Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Views on Interprofessional Collaboration in a Dutch Sexual Assault Center: A Qualitative Study Among Workers
Authors Mulder J, Teunissen TAM ![]() , Peters VMJ, Moors ML, Lagro-Janssen ALM
, Peters VMJ, Moors ML, Lagro-Janssen ALM ![]()
Received 13 April 2023
Accepted for publication 29 June 2023
Published 17 July 2023 Volume 2023:16 Pages 2001—2012
DOI https://doi.org/10.2147/JMDH.S416996
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jasmijn Mulder,1 Theodora Alberta Maria Teunissen,1 Veranie Maria Johanna Peters,1 Marie Louise Moors,2 Antoinette Leonarda Maria Lagro-Janssen1
1Department of Primary and Community Care, Gender and Women’s Health, Radboud University Medical Center, Nijmegen, the Netherlands; 2Emergency Department, Radboud University Medical Center, Nijmegen, the Netherlands
Correspondence: Jasmijn Mulder, Radboudumc, Afdeling Eerstelijnsgeneeskunde, Huispost 121, t.a.v. Jasmijn Mulder, Postbus 9101, Nijmegen, 6500HB, the Netherlands, Email [email protected]
Purpose: As the response to sexual assault victims proved to be shattered and substandard, sexual assault centers were set up to improve care by providing the victims with medical, psychosocial and legal care. The Dutch Centers for Sexual Assault were launched in 2012. We wished to examine the challenges in interprofessional collaboration experienced in a long-running Dutch Sexual Assault Center.
Methods: In this qualitative study, data was collected via semi-structured explorative interviews which were analyzed using thematic analysis in an iterative process. The semi-structured interviews were held with fifteen professionals from medical, psychosocial and legal disciplines. An interview guide was developed based on expert opinion and the Bronstein Index of Interprofessional Collaboration. Qualitative analyses were done using the method of thematic analysis in ATLAS.ti and were reported according to the COREQ criteria. The themes of the experienced challenges in interprofessional collaboration were further clarified using quotations.
Results: Participants mentioned three themes that challenged interprofessional collaboration: 1. discrepancies in professional involvement, 2. conflicting goals and 3. a lack of connection. Discrepancies in motivation and affinity to work with victims of sexual violence between professionals proved to be the most pivotal challenge to collaboration, leading to disturbing differences in professional involvement. A low caseload and time restraints complicated gaining expertise, affinity and motivation. Conflicting goals and confidentiality issues arose between the medical and legal disciplines due to their contrasting aims of caring for victims versus facilitating prosecution. Some professionals felt a lack of connection, particularly due to missing face-to-face personal contact, which hindered the sharing of complex or burdensome cases and gaining insight into the other discipline’s competences.
Conclusion: Building collective ownership and equal professional involvement are crucial for interprofessional collaboration. Professional involvement should be increased by training courses to clarify conflicting goals and to improve reciprocal personal contact between professionals. Training courses should be facilitated with organizational financial support.
Keywords: interprofessional collaboration, sexual assault center, challenges, sexual assault, sexual violence, qualitative methods
Introduction
Sexual assault is defined as forcing someone to perform or undergo sexual acts and/or undergo manual, oral, vaginal or anal sex against their will.1 In the Netherlands, approximately 22% of women and 6% of men have experienced sexual assault.2 This large number of victims requires a united approach between medical, psychosocial and legal disciplines to provide victims with the best possible care. Medical care is required to treat acute injuries and prevent sexually transmitted diseases or possibly rape-related pregnancy; psychosocial care is needed to monitor mental health; and legal services are required to increase the likelihood of perpetrators being prosecuted. All of these are important for sexual assault victims.3–6 However, victims who do seek help often have negative experiences such as insensitive, inexperienced and victim-blaming treatment from professionals, which can lead to secondary victimization.3,4 If medical, psychosocial and legal disciplines do not collaborate appropriately, with workers from each discipline lacking expertise on how to treat sexual assault victims and lacking knowledge of how other disciplines operate, the response to sexual assault victims is often shattered.5–7
Therefore, sexual assault centers were set up to improve care for victims of sexual assault. Sexual assault centers aim to provide 24/7 multidisciplinary care to victims of sexual assault with medical, psychosocial and legal services being provided in one place and offering adequate aftercare and referral services to the victims. In the Netherlands, Centers for Sexual Assault (CSGs) have been set up since 2012. The Center for Sexual Assault Gelderland-Zuid en -Midden (CSG-GZM) was one of the first operating sexual assault centers in the Netherlands and serves over 1.2 million residents of the southern and middle part of the province of Gelderland. The CSG-GZM is an interprofessional collaboration amongst professionals from three disciplines: the medical, psychosocial and legal disciplines. Collaboration in such an interprofessional team is a complex process bringing together professionals with different goals and aiming to realize an effective interpersonal process that will facilitate the achievement of goals that cannot be reached when individual professionals act on their own.5,8,9
Although interprofessional collaboration can improve quality of care, it is also known to pose challenges. Literature about interprofessional collaboration in Sexual Assault Response Teams in the United States found that role conflicts are likely to occur when multiple disciplines with diverse roles and priorities work together while facing differences in philosophies, principles and perspectives on sexual assault and victims’ needs.10–13 Different orientations to the victim, particularly those between victims’ advocates and law enforcement officers, were a frequent explanation for conflict.10 Victim confidentiality, particularly leading to complicated communication and conflict between medical and legal disciplines, impeded interprofessional collaboration.12 Another perceived challenge involved case characteristics, such as alcohol use, that make prosecution more difficult.14
Shortly after the CSG-GZM had been launched, the difficulties encountered in interprofessional collaboration were assessed.15 Interprofessional collaboration turned out to be particularly challenged by the urgent need to define precise roles for professionals, the struggle to create a shared vision of optimal care and the high emotional cost involved, which affected the professionals’ motivation. These findings led to the implementation of structural meetings, education courses and further protocolling. As the CSG-GZM has now been operating for many years and initial problems may have been solved, the following research question was formulated: what do professionals at a long-running Dutch Sexual Assault Center perceive to be challenges in interprofessional collaboration?
Materials and Methods
Study Design
This study used a qualitative approach, collecting data via semi-structured explorative interviews. The interviews were analyzed using the thematic analysis method in an iterative process.16 The interviews took place from mid-June 2020 until the end of July 2020. The remainder of the Methods section adheres to the COREQ checklist for reporting qualitative research.17
Research Setting
This study was performed at the CSG-GZM, an interprofessional collaboration amongst medical, legal and psychosocial disciplines. The medical discipline is represented by the Emergency Department (ED) of the Radboud University Medical Center; the psychosocial discipline is represented by an Academic Primary Health Care Center; and the legal discipline is represented by the Community Health Services (providing forensic physicians) and the Dutch Eastern District Police Department.
The CSG-GZM offers acute (≤ 7 days) and follow-up care for victims of sexual assault in the three domains of medical, legal and psychosocial care. Medical and legal care for victims of acute sexual assault is arranged at the ED. A 7-day limit was set as this period offers sufficient opportunity to preserve forensic evidence to build a legal case. The ED staff test and prevent STDs, take preventive pregnancy measures if necessary and, at the victim’s request, contact the police to visit the ED. The police provide legal care by providing an informative consultation about possible legal steps and pressing charges. A forensic physician can be called in by the police to perform a forensic medical examination (FME). A day after acute care has been provided, psychosocial follow-up care is initiated by a case manager, who invites the victim for a consultation either via phone or at the Academic Primary Health Care Center. The case managers are mental health nurse practitioners. The case manager’s follow-up care consists of psychosocial guidance and screening for posttraumatic stress disorder (PTSD) after 4–6 weeks. In the case of PTSD or other psychological disorders, case managers refer victims to psychologists at affiliated practices. The CSG-GZM has a coordinator, acting as the point of contact for all professionals working for the center. Next to the coordinator, one representative from each organization (the ED, Academic Primary Health Care Center, Community Health Services and Dutch Eastern Police Department) is involved in CSG-GZM management. As representatives have a more extensive role in the management of the CSG-GZM, they act as a translator between management and professionals at the floor. They may gather problems their colleagues perceive to discuss in management meetings, as well as translate new policy to their colleagues by educating their colleagues in meetings or by implementing local guidelines.
The professionals working for the CSG-GZM range from professionals such as the representatives and case managers who consciously decided to be heavily involved in the CSG-GZM to ED staff, police and forensic physicians who are expected to work for the CSG-GZM when they are on call and a victim is admitted to the ED. When a victim is admitted to the ED and a FME is to be performed, the ED staff, police and the forensic physician discuss prior to the examination what information the ED and police have gathered. In this way, the victim does not have to retell their story to every new professional. After the FME, there is a debrief regarding how the examination and collaboration went and what could be improved. Whilst ED staff, police and forensic physicians may meet each other at the ED, case managers and psychologists do not work at the ED nor have frequent contact with the medico-legal disciplines.
The CSG-GZM has two structural meetings: a management meeting and a process meeting. In the management meeting, the representatives reflect on the way the center operates, engage in policymaking and resolve possible conflict. In the process meeting, all professionals involved in the CSG-GZM are invited four times a year to reflect on quality of care and collaboration. The core activity within the process meetings is discussing individual complicated cases. Furthermore, protocolling and continuing education courses have been implemented with the aim of enhancing understanding of the roles played by each discipline and to facilitate a better connection between professionals. Every professional from the CSG-GZM is welcome to join the education courses for free. All professionals working for the CSG-GZM are expected to be up to date with policy and guidelines. Professionals are free to decide whether they want to attend the process meetings or education courses.
Participants and Sampling
To promote trustworthiness of the data, we used purposive sampling reflecting a variety of worker characteristics and experiences. We included at least two workers from every discipline (ED physicians, ED nurses, squad police officers, forensic physicians, general practitioners, trauma-psychologists, and the coordinator of the center). We also selected representatives as well as other professionals with variable working experience at the CSG-GZM and of different ages. Participants who had worked for the CSG-GZM for less than six months were excluded. We aimed to include participants till saturation was reached.18
The interviews were conducted by a trained female Master’s student in Medicine (VP). The research committee consisted of a professor in the field of sexual violence (TLJ), a researcher and medical teacher at the Radboud University Medical Center (DT), an ED physician and representative of the CSG-GZM at the ED and a PhD medical student (JM).
Instruments
An interview guide was developed based on expert opinion (our research committee) and the Bronstein Index of Interprofessional Collaboration, a validated instrument developed to measure collaboration between social workers and other professionals.8 The topics from this model were rewritten into open-ended questions and discussed by the research committee (Table 1).
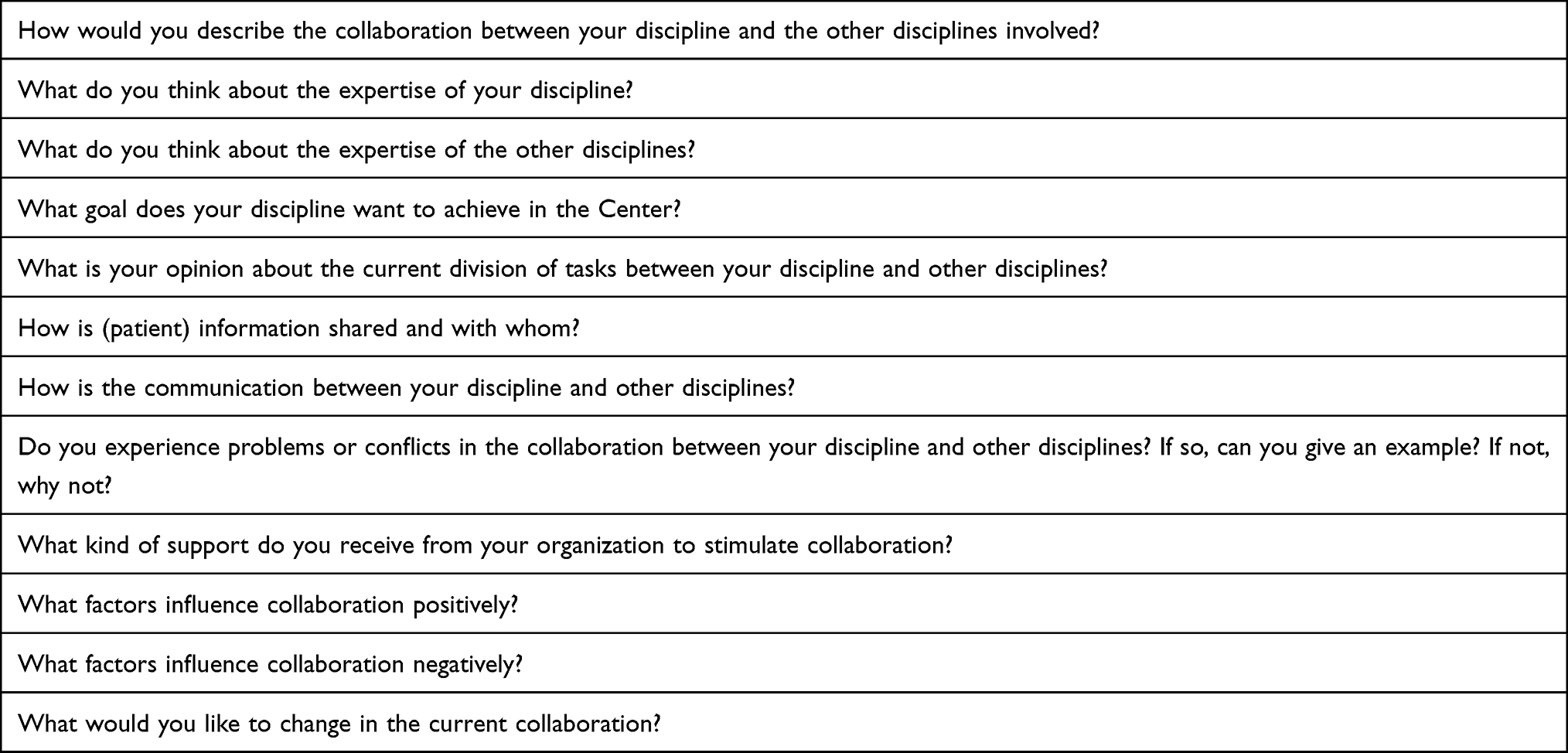 |
Table 1 Interview Guide |
Data Collection
After approval, the interviewer contacted the participants by email and supplied them with an information letter, an informed consent form and a short questionnaire for background information. If participants agreed to participate, a telephone interview was scheduled. Participants were asked to return the informed consent form and the questionnaire before the start of the interview. The interviews lasted between 30–60 minutes. With the participants’ oral consent, single interviews were recorded and transcribed verbatim by using f4 audio transcription software. At the end of each interview, the interviewer verbally summarized the conversation to the interviewee. The interviewees were asked to approve the content of the summary. All but one participant gave their permission to be quoted. No field notes were made during the interviews. As no new issues were found after the intended number of interviews, saturation had been reached.
Data Analysis
The interviews were analyzed with ATLAS.ti (version 8.4.20). Coding was done following open, axial and selective coding.19 Two researchers read the transcripts and used open coding to conceptualize the data. After the first three interviews, the researchers discussed their codes, and after consensus had been reached, a code list was made. In case of conflicts, a third person was available for decision-making. The first coder coded all transcripts. The second coder coded transcripts 1 through 3 and 6 through 11. When open coding was completed, axial coding was initiated by reflecting on the codes and grouping them into categories.
Lastly, the coders developed the categories into overarching themes. Categories and themes were discussed with the research committee to establish the definitive themes. We decided to identify a quotation only by number (not by discipline or position) to guarantee the participants’ anonymity. The numbering order was known only by the researcher and by the research committee. Some, many or most indicate that < 4, 4–9, 9–15 participants, respectively, shared an opinion.
Ethical Considerations
In accordance with the Dutch law, ethical approval of this study was not obligatory. All participants signed an informed consent form which was confirmed orally prior to the start of the interview.
Results
A total of sixteen participants were approached, fifteen of whom agreed to be interviewed. One person (police officer) declined participation due to time constraints caused by the Covid-19 pandemic. The majority of the participants were females with a great variety in age and level of work experience (Table 2).
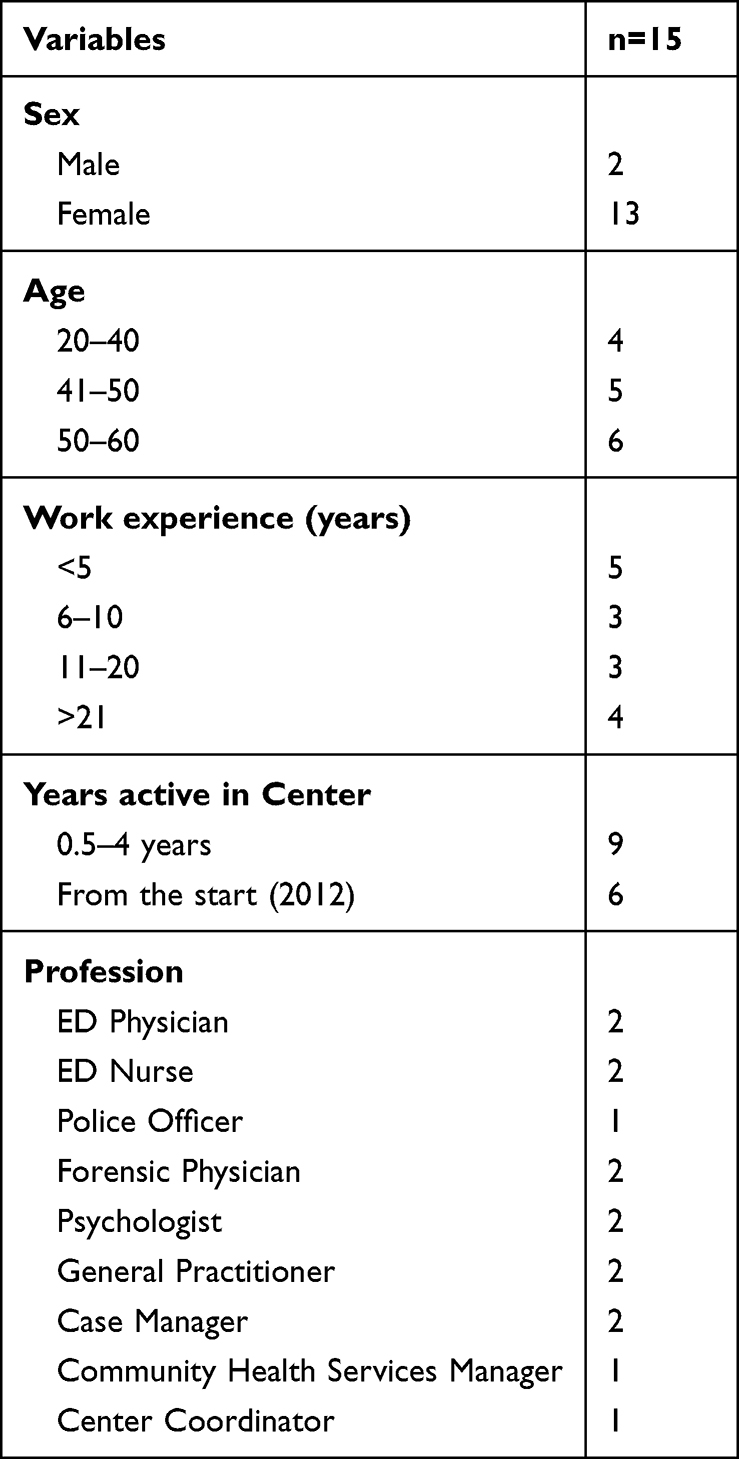 |
Table 2 Participant Characteristics |
The following three themes emerged to be important challenges in the Assault Center’s daily practice: professional involvement, conflicting goals and a lack of connection. Professional involvement proved to be the most pivotal requirement for efficient and smooth interprofessional collaboration, as mentioned by most participants. Professionals differed in the interest and affinity they had in the tasks that needed to be performed at an assault center. Conflicting goals were mentioned particularly between medical and legal disciplines and were frequently a result of confidentiality issues. A lack of connection between professionals was provoked by the absence of easily accessible personal and face-to-face contact. Participants’ quotations are shown in italics with an interviewee number.
Professional Involvement
Professional involvement refers to people’s professional commitment to and affinity with providing care to victims of sexual violence. Our findings reveal that involvement was experienced as a very important foundation for effective and satisfying interprofessional collaboration. Professional involvement relates to whether caring for victims of sexual violence is one of the core competences of your work. ED physicians and nurses, for instance, have not been specifically appointed to offer care to victims of sexual violence but are regular ED staff who are expected to offer care to any patient, including victims entering the ED through the CSG-GZM. Though all ED physicians and nurses have been trained to deal with victims of sexual violence, some have a greater affinity with providing help to such victims than others, who might feel that dealing with critically ill patients is more in line with their professional calling. This also holds for forensic physicians, who may originally have chosen their profession to perform other forensic tasks, such as post-mortem examinations. And yet, everyone is expected to be prepared to provide appropriate 24/7 care to victims of sexual violence, irrespective of their preferences. On the other hand, representatives had a high affinity with caring for victims of sexual violence and consciously chose to be extensively involved in the CSG-GZM.
Some participants felt that the representatives admittedly expected them to deliver a very high quality of care within their discipline, but that their colleagues could not always live up to these standards. (Q1, Table 3) Care for sexual assault victims requires a specific and sensitive approach that might not correspond with the medical care usually provided by ED staff and forensic physicians. (Q2, Table 3) They expressed more affinity with their customary care. Such customary care made them feel more confident about their skills and expertise. For professionals such as ED personnel and forensic physicians who met a low number of victims, it was difficult to develop appropriate skills and feelings of competence. (Q3, Table 3) Police officers and case managers, on the contrary, felt they were well-equipped for the job and showed great involvement.
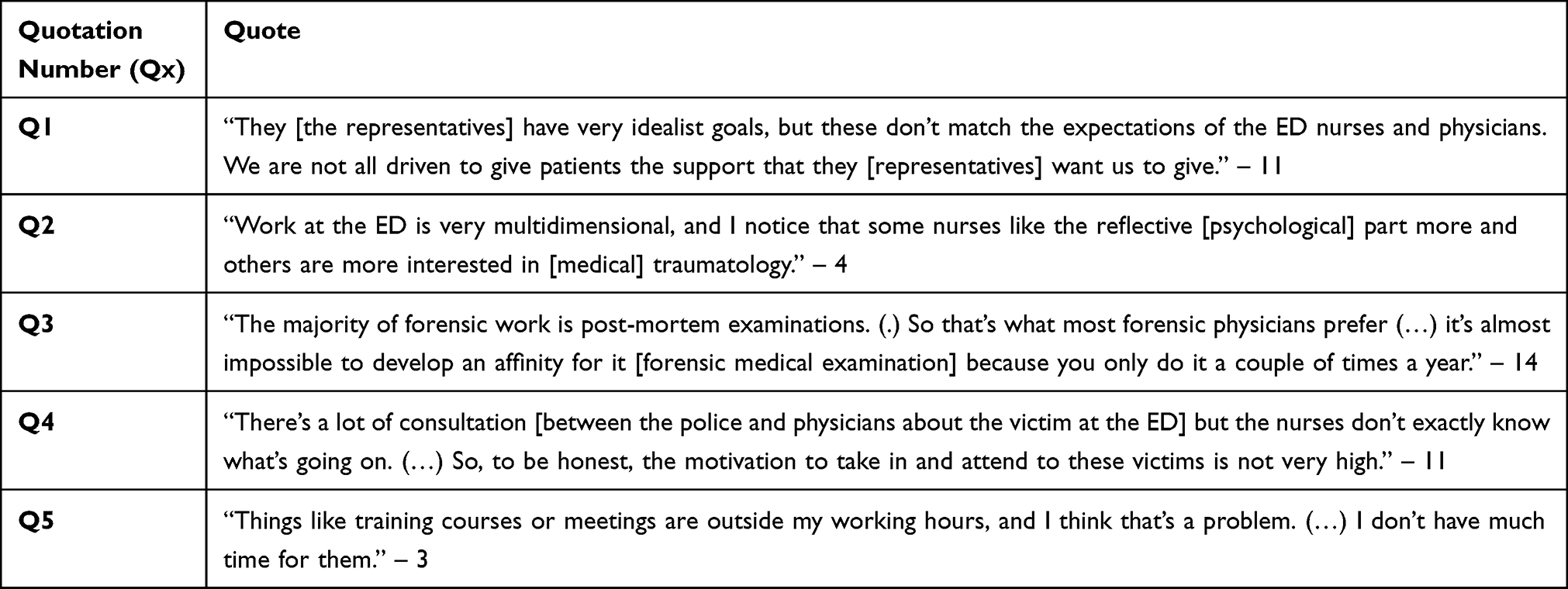 |
Table 3 Theme 1: Professional Involvement |
Most interviewees considered ED nurses to be the least professionally involved in this type of acute care. Their tasks in the care process at the ED were small as ED physicians mostly took the lead, providing them with limited insight into specific characteristics of the care for victims. Feeling excluded from the process lowered their internal motivation (Q4, Table 3).
ED nurses as well as forensic physicians barely attended meetings and education courses, further marginalizing their involvement. Many participants mentioned that time constraints were one of the reasons for low attendance rates, as meetings and training courses could be beyond their work shifts. Some professionals did not want to spend their spare time on education about sexual violence (Q5, Table 3).
Conflicting Goals
Many participants noticed that the goals of one discipline might conflict with those of another. Whereas medical disciplines aimed to improve care for victims and their family and friends, legal disciplines aimed to prosecute perpetrators and act in the interest of social safety. Some participants found it difficult to understand the complicated aspects of legal prosecutions without losing sight of the victims’ medical needs. (Q1, Table 4) They considered that the strong focus on prosecuting the perpetrator was sometimes contrary to their own profession’s aim of providing patient-centered center quality care. Some workers struggled with adhering purely to their own profession’s tasks, sometimes crossing the boundaries of their own profession. (Q2, Table 4) Psychologists mentioned that police rules were perceived to be problematic by other disciplines. (Q3, Table 4) Medical disciplines found it difficult to trust legal disciplines. (Q4, Table 4) Most interviewees mentioned that information sharing was limited due to different confidentiality rules amongst disciplines, particularly between the medical and legal disciplines. Some participants would not share information if they thought this might be harmful to victims (Q5, Table 4).
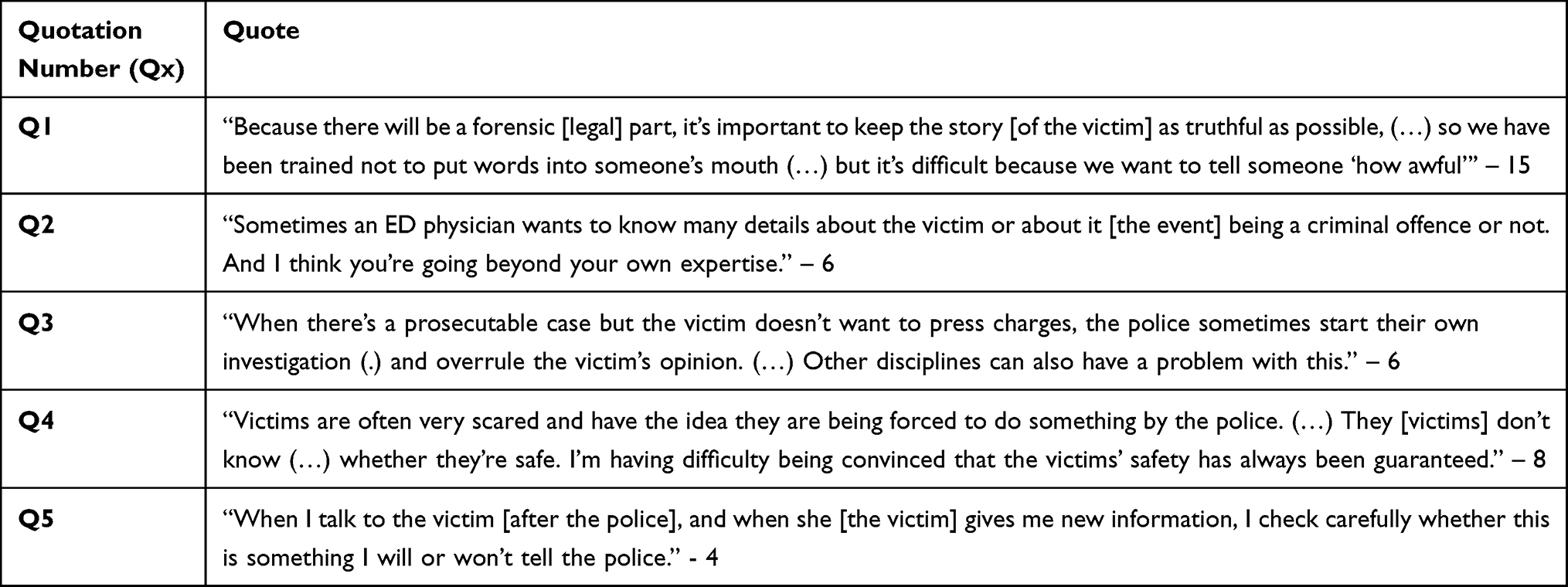 |
Table 4 Theme 2: Conflicting Goals |
Lack of Connection
Interviewees felt that there was a lack of connection between personnel working for the CSG-GZM. To build a better connection, participants wished for more personal and face-to-face contact with their colleagues (Q1, Table 5). The lack of connection limited the opportunity to discuss complex or burdensome cases. Some interviewees mentioned they felt powerless as sexual assault was so widespread and recurrent, which made them realize that their contribution might have limited influence and preventive value. This feeling jeopardized their motivation. (Q2, Table 5) They indicated that, to enhance their engagement and motivation, they wanted more time to share and be supported by colleagues. (Q3, Table 5) Familiarizing with the other professionals could help to overcome misunderstandings and frustrations. (Q4 Table 5) Workers felt that professionals from other disciplines were only partly aware of the worker’s obligations and priorities, which led to frustration. A few participants said they struggled with the lack of reciprocity as, due to confidentiality laws, they received limited information from workers performing tasks before and after them in the caring process. (Q5, Table 5) Participants mentioned that, in order to feel more engaged in the care process as a whole, they would like to receive feedback on the outcome of the care and legal services.
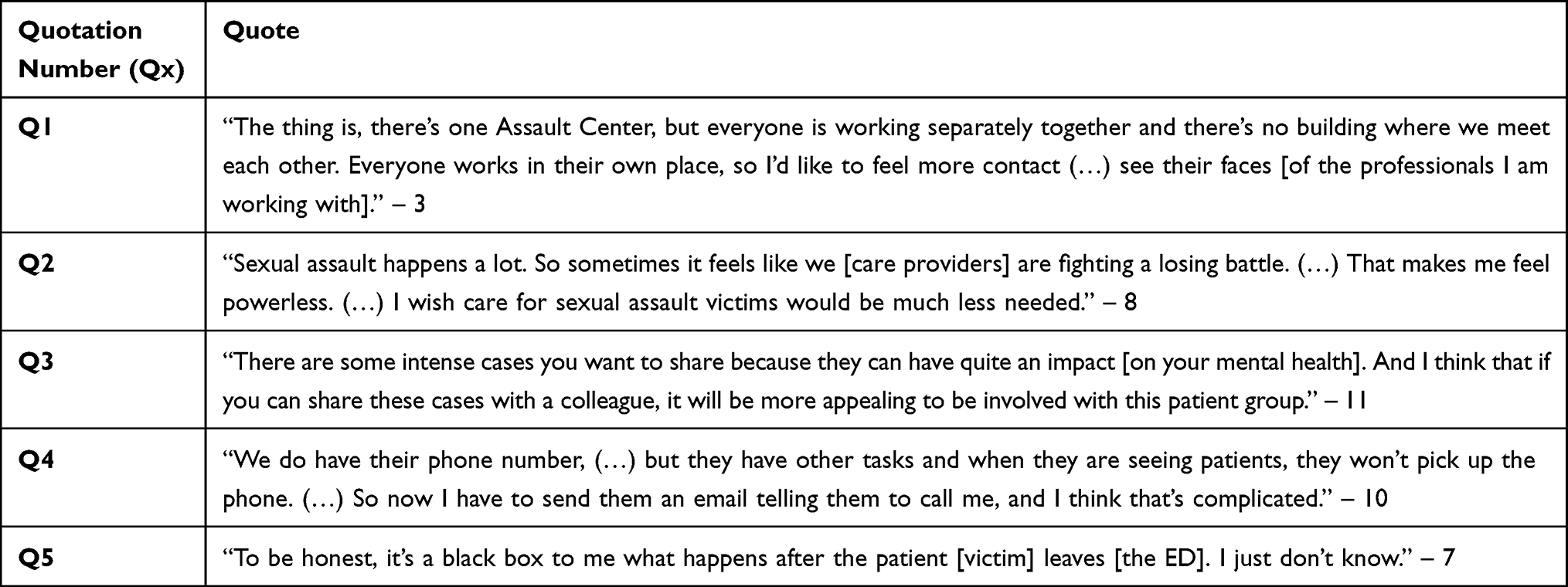 |
Table 5 Theme 3: Lack of Connection |
Discussion
Our study provides important tools to improve interprofessional collaboration at a sexual assault center after its initial set-up. Three themes arose as challenges to interprofessional collaboration, with professional involvement being the biggest challenge. Professional involvement differed substantially among professionals due to discrepancies in motivation and affinity levels. Less affinity was mentioned by ED personnel and forensic physicians. Limited time during working hours and a low caseload further complicated their gaining expertise, affinity and motivation. Conflicting goals and confidentiality issues mostly arose between medical and legal disciplines and were seen as inhibiting factors. Confidentiality requirements hindered information-sharing. Due to a lack of connection, disciplines were only partly aware of the obligations and priorities of other disciplines. Authentic personal contact was considered vital as it gave people the opportunity to share complex and burdensome cases, which ultimately increased their engagement and motivation.
Based on our findings, we identify three requirements for optimal interprofessional collaboration. First, professional involvement is fundamental for successful collaboration. Whereas the representatives of the disciplines are extensively involved, highly motivated, up to date with the protocols, well-informed and have the necessary skills, some other professionals lack personal commitment and affinity with the center and its victims and are poorly informed. In Danish sexual assault centers, the discrepancy between the representatives and their colleagues has also been mentioned.20 They concluded that the representatives are important facilitators by showing characteristics such as leadership, high internal motivation and enthusiasm. Major staff changes affecting these representatives threaten the operation of the center. Our study shows, in addition, that highly motivated, committed and skilled colleagues are vital for successful interprofessional collaboration.
To enable sustainable and long-term interprofessional collaboration, representatives should facilitate collective ownership. The Bronstein model explains that collective ownership is a core component in optimal collaboration: representatives and their colleagues should be equally involved and should feel equally responsible for good quality of care.8 Key components of establishing collective ownership are well-defined and realistic goals, a shared vision and agreed-on mission, involving all professionals in decision-making and having professionals willing to compromise if needed.8 It is important for the team leader of an interprofessional team − and the representatives in our study − to consciously share the leadership role in order to facilitate joint decision-making.21 Empowering the team members is crucial in facilitating shared leadership.21,22 Democratic structures, such as the process meetings in the CSG-GZM, are needed to facilitate such shared decision-making. It is important to constantly involve new members in the interprofessional collaboration. In South Africa, centers with less fluctuations in staff proved to have less conflict.23 When adding new members to the interprofessional collaboration, these members should be immediately involved and educated.
As professionals mentioned they felt more comfortable providing their customary care, gaining individual competency with care for victims of sexual violence will improve professional involvement and cause professionals to feel more secure in performing their tasks. Creating team competency is equally important, as collective competencies seek to leverage the expertise of all team members and to create and achieve mutual goals.24,25 A sufficient caseload is crucial for gaining individual competency. Familiarity with cases can also be achieved collectively by discussing cases in regular meetings, facilitating both individual and collective competency.
Our results confirm that discussing cases under supervision with other colleagues is supportive as caring for victims of sexual assault can be emotionally burdensome. In the previous study about interprofessional collaboration at the same CSG-GZM, professionals felt frustrated or disappointed, for instance, if victims did not accept help or would not report to the police.15 The previous study also described the high emotional cost of caring as the greatest potential threat to collaboration. Out of professional involvement, care providers might experience secondary traumatization or compassion fatigue, which may threaten collaboration by dampening initial enthusiasm, motivation and commitment.15,26,27
Preventing compassion fatigue and ultimately burn-out continues to be crucial in the center’s operation. Whilst our participants still experience sexual violence as an emotionally charged topic with significant impact, leading to feelings of powerlessness, it was less commonly mentioned than in the first study at the CSG-GZM. In particular, participants did not mention that the emotional impact required greater time investment. An explanation might be that, due to the huge annual increase of victims attending the center, more colleagues besides the representatives currently participate in the collaboration, which highlights the importance of establishing continuous collective ownership. Keeping all professionals motivated and professionally involved is a main challenge in an expanding successful center.
Secondly, clarity on the goals of other disciplines is important to avoid conflicts.11,28,29 We found that the ED staff struggles maintaining a balance between medical goals and the legal goal of perpetrator tracing, which is consistent with literature.12 Law disciplines report that medical staff have difficulty remaining objective as this contradicts their compassionate patient-centered attitude, causing role blurring, as medical staff take on the role of being victims’ advocates instead of providing medical care as they would to all other patients.30 Medical and legal goals can lead to opposite attitudes towards victims: either providing help or cautiously taking care not to disturb traces and the legal process. This struggle to prioritize reveals that professionals may be unsure about their own goals as well as unsure about the overarching goal of the center.13,31,32 This uncertainty is partly due to assertions of authority, in which certain professionals may privilege their own goal, thus creating systematic inequality between disciplines.13
Role competition and role blurring proved to be challenges in the collaboration between medical and social disciplines as mentioned in literature. Mainly physicians prove to be too dominant, not always relying on the expertise of social workers in the collaboration.33,34 In our study, the ED nurses in particular felt insecure about what care they were expected to deliver to victims as they felt their role was limited, which lowered their inner motivation. Reciprocity between acute care and follow-up psychosocial care and legal processes is important and will benefit clarity on the roles played by other disciplines. Confidentiality obligations limit such reciprocity. Our previous study about collaboration at the CSG-GZM as well as other literature reported tensions between professionals due to confidentiality obligations.5,10,12,15 As not all professionals value the confidentiality laws in the same manner, this hampers mutual understanding.12,35 Moreover, confidentiality laws are experienced as complex.12 Involvement of all professionals in process meetings and educational courses is important to gain understanding of these confidentiality laws. A higher understanding of the confidentiality laws could aid in lowering the complexity and therefore fear of violating these laws. Confidentiality laws are important to follow, but should not hamper compassionate victim-centered care.
Thirdly, connecting with colleagues is perceived to be essential, mostly to discuss complex cases and to support each other. Personal contact facilitates familiarity, which is especially important for the Dutch centers, in which professionals do not all work under one roof. Being familiar with the other professionals and thus lowering the threshold to discussing burdensome cases will help to lower the likelihood of compassion fatigue. Participants mentioned that connecting with other professionals benefited their internal motivation and sense of engagement, potentially strengthening their professional involvement. Face-to-face communication is a known strong facilitator of interprofessional collaboration and is known to prevent conflicts.5,36,37 It helps to understand the tasks and work context of another discipline and its roles and goals.36 Perhaps the COVID-19 pandemic, introducing many constraints in normal contacts, has served to stress the importance of a good connection with colleagues even more. Although the Covid-19 pandemic served as a large stressor for many interprofessional collaborative teams, this was not mentioned to be an issue at the CSG-GZM. Perhaps partly due to the fact that work location and the amount of face-to-face contact with colleagues did not change significantly as most of the personnel did not work on location prior to the Covid-19 lockdown. Moreover, the CSG-GZM saw a decline in victims presenting at the ED during the Covid lockdowns, similar to other sexual assault centers.38,39 The lower caseload could have possibly made it more manageable to maintain adequate interprofessional collaboration, despite the challenges that the Covid-19 pandemic raised.
Strength and Limitations
This study provides valuable information about interprofessional collaboration in a long-running sexual assault center. Purposive sampling brought together a diverse group of participants, providing information from various perspectives. We carefully followed the COREQ criteria. Checking the content of the interviews by providing a summary to all interviewees enhanced their credibility. The transferability of our study was secured by providing a thorough description of the research setting and individual characters of the CSG-GZM. Dependability was established by using the thematic analysis, in which we carefully analyzed the recorded interviews, and then formed codes, categories and themes, discussed by the research committee. By supplying participants’ quotes, we further ensured the confirmability. However, qualitative research always involves a certain level of interpretation, which is a limitation in this study. Lastly, some participants may not have expressed honest opinions, possibly fearing that other professionals would be able to recognize them once their quotes were published. Despite our statement at the outset of every interview that the data would be processed anonymously, one participant did not want to be quoted. We do not believe that this has affected our findings.
Implications for Practice
All participants felt the need and expressed the will to be more involved. The ED nurses should be the central contacts at the ED for other disciplines and simply be there for the victims, showing empathy and caring. Professional involvement of the ED nurses and forensic physicians will be improved by having them represented at the process meetings.37 Professional involvement could be further enhanced by attending the interprofessional training courses, leveraging collective competence. Every organization should make participation mandatory, rewarding professionals with certification. Interprofessional training should be organized structurally and for free in order to continuously educate workers and new employees.40 Continuing training of professionals must strongly be supported and facilitated at an organizational level. Establishing equal involvement, collective ownership, clear roles and shared goals is important not just in sexual assault centers but in all innovative healthcare organizations. Having more professionals attend interprofessional training courses also facilitates connecting with colleagues, improving familiarity. Interprofessional training courses and process meetings should also focus on creating shared understanding of confidentiality laws.
Supervision should be available for workers to discuss their feelings about intense cases and prevent them from developing burnout.41 There should be set dates for supervision and reflection. Although burnout is not an issue at our center yet, preventing burnout will reduce absenteeism and avoid trained personnel dropout. Practical solutions should be implemented to enable easily accessible contacts, improving accessibility.
Lastly, to further elaborate on our findings, we suggest that the implications for practice should be evaluated. Innovative care projects are work in progress, which makes reflections at regular times necessary.
Conclusion
Discrepancies in professional involvement, conflicting goals between medical and legal disciplines and a lack of connection prove to be the three pivotal challenges to interprofessional collaboration, with a lack of professional involvement being the most considerable drawback. Building collective ownership and equal involvement are crucial. Financial and time support to attend interprofessional training, offering supervision and facilitating connecting with other professionals will enhance interprofessional collaboration, ultimately improving overall care for victims of sexual assault.
Abbreviations
CSGs, The Dutch Centers for Sexual Assault. Sixteen centers throughout the Netherlands providing 24/7 care to victims of sexual assault; CSG-GZM, The Center for Sexual Assault Gelderland-Zuid en -Midden. A center for victims of sexual assault, specifically for victims living in the southern and central part of the Dutch province of Gelderland; ED, Emergency Department; FME, Forensic medical examination; PTSD, Posttraumatic stress disorder.
Acknowledgments
We would like to thank all professionals working for the CSG-GZM who shared their views on interprofessional collaboration.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Garcia-Morena C, Guedes A, Knerr W. Understanding and Addressing Violence Against Women. Geneva: World Health Organization; 2012.
2. De Graaf H, Wijsen C. Seksuele Gezondheid in Nederland [Sexual Health in the Netherlands]. Utrecht: Rutgers; 2017. Dutch.
3. Ranjbar V, Speer SA. Revictimization and recovery from sexual assault: implications for health professionals. Violence Vict. 2013;28(2):274–287. doi:10.1891/0886-6708.11-00144
4. Campbell R. The psychological impact of rape victims. Am Psychol. 2008;63(8):702–717. doi:10.1037/0003-066X.63.8.702
5. Greeson MR, Campbell R. Sexual assault response teams (SARTs): an empirical review of their effectiveness and challenges to successful implementation. Trauma Violence Abuse. 2013;14(2):83–95. doi:10.1177/1524838012470035
6. Hendriks B, Vandenberghe AMA, Peeters L, Roelens K, Keygnaert I. Towards a more integrated and gender-sensitive care delivery for victims of sexual assault: key findings and recommendations from the Belgian sexual assault care centre feasibility study. Int J Equity Health. 2018;17(1):152. doi:10.1186/s12939-018-0864-3
7. Vandenberghe A, Hendriks B, Peeters L, Roelens K, Keygnaert I. Establishing sexual assault care centres in Belgium: health professionals’ role in the patient-centred care for victims of sexual violence. BMC Health Serv Res. 2018;18(1):807. doi:10.1186/s12913-018-3608-6
8. Bronstein R. A model for interdisciplinary collaboration. Soc Work. 2003;48(3):297–306. doi:10.1093/sw/48.3.297
9. Bruner C. Ten Questions and Answers to Help Policy Makers Improve Children’s Services. Washington DC: Education and Human Servides Consortium; 1991.
10. Cole J. Structural, organizational, and interpersonal factors influencing interprofessional collaboration on sexual assault response teams. J Interpers Violence. 2018;33(17):2682–2703. doi:10.1177/0886260516628809
11. Campbell R, Greeson M, Patterson D. Defining the boundaries: how sexual assault nurse examiners (SANEs) balance patient care and law enforcement collaboration. J Forensic Nurs. 2011;7(1):17–26. doi:10.1111/j.1939-3938.2010.01091.x
12. Cole J. Victim confidentiality on Sexual Assault Response Teams (SART). J Interpers Violence. 2011;26(2):360–376. doi:10.1177/0886260510362895
13. Moylan CA, Lindhorst T, Tajima EA. Contested discourses in multidisciplinary Sexual Assault Response Teams (SARTs). J Interpers Violence. 2017;32(1):3–22. doi:10.1177/0886260515585530
14. Cole J, Logan TK. Interprofessional collaboration on Sexual Assault Response Teams (SART): the role of victim alcohol use and a partner--perpetrator. J Interpers Violence. 2010;25(2):336–357. doi:10.1177/0886260509334406
15. Zijlstra E, Lo Fo Wong S, Teerling A, Hutschemaekers G, Lagro-Janssen A. Challenges in interprofessional collaboration: experiences of care providers and policymakers in a newly set-up Dutch assault centre. Scand J Caring Sci. 2018;32(1):138–146. doi:10.1111/scs.12439
16. Braun V, Clarke V. Using thematic analysis in psychology. Qual Res Psychol. 2006;3(2):77–101. doi:10.1191/1478088706qp063oa
17. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
18. Saunders B, Sim J, Kingstone T, et al. Saturation in qualitative research: exploring its conceptualization and operationalization. Qual Quant. 2018;52(4):1893–1907. doi:10.1007/s11135-017-0574-8
19. Corbin JM, Strauss A. Grounded theory research: procedures, canons, and evaluative criteria. Qual Sociol. 1990;13:3–21. doi:10.1007/BF00988593
20. Bramsen R, Elklit A, Nielsen L. A Danish model for treating victims of rape and sexual assault: the multidisciplinary public approach. J Aggress Maltreat Trauma. 2009;18:886–905. doi:10.1080/10926770903291811
21. Smith T, Fowler-Davis S, Nancarrow S, Ariss SMB, Enderby P. Leadership in interprofessional health and social care teams: a literature review. Leadersh Health Serv. 2018;31(4):452–467. doi:10.1108/LHS-06-2016-0026
22. McCray J. Leading interprofessional practice: a conceptual framework to support practitioners in the field of learning disability. J Nurs Manag. 2003;11(6):387–395. doi:10.1046/j.1365-2834.2003.00430.x
23. Vetten L. “It sucks/It’s a wonderful service”: post-rape care and the micro-politics of institutions. Johannesburg: Shukumisa Campaign and ActionAid South Africa; 2015. Available from: https://shukumisa.org.za/wp-content/uploads/2017/09/Thuthuzela-Care-Centres-Shukumisa-Report-2015.pdf.
24. Lingard L. Paradoxical truths and persistent myths: reframing the team competence conversation. J Contin Educ Health Prof. 2016;36(Suppl 1):S19–21. doi:10.1097/CEH.0000000000000078
25. McLaney E, Morassaei S, Hughes L, Davies R, Campbell M, Di Prospero L. A framework for interprofessional team collaboration in a hospital setting: advancing team competencies and behaviours. Healthc Manag Forum. 2022;35(2):112–117. doi:10.1177/08404704211063584
26. Goldblatt H. Caring for abused women: impact on nurses’ professional and personal life experiences. J Adv Nurs. 2009;65(8):1645–1654. doi:10.1111/j.1365-2648.2009.05019.x
27. Canfield J. Secondary traumatization, burnout, and vicarious traumatization. Smith Coll Stud Soc Work. 2005;75(2):81–101. doi:10.1300/J497v75n02_06
28. Blackmore G, Persaud DD. Diagnosing and improving functioning in interdisciplinary health care teams. Health Care Manag. 2012;31(3):195–207. doi:10.1097/HCM.0b013e3182619d48
29. Supper I, Catala O, Lustman M, Chemla C, Bourgueil Y, Letrilliart L. Interprofessional collaboration in primary health care: a review of facilitators and barriers perceived by involved actors. J Public Health. 2015;37(4):716–727.
30. Canaff R. Nobility in objectivity: a prosecutor’s case for neutrality in forensic nursing. J Forensic Nurs. 2009;5(2):89–96. doi:10.1111/j.1939-3938.2009.01039.x
31. Greeson MR, Campbell R. Coordinated community efforts to respond to sexual assault: a national study of sexual assault response team implementation. J Interpers Violence. 2015;30(14):2470–2487. doi:10.1177/0886260514553119
32. Clark MR, Nackerud L, Larrison CR, Neiderman R. Assessing the congruence between conceptualization and implementation of the collaborative objective in a child sexual abuse response team. J Child Sex Abus. 1998;7(2):47–63. doi:10.1300/J070v07n02_03
33. Abramson JS, Mizrahi T. When social workers and physicians collaborate: positive and negative interdisciplinary experiences. Soc Work. 1996;41(3):270–281.
34. Atwal A, Caldwell K. Do all health and social care professionals interact equally: a study of interactions in multidisciplinary teams in the United Kingdom. Scand J Caring Sci. 2005;19(3):268–273. doi:10.1111/j.1471-6712.2005.00338.x
35. Hall P. Interprofessional teamwork: professional cultures as barriers. J Interprof Care. 2005;19:188–196. doi:10.1080/13561820500081745
36. Sangaleti C, Schveitzer MC, Peduzzi M, Zoboli E, Soares CB. Experiences and shared meaning of teamwork and interprofessional collaboration among health care professionals in primary health care settings: a systematic review. JBI Database System Rev Implement Rep. 2017;15(11):2723–2788. doi:10.11124/JBISRIR-2016-003016
37. Cole J, Logan TK. Negotiating the challenges of multidisciplinary responses to sexual assault victims: sexual assault nurse examiner and victim advocacy programs. Res Nurs Health. 2008;31(1):76–85. doi:10.1002/nur.20234
38. Kaswa R. The impact of the COVID-19 pandemic on healthcare service access for the victims of sexual assault. S Afr Fam Pract. 2021;63(1):e1–e4. doi:10.4102/safp.v63i1.5344
39. Muldoon KA, Denize KM, Talarico R, et al. COVID-19 pandemic and violence: rising risks and decreasing urgent care-seeking for sexual assault and domestic violence survivors. BMC Med. 2021;19(1):20. doi:10.1186/s12916-020-01897-z
40. Martin SL, Young SK, Billings DL, Bross CC. Health care-based interventions for women who have experienced sexual violence: a review of the literature. Trauma Violence Abuse. 2007;8(1):3–18. doi:10.1177/1524838006296746
41. Geoffrion S, Morselli C, Guay S. Rethinking compassion fatigue through the lens of professional identity: the case of child-protection workers. Trauma Violence Abuse. 2016;17(3):270–283. doi:10.1177/1524838015584362
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Scoping Review of Qualitative Evaluation Methods for Mono- and Interprofessional Consultations – What Needs to Be Known and Considered?
Bossert J, Dürsch H, Korus B, Boltenhagen U, Stie M, Klafke N
Nursing: Research and Reviews 2024, 14:103-115
Published Date: 27 June 2024