Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Video-Based Skill Assessment for Postoperative T-Tube Nursing is Associated with Improved Clinical Outcomes and Patient Satisfaction: A Single-Center Retrospective Comparative Study
Received 18 December 2025
Accepted for publication 17 March 2026
Published 7 April 2026 Volume 2026:19 590108
DOI https://doi.org/10.2147/JMDH.S590108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Charles V Pollack
Bo Zhang,1 Yanran Li,2 Hui Zhao3
1Department of Pancreaticobiliary Surgery, Xingtai People’s Hospital, Xingtai, 054001, People’s Republic of China; 2Department of Preventive Healthcare, Xingtai People’s Hospital, Xingtai, 054001, People’s Republic of China; 3Department of Nursing, Xingtai People’s Hospital, Xingtai, 054001, People’s Republic of China
Correspondence: Hui Zhao, Department of Nursing, Xingtai People’s Hospital, No. 16 Hongxing Street, Xingtai, 054001, People’s Republic of China, Email [email protected]
Background: Ensuring standardized competencies in T-tube management is pivotal for optimizing recovery and minimizing postoperative morbidity. Despite its growing use in clinical training, the impact of structured video-based skill assessments on nursing practice has not been clearly defined.
Methods: We conducted a retrospective comparative analysis at Xingtai People’s Hospital, enrolling adult inpatients who underwent T-tube placement between January 2019 and December 2023. Participants were stratified according to whether their primary nurse had completed a formal video-based assessment of T-tube care. Primary endpoints were T-tube retention time distribution and length of postoperative hospital stay. Tube-related complications were analyzed as secondary/exploratory outcomes. Secondary endpoints included patient satisfaction, internal nursing quality indicators, and nurse-reported confidence. Intergroup comparisons were performed using independent-sample t tests and chi-square tests, with significance set at P < 0.05.
Results: Among 200 eligible patients, 80 were retrospectively classified into the video-based assessment (VBA) group and 120 into the traditional clinical assessment (TCA) group according to the credentialing status of the primary nurse responsible for T-tube care at the time care was delivered. The VBA group exhibited a more concentrated retention time distribution (42.1 ± 3.6 vs 44.8 ± 6.2 days; P < 0.001) and a shorter postoperative hospital stay (5.8 ± 1.2 vs 6.2 ± 1.5 days; P = 0.02). Tube-related complications were numerically fewer in the VBA group (6.3% vs 10.8%), with significantly lower infection rate (2/80 [2.5%] vs 8/120 [6.7%]; Fisher’s exact test, P = 0.04), while rates of accidental dislodgement and blockage did not differ significantly. Patient satisfaction scores and internal nursing quality ratings were consistently superior in the VBA group across all assessed domains (all P < 0.01).
Conclusion: Implementation of structured video-based nursing assessments was associated with more standardized T-tube retention time, shorter hospitalization, a lower observed rate of local infection and enhanced patient-reported and nursing quality outcomes. Given the retrospective observational design and routine staffing-based (non-random) nurse assignment, these findings should be interpreted as associations rather than causal effects. Complication endpoints were infrequent, and safety-related differences require confirmation in larger prospective studies. Integrating video-based evaluation into routine nursing competency frameworks may represent a scalable quality-assurance strategy for postoperative T-tube management and warrants confirmation in prospective, preferably randomized or mixed-method, studies.
Keywords: video-based assessment, nursing education, T-tube care, postoperative outcomes, patient satisfaction, retrospective study
Introduction
T-tube placement remains a widely employed surgical technique for biliary drainage following common bile duct exploration, particularly in high-volume centers across East Asia. While the surgical procedure is generally standardized, the success of postoperative recovery is often contingent upon meticulous nursing care, especially in the management of the T-tube during the inpatient period.1,2 Complications such as local infection, tube dislodgement, and obstruction, although not uncommon, can frequently be attributed to suboptimal handling, delayed recognition of warning signs, or inconsistent adherence to nursing protocols.3,4 In this context, the quality of nursing care exerts a direct influence on both clinical outcomes and patient-reported satisfaction.
Efforts to improve nursing care for high-risk procedures like T-tube management have traditionally focused on in-service training and protocol dissemination. However, existing educational practices—often reliant on passive instruction or brief skill demonstrations—may fall short in ensuring procedural consistency across nursing staff with varying levels of clinical experience.5,6 Moreover, conventional assessment methods tend to emphasize knowledge recall rather than actual operational capability, leaving a gap between training and bedside performance.7–9 In Xingtai Peoples’ Hospital where nurse turnover and cross-department assignments are common, this discrepancy poses a critical challenge to maintaining uniform care quality.
In recent years, structured video-based skill assessment models have been introduced in various domains of healthcare training, offering standardized, repeatable, and visually demonstrative content that may enhance procedural accuracy and retention.10,11 Such approaches allow for centralized evaluation, consistent criteria across evaluators, and objective documentation of competencies.12,13 In nursing education, video assessment has been explored in simulation settings, yet its real-world integration into institutional quality assurance frameworks remains limited.14 Particularly in the context of high-acuity postoperative care, the extent to which this modality influences measurable patient outcomes has not been systematically investigated.11,14
Against this backdrop, Xingtai Peoples’ Hospital implemented a video-based nursing assessment system targeting key procedures including T-Tube care. The initiative aimed to improve nursing competency through structured visual instruction and individualized feedback, with certification required prior to independent clinical deployment. This policy shift provided a unique opportunity to evaluate whether such assessments, beyond educational value, could translate into tangible improvements in patient recovery and care experience.15–17 Importantly, the implementation occurred as part of a hospital-wide quality reform, not an experimental trial, offering a pragmatic context for examining effectiveness in routine practice.18
To date, limited empirical evidence exists regarding the downstream clinical impact of structured nursing assessments, particularly in surgical recovery pathways where nursing actions are temporally and functionally proximal to outcome generation.17,19 Therefore, this study was designed to assess whether patients who received care from video assessed nurses experienced better clinical outcomes and satisfaction following T-Tube surgery compared to those managed by traditionally evaluated staff. By leveraging a real-world cohort from a high-volume hospital, the study aims to inform institutional training strategies and contribute evidence toward optimizing nursing evaluation models in procedure-sensitive care domains.16,19
Methods
Study Design and Context
This retrospective observational study was conducted at Xingtai People’s Hospital in China and included hospitalized patients who underwent T-tube surgery with postoperative nursing care between January 2019 and December 2023. The primary objective was to evaluate whether patients whose postoperative care was delivered by nurses who had successfully completed a structured video-based skill assessment (video-based assessment (VBA) group, VBA) experienced different outcomes compared with those managed by nurses evaluated through conventional methods (traditional clinical assessment, TCA).
The hospital-wide video-based nursing assessment system was initially piloted in 2017 as part of a broader initiative to standardize procedural nursing competencies, particularly in T-tube management. For the present analysis, consecutive patients treated both before and after implementation of this quality-assurance program were included. Importantly, no changes were made to surgical or clinical care protocols during the study period. Ethical approval for this retrospective observational study was obtained from the Institutional Review Board of Xingtai People’s Hospital (Approval No. AF/SS-07/02.0), which waived the requirement for informed consent because the study used anonymized routinely collected data.
Patient Inclusion and Nursing Assignment
Adult inpatients who underwent T-tube placement and received postoperative nursing care at Xingtai People’s Hospital between January 2019 and December 2023 were retrospectively screened for eligibility. Cases were identified through the institutional electronic medical record system using standardized procedural codes for biliary drainage surgery. Patients were eligible if they were 18 years of age or older, had complete perioperative and follow-up documentation, and received at least 48 hours of in-hospital nursing care following surgery. Exclusion criteria included discharge within 48 hours postoperatively, transfer to another facility before T-tube removal, or missing data on primary outcomes or satisfaction measures.
A total of 200 patients met these criteria and were included in the analysis. Of these, 80 patients received postoperative care from nurses who had completed the certified video-based assessment module (VBA) at the time of care, whereas 120 were cared for by nurses who had not (TCA); patients were therefore classified retrospectively according to the credentialing status of the primary nurse responsible for T-tube care. Group classification was determined retrospectively based on the qualifications of the primary nurse providing postoperative care. Patients in the VBA group were cared for exclusively by nurses who had successfully completed the hospital’s certified video-based assessment module in T-tube management prior to the clinical encounter, whereas those in the TCA group were managed by nurses who had not undergone such training. Nursing assignments followed routine hospital shift rotations and were not influenced by patient characteristics or preferences; however, this routine staffing-based assignment does not constitute randomization. Importantly, patients were unaware of their nurse’s assessment status, and no crossover of nursing staff occurred between groups during the inpatient stay. Across the overall study period, some nurses may have transitioned from TCA to VBA after completing credentialing; however, group assignment was defined by each nurse’s credentialing status at the time each patient received care.
Nursing Assessment Model and Group Definition
In response to institutional quality-improvement mandates and aligned with national recommendations for standardized technical skill evaluation in nursing practice, Xingtai People’s Hospital formally rolled out a video-based skill assessment program in January 2022, following an earlier pilot phase initiated in 2017. This initiative aimed to enhance procedural consistency in critical nursing tasks, including T-tube management, which has been identified by both national nursing guidelines and hospital-level competency frameworks as a high-risk practice requiring specialized training and evaluation.
The video-based assessment protocol was first piloted in 2017 as a structured alternative to traditional face-to-face evaluations. The program followed a standardized sequence consisting of didactic instruction, guided practice, self-recorded demonstrations, and secure video submission. Each nurse was required to record and submit procedures for 23 designated core skills, which were independently reviewed by head nurses designated for each domain. To ensure inter-rater reliability, one to three “standard nurses” were appointed per skill to serve as benchmarks, and evaluators adhered to a unified scoring rubric. Key assessment domains included procedural accuracy, aseptic technique, patient communication, and safe instrument handling. All evaluations were anonymized, and asynchronous review minimized bias while allowing temporal flexibility. More than 5000 video submissions were collected during the implementation period, reflecting a high degree of reproducibility and fidelity.
The assessment module was developed internally by a multidisciplinary task force of senior surgical nurses, clinical educators, and quality assurance officers. The curriculum incorporated procedural demonstrations, safety checkpoints, and complication scenarios. Nurses were required to pass both a knowledge-based examination and a practical video assessment before being certified to independently provide postoperative T-tube care. Only those who successfully passed were categorized into the VBA group.
For this analysis, patient group assignment was defined exclusively by the credentialing status of the primary nurse responsible for most T-tube care during hospitalization. No crossover of staff occurred, and no patient received mixed care. Nurses who had not yet completed the certification process during the study period, or who were practicing prior to the hospital-wide rollout, provided care to patients in the TCA.
Implementation timeline. The video-based assessment (VBA) pathway was initially piloted in 2017 as a quality-improvement initiative within the department, with limited use during the early implementation phase. Formal departmental rollout began in January 2022, when VBA credentialing became more widely available as part of routine competency assessment for postoperative T-tube nursing care. Throughout the study period, patients were classified according to the credentialing status of the primary nurse responsible for T-tube care at the time care was delivered, rather than by calendar period alone. During transitional periods, nurses who had not yet completed VBA credentialing were classified as TCA, whereas nurses who had completed VBA credentialing were classified as VBA. Nurse-level structure. During the study period, patient care in the analytic cohort was delivered by 18 nurses in the VBA pathway and 24 nurses in the TCA pathway. The median number of study patients per nurse was 4 (IQR, 3–6) in the VBA pathway and 4 (IQR, 3–5) in the TCA pathway. These data are reported to provide context regarding the potential for within-nurse clustering of patient outcomes.
Traditional Clinical Assessment (TCA)
Traditional clinical assessment (TCA). In the TCA pathway, competency in postoperative T-tube nursing care was evaluated through routine bedside observation and sign-off during clinical shifts. Training consisted of standard ward orientation and bedside teaching, including review of the T-tube care protocol, demonstration by senior staff, and supervised practice during routine patient care. Assessment was typically conducted in person by the ward educator and/or a senior nurse (eg, charge nurse or nurse manager) who observed the nurse performing key steps of T-tube management at the bedside. Performance was documented as a competency sign-off in the ward training record (pass/fail or brief checklist-based confirmation), and feedback was provided verbally at the time of observation. When performance was judged insufficient, additional supervised practice was recommended and reassessment was performed according to routine departmental practice. A structured rubric, anonymized scoring, and asynchronous review were not routinely used in the TCA pathway. A side-by-side comparison of the VBA and TCA pathways (training content, assessment format, scoring criteria, assessor identity/training, timing/frequency, documentation, and remediation/retest policies) is provided in Table S1. Group assignment reconstruction and exclusions. For patients whose VBA/TCA group assignment was not explicitly recorded in the analytic dataset, we attempted to reconstruct group status where feasible by cross-referencing ward staffing records and the credentialing roster (ie, whether the primary nurse responsible for T-tube care had completed VBA credentialing at the time of care). Patients whose group status could not be reliably reconstructed were retained as “unknown” for reporting purposes and were excluded from the primary comparative analyses. Reasons for exclusion were prespecified (eg, early discharge, incomplete documentation, and missing satisfaction data) and are reported by group where available (Table S2).
Clinical Outcomes and Scoring Instruments
Clinical outcomes were evaluated using a combination of objective perioperative measures and structured subjective assessments. The primary endpoints included the time to T-tube removal—defined as the interval between surgery and documented removal by the inpatient care team. Optimal outcomes were characterized by removal clustering within 42–45 days, which reflects adherence to standardized discharge guidance and precision in postoperative follow-up. The second primary outcome was total postoperative length of hospital stay. Tube-related complications, including local infection at the insertion site, accidental dislodgement, and lumen obstruction, were systematically recorded based on physician documentation and nursing reports. Local infection was defined as clinically documented erythema, purulent discharge, or physician-diagnosed insertion-site infection requiring local treatment or antibiotics, as recorded in the medical or nursing record. Each event was classified according to institutional adverse event criteria and independently validated by a secondary reviewer to ensure consistency.
Secondary outcomes comprised both patient-reported and nurse-reported assessments. Patient satisfaction was measured prior to discharge using a institutional routine questionnaire with acceptable internal consistency in the current cohort covering four domains (communication, timeliness of care, emotional support, and overall satisfaction), each rated on a 5-point Likert scale ranging from 1 (very dissatisfied) to 5 (very satisfied). In addition, overall nursing care quality was quantified with a 10-point numeric rating scale, with higher values denoting superior perceived competence and responsiveness. Nurse self-reported confidence was collected anonymously after each care episode using a 5-point ordinal scale. All survey data and outcome entries were systematically reviewed for completeness before inclusion in the final dataset.
Clinical data were extracted from the electronic medical record system using a prespecified case report form. Two trained investigators independently abstracted key variables and outcomes, and discrepancies were resolved by discussion with a third senior reviewer. A random sample of records was cross-checked to ensure consistent application of variable definitions and outcome ascertainment.
Patient satisfaction questionnaire. Patient-reported satisfaction was assessed using the hospital’s routine inpatient nursing satisfaction questionnaire, a brief multidimensional instrument administered at discharge. The questionnaire used a 5-point Likert scale and covered communication, timeliness of care, emotional support, and overall satisfaction. The instrument was developed in Chinese for routine local quality-monitoring purposes; therefore, no additional cultural or linguistic translation was required for the present study. Before implementation, item content was reviewed by senior nursing educators and quality-management staff to ensure relevance to postoperative nursing care. In the current cohort, the internal consistency of the patient satisfaction scale was acceptable, with a Cronbach’s alpha of 0.88. Because this instrument was designed for institutional quality monitoring rather than as a formally standardized research scale, findings derived from it should be interpreted accordingly. Nurse confidence was assessed using a pragmatic single-item measure rather than a validated multi-item self-efficacy scale; therefore, measurement precision may be limited and this finding should be interpreted as supportive. Future studies should consider validated multi-item self-efficacy instruments.
Internal nursing quality ratings. Internal nursing quality was evaluated using a structured ward audit tool covering aseptic technique, tube fixation, and documentation quality, each scored on a 10-point scale, with higher scores indicating better performance. Ratings were performed by two senior nursing quality-control reviewers who received standardized orientation to the scoring criteria before data collection. Audits were completed during routine inpatient care review within the index hospitalization. To assess scoring consistency, a random subset of records was independently rated by both reviewers, yielding acceptable inter-rater reliability (intraclass correlation coefficient, ICC = 0.84). Because the scoring process was embedded in routine departmental quality monitoring, reviewers were not fully blinded to the assessment pathway.
Nurse-reported confidence. Nurse self-confidence in T-tube management was assessed using a single-item 5-point Likert question embedded in the routine ward quality-monitoring workflow (1 = not confident at all; 5 = very confident). This pragmatic single-item approach was chosen to minimize respondent burden in routine clinical practice; however, it is not a formally validated multi-item self-efficacy scale.
Outcomes
Outcomes. The primary outcomes were prespecified as recovery-related clinical endpoints, namely T-tube retention time and postoperative length of stay, because these measures most directly reflected procedural consistency and discharge coordination in routine postoperative T-tube care. These endpoints were considered hypothesis-confirming outcomes. Secondary outcomes included tube-related complications (local infection, accidental tube dislodgement, and tube blockage), patient-reported satisfaction domains, internally audited nursing quality scores, and nurse self-confidence in T-tube management. Given the observational quality-improvement context and the low frequency of some complication events, secondary outcomes were interpreted as supportive or exploratory rather than confirmatory.
Statistical Analysis
All statistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY). Continuous variables were summarized as means with standard deviations and compared between groups using independent t-tests. Categorical variables were expressed as counts with percentages and analyzed with the chi-square or Fisher’s exact test, as appropriate. No imputation was performed for missing data; patients lacking outcome information were excluded from the corresponding analyses.
The primary analyses compared recovery-related endpoints and satisfaction measures between the VBA group and the TCA. To mitigate confounding inherent to the retrospective design and non-random nurse assignment, we additionally performed multivariable regression analyses for prespecified outcomes. All adjusted models included baseline covariates selected a priori based on clinical relevance and Table 1 availability (eg, age, sex, key comorbidities, and perioperative factors), and calendar time was additionally considered to account for potential temporal trends across the study period. Nurse assignment followed routine staffing schedules and was not influenced by patient-specific clinical factors; however, this routine staffing-based assignment does not constitute randomization. As a sensitivity analysis for unmeasured confounding, we calculated E-values for key binary outcomes to quantify the minimum strength of association that an unmeasured confounder would need to have with both exposure (VBA care) and the outcome, beyond measured covariates, to fully explain away the observed association.
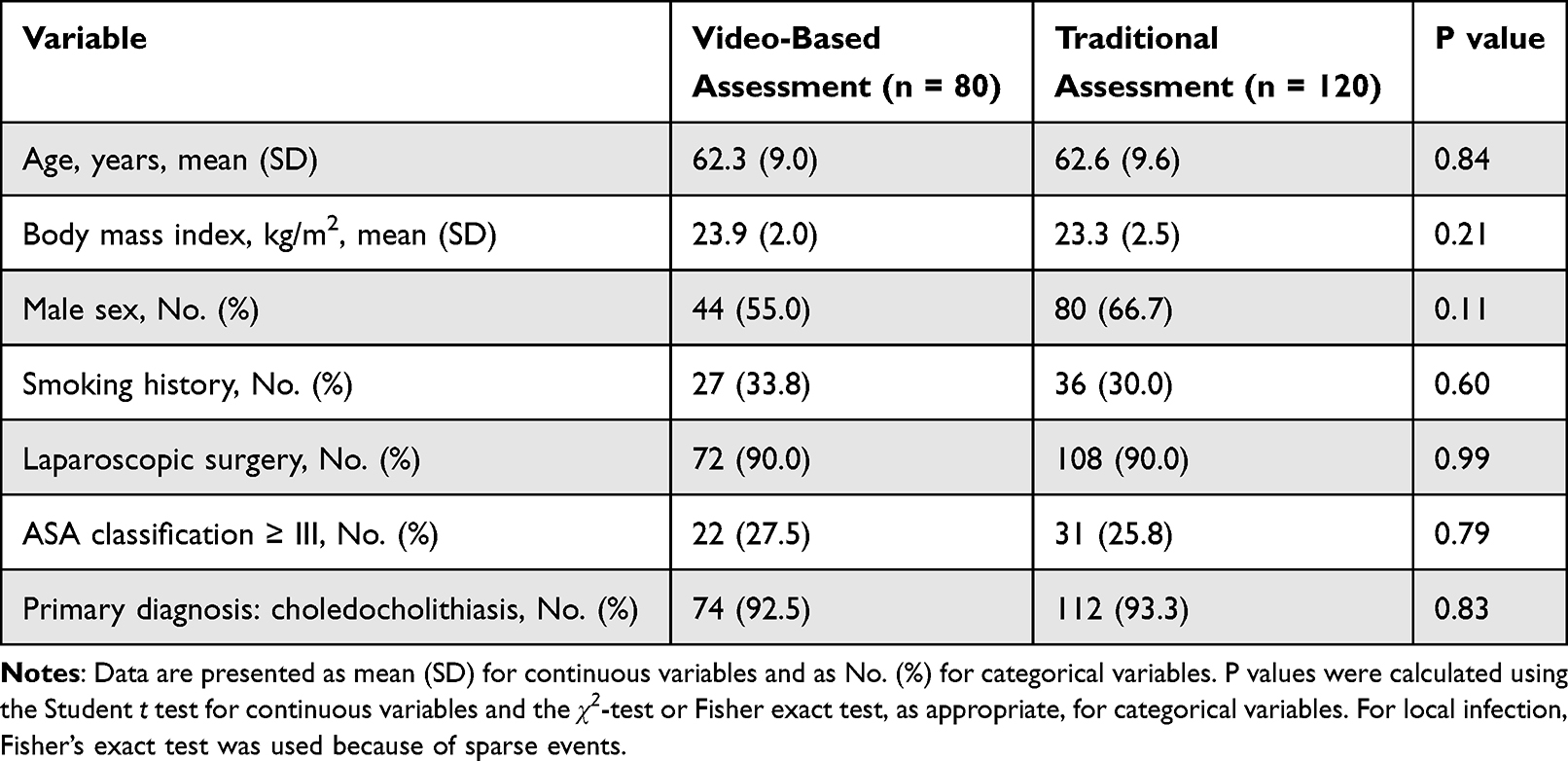 |
Table 1 Baseline Characteristics of Patients in the Video-Based and TCA Groups |
To assess the adequacy of the sample size, we focused on the precision of effect estimates rather than post hoc power calculations. For continuous endpoints such as time to T-tube removal and length of postoperative stay, the observed between-group differences were estimated with relatively narrow 95% confidence intervals, supporting reasonable precision for these recovery-related outcomes. In contrast, tube-related complications were infrequent in both groups (eg, 2.5% vs 6.7% for local infection), and estimates for several safety-related endpoints (including dislodgement, blockage, and overall complications) were therefore imprecise, as reflected by wider confidence intervals. Accordingly, the absence of statistically significant differences for some complication outcomes should be interpreted cautiously and should not be taken to establish safety equivalence; larger cohorts and prospective studies designed around complication endpoints are needed for more definitive safety inference.
This observational study was reported with reference to the STROBE recommendations, with additional attention to transparency relevant to quality-improvement implementation (Table S3). To address multiplicity across multiple secondary/exploratory endpoints, we applied false discovery rate (FDR) control using the Benjamini–Hochberg procedure within prespecified outcome families (patient satisfaction domains; tube-related complication endpoints). Both unadjusted P values and FDR-adjusted q values are reported, and findings are interpreted accordingly. Primary (hypothesis-confirming) outcomes were not subjected to multiplicity correction.
Results
Patient Characteristics and Group Allocation
A total of 234 patients who underwent T-tube surgery at Xingtai People’s Hospital between January 2019 and December 2023 were screened for eligibility. Thirty-four were excluded due to early discharge within 48 hours (n = 14), incomplete documentation (n = 12), or absence of satisfaction data (n = 8). The final analytic cohort comprised 200 patients, with 80 retrospectively classified into the video-based assessment (VBA) group and 120 into the traditional clinical assessment according to the credentialing status of the primary nurse providing postoperative care at the time care was delivered (Figure 1). Among the excluded patients, group status was reconstructed where feasible; the distribution of exclusions by group and by reason is summarized in Table S2.
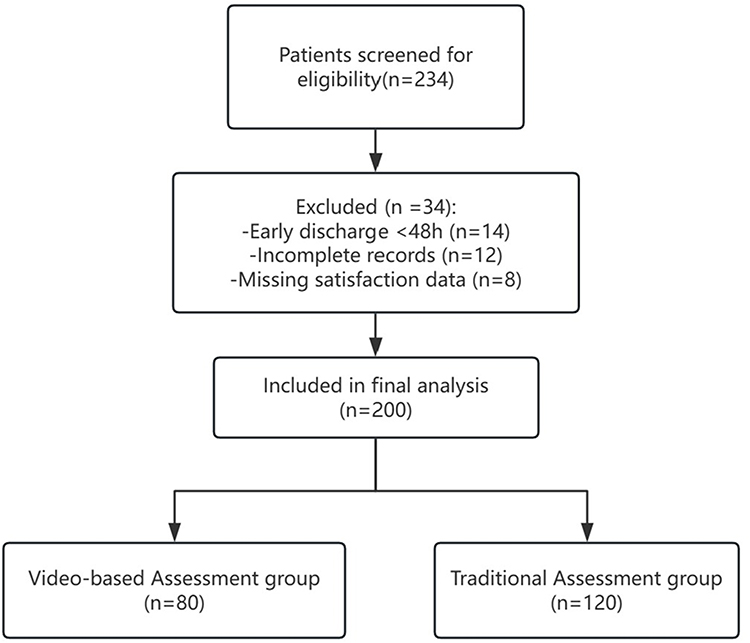 |
Figure 1 Patient enrollment and group allocation flowchart. A total of 234 patients who underwent T-tube surgery between January 2019 and December 2023 were retrospectively screened for eligibility. After excluding 34 individuals due to early discharge within 48 hours (n = 14), incomplete clinical documentation (n = 12), or missing patient satisfaction assessments (n = 8), 200 patients were included in the final analysis. Based on the credentialing status of the primary postoperative nurse at the time of care, 80 patients were retrospectively classified into the video-based assessment (VBA) group and 120 into the traditional clinical assessment (TCA) group. At the nurse level, 18 nurses contributed to the VBA group and 24 to the TCA group. The median number of study patients per nurse was 4 (IQR, 3–6) in the VBA group and 4 (IQR, 3–5) in the TCA group. |
As detailed in Table 1, demographic and clinical baseline characteristics were well balanced between groups. The mean age was 62.3 ± 9.0 years in the video-based assessment (VBA) group and 62.6 ± 9.6 years in the traditional clinical assessment group (P = 0.84). Men accounted for 55.0% and 66.7% of each cohort, respectively (P = 0.11). Mean body mass index was 23.9 ± 2.0 kg/m2 versus 23.3 ± 2.5 kg/m2 (P = 0.21). Current smoking was reported in 33.8% of the video-based assessment (VBA) group and 30.0% of the traditional clinical assessment (P = 0.60).
Surgical characteristics were likewise comparable: laparoscopic procedures predominated in both groups, each at 90.0% (P = 0.99). Patients with an American Society of Anesthesiologists (ASA) classification of grade III or higher represented 27.5% in the video-based assessment (VBA) group and 25.8% in the traditional clinical assessment (P = 0.79). The principal diagnosis was choledocholithiasis, documented in 92.5% and 93.3% of patients, respectively (P = 0.83).
Collectively, these findings confirm the absence of significant baseline imbalances, thereby strengthening the validity of subsequent comparisons in postoperative outcomes.
Primary Clinical Outcomes
As prespecified primary (hypothesis-confirming) outcomes, recovery-related endpoints were compared first between groups. The mean retention time of the T-tube was significantly shorter in the VBA group (42.1 ± 3.6 days) compared with the TCA group (44.8 ± 6.2 days; P < 0.001), and this association remained after multivariable adjustment (adjusted β = −2.32 days; 95% CI, −3.08 to −1.56). Similarly, postoperative hospital stay was modestly shorter in the VBA group (5.8 ± 1.2 vs 6.2 ± 1.5 days; P = 0.02), with a consistent adjusted estimate (adjusted β = −0.34 days; 95% CI, −0.63 to −0.05).
Tube-related complications were infrequent in both groups. Adjusted effect estimates with 95% confidence intervals for all binary outcomes are reported in Table 2. Local infection was observed less often in the VBA group, and a penalized logistic model was used to address sparse events (adjusted aOR = 0.09; 95% CI, 0.01 to 0.72). An E-value sensitivity analysis for local infection suggested that a very strong unmeasured confounder would be required to fully explain away the observed association (E-value = 21.7; E-value for the upper confidence limit = 2.12). Given the low event rates for dislodgement, blockage, and overall tube-related complications, confidence intervals were wide for several safety-related endpoints; therefore, non-significant findings should be interpreted cautiously and should not be interpreted as establishing safety equivalence.
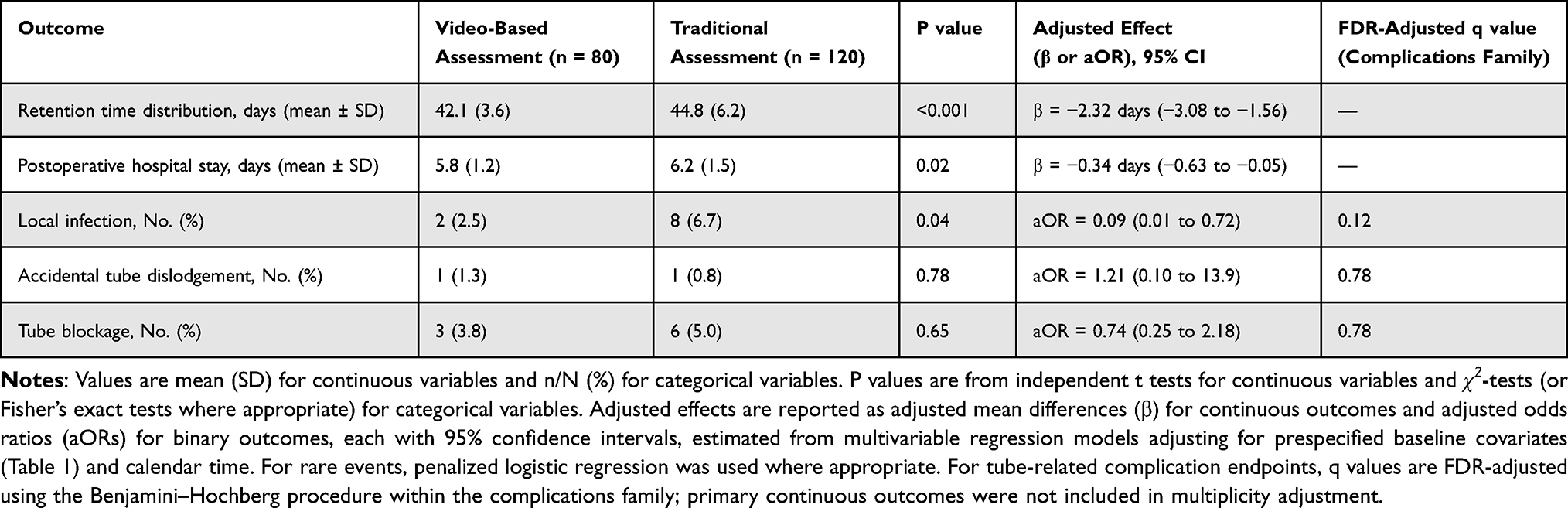 |
Table 2 Postoperative Outcomes |
Although the overall complication rate showed only a nonsignificant trend favoring the video-based assessment (VBA) group, the lower observed infection rate supports the potential clinical value of structured video-based skill assessment for nursing practice.
Secondary Outcomes
Secondary outcomes were analyzed as supportive or exploratory endpoints, including complication profiles, patient-reported satisfaction, and nursing quality indicators. Communication with nursing staff was rated 4.6 ± 0.5 compared with 4.2 ± 0.6 in the traditional clinical assessment (P < 0.001). Similar advantages were observed for timeliness of care (4.6 ± 0.4 vs 4.0 ± 0.6; P < 0.001) and emotional support (4.3 ± 0.5 vs 3.9 ± 0.7; P = 0.002). Overall satisfaction was also significantly higher in the video-based assessment (VBA) group (4.6 ± 0.4 vs 4.2 ± 0.6; P < 0.001).
Internally audited performance scores mirrored these findings. The mean nursing quality rating was 8.6 ± 0.9 in the video-based assessment (VBA) group, compared with 7.9 ± 1.1 in the traditional clinical assessment (P < 0.001). In parallel, nurses in the VBA pathway reported greater self-confidence in their T-tube management skills (4.4 ± 0.6 vs 3.8 ± 0.7; P < 0.001). Confidence responses were available for all nurses included in the analysis (VBA: 80/80; TCA: 120/120), with no missing data.
Collectively, these results suggest that structured video-based evaluation not only enhances patient-perceived satisfaction but also reinforces objective indicators of nursing quality and professional confidence. Given the low event rates for dislodgement, blockage, and overall tube-related complications, these null findings should be interpreted cautiously because the study may be underpowered to detect modest but clinically important differences. Sensitivity analyses for missing satisfaction data yielded directionally consistent conclusions under extreme-case assumptions (best–worst and worst–best scenarios), suggesting that the observed between-group differences in satisfaction were not solely driven by missingness (Table S4). Across secondary/exploratory endpoints, FDR adjustment was applied within prespecified outcome families (Tables 2–3). Results were generally consistent after FDR correction; where q values exceeded 0.05, findings were interpreted as exploratory signals rather than hypothesis-confirming effects.
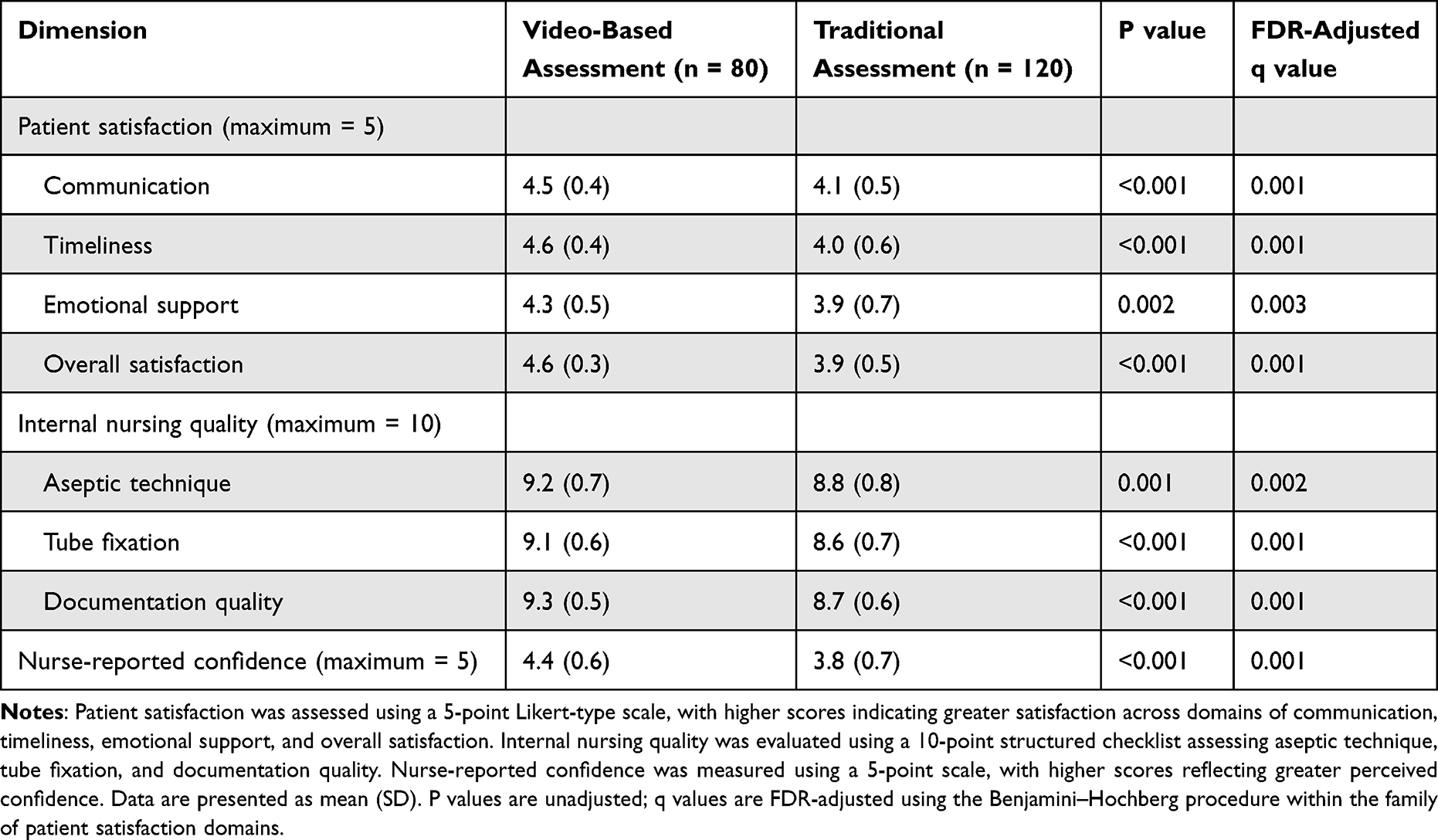 |
Table 3 Patient Satisfaction, Internal Nursing Quality, and Nurse-Reported Confidence |
Exploratory Visualization of Outcomes
Graphical representations of selected clinical and experiential endpoints are illustrated in Figures 2–4. The radar chart (Figure 2A) demonstrates higher patient-reported satisfaction across all four surveyed domains in the video-based assessment (VBA) group, with the largest differences in communication and timeliness, consistent with the findings summarized in Table 3. Figure 2B illustrates the distribution of T-tube removal times, showing a more condensed clustering around the recommended 42–45 days in the video-based assessment (VBA) group, in line with the significantly shorter mean duration reported in Table 2.
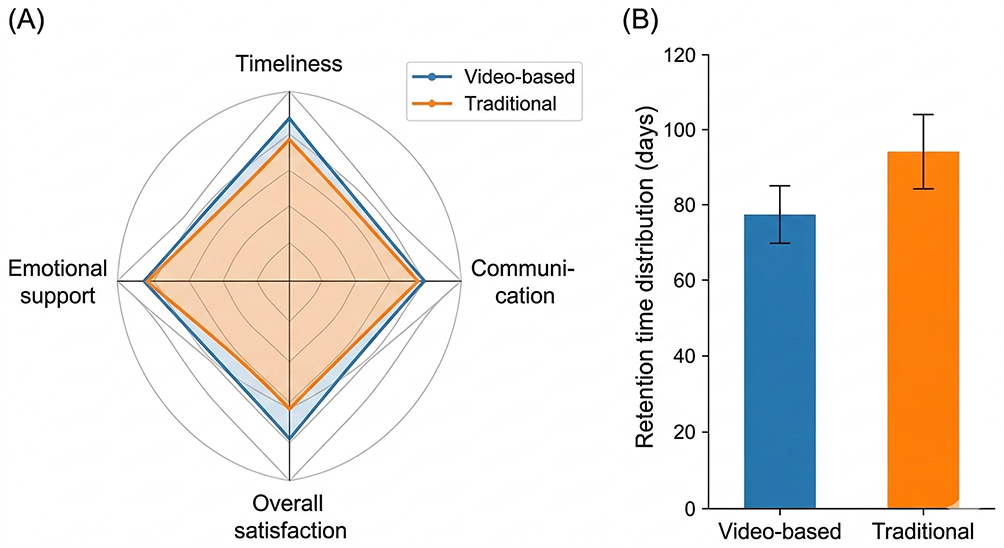 |
Figure 2 Comparative Outcomes Between Video-Based and Traditional Nurse Assessment in T-tube Care. (A) Radar plot showing patient satisfaction scores across domains (communication, timeliness, emotional support, and overall satisfaction). Higher scores indicate greater satisfaction. (B) Retention time distribution of T-tube removal between the video-based and TCA groups, presented as mean ± standard deviation. Greater concentration of removal times around 42–45 days indicates more consistent discharge guidance. |
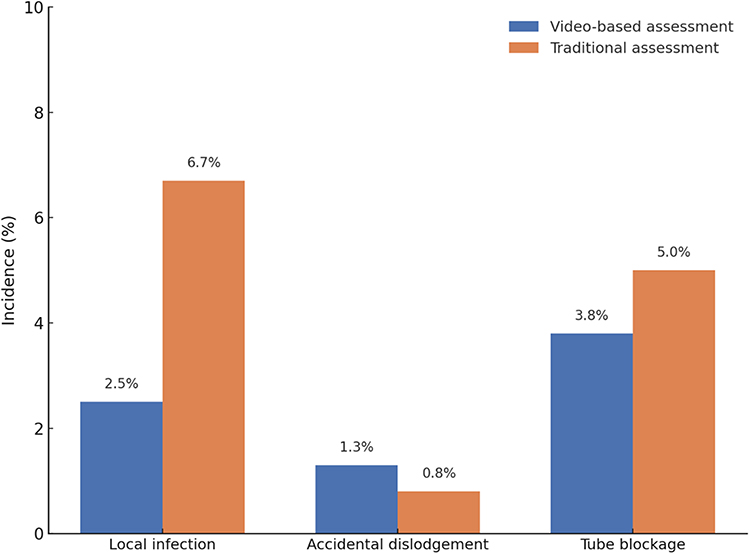 |
Figure 3 Incidence of Tube-Related Complications in Video-Based and TCA groups. Bar chart showing the incidence rates of tube-related complications, including local infection, accidental dislodgement, and tube blockage, in patients assessed by video-based versus traditional methods. Data are presented as percentages. Video-based assessment: Local infection 2.5%, accidental dislodgement 1.3%, tube blockage 3.8%. Traditional assessment: Local infection 6.7%, accidental dislodgement 0.8%, tube blockage 5.0%. This visualization directly reflects the complication data in Table 2, highlighting a lower local infection rate in the video-based group. |
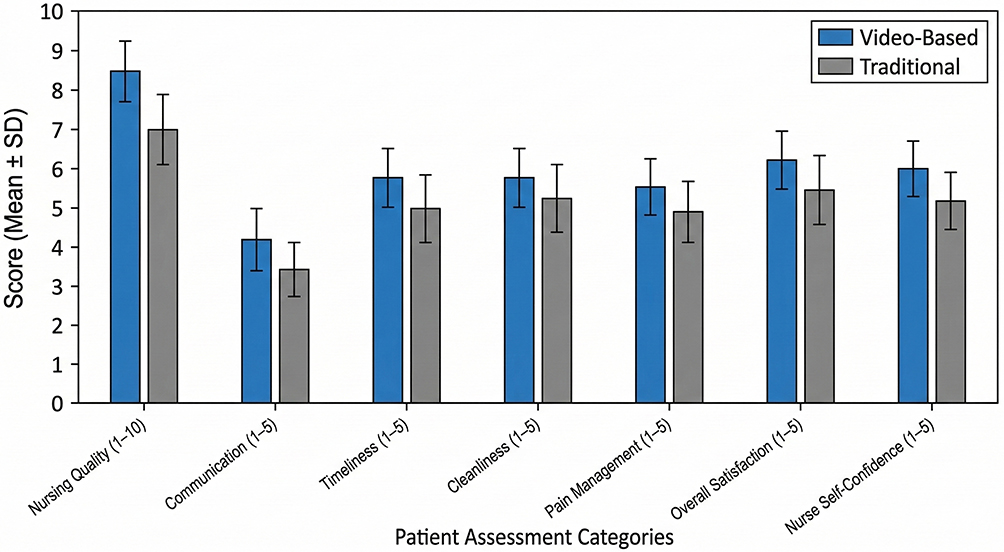 |
Figure 4 Perceived Care Quality and Nursing Satisfaction Scores in Video-Based and Traditional Groups. Bar graph demonstrates mean (±SD) scores across seven domains, including objective nursing quality (scale: 1–10) and five subjective satisfaction dimensions (scale: 1–5). Patients in the video-based assessment group consistently reported higher ratings across all measures. Between-group differences were statistically significant for all domains (P < 0.01), as shown in Table 3. |
Comparative rates of tube-related complications are depicted in Figure 3. Although overall complication rates were lower in the video-based assessment (VBA) group, only the reduction in local infection reached statistical significance, while dislodgement and blockage rates did not differ meaningfully between groups, again mirroring Table 2.
Finally, Figure 4 presents a multi-panel bar chart integrating nursing quality ratings, patient satisfaction scores, and nurse self-confidence. These visual data reinforce the superior performance of the video-based assessment (VBA) group across all seven quality indicators, complementing the quantitative results of Table 3.
Taken together, the figures provide a visual summary that corroborates the tabulated data and highlights the consistency of improvements observed under the video-based nursing evaluation model.
Discussion
The findings of this retrospective comparative study suggest that video-based nursing skill assessment may be associated with improved clinical outcomes and higher patient satisfaction following T-tube surgery. Patients who received care from nurses who had completed structured video assessment modules were more likely to have their T-tube removal scheduled within the recommended 42–45 day window, reflecting more standardized discharge guidance and more precise coordination of inpatient and follow-up care pathways.16,20 These differences were accompanied by consistently higher patient ratings in communication, emotional support, and overall satisfaction, as well as improved internal ratings of nursing care quality.16,21 Although the overall incidence of tube-related complications was numerically lower in the video-based assessment (VBA) group, the difference did not reach statistical significance, likely owing to the limited number of events observed across both cohorts.21,22
The potential advantages associated with video-based skill assessment may lie in its ability to enhance procedural uniformity and reinforce adherence to clearly defined care protocols.16,20 In contrast to conventional teaching formats such as oral briefings or observational shadowing, video-based evaluation delivers a standardized visual framework through which each nurse is assessed using identical reference criteria.22,23 This not only mitigates interobserver variation but also promotes the internalization of sequential technical steps essential to safe T-tube management.20,23 In the setting of a high turnover surgical ward, where nurses frequently rotate across units and differ in levels of procedural familiarity, a unified assessment approach may serve to reduce practice variability and maintain consistent performance standards irrespective of individual background or shift assignment.21,23
Our findings align with prior studies that have explored the use of video-based instruction in nursing education. Existing literature has shown that video feedback can enhance both knowledge retention and skill acquisition in controlled simulation environments. However, few studies have extended this framework to real world patient care settings or examined outcome level metrics beyond procedural pass rates or self reported confidence. In this context, our study provides one of the first institutional level evaluations linking video-based skill assessment to tangible clinical endpoints, including hospitalization parameters and patient reported experiences. While direct comparisons are limited due to heterogeneity in interventions and populations, a recent study evaluating structured nursing onboarding programs similarly reported improvements in documentation accuracy and patient safety indicators, supporting the broader relevance of skills standardization in care delivery.
Notably, per institutional postoperative care pathways, hospital stays after T-tube surgery are typically 3 to 7 days, depending on recovery milestones. In our cohort, the mean postoperative length of stay was 5.8 ± 1.2 days in the VBA group and 6.2 ± 1.5 days in the TCA group (Table 2). Definitive T-tube removal, however, generally occurred approximately six weeks after surgery during scheduled outpatient follow-up visits. During this interval, patients were responsible for managing their T-tubes at home without direct professional supervision. Although this circumstance could introduce variability in complication risk, the comparatively lower incidence of tube-related complications observed in the VBA group may, at least in part, be attributable to more effective discharge education and home-care instruction provided by video-assessed nurses. This suggests that video-based competency evaluation may enhance not only technical proficiency in hospital settings, but also nurses’ ability to equip patients with the knowledge and confidence required for safe home-based recovery. Beyond statistical significance, the magnitude of the observed effects should be interpreted in clinical context. The approximately 2.3-day adjusted reduction in T-tube retention time may be clinically meaningful because it suggests closer adherence to a more standardized target window and potentially more consistent follow-up coordination. By contrast, the adjusted reduction in postoperative length of stay (approximately 0.3–0.4 days) is modest at the individual-patient level and should not be overstated; however, even a small reduction may still be operationally relevant in high-volume surgical settings if it reflects more efficient discharge readiness and nursing workflow coordination. Similarly, the lower adjusted odds of local infection may be clinically important in direction, but the low number of events warrants cautious interpretation.
Several limitations of this study should be acknowledged. First, the retrospective observational design inherently limits causal inference.24,25 Although baseline characteristics were well balanced between groups, the possibility of residual confounding from unmeasured variables cannot be ruled out.24 Routine staffing-based nurse assignment is not equivalent to randomization; therefore, despite apparently balanced baseline characteristics (Table 1), residual and unmeasured confounding may plausibly explain part (or all) of the observed between-group differences. Complication endpoints were infrequent, resulting in limited precision (wide confidence intervals) and insufficient power to exclude modest but clinically meaningful differences; thus, non-significant results should not be interpreted as establishing equivalence. Group allocation was determined by routine staffing schedules rather than randomization, although patient assignment was independent of nurse credentialing status, and blinding was maintained at the patient level. Furthermore, the interpretation of subjective outcomes such as satisfaction and perceived care quality may have been influenced by non-clinical factors including communication preferences and cultural expectations.
Bias and confounding. Several concrete sources of residual confounding may have influenced the observed associations. First, nurse experience and seniority were not explicitly captured; more experienced nurses may deliver better outcomes irrespective of assessment format. Second, self-selection into VBA (eg, motivation and engagement among nurses who completed credentialing) may be associated with higher overall performance, which could partially account for observed differences. Third, temporal improvements in institutional protocols during 2019–2023 (including broader quality-improvement initiatives) may have coincided with VBA scale-up and contributed to better outcomes over time. Fourth, although baseline characteristics were balanced, patient acuity and surgical complexity may not have been fully captured in available records. Fifth, surgeon-level differences in T-tube practices (eg, preferred retention targets and follow-up patterns) could influence recovery endpoints. Finally, a Hawthorne-like behavior change among assessed nurses may have temporarily improved adherence to best practices during the credentialing period. To mitigate confounding, we performed multivariable adjustment incorporating clinically relevant baseline covariates and calendar time; however, residual and unmeasured confounding cannot be excluded and causal inference is not warranted. Although we attempted to reconstruct group status for excluded patients and reported exclusions by group and reason (Table S2), selection bias related to early discharge, documentation completeness, and missing satisfaction data cannot be fully excluded; therefore, satisfaction findings were additionally tested in sensitivity analyses (Table S4).
Importantly, the study may have limited precision to detect modest differences in infrequent outcomes such as tube-related complications because event rates were low. Consequently, effect estimates for several safety-related endpoints were imprecise, as reflected by wide confidence intervals, and the possibility of a type II error cannot be excluded. Therefore, the non-significant difference in complication rates should be interpreted with caution, and not assumed to reflect clinical equivalence.26,27 Accordingly, our findings should not be interpreted as establishing safety equivalence, and larger multicenter cohorts and prospective studies designed around complication endpoints are needed for more definitive safety inference. In addition, because multiple patients may have been cared for by the same nurse, some outcomes may have been correlated within nurses. We therefore reported the number of nurses contributing to each group and the number of patients cared for per nurse; however, formal cluster-adjusted analyses were not performed in the present study. Accordingly, standard errors may have been underestimated, and this should be considered when interpreting the statistical significance of between-group comparisons. Additionally, the absence of long-term follow-up precludes assessment of delayed complications or extended recovery outcomes.
Finally, while the video assessment protocol was institutionally standardized, variability in its delivery and adherence across different assessors over time could not be formally quantified.28
Another consideration relates to the unequal group sizes, with the TCA group comprising a larger proportion of the cohort. While baseline features were statistically comparable, this imbalance could reduce statistical power to detect differences in less frequent outcomes and may have influenced the overall sensitivity of the analysis.27 Additionally, although 59 patients were excluded based on predefined criteria, their group assignment status was not recorded, and the possibility of differential exclusion bias cannot be entirely ruled out.24,25
These findings have practical implications for nursing quality assurance systems in tertiary care settings. The implementation of structured, reproducible, and observable skill evaluations may represent a feasible strategy to enhance procedural nursing care, particularly for tasks with high technical sensitivity and complication risk. Because the credentialing program was implemented and scaled over time, it is possible that some nurses contributed to both pre-credentialing (TCA) and post-credentialing (VBA) care at different time points. This may reflect a learning or training effect inherent to quality-improvement implementation, and should be considered when interpreting the observed between-group differences. In addition, some secondary outcomes may have been influenced by broader, contemporaneous quality-improvement changes accompanying the wider implementation of VBA (eg, increased supervision, reinforcement of standardized workflows, and team learning), and therefore may not be attributable to the assessment format alone. In addition, several clinically important safety endpoints were rare in our cohort. Consequently, while we did not observe statistically significant between-group differences in dislodgement, blockage, or overall tube-related complications, the corresponding effect estimates were imprecise and do not rule out clinically meaningful differences. Therefore, our data should not be interpreted as establishing safety equivalence; larger multicenter cohorts and prospective studies designed around complication endpoints are needed to provide more definitive safety inference. Because the VBA pathway comprises multiple components beyond video capture (including a structured rubric, asynchronous review, documentation/auditability, and potential assessor calibration), this observational study cannot disentangle the independent contribution of any single component (eg, video per se versus rubric standardization) to the observed associations. During 2019–2023, nurses and patients may also have been exposed to broader institutional quality-improvement activities (eg, documentation standardization, infection-control reinforcement, and general nursing quality initiatives), although no separate formal program specifically targeting postoperative T-tube management was implemented in parallel. These contemporaneous changes may have contributed to some observed differences and should be considered when interpreting secondary outcomes. In addition, patient satisfaction was measured using a routine hospital questionnaire developed for local quality-monitoring purposes rather than a formally standardized research instrument, although internal consistency was acceptable in the present cohort. Because internal nursing quality ratings were generated through routine departmental audit rather than fully blinded research assessment, observer bias cannot be completely excluded.
Future research should explore the generalizability of these results across other procedures and institutions, and prospective studies with randomized allocation or mixed method designs may help elucidate the mechanisms through which assessment format influences clinical care. Integrating such models into ongoing nursing education and credentialing systems may offer a scalable path toward improved safety and patient centered outcomes. Future studies should account for potential within-nurse clustering using mixed-effects or cluster-robust methods. Future prospective studies should incorporate a priori sample size planning based on clinically meaningful differences in prespecified primary endpoints; substantially larger samples will likely be required if complication outcomes are intended as confirmatory safety endpoints.
Conclusion
In this retrospective study of patients undergoing T-tube surgery, nursing care delivered by video-assessed staff was associated with modest but clinically meaningful improvements in recovery time and patient satisfaction. Because routine staffing-based nurse assignment is not equivalent to randomization, and residual or unmeasured confounding may remain, causality cannot be inferred. These findings suggest that structured video-based skill assessment may be associated with more consistent nursing performance in procedure-sensitive contexts. Incorporating standardized visual evaluation into institutional nursing education and credentialing systems may represent a practical quality-assurance strategy to enhance care quality and support patient-centered outcomes, and should be confirmed in prospective studies.
Ethics Approval and Consent to Participate
This retrospective observational study was approved by the Institutional Review Board of Xingtai People’s Hospital (Approval No. AF/SS-07/02.0). The requirement for informed consent was waived because the study used anonymized routinely collected data.
Author Contributions
Conceived and designed the study: Hui Zhao. Performed the literature search, data extraction, and drafted the manuscript: Bo Zhang. Review and editing and data extraction: Yanran Li. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the 2019 Hebei Province Medical Science Research Project Plan (Grant No. 20191699), entitled Application of a Self-Developed Video Assessment Model in Standardized Nursing Skills Training.
Disclosure
The authors declare that there are no conflicts of interest related to this study.
References
1. Maneesh S, Chaudhary S, Sharma R, Amit M. A prospective study of complications of T-tube drainage of common bile duct in the management of choledocholithiasis. IOSR J Dental Med Sci. 2016;15(10):09–15. doi:10.9790/0853-1510020913
2. Rajput D, Itish P, Sruthi S, Beeram KPK, Amit G. Fractured T-tube fragment in common bile duct during retrieval: an unforeseen mishap. Surg J. 2021;7(03):e251–e254. doi:10.1055/s-0041-1735643
3. Xuan-J W. Factors inducing drainage tube complications after hepatobiliary surgery. 2022.
4. Yu-Lin H, Meng-Chang L, Bai-Yun W. Efficacy and safety analysis of continued nursing of complications in discharged patients after percutaneous transhepatic biliary drainage. World J Clin Cases. 2024;12(19):3898–3907. doi:10.12998/wjcc.v12.i19.3898
5. Choi D, Lee H, Choi M-J, Kim K, Shin Y, Kim J-S. Development of a drainage tube (Jackson-Pratt Drain or Hemovac) management protocol. J Korean Acad Fundam of Nurs. 2023;30(3):371–381. doi:10.7739/jkafn.2023.30.3.371
6. Merrou S, Baslam A, Jouicha AI, Ouhaz Z, El Adib AR. Blended learning and simulation in nursing education: a quasi-experimental study on a nursing institute. J Educ Health Prom. 2023;12(1). doi:10.4103/jehp.jehp_72_23
7. Alhashemi SH, Ghorbani R, Vazin A. Improving knowledge, attitudes, and practice of nurses in medication administration through enteral feeding tubes by clinical pharmacists: a case–control study. Adv Med Educ Pract. 2019;10:493–500. doi:10.2147/AMEP.S203680
8. Helmy NM, Aly AA, Atia RRA, Mohammed BMAH, Abouelezz ZGME. Effect of educational guidelines on nurses’ performance regarding percutaneous nephrostomy tube. Egyptian J Health Care. 2023;14(1):578–593.
9. Park SJ, Lim Y-S, Ko G, et al. Development of the evidence-based pain management, pressure ulcer care, fall prevention care, and drainage tube management protocol for nursing students. Korean Soc Nurs Res. 2023;7(2):71–89. doi:10.34089/jknr.2023.7.2.71
10. Khaqan HA, Mahboob U, Md Ali H, Hasnain Muhammad B, Hafiz Ateeq Ur R. Effectiveness of video observation of procedural skills in surgical performance of ophthalmology residents. Pak J Med Health Sci. 2022;16(1):160–162. doi:10.53350/pjmhs22161160
11. Tuma F. Evaluating operative skills using video-recording-aided objective test. Surg Innov. 2020;27(5):421–423. doi:10.1177/1553350620965818
12. Hassanpour N, Rebecca IC, Baikpour M, Moghimi S. Video observation of procedural skills for assessment of trabeculectomy performed by residents. J Curr Ophthalmol. 2016;28(2):61–64. doi:10.1016/j.joco.2016.03.003
13. Laura J, Laurie AH, Stephen EM, et al. Development and validation of simulation-based procedural checklists for evaluation of neonatal nurse practitioner performance. Adv Neonatal Care. 2018;18(5):386–392. doi:10.1097/ANC.0000000000000520
14. Nermine ME, Jaramillo J, Llaguno M, Seweid M, Mousa O. Student nurses as modern digital nomads: developing nursing skills competence and confidence through video-based learning. Int J Innov Res Med Sci. 2022;7(6):254–271. doi:10.23958/ijirms/vol07-i06/1418
15. Husain N. Assess the effectiveness of structured video assisted teaching programme (SVATP) regarding role & responsibilities of a nurse in intubation and suctioning of a patient with an endotracheal tube. Int J Sci Res. 2023;12(8):38–39. doi:10.21275/SR23727203107
16. Jairus R, Ritu PN, Sangeetha S. Effectiveness of structured video-assisted learning vs demonstration on closed tracheal suction among undergraduate student nurses. Nurs Midwifery Res J. 2023;19(1):22–33. doi:10.1177/0974150X221141743
17. Lewis P, Hunt L, Ramjan L, Miranda D, O’Reilly R, Salamonson Y. Factors contributing to undergraduate nursing students’ satisfaction with a video assessment of clinical skills. Nurse Educ Today. 2019;84:104244. doi:10.1016/j.nedt.2019.104244
18. Sun Kyung K, Youngho L, Hye Ri H, Oe Nam K. Wearable smart glasses for first-person video analysis to evaluate nursing skills: a pilot study with a mixed method design. J Comput Assist Learn. 2024;41(1):e13080. doi:10.1111/jcal.13080
19. Burak Y, Gamze K, Hanım Duru Yüce B, Bahar Ç. Watch and learn your performance: the effect of self-assessment with video recording on nursing students’ knowledge and skills of nasogastric catheter placement. Nurse Educ Pract. 2025;83:104251. doi:10.1016/j.nepr.2025.104251
20. Chao YC, Hu SH, Chiu HY, Huang PH, Tsai H, Chuang Y. The effects of an immersive 3d interactive video program on improving student nurses’ nursing skill competence: a randomized controlled trial study. Nurse Educ Today. 2021;103:104979. doi:10.1016/j.nedt.2021.104979
21. Kim ON. Experience of applying the video evaluation method on core nursing skills evaluation. Asia-Pacific J Convergent Res Interchange. 2022;65–73. doi:10.1016/J.MIDW.2018.10.004
22. Eom M, Kim SK, Park MH. Effectiveness of video recording and self-evaluation for skill training in undergraduate nursing education. Medico-Legal Update. 2020;20:2143–2148.
23. Sari I, Sundari S. The use of video as a learning strategy in supporting the increasing knowledge and clinical skills of nursing students. Media Keperawatan Indonesia. 2021;4(1):47. doi:10.26714/mki.4.1.2021.47-55
24. Imrey P, Imrey PB. Clinical research methodology 2: observational clinical research. Anesthesia Analg. 2015;121(4):1043–1051. doi:10.1213/ANE.0000000000000861
25. Oijen MV. Clinical relevance of retrospective observations. Nederlands Tijdschrift voor Geneeskunde. 2010;154:A2174.
26. Belov D, Nikolaenko V, Nizametdinova Y. Reasonability of accounting for gender in intraocular lens power calculation. Rus Ann Ophthal. 2023;139(5):68. doi:10.17116/oftalma202313905168
27. O’Keefe D. Brief Report: Post Hoc Power, Observed Power, A Priori Power, Retrospective Power, Prospective Power, Achieved Power: Sorting Out Appropriate Uses of Statistical Power Analyses. Communication Methods and Measures. 2007;1:291–299. doi:10.1080/19312450701641375
28. Ramgopal S, Benedetti J, Cotter JM. Performing a Multicenter Retrospective Study. Hospital Pediatrics. 2025;15(2):e77–e82. doi:10.1542/hpeds.2024-008020
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.