubh.2020.567395
38. Heitzman J. Impact of COVID-19 pandemic on mental health. Psychiatr Pol. 2020;54(2):187–198. doi:10.12740/PP/120373
39. World Health Organization. Coronavirus Disease (COVID-19): Virus Evolution. World Health Organization; 2020.
40. Yusuf A, Aditya RS, Yunitasari E, Aziz AN, Solikhah FK. Experience of persons affected by leprosy in facing psychosocial problems: a qualitative method. Syst Rev Pharm. 2020;11(7):219–223.
41. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
42. Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8(4):420–422. doi:10.1016/S2213-2600(20)30076-X
43. Cao X. COVID-19: immunopathology and its implications for therapy. Nat Rev Immunol. 2020;20(5):269–270. doi:10.1038/s41577-020-0308-3
44. Aditya RS, Yusuf A, Solikhah FK, Kurniawan SB, Abdullah SRS. Nurse’s experiences in handling stretcher patients on commercial medical escort in Indonesia: a qualitative study. Bangladesh J Med Sci. 2022;21(3):502–511. doi:10.3329/bjms.v21i3.59562
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.