Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Visceral and Subcutaneous Fat Deposits Exhibit Distinct Roles in the Initiation and Progression of Breast Cancer
Authors Zhang Y, Li Q ![]() , Zhao L, Pang Y, Li L, Niu WW, Xing Y, Liu Y
, Zhao L, Pang Y, Li L, Niu WW, Xing Y, Liu Y ![]() , Zhang FQ, Fan YC, Bao YY, Li CW, Yu K
, Zhang FQ, Fan YC, Bao YY, Li CW, Yu K ![]()
Received 16 September 2025
Accepted for publication 26 January 2026
Published 16 February 2026 Volume 2026:18 565061
DOI https://doi.org/10.2147/BCTT.S565061
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Yu Zhang,1,* Qi Li,2,* Li Zhao,3,* Yi Pang,2 Lin Li,2 Wei-Wei Niu,2 Yu Xing,2 Yu Liu,2 Fu-Quan Zhang,2 Yu-Chen Fan,2 Yuan-Yuan Bao,1 Chun-Wei Li,4 Kang Yu1
1Department of Clinical Nutrition, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China; 2Department of General Surgery, Central Hospital, Tianjin University/Tianjin Third Central Hospital, Tianjin, People’s Republic of China; 3Department of General Surgery, Tianjin Third Central Hospital Branch (Tianjin Institute of Geriatrics), Tianjin, People’s Republic of China; 4Department of Clinical Nutrition, Institute of Clinical Medicine, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Kang Yu, Department of Clinical Nutrition, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences (CAMS) and Peking Union Medical College (PUMC), Beijing, People’s Republic of China, Tel +86-10-69155550, Fax +86-10-65253037, Email [email protected] Chun-Wei Li, Department of Clinical Nutrition, Institute of Clinical Medicine, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences (CAMS) and Peking Union Medical College (PUMC), Beijing, People’s Republic of China, Tel +86-10-69155550, Fax +86-10-65253037, Email [email protected]
Purpose: Evidence suggests that ectopic fat deposition and muscle atrophy may contribute to tumor development and progression; however, their dual roles in breast cancer (BC) remain incompletely understood. This study aims to elucidate the complex relationships between specific body composition features and both BC initiation and progression.
Patients and methods: A multicenter observational study was conducted from March 2020 to May 2025, integrating case-control and longitudinal data on body composition parameters, covariates, and survival outcomes from 213 BC patients and 430 cancer-free controls. The case-control analysis employed inverse probability weighting, lasso and logistic regression to evaluate associations between body composition and BC risk. The XGBoost model was used to further identify key body composition predictors. Kaplan-Meier and Cox regression analyses were conducted to evaluate the effect of body composition parameters on distant metastasis-free survival (DMFS) in BC patients following radical mastectomy.
Results: Trunk muscle mass (TMM) exerted a protective effect against BC development (OR=0.965, 95% CI: 0.949~0.982), whereas muscle mass (MM: OR=1.027, 95% CI: 1.008~1.047) trunk fat mass (TFM: OR=1.046, 95% CI: 1.025~1.068) and visceral adipose tissue (VAT: OR=1.003, 95%: 1.0005~1.005) emerged as independent risk factors, even after adjusting for menopause status, comorbidities, laboratory indices, and lifestyle factors. The XGBoost model corroborated TFM, VAT, and TMM as pivotal predictors of carcinogenesis. Paradoxically, in post-mastectomy BC patients, higher subcutaneous adipose tissue compartments, specifically TFM (HR= 0.794, 95% CI: 0.634~0.994) was significantly correlated with improved DMFS, particularly among postmenopausal women (HR=0.721, 95% CI: 0.530~0.981), while VAT showed no significant impact on survival. Higher LMM was also associated with improved DMFS in postmenopausal women.
Conclusion: This study reveals a paradoxical role of adipose tissue in breast cancer, as it may promote tumorigenesis yet confer a post-mastectomy survival advantage. Body composition’s prognostic complexity necessitates targeted therapies targeting fat-muscle crosstalk in cancer management.
Keywords: breast carcinogenesis, fat distribution, risk factor, distant metastasis-free survival
Introduction
Breast cancer (BC) is the most commonly diagnosed malignancy and the fifth leading cause of cancer death worldwide.1 Notably, breast cancer (postmenopausal) has been specifically identified as an obesity-related cancer, with the International Agency for Research on Cancer working group concluding that avoiding weight gain has a cancer-preventive effect for this malignancy.2 Obesity is associated with unfavorable cancer outcomes, with epidemiological data indicating a U-shaped quadratic association between Body Mass Index (BMI) and cancer risk.3 The mechanisms linking obesity to tumors are debated, but evidence indicates that low muscle mass and ectopic deposition of body fat are associated with tumor development and progression.4
Emerging evidence highlights the critical role of adipose distribution, particularly trunk and visceral fat accumulation, in breast cancer pathogenesis and prognosis.5,6 Adipose tissue functions as an active endocrine organ, especially in postmenopausal women, producing hormones and pro-inflammatory cytokines leading to systemic inflammation, oxidative stress, and insulin resistance.7 Visceral adipose tissue (VAT) is metabolically distinct and more active than subcutaneous adipose tissue (SAT), extending beyond energy storage to complex endocrine roles.8 In postmenopausal women, obesity leads to an increased androgen-to-estrogen conversion, promoting cell proliferation and inhibiting cell apoptosis.9 Adipose tissue further drives breast cancer risk by secreting adipokines, leptin reprograms fatty acid metabolism to fuel tumor growth,10 while low adiponectin levels (especially correlated with visceral fat) cause insulin growth factors dysregulation, chronic inflammation, and sex hormone imbalance, promoting malignancy.11 Additionally, VAT is associated with oxidative stress, inflammation, insulin resistance, hyperinsulinemia, and dyslipidemia, all of which are risk factors for cancer, including breast cancer.12–15 Research also indicates that decreased visceral fat correlates with improved levels of circulating and breast biopsy biomarkers associated with inflammation, thus reducing breast cancer risk.16,17
Besides its significant impact on breast cancer development, obesity also serves as a critical modifiable prognostic factor influencing survival outcomes. Research has shown that adiposity elevates overall mortality, however, BMI alone proves inadequate for risk stratification as it fails to capture ectopic fat deposition and other aspects of body composition.7,10,18 Research conflicts persist regarding the prognostic value of visceral and subcutaneous fat, with studies reporting either negative, protective, or neutral effects on survival.13–15,17,19 These conflicting results largely reflect the current insufficient understanding of the molecular mechanisms underlying VAT-specific (compared to SAT) metabolic and immunoinflammatory profiles,20,21 its unique secretory factor profile,22 and how these factors specifically influence malignant biological behaviors of cancer cells, such as proliferation, invasion, and migration, as well as shape an immunosuppressive tumor microenvironment. Furthermore, methodological heterogeneity across studies, including inconsistent measurement protocols, heterogeneous population characteristics, and the lack of standardized cutoff values, further compounds the inconsistency in conclusions.
Similar to adipose tissue, skeletal muscle exhibits metabolic activity and the two engage in close interaction. In contrast to the elusive role of fat in breast cancer risk, muscle was recognized as a protective factor against the disease.23 The toxicities of anti-cancer treatments, along with hormonal and lifestyle changes in BC patients, can worsen body composition phenotype,24 which results in muscle atrophy, also known as sarcopenia. In turn, these mutual changes triggered chemotherapy and radiation-related toxicities and postoperative complications in cancer patients, even tumor progression and mortality.25 Furthermore, muscle atrophy is associated with systemic inflammation and altered immune responses, which can contribute to tumor progression and metastasis.23 The metabolic crosstalk between muscle and adipose tissue, exemplified by the modulation of insulin sensitivity and systemic metabolic homeostasis, together with its potential role in shaping the tumor microenvironment, has been receiving increasing attention.26
Although numerous studies have investigated the association between body composition and breast cancer development and progression, conclusive evidence has not been established. This study aims to comprehensively evaluate the effects of both adipose and muscle tissue distribution patterns on breast cancer risk and prognostic outcomes within the same population cohort, employing standardized measurement protocols to ensure methodological consistency.
Methods
Participants
This is a multi-center, retrospective and longitudinal, observational study organized by Peking Union Medical College Hospital (PUMCH) multicenter Prospective Longitudinal Sarcopenia study (PPLSS), approved by the Ethic Committee (No. HS889). This ongoing interdisciplinary cohort and cross-sectional study on the management of sarcopenic and sarcopenic obesity was established in 2015 to evaluate changes in muscle mass, muscle strength, fat mass, fat distribution, and clinical outcomes among older adults in China with these conditions. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.
Patients with breast cancer were recruited, with written permission, at the General Surgery Unit of Central Hospital, Tianjin University (CHTU, Tianjin, China) from March 2020 to May 2025 from the Central Hospital, Tianjin University Retrospective Longitudinal Obesity-related Metabolic Tumor Study (TRLOMTS), part of the PPLSS. This part of PPLSS aims to assess changes in body composition and clinical outcomes in patients with obesity-related tumors. The TPLOCMS protocol was approved by the Human Ethics Committee of the CHTU (No. IRB2021-037-02). Healthy controls were recruited, with written permission, from the PPLSS cohort and selected based on the inclusive and exclusive criteria.
The case-control study enrolled untreated, pathologically confirmed primary female breast cancer patients (≥18 years) as cases, and cancer-free individuals as controls. All participants completed bioelectrical impedance analysis (BIA), clinical examinations, and lifestyle questionnaires within one month pre-enrollment. Exclusion criteria included severe cardiorenal/hepatic diseases, communicable diseases, cognitive impairment, body composition interference factors (such as pacemakers, edema), and incomplete data. For the cohort study, breast cancer patients meeting the above criteria were further excluded if they: (1) did not undergo radical mastectomy; (2) had incomplete clinical treatment/postoperative complication records; (3) demonstrated poor compliance during follow-up. All participants underwent an ethical review and provided written informed consent. Six hundred and forty-three participants were enrolled based on the inclusive and exclusive criteria, comprising 213 subjects with breast cancer and 430 control subjects with non-breast disease women (healthy control) or benign breast nodules (Figure 1).
 |
Figure 1 The flowchart of patient recruitment. Flowchart detailing inclusion and exclusion criteria for participants enrolled in the study. |
All patients presenting to the General Surgery Unit of CHTU were asked to provide written informed consent for body composition analysis, questionnaire administration, and clinical specimen collection. From this population with written permission, breast cancer patients who met the inclusion and exclusion criteria were identified and enrolled as cases. Likewise, healthy female and benign breast nodules patients were included as controls from the two centers who provided the same informed consent before undergoing the procedures. Trained research staff explained the study and the voluntary nature of participation. Those who agreed signed a written informed consent form permitting the anonymized use of their data for research.
Body Composition Analysis
The H-Key 350 body composition analyzer (Beijing Sihai Huachen Science and Technology Co., Ltd. Beijing, China) was used to measure body composition parameters including body weight (kg), fat percentage (FP, %), fat mass (FM, kg), fat free mass (FFM, kg), muscle mass (MM, kg), limb muscle mass (LMM, kg), trunk muscle mass (TMM, kg), limb fat mass (LFM, kg), trunk fat mass (TFM, kg), and visceral adipose tissue (VAT, cm2). Before testing, participants were instructed to abstain from alcohol, caffeine, and vigorous exercise for 24 hours. Standardized pre-measurement protocols included bladder emptying, avoidance of excessive fluid intake, and confirmation of device calibration and functionality. Skin contact sites were cleaned, dried, and freed from metal accessories. Participants stood barefoot on the analyzer with parallel feet, firmly gripping the hand electrodes, and maintained a stationary position for 2 minutes during data acquisition. Height (cm) was measured once, and BMI was calculated as body weight/body height2 (kg/m2).
Assessment of Covariates
The case-control study assessed data including age, menopausal status, marital status, exercise, smoking, drinking habits, and comorbidities, collected through a designed questionnaire. Blood biochemical parameters, including homeostasis model assessment of insulin resistance (HOMA-IR), triglyceride (TG), total cholesterol (TC), high-density lipoprotein (HDL), low-density lipoprotein (LDL), free fatty acid (FFA), low-density lipoprotein to high-density lipoprotein ratio (LHR), albumin, and neutrophil-to-lymphocyte ratio (NLR), were derived from laboratory test. The cohort study further analyzed tumor characteristics and treatment details extracted from medical records, including tumor long diameter, pathological type, TNM stage, metastatic sites (bone, liver, lung, brain, others), HER2 status, estrogen receptor (ER) status, progesterone receptor (PR) status, and molecular subtype. Data were collected from the date of diagnosis until the last follow-up or death. Tumor markers, like carcinoembryonic antigen (CEA), carbohydrate antigen, were derived from laboratory tests. All tumors were confirmed histologically and staged according to the conventional American Joint Committee on Cancer (AJCC) TNM Classification (8th edition). Distant metastasis-free survival (DMFS) was assessed as the postoperative outcome. Distant metastasis was defined as pathological, radiological, or endoscopic evidence of malignancy after curative surgery in distant fields or organs. The date of distant metastasis was determined according to the medical record or telephone follow-up. For patients without distant metastasis, censoring occurred at the last follow‐up date registered in the medical record.
Statistical Analysis
We conducted both an inverse probability weighted (IPW) case-control study and a prospective cohort study in patients with breast cancer. First, the IPW case-control study assessed the potential role of body composition parameters, measured via BIA, as risk factors for breast cancer. Subsequently, a cohort of patients who underwent radical mastectomy for breast cancer was selected and followed to evaluate the impact of these parameters on clinical outcomes: overall survival, metastasis, and relapse.
The IPW, implemented using the R package “ipw” (R 4.4.1), was applied to balance the baseline characteristics between the treatment and control groups. Weights were derived from a logistic regression model in which breast cancer status served as the dependent variable, adjusted for potential confounders including age, menopausal status, marital status, physical exercise, smoking and drinking habits, comorbidities, and blood biochemical parameters. These variables were selected based on clinical knowledge of the factors that might affect breast cancer risk and were essential for ensuring comparability in body composition between the case and control groups. The weighted standardized mean difference was computed for all baseline characteristics to evaluate intergroup balance after weighting. A standardized mean difference below 0.2 was considered indicative of adequate balance between the groups.27
Data analysis was conducted using R 4.4.1. Continuous data were reported as median (Interquartile Range) or mean ± SD based on the Shapiro–Wilk test, while categorical data appeared as counts and percentages. Group comparisons were performed using the Mann–Whitney U-test or independent-samples t test for continuous variables and the Chi-square or Fisher’s exact test for categorical variables. Variance inflation factor (≥10) was used to eliminate multicollinearity before analysis. Univariate analysis of risk factors was conducted using a univariate logistic regression model. For the multivariable assessment, predictor selection was performed with Lasso regression, and the variables retained were subsequently entered into a multivariable logistic regression to estimate their associations with BC. Because visceral adipose tissue (VAT) and total fat mass (TFM) were highly correlated, we generated two alternative datasets for Lasso modelling: one excluding VAT (Model 2) and the other excluding TFM (Model 3), in order to compare their respective contributions. Lasso models were fitted using the lambda.min criterion, while the more conservative lambda.1se criterion was applied in a sensitivity analysis to enhance the robustness and interpretability of the selected predictors (Supplementary Figure 1). We used an XGBoost model to determine the feature importance scores of body composition parameters, thereby identifying key factors contributing to breast cancer risk. The study population (n=643) was divided into a training group (70%) and a test group (30%). During model training, 10-fold cross-validation was employed. The performance of model was then evaluated using the area under the receiver operating characteristic (ROC) curve (area under the curve, AUC). Kaplan-Meier analysis, along with the Log rank test, was used to assess the prognostic value of body composition phenotypes for distant metastasis-free survival (DMFS) in the breast cancer cohort. The cutoff values for LFM, TFM, and VAT were determined using X-tile (3.6.1) based on DMFS. Univariate Cox regression was used to assess the associations between all body composition parameters and DMFS in the entire cohort and in the subgroup of postmenopausal patients, followed by a multivariable model adjusting for potential confounders. We checked the proportional hazards assumption using the Schoenfeld residuals. Given that follow-up time varied among patients, a sensitivity analysis was performed by restricting the follow-up period to a minimum of 2 years for all patients. Differences were considered significant at p < 0.05.
Sample size calculations were performed using PASS 15. For the case-control arm, we calculated that 206 participants (137 cases and 69 controls) were needed to detect an OR of 3.3 for breast cancer28 associated with abdominal obesity (54.4% prevalence).29 Cohort-arm calculations assumed a baseline 5‑year disease‑free survival of 63.6% and calculated required sample sizes of 180 (HR = 2.16 for low VAT)15 and 108 (HR = 2.67 for high waist–hip ratio).30 All calculations were conducted with 90% power, a 5% significance level (two-sided), and 20% dropout rate.
Results
Baseline Characteristic
Patients with breast cancer were older (65 yr vs 57 yr, P<0.001), and had a higher prevalence of hypertension, insulin resistance, dyslipidemia, liver dysfunction, and renal dysfunction compared to controls (P<0.05) After IPW adjustment, all baseline covariates met thresholds of SMD of 0.2 or less, indicating that between-group differences in covariates were eliminated and that differences in outcomes stemmed from different body composition phenotype (Table 1).
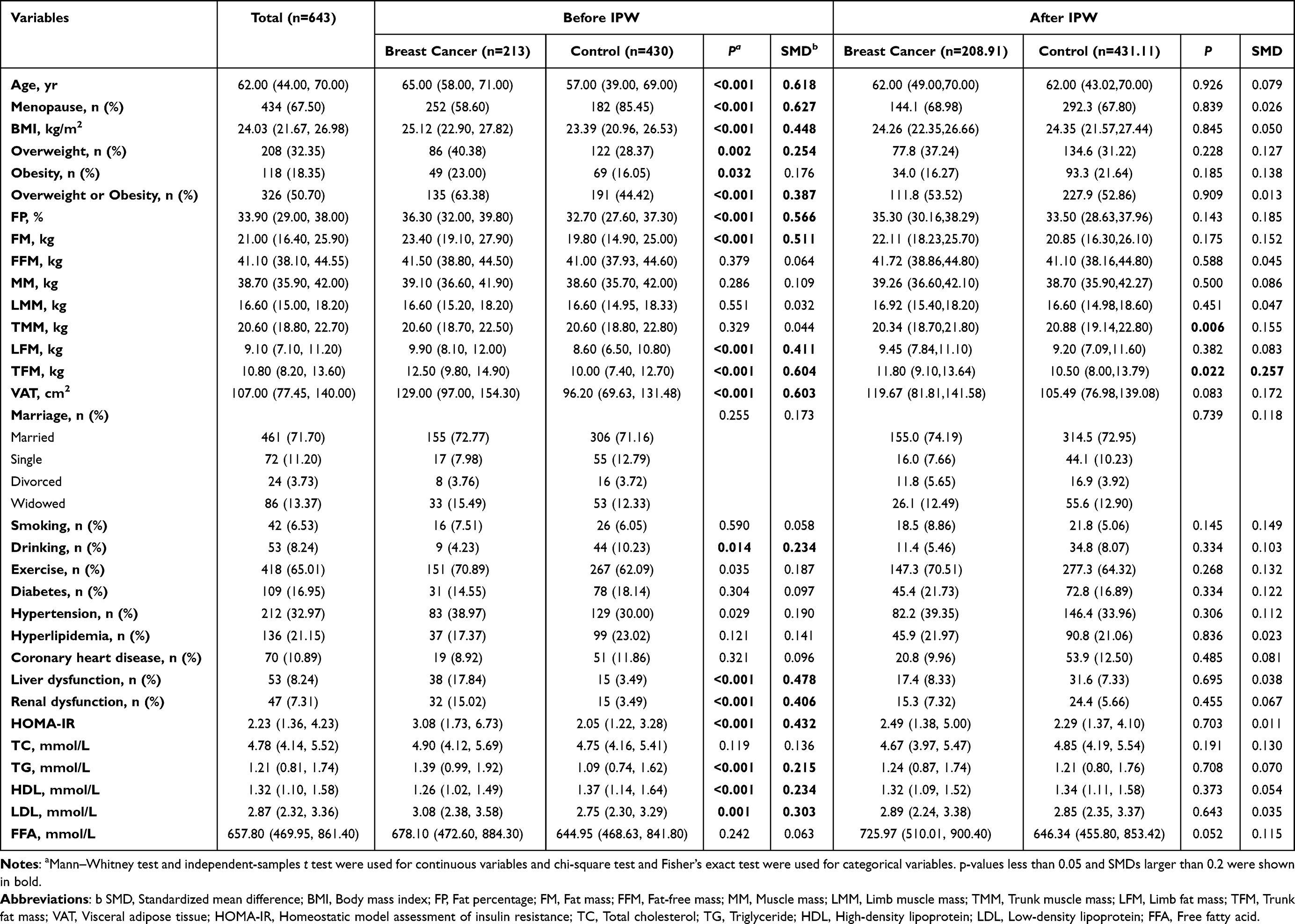 |
Table 1 Baseline Characteristic of Participants Before and After Inverse Probability Weighting (IPW) |
Body composition analysis showed that BC patients had significantly higher values across multiple metrics, all indicative of elevated rates of overweight and obesity. These included BMI (25.12 [22.90, 27.82] kg/m2 vs 23.39 [20.96, 26.53] kg/m2, P<0.001), FP (36.30 [32.00, 39.80] % vs 32.70 [27.60, 37.30] %, P<0.001), FM (23.40 [19.10, 27.90] kg vs 19.80 [14.90, 25.00] kg, P<0.001), LFM (9.90 [8.10, 12.00] kg vs 8.60 [6.50, 10.80] kg, P<0.001), TFM (12.50 [9.80, 14.90] kg vs 10.00 [7.40, 12.70] kg, P<0.001), and VAT (129.00 [97.00, 154.30] cm2 vs 96.20 [69.63, 131.48] cm2, P<0.001). No significant differences were observed in muscle-related parameters or other demographic variables between the groups. After IPW, the level of TFM was still significantly higher in the BC group than in the control group (Table 1).
To further bolster the hypothesis that alterations in body composition are a risk factor rather than a consequence of cancer, we examined a body composition gradient within the control population. The subjects with benign breast nodules were younger (P<0.001, SMD=0.639), had a higher prevalence of diabetes (P=0.027, SMD=0.242) and hyperlipidemia (P=0.009, SMD=0.272), and presented higher LMM (16.92 [15.40, 18.87], kg vs 16.20 [14.50, 18.10] kg, P=0.019, SMD=0.212), but lower TMM (19.70 [18.10, 21.94] kg vs 21.80 [20.21, 23.21] kg, P<0.001, SMD=0.617), and lower LFM (8.80 [6.72, 11.00], kg vs 9.50 [7.50, 11.91] kg, P=0.061, SMD=0.249), even after IPW. Other demographics, comorbidities, laboratory indicators, and remaining body composition parameters were comparable (P>0.05, SMD<0.2) (Supplementary Table 1). This specific phenotype, characterized by a disproportionate reduction in trunk muscle and fat, may reflect a pre-existing systemic metabolic dysregulation that is also linked to a greater burden of conditions such as diabetes and hyperlipidemia. These findings suggest that the link between body composition changes and breast disease risk exists along a continuum, extending from benign conditions to cancer, rather than being merely a consequence of malignancy.
The Effect of Body Composition on Breast Carcinogenesis Risk
To investigate the potential interplay between breast cancer and adipose tissue distribution, we used lasso and logistic regression to assess the relationship between body composition parameters and breast cancer risk. The univariate logistic regression analysis indicated that higher TFM (OR=1.014, 95% CI: 1.005~1.023, P=0.003) and VAT (OR=1.001, 95% CI: 1.00003~1.002, P=0.043) were associated with an increased risk of breast cancer (Table 2). Multivariable analyses further substantiated that after adjustment for age, menopause and marital status, comorbidities, laboratory test indicators, and lifestyle factors higher MM (OR=1.027, 95% CI: 1.008~1.047, P=0.005), TFM (OR=1.046, 95% CI: 1.025~1.068, P<0.001) and VAT (OR=1.003, 95% CI: 1.0005~1.005, P=0.017) increased BC risk, while LFM (OR=0.971, 95% CI: 0.950~0.992, P=0.008) and TMM (OR=0.967, 95% CI: 0.951~0.984, P<0.001) decreased BC risk. Furthermore, sensitivity analysis confirmed that TFM and LFM remained risk factors, while TMM remained a protective factor (Table 2).
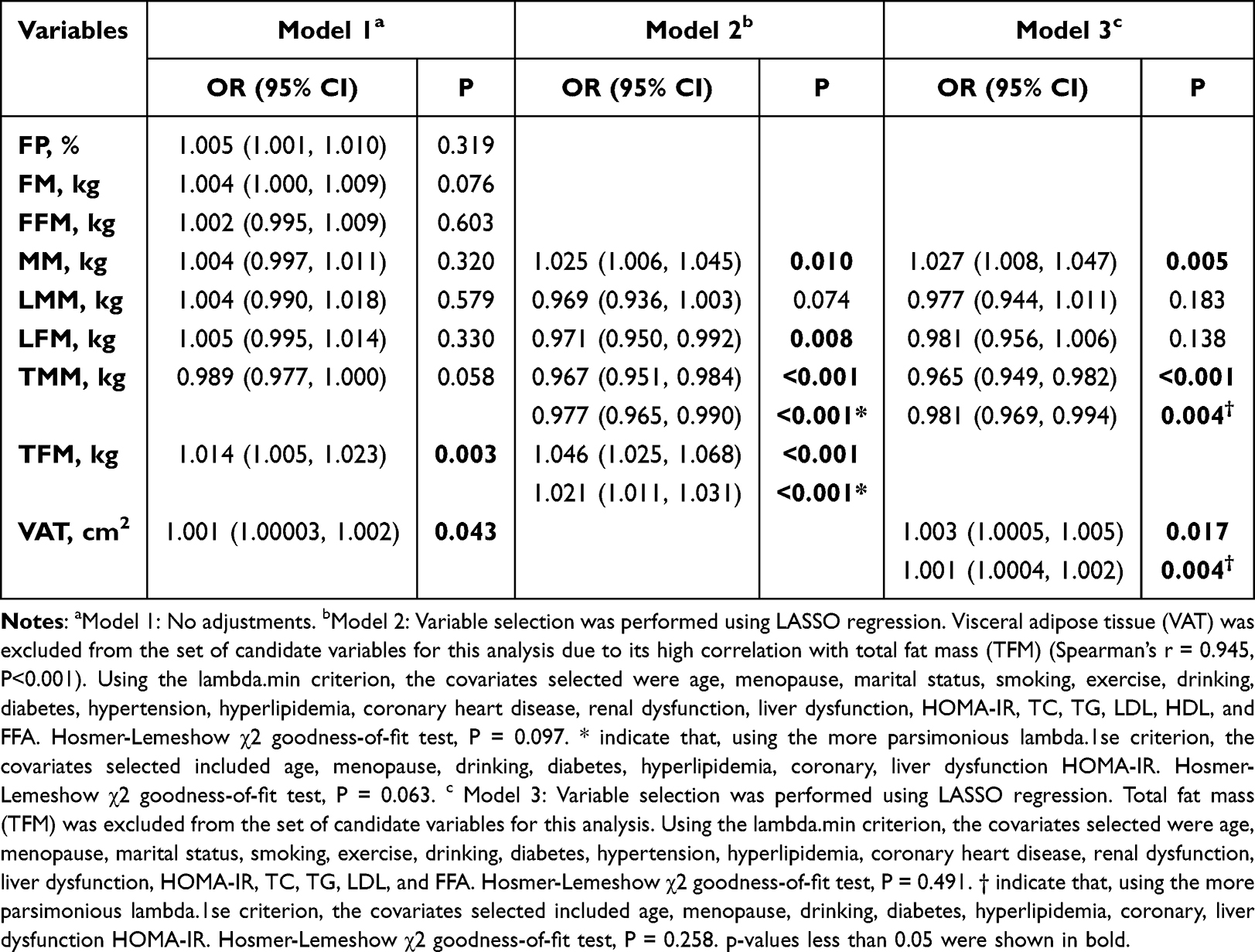 |
Table 2 The Association of Body Composition and Breast Cancer Risk After IPW |
To identify the key body composition parameters contributing to breast carcinogenesis, we developed an XGBoost model to explore their associations. After eliminating redundant parameters through multi-collinearity analysis and 10-fold cross-validation, the optimized model demonstrated robust predictive performance, with a training AUC of 0.826 (95% CI: 0.787~0.865) (Figure 2a) and a testing AUC of 0.764 (95% CI: 0.6906~0.837) (Figure 2b). Analysis of feature importance scores revealed that TFM, VAT, and TMM were among the top 10 features, suggesting that muscle atrophy and ectopic fat deposition contribute to BC (Figure 2c and d). These results suggested that different types of ectopic fat deposition in the visceral organs, trunk, and limb could play different roles in the metabolic regulation of breast cancer.
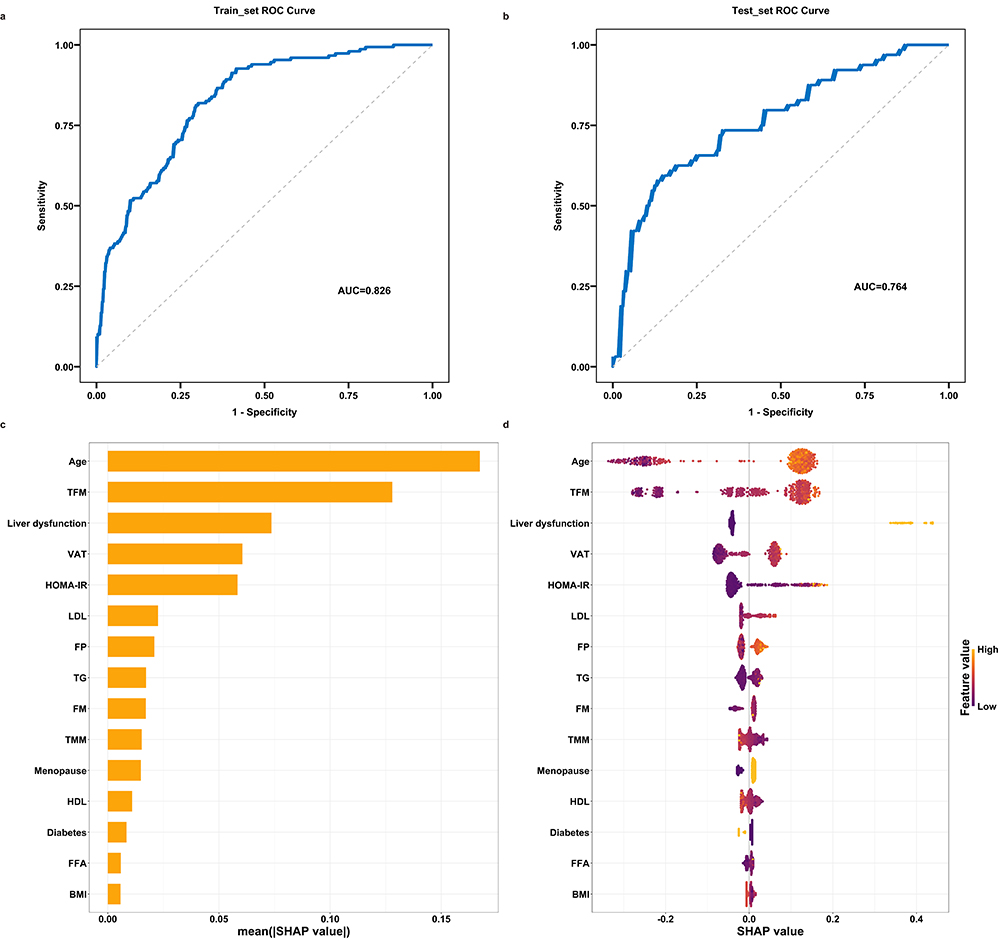 |
Figure 2 The feature importance score of body composition parameters. The models were established based on the XGBoost algorithm. (a) The ROC curve evaluates the training model. (b) The ROC curve evaluates the test model. (c) Feature importance based on mean (|SHAP|). (d) SHAP summary plot for XGBoost model. Abbreviations: TFM, Trunk fat mass; VAT, Visceral adipose tissue; HOMA-IR, Homeostatic model assessment of insulin resistance; LDL, Low‐density lipoprotein; FP, Fat percentage; TG, Triglyceride; FM, Fat mass; TMM, Trunk muscle mass; HDL, High‐density lipoprotein; FFA, Free fatty acid; BMI, Body mass index. |
The Influences of Body Composition on the Survival Outcome in Patients with Breast Cancer Post-Radical Mastectomy
Follow-up for this study was completed in May 2025 with a median follow-up period of 18 months (3–62 months). Survival data were available for 187 patients with BC who underwent radical mastectomy (27–86 years) (Figure 1). Among the enrolled patients, the majority were diagnosed with TNM stage I (25.67%) or II (58.29%), and 85.56% were postmenopausal. Notably, postmenopausal patients with BC demonstrated significantly elevated CEA (2.13 [1.42, 3.46] ng/mL vs 1.56 [0.84, 2.08] ng/mL, P=0.011), TC (5.00 [4.10, 5.77] mmol/L vs 4.40 [3.88, 4.93] mmol/L, P=0.006), and LDL (3.17 [2.47, 3.70] mmol/L vs 2.62 [2.27, 3.01] mmol/L, P=0.005), along with a reduction in LMM (16.40 [15.17, 18.02] vs 17.40 [16.10, 18.20], P=0.046). By the end of the follow-up period, 10 patients (5.35%) had developed distant metastasis; no relapse or death was recorded (Supplementary Table 2). The distant DMFS rates at 3, 12, 36, and 60 months were as follows: overall, 100.0%, 97.2%, 92.9%, and 73.5%; for postmenopausal patients, 100.0%, 98.4%, 93.1%, and 69.9%; for patients with TNM stage I–II BC, 100.0%, 98.4%, 93.2%, and 87.7%; and for those with TNM stage III–IV BC, 100.0%, 90.9%, 90.9%, and 45.5%.
Despite the pro-carcinogenic role of TFM, Kaplan-Meier analysis demonstrated improved DMFS in BC patients with higher TFM (Figure 3a), particularly among postmenopausal women (Figure 3b). After adjusting for age, TNM stage, HER2 status, ER, PR, pre- and postoperative treatments, preoperative distant metastasis, HOMA-IR, TG, TC, NLR, lifestyle factors, and comorbidities, multivariable Cox analysis identified FP (HR=0.829, 95% CI: 0.699~0.984, P=0.032), FM (HR=0.875, 95% CI: 0.774~0.989, P=0.033), and TFM (HR= 0.794, 95% CI: 0.634~0.994, P=0.044) were protective factors (Figure 3c). These same associations were also observed in the subgroup of postmenopausal patients (Figure 3d). Notably, no significant impact of VAT on DMFS was observed, suggesting distinct roles of visceral versus subcutaneous fat depots in tumor initiation and progression. Regarding muscle-related indicators, univariable Cox regression analysis indicated that LMM was associated with improved DMFS (HR=0.750, 95% CI: 0.590~0.953, P=0.019) (Supplementary Table 3). Furthermore, multivariable analysis demonstrated that LMM remained an independent protective factor for DMFS specifically in postmenopausal patients (Figure 3d). Taken together, these results indicated that subcutaneous adipose tissue and lean body mass may contribute to improving the DMFS among patients with BC post-radical mastectomy.
 |
Figure 3 Kaplan–Meier and Cox analysis of the relationship between fat distribution and distant metastasis-free survival in breast cancer and postmenopausal patients. (a) The Kaplan-Meier analysis compared distant metastasis-free survival based on trunk fat mass (TFM) quartiles in patients with breast cancer. (b) The Kaplan-Meier analysis compared distant metastasis-free survival based on trunk fat mass (TFM) quartiles in postmenopausal patients with breast cancer. (c) The hazard ratio of different body composition parameters and distant metastasis-free survival in patients with breast cancer, adjusting for age, TNM staging, HER2 status, ER status, PR status, preoperative and postoperative treatments, preoperative distant metastasis, HOMA-IR, TG, TC, NLR, lifestyle factors, and comorbidities. The Harrell’s C-index is 0.889, 0.878, 0.859, 0.860, 0.851, 0.854, 0.878, 0.869, 0.912, respectively. (d) The hazard ratio of different body composition parameters and distant metastasis-free survival in postmenopausal patients with breast cancer, adjusting for age, TNM staging, marital status, HER2 status, ER status, PR status, postoperative treatments, preoperative distant metastasis, HOMA-IR, TG, LHR, NLR, lifestyle factors, and comorbidities. The Harrell’s C-index is 0.945, 0.952, 0.931, 0.931, 0.947, 0.942, 0.924, 0.945, 0.952, respectively. The figures were generated with R software (Version 4.3.1). The cut-off values of TFM were recommended by X-tile based on distant metastasis-free survival. |
Given the variability in follow-up duration among patients, a sensitivity analysis was performed using a standardized follow-up period of at least two years, with results remaining consistent with the primary findings. Kaplan-Meier survival analysis revealed that patients with higher TFM (Figure 4a) and LFM (Figure 4b) exhibited significantly improved DMFS. Univariable Cox regression analysis showed that FP (HR=0.780, 95% CI: 0.622~ 0.978, P=0.032), FM (HR=0.762, 95% CI: 0.598~0.971, P=0.028), LFM (HR=0.481, 95% CI: 0.263~0.880, P=0.018) TFM (HR=0.639, 95% CI: 0.422~0.967, P=0.034), and VAT (HR=0.959, 95% CI: 0.923~0.998, P=0.037) were protective factors for DMFS. No significant association between muscle-related parameters and DMFS was observed in the univariable analysis (Supplementary Table 3). Multivariable Cox analysis confirmed FP (HR=0.710, 95% CI: 0.511~0.987, P=0.041), FM (HR=0.786, 95% CI: 0.620~0.995, P=0.045), and TFM (HR=0.632, 95% CI: 0.409~0.977, P=0.039) as protective factors for DMFS (Figure 4c).
 |
Figure 4 Kaplan–Meier and Cox analysis of the relationship between fat distribution and distant metastasis-free survival in breast cancer patients (≥ 2 years follow-up). (a) The Kaplan-Meier analysis compared distant metastasis-free survival based on limb fat mass (LFM) quartiles in patients with breast cancer with ≥2 years of follow-up. (b) The Kaplan-Meier analysis compared distant metastasis-free survival based on trunk fat mass (TFM) quartiles in patients with breast cancer with ≥2 years of follow-up. (c) The hazard ratio of different body composition parameters and distant metastasis-free survival in patients with breast cancer with ≥2 years of follow-up, adjusting for age, TNM staging, HER2 status, ER status, PR status, postoperative treatments, preoperative distant metastasis, HOMA-IR, NLR, lifestyle factors, and comorbidities. The Harrell’s C-index is 0.970, 0.965, 0.913, 0.909, 0.930, 0.896, 0.970, 0.952, 0.970, respectively. The figures were generated with R software (Version 4.3.1). The cut-off values of TFM and LFM were recommended by X-tile based on distant metastasis-free survival. Abbreviations: FP, Fat percentage; FM, Fat mass; FFM, Fat-free mass; MM, Muscle mass; LMM, Limb muscle mass; TMM, Trunk muscle mass; LFM, Limb fat mass; TFM, Trunk fat mass; VAT, Visceral adipose tissue. |
Discussion
Our research revealed that BC patients exhibited more prominent abdominal obesity, characterized by significantly higher levels of TFM and VAT, with TFM remaining notably elevated after IPW adjustment. This finding aligns with the established characterization of breast cancer as an obesity-associated malignancy and further corroborates that BMI fails to accurately reflect body composition characteristics, particularly the distribution of muscle and fat. The study found distinct links between fat depots and breast cancer: abdominal fat (TFM and VAT) raised the risk of cancer development, while LFM reduced it. Notably, during tumor progression, both TFM and LFM had a protective effect, improving DMFS, whereas no such association was observed for VAT. These results suggest that subcutaneous fat (LFM and TFM) may protect against breast cancer initiation and progression, whereas visceral fat (VAT) has the opposite adverse effect. Interestingly, MM was identified as a risk factor for BC, suggesting that the underlying mechanism may not be the muscle mass per se, but rather the intramuscular fat infiltration, which is often undetectable by BIA alone. TMM and LMM were associated with a significantly reduced cancer incidence and improved survival outcomes, respectively.
Emerging evidence challenges the reliance on BMI for defining obesity in breast cancer risk assessment, suggesting that more precise body composition metrics could provide superior predictive value for disease risk.31 Recent evidence indicates that general adiposity, defined by BMI, decreases the risk of breast cancer and its ER− and ER+ subtypes.32,33 In contrast, abdominal fat, especially visceral fat accumulation, increases the risk of breast cancer both before and after menopause, as measured by different measurements including anthropometric indicators (waist-hip ratio), CT, and BIA.32,34,35 These insights are consistent with our findings that both TFM and VAT significantly increase the risk of breast carcinogenesis. Obesity promotes breast cancer development through metabolic dysregulation, chronic inflammation, immune suppression, and tumor microenvironment remodeling.36 In our study, patients with breast cancer exhibited significantly more pronounced insulin resistance (IR) and dyslipidemia compared with controls, which is consistent with prior mechanistic evidence. Compared to conventional obesity parameters such as BMI and waist circumference, visceral adipose tissue area demonstrated a stronger association with the risk of developing type 2 diabetes. Furthermore, patients with visceral obesity exhibited more pronounced IR and hyperleptinemia.37 Conversely, IR and hyperleptinemia may further exacerbate ectopic fat distribution, creating a vicious cycle that amplifies both generalized obesity and visceral fat accumulation.38 Notably, our study identified LFM as a protective factor against breast cancer development, underscoring the beneficial role of SAT. As previously established, SAT acts as a metabolically favorable “metabolic sink” characterized by elevated adipose tissue lipoprotein lipase activity and reduced hormone-sensitive lipase activity. This functional profile facilitates the storage of excess fatty acids, thereby preventing ectopic fat deposition and its associated adverse metabolic consequences. Furthermore, SAT secretes higher levels of adiponectin and lower levels of proinflammatory cytokines, which are linked to a reduced risk of breast cancer.39 This observed bidirectional crosstalk between ectopic fat deposition and these metabolic perturbations (IR/dyslipidemia) may represent a critical pathway in breast carcinogenesis, potentially explaining the obesity-oncology link beyond interpretations reliant solely on BMI.
Although obesity is a well-established risk factor for breast cancer, prognostic heterogeneity persists, attributable to methodological discrepancies, the threshold effects of BMI, and tumor subtypes.40 Interestingly, our findings indicate that higher TFM is a protective factor against distant metastasis in BC patients following radical mastectomy. Abdominal (trunk) fat consists of subcutaneous, visceral, and intermuscular adipose depots, and thigh fat consists primarily of subcutaneous adipose and intermuscular adipose. Existing evidence highlights distinct structural and functional differences between SAT and VAT, suggesting that the protective effect of TFM against breast cancer may be primarily attributed to its subcutaneous component,41 which is further supported by the protective effect of LFM in the sensitive analysis. SAT contains more small adipocytes, which are more insulin-sensitive and have high avidity for FFAs and TGs uptake, preventing their deposition in non-adipose tissue like intermuscular areas that would otherwise promote lipotoxicity, IR, and pro‐inflammatory cytokines secretion.41,42 Notably, these protective mechanisms may intersect with estrogen signaling, a critical regulator of breast cancer prognosis, as ER+ patients generally exhibit higher overall survival rates.43 Estrogen receptors are widely expressed in adipose tissue, showing greater binding capacity in SAT. This hormonal influence promotes preferential accumulation of gluteofemoral SAT, a phenomenon potentially associated with metabolic protection.41 Collectively, these findings suggest that SAT confers protection against breast cancer through both intrinsic metabolic advantages and synergistic interactions with estrogen-mediated signaling, creating a dual defense against harmful lipid redistribution and systemic inflammation.
The role of muscle-related parameters in breast cancer development and progression has been extensively investigated, primarily in the context of muscle atrophy. Epidemiological studies have established muscle atrophy as a significant risk factor for various cancers, including breast cancer.44 Our research found no significant evidence of muscle loss in BC patients, likely because they were at a relatively early TNM stage. Nevertheless, substantial evidence supports a protective role for muscle mass against breast cancer progression. Low muscle mass, including reduced limb and trunk muscle mass, has been associated with chemotherapy toxicities, dose reductions, dose delays, treatment discontinuation, and poorer overall survival in BC patients.18,45,46 Additionally, healthy skeletal muscle is a metabolically active endocrine organ that secretes myokines, which can inhibit cancer cell proliferation and migration, and induce apoptosis.46 Furthermore, relevant research has identified that expression of muscle aging-related genes may play a crucial role in breast cancer prognosis and represent a potential novel prognostic biomarker.47
Interestingly, in contrast to these previous findings, our study using BIA revealed that higher total muscle mass was associated with an increased risk of BC. A plausible explanation is that BIA cannot distinguish between healthy lean muscle tissue and muscle with fat infiltration (myosteatosis). Excessive lipid deposition within muscle fibers has been linked to metabolic dysfunction, insulin resistance, and chronic inflammation, all of which may contribute to tumor development and progression. Therefore, our results may reflect the detrimental metabolic impact of intramuscular fat rather than the favorable effects of contractile muscle mass.42,48 This discrepancy underscores the importance of considering muscle quality, not only quantity, in cancer risk assessment. These findings collectively emphasize that integrating both muscle mass and muscle quality evaluation into comprehensive breast cancer management strategies could improve risk stratification and therapeutic decision-making.
Nevertheless, this study has several limitations that warrant consideration. First, the relatively small sample size may limit statistical power and generalizability. Second, the case-control design inherently restricts causal inference, despite the propensity score matching being employed. Third, the underrepresentation of advanced-stage (III/IV) patients limits mortality assessment and broader applicability. Additionally, the use of BIA for assessing visceral adiposity introduces methodological constraints. Specifically, BIA lacks the precision of gold-standard imaging modalities (CT or MRI) for quantifying visceral fat and cannot differentiate SAT from VAT. Future studies utilizing imaging-based assessment of body composition could provide a more precise characterization of adipose tissue distribution and its pathophysiological role. Moreover, future prospective multicenter studies with longitudinal designs that actively enroll more patients with advanced-stage disease would enhance causal inference, prognostic accuracy, and clinical relevance. Larger multicenter cohorts with longitudinal follow‑up and enriched recruitment of advanced‑stage cases would better support causal inference, refine prognostic models, and increase the clinical applicability.
Conclusion
In conclusion, our study emphasizes the importance of detailed body composition analysis for the assessment of breast cancer risk and prognosis. We demonstrate that higher trunk muscle mass protects against breast cancer development, while greater overall muscle mass, trunk fat, and visceral fat increase risk. However, after mastectomy, higher subcutaneous fat (trunk and limb) is linked to better survival, especially in postmenopausal women. These findings underscore the distinct roles of different adipose depots and the importance of muscle quality in modulating cancer outcomes. Our results support the integration of body composition assessment into clinical practice to improve risk stratification and personalized management strategies. Future research employing advanced imaging techniques in larger, longitudinal cohorts is warranted to elucidate the underlying mechanisms and translate these insights into targeted interventions for breast cancer prevention and treatment.
Abbreviations
BC, Breast Cancer; DMFS, Distant Metastasis-Free Survival; TMM, Trunk Muscle Mass; TFM, Trunk Fat Mass; VAT, Visceral Adipose Tissue; LMM, Limb Muscle Mass; BMI, Body Mass Index; SAT, Subcutaneous Adipose Tissue; BIA, Bioelectrical Impedance Analysis; FP, Fat Percentage; FM, Fat Mass; FFM, Fat Free Mass; MM, Muscle Mass; LFM, Limb Fat Mass; HOMA-IR, homeostasis Model Assessment of Insulin Resistance; TG, Triglyceride; TC, Total Cholesterol; HDL, High-Density Lipoprotein; LDL, Low-Density Lipoprotein; FFA, Free Fatty Acid; LHR, Low-Density Lipoprotein to High-Density Lipoprotein Ratio; NLR, Neutrophil-to-Lymphocyte Ratio; ER, Estrogen Receptor; PR, Progesterone Receptor; CEA, Carcinoembryonic Antigen; IPW, Inverse probability weight; ROC, Receiver operating characteristic; AUC, Area under the curve; IR, Insulin Resistance.
Data Sharing Statement
The data generated in this study are available upon request from Kang Yu, the corresponding author.
Ethics Statement and Informed Consent
All study participants gave written consent, and ethical approval was provided by the Ethics Committee of Peking Union Medical College Hospital (No. HS889), Central Hospital, Tianjin University (No. IRB2021-037-02). No sex-based or racial/ethnic-based differences were present. This study was conducted in accordance with the Declaration of Helsinki.
Funding
This work was supported by the National Key R&D Program of China 2022YFF1100600/2022YFF1100604; the National Natural Science Foundation of China (82404264); Postdoctoral Fellowship Program of CPSF (GZC20230296); the China Postdoctoral Science Foundation (2023M730321).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71:209–14.
2. Lauby-Secretan B, Scoccianti C, Loomis D, et al. Body Fatness and Cancer--Viewpoint of the IARC Working Group. N Engl J Med. 2016;375(8):794–798. doi:10.1056/NEJMsr1606602
3. Bardou M, Barkun AN, Martel M. Obesity and colorectal cancer. Gut. 2013;62(6):933–947. doi:10.1136/gutjnl-2013-304701
4. Bowen TS, Schuler G, Adams V. Skeletal muscle wasting in cachexia and sarcopenia: molecular pathophysiology and impact of exercise training. J Cachexia, Sarcopenia Muscle. 2015;6(3):197–207. doi:10.1002/jcsm.12043
5. Iyengar NM, Arthur R, Manson JE, et al. Association of Body Fat and Risk of Breast Cancer in Postmenopausal Women With Normal Body Mass Index: a Secondary Analysis of a Randomized Clinical Trial and Observational Study. JAMA Oncol. 2019;5(2):155–163. doi:10.1001/jamaoncol.2018.5327
6. Bea JW, Ochs-Balcom HM, Valencia CI, et al. Abdominal visceral and subcutaneous adipose tissue associations with postmenopausal breast cancer incidence. JNCI Cancer Spectr. 2025;9(1):pkaf007. doi:10.1093/jncics/pkaf007
7. Murawiak M, Krzymińska-Siemaszko R, Kaluźniak-Szymanowska A, et al. Sarcopenia, Obesity, Sarcopenic Obesity and Risk of Poor Nutritional Status in Polish Community-Dwelling Older People Aged 60 Years and Over. Nutrients. 2022;14(14):2889. doi:10.3390/nu14142889
8. Palau-Rodriguez M, Marco-Ramell A, Casas-Agustench P, et al. Visceral Adipose Tissue Phospholipid Signature of Insulin Sensitivity and Obesity. J Proteome Res. 2021;20(5):2410–2419. doi:10.1021/acs.jproteome.0c00918
9. Yiallourou A, Pantavou K, Markozannes G, et al. Non-genetic factors and breast cancer: an umbrella review of meta-analyses. BMC Cancer. 2024;24:903.
10. Pham DV, Tilija Pun N, Park PH. Autophagy activation and SREBP-1 induction contribute to fatty acid metabolic reprogramming by leptin in breast cancer cells. Mol Oncol. 2021;15:657–678.
11. Larsson SC, Spyrou N, Mantzoros CS. Body fatness associations with cancer: evidence from recent epidemiological studies and future directions. Metabolism. 2022;137:155326.
12. Acevedo-León D, Gómez-Abril SÁ, Monzó-Beltrán L, et al. Adherence to the Mediterranean Diet Has a Protective Role against Metabolic and DNA Damage Markers in Colorectal Cancer Patients. Antioxidants. 2022;11:499.
13. Park YM, Shivappa N, Petimar J, et al. Dietary inflammatory potential, oxidative balance score, and risk of breast cancer: findings from the Sister Study. Int J Cancer. 2021;149(3):615–626. doi:10.1002/ijc.33581
14. Bradshaw PT, Cespedes Feliciano EM, Prado CM, et al. Adipose Tissue Distribution and Survival Among Women with Nonmetastatic Breast Cancer. Obesity. 2019;27(6):997–1004. doi:10.1002/oby.22458
15. Yücel KB, Aydos U, Sütcüoglu O, et al. Visceral obesity and sarcopenia as predictors of efficacy and hematological toxicity in patients with metastatic breast cancer treated with CDK 4/6 inhibitors. Cancer Chemother Pharmacol. 2024;93(5):497–507. doi:10.1007/s00280-024-04641-z
16. Fabian CJ, Klemp JR, Marchello NJ, et al. Rapid Escalation of High-Volume Exercise during Caloric Restriction; Change in Visceral Adipose Tissue and Adipocytokines in Obese Sedentary Breast Cancer Survivors. Cancers. 2021;13(19):4871. doi:10.3390/cancers13194871
17. Kwon MR, Ko ES, Park MS, et al. Impact of Skeletal Muscle Loss and Visceral Obesity Measured Using Serial CT on the Prognosis of Operable Breast Cancers in Asian Patients. Korean J Radiol. 2022;23(2):159–171. doi:10.3348/kjr.2020.1475
18. Caan BJ, Cespedes Feliciano EM, Prado CM, et al. Association of Muscle and Adiposity Measured by Computed Tomography With Survival in Patients With Nonmetastatic Breast Cancer. JAMA Oncol. 2018;4(6):798–804. doi:10.1001/jamaoncol.2018.0137
19. Calle EE, Kaaks R. Overweight, obesity and cancer: epidemiological evidence and proposed mechanisms. Nat Rev Cancer. 2004;4(8):579–591. doi:10.1038/nrc1408
20. Heeran AB, McCready J, Dunne MR, et al. Opposing Immune-Metabolic Signature in Visceral Versus Subcutaneous Adipose Tissue in Patients with Adenocarcinoma of the Oesophagus and the Oesophagogastric Junction. Metabolites. 2021;11(11):768. doi:10.3390/metabo11110768
21. Mathur N, Severinsen MCK, Jensen ME, et al. Human visceral and subcutaneous adipose stem and progenitor cells retain depot-specific adipogenic properties during obesity. Front Cell Dev Biol. 2022;10:983899. doi:10.3389/fcell.2022.983899
22. Vilaca T, Evans A, Gossiel F, Paggiosi M, Eastell R, Walsh JS. Fat, adipokines, bone structure and bone regulatory factors associations in obesity. Eur J Endocrinol. 2022;187(6):743–750. doi:10.1530/EJE-22-0530
23. Dai Y, Lan J, Li S, Xu G. Exploring the Impact of Sarcopenia on Mortality in Breast Cancer Patients: a Comprehensive Systematic Review and Meta-Analysis. Breast Care. 2024;19(6):316–328. doi:10.1159/000541421
24. Iwase T, Wang X, Shrimanker TV, Kolonin MG, Ueno NT. Body composition and breast cancer risk and treatment: mechanisms and impact. Breast Cancer Res Treat. 2021;186(2):273–283. doi:10.1007/s10549-020-06092-5
25. Williams GR, Dunne RF, Giri S, Shachar SS, Caan BJ. Sarcopenia in the older adult with cancer. J Clin Oncol. 2021;39(19):2068–2078. doi:10.1200/JCO.21.00102
26. Shen S, Liao Q, Zhang T, Pan R, Lin L. Myricanol modulates skeletal muscle-adipose tissue crosstalk to alleviate high-fat diet-induced obesity and insulin resistance. Br J Pharmacol. 2019;176(20):3983–4001. doi:10.1111/bph.14802
27. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
28. Shahar S, Salleh RM, Ghazali AR, Koon PB, Mohamud WN. Roles of adiposity, lifetime physical activity and serum adiponectin in occurrence of breast cancer among Malaysian women in Klang Valley. Asian Pac J Cancer Prev. 2010;11(1):61–66.
29. Ma S, Xi B, Yang L, Sun J, Zhao M, Bovet P. Trends in the prevalence of overweight, obesity, and abdominal obesity among Chinese adults between 1993 and 2015. Int J Obes Lond. 2021;45(2):427–437. doi:10.1038/s41366-020-00698-x
30. Chung GKK, Yeo W, Cheng A, et al. Prognostic significance of abdominal obesity and its post-diagnosis change in a Chinese breast cancer cohort. Breast Cancer Res Treat. 2022;193(3):649–658. doi:10.1007/s10549-022-06526-2
31. Feliciano EMC, Winkels RM, Meyerhardt JA, Prado CM, Afman LA, Caan BJ. Abdominal adipose tissue radiodensity is associated with survival after colorectal cancer. Am J Clin Nutr. 2021;114(6):1917–1924. doi:10.1093/ajcn/nqab285
32. Freuer D, Linseisen J, O’Mara TA, et al. Body Fat Distribution and Risk of Breast, Endometrial, and Ovarian Cancer: a Two-Sample Mendelian Randomization Study. Cancers. 2021;13(20):5053. doi:10.3390/cancers13205053
33. Zhang Z, Curran G, Shannon J, et al. Body Mass Index Is Inversely Associated with Risk of Postmenopausal Interval Breast Cancer: results from the Women’s Health Initiative. Cancers. 2022;14(13):3228. doi:10.3390/cancers14133228
34. Park YM, White AJ, Nichols HB, O’Brien KM, Weinberg CR, Sandler DP. The association between metabolic health, obesity phenotype and the risk of breast cancer. Int J Cancer. 2017;140(12):2657–2666. doi:10.1002/ijc.30684
35. Kim MS, Choi YJ, Lee YH. Visceral fat measured by computed tomography and the risk of breast cancer. Transl Cancer Res. 2019;8(5):1939–1949. doi:10.21037/tcr.2019.09.16
36. Devericks EN, Carson MS, McCullough LE, Coleman MF, Hursting SD. The obesity-breast cancer link: a multidisciplinary perspective. Cancer Metastasis Rev. 2022;41(3):607–625. doi:10.1007/s10555-022-10043-5
37. Barbarash O, Gruzdeva O, Uchasova E, et al. The role of adipose tissue and adipokines in the manifestation of type 2 diabetes in the long-term period following myocardial infarction. Diabetol Metab Syndr. 2016;8(1):24. doi:10.1186/s13098-016-0136-6
38. Kraakman MJ, Liu Q, Postigo-Fernandez J, et al. PPARγ deacetylation dissociates thiazolidinedione’s metabolic benefits from its adverse effects. J Clin Invest. 2018;128(6):2600–2612. doi:10.1172/JCI98709
39. Singh P, Covassin N, Marlatt K, Gadde KM, Obesity HSB. Body Composition, and Sex Hormones: implications for Cardiovascular Risk. Compr Physiol. 2021;12:2949–2993.
40. Cespedes Feliciano EM, Kwan ML, Kushi LH, et al. Body mass index, PAM50 subtype, recurrence, and survival among patients with nonmetastatic breast cancer. Cancer. 2017;123(13):2535–2542. doi:10.1002/cncr.30637
41. Ibrahim MM. Subcutaneous and visceral adipose tissue: structural and functional differences. Obes Rev. 2010;11(1):11–18. doi:10.1111/j.1467-789X.2009.00623.x
42. Li CW, Yu K, Shyh-Chang N, et al. Pathogenesis of sarcopenia and the relationship with fat mass: descriptive review. J Cachexia, Sarcopenia Muscle. 2022;13(2):781–794. doi:10.1002/jcsm.12901
43. Belete AM, Aynalem YA, Gemeda BN, Demelew TM, Shiferaw WS. The Effect of Estrogen Receptor Status on Survival in Breast Cancer Patients in Ethiopia. Retrospective Cohort Study. Breast Cancer. 2022;14:153–161. doi:10.2147/BCTT.S365295
44. Sun MY, Chang CL, Lu CY, Wu SY, Zhang JQ. Sarcopenia as an Independent Risk Factor for Specific Cancers: a Propensity Score-Matched Asian Population-Based Cohort Study. Nutrients. 2022;14(9):1910. doi:10.3390/nu14091910
45. Jang MK, Park S, Raszewski R, Park CG, Doorenbos AZ, Kim S. Prevalence and clinical implications of sarcopenia in breast cancer: a systematic review and meta-analysis. Support Care Cancer. 2024;32(5):328. doi:10.1007/s00520-024-08532-0
46. Huang WJ, Zhang ML, Wang W, et al. Preoperative Pectoralis Muscle Index Predicts Distant Metastasis-Free Survival in Breast Cancer Patients. Front Oncol. 2022;12:854137. doi:10.3389/fonc.2022.854137
47. Wang Y, Zhong P, Wang C, Huang W, Yang H. Genetic overlap between breast cancer and sarcopenia: exploring the prognostic implications of SLC38A1 gene expression. BMC Cancer. 2024;24(1):1533. doi:10.1186/s12885-024-13326-y
48. Costa-Pereira JP, Macêdo IF, Barbosa GA, et al. Myosteatosis is associated with advanced TNM stage and tumor features in young females with breast cancer. BMC Cancer. 2025;25(1):1576. doi:10.1186/s12885-025-15047-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.