Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Victimization in Childhood Influences Presenteeism in Adulthood via Mediation by Neuroticism and Perceived Job Stressors
Authors Hashimoto S, Ichiki M, Ishii Y, Morishita C ![]() , Shimura A
, Shimura A ![]() , Kusumi I
, Kusumi I ![]() , Inoue T
, Inoue T ![]() , Masuya J
, Masuya J ![]()
Received 11 October 2021
Accepted for publication 28 January 2022
Published 15 February 2022 Volume 2022:18 Pages 265—274
DOI https://doi.org/10.2147/NDT.S343844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Taro Kishi
Shogo Hashimoto,1,* Masahiko Ichiki,2,* Yoshitaka Ishii,2,3 Chihiro Morishita,2 Akiyoshi Shimura,2 Ichiro Kusumi,1 Takeshi Inoue,2 Jiro Masuya2
1Department of Psychiatry, Hokkaido University Graduate School of Medicine, Sapporo, 060-8638, Japan; 2Department of Psychiatry, Tokyo Medical University, Tokyo, 160-0023, Japan; 3Fuji Psychosomatic Rehabilitation Institute Hospital, Fujinomiya, Shizuoka, 418-0035, Japan
*These authors contributed equally to this work
Correspondence: Takeshi Inoue, Tel +81 3 3342 6111, Fax +81 3 3340 4499, Email [email protected]
Background: Victimization in childhood profoundly influences the mental health of individuals in adulthood, causing depression, anxiety disorder, suicidality, and self-harm, which leads to productivity loss in the workplace, ie, presenteeism. However, the specific effects of victimization on presenteeism remain unclear. We hypothesized that victimization affects the presenteeism of workers through neuroticism and perceived job stressors and analyzed the association among these factors by path analysis.
Methods: A questionnaire survey, including demographic and clinical data, Japanese versions of victimization scale in childhood, Brief Job Stress Questionnaire, and Work Limitations Questionnaire (WLQ), was administered to 443 adult volunteers between April 2017 and April 2018 in Tokyo, Japan. Multiple variables were analyzed by multiple regression analysis and path analysis. The Institutional Review Board of Tokyo Medical University approved this study.
Results: Path analysis demonstrated that neuroticism and perceived job stressors had direct effects on presenteeism in the WLQ. Victimization indirectly increased presenteeism via neuroticism and its subsequent effects on perceived job stressors. This model accounted for 18% of the variability of presenteeism (R2 = 0.180).
Limitations: There may be possible recall bias owing to the self-administration of the questionnaire. In addition, this study had a cross-sectional design, and hence the causal associations among variables should be validated in a prospective study.
Conclusion: The present study indicates that the experience of victimization in childhood is a risk factor of adulthood presenteeism, and this effect is mediated by neuroticism and adverse effects on job stressors. These results suggest that multiple factors, including childhood victimization, neuroticism, and job stressors, should be considered when assessing and preventing presenteeism.
Keywords: victimization, neuroticism, job stressor, presenteeism, childhood
Introduction
Various adverse experiences, such as abuse, inappropriate parenting, and stressful life events, during childhood and adulthood influence mental health, such as leading to depression.1–4 In addition to parental maltreatment during childhood, victimization from peers in school and the community also influences overall mental health, subsequently leading to depression, anxiety disorder, suicidality, and self-harm in adolescence.5–8 Neuroticism, which is one of the Big Five personality traits, is a well-known established risk factor for depression, as well as other mental illnesses.9–11 Several lines of evidence suggest that neuroticism is a common vulnerability and mediator in the associations of childhood maltreatment, parenting, and victimization with depression.1,2,6
The loss of productivity of workers due to sickness (presenteeism), as well as the absence of workers from their workplace due to sick leave (absenteeism) is a major concern in the workplace, and results in high social costs.12 Mental and behavioral disorders cause the highest total cost burden among medical diseases in aspects of total health-associated costs, including presenteeism, absenteeism, and medical and pharmaceutical expenses.12,13 Various factors, such as sex, workplace environment, and social policy may influence absenteeism.14 The most common reasons for presenteeism are similar to those for absenteeism, including musculoskeletal disorders, gastrointestinal symptoms, and common mental health problems including depression and anxiety disorders.15 Job stress, fully remote work, sleep disturbances, economic factors, workplace cultures, positive orientations toward work, etc., may increase presenteeism.15–19 The contribution of depression to presenteeism is significant and has been investigated in detail previously.20 Hence, adverse experiences in childhood and neuroticism, which are closely associated with depression, are expected to influence presenteeism. However, there have been very few studies to date on this issue; ie, only one study reported that a higher level of childhood maltreatment showed more presenteeism in adult workers, and this association was mediated by current depressive disorder and current comorbid depression-anxiety.21 Thus, the effects of victimization from peers in school and the community or neuroticism on presenteeism have not been reported to date.
Previous studies showed that job stressors worsened presenteeism through their effects on psychological and physical responses, and sleep disturbances.19,22,23 Job stressors, which are reportedly affected by childhood parenting, resilience, and neuroticism, induce psychological and physical responses in workers.24,25 Job stressors are a mediator among childhood parenting, resilience, neuroticism, and psychological and physical responses.24,25 Taken together with the previous findings mentioned above regarding the associations among adverse stresses in childhood, including victimization, neuroticism, depression, and presenteeism,1,2,6,21,22,24–26 it can be assumed that childhood victimization influences neuroticism, job stressors, and presenteeism. However, these associations of childhood victimization with neuroticism, job stressors, and presenteeism have not yet been studied in detail. As a theoretical basis for personality traits and job stressors as mediators between childhood adverse stress and depressive symptoms or job stress responses has been proposed,1,2,6,22,24–26 an investigation is necessary to clarify this issue.
Based on the above information and theoretical basis, we hypothesized that victimization in childhood affects job stressors and presenteeism in adult workers, and that this effect is mediated by neuroticism; similarly to the mediation that has been confirmed among maltreatment, parenting, and victimization in childhood and depression.1,2,6 We hence conducted a questionnaire survey in 443 adult worker volunteers and verified our hypothesis by path analysis (covariance structure analysis).
Subjects and Methods
Study Design
A cross-sectional observational study was conducted on Japanese adult workers, by collecting data using self-administered questionnaire surveys.
Subjects
The subjects were 443 adult workers (195 men and 248 women, mean age: 40.9 ± 11.8 years), who voluntarily participated in the study from April 2017 to April 2018 through our acquaintances in Tokyo and environs. Subjects were 20 years or older and had no severe physical diseases or organic brain diseases. The study was conducted by a paper-based survey. Most of the participants were office workers and nurses. This study was part of a larger study, which investigated stress, personality traits, affective symptoms, sleep, quality of life, well-being, resilience, etc., in adult volunteers by a questionnaire survey.24 The study was approved by the Institutional Review Board of Tokyo Medical University (study approval number: SH3502), and complied with the Declaration of Helsinki (amended in Fortaleza in 2013). All subjects provided written informed consent to participate in this study.
Questionnaires
Demographic and clinical information, and the following four questionnaires were collected by self-report of the participants.
Assessment Scale of Victimization in Childhood
The original scale, which was reported previously, was used for evaluating the frequency and degree of victimization experiences in the community and school during childhood.6 This study investigated general childhood victimization by negative actions rather than childhood bullying. Childhood victimization in this study was not necessarily intentional victimization or involving an imbalance of power, and included three types of victimization, ie, physical victimization, verbal victimization, and relational victimization.6 The five items for victimization were measured using a 5-point Likert scale (0 to 4 points), and the total score of the five items was analyzed as the victimization score. A high score indicates a high degree of victimization. In our previous study, the score of the victimization scale significantly correlated with neuroticism, having depression, and the severity of depressive symptoms.6 In the present study, Cronbach’s α coefficient calculated for this scale was 0.862, indicating very high internal consistency.
Eysenck Personality Questionnaire-Revised (EPQ-R) Neuroticism Subscale
The neuroticism subscale of the shortened version of the EPQ-R was used to evaluate neuroticism.27 Neuroticism is a tendency of having an unstable mood, and readily feeling miserable, worried, hurt, fed up, nervous, tense, lonely, guilty, and irritable.27 The neuroticism score is derived from 12 items evaluated on a yes-no scale (yes: 1; no: 0). The validity and reliability of the Japanese shortened version of the EPQ-R were confirmed in our previous study.28 We used this subscale for the path analysis recently.1,2,6,24
Brief Job Stress Questionnaire (BJSQ)
The BJSQ is a 57-item multidimensional job stress questionnaire that is used to measure an individual’s stress response.29,30 It is widely used in workplaces as the recommended protocol of the Stress Check Program in Japan.31 Among the four subscales of the BJSQ, ie, perceived job stressors, psychological and physical stress responses, social support, and satisfaction, in this study, the total score of the perceived job stressors (17 items assessed on a 4-point Likert scale [1 to 4 points], eg, quantitative job overload, qualitative job overload, and job control) was used for the analysis. We recently used this subscale for path analysis.24,25 The higher the score of the subscale, the higher the stress.
Work Limitations Questionnaire (WLQ)
WLQ is a self-report questionnaire that asks about the influence of health issues on work, and evaluates presenteeism.32 The short form and the validated Japanese version was used.33 The percentage of productivity loss owing to health problems in the previous 2 weeks measured by the WLQ was used as an indicator of presenteeism in the analysis.
Data Analysis
The associations of demographic, clinical, and questionnaire data with presenteeism (%WLQ productivity loss) were determined by the Pearson correlation coefficient or Student’s t-test using SPSS Statistics 27.0J software (IBM, Armonk, NY, USA). Multiple regression analysis was conducted using the forced entry method, with presenteeism as the dependent variable and the following nine variables as independent variables: age, sex, education years, past history of psychiatric disease, current psychiatric disease, marital status, victimization score in childhood, neuroticism score (EPQ-R), and BJSQ perceived job stressor score. In addition, two multiple regression analyses with neuroticism score (EPQ-R) and BJSQ perceived job stressor score as the dependent variable were conducted.
Based on the hypothesis presented in the Introduction section, a path analysis model was built using victimization score in childhood, neuroticism (EPQ-R), perceived job stressors (BJSQ), and presenteeism (%productivity loss of WLQ). This model assumed that the experience of victimization in childhood influences presenteeism directly and indirectly through neuroticism and perceived job stressors. The Mplus 8.4 software (Muthén & Muthén, Los Angeles, CA, USA) was used for covariance structure analysis with the robust maximum likelihood estimation method. The level of statistical significance was set at p < 0.05.
Results
Demographic and Clinical Information, and Questionnaire Data Associated with Presenteeism
Table 1 shows the results of the associations among demographic, clinical, and questionnaire data and presenteeism (WLQ %productivity loss) in 443 adult volunteers. Unmarried status, current psychiatric disease, and past history of psychiatric disease were significantly associated with high presenteeism. Victimization in childhood, EPQ-R neuroticism, and BJSQ perceived job stressor scores positively correlated with presenteeism.
 |
Table 1 Demographic and Clinical Characteristics and Questionnaire Measures of 443 Adult Workers, and Their Correlation with %productivity Loss of WLQ |
Multiple Regression Analysis with Presenteeism as the Dependent Variable
Table 2 shows the results of multiple regression analysis using the forced entry method for presenteeism (WLQ %productivity loss). Presenteeism significantly correlated with BJSQ perceived job stressors (standardized partial regression coefficient β: 0.264), neuroticism (β: 0.225), current psychiatric disease (β: 0.099), and married status (β: –0.118). The other 5 independent variables showed no statistically significant correlation with presenteeism. Multicollinearity was denied. This regression model explained 21% of the variability in presenteeism.
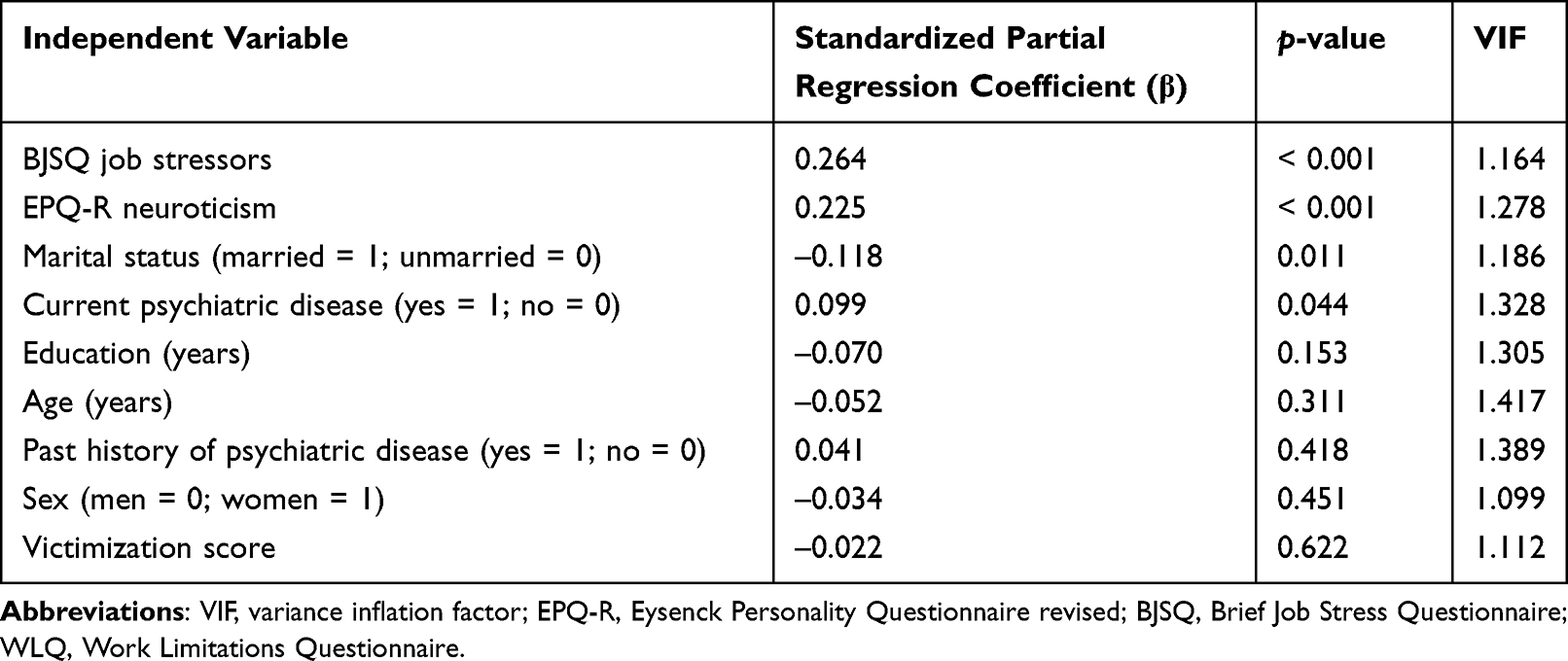 |
Table 2 Results of Multiple Regression Analysis of % Productivity Loss of WLQ |
Table 3 shows the results of multiple regression analysis using the forced entry method for BJSQ perceived job stressors. BJSQ perceived job stressors significantly correlated with neuroticism (β: 0.278), past history of psychiatric disease (β: –0.143), education (β: –0.131), and victimization score (β: 0.103). The other 4 independent variables showed no statistically significant correlation with BJSQ perceived job stressors. Multicollinearity was denied. This regression model explained 12% of the variability in BJSQ perceived job stressors.
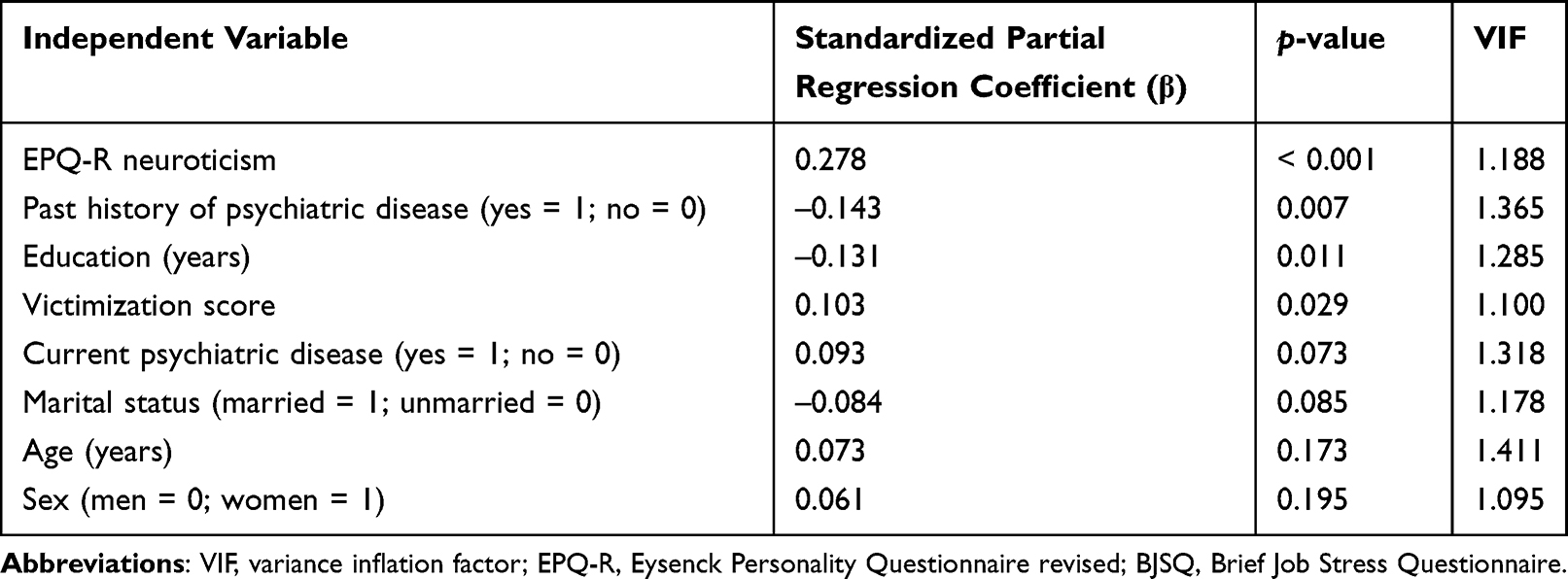 |
Table 3 Results of Multiple Regression Analysis of BJSQ Perceived Job Stressors |
Table 4 shows the results of multiple regression analysis using the forced entry method for neuroticism. Neuroticism significantly correlated with age (β: –0.198), past history of psychiatric disease (β: 0.190), and victimization score (β: 0.187). The other 4 independent variables showed no statistically significant correlation with neuroticism. Multicollinearity was denied. This regression model explained 14% of the variability in neuroticism.
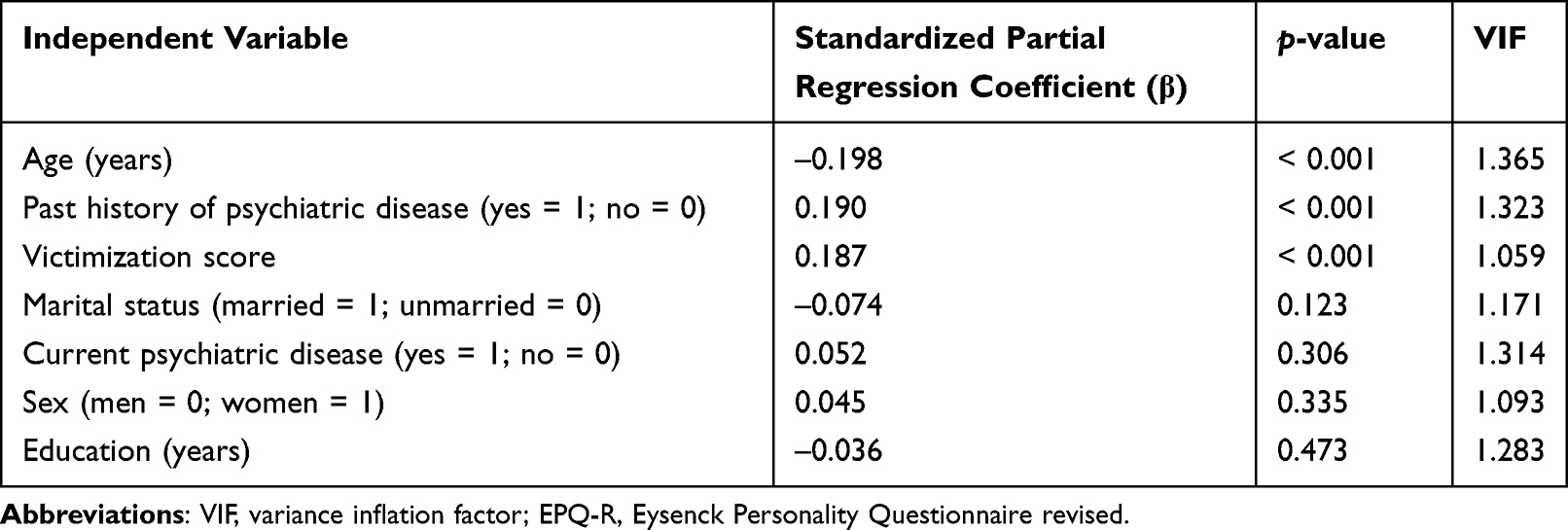 |
Table 4 Results of Multiple Regression Analysis of EPQ-R Neuroticism |
Path Analysis of Presenteeism
Multiple regression analysis showed the significant effects of perceived job stressors and neuroticism on presenteeism, but did not show a significant effect of victimization in childhood on presenteeism, despite a significant univariable correlation. Based on the hypothesis in the Introduction and Methods sections, the effects of victimization in childhood on presenteeism are speculated to be mediated by neuroticism and perceived job stressors. The path analysis shown in Figure 1A demonstrated the significant direct effects in which victimization increases neuroticism, neuroticism increases job stressors, and both neuroticism and job stressors increase presenteeism, as expressed by %productivity loss in the WLQ.
 |
Figure 1 Results of the path analysis model with victimization in childhood, neuroticism on the EPQ-R, perceived job stressors on the BJSQ, and %productivity loss (presenteeism) on the WLQ. Direct effects (A) and indirect effects (B) are shown. The numbers show the standardized path coefficients (–1 ≤ β ≤ 1). **p < 0.01; ***p< 0.001. Abbreviation: ns, not statistically significant. |
Consistent with the results of multiple regression analysis, victimization did not increase presenteeism directly. However, victimization had significant indirect effects on the increase in presenteeism through two paths; one including neuroticism, and the other including both neuroticism and job stressors (Figure 1B). In addition, the indirect effects of neuroticism on presenteeism via job stressors and the indirect effects of victimization on job stressors via neuroticism were statistically significant (Figure 1B). The coefficient of determination of presenteeism was 0.180; ie, this model accounts for 18.0% of the variability of presenteeism.
Discussion
In this study, we showed that victimization in childhood indirectly increased presenteeism, and that neuroticism and subsequent increased perceived job stressors were mediators. As there is a very long interval between adverse events in childhood and presenteeism in workers in adulthood, the existence of mediators that link these two events is reasonable, and provides answers to clinical questions as to how events that occurred a long time ago can influence the current state of an individual. Consistent with the present results, the role of personality traits as mediators for childhood adversities, depression, and job stress has been reported recently.1,2,24,26
Among the various types of personality traits, the role of neuroticism in mental health has been clarified. Neuroticism is a well-established risk factor for depression and other major mental illnesses.9,10 Neuroticism mediates the indirect effects of childhood maltreatment and poor parenting experiences on depression.1,2,26 These previous studies are consistent with the results of this study, which identified neuroticism as a mediator for the influence of childhood events on presenteeism in adulthood. Tachi et al reported that neuroticism mediated the effects of victimization in childhood on depression in adulthood.6 In a study on adolescents, victims of bullying showed high neuroticism.34 A previous 3-year prospective study reported that being victimized in the workplace increased neuroticism in adults, and neuroticism decreased in the absence of victimization, indicating that neuroticism is not an unchangeable temperament and can be changed by stressors, such as victimization from colleagues.35 These studies suggest that victimization in childhood and adulthood leads to high neuroticism, and then high neuroticism leads to mental health problems in adulthood, supporting our idea that neuroticism acts as a mediator between victimization in childhood and presenteeism in adulthood.
From the aspect of job stress, our recent study reported that low care and high overprotection from parents in childhood increased neuroticism, and worsened perceived job stress and subsequent psychological and physical reactions through the mediating effect of neuroticism.24 Although the association between neuroticism and job stress has been reported, very few studies before our recent study have reported the effects of childhood maltreatment or parenting experiences on job stress.21,24,36,37 In addition, the mediation effect of neuroticism between childhood stress and depression has been reported in some studies, but only one study has reported its mediation effect between childhood stress and job stress.1,2,6,24,26 The present study expanded the earlier finding of the mediation effect of neuroticism between childhood stress and job stress to subjects who experienced victimization in childhood. This is the main strength of the present study. Hence, when we evaluate job stress in workers, their history of childhood stress, such as victimization, and assessment of their personality trait of neuroticism are essential to understand their susceptibility to presenteeism, which was poorly schematized in the job stress model of the National Institute for Occupational Safety and Health (NIOSH).38
Presenteeism in the workplace is influenced strongly by job stressors and subsequent psychological and physical stress responses.18,19,22,23 Social support in workplaces and at home reduces presenteeism through a reduction in job stress reactions.18,19,22 Other factors, such as sleep disturbances and irregular mealtimes also worsen presenteeism by influencing job stress reactions.16,22 In this study, we first clarified that childhood victimization and neuroticism worsen presenteeism by increasing perceived job stressors. As described in the Introduction section, victimization from peers in school and the community induces various mental health problems in individuals in later life.5–8 Moreover, victimization in childhood is assumed to worsen presenteeism in the workplace, and this association was clarified in the present study. From a nation’s point of view, measures against victimization in childhood as well as harassment in the workplace, both of which have already been legislated in Japan, are necessary for improving work productivity and reducing presenteeism.
Multiple regression analysis in this study showed a significant association of marital status with presenteeism (Table 2); ie, unmarried status was associated with presenteeism, which was consistent with a previous report.39 In this study, higher scores of victimization in childhood were associated with unmarried status (data not shown). Thus, there is a possibility that unmarried status influences the association between childhood victimization and high presenteeism. In the additional multiple regression analyses (Tables 3 and 4), marital status was not significantly associated with neuroticism and perceived job stressors. Therefore, marital status might not influence the association between childhood victimization and presenteeism in adult workers.
The present findings provide new viewpoints to healthcare and management, and the governance of the workplace. At least in Japan, job stress and presenteeism are major healthcare problems occurring in the workplace.12,31 However, individual factors of workers should be considered for the prevention of and measures against job stress and presenteeism, as indicated by the job stress model of the NIOSH.38 Among several individual factors, the present study showed that victimization in childhood and neuroticism are significant factors that affect presenteeism.
There are several limitations to this study. As this study had a cross-sectional design, we were unable to conclude the causal associations among the factors. To verify the causal associations of the possible mediations analyzed in this study, a very long-term large-scale study would be required. However, the feasibility of such a study is low, and hence a cross-sectional study like the present study is thought to be useful for analyzing this hypothesis at the moment. The use of the self-report questionnaire, in which the participants needed to recall childhood events, may have caused recall bias. The nature of the subjects being Japanese adult volunteers limits the generalization of the present findings to other populations, such as those from other countries.
Conclusions
This study indicated that victimization in childhood leads to presenteeism in adult workers, and that this long-term effect is mediated by neuroticism and subsequent perceived job stressors. Therefore, to prevent presenteeism in the workplace, individual factors involving adverse childhood experiences and personality traits should be considered together with job stress in the workplace.
Acknowledgments
We thank Dr. Nobutada Takahashi of Fuji Psychosomatic Rehabilitation Institute Hospital, Dr. Hiroshi Matsuda of Kashiwazaki Kosei Hospital, Dr. Yasuhiko Takita (deceased) of Maruyamasou Hospital, and Dr. Yoshihide Takaesu of Izumi Hospital for their collection of subject data. We thank Dr. Helena Popiel of the Department of International Medical Communications, Tokyo Medical University, for editorial review of the manuscript. Shogo Hashimoto and Masahiko Ichiki are co-first authors for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Masahiko Ichiki has received personal compensation from Otsuka Pharmaceutical, Pfizer, Eli Lilly, Mitsubishi Tanabe Pharma, Mochida Pharmaceutical, Meiji Seika Pharma, Janssen Pharmaceutical, Takeda Pharmaceutical Company, Yoshitomiyakuhin, Daiichi Sankyo, MSD, Dainippon Sumitomo Pharma, and Eisai; grants from Otsuka Pharmaceutical, Eli Lilly, Eisai, Shionogi, Takeda Pharmaceutical, MSD, and Pfizer; and is a member of the advisory board of Meiji Seika Pharma. Dr Akiyoshi Shimura has received lectures fees from Dainippon Sumitomo Pharma, MSD, and Eisai outside of the submitted work. Ichiro Kusumi has received personal compensation from Daiichi Sankyo, Dainippon Sumitomo Pharma, Eisai, Eli Lilly, Janssen Pharmaceutical, Lundbeck, Meiji Seika Pharma, Mochida Pharmaceutical, MSD, Mylan, Novartis Pharma, Ono Pharmaceutical, Otsuka Pharmaceutical, Pfizer, Shionogi, Shire, Taisho Toyama Pharmaceutical, Takeda Pharmaceutical, Tsumura, and Yoshitomiyakuhin, and has received research/grant support from Asahi Kasei Pharma, Astellas, Daiichi Sankyo, Dainippon Sumitomo Pharma, Eisai, Eli Lilly, Mochida Pharmaceutical, Novartis Pharma, Otsuka Pharmaceutical, Pfizer, Shionogi, Takeda Pharmaceutical, and Tanabe Mitsubishi Pharma. Takeshi Inoue has received personal fees from Mochida Pharmaceutical, Takeda Pharmaceutical, Eli Lilly, Janssen Pharmaceutical, MSD, Taisho Toyama Pharmaceutical, Yoshitomiyakuhin, and Daiichi Sankyo; grants from Shionogi, Astellas, Tsumura, and Eisai; and grants and personal fees from Otsuka Pharmaceutical, Dainippon Sumitomo Pharma, Mitsubishi Tanabe Pharma, Kyowa Pharmaceutical Industry, Pfizer, Novartis Pharma, and Meiji Seika Pharma; and is a member of the advisory boards of Pfizer, Novartis Pharma, and Mitsubishi Tanabe Pharma. Jiro Masuya has received personal compensation from Otsuka Pharmaceutical, Eli Lilly, Astellas, and Meiji Yasuda Mental Health Foundation, and grants from Pfizer. The other authors declare that they have no actual or potential conflicts of interest associated with this study.
References
1. Ono K, Takaesu Y, Nakai Y, et al. Associations among depressive symptoms, childhood abuse, neuroticism, and adult stressful life events in the general adult population. Neuropsychiatr Dis Treat. 2017;13:477–482. doi:10.2147/NDT.S128557
2. Ono Y, Takaesu Y, Nakai Y, et al. The influence of parental care and overprotection, neuroticism and adult stressful life events on depressive symptoms in the general adult population. J Affect Disord. 2017;217:66–72. doi:10.1016/j.jad.2017.03.058
3. Kessler RC, Magee WJ. Childhood adversities and adult depression: basic patterns of association in a US national survey. Psychol Med. 1993;23:679–690. doi:10.1017/S0033291700025460
4. Caspi A, Sugden K, Moffitt TE, et al. Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science. 2003;301:386–389. doi:10.1126/science.1083968
5. Takizawa R, Maughan B, Arseneault L. Adult health outcomes of childhood bullying victimization: evidence from a five-decade longitudinal British birth cohort. Am J Psychiatry. 2014;171:777–784. doi:10.1176/appi.ajp.2014.13101401
6. Tachi S, Asamizu M, Uchida Y, et al. Victimization in childhood affects depression in adulthood via neuroticism: a path analysis study. Neuropsychiatr Dis Treat. 2019;15:2835–2841. doi:10.2147/NDT.S220349
7. Bowes L, Joinson C, Wolke D, Lewis G. Peer victimisation during adolescence and its impact on depression in early adulthood: prospective cohort study in the United Kingdom. BMJ. 2015;350:h2469. doi:10.1136/bmj.h2469
8. Lereya ST, Copeland WE, Costello EJ, Wolke D. Adult mental health consequences of peer bullying and maltreatment in childhood: two cohorts in two countries. Lancet Psychiatry. 2015;2:524–531. doi:10.1016/S2215-0366(15)00165-0
9. Ormel J, Jeronimus BF, Kotov R, et al. Neuroticism and common mental disorders: meaning and utility of a complex relationship. Clin Psychol Rev. 2013;33:686–697. doi:10.1016/j.cpr.2013.04.003
10. Kendler KS, Kuhn J, Prescott CA. The interrelationship of neuroticism, sex, and stressful life events in the prediction of episodes of major depression. Am J Psychiatry. 2004;161:631–636. doi:10.1176/appi.ajp.161.4.631
11. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. Washington, D.C.: American Psychiatric Publication Inc.; 2013.
12. Nagata T, Mori K, Ohtani M, et al. Total health-related costs due to absenteeism, presenteeism, and medical and pharmaceutical expenses in Japanese employers. J Occup Environ Med. 2018;60:e273–e280. doi:10.1097/JOM.0000000000001291
13. Schultz AB, Chen CY, Edington DW. The cost and impact of health conditions on presenteeism to employers: a review of the literature. Pharmacoeconomics. 2009;27:365–378. doi:10.2165/00019053-200927050-00002
14. Antczak E, Miszczynska KM. Causes of sickness absenteeism in Europe-analysis from an intercountry and gender perspective. Int J Environ Res Public Health. 2021;18:11823. doi:10.3390/ijerph182211823
15. Kinman G. Sickness presenteeism at work: prevalence, costs and management. Br Med Bull. 2019;129:69–78. doi:10.1093/bmb/ldy043
16. Hayashida T, Shimura A, Higashiyama M, Fujimura Y, Ono K, Inoue T. Psychosomatic stress responses and sleep disturbance mediate the effects of irregular mealtimes on presenteeism. Neuropsychiatr Dis Treat. 2021;17:315–321. doi:10.2147/NDT.S292249
17. Shimura A, Yokoi K, Ishibashi Y, Akatsuka Y, Inoue T. Remote work decreases psychological and physical stress responses, but full-remote work increases presenteeism. Front Psychol. 2021;12:730969. doi:10.3389/fpsyg.2021.730969
18. Taya H, Shimura A, Ishibashi Y, Misaki S, Inoue T. [Presenteeism associated with job stress]. Psychiatry. 2020;62:1037–1043. Japanese.
19. Yang T, Shen YM, Zhu M, et al. Effects of co-worker and supervisor support on job stress and presenteeism in an aging workforce: a structural equation modelling approach. Int J Environ Res Public Health. 2016;13:72. doi:10.3390/ijerph13010072
20. Okumura Y, Higuchi T. Cost of depression among adults in Japan. Prim Care Companion CNS Disord. 2011;13:10m01082.
21. De Venter M, Elzinga BM, Van Den Eede F, et al. The associations between childhood trauma and work functioning in adult workers with and without depressive and anxiety disorders. Eur Psychiatry. 2020;63:1–28. doi:10.1192/j.eurpsy.2020.70
22. Furuichi W, Shimura A, Miyama H, et al. Effects of job stressors, stress response, and sleep disturbance on presenteeism in office workers. Neuropsychiatr Dis Treat. 2020;16:1827–1833. doi:10.2147/NDT.S258508
23. Oshio T, Tsutsumi A, Inoue A, Suzuki T, Miyaki K. The reciprocal relationship between sickness presenteeism and psychological distress in response to job stressors: evidence from a three-wave cohort study. J Occup Health. 2017;59:552–561. doi:10.1539/joh.17-0178-OA
24. Seki T, Shimura A, Miyama H, et al. Influence of parenting quality and neuroticism on perceived job stressors and psychological and physical stress response in adult workers from the community. Neuropsychiatr Dis Treat. 2020;16:2007–2015. doi:10.2147/NDT.S260624
25. Sameshima H, Shimura A, Ono K, et al. Combined effects of parenting in childhood and resilience on work stress in nonclinical adult workers from the community. Front Psychiatry. 2020;11:776. doi:10.3389/fpsyt.2020.00776
26. Enns MW, Cox BJ, Larsen DK. Perceptions of parental bonding and symptom severity in adults with depression: mediation by personality dimensions. Can J Psychiatry. 2000;45:263–268. doi:10.1177/070674370004500305
27. Eysenck SBG, Eysenck HJ, Barrett P. A revised version of the psychoticism scale. Person individ Diff. 1985;6:21–29. doi:10.1016/0191-8869(85)90026-1
28. Nakai Y, Inoue T, Toyomaki A, et al. A study of validity about Japanese version of neuroticism scores of the shortened EPQ-R.
29. Ando E, Kawakami N, Shimazu A, Shimomitsu T, Odagiri Y. Reliability and validity of the English version of the New Brief Job Stress Questionnaire.
30. Shimomitsu T, Haratani T, Nakamura K, et al. Final development of the Brief Job Stress Questionnaire mainly used for assessment of the individuals. In:Kato M, editor. The Ministry of Labor Sponsored Grant for the Prevention of Work-Related Illness, FY 1999 Report. Tokyo Medical College; 2000:126–164. in Japanese.
31. Kawakami N, Tsutsumi A. The Stress Check Program: a new national policy for monitoring and screening psychosocial stress in the workplace in Japan. J Occup Health. 2016;58:1–6. doi:10.1539/joh.15-0001-ER
32. Lerner D, Amick BC, Rogers WH, Malspeis S, Bungay K, Cynn D. The work limitations questionnaire. Med Care. 2001;39:72–85. doi:10.1097/00005650-200101000-00009
33. Takegami M, Yamazaki S, Greenhill A, Chang H, Fukuhara S. Work performance assessed by a newly developed Japanese version of the Work Limitation Questionnaire in a general Japanese adult population. J Occup Health. 2014;56:124–133. doi:10.1539/joh.13-0087-OA
34. Alonso C, Romero E. Aggressors and victims in bullying and cyberbullying: a study of personality profiles using the five-factor model. Span J Psychol. 2017;20:E76. doi:10.1017/sjp.2017.73
35. Persson R, Hogh A, Grynderup MB, et al. Relationship between changes in workplace bullying status and the reporting of personality characteristics. J Occup Environ Med. 2016;58:902–910. doi:10.1097/JOM.0000000000000822
36. Bianchi R. Burnout is more strongly linked to neuroticism than to work-contextualized factors. Psychiatry Res. 2018;270:901–905. doi:10.1016/j.psychres.2018.11.015
37. Lachowska BH. [Neuroticism, work demands, work-family conflict and job stress consequences]. Med Pr. 2014;65:387–398. Polish.
38. Hurrell JJ, McLaney MA. Exposure to job stress–a new psychometric instrument. Scand J Work Environ Health. 1988;14(Suppl 1):27–28.
39. Toyoshima K, Inoue T, Shimura A, et al. Mediating roles of cognitive complaints on relationships between insomnia, state anxiety, and presenteeism in Japanese adult workers. Int J Environ Res Public Health. 2021;18:4516. doi:10.3390/ijerph18094516
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.