Back to Journals » Infection and Drug Resistance » Volume 17
Venous Thromboembolism and Associated Factors in Hospitalized Patients with COVID-19 at Addis Ababa COVID-19 Field Hospital, Ethiopia
Authors Haile AT ![]() , Haile RG
, Haile RG ![]() , Gebrehiwot EH, Abeje EW
, Gebrehiwot EH, Abeje EW
Received 11 December 2023
Accepted for publication 19 January 2024
Published 26 January 2024 Volume 2024:17 Pages 305—317
DOI https://doi.org/10.2147/IDR.S449401
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Abel Teklit Haile,1,2 Robel Gemechu Haile,1– 3 Esrom Hagos Gebrehiwot,1– 3 Eden Workalemahu Abeje1– 3
1Research Department, Saint Peter Specialized Hospital, Addis Ababa, Ethiopia; 2Department of Internal Medicine, Wollo University, Dessie, Ethiopia; 3School of Public Health, Gamby Medical and Business College, Addis Ababa, Ethiopia
Correspondence: Abel Teklit Haile, Email [email protected]; Robel Gemechu Haile, School of Public Health, Gamby Medical and Business College, Addis Ababa, Ethiopia, Email [email protected]
Background: The association of COVID-19 with venous thromboembolism is of particular interest as there are reports that have associated thrombotic events with the pandemic. COVID-19 may predispose to venous thromboembolism. There is initial evidence suggesting that individuals with COVID-19 may be more prone to developing venous thromboembolism (VTE). This study aims to assess venous thromboembolism and associated factors in 19 patients admitted to Addis Ababa’s field hospital for COVID-19.
Objective: To identify associated factors that affect the development of thromboembolism in patients admitted with the diagnosis of COVID-19.
Methods: To determine the risks of VTE patients, an institution-based case control research was conducted using SPSS version 26, multivariable binary logistic regression analysis was used.
Results: Significant factors associated with the development of VTE in COVID-19 patients included having a severe case (AOR = 0.38, 95% CI = 0.149– 0.961), risk factors for VTE (AOR = 2.57, 95% CI = 1.18– 5.33), diabetes (AOR = 3.745, 95% CI = 1.715– 8.176), chest pain (AOR = 4.13, 95% CI = 1.89– 9), stage 1 hypertension levels (AOR = 3.67, 95% CI = 1.37– 9.836), and hospital anticoagulation (AOR = 11.78, 95% CI = 5.25– 26.4).
Conclusion: The results of VTE in individuals with COVID-19 imply a direct association between severe COVID-19 and diabetes, having risk factors, hypertension, and hospital anticoagulation.
Keywords: COVID-19, venous thromboembolism, case control, logistic regression, Addis Ababa, Ethiopia
Background
Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) is a new coronavirus that first appeared in Wuhan, China, toward the end of 2019. Since then, it has spread to over 190 countries worldwide. According to reports from March 2021, there were over 117 million confirmed cases worldwide, with an estimated 2,600,000 deaths across 220 nations, translating into a fatality rate of almost 2%, at that time.1 The severity of the disease has different categories, ranging from asymptomatic to critical.2 In March 2021, it was reported that there were more than 117 million confirmed cases in the world, and the total number of deaths in the world was around 2,600,000 in 220 countries, with a mortality rate of around 2%.3 Acute Respiratory Distress Syndrome (ARDS), a prominent complication of COVID-19, is linked to a substantial mortality rate and stands as the primary contributor to fatalities.4
One of the worst effects of the illness is venous and arterial thrombosis, which also has a dismal prognosis.5 Patients with COVID-19 may have an increased risk of thrombotic consequences as a result of platelet activation, endothelial dysfunction, excessive inflammatory response, and blood flow stasis.6 Due to high inflammation in vascular systems there have been different cardiovascular complications.7 Early research on COVID-19 individuals described coagulopathy and aberrant coagulation with a somewhat prothrombotic character.8
Venous thromboembolism (VTE), a disease category that includes pulmonary embolism (PE) and deep vein thrombosis (DVT), has been identified as a specific complication of COVID-19 because of improved knowledge of the virus and its clinical course. High rates of VTE were found in those categorized as having severe COVID-19 that were admitted to the ICU.9
Knowing the actual frequency of VTE in COVID-19 is crucial and may aid in supporting clinical decision-making, especially in view of the rapidly rising infection rates around the world and the clinical difficulties in patient treatment. A prior meta-analysis with 1,783 patients who were seriously infected revealed 12.7% diagnosis rates for VTE.10
Added to the risk factors, COVID-19 has been associated with hypercoagulability that predisposes to thrombotic states.11,12 Zhou et al discovered thrombotic events in 2.9% of their patient sample when they initially revealed a link between COVID-19 and venous thromboembolism (VTE). Prior Asian research found that thromboembolic events were associated with a poor prognosis for about 25% of COVID-19 patients in intensive care units.13 According to reports, venous thromboembolism (VTE) affects 27–69% of critically ill SARS–CoV–2 patients.14 A common presentation of risk factors for venous thromboembolism (VTE) in hospitalized pneumonia patients is respiratory illness, infections, reduced movement, elders (>65 years), malignancies, overweight, pregnancy, heart failure, or a prior case of VTE.15,16
Methods
Study Area and Period
This study employed a case-control study design to explore the occurrence of venous thromboembolism (VTE) among inpatients admitted to the Addis Ababa COVID-19 field hospital. The study was conducted from October 15, 2021, to February 20, 2022. The source population comprised every admitted patient to the field hospital with a diagnosis of COVID-19 that used Real Time Polymerase Chain Reaction (RT-PCR), as mandated by the Federal Ministry of Health Ethiopia.17
a) Case: Every patient who was admitted to the field hospital with VTE and COVID-19 infection and was found to be infected by RT-PCR.
b) Control: Every patient with COVID-19 infection confirmed by RT-PCR who was admitted to the field hospital and did not have VTE (PE/DVT).
This case-control study aims to provide insights into the relationship of COVID-19 and the occurrence of VTE among the patients who were admitted to the field hospital within the allotted time. Sample size determination for the study utilized a difference in proportion formula, assuming an odds ratio of 2, a proportion exposed in the control group of 40%, and aiming for an 80% power level at a 0.05 significance level. The calculated sample size was 19.6 and, to ensure practicality and with a 1:2 case-to-control ratio, 398 participants (106 cases and 292 controls) were included in the final sample.
The selection of controls was done by simple random sampling. Data were compiled from charts and EMR registrations. A complete list of patients admitted was obtained from electronic data and a sampling frame was constructed using medical record number for the controls. Cases were selected by screening all the charts and EMR data within the study period with the diagnosis of VTE.
Study Variables
Dependent variables: Events of venous thromboembolism in COVID-19 patients.
Independent variables: Age, sex, residence.
Clinical factors: Cough, sore throat, arthralgia, fever, shortness of breath, headache, myalgia, fatigue, hemoptysis, leg swelling, chest pain, palpitation, COVID-19 category, vital signs.
Laboratory-related factors: WBC count, lymphocytes, prothrombin time, activated partial thromboplastin time, hemoglobin, platelets, INR.
Comorbid factors: Diabetes, hypertension, dyslipidemia, malignancy, asthma, CKD, CHF.
Management-related factors: Baseline investigations, ICU admission, anticoagulation.
Operational Definition
The WHO categorization was used to calculate the COVID-19 severity score, which is as follows: 1) Moderate disease: patients with one or more lower respiratory symptoms; mild disease: fever, malaise, cough, upper respiratory symptoms, and/or less prevalent COVID-19 characteristics. On a chest X-ray, they might have infiltrated. On room air, these patients can sustain their oxygenation.
DVT diagnosis: Duplex ultrasonography diagnoses DVT by finding blood clots or obstructions in the deep veins. It is the typical imaging test used to identify DVT and was used for this study.18
Risk factors for VTE were determined based on Wells score. This is the most well-known clinical likelihood assessment instrument for VTE that is clinically suspected which includes obesity, active cancer, history of VTE, history of surgery, current estrogen use, stroke, and trauma to the extremities.19,20
Pulmonary thromboembolism: A diagnosis is made when a thrombus, or blood clot, lodges in a pulmonary artery and prevents blood flow to the lung. The gold standard for diagnosing pulmonary embolism in this investigation was computed tomography angiography.21
Data Collection, Technique, Data Management, and Analysis
Patient medical data, extracted through an English-language abstraction tool from various research studies and physician notes, was collected by two general practitioners, one serving as a supervisor. Daily checks by the supervisor and principal investigator ensured data completeness and consistency before entry into Epi-info version 7.2.1.0. After cleaning and coding, data was exported to SPSS version 26.0 for analysis. Categorical covariates were summarized using frequencies and percentages. Chi-square tests (for categorical) and independent t-tests (for numerical variables) assessed differences between cases and controls. Variables with a p-value ≤0.05 were deemed statistically significant. Binary logistic regression examined the association between VTE risk factors and variables. Univariate analysis calculated adjusted odds ratios, with variables having p ≤0.25 considered for the multiple regression model. A final model’s adequacy was tested using the Hosmer-Lemeshow goodness-of-fit test, ensuring robust statistical analysis of VTE development.
Results
Demographic, Co-Morbid Illness, and Risk Factors Associated between Cases (VTE) and Controls (without VTE)
The incidence of VTE was considerably greater in those 50 years of age and older (64%) than in the other age groups (18.9% and 17%). The age group of 39–49 years old accounted for the lowest percentage of patients (14.8%), with the bulk of patients (43%) being younger than 39. Males had VTE development at a higher rate (63.8%) than females (56.6%), suggesting a gender-related trend. Most patients were from urban areas (68.1%). A higher proportion of participants with severe COVID-19 had VTE in comparison with those in the mild COVID-19 category (69.8% vs 12.7%). The commonest COVID category was the non-severe group 287 (72.1%), followed by severe cases 111 (27.9%).
One fourth of the participants had at least one risk factor for VTE (10; 27.4%). The most common was current estrogen use (8%), followed by trauma to the extremities (4.8%), active cancer (4.8%), obesity (3.5%), stroke (3.3), history of surgery (3.3%), and history of VTE (2.8%).
The most common comorbid illness was hypertension (27.6%) Diabetes mellitus was the subsequent leading factor (25.1%), followed by cardiac illness (8.8%), HIV (3.3%), asthma (3%), chronic liver disease (1.8%), COPD (1.3%), CKD (1.3%), and tuberculosis (0.5%)
Like those without diabetes mellitus, patients with diabetes also showed a significant correlation with VTE (48.1% vs 16.8%, p-value = 0.001). On the other hand, VTE episodes occurred in a significant percentage of those with a history of hypertension (50% vs 19.5%, p-value = 0.001).
Presenting Symptom-Related Variables and Comparison between Cases (VTE) Vs Controls (without VTE)
At the time of admission, nearly every patient had a history of one or more symptoms. The most common complaints were cough (69.1%), headache (57.3%), and sore throat (46%), then exhaustion (59%), dyspnea (41.2%), arthralgia (33.2%), fever (359.9%), palpitations (24.9%), leg swelling (17.3%), lower limb discomfort (15.3%), and hemoptysis (5.8%).
Compared to individuals without VTE, a notably greater percentage of those with VTE (87.7 vs 24.3%, p = 0.0001) had SOB. A greater percentage (51.9 vs 48.1) of those with VTE experienced lower limb pain (Table 1).
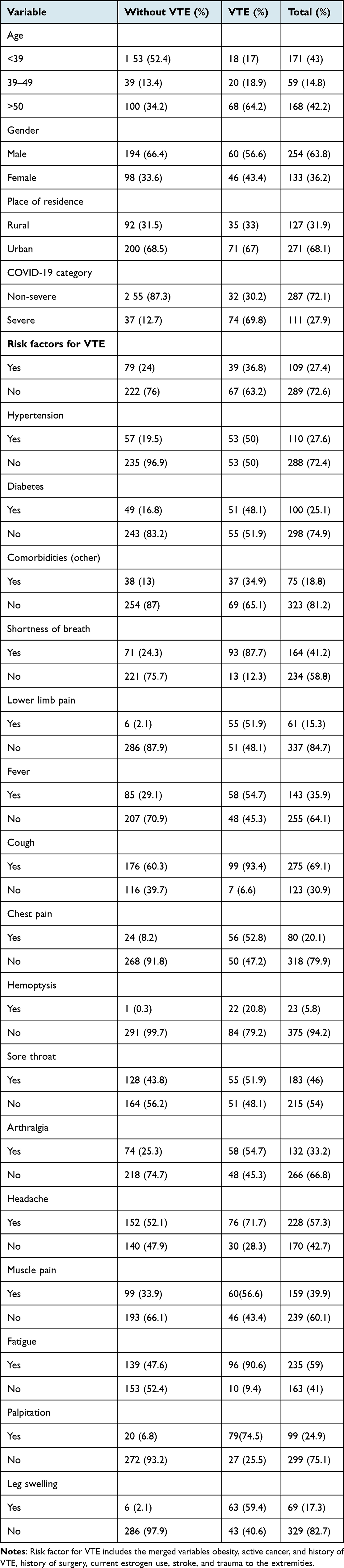 |
Table 1 Comparison of Soci odemographic, Co-Morbid Conditions, Risk Variables, and Presenting Symptoms between VTE Case s and Controls (without VTE) |
Initial Vital Signs, Laboratory Outcomes, and Management-Associated Variables
Cases
Amongst cases, 80 (75.5%) had severe hypoxia while 5.7% had normal saturation. The majority of the cases had a normal temperature (78; 73.6%) compared to those with fever (28; 26.4%) The majority of cases (43; 40.6%) exhibited normal blood pressure, with mean systolic and diastolic blood pressure values of 124 and 79, respectively. Thirty-seven (34.9%) cases had stage 2 hypertension. More than one third of the cases had a normal heart rate (80; 75.5%) compared to those with tachycardia, which was 26 (24.5%). Two thirds of the cases had tachypnea compared to those with normal respiratory rate (63.2% vs 36.8%).
The majority of the cases had normal WBC count compared with those with leukocytosis (63.2% vs 36.8%), lymphopenia compared to lymphocytosis (63.2% vs 10.4%), and more than one third had a normal hemoglobin level (85; 80.2%) while 21 (19.8%) had anemia. The majority of the cases had a normal platelet count (17.9 vs 82.1). One third of the cases had a normal prothrombin time, while 39 (42.9%) had results that were prolonged and more than one third had missing values (165; 41.5%). It was therefore decided to exclude this calculation and the same goes for activated partial prothrombin time and INR.
The majority of the cases received anticoagulation (84; 79.2%), while 22 (20.8%) did not receive hospital anticoagulation. Three fourths of the patients (97; 91.5%) were not on antiplatelet management and 71 (67%) received steroids as management. Almost all cases did not receive antiviral treatments (98; 92.5%) with 25 (23.6%) of the cases resorted to invasive mechanical ventilation. The majority of the cases (52; 49.1%) had a length of admission of 9–19 days.
Controls
Among the controls, 131 (44.9%) of them had mild hypoxia with 22.9% of them classified as having severe hypoxia. Almost one third of the controls (68.5%) had normal temperature and the mean systolic and diastolic blood pressure was 124 and 79, respectively, with 226 (77.4%) patients having normal blood pressure and 34 (11.6%) having stage 2 hypertension. Two hundred and seventy-one (92.8%) patients had a normal heart rate, while 21 (7.2%) had tachycardia; the majority of the controls had a normal heart rate (228; 78.1%).
Out of the total controls, 85 (30.6%) had leukocytosis, 126 (45.3%) had lymphocytosis, and 44 (15.8%) had lymphopenia. More than one third of the population had a normal hemoglobin level (251; 90.3%), with 27 (9.7%) having anemia. Almost all the patients had a normal platelet count (269; 96.8%), while 9 (3.2%) had thrombocytopenia. Two thirds of the patients had a normal prothrombin time, while 4 (2.8%) had results that were prolonged and more than one third had missing values (165; 41.5%). It was therefore decided to exclude this measure, and the same goes for activated partial prothrombin time and INR.
The majority of the patients (256; 87.7%) did not receive anticoagulation, while 36 (12.3%) were anticoagulated. Three fourths of the patients (267; 91.4%) were not on antiplatelet management and 51 (17.5%) received steroids as management. Almost all did not receive antiviral treatments (289; 99%), with 7 (2.4%) resorting to invasive ventilation (Table 2).
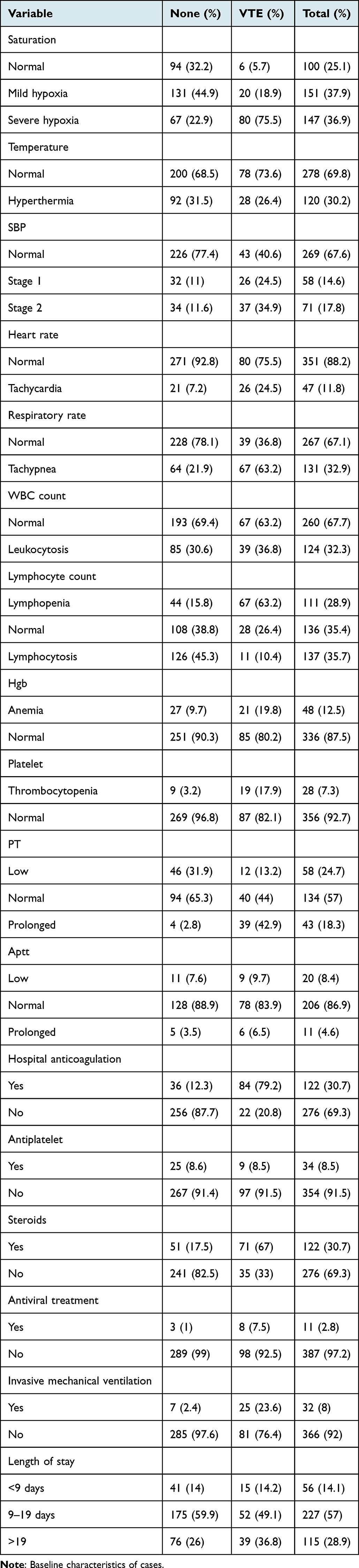 |
Table 2 Baseline Vital Signs, Factors Linked to the Laboratory and Management, and Comparison |
Factors Linked to COVID-19 Participants’ VTE Outcomes
In accordance with the findings of the univariate analysis at the 25% significance; age, COVID-19 category, risk factor for VTE, hypertension, diabetes, fever, chest pain, temperature, systolic blood pressure, heart rate, respiratory rate, hemoglobin count, hospital anticoagulation, and steroids use were found to be significantly associated with COVID-19 treatment outcome. In the multivariable logistic regression model at a 5% significance level, only a history of systolic blood pressure, VTE risk factors, diabetes mellitus, COVID-19 category, hospital anticoagulation, and chest pain demonstrated significant associations with venous thromboembolic events (VTE vs none). Adjusting for other covariates, patients with non-severe COVID-19 had a 62.2% lower likelihood of developing VTE compared to those with severe COVID-19 (AOR = 0.378, 95% CI = 0.149–0.961). Individuals with VTE risk factors were 2.5 times more likely to experience VTE than those without (AOR = 2.57, 95% CI = 1.18–5.33, p = 0.017). The odds of VTE were 3.74 times higher in patients with a history of diabetes (AOR = 3.745, 95% CI = 1.715–8.176, p = 0.001). Patients with chest pain had 4.13 times higher odds of developing VTE (AOR = 4.13, 95% CI = 1.89–9, p = 0.0001). Additionally, individuals with stage 1 hypertension at admission had 3.670 times higher odds of VTE compared to those with normal blood pressure levels (AOR = 3.67, 95% CI = 1.37–9.836, p = 0.010). Moreover, those without hospital anticoagulation had an 11.7 times higher risk of developing VTE than those receiving anticoagulation (AOR = 11.78, 95% CI = 5.25–26.4, p = 0.0001) (Table 3).
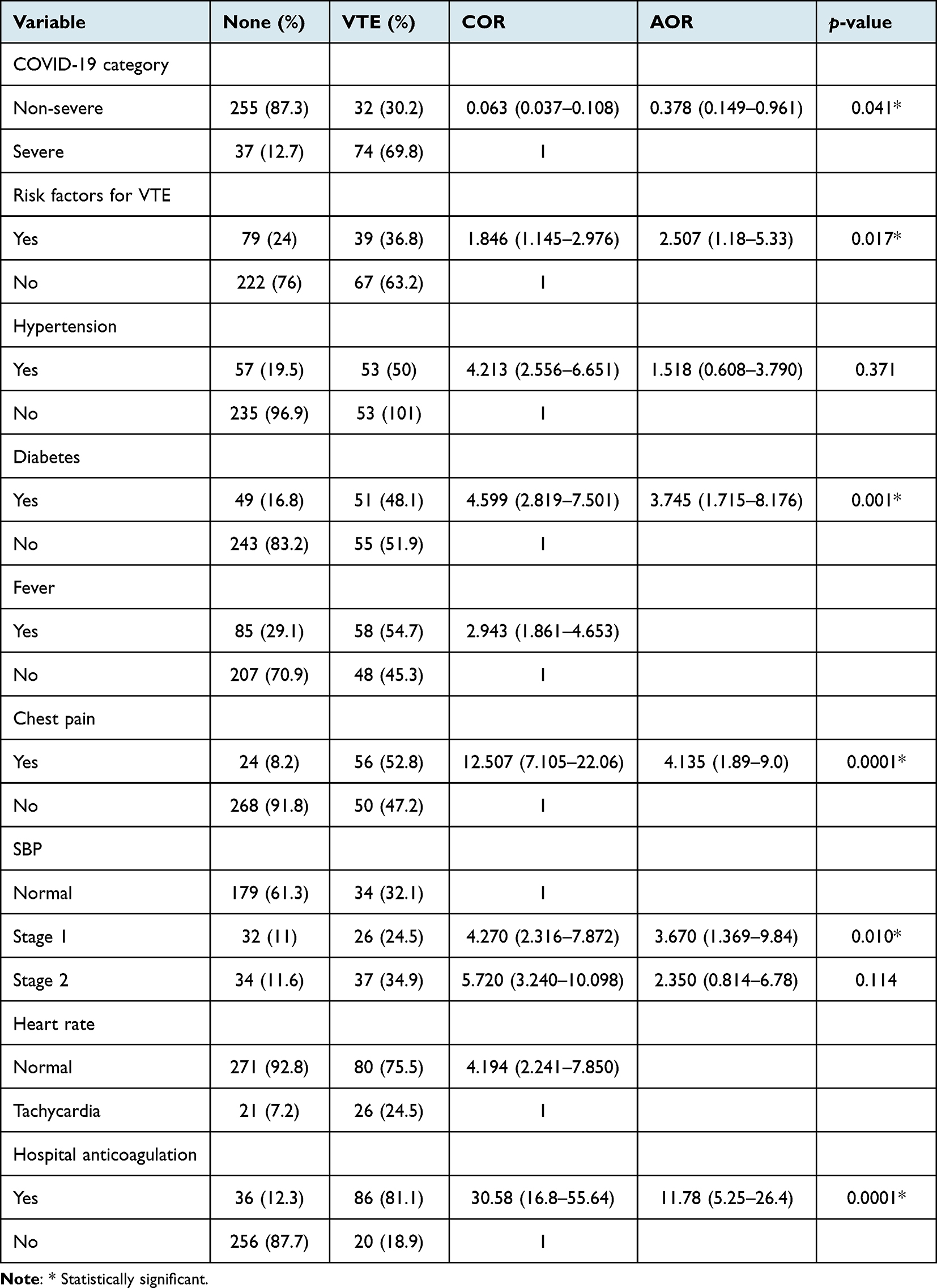 |
Table 3 Findings from the Ultimate Multivariable Binary Logistic Regression Model Among the Patients |
Discussion
COVID-19 may trigger systemic coagulation activation and thrombotic complications, necessitating heightened clinical suspicion. This study evaluated factors linked to VTE in hospitalized COVID-19 patients at a field hospital. According to the study, there was a correlation between the development of VTE and increased systolic blood pressure, diabetes, severe COVID-19 categorization, VTE risk factors, and chest discomfort. In addition, the univariate analysis, age group, COVID-19 category, risk factors for VTE, hypertension, diabetes, fever, chest pain, oxygen saturation, temperature, systolic blood pressure, heart rate, respiratory rate, hemoglobin count, hospital anticoagulation, and steroids were found to be significantly associated with VTE.
A retrospective analysis of Mexican patients hospitalized in a tertiary and referral center for COVID-19 in Mexico City and diagnosed with PE and COVID-19 revealed that 38% of the patients had obesity, 19% had arterial hypertension, and 19% had type 2 diabetes mellitus as comorbidities, which is similar to the study findings and further has been associated with development of VTE incidents.22
PE and DVT, though reported in other viral pneumonias, occur more frequently in COVID-19 patients. Hospital anticoagulation emerged as a crucial predictor, with a substantial 11.7 times higher risk of VTE for those without anticoagulation. COVID-19 coagulopathy primarily manifests as venous thromboembolism, prompting frontline providers to consider therapeutic anticoagulation for hospitalized patients, even without confirmed thrombosis. Similar findings from studies in China and the US underscore the benefits of anticoagulation in preventing VTE. Emphasizing the potential advantages of therapeutic doses during clinical deterioration, especially in the absence of confirmed PE, is crucial until further imaging tests are available.16,19,23–27
The odd of developing VTE (cases) compared to those without VTE (controls) is 2.5 times higher amongst those with risk factors (obesity, active cancer, history of surgery and stroke) than those without. Obesity and cancer seem to be risk factors that enhance the inflammatory load, and other patient-related factors (hospitalization, immobility) may also be risk factors for VTE in COVID-19 patients.28
The study found that having severe COVID-19 category at admission is associated with developing VTE. Those with a non-severe category of COVID-19 were 62.2% less likely to develop VTE. Severe COVID-19 cases carry a higher risk of VTE compared to non-severe ones. Another study at Union Hospital’s ICU revealed a 25% incidence of lower extremity DVT in severe COVID-19 patients without VTE prophylaxis.29,30
Patients with VTE had 4.135 times higher symptoms of chest pain compared to those without VTE. Even though there is much pathology that leads to chest pain, these study patients with chest pain had a higher chance of developing VTE (cases) compared to those without chest pain. Though not specific, it is one of the commonest presentations of VTE episodes and research findings report chest pain in this study signifies a condition characterized by pulmonary infiltration, where pain is associated with both breathing and posture. This clinical presentation serves as evidence of significant pulmonary infarction, as identified in the study.31
Diabetes and stage 1 hypertension (stage 1 systolic blood pressure) were important predicators of VTE. The odds of being diabetic were 3.74 times higher compared to those without diabetes and the odds of developing VTE among patients who presented with stage 1 hypertension at admission had 3.670 times higher odds compared to those with normal blood pressure levels. Diabetes, known for its potential complications such as microvascular occlusive diseases (diabetic retinopathy, nephropathy, or neuropathy), may also contribute to VTE. An Italian study reported comorbidities in 84% of cases, with the most common being arterial hypertension in 44% and type II diabetes in 16%. Regarding risk factors for VTE, the odds of getting VTE is 1.846 times higher amongst those with risk factors than those without.20,21
Limitations and Strengths
The study’s limitations include its single-center setting, restricting the generalizability of results. The design lacks precise prevalence figures and a full understanding of the observed phenomena. Uncertainty about when pulmonary embolism (PE) occurred, whether in the hospital or before admission, introduces temporal ambiguity. The retrospective nature, relying on case control charts and Electronic Medical Record (EMR) reviews, poses limitations due to incomplete documentation. Selective imaging for PE based on clinical signs may overlook subclinical cases, potentially underestimating prevalence. Non-hospitalized individuals with COVID-19 pneumonia were not explicitly studied, impacting result generalizability. These constraints emphasize caution in extrapolating findings and suggest avenues for future research. The study's strengths lie in the focused single-center investigation, offering detailed insights into diabetes, stage 1 hypertension, and VTE development in COVID-19 patients. A robust case-control design, coupled with EMR reviews, enhances predictive ability in a clinical context.
Conclusions
Hospitalized patients with stage 1 hypertension, diabetes, chest pain, and severe COVID-19 face an increased risk, necessitating preventive measures. Further research is crucial for those not receiving hospital anticoagulation to understand associated thrombosis risks. In summary, individuals with hypertension, diabetes, severe COVID-19, and no anticoagulation have a higher risk. The emphasis on early detection and treatment, especially in severe COVID-19 cases with chest discomfort, underscores the need for proactive approaches. More data is essential for understanding correlations and effective treatments for those with risk factors and early signs of venous thromboembolism (VTE). This study advocates for a comprehensive, tailored approach to patient care in the context of COVID-19, integrating management for comorbidities and risk factors to reduce VTE incidence and impact in the face of the virus’s dynamic nature.
Abbreviations
AOR, Adjusted Odds Ratio; aPTT, Activated Partial Thromboplastin Time; BMI, Body Mass Index; CI, Confidence Interval; COPD, Chronic Obstructive Lung Disease; COVID-19, Coronavirus Disease 2019; CKD, Chronic Kidney Disease; CRP, C-reactive protein; DVT, Deep Vein Thrombosis; FMOH, Federal Ministry of Health; ICU, Intensive Care Unit; IL-6, Interleukin-6; INR, International Normalized Ratio; OR, Odds Ratio; PE, Pulmonary Embolism; PLT, Platelet Count; PT, Prothrombin Time; RT-PCR, Real Time Polymerase Chain Reaction; SPSS, Statistical Package for Social Sciences; ULN, Upper Limit of Normal; VTE, Venous Thromboembolism; WBC, White Blood Cell; WHO, World Health Organization.
Data Sharing Statement
The corresponding author can provide the datasets used and analyzed in this study upon reasonable request.
Ethics Approval and Consent
The study at Addis Ababa Field Hospital, Ethiopia, was approved by the internal review board of Saint Peter Specialized Hospital and the GAMBY Medical and Business College Ethical Review Board. In lieu of obtaining agreement directly from patients, unit heads (case managers) provided consent for the analysis of secondary data (version V380/29/11/2021) without direct patient contact. Because individual consent is retrospective, carries little risk, and is hard to obtain individually, ethical committees authorized the waiving of individual consent. Strict confidentiality procedures were followed, utilizing non-identifiable data and only allowing authorized personnel to access it. Respecting institutional and national guidelines, the study did not affect participants, protecting patient confidentiality and quality of care. There were no repercussions or extra hazards for participants because of the research design.
Acknowledgments
The authors express their gratitude to the staff and patients of Saint Peter Specialty Hospital, GAMBY Medical and Business College, Dr. Tigist Workneh Leulseged, and patients and staff at Addis Ababa COVID-19 Field Hospital for their support during data collection. Their contributions were crucial to the success of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No grant from a public, private, or nonprofit organization was given for this research.
Disclosure
The writers claim to have no conflicts of interest.
References
1. Alwafi H, Naser AY, Qanash S. Predictors of Length of Hospital Stay, Mortality, and Outcomes among Hospitalised COVID-19 Patients in Saudi Arabia:No Title. J Multidiscip Healthc. 2021;14:839–852. doi:10.2147/JMDH.S304788
2. Kaminetzky M, Moore W, Fansiwala K, et al. Pulmonary Embolism at CT Pulmonary Angiography in Patients with COVID-19. Radiol Cardiothorac Imaging. 2020;2(4):e200308. doi:10.1148/ryct.2020200308
3. Gautam S. The Influence of COVID-19 on Air Quality in India: a Boon or Inutile. Bull Environ Contam Toxicol. 2020;104(6):724–726. doi:10.1007/s00128-020-02877-y
4. Vardavas CI, Nikitara K. COVID-19 and smoking: a systematic review of the evidence. Tob Induc Dis. 2020;18(March):1–4. doi:10.18332/tid/119324
5. Tapson VF. The role of smoking in coagulation and thromboembolism in chronic obstructive pulmonary disease. Proc Am Thorac Soc. 2005;2(1):71–77. doi:10.1513/pats.200407-038MS
6. Chi G, Lee JJ, Jamil A, et al. Venous Thromboembolism among Hospitalized Patients with COVID-19 Undergoing Thromboprophylaxis: a Systematic Review and Meta-Analysis. J Clin Med. 2020;9(8):2489. doi:10.3390/jcm9082489
7. Ackermann M, Verleden SE, Kuehnel M, et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N Engl J Med. 2020;383(2):120–128. doi:10.1056/NEJMoa2015432
8. Tang N, Bai H, Chen X, Gong J, Li D, Sun Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb Haemost. 2020;18(5):1094–1099. doi:10.1111/jth.14817
9. Temgoua MN, Kuaté LM, Ngatchou W, et al. Thromboembolic risks in patients with COVID-19: major concern to consider in our management. Pan Afr Med J. 2020;35(Supp 2):80. doi:10.11604/pamj.supp.2020.35.2.22945
10. Moll M, Zon RL, Sylvester KW, et al. VTE in ICU Patients With COVID-19. Chest. 2020;158(5):2130–2135. doi:10.1016/j.chest.2020.07.031
11. Bikdeli B, Madhavan MV, Jimenez D, et al. COVID-19 and Thrombotic or Thromboembolic Disease: implications for Prevention, Antithrombotic Therapy, and Follow-Up: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020;75(23):2950–2973. doi:10.1016/j.jacc.2020.04.031
12. Søgaard KK, Schmidt M, Pedersen L, Horváth-Puhó E, Sørensen HT. 30-Year mortality after venous thromboembolism a population-based cohort study. Circulation. 2014;130(10):829–836. doi:10.1161/CIRCULATIONAHA.114.009107
13. Cui S, Chen S, Li X, Liu S, Wang F. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J Thromb Haemost. 2020;18(6):1421–1424. doi:10.1111/jth.14830
14. Middeldorp S, Coppens M, van Haaps TF, et al. Incidence of venous thromboembolism in hospitalized patients with COVID-19. J Thromb Haemost. 2020;18(8):1995–2002. doi:10.1111/jth.14888
15. Giannis D, Barish MA, Goldin M, et al. Incidence of Venous Thromboembolism and Mortality in Patients with Initial Presentation of COVID-19. J Thromb Thrombolysis. 2021;51(4):897–901. doi:10.1007/s11239-021-02413-7
16. Barnes GD, Burnett A, Allen A, et al. Thromboembolism and anticoagulant therapy during the COVID-19 pandemic: interim clinical guidance from the anticoagulation forum. J Thromb Thrombolysis. 2020;50(1):72–81. doi:10.1007/s11239-020-02138-z
17. Ministry of Health-Ethiopia. National Comprehensive COVID 19 Clinical Management Handbook for Ethiopia; 2020 September:1–167.
18. Zhang L, Feng X, Zhang D, et al. Deep Vein Thrombosis in Hospitalized Patients with COVID-19 in Wuhan, China: prevalence, Risk Factors, and Outcome. Circulation. 2020;142(2):114–128. doi:10.1161/CIRCULATIONAHA.120.046702
19. Wu C, Liu Y, Cai X, Zhang W, Li Y, Fu C. Prevalence of Venous Thromboembolism in Critically Ill Patients With Coronavirus Disease 2019: a Meta-Analysis. Front Med. 2021;8:603558.
20. Vardavas CI, Nikitara K, Tang N, et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. J Thromb Haemost. 2020;18(1):2489. doi:10.1016/j.jvsv.2021.01.012
21. Monfardini L, Morassi M, Botti P, et al. Pulmonary thromboembolism in hospitalised COVID-19 patients at moderate to high risk by Wells score: a report from Lombardy, Italy. Br J Radiol. 2020;93(1113):1–6. doi:10.1259/bjr.20200407
22. Bobadilla-Rosado LO, Mier Y, Teran-Ellis S, Lopez-Pena G, Anaya-Ayala JE, Hinojosa CA. Clinical Outcomes of Pulmonary Embolism in Mexican Patients With COVID-19. Clin Appl Thromb. 2021;27:0–3. doi:10.1177/10760296211008988
23. Llitjos JF, Leclerc M, Chochois C, et al. High incidence of venous thromboembolic events in anticoagulated severe COVID-19 patients. J Thromb Haemost. 2020;18(7):1743–1746. doi:10.1111/jth.14869
24. Malato A, Dentali F, Siragusa S, et al. The impact of deep vein thrombosis in critically ill patients: a meta-analysis of major clinical outcomes. Blood Transfus. 2015;13(4):559–568. doi:10.2450/2015.0277-14
25. Buckner TW, Key NS. Venous thrombosis in blacks. Circulation. 2012;125(6):837–839. doi:10.1161/CIRCULATIONAHA.111.073098
26. Chen S, Zhang D, Zheng T, Yu Y, Jiang J. DVT incidence and risk factors in critically ill patients with COVID-19. J Thromb Thrombolysis. 2021;51(1):33–39. doi:10.1007/s11239-020-02181-w
27. Sakr Y, Giovini M, Leone M, et al. Pulmonary embolism in patients with coronavirus disease-2019 (COVID-19) pneumonia: a narrative review. Ann Intensive Care. 2020;10(1). doi:10.1186/s13613-020-00741-0
28. Kyriakoulis KG, Kokkinidis DG, Kyprianou IA, et al. Venous thromboembolism in the era of COVID-19. Phlebology. 2021;36(2):91–99. doi:10.1177/0268355520955083
29. Ozsu S, Gunay E, Konstantinides SV. A review of venous thromboembolism in COVID-19: a clinical perspective. Clin Respir J. 2021;15(5):506–512. doi:10.1111/crj.13330
30. Helms J, Tacquard C, Severac F, et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Med. 2020;46(6):1089–1098. doi:10.1007/s00134-020-06062-x
31. Morrone D, Morone V. Acute pulmonary embolism: focus on the clinical picture. Korean Circ J. 2018;48(5):365–381. doi:10.4070/kcj.2017.0314
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.