Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 18
Visual Ordinal Coronary Artery Calcium Score from Non-Gated Chest CT Predicts Mortality After Severe Chronic Obstructive Pulmonary Disease Exacerbation
Received 27 August 2023
Accepted for publication 15 December 2023
Published 28 December 2023 Volume 2023:18 Pages 3115—3124
DOI https://doi.org/10.2147/COPD.S437401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Prof. Dr. Richard Russell
Huiying Xu,1 Min Sen Yew2
1Department of Respiratory and Critical Care Medicine, Tan Tock Seng Hospital, Singapore, Singapore; 2Department of Cardiology, Tan Tock Seng Hospital, Singapore, Singapore
Correspondence: Huiying Xu, Department of Respiratory and Critical Care Medicine, Tan Tock Seng Hospital, 11 Jln Tan Tock Seng, Singapore, 308433, Singapore, Tel +65 6256 6011, Email [email protected]
Purpose: Chronic obstructive pulmonary disease (COPD) patients often undergo chest CT for various indications. Coronary artery calcium (CAC) can be quantified visually on ungated chest CT using an ordinal score that has been shown to correlate well with traditional Agatston CAC scoring. The prognostic role of CAC was studied mainly in stable COPD patients. We aim to study the association between ordinal CAC and mortality amongst patients admitted for acute exacerbation of COPD (AECOPD).
Patients and Methods: Retrospective study of AECOPD cases with no previous coronary revascularization admitted between 1st January 2016 to 30th June 2017 with a chest CT performed during admission or within 365 days prior. Ordinal CAC scoring (scale of 0– 12) was performed by an experienced CT cardiologist blinded to patient data and outcomes. Patient demographics and future clinical events were retrieved from electronic medical records.
Results: There were 93 patients included (87.1% male, mean age 75 years) with the majority (59.1%) in GOLD Stage III. There were 21 (22.6%) patients with no CAC as well as 39 (41.9%) and 33 (35.5%) with ordinal CAC of 1– 3 and 4– 12, respectively. There were no significant differences in Charlson Comorbidity Index (CCI) and the proportion of patients with traditional cardiovascular risk factors (namely hypertension, dyslipidaemia, diabetes and smoking status) between the ordinal CAC score groups. Over a median follow-up period of 2.9 (1.1– 3.9) years, there were 51 (54.8%) deaths. An ordinal CAC score of 4– 12 was the only significant predictor of mortality after multivariate Cox-regression analysis adjustment for age, gender, body mass index, prior exacerbations, FEV1, cardiovascular risk factors and CCI [HR 3.944, (95% confidence interval 1.647– 9.433, p = 0.002)].
Conclusion: Ordinal CAC measured from a current or recent ungated chest CT is an independent predictor of all-cause mortality in admitted AECOPD patients with no previous coronary revascularization.
Keywords: chronic obstructive pulmonary disease, exacerbation, coronary artery calcium, mortality
Introduction
Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is associated with increased short and longer term all-cause mortality, with almost 50% of patients dying within 4 years.1 The presence of coronary artery disease (CAD) has been shown in several studies to be an important independent predictor of mortality after AECOPD.2,3 Of note, patients with severe AECOPD are at high increased risk of cardiac events, particularly within the initial 30 days after the exacerbation.4 As both COPD and CAD share similar pathophysiological determinants such as cigarette smoking and systemic inflammation, it is unsurprising that COPD is independently associated with underlying subclinical CAD.5 Chest CTs are frequently performed in COPD patients for various indications such as airway evaluation, infections or suspected pulmonary embolism,6 giving rise to opportunities to diagnose subclinical CAD by the detection of coronary artery calcium (CAC). Formal quantitative measurement of CAC using the Agatston score, which is a sum of the attenuation (in Hounsfield units) and area of all CAC lesions in the coronary arteries assessed using a non-contrast gated cardiac CT, is strongly associated with the risk of incident major adverse cardiac events.7 Given the wealth of data supporting the prognostic utility of CAC measurement, the 2016 Society of Cardiovascular Computed Tomography (SCCT) and the Society of Thoracic Radiology guidelines assigned a class I recommendation for routine qualitative CAC assessment on non-gated thoracic scans regardless of the indication.8 One of the CAC scoring methods proposed in the guideline is known as ordinal scoring and involves visually grading the severity of CAC in the left main, left anterior descending, left circumflex, and right coronary arteries as absent, mild, moderate, or severe which are then scored as 0, 1, 2, or 3, respectively.8 We aim to assess the relationship of the ordinal CAC score and subsequent mortality in patients admitted for an AECOPD.
Materials and Methods
Patient Population
We performed a retrospective data analysis of all patients discharged with a primary diagnosis of AECOPD in our institution between 1st January 2016 to 30th June 2017, who had at least one chest CT performed either during the index admission or within 365 days before admission. All patients must have a prior diagnosis of COPD fulfilling the Global Initiatives for Chronic Obstructive Lung Disease (GOLD) spirometric criteria.9 Patients with known coronary revascularization and/or previous myocardial infarction were excluded. This study was conducted in accordance with the principles of the Declaration of Helsinki. Ethical approval, including a waiver of need for written informed consent, was obtained from the Domain Specific Review Board (DSRB) of the National Healthcare Group (IRB 2018/00237), the cluster for which our institution is a member hospital of. The data accessed complied with all relevant data protection and privacy regulations.
Clinical Variables and Ordinal CAC Scoring
Patient data, including baseline characteristics such as age, gender, GOLD staging for COPD severity, smoking status, comorbidities (specifically diabetes mellitus, hypertension, and hyperlipidemia) and subsequent mortality were retrieved from electronic medical records. Chest CT images were retrieved from the hospital’s Picture Archiving and Communication System (PACS). The CT performed closest to the time of admission was used if there was more than one performed within 365 days. A single experienced CT cardiologist with Certification Board of Cardiovascular Computed Tomography (CBCCT) qualification, blinded to patient data, read all the CT images and performed ordinal CAC scoring in accordance with guidelines.8 In brief, the presence of CAC in the left main, left anterior descending, left circumflex, and right coronary arteries was categorized as absent, mild, moderate, or severe and scored as 0, 1, 2, or 3, respectively. CAC was classified as mild if less than 1/3 of the length of the entire artery contained calcification (CAC = 1), moderate if 1/3-2/3 (CAC = 2) and severe if more than 2/3 of the artery showed calcification (CAC = 3). The final score was the sum of the individual artery scores, ranging from 0 to 12, and were divided into 3 categories of increasing severity: 0, 1–3, and 4–12.8
Statistical Analysis
Data were stratified according to 3 ordinal CAC categories. All continuous variables were reported as mean with standard deviation (SD) and compared using ANOVA. All categorical variables were expressed as numbers with percentages and were compared using chi-squared test. Cox regression modelling was used for univariate and multivariate analysis of the various demographic and clinical parameters against survival. All factors with a P-value of <0.05 following a univariate analysis, as well as traditional risk factors for mortality, were included in the multivariate analysis. Hazard ratios (HRs) were calculated with their 95% CIs. All tests were two sided with a 0.05 significance level. Statistical analysis was performed with the SPSS Statistics software (SPSS 26, SPSS Inc, Chicago, IL, USA) where P <0.05 was considered significant.
Results
Participants and Baseline characteristics
A total of 93 patients were included in this study (Figure 1). The baseline characteristics, COPD severity and comorbidities stratified by ordinal CAC score are shown in Table 1. The included patients were predominantly male (87.1%) with a mean age of 75 years. The majority (59.1%) were in GOLD Stage III. There were no significant differences in Charlson Comorbidity Index or the proportion of patients with traditional cardiovascular risk factors (namely hypertension, dyslipidaemia, diabetes and smoking status) between the ordinal CAC score groups. There was no significant difference in the GOLD stage between groups. However, the predicted Forced Expiratory Volume in 1 s [FEV1 (%)] was significantly different between groups, with the highest FEV1 seen in the group with highest CAC.
 |
Table 1 Comparison of Clinical Variables in AECOPD Patients by Ordinal CAC Score |
 |
Figure 1 Patient selection flowchart. |
Chest CT and Ordinal CAC Score
The chest CTs used for ordinal CAC scoring were performed at a mean of 93 days prior to AECOPD admission. The majority (41.9%) of patients had an ordinal CAC between 1 and 3, with 33 (35.4%) having an ordinal CAC of 4–12.
Predictors of Mortality
Over a median follow-up period of 2.9 (1.1–3.9) years, there were 51 (54.8%) deaths. The most common causes of death were related to respiratory followed by cardiac causes (23.7 and 22.6%, respectively). On univariate analysis, ordinal CAC score of 4–12, hypertension and FEV1% were predictors of all-cause mortality. After multivariate Cox-regression analysis with adjustment for age, gender, body mass index (BMI), prior exacerbation history, FEV1, cardiovascular risk factors and Charlsons comorbidity index, an ordinal CAC score of 4–12 was found to be the only significant predictor of mortality [HR 3.944, (95% confidence interval 1.647–9.433, p = 0.002)] (Table 2). Figure 2 shows the Kaplan–Meier plot categorized by ordinal CAC score.
 |
Table 2 Predictors of All-Cause Mortality After AECOPD Hospitalization |
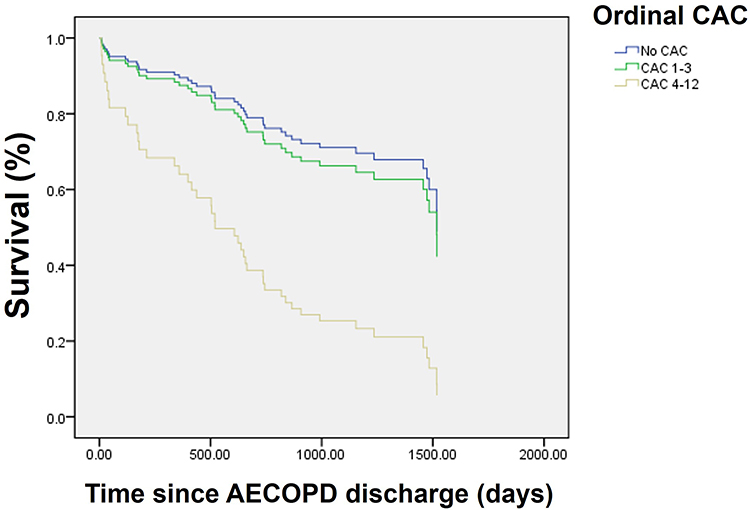 |
Figure 2 Kaplan–Meier curve for survival after acute exacerbation of COPD, stratified by ordinal calcium artery score categories. |
Discussion
In this study of admitted AECOPD patients with a non-gated chest CT performed either during admission or within the preceding 365 days, ordinal CAC scoring was a significant predictor of all-cause mortality independent of age, gender, COPD severity, lung function and traditional cardiovascular risk factors.
CAC is traditionally measured using the Agatston score, which requires a non-enhanced ECG-synchronized cardiac CT to be performed according to a fixed protocol and scanner settings.10 Data from many large studies, such as the Multi-Ethnic Study of Atherosclerosis (MESA), support the utility of Agatston CAC score for prognostication of future adverse cardiac events and guiding primary prevention pharmacotherapy.8 In particular, the MESA study showed that the risk of coronary event was increased almost 10 fold among participants with Agatston scores above 300 when compared to those with no coronary calcium.11 As such, the SCCT guidelines state that an Agatston CAC above 300 is associated with moderate to severely increased cardiovascular risk and recommends initiation of high-intensity statin and aspirin in these patients.12
Despite its utility, the cardiac CT used for the Agatston score must be ECG-gated, performed according to fixed protocol and requires dedicated software for interpretation. More recently, it has been shown that visual ordinal CAC scoring of non-gated chest CTs correlate well with formal Agatston scoring using ECG-gated CTs.13 A study of 222 patients with both ECG-gated and non-gated chest CT performed on the same day showed strong correlation between the non-gated ordinal and ECG gated Agatston scores.13 Of note, this study demonstrated that an ordinal CAC score of 4–5 corresponded to an average Agatston score of 350.6 (264.9–436.3).13 In other words, an ordinal CAC of at least 4 likely identifies patients at moderate-to-severe increase in cardiovascular risk, similar to that seen with an Agatston score of at least 300. The utility of ordinal CAC scoring to predict cardiovascular outcomes was mainly assessed in cohorts undergoing low dose thoracic CT for lung cancer screening. An ordinal score of at least 4 was shown to be a significant predictor of cardiovascular death even after adjustment for age, gender and pack-years of smoking.14
Our data showed that more than three-quarters of the included patients have detectable CAC, with more than a third having an ordinal score of at least 4. Indeed, patients with COPD are at risk of CAD due to shared pathophysiological processes such as smoking and systemic inflammation.5 However, amongst smokers with no known CAD recruited from the Danish Lung Cancer Screening Trial, the presence of COPD according to GOLD classification independently predicted CAC level although there was not a dose–response relationship between COPD severity and CAC level.5 Similarly, data from the Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) study showed that COPD patients had higher Agatston CAC than smokers with normal spirometry or non-smokers, despite correction for age, gender, ethnicity and pack-year smoking history.15 Of note, it has been shown that only lung hyperinflation and not FEV1 or emphysema severity had an association with CAC.16 The authors hypothesized the mechanism may be related to increased left ventricular mass from lung hyperinflation causing downstream coronary inflammation, atherosclerotic vascular injury and systemic endothelial dysfunction.16 Collectively, these data indicate a preponderance for CAC amongst COPD patients that may be due to mechanisms beyond cardiovascular risk factors and smoking alone.
Having established that CAC is common amongst COPD patients, it is therefore important to review the impact of CAC on prognosis. Studies assessing the implications of CAC in COPD patients were mainly limited to stable COPD. In terms of cardiac risk, visual estimation of CAC on baseline CT scans in the Genetic Epidemiology of COPD (COPDGene) patient cohort was associated with time to first acute coronary event, after adjustment for standard risk factors and COPD severity.17 In a study of stable COPD patients in an outpatient pulmonary clinic, ordinal CAC score was the best predictor of future cardiovascular events.18 Of note, the FEV1 was not different between groups with or without a subsequent cardiac event.18 Apart from cardiac events, CAC is also predictive of mortality in general. A higher Agatston CAC is associated with adverse functional capacity and increased mortality in patients from ECLIPSE.15 Amongst stable COPD patients undergoing non-contrast chest CT, an ordinal CAC greater than 4 was also associated with a hazard ratio of 2.03 for all-cause mortality.19
The prognosis after an AECOPD episode is poor with a mean life expectancy of 3.4 to 9.7 years depending on GOLD stage.20 Many studies have been performed to identify risk factors for mortality after AECOPD. A large systematic review and meta-analysis identified clinically known CAD as one of the factors significantly associated with long-term mortality after AECOPD hospitalization, with the other factors being age, low BMI, cardiac failure, diabetes mellitus, malignancy and indices of COPD severity.2 In our study, we have demonstrated that the presence of subclinical coronary atherosclerosis quantified by the ordinal CAC score is independently associated with all-cause mortality after AECOPD hospitalization, even in patients without overt clinical CAD. This is of great clinical and practical importance. The AECOPD hospitalization is a golden opportunity for the physician to review any chest CTs performed within the year not only for respiratory pathology but also for the severity of CAC which can prognosticate the patient for risk of subsequent death. Moreover, we showed that CAC was related to not only cardiac death but all-cause death including respiratory and malignant causes. This is not a surprising finding. Data from the MESA study showed that individuals with an Agatston CAC above 400 had an increased hazard ratio for cancer and COPD.21 This does not necessarily indicate a causal relationship between CAC and these diseases. Instead, it is hypothesized that CAC is a risk integrator that reflects the aggregated lifetime exposure to both measured and unmeasured risk factors that are common between CAD, COPD as well as cancer.21 Systemic inflammation is possibly an important underlying mechanism. For example, bronchial inflammation in COPD, through the activation of transforming growth factor-β as well as the receptor tyrosine kinase/RaS pathway, promotes a carcinogenic process known as epithelial-to-mesenchymal transition.22 CAC may also be an indirect marker of poor prognosis independent of its coronary implications. The Muscle Health Study, an ancillary study of the COPDGene cohort, showed that COPD patients with elevated CAC exhibit greater perceptions of difficulty when performing daily physical activities.23 In turn, physical activity level is itself a robust predictor of all-cause mortality in patients with COPD.24 To summarize, CAC is associated with mortality in COPD patients not only due to a direct link to cardiac events but also through its association with systemic inflammation, cancer and even physical inactivity.
We observed that close to 50% of patients in our cohort with an ordinal CAC of at least 4 were not on any statin at the time of the AECOPD admission. There is currently a large body of evidence for statin initiation and intensification to reduce cardiac events in patients with elevated CAC, particularly in those with Agatston score of at least 300–400.25 This suggests that we have missed the opportunity to improve the cardiovascular outcome for a significant proportion of AECOPD inpatients if their CAC was overlooked or not quantified from an existing chest CT. The data for statins and non-cardiac mortality, specifically in COPD patients, are more limited. In the Rosuvastatin treatment in stable COPD (RODEO) randomized trial, rosuvastatin treatment significantly reduced systemic inflammation as quantified by high-sensitivity C-reactive protein (hsCRP) and improved endothelial-dependent vascular function.26 Given that CRP level is not only significantly associated with mortality in COPD patients but also in other related co-morbidities such as cardiovascular disease and cancer,27 it is possible that physicians may be able to reduce both cardiac and non-cardiac mortality by identifying COPD patients with elevated CAC for statin use.
There are several limitations in our study. This is a single-center study in an Asian population with results that may not be generalizable to other patient groups. The number of included patients is small due to a stringent inclusion criterion that required the CT to be performed during or within 365 days before the admission. Increasing the duration between the CT scan and AECOPD admission would have resulted in more included cases. However, as there are insufficient data on CAC progression in COPD patients, we decided to use a more conservative time frame of 365 days, although studies in healthy individuals with an initial 0 Agatston CAC showed that CAC progressed (to non 0) in only 0.3% and 1.9% of the cases over 1 and 2 years, respectively.28 Given that the ordinal CAC scale is less sensitive to small CAC changes as compared to the Agatston score, we can be confident that the ordinal CAC seen in the scan performed within 365 days would still be reflective of the patient’s clinical status at the time of the AECOPD admission. All the ordinal CACs in the study were assessed by a single cardiologist experienced in cardiac CT, and similar results may not be reproducible when scans are interpreted by a non-expert reader. Inter-observer variability was not evaluated in our study, although prior studies generally showed good to high inter-reader agreement amongst radiologists performing visual CAC assessment.29 There are also inherent technical challenges with quantification of CAC on general ungated chest CTs. For example, heart rate differences, variable slice thickness and scanner parameters can affect visual CAC assessment.13 However, the study design was not aimed at obtaining precise quantification of CAC but rather to reflect the “real-world” situation where physicians only have an existing non-dedicated CT performed for a non-cardiac indication.
Conclusion
In summary, the majority of admitted AECOPD patients with no known coronary revascularization and a current or recently performed chest CT have detectable CAC, with more than a third having severe CAC as defined by an ordinal CAC of at least 4. A significant proportion of these patients did not receive adequate primary preventive therapy such as statins, reflecting the missed opportunities for treatment optimization had the CAC been identified. The presence of severe CAC remains an independent predictor for all-cause mortality even after adjustment for patient demographics, traditional cardiovascular risk factors and COPD severity. We hope that the results of this study can motivate physicians to actively review COPD patients’ previous chest CTs for evidence of CAC. Further studies are required to assess if early intervention in these higher risk patients can affect future outcomes.
Abbreviations
AECOPD, Acute Exacerbation of Chronic Obstructive Pulmonary Disease; BMI, Body Mass Index; CAC, Coronary Artery Calcium; CAD, Coronary Artery Disease; CBCCT, Certification Board of Cardiovascular Computed Tomography; CI, Confidence interval; COPDGene, Genetic Epidemiology of COPD; DSRB, Domain Specific Review Board; ECLIPSE, Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints; GOLD, Global Initiatives for Chronic Obstructive Lung Disease; HR, Hazard Ratio; HSCRP, High-sensitivity C reactive protein; MESA, Multi-Ethnic Study of Atherosclerosis; PACS, Picture Archiving and Communication System; RODEO, Rosuvastatin treatment in stable COPD; SCCT, Society of Cardiovascular Computed Tomography; SD, Standard deviation.
Data Sharing Statement
The data analyzed are available upon reasonable request to the corresponding author (Dr H Xu).
Acknowledgments
The authors would like to acknowledge the support from the Department of Respiratory and Critical Care Medicine, Tan Tock Seng Hospital, for data collection in this study.
Funding
The authors did not receive funding for this study.
Disclosure
The authors do not have any relevant conflict of interests to declare.
References
1. Suissa S, Dell’Aniello S, Ernst P. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67(11):957–963. doi:10.1136/thoraxjnl-2011-201518
2. Singanayagam A, Schembri S, Chalmers JD. Predictors of mortality in hospitalized adults with acute exacerbation of chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2013;10(2):81–89. doi:10.1513/AnnalsATS.201208-043OC
3. Esteban C, Castro-Acosta A, Alvarez-Martínez CJ, Capelastegui A, López-Campos JL, Pozo-Rodriguez F. Predictors of one-year mortality after hospitalization for an exacerbation of COPD. BMC Pulm Med. 2018;18(1):18. doi:10.1186/s12890-018-0574-z
4. Løkke A, Lange P, Ibsen R, Telg G, Lykkegaard J, Hilberg O. Association of COPD exacerbations with cardiovascular events – a population-based cohort study. Eur Respir J. 2022;60(suppl 66). doi:10.1183/13993003.congress-2022.4337
5. Rasmussen T, Køber L, Pedersen JH, et al. Relationship between chronic obstructive pulmonary disease and subclinical coronary artery disease in long-term smokers. Eur Heart J Cardiovasc Imaging. 2013;14(12):1159–1166. doi:10.1093/ehjci/jet057
6. Ezponda A, Casanova C, Divo M, et al. Chest CT-assessed comorbidities and all-cause mortality risk in COPD patients in the BODE cohort. Respirology. 2022;27(4):286–293. doi:10.1111/resp.14223
7. Obisesan OH, Osei AD, Uddin SMI, Dzaye O, Blaha MJ. An update on coronary artery calcium interpretation at chest and cardiac CT. Radiology. 2021;3(1):e200484. doi:10.1148/ryct.2021200484
8. Hecht HS, Cronin P, Blaha MJ, et al. 2016 SCCT/STR guidelines for coronary artery calcium scoring of noncontrast noncardiac chest CT scans: a report of the society of cardiovascular computed tomography and society of thoracic radiology. J Cardiovasc Comput Tomogr. 2017;11(1):74–84. doi:10.1016/j.jcct.2016.11.003
9. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 Report. GOLD executive summary. Am J Respir Crit Care Med. 2017;195(5):557–582. doi:10.1164/rccm.201701-0218PP
10. Abbara S, Blanke P, Maroules CD, et al. SCCT guidelines for the performance and acquisition of coronary computed tomographic angiography: a report of the society of cardiovascular computed tomography guidelines committee: endorsed by the North American Society for Cardiovascular Imaging (NASCI). J Cardiovasc Comput Tomogr. 2016;10(6):435–449. doi:10.1016/j.jcct.2016.10.002
11. Detrano R, Guerci AD, Carr JJ, et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. 2008;358(13):1336–1345. doi:10.1056/NEJMoa072100
12. Hecht HS, Blaha MJ, Kazerooni EA, et al. CAC-DRS: coronary artery calcium data and reporting system. An expert consensus document of the society of cardiovascular computed tomography (SCCT). J Cardiovasc Comput Tomogr. 2018;12(3):185–191. doi:10.1016/j.jcct.2018.03.008
13. Azour L, Kadoch MA, Ward TJ, Eber CD, Jacobi AH. Estimation of cardiovascular risk on routine chest CT: ordinal coronary artery calcium scoring as an accurate predictor of Agatston score ranges. J Cardiovasc Comput Tomogr. 2017;11(1):8–15. doi:10.1016/j.jcct.2016.10.001
14. Shemesh J, Henschke CI, Shaham D, et al. Ordinal scoring of coronary artery calcifications on low-dose CT scans of the chest is predictive of death from cardiovascular disease. Radiology. 2010;257(2):541–548. doi:10.1148/radiol.10100383
15. Williams MC, Murchison JT, Edwards LD, et al. Coronary artery calcification is increased in patients with COPD and associated with increased morbidity and mortality. Thorax. 2014;69(8):718–723. doi:10.1136/thoraxjnl-2012-203151
16. Chandra D, Gupta A, Kinney GL, et al. The association between lung hyperinflation and coronary artery disease in smokers. Chest. 2021;160(3):858–871. doi:10.1016/j.chest.2021.04.066
17. Bhatt SP, Kazerooni EA, Newell JD, et al. Visual estimate of coronary artery calcium predicts cardiovascular disease in COPD. Chest. 2018;154(3):579–587. doi:10.1016/j.chest.2018.05.037
18. Zagaceta J, Bastarrika G, Zulueta JJ, et al. Prospective comparison of non-invasive risk markers of major cardiovascular events in COPD patients. Respir Res. 2017;18(1):175. doi:10.1186/s12931-017-0658-y
19. O’Hare PE, Ayres JF, O’Rourke RL, et al. Coronary artery calcification on computed tomography correlates with mortality in chronic obstructive pulmonary disease. J Comput Assist Tomogr. 2014;38(5):753–759. doi:10.1097/RCT.0000000000000119
20. Hirtum PV, Sprooten RTM, Noord JA, Vliet M, Kruif MD. Long term survival after admission for COPD exacerbation: a comparison with the general population. Respir Med. 2018;137:77–82. doi:10.1016/j.rmed.2018.02.015
21. Handy CE, Desai CS, Dardari ZA, et al. The association of coronary artery calcium with noncardiovascular disease: the multi-ethnic study of atherosclerosis. JACC Cardiovasc Imaging. 2016;9(5):568–576. doi:10.1016/j.jcmg.2015.09.020
22. Cavaillès A, Brinchault-Rabin G, Dixmier A, et al. Comorbidities of COPD. Eur Respir Rev. 2013;22(130):454–475. doi:10.1183/09059180.00008612
23. Tiller NB, Kinninger A, Abbasi A, et al. Physical activity, muscle oxidative capacity, and coronary artery calcium in smokers with and without COPD. Int J Chron Obstruct Pulmon Dis. 2022;17:2811–2820. doi:10.2147/COPD.S385000
24. W B, K A, H O, et al. Physical activity is the strongest predictor of all-cause mortality in patients with COPD: a prospective cohort study. Chest. 2011;140(2). doi:10.1378/chest.10-2521
25. Zhou Z, Ong KL, Breslin M, Allison MA, Curtis AJ, Nelson MR. Association of statin use with cardiovascular outcomes by coronary calcium: mesa. JACC Cardiovasc Imaging. 2020;13(4):1094–1096. doi:10.1016/j.jcmg.2019.11.009
26. Neukamm A, Høiseth AD, Einvik G, et al. Rosuvastatin treatment in stable chronic obstructive pulmonary disease (RODEO): a randomized controlled trial. J Intern Med. 2015;278(1):59–67. doi:10.1111/joim.12337
27. Leuzzi G, Galeone C, Taverna F, Suatoni P, Morelli D, Pastorino U. C-reactive protein level predicts mortality in COPD: a systematic review and meta-analysis. Eur Respir Rev. 2017;26(143):160070. doi:10.1183/16000617.0070-2016
28. Lee W, Yoon YE, Kwon O, et al. Evaluation of coronary artery calcium progression in asymptomatic individuals with an initial score of zero. Korean Circ J. 2019;49(5):448–457. doi:10.4070/kcj.2018.0318
29. Chiles C, Duan F, Gladish GW, et al. Association of coronary artery calcification and mortality in the national lung screening trial: a comparison of three scoring methods. Radiology. 2015;276(1):82–90. doi:10.1148/radiol.15142062
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Treatment Patterns, Socioeconomic Status and Clinical Burden in Mild COPD: A Swedish Real-World, Retrospective Cohort Study, the ARCTIC Study
Larsson K, Lisspers K, Ställberg B, Johansson G, Gutzwiller FS, Mezzi K, Bjerregaard BK, Jorgensen L, Koo H, Janson C
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1409-1421
Published Date: 21 June 2022
Short-Term Oxygen Therapy Outcomes in COPD
Soumagne T, Maltais F, Corbeil F, Paradis B, Baltzan M, Simão P, Abad Fernández A, Lecours R, Bernard S, Lacasse Y
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:1685-1693
Published Date: 28 July 2022
The Association of Renin-Angiotensin System Blockades and Mortality in Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease and Acute Respiratory Failure: A Retrospective Cohort Study
Ruan Z, Li D, Hu Y, Qiu Z, Chen X
International Journal of Chronic Obstructive Pulmonary Disease 2022, 17:2001-2011
Published Date: 1 September 2022
A Prediction Scoring Model for the Effect of Withdrawal or Addition of Inhaled Corticosteroids in Patients with Chronic Obstructive Pulmonary Disease
Lee JH, Kim S, Oh YM
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:113-127
Published Date: 15 February 2023
Effects of Early Pulmonary Rehabilitation on Hospitalized Patients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-Analysis
Lu HY, Chen CF, Lee DL, Tsai YJ, Lin PC
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:881-893
Published Date: 15 May 2023