")
Back to Journals » International Journal of General Medicine » Volume 16
Vulnerability of NCDs and Mediating Effect of Risk Behaviors Among Tuberculosis Patients and Their Household Contacts Compared to the General Population in the Yangon Region, Myanmar
Authors Zayar NN , Chotipanvithayakul R , Bjertness E , Htet AS , Geater AF , Chongsuvivatwong V
Received 8 September 2023
Accepted for publication 4 December 2023
Published 13 December 2023 Volume 2023:16 Pages 5909—5920
DOI https://doi.org/10.2147/IJGM.S439141
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sandul Yasobant
Nyi Nyi Zayar,1 Rassamee Chotipanvithayakul,1 Espen Bjertness,2 Aung Soe Htet,2 Alan Frederick Geater,1 Virasakdi Chongsuvivatwong1
1Department of Epidemiology, Faculty of Medicine, Prince of Songkla University, Hat Yai, Songkhla, 90110, Thailand; 2Department of Community Medicine and Global Health, Institute of Health and Society, Faculty of Medicine, University of Oslo, Oslo, Norway
Correspondence: Rassamee Chotipanvithayakul, Department of Epidemiology, Faculty of Medicine, Prince of Songkla University, 6th Floor of Administrative Building, 15 Kanjanavanich Road, Hat Yai, Songkhla, 90110, Thailand, Tel +66-074-451165, Email [email protected]
Purpose: We investigated the association of TB patients and their household contacts with diabetes mellitus (DM) and hypertension compared to the general population, and the mediating effects of risk behaviors including current smoking, alcohol drinking, and poor diet quality.
Patients and Methods: A cross-sectional study on screening for DM, hypertension, and risk behaviors among newly diagnosed TB patients (n = 221) and their household contacts (n = 257) aged 25– 74 years in Yangon in 2018. Health data of the general population (n = 755) were obtained from an NCD risk factor survey in Yangon. A directed acyclic graph is used to identify possible pathways of association between variables. Associations are presented as adjusted odds ratios (aOR).
Results: Compared to the general population, both TB patients and their household contacts were associated with current smoking and drinking, and TB patients were more likely to be underweight. Without considering mediating effects, TB patients had higher odds of DM (aOR = 6.3, 95% CI: 3.8– 10.6), but both TB patients and household contacts had lower odds of hypertension (aOR = 0.54; 95% CI: 0.33– 0.87) and (aOR = 0.68; 95% CI: 0.47– 0.98), respectively. The body mass index-mediated pathway reduced the odds of DM and hypertension among TB patients (aOR = 3.4; 95% CI: 2.2– 5.3) and (aOR = 0.3; 95% CI: 0.2– 0.5), respectively.
Conclusion: The shared risk behaviors among TB patients and household contacts with high burden of DM in TB patients endorse screening of risk behaviors and strengthening the integration of NCD services among TB patients and household contacts in this dual-burden country.
Keywords: TB, diabetes mellitus, hypertension, non-communicable diseases, screening, mediator
Introduction
Globally, communicable diseases account for more than 60% of the disease burden in low-income countries, while non-communicable diseases (NCDs) account for more than 80% in high-income countries.1 Yet, the burden of both communicable diseases and NCDs is higher in low- and middle-income countries with socioeconomic and demographic transitions like Myanmar.2 Tuberculosis is the second leading cause of death among patients with communicable diseases, and the prevalence of tuberculosis (TB) in Myanmar was 468 (95% CI: 391–546) per 100,000 in 2018,3 which was three times the global average.4 The prevalence of major NCDs, including diabetes mellitus (DM) and hypertension, were 10.5% and 26.4%,5 respectively, which was similar to regional averages.6,7 Both communicable diseases and NCDs are significantly associated with behavioral risk factors such as smoking, alcohol drinking, and impaired diet quality.8 Almost one-fourth of the population in Myanmar was reported to have at least one behavioral risk factor.5 Therefore, exploring the dual impact of TB alongside DM and hypertension, which are all linked to behavioral risk factors, is essential to identify the scale of the problem and develop a strategy to address the interconnected health issues simultaneously.
Patients with TB are not only associated with NCDs through a direct link via pathophysiological changes,9,10 but they also share behavioral risk factors, including smoking, alcohol consumption, and poor diet.8 Identifying the direct and the total effects of association would allow us to understand the mediating effects of behavioral risk factors between TB and the comorbidities of DM and hypertension. Furthermore, family members in the same household usually share the same socioeconomic status and risk behaviors such as smoking and alcohol drinking.11,12 Therefore, we hypothesized that household contacts of TB patients even without TB might have a higher risk of getting NCDs due to having similar risk behaviors.
The global action plan on NCDs recognized the significant interaction between TB and NCDs and endorsed the integration of programs and services between these diseases.13 The World Health Organization (WHO) has recommended bi-directional screening programs for TB and DM in developing countries since 2011.14 This program has been implemented in some pilot areas at central and township-level TB clinics in Myanmar since 2018. Nevertheless, the program did not include identifying and reducing the burdens of NCDs like hypertension and behavioral risk factors among TB patients and their household contacts. Understanding the co-existence of NCDs and behavioral risk factors among TB patients and their household contacts without TB would allow healthcare planners to evaluate existing healthcare programs and plan for further control action.
Therefore, this study aimed to investigate the direct effect of association between the population groups (ie, TB patients, household contacts, and the general population of the Yangon Region) with risk behaviors (ie, smoking, alcohol drinking, and poor diet, which are associated with body mass index [BMI]). Primarily, we aimed to investigate the total and direct effects of the associations between the population groups and the comorbidities of diabetes mellitus and hypertension with the mediating effect of selected risk behaviors.
Materials and Methods
Study Design and Setting
A cross-sectional study was conducted in township TB clinics and households of TB patients in the townships of Insein and North Okkalapa in Yangon, Myanmar from April to December 2018. The study obtained information of index TB patients from TB registration and their household contacts. Moreover, we received approval to use secondary data from the NCD risk factor survey done in the Yangon Region as a comparison group.15 The survey was based on the WHO STEPwise approach for the surveillance of NCD risk factors developed by WHO to help countries develop and strengthen their NCD surveillance systems.16 This NCD risk factor survey was done in the Yangon urban area from September to November 2013.
Study Sample, Sample Size, and Sampling Technique
Our study consecutively recruited patients with newly diagnosed TB from two selected township TB clinics and further investigated their household contacts aged 25–74 years. We expected to have at least 80 TB patients and 80 participants from the general population to test the hypothesis that TB patients have at least 4 times and 3 times higher odds of having DM and hypertension than the general population, respectively, with a 20% non-response rate. We used two independent proportions formulas using 12.1%17 and 34.5%18 prevalence rates of DM and hypertension in the general population, respectively. For household contacts, we expected to have at least 220 participants and 220 participants from the general population to test the hypothesis that they had at least 2.5 times and 2 times higher odds of having DM and hypertension compared to the general population, respectively, with a 30% non-response rate. The same prevalence of DM17 and hypertension18 in the general population were applied using the same formulas.
In the NCD risk factor survey, 755 participants aged 25–74 years from the general population were recruited in urban areas of the Yangon Region in Myanmar.17 Buddhist monks, nuns, institutionalized people, military people, and pregnant women were excluded. Multi-stage cluster sampling was done. First, six townships in urban areas were randomly selected. Then, five township sub-units were randomly selected from the six townships to achieve a total of 30 sub-units. From each sub-unit, 26 to 27 households were randomly selected. Only one eligible household member was randomly recruited.
Data Collection Tools and Process
The data collection process and measurements of variables used in this study and in the NCD risk factor survey were comparable in regard to the NCD risk factors but differed slightly in the screening tools used for DM and hypertension as summarized in Table 1.
 |
Table 1 Comparing the Data Collection Processes and Measurements of Variables Used in Our TB and Household Contact Study with the NCD Risk Factor Survey |
In this study, a list of newly diagnosed sputum-positive TB patients aged 25–74 years was obtained from the two township TB registers. They were informed of the study and invited to participate. After informed consent was received, patients were interviewed at the TB clinic about their sociodemographic characteristics, NCD risk behaviors, and NCD outcomes using a structured questionnaire. Following the WHO STEPS manual,16 current smoking was defined as currently smoking any tobacco products daily and current drinking was defined as drinking alcohol within the past 30 days, DM was assessed by a diagnosis given by a medical doctor, whereas hypertension was assessed by a history of taking any medication for increased blood pressure due to hypertension prescribed by a health worker within the past 2 weeks.
In addition, a physical examination on anthropometric parameters, blood pressure measurements, and blood glucose tests were also performed following the WHO STEPS manual.16 Height was measured without footwear, and hat using a measuring tape and weight was measured using a weighing scale and measurement was taken up to the nearest 0.1 kg. The blood pressure measurement was taken after letting the participant rest for at least 10 min. The sphygmomanometer cuff was placed over the left arm. Three readings were conducted, and the average was taken. Fasting capillary blood glucose (FCG) tests were done after 10 hr fasting in the following morning at the clinic.
Household contact tracing was done among those who lived in the same household with TB patients for at least 3 months. Healthcare volunteers visited their home, explained the risks of tuberculosis infection, asked them to complete a questionnaire that screened for signs and symptoms of TB. A similar interview, measurements, and blood tests for NCD risk factors, DM, and hypertension were applied to household contacts. They were subsequently requested to attend the TB clinic within 2 weeks for a chest X-ray (CXR) and FCG testing. If the TB contacts did not visit the clinic as appointed, a second home visit was conducted to collect early morning FCG and the TB contacts were reinvited to the clinic for a CXR. TB contacts with positive signs and symptoms of TB or whose CXR was suggestive of TB underwent sputum examination and the GeneXpert test. Household contacts who were diagnosed with TB were considered newly diagnosed TB patients.
In the NCD risk factor survey, researchers provided information to eligible participants at their home. After obtaining informed consent, they were interviewed concerning general profile and health risk behaviors using the same manual.16 Anthropometric indices, blood pressure, and fasting plasma glucose test were also measured following the same manual16 but using different tools as described in Table 1.
Variables
This study and the NCD risk factor survey used the same definitions and cutoff levels for all variables. A smear-positive TB patient was defined using positive results from either the sputum smear test or the GeneXpert test for both index patients and contacts as bacteriologically positive TB.21 For those who could not produce sputum, a clinical diagnosis using positive signs and symptoms of TB and CXR suggestive of TB was used. DM was identified either as a self-reported DM noted to be diagnosed by a medical doctor or as a blood glucose screening test with an FPG level ≥7 mmol/L, or both, based on the NCD risk factor survey, which followed the WHO criteria.15,16,22 Hypertension was defined as self-reported hypertension with use of antihypertensive medication within 2 weeks prior to the interview, or systolic blood pressure (SBP) ≥140 mmHg, or diastolic blood pressure (DBP) ≥90 mmHg in the study, or all of these.5,15
Definitions of independent variables that included sociodemographic characteristics, such as age group, education, and occupation and behavioral risk factors, such as current smoking and drinking, followed the WHO STEPS survey methodology and reports in Myanmar.5,16 Age groups were categorized into 10-year intervals from 25 to 74 years. Education levels were categorized into no formal schooling, less than primary school, primary school completed, secondary school completed, high school completed, and college/university. Occupation levels were categorized into retired, dependent, self-employed, non-government employee, and government employee. Daily income per household member was calculated from the total household income divided by the total number of household members to arrive at a value in the national currency of Myanmar Kyat (MMK). MMK was then converted into United States dollars (USD) using the exchange rate of 1 USD = 1328 MMK during our study in 2018 and the exchange rate of 1 USD = 953.8 MMK in the NCD risk factor survey in 2013.23 The average daily household incomes per person/day calculated by the World Bank for the years 2013 and 2018 were 1.9 USD and 3.1 USD, respectively, which were used as the poverty level cutoff values in this study.24
Behavioral risk factors included current smoker and current drinker defined as an individual who currently smoked any tobacco products daily, and an individual who drank alcohol within the past 30 days. BMI was classified into four groups following the WHO expert consultation for the Asian population as underweight (<18.5 kg/m2), normal weight (18.5–22.9 kg/m2), overweight (23.0–27.4 kg/m2), and obese (≥27.5 kg/m2).25
Statistical Analysis
Data analysis was done using R software.26 Background characteristics of TB patients, their household contacts, and the general population are presented using descriptive statistics. Chi-square test was used to test the differences between the prevalence of risk behaviors and NCDs among different types of population. A directed acyclic graph (DAG) was constructed using DAGitty v3.0 software27 to identify the possible pathways influencing the association between population type with risk behaviors (ie, current smoking, current drinking, and BMI) and DM and hypertension (Figure 1). Direct effects of association were identified to detect the association between population type and the selected risk behavior and not explicitly mediated by other risk behaviors. The associations of population type with current alcohol drinking and smoking were explored using binary logistic regression reported by adjusted odds ratio (aOR) and with status of BMI using multinomial regression reported by adjusted relative risk ratio (aRRR). A likelihood ratio test (p-value <0.05) was considered as the level of significance in binary logistic regression and the Wald test was used to define the significance level of each outcome in a multinomial regression model.
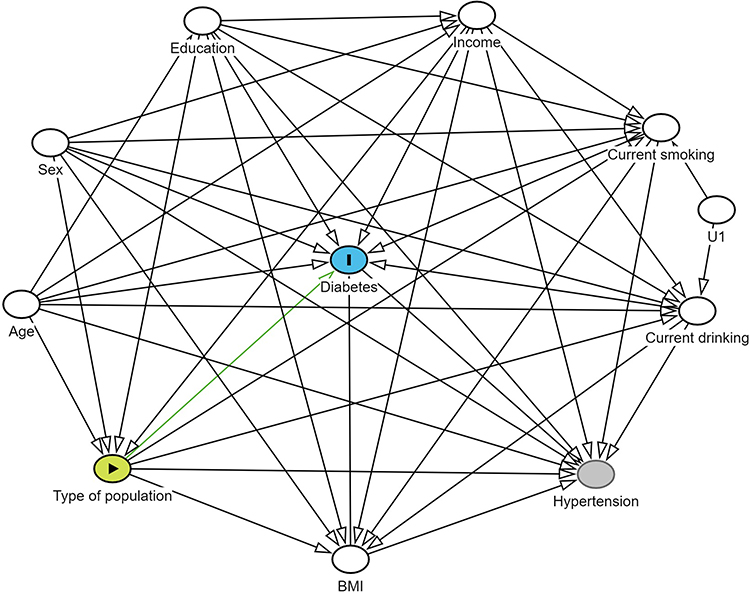 |
Figure 1 Direct Acyclic Graph for association between type of population with DM and Hypertension. (The current figure showed a model for direct effect of association between type of population and DM by adjusting potential confounders. A similar causal relationship pattern was used to identify the direct, sub-total, and total effects of association between population type with DM and hypertension). Abbreviations: BMI, body mass index; U1, an unmeasured variable influencing current smoking and current drinking behavior. Notes: Green circle with black arrowhead: exposure variable. Blue circle with “I” symbol: outcome variable of interest. White circles: adjusted variables. Grey circle: unobserved variable. Green arrow: causal path between exposure and outcome in current model. Black arrow: causal relationship between variables. |
Both direct effect and total effect of population type on DM and hypertension were tested to see the effects of risk behaviors on the association. For the total effect of an association, all confounders identified in the DAG were controlled to estimate the combined effect of exposure going directly to the outcome and the effect going through other variables (mediators). For the direct effect of an association, mediators were adjusted in addition to confounders to remove the effect of exposure going through other variables (mediators).28 In DAG, age, sex, level of education, and income level were considered as confounders and risk behaviors (ie, current smoking, current alcohol drinking, and BMI) were placed as mediators between population type and DM or hypertension. Selected mediation effects were estimated by separately adding potential mediation pathways to the direct effect models, referred to here as “sub-total models”, to see the effect of selected risk behavior on the association. DM is also considered as a mediator between population type and hypertension. Multivariable logistic regression was used to control the minimal set of confounders and to selectively include or exclude mediated pathways indicated by the DAG to estimate the risks of getting DM or hypertension among different population types. In the regression models, only confounders were adjusted to test the total effect and both confounders and mediators were included for the direct effect.
Results
Two hundred and twenty-one eligible index TB patients gave consent to participate in the study and received a full investigation for a 100% response rate. Out of 336 household contacts, 71 and 8 of them were excluded due to unavailable data of TB and DM, respectively, for a 24% non-response rate. Two hundred and fifty-seven household contacts remained for the data analysis. A total of 755 subjects from the general population were included in the study for a non-response rate of 14%.
Table 2 shows the background characteristics of the populations in this study. A majority of household contacts were female (68.9%), while most TB patients were male (66.1%) and the proportions of each sex were more or less equal in the general population. The age distribution of participants in the three distinct populations was fairly similar across all age groups, but with a slight decrease in the proportion of individuals older than 65 years among TB patients. Almost half of the participants among household contacts and TB patients had received less than secondary school level education, while more than 70% of the general population had at least secondary school level. Individuals who were self-employed were over-represented among TB patients, while dependents were more common in household contacts. TB patients and their household contacts had higher incomes than the general population.
 |
Table 2 Background Characteristics of TB Patients, Household Contacts, and the General Population |
Table 3 reveals that TB patients had about two and three times the percentages of current smokers and current drinkers, respectively, compared to the general population. TB patients also had five times and seven times higher percentages of being underweight compared to household contacts and the general population, respectively. Similarly, the percentage of patients with TB was nearly twice the general population. In contrast, both the patients with TB and their household contacts had a lower proportion of hypertension than the general population.
 |
Table 3 Prevalences of Risk Behaviors and Non-Communicable Diseases Among TB Patients, Household Contacts of TB Patients, and the General Population |
Association Between Population Type and Risk Behaviors Including Smoking, Alcohol Drinking, and Body Mass Index
Table 4 shows the direct association between population type and behavioral risk factors that include current smoking, current drinking, and BMI. TB patients and household contacts had higher odds of current smoking and drinking. Household contacts had 1.7 times and 2.1 times higher odds of current smoking and drinking, while TB patients had 2.5 times and 4.6 times higher odds of current smoking and drinking than the general population. Using a normal BMI as the baseline, TB patients had 7 times the relative probability of being underweight and 62% and 92% lower relative probability of being overweight and obese, respectively, compared to the general population. Household contacts also showed a higher relative probability of being underweight, though this was not statistically significant.
 |
Table 4 Direct Effect of Association Between Population Type and Risk Behaviors Including Current Smoking, Current Alcohol Drinking, and Body Mass Index |
Risk of DM and Hypertension Among TB Patients and Their Household Contacts Compared to the General Population
Table 5 depicts the multivariable logistic regressions to test the direct, sub-total, and total effects of association between population type with DM and hypertension adjusted by other variables suggested by the DAG. No significant association was found between household contacts and DM in either the direct or the total effect models. However, the direct effect model reported that TB patients had 6.3 times higher odds of having DM compared to the general population. The sub-total effect shows similar results when either current smoking or drinking is considered as a mediator in the model. However, the odds were reduced significantly to 3.4 when the BMI-mediated pathway was opened (p ≤ 0.001). TB patients had 3 times higher odds of DM when all three risk behavior-mediated pathways were operative.
 |
Table 5 Logistic Regression of the Direct Effect, Sub-Total Effect, and Total Effect of Population Type on the Risks of Diabetes Mellitus and Hypertension |
In contrast, both household contacts and TB patients showed significantly lower odds of hypertension in both direct, sub-total, and total effect models compared to the general population. Household contacts had 32% lower odds of hypertension in both direct, sub-total, and total effect estimations. TB patients showed around 45% lower odds of being associated with hypertension in direct effect estimation and showed similar results when an additional pathway mediated by current smoking or by current drinking was opened. Opening the BMI-mediated pathway, however, caused a further decrease in the odds of hypertension (p < 0.001) to 71% lower than the general population.
Discussion
This study reports four main results. First, TB disease is not the only health problem among TB patients. They had higher risks of smoking, drinking, being underweight, and having DM than the general population. Second, the study newly reported increased risks of smoking and drinking behaviors among household contacts, even without TB, compared to the general population. Third, we found BMI was an important mediating factor for DM and hypertension among patients with TB. Last, but not least, TB patients and their household contacts had lower odds of hypertension.
TB patients had 1.8 times and 4.6 times higher odds of current smoking and drinking compared to the general population. This finding is similar to findings from previous studies done in India,29,30 and both smoking and drinking were significant risk factors for TB infection.31,32 Both smoking and alcohol drinking not only impose a burden on NCDs but also have a negative impact on the treatment outcome of TB.29,33,34 Although information on risk factors for NCDs among household contacts is limited, our study also highlighted increased odds of current smoking (1.7 times) and drinking (2.1 times) compared to the general population. This may be associated with increased patterns of smoking and drinking among TB patients. Previous studies revealed that family members have a common inclination towards risky behaviors, and the status of smoking and drinking is highly associated with family influences.11,12 This finding suggests that health personnel should assess health risk behaviors in both TB patients and their household contacts, and also provide appropriate intervention to control them.
TB patients had a seven times higher risk of being underweight compared to the general population. Malnutrition associated with a poor socioeconomic condition leads to immunodeficiency and increases susceptibility to TB infection.35 Tuberculosis itself also results in malnutrition because of decreased appetite, malabsorption of macro- and micro-nutrients, and the change in metabolism leads to wasting.35 As a result, underweight was significantly more common in patients with TB than in the general population.36 In turn, being underweight can delay TB recovery and result in a higher mortality rate.36,37
When no explicit mediating effect was taken into account, patients with TB had 6.3 times higher odds of DM compared to the general population. A previous meta-analysis reported that DM patients had a 3 times higher risk of TB due to their immunocompromised condition.38 When BMI status was taken as a mediator, our study found that the association between TB and DM was reduced by almost half (aOR = 3.4; 95% CI: 2.2–5.3). This may be due to almost half of the TB patients in this study being underweight. Similarly, a previous study in India reported that underweight TB patients had significantly lower odds of DM compared to normal weight TB patients.39 However, this mediating effect was not observed among the household contacts compared to the general population.
Compared to the general population, the odds of hypertension were reduced by 50% among TB patients and 30% among household contacts. This may be related to unobserved variables associated with socioeconomic characteristics and environment. When taking BMI status into account as a mediating factor, the odds of hypertension among TB patients showed a further reduction to 70% compared with the general population but no change was observed in household contacts. Consistently, a case–control study done in North-West England found that TB patients were 2.6 times less likely to have hypertension compared to those without TB.40 Overweight and obesity are already known to be significant risk factors for hypertension. A previous meta-analysis of 25 randomized controlled trials revealed an association between net weight reduction and the decrease in both SBP and DBP.41 TB patients in our study, however, were more likely to be underweight compared to the general population. Therefore, reduced BMI among TB patients could subsequently reduce the risk of getting hypertension among TB patients. When taking smoking and drinking behaviors into consideration, a mediating effect was not observed in either DM or hypertension in TB patients and household contacts compared to the general population.
Our study has some limitations to address. Our TB patients and household contacts had higher average household income than the general population. This likely occurred because our TB patients who could access healthcare might have higher socioeconomic status than those who could not access healthcare. Another factor may be the difference in inflation rates from the time of the NCD survey and the time of our study 5 years later. However, this should not change the mediating effects reported in this study because daily household income was adjusted in the model.
Due to limited resources, full investigations for NCDs were not feasible. However, the study accommodated the measurements recommended by the WHO STEPS guideline.16 Single-time blood glucose testing was conducted and this made it comparable with the NCD risk factor survey.15 Screening of diabetes in our study was done using an ACCU-CHEK® Performa glucometer, while the NCD risk factor survey used the FPG test. The ACCU-CHEK® Performa glucometer showed ≥96% of the results equivalent (±0.6 mmol/L) to the glucose concentrations in plasma.42 The WHO recommends using capillary sampling in under-resourced countries and accepts that the fasting values for capillary plasma glucose and venous blood are identical.22 Blood pressure measurements were performed three times during a single visit in both studies due to time constraints and limited resources. However, it is comparable to the NCD risk factor survey15 and STEPS survey report in Myanmar.5 Additionally, our study was able to detect an association between TB and hypertension regardless of nondifferential misclassification bias towards the null hypothesis.
Our study findings suggest that a TB control program should also provide investigations for other NCDs, including fasting blood glucose and blood pressure monitoring. Even though our study showed that the BMI-mediated effect reduced the odds of DM and hypertension among TB patients, a high proportion of underweight status may impact treatment outcomes of TB. Therefore, maintaining a normal BMI status should be targeted. Screening for NCDs and risk factors does not require sophisticated tools and is not time-consuming but is very useful for both TB and NCD control.
Conclusions
Compared to the general population, TB patients had increased proportions of current smoking, current alcohol drinking, and underweight status and a high burden of DM, while household contacts of TB patients showed higher proportions of smoking and alcohol drinking. The mediation effect of BMI among TB patients significantly reduced the odds of DM and of hypertension. The integrated TB-NCD programs need to be strengthened to identify and address both risk behaviors and DM among TB patients. Furthermore, another need is to screen and reduce risk behaviors in household contacts during contact tracing activity to ensure improved control of NCDs in Myanmar.
Abbreviations
NCDs, non-communicable diseases; DM, diabetes mellitus; BMI, body mass index; WHO, World Health Organization; FPG, fasting venous plasma glucose; FCG, fasting capillary plasma glucose; CXR, chest X-ray; SBP, systolic blood pressure; DBP, diastolic blood pressure; MMK, Myanmar Kyat; USD, United States dollar; DAG, directed acyclic graph, aOR, adjusted odds ratio; aRRR, adjusted relative risk ratio; CI, confidence interval; ref, reference.
Data Sharing Statement
The dataset supporting the conclusion of this article is available upon request from the corresponding author.
Ethics Approval
Ethical approval of the TB patients and household contacts survey was obtained from the Ethics Review Committee at Prince of Songkla University (33/2017) and the Ethics Review Committee at the Department of Medical Research, Myanmar (023/2018). Approval for NCD risk factor survey data was obtained from the Department of Health, Myanmar, and Ethics Committee from the Norwegian Regional Committees for Medical and Health Research Ethics (2013/1088). The study complies with the Declaration of Helsinki.
Acknowledgments
This research was supported by the Prince of Songkla University under the Postdoctoral Fellowship Program. We would like to acknowledge Saw Saw and Si Thu Aung for their supervision and support during the data collection period. We would also like to acknowledge all study participants, research assistants, township tuberculosis coordinators, township health officers, and basic health staff in the study townships and responsible persons in the Yangon Regional Tuberculosis Program, Department of Public Health, Myanmar. We also want to express our gratitude to the University of Oslo and Norad/NORHED, Project: MMY-13/0049 “Health and Sustainable Development in Myanmar—Competence Building in Public Health and Medical Research and Education (MY-NORTH)”, for sharing data of the NCD risk factors survey in the Yangon Region.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Research reported in this publication was supported by the Fogarty International Center and the National Institute of Allergy and Infectious Diseases of the National Institutes of Health under Award Number D43TW009522. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Additional funding was also available from the Department of Medical Research, Myanmar, and a Graduate School Scholarship from Prince of Songkla University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Roser M, Ritchie H, Spooner F. Burden of disease. Our World in Data; September 25, 2021. Available from: https://ourworldindata.org/burden-of-disease.
2. Boutayeb A. The Burden of Communicable and Non-Communicable Diseases in Developing Countries. In: Preedy VR, Watson RR editors. Handbook of Disease Burdens and Quality of Life Measures. Springer; 2010:531–546. doi:10.1007/978-0-387-78665-0_32.
3. Aung ST, Nyunt WW, Moe MM, et al. The Fourth National Tuberculosis Prevalence Survey in Myanmar. PLOS Global Public Health. 2022;2(6):e0000588. doi:10.1371/journal.pgph.0000588
4. End TB in Myanmar | endTB. Available from: https://endtb.org/myanmar.
5. 2014 STEPS Country Report Myanmar. Available from: https://www.who.int/publications/m/item/2014-steps-country-report-myanmar.
6. Roglic G, Varghese C, Thamarangsi T. Diabetes in South-East Asia: burden, gaps, challenges and ways forward. WHO South-East Asia J Public Health. 2016;5(1):1. doi:10.4103/2224-3151.206546
7. Neupane D, McLachlan CS, Sharma R, et al. Prevalence of hypertension in member countries of South Asian Association for Regional Cooperation (SAARC): systematic review and meta-analysis. Medicine (Baltimore). 2014;93(13):e74. doi:10.1097/MD.0000000000000074
8. NCDs | major NCDs and their risk factors. WHO. Available from: https://www.who.int/health-topics/noncommunicable-diseases.
9. Jeon CY, Harries AD, Baker MA, et al. Bi-directional screening for tuberculosis and diabetes: a systematic review. Trop Med Int Health. 2010;15(11):1300–1314. doi:10.1111/j.1365-3156.2010.02632.x
10. Huaman MA, Henson D, Ticona E, Sterling TR, Garvy BA. Tuberculosis and cardiovascular disease: linking the epidemics. Trop Dis Travel Med Vaccines. 2015;1(1):10. doi:10.1186/s40794-015-0014-5
11. Joung MJ, Han MA, Park J, Ryu SY. Association between family and friend smoking status and adolescent smoking behavior and e-cigarette use in Korea. Int J Environ Res Public Health. 2016;13(12):1183. doi:10.3390/ijerph13121183
12. LaBrie JW, Kenney SR, Lac A, Migliuri SF. Differential drinking patterns of family history positive and family history negative first semester college females. Addict Behav. 2009;34(2):190–196. doi:10.1016/j.addbeh.2008.10.012
13. Integration of Prevention and Control of Non-Communicable Diseases and Tuberculosis: A Case for Action. World Health Organization. Available from: https://www.who.int/publications-detail-redirect/9789240061682.
14. Stop TB Initiative (World Health Organization), World Health Organization, Department of Chronic Diseases and Health Promotion, International Union against Tuberculosis and Lung Disease. Collaborative Framework for Care and Control of Tuberculosis and Diabetes. 2011.
15. Htet AS, Bjertness MB, Sherpa LY, et al. Urban-rural differences in the prevalence of non-communicable diseases risk factors among 25–74 years old citizens in Yangon Region, Myanmar: a cross sectional study. BMC Public Health. 2016;16(1):1225. doi:10.1186/s12889-016-3882-3
16. WHO STEPwise approach to noncommunicable disease risk factor surveillance (STEPS). Available from: https://www.who.int/teams/noncommunicable-diseases/surveillance/systems-tools/steps/manuals.
17. Aung WP, Htet AS, Bjertness E, Stigum H, Chongsuvivatwong V, Kjøllesdal MKR. Urban–rural differences in the prevalence of diabetes mellitus among 25–74 year-old adults of the Yangon Region, Myanmar: two cross-sectional studies. BMJ Open. 2018;8(3):e020406. doi:10.1136/bmjopen-2017-020406
18. Htet AS, Bjertness MB, Oo WM, et al. Changes in prevalence, awareness, treatment and control of hypertension from 2004 to 2014 among 25-74-year-old citizens in the YangonRegion, Myanmar. BMC Public Health. 2017;17(1):847. doi:10.1186/s12889-017-4870-y
19. Topouchian J, Agnoletti D, Blacher J, et al. Validation of four devices: omron M6 Comfort, Omron HEM-7420, Withings BP-800, and Polygreen KP-7670 for home blood pressure measurement according to the European Society of Hypertension International Protocol. VHRM. 2014;10:33–44. doi:10.2147/VHRM.S53968
20. Accu-Chek Performa. Accu-Chek®. Available from: https://www.accu-chek.com.au/meter-systems/performa.
21. World Health Organization. Chest Radiography in Tuberculosis Detection: Summary of Current WHO Recommendations and Guidance on Programmatic Approaches. World Health Organization; 2016. Available from: https://apps.who.int/iris/handle/10665/252424.
22. World Health Organization, International Diabetes Federation. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycaemia: Report of a WHO/IDF Consultation; 2006. Available from: https://www.who.int/publications-detail-redirect/definition-and-diagnosis-of-diabetes-mellitus-and-intermediate-hyperglycaemia.
23. Reference Exchange Rate - History. Available from: https://forex.cbm.gov.mm/index.php/fxrate/history.
24. Ferreira FHG, Chen S, Dabalen AL, et al. A Global Count of the Extreme Poor in 2012: data Issues, Methodology and Initial Results. The World Bank; 2015:1–66. Available from: http://documents.worldbank.org/curated/en/360021468187787070/A-global-count-of-The-extreme-poor-in-2012-data-issues-methodology-and-initial-results.
25. WHO expert consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–163. doi:10.1016/S0140-6736(03)15268-3
26. R: the R Project for Statistical Computing; January 21, 2020. Available from: https://www.r-project.org/.
27. Textor J, van der Zander B, Gilthorpe MS, Liśkiewicz M, Ellison GT. Robust causal inference using directed acyclic graphs: the R package ‘dagitty. Int JEpidemiol. 2016;45(6):1887–1894. doi:10.1093/ije/dyw341
28. Tennant PWG, Murray EJ, Arnold KF, et al. Use of directed acyclic graphs (DAGs) to identify confounders in applied health research: review and recommendations. Int JEpidemiol. 2021;50(2):620–632. doi:10.1093/ije/dyaa213
29. Mahishale V, Patil B, Lolly M, Eti A, Khan S. Prevalence of smoking and its impact on treatment outcomes in newly diagnosed pulmonary tuberculosis patients: a hospital-based prospective study. Chonnam Med J. 2015;51(2):86–90. doi:10.4068/cmj.2015.51.2.86
30. Thapa P, Kamath R, Shetty BK, Monteiro A, Sekaran VC. Prevalence and associated factors of alcoholism among tuberculosis patients in Udupi Taluk, Karnataka, India: a Cross Sectional Study. J Nepal Health Res Counc. 2014;12(28):177–181.
31. Lienhardt C, Fielding K, Sillah JS, et al. Investigation of the risk factors for tuberculosis: a case–control study in three countries in West Africa. Int J Epidemiol. 2005;34(4):914–923. doi:10.1093/ije/dyi100
32. Soh AZ, Chee CBE, Wang YT, Yuan JM, Koh WP. Alcohol drinking and cigarette smoking in relation to risk of active tuberculosis: prospective cohort study. BMJ Open Respir Res. 2017;4(1):e000247. doi:10.1136/bmjresp-2017-000247
33. Mujezinović A, Čalkić L, Hasanica N, Tandir S. Tobacco and alcohol usage as risk factors of non-communicable diseases among students of Zenica University (Bosnia and Herzegovina). Medicinski Glasnik. 2018;15(1):81–86. doi:10.17392/933-18
34. Cox SR, Gupte AN, Thomas B, et al. Unhealthy alcohol use independently associated with unfavorable TB treatment outcomes among Indian men. Int J Tuberc Lung Dis. 2021; 25:182–190. doi:10.5588/ijtld.20.0778
35. Gupta KB, Gupta R, Atreja A, Verma M, Vishvkarma S. Tuberculosis and nutrition. Lung India. 2009;26(1):9–16. doi:10.4103/0970-2113.45198
36. Cegielski JP, Arab L, Cornoni-Huntley J. Nutritional Risk Factors for Tuberculosis Among Adults in the United States, 1971–1992. Am J Epidemiol. 2012;176(5):409–422. doi:10.1093/aje/kws007
37. Sahile Z, Tezera R, Mariam DH, Collins J, Ali JH. Nutritional status and TB treatment outcomes in Addis Ababa, Ethiopia: an ambi-directional cohort study. PLoS One. 2021;16(3):e0247945. doi:10.1371/journal.pone.0247945
38. Jeon CY, Murray MB. Diabetes mellitus increases the risk of active tuberculosis: a systematic review of 13 observational studies. PLOS Med. 2008;5(7):e152. doi:10.1371/journal.pmed.0050152
39. Pande T, Huddart S, Xavier W, et al. Prevalence of diabetes mellitus amongst hospitalized tuberculosis patients at an Indian tertiary care center: a descriptive analysis. PLoS One. 2018;13(7):e0200838. doi:10.1371/journal.pone.0200838
40. Tocque K, Bellis MA, Beeching NJ, Syed Q, Remmington T, Davies PDO. A case-control study of lifestyle risk factors associated with tuberculosis in Liverpool, North-West England. Eur Respir J. 2001;18(6):959–964. doi:10.1183/09031936.01.00211701
41. Neter JE, Stam BE, Kok FJ, Grobbee DE, Geleijnse JM. Influence of weight reduction on blood pressure. Hypertension. 2003;42(5):878–884. doi:10.1161/01.HYP.0000094221.86888.AE
42. Freckmann G, Schmid C, Baumstark A, Pleus S, Link M, Haug C. System accuracy evaluation of 43 blood glucose monitoring systems for self-monitoring of blood glucose according to DIN EN ISO 15197. J Diabetes Sci Technol. 2012;6(5):1060. doi:10.1177/193229681200600510
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.