Back to Journals » Neuropsychiatric Disease and Treatment » Volume 17
Ventilation Adjustment in ECT During COVID-19: Voluntary Hyperventilation is an Effective Strategy
Authors de Arriba-Arnau A ![]() , Dalmau Llitjos A, Soria V, Labad J, Menchón JM
, Dalmau Llitjos A, Soria V, Labad J, Menchón JM ![]() , Urretavizcaya M
, Urretavizcaya M
Received 27 January 2021
Accepted for publication 21 April 2021
Published 20 May 2021 Volume 2021:17 Pages 1563—1569
DOI https://doi.org/10.2147/NDT.S303877
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Aida de Arriba-Arnau,1,2 Antònia Dalmau Llitjos,3 Virginia Soria,1,2,4 Javier Labad,2,5,6 José Manuel Menchón,1,2,4 Mikel Urretavizcaya1,2,4
1Department of Psychiatry, Bellvitge University Hospital-ICS, Bellvitge Biomedical Research Institute (IDIBELL), Neurosciences Group - Psychiatry and Mental Health. L’Hospitalet de Llobregat, Barcelona, Spain; 2Centro de Investigación Biomédica en Red de Salud Mental (CIBERSAM), Carlos III Health Institute, Barcelona, Spain; 3Department of Anesthesiology, Reanimation and Pain Clinic, Bellvitge University Hospital-ICS, Universitat de Barcelona (UB), Barcelona, Spain; 4Department of Clinical Sciences, School of Medicine, Universitat de Barcelona (UB), Barcelona, Spain; 5Department of Mental Health, Consorci Sanitari del Maresme, Mataró, Spain; 6Parc Taulí, Institut d’Investigació i Innovació Parc Taulí (I3PT), Barcelona, Spain
Correspondence: Mikel Urretavizcaya
Sarachaga Department of Psychiatry. Bellvitge University Hospital – ICS, IDIBELL, CIBERSAM; UB Feixa Llarga s/n, 08907, L’Hospitalet de Llobregat, Barcelona, Spain
Tel +34 932607922
Fax +34 932607658
Email [email protected]
Purpose: Airway management is a key objective in adapted electroconvulsive therapy (ECT) protocols during the COVID-19 pandemic to prevent infection. The objective of this study was to describe the effectiveness of a modified ventilation procedure designed to reduce aerosol-generating bag-mask ventilation (BMV) and isolate possible droplets while maintaining adequate respiratory gas values in ECT sessions.
Materials and Methods: This prospective study analyzed the results of the modified protocol applied over a month. Adaptations entailed preoxygenation and extension of the voluntary hyperventilation (VHV) time for two minutes before anesthesia induction, asking patients to hyperventilate with oxygen therapy via nasal cannula and while wearing a face mask. Thereafter, vigorous hyperventilation was avoided, and patients were only assisted with tightly sealed BMV until emergence from anesthesia, isolating the ventilation by using a single-use plastic device. Oxygen saturation (SpO2) and transcutaneous partial pressure of carbon dioxide (TcPCO2) were recorded throughout the session.
Results: The study included 74 sessions of bilateral ECT with the modified ventilation protocol in 15 subjects. After VHV, the mean SpO2 increase was 2.12± 2.14%, and the mean TcPCO2 decrease was 4.05± 2.98 mmHg. TcPCO2 values at the moment of stimulus administration were 2.22± 3.07 mmHg below pre-ECT values. The mean EEG seizure was 38.70± 17.03 s, and postictal suppression was 68.31± 34.58% and 2.13± 0.75 on a 0– 3 scale. Brief desaturation (SpO2 < 90) of 4– 5 seconds duration was observed in 4 sessions.
Conclusion: This modified ventilation protocol was effective during COVID-19, and it did not elicit significant side effects. In addition to avoiding vigorous BMV, it induced moderate hypocapnia, which has been tied to seizure optimization and less hypercapnia during the apnea period.
Keywords: electroconvulsive therapy anesthesia, ECT, airway, bag-mask ventilation, oxygenation, self-hyperventilation, hypocapnia
Introduction
The quick overwhelming impact that the COVID-19 pandemic produced on many countries’ health care systems initially decreased the activity of some electroconvulsive therapy (ECT) units. Many physicians have claimed that this treatment should be administered to patients who need it despite current circumstances,1–3 and there is a clear and universal consensus that ECT is a critical and essential treatment.4,5
There are inherent aspects of ECT that increase its risk during the pandemic. Many patients are older adults who are at higher risk of COVID-19 than the general population and have comorbidities,5 the staff usually rotate, and the ECT procedure under anesthesia involves airway management requirements.6 Additionally, ventilation during the treatment facilitates aerosol dispersion,5,7 and COVID is transmitted through respiratory droplets. Hence, the ECT procedure has been rapidly adapted with changes intended to maintain safety for patients and staff.5
One of the key ECT-specific procedure changes in clinical practice to minimize infection exposure is airway management. Several modifications in terms of ventilation during the ECT application technique have been proposed, but unfortunately, the impact of many of these interventions on ECT results has not been studied.
Hyperventilation is widely recommended in ECT guidelines because it is a simple and effective strategy for improving seizure quality and patient safety.8 However, in the setting of COVID-19, some authors recommend avoiding or minimizing hyperventilation because it is usually performed by manual bag-mask ventilation (BMV).6 BMV is an aerosol-generating or droplet dispersion procedure5,9,10 due to its poor airway seal, which poses the greatest exposure risk to patients and staff.5 Other authors proposed improving preoxygenation instead,1 with a regular or nonrebreather mask for several minutes pretreatment5 and avoiding BMV unless severe desaturation occurred,10 but some patients still require BMV.5,10
The use of procedures that allow a good airway seal through more invasive methods has also been recommended by some authors. However, using tracheal intubation in all patients may prolong the ECT procedure and induce gagging and coughing.11 Others recommended the use of supraglottic airways (establishing a closed circuit system and extubating under a plastic tent) because its insertion and removal limits aerosolization more than tracheal intubation.7 It has also been proposed that ECT should be administered in an operating room setup with negative pressure, if available,9 especially if the patient is ill with COVID-19, but this is not always available in all centers.5
The aim of this study was to describe the effectiveness of a modification to the ventilation procedure protocol proposed during the COVID-19 pandemic that addresses the need to reduce aerosol-generating BMV and isolate possible droplets. We hypothesize that by implementing voluntary hyperventilation, hypocapnia and adequate oxygenation can be optimized.
Materials and Methods
We prospectively collected data from the sessions performed in the ECT Unit of the Bellvitge University Hospital during June 2020 using a ventilation protocol that addresses the need to reduce aerosol-generating bag-mask ventilation and isolate possible droplets during the COVID-19 pandemic.12 We analyzed the effectiveness of this protocol in reaching adequate values of respiratory gases in ECT sessions and adequate seizures. All patients provided written informed consent, and the study was approved by the Bellvitge University Hospital Clinical Research Ethics Committee. All procedures were performed according to the Declaration of Helsinki.
Bilateral ECT was applied using a Thymatron System IV device (Somatics, LLC, Lake Bluff, III). Anesthesia was induced with thiopental (1.5–2.5 mg/kg) or etomidate (0.1–0.3 mg/kg), and succinylcholine (~0.5 mg/kg), adapting dosages to patients’ needs. Concomitant psychotropic medications were maintained during the treatment course.
The standard ECT procedure was adapted by a multidisciplinary team covering mainly prevention of infection risk and the airway management maneuvers involved in modern ECT. A specific hospital protocol (Electroconvulsive therapy procedure during the COVID-19 pandemic (v15.05.2020)), which followed the recommendations of international (International Society of ECT and Neurostimulation (ISEN)11) and Spanish societies (the Spanish Society of Biological Psychiatry (SEPB) general recommendations to adapt the practice of electroconvulsive therapy during the COVID-19 pandemic6), local COVID-19 guidelines, and the current literature,7,9,10,13 was developed. This protocol was approved by the hospital’s quality department and was applied in all patients treated with ECT.
The ECT unit applied structural adjustments to keep a safe distance and a separated clean circuit patient flow; organizational changes included keeping minimum staff during the treatment; controlled appointment time; a decreased number of patients; natural ventilation of the room for 15–30 minutes to allow more air recirculation between patients and cleaning with disinfectant wipes between patients; and a comprehensive intensive room cleaning protocol applied at the end of the day sessions or between outpatients’ and inpatients’ sessions.
Before entering the ECT Unit, patients underwent a screening for potential contact with COVID-19 patients, reported clinical symptoms, vital signs, respiratory rate, SpO2, temperature control, negative polymerase chain reaction (PCR) testing for SARS-CoV-2 (in the last 48 h), and absence of respiratory symptoms. Patients wear protective surgical face masks at all times inside the ECT unit,14 and the staff also wears the required personal protective equipment (PPE).
The half-age method of stimulation15 was used to avoid titration restimulations and possible lengthening of the session duration and the time the patient was not being ventilated, and succinylcholine was optimized at the lower dose range for a quicker return to spontaneous breathing after the seizure.5
During the treatment, a single-use standard nasal cannula was used for oxygenation,9 and single-use adherent stimulus electrodes were used to prevent contamination and cross-infection and maintain distance. A disinfected mouth guard that allowed ventilation through itself was appropriately placed before the patient was anesthetized. Further manipulation of the airway, such as the introduction of the Guedel cannula, was avoided when possible. Additionally, a single-use disposable plastic cover with an adaptable hole to connect the disinfected bag mask and antimicrobial air filter was used to prevent aerosol spreading.
Changes to the usual ventilation procedure were applied to minimize aerosol generation and droplet dispersion while maintaining adequate respiratory gases and seizure parameters. The modifications included preoxygenation with a single-use nasal cannula with oxygen at ≈4 L/min below the protective surgical face mask that patients wore. Then, to decrease TcPCO2 basal values, voluntary hyperventilation (VHV) was performed asking the patient to self-hyperventilate for 2 minutes before anesthetic induction. Afterwards, once the patient was asleep, the waterproof plastic cover was in place to isolate ventilation and the airways. The protocol avoids vigorous BMV manual hyperventilation and mouth manipulation if possible, performing ventilation through the mouth guard if needed and maintaining oxygenation and manual ventilation assistance with a tight sealed BMV under the plastic tent until the patient recovers spontaneous breathing.12
Patients underwent continuous monitoring throughout all sessions using assessments of electrocardiogram, blood pressure, oxygen saturation (SpO2) by pulse oximetry (Datex Engstrom AS/3™ (Datex-Engström, Helsinki, Finland) anesthesia monitor), and transcutaneous partial pressure of carbon dioxide (TcPCO2) using a noninvasive estimation of partial arterial CO2 pressure (SenTec® Digital Monitoring System (SenTec AG, Therwil, Switzerland)).
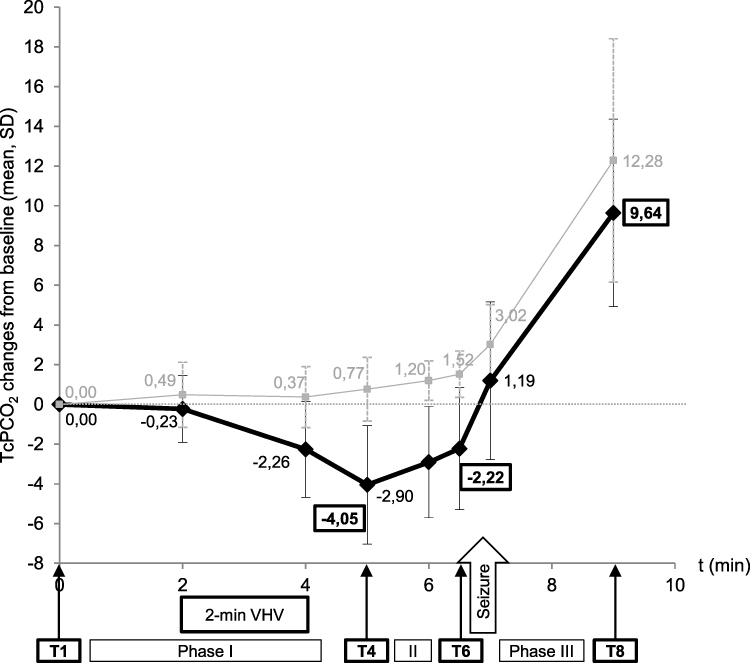
TcPCO2 was continuously monitored throughout all sessions, and TcPCO2 values were specifically recorded at each phase of ventilation management: T1, basal values of TcPCO2 before the treatment session; T2, during preoxygenation and at the beginning of voluntary hyperventilation; T3, at the end of voluntary hyperventilation and beginning of anesthesia induction; T4, minimum value achieved after the 2-min voluntary hyperventilation; T5, after manual ventilation assistance performed avoiding vigorous hyperventilation, once the patient is asleep; T6, values at the moment of ECT stimulus delivery; T7, values at the end of the seizure; T8, post-ECT period value after patient’s recovery of autonomous breathing and consciousness and at the time of transferring the patient to the recovery room.
The main values considered in the study were T1, T4, T6, and T8 (see Figure 1).


Seizure characteristics were determined by 2-channel electroencephalogram (EEG), duration and postictal suppression index (PSI) were provided by the Thymatron device, and the motor and EEG seizure duration plus the postictal suppression rating (PSIr) using a 0–3 scale16,17 were determined visually by a psychiatrist with expertise in ECT.
Statistical analyses were performed using SPSS v19.0 (SPSS, an IBM company, Chicago, Illinois, USA); R18 and R studio.19 The statistical significance was set at p<0.05 (bilateral).
To study the TcPCO2 dynamics during the sessions that is presented in Figure 1, R and R studio were used for exploring longitudinal changes in TcPCO2 after VHV. The lme4 package was used for fitting linear mixed effect models with the maximum likelihood method. Fixed effects were considered for the number of ECT sessions, time, and cooperation with the VHV procedure. Random effects were assigned to each participant. Time and cooperation variables were defined as factors, and the interaction between time and cooperation was tested. The reference categories for these two factors were baseline time (T1) and lack of cooperation. With this decision, the model allows to estimate the changes in TcPCO2 from baseline time and to consider whether the change at each time depends upon the cooperation of the patient with the VHV procedure (tested with an interaction).
Pearson correlations were used to analyse the relationships between ventilation parameters and seizure characteristics (duration and postictal suppression).
Results
A total of 74 sessions in 15 consecutive patients were performed during the study period. In seven of these sessions, patients were unable to cooperate with the proposed VHV maneuvers due to their clinical status.
The characteristics of the sample, the ventilation parameters, and the seizures obtained while performing this ventilation approach are presented in Table 1.
 |
Table 1 Ventilation Parameters and Demographic, Clinical, and ECT Characteristics of the Study Population |
After VHV, the mean SpO2 increase was 2.12±2.14%, and the mean decrease in TcPCO2 from basal values was 4.05±2.98 mmHg. CO2 dynamics during the sessions are presented in Figure 1.
After anesthetic induction, TcPCO2 values increased because vigorous hyperventilation was avoided to prevent aerosol generation. Nevertheless, a mean reduction from baseline values of 2.22±3.07 mmHg in TcPCO2 was still maintained at the moment of stimulus administration.
Changes in TcPCO2 during the ECT procedure by cooperation with the VHV procedure are described in Figure 1. The linear mixed model analysis testing the contribution of time and cooperation shows that changes at T7 and T8 (after the seizure) are significant from baseline independently of the cooperation, although there are significant differences, with lower TcPCO2 concentrations, in the group of participants who cooperated with the VHV, at times T4 and T5 (before the seizure). This analysis was adjusted for the number of ECT sessions. The results of the fixed effects are shown in Table S1.
EEG duration correlated with the oxygen increase at the ECT stimulus delivery (T6) (r=0.41, p=0.001). PSI was correlated with the TcPCO2 decrease at T4 (r=0.31, p=0.031) and TcPCO2 values after VHV at T4 (r=−0.26, p=0.037) and the ECT stimulus delivery (T6) (r= −0.33, p=0.009).
In 4 sessions, SpO2<90% was observed after the seizure, and these values recovered 4–5 seconds after restarting ventilation support. All 4 instances occurred in patients with baseline SpO2<95% and long seizures; all were smokers, and one of these patients was obese. No other complications were noted.
Finally, in the 7 sessions where the patients were unable to cooperate with the 2-minute VHV, the mean post-ECT SpO2 was 95.57% and TcPCO2 monitoring showed higher values than baseline after anesthesia induction (Figure 1).
Additionally, the mean seizure duration was shorter (motor 19.14±6.51 s and EEG 27.86±6.33 s) than in the sessions of patients who cooperated in VHV (analyzed in Table 1), while the PSI was similar.
Discussion
The results of this modified ventilation protocol, including preoxygenation and 2-minute VHV, while avoiding vigorous BMV hyperventilation, were analyzed. These changes in the ventilation procedure were implemented due to the COVID-19 pandemic and effectively induced moderate hypocapnia without eliciting significant side effects.
The mean TcPCO2 decreases after two minutes of VHV (−4.05 mmHg) and almost doubled the values of the one-minute VHV tested in a previous protocolized hyperventilation procedure (−2.61 mmHg).20 This finding reinforces the notion that VHV performed actively by the patient before anesthesia induction is an important maneuver to decrease TcPCO220 and suggests that a longer duration of VHV performance might further reduce the achieved TcPCO2 values. In standard electroencephalography recordings, VHV for longer periods (usually approximately 3 minutes) was reported as a safe widespread epileptogenic activation maneuver for seizure provocation without significant side effects.21 Additionally, VHV has been allowed in EEG recommendations for COVID-19-negative patients or when the absence of seizures is suspected despite no prior testing being available.22
In our study, a reduction of 2.22 mmHg from baseline was maintained until the stimulus application moment, with similar values to the 2.18 decrease reached at T3 in the previous PHV procedure.20 This decrease in approximately 2 points from the patient’s basal values was associated with reduced hypercapnia and lower TcPCO2 over the whole session, as well as increased seizure duration and correlation with seizure quality indexes.20
Furthermore, because some sites use different lengths of preoxygenation and others use patients self-hyperventilation, and since it has been proposed that these maneuvers may allow for the elimination of BMV in some cases,5 the present study findings are reassuring and illustrate the effectiveness of these maneuvers in everyday clinical ECT practice in terms of ventilation gases and seizure parameters.
Desaturation can occur during ECT, especially in patients with risk factors (obesity,10,23,24 high seizure length,23 baseline respiratory compromise10), and ventilation management is important to prevent this. Patient positioning, ventilation maneuvers, airway devices, and neuromuscular blocking agent recommendations have been reported to minimize desaturation incidence in morbidly obese patients.24 Using our study’s proposed ventilation approach, SpO2<90% occurred in only 5.9% of sessions. However, in another recent study where 3–5 minute preoxygenation was performed with a nonrebreather mask while avoiding BMV hyperventilation before the stimulus, SpO2 decreased below 85% during the apneic period in 51/106 (48.1%) of the patients, and BMV was required to recover adequate saturations.10 Of note, CO2 was not measured, so the incidence of hypercapnia could not be quantified, but EEG seizure duration was found to be slightly reduced.10
Some limitations of this study merit discussion. The study described the results of the modified ECT protocol in our unit; however, the changes in ventilation procedures applied are easy and replicable in other centers, and they are applicable even if CO2 monitoring is not available. Analyses were exploratory and could be underpowered because of the relatively small sample size, and due to the observational design there was not a proper comparison group.
Conclusion
Our findings suggest that preoxygenation and 2 minutes of VHV is useful and well tolerated during the COVID-19 pandemics because, in addition to minimize BMV hyperventilation, it still induces moderate hypocapnia, which has been tied to seizure optimization and less hypercapnia during the apnea period in ECT sessions. Additionally, the results strengthen the importance of preoxygenation24 and support the role of VHV, the impact of ventilation in gas dynamics during ECT sessions,20,25 and the relevance of CO2 and O2 values in the obtained seizure characteristics.8
Acknowledgments
We appreciate the participation from all the patients, their relatives and the staff from the ECT Unit of Bellvitge University Hospital. We also thank the CERCA Programme/Generalitat de Catalunya for institutional support.
Disclosure
Dr José Manuel Menchón reports personal fees from Janssen, personal fees from AbBiotics, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Sienaert P, Lambrichts S, Popleu L, Van Gerven E, Buggenhout S, Bouckaert F. Electroconvulsive therapy during COVID-19-times: our patients cannot wait. Am J Geriatr Psychiatry. 2020;28(7):772–775. doi:10.1016/j.jagp.2020.04.013
2. Espinoza RT, Kellner CH, McCall WV. Electroconvulsive therapy during COVID-19: an essential medical procedure-maintaining service viability and accessibility. J ECT. 2020;36(2):78–79. doi:10.1097/YCT.0000000000000689
3. Tor PC, Phu AHH, Koh DSH, Mok YM. Electroconvulsive therapy in a time of coronavirus disease. J ECT. 2020;36(2):80–85. doi:10.1097/YCT.0000000000000690
4. APA. Practice Guidance for COVID-19. 2020. Available from: https://www.psychiatry.org/psychiatrists/covid-19-coronavirus/practice-guidance-for-covid-19.
5. Lapid MI, Seiner S, Heintz H, et al. Electroconvulsive therapy practice changes in older individuals due to COVID-19: expert consensus statement. Am J Geriatr Psychiatry. 2020;28(11):1133–1145. doi:10.1016/j.jagp.2020.08.001
6. Martínez Amorós E, Urretavizcaya M Recomendacines generales de la SEPB para adaptar la práctica de la terapia electroconvulsiva durante la pandemia de COVID-19. https://sepb.es/webnew/wp-content/uploads/2020/05/TEC-COVID.pdf.
7. Thiruvenkatarajan V, Dharmalingam A, Armstrong-Brown A, Weiss A, Waite S, Van Wijk R. Uninterrupted anesthesia support and technique adaptations for patients presenting for electroconvulsive therapy during the COVID-19 era. J ECT. 2020;36(3):156–157. doi:10.1097/YCT.0000000000000707
8. Gómez-Arnau J, de Arriba-arnau A, Correas-Lauffer J, Urretavizcaya M. Hyperventilation and electroconvulsive therapy: a literature review. Gen Hosp Psychiatry. 2018;50:54–62. doi:10.1016/j.genhosppsych.2017.09.003
9. Flexman AM, Abcejo AS, Avitsian R, et al. Neuroanesthesia practice during the COVID-19 pandemic: recommendations from Society for Neuroscience in Anesthesiology and Critical Care (SNACC). J Neurosurg Anesthesiol. 2020;32(3):202–209. doi:10.1097/ANA.0000000000000691
10. Luccarelli J, Fernandez-Robles C, Fernandez-Robles C, et al. Modified anesthesia protocol for electroconvulsive therapy permits reduction in aerosol-generating bag-mask ventilation during the COVID-19 pandemic. Psychother Psychosom. 2020:1–6. doi:10.1159/000509113.
11. International Society for ECT and Neurostimulation (ISEN). COVID-19 and ECT. 2020. Available from: https://isen-ect.org/sites/default/files/ISEN.COVID19.letter.pdf.
12. de Arriba-arnau A, Dalmau Llitjos A, Soria V, Menchón JM, Urretavizcaya M. Adaptation of ventilation in ECT sessions during the COVID-19 pandemic. J ECT. 2021;00(00):00. doi:10.1097/YCT.0000000000000748
13. Gil-Badenes J, Valero R, Valentí M, et al. Electroconvulsive therapy protocol adaptation during the COVID-19 pandemic. J Affect Disord. 2020;276:241–248. doi:10.1016/j.jad.2020.06.051
14. Montero Feijoo A, Maseda E, Adalia Bartolomé R, et al. Practical recommendations for the perioperative management of the patient with suspection or serious infection by coronavirus SARS-CoV. Rev Esp Anestesiol Reanim. 2020;67(5):253–260. doi:10.1016/j.redar.2020.03.003
15. Petrides G, Fink M. The “half-age” stimulation strategy for ECT dosing. Convuls Ther. 1996;12(3):138–146.
16. Martin DM, Gálvez V, Lauf S, et al. The clinical alliance and research in electroconvulsive therapy network. J ECT. 2017;1. doi:10.1097/YCT.0000000000000435
17. Nobler MS, Sackeim HA, Solomou M, Luber B, Devanand DP, Prudic J. EEG manifestations during ECT: effects of electrode placement and stimulus intensity. Biol Psychiatry. 1993;34(5):321–330.
18. R Core Team. R: A Language and Environment for Statistical Computing [Website]. Vienna, Austria: R Foundation for Statistical Computing; 2020. Available from: https://www.r-project.org/.
19. RStudio Team. RStudio: Integrated Development for R [Website]. Boston, MA: RStudio, PBC; 2020. Available from: http://www.rstudio.com/.
20. de Arriba-arnau A, Dalmau A, Soria V, et al. Protocolized hyperventilation enhances electroconvulsive therapy. J Affect Disord. 2017;217:225–232. doi:10.1016/j.jad.2017.04.007
21. Kane N, Grocott L, Kandler R, Lawrence S, Pang C. Hyperventilation during electroencephalography: safety and efficacy. Seizure. 2013;23(2):129–134. doi:10.1016/j.seizure.2013.10.010
22. Vidaurre J, Islam MP, Mytinger JR. Pediatric EEG and the COVID-19 pandemic: can we develop a safe transition pathway to reopen our laboratories? J Pediatr Epilepsy. 2020;09(02):029–030. doi:10.1055/s-0040-1712911
23. Surve R, Bansal S, Sriganesh K, Subbakrishna DK, Thirthalli J, Umamaheswara Rao GS. Incidence and risk factors for oxygen desaturation during recovery from modified electroconvulsive therapy: a prospective observational study. J Anaesthesiol Clin Pharmacol. 2015;31(1):99–103. doi:10.4103/0970-9185.150555JOACP-31-99
24. Koyama Y, Tsuzaki K, Suzuki T, Ozaki M, Saito S. Prevention of oxygen desaturation in morbidly obese patients during electroconvulsive therapy. J ECT. 2020;36(3):161–167. doi:10.1097/YCT.0000000000000664
25. Aksay SS, Bumb JM, Janke C, Hoyer C, Kranaster L, Sartorius A. New evidence for seizure quality improvement by hyperoxia and mild hypocapnia. J ECT. 2014;30(4):287–291. doi:10.1097/YCT.0000000000000109
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.