Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 21
VE-VCO2 Slope During Cardiopulmonary Exercise Test Predicts Acute Exacerbations of Chronic Obstructive Pulmonary Disease: A Retrospective Cohort Study
Authors Li X ![]() , Lin F, Wu J, Zhang J, Liu S, Qiu M, Yuan W, Nie S, Yan F, Xu B, Li Y
, Lin F, Wu J, Zhang J, Liu S, Qiu M, Yuan W, Nie S, Yan F, Xu B, Li Y
Received 15 November 2025
Accepted for publication 22 March 2026
Published 28 March 2026 Volume 2026:21 581813
DOI https://doi.org/10.2147/COPD.S581813
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Xiaona Li,1 Fang Lin,1 Jingxuan Wu,2 Jianxiong Zhang,2 Siqi Liu,1 Mengmeng Qiu,1 Wei Yuan,1 Shan Nie,1 Fugui Yan,1 Bo Xu,1 Yunxiao Li1
1Department of Respiratory Medicine, Capital Medical University Affiliated Beijing Friendship Hospital, Beijing, People’s Republic of China; 2Research Ward, Capital Medical University Affiliated Beijing Friendship Hospital, Beijing, People’s Republic of China
Correspondence: Bo Xu, Email [email protected] Yunxiao Li, Email [email protected]
Background: Cardiopulmonary Exercise Test (CPET) serves as an integrative assessment tool to evaluate cardiac function, respiratory responses, and neuromuscular capacity in patients with chronic obstructive pulmonary disease (COPD) during incremental cycling exercise. VE-VCO2 slope during CPET was not fully understood in predicting acute exacerbations of COPD (AECOPD). This study aims to establish a predictive model for AECOPD based on the VE-VCO2 slope.
Methods: In total, 79 patients with COPD were recruited between 2013 and 2019. All participants underwent baseline pulmonary function tests and CPET and were followed up for 5 years thereafter. Independent two-sample t-tests and Chi-square tests were used to compare AECOPD and Non-AECOPD groups. Univariate and multivariate Cox regression analyses were utilized to identify predictive factors for AECOPD. The diagnostic performance of these variables was evaluated by receiver operating characteristic (ROC) curve analysis. The optimal cutoff values calculated by Youden’s index. Kaplan-Meier survival analysis between subgroups was based on the optimal cutoff values. Generating Forest plots to visualize Cox regression analysis results.
Results: The AECOPD group contains 62 participants and the Non-AECOPD group contains 17 participants. Groups comparisons revealed significant differences in VE-VCO2 slope, age, BMI, FEV1%predicted, FEV1/FVC ratio, and EqCO2. Multivariate Cox regression analysis identified VE-VCO2 slope (OR = 1.19, 95% CI: 1.09– 1.29, p < 0.001), age (OR = 1.05, 95% CI: 1.02– 1.09, p = 0.005), and FEV1%predicted (OR = 0.96, 95% CI : 0.94– 0.99, p = 0.015) as significant predictors of AECOPD. The ROC curve analysis results about the above predictors found that the AUC of VE-VCO2 slope is highest independently in 1 year, 3 years and 5 years, with the optimal cutoff values = 28.42 in 5 years (hazard ratio = 3.18, 95% CI: 1.639– 6.2, p < 0.001).
Conclusion: The stratification of VE-VCO2 slope ≥ 28.42 was an independent predictor of AECOPD. Our study established VE-VCO2 slope as a novel stratified clinical biomarker for predicting AECOPD.
Keywords: COPD, exacerbation, CPET, VE-VCO2 slope, ventilation-perfusion mismatch
Introduction
Chronic obstructive pulmonary disease (COPD) is a heterogeneous respiratory disorder characterized by persistent and irreversible airflow limitation. It is important to clarify that the term “irreversible” refers to the progressive nature of the underlying structural damage (eg small airway remodeling and emphysema), which cannot be completely normalized by current pharmacotherapy.1 Clinically, this does not imply a lack of therapeutic benefit. Inhaled bronchodilators remain the cornerstone of symptomatic management. They improve expiratory flow by reducing airway smooth muscle tone, decrease exercise-induced dynamic hyperinflation, increase exercise tolerance, and alleviate dyspnea. Furthermore, while bronchodilators alone may not slow the long-term decline in lung function, they significantly reduce the frequency of acute exacerbations. Importantly, inhaled corticosteroids (ICS), particularly when combined with long-acting bronchodilators in patients with frequent exacerbations, have been shown to reduce exacerbation rates and may modestly attenuate the progression of airflow obstruction in specific phenotypes.2 A 2019 systematic analysis conducted at global regional and national levels revealed that the prevalence of COPD among individuals aged 30–79 years reached 10.3%, with male sex, smoking history, and low body mass index (BMI < 18.5kg/m2) being identified as significant predisposing risk factors.3 Most patients with COPD experience acute exacerbations during clinical progression, typically manifested as recurrent cough, dyspnea, rehospitalization, frequent outpatient visits requiring intensified antibiotic therapy. Frequent exacerbations significantly accelerate pulmonary function decline, and correlating strongly with elevated mortality.4
Frequent acute exacerbations in COPD patients not only impose substantial healthcare burdens but also significantly impair quality of life, correlating with adverse prognostic outcomes.5 Increasing research studies focus on identifying clinical and biomarkers of disease severity to develop prevention strategies about AECOPD. A Chinese prospective cohort study utilizing CT imaging revealed airway mucus plugs strongly associate with exacerbation frequencies, and a significant proportion of COPD patients demonstrates that radiologically detectable mucus retention provides critical clinical implications for exacerbation surveillance.6 Simplified nutritional assessments demonstrate malnutrition is a significant exacerbation risk factor.7 Systematic reviews identify that age, sex, MRC Dyspnea Scale scores, CAT scores, platelet/leukocyte counts, blood eosinophil percentages and prior exacerbation history are the key determinants of exacerbations among patients with COPD.8
Cardiopulmonary Exercise Testing (CPET) provides a comprehensive assessment for COPD patients through neuromuscular strength, respiratory gas exchange, and cardiovascular hemodynamics.9 Analysis between ventilation (VE) and carbon dioxide output (VCO2) during CPET reveals critical cardiopulmonary functional status and disease progression patterns.10 In previous studies, the relationship between VE and VOC2 has been extensively investigated, primarily through three approaches: the carbon dioxide ventilation equivalent (EqCO2), which refers to the ratio of VE to VCO2 at a specific time point, the CO2 ventilation efficiency nadir (EqCO2 nadir) and the VE-VCO2 slope. The VE-VCO2 slope is a key index of ventilatory efficiency derived during CPET. It’s calculated using linear regression analysis to quantify the relationship between minute ventilation (VE) and carbon dioxide output (VCO2) during incremental exercise (The data start from a work rate about 15 to 25 Watts until strictly only up to the Respiratory Compensation Point).10 In heart failure research, VE-VCO2 slope ≥36 independently predicts mortality, while VE-VCO2 slope ≥34 significantly forecasts hospitalization risk.11 Machine learning analyses of chronic heart failure cohorts identify VE-VCO2 slope ≥30 is optimal threshold for adverse event prediction.12 Comparative studies of exercise parameters by Alba demonstrated the VE-VCO2 slope’s superior prognostic power versus VE, OUES (Oxygen Uptake Efficiency Slope) and peak VO2.13 Despite established cardiac applications, VE-VCO2 slope’s predictive value for AECOPD remains uninvestigated. Thus, this retrospective cohort study evaluates VE-VCO2 slope’s capacity to predict exacerbations in patients with COPD followed up by 5 years after finishing CPET.
Materials and Method
Study Participants
Inclusion and Exclusion Criteria
This is a retrospective study that enrolled COPD patients recruited from the outpatient clinic of the Beijing Friendship Hospital between 2013 and 2019. All participants before the training, all participants were provided with written and oral information about this program and signed an informed consent form. Our study complies with the Declaration of Helsinki. The Ethics Committee of Beijing Friendship Hospital approved the study protocol (No: 2024-P2-125-01, Date: 2024-04-19).
This retrospective cohort study analyzed COPD patients enrolled between 2013 and 2019, their age were between 40 and 85 years, including 68 males and 11 females, meeting the GOLD diagnostic confirmation (post-bronchodilator FEV1/FVC <0.70), clinically stable status (within 6 weeks prior to study participation).14 Patients with cardiac morbidities (heart failure, arrhythmias, valvulopathies, or coronary artery disease), using β-blocker/outcome-interfering medication, hypoxemia requiring supplemental oxygen (SpO2 < 90% on room air) and physical limitations contraindicating CPET (degenerative knee pathologies incompatible with cycle ergometry) were excluded.
Pulmonary Function Tests
All patients underwent pulmonary function test by using the Master Screen Body plethysmograph (CareFusion Corp, San Diego, CA, USA). The evaluation protocol included: Spirometry: VC (Vital Capacity), FVC (Forced Vital Capacity), FEV1 (Forced Expiratory Volume in 1 second) and DLCO (diffusion Capacity), KCO (Transfer Factor: KCO = DLCO/VA: Carbon Monoxide Diffusing Capacity per Alveolar Volume). RV (Residual Volume), TLC (Total Lung Capacity) and RV/TLC ratio were detected by Body Plethysmography. All procedures strictly adhered to European Respiratory Society (ERS) technical standards.15
Cardiopulmonary Exercise Test
The standards and implementation procedures of CPET were referenced from the guidelines of the American Thoracic Society/European Respiratory Society.16 After excluding contraindications, all patients with COPD were required to rest on a cycle ergometer for 3 minutes after attaching electrocardiogram (ECG) electrodes, blood pressure cuffs, pulse oximetry sensors, and standard mouthpieces. Subsequently, they underwent 3 minutes of unloaded cycling exercise. Then, an incremental symptom-limited exercise test was conducted using an electronically braked cycle ergometer (model Via Sprint, CareFusion Corporation, Sieberg, Germany) at a speed of 40–70 revolutions per minute (rpm), usually approximately 60 rpm. Before CPET, patients with COPD needed to undergo static pulmonary function tests to obtain forced expiratory volume in one second (FEV1) data. Then combining with height, weight and the body mass index (BMI) values, the CPET device calculated the maximal oxygen uptake (VO2max) and target load. Generally, it took about 10 minutes for COPD patients to complete the entire incremental power cycling test. The incremental power per minute was calculated based on the maximum target power.9 The criteria for completing the CPET test were achieving the maximum effort exercise goal or encountering circumstances that required termination, such as arrhythmia, dyspnea, chest pain. During the test, blood pressure was measured every 2 minutes, and continuous attention was paid to changes in blood oxygen saturation and electrocardiogram (ECG) signals.17 The VE-VCO2 slope (the slope of the relationship curve between VE and carbon dioxide production VCO2 was calculated by linear regression of VE and VCO2, data start from a work rate about 15 to 25 Watts until strictly only up to the Respiratory Compensation Point). The one-minute heart rate recovery (HRR1) was defined as the peak heart rate during exercise minus the heart rate at 1 minute of recovery.
Follow Up of AECOPD Patients
Seventy-nine research subjects underwent a 5 years’ follow up after completing baseline tests and the collection of clinical indicators. The subjects were followed up at three months intervals. Clinical symptoms, comorbidities, smoking status and frequency of outpatient visits were recorded. Whether administering additional antibiotics and hospitalization to alleviate the condition was necessary to record. During the follow up, acute exacerbations of COPD (AECOPD) were defined as the emergence of frequent respiratory symptoms and the need for hospitalization and additional outpatient treatments.18
Statistical Analyses
Statistical analyses were performed using SPSS (version 31.0) and R software (version 4.4.0). Continuous variables were summarized as mean ± standard deviation and compared between the AECOPD and Non-AECOPD groups using independent samples t-tests, with Levene’s test employed to assess homogeneity of variance. When variances were heterogeneous, the Mann–Whitney U-test was applied. Categorical variables were presented as frequencies and percentages and analyzed using the chi-square test or Fisher’s exact test where appropriate. Univariate and multivariate Cox proportional hazards regression models were conducted to identify significant predictors of AECOPD. To identify factors associated with AECOPD, we first performed univariable regression analysis to screen potential predictors. All variables with a p-value < 0.05 in the univariable analysis were then entered into the multivariable regression model to adjust for potential confounders. The multivariable analysis was performed to determine the independent predictors of AECOPD. The diagnostic performance of these predictors was evaluated through receiver operating characteristic (ROC) curve analysis. Kaplan-Meier survival curves were generated using R packages survival and survminer, with differences assessed via the Log rank test. Forest plots were constructed to visualize hazard ratios and 95% confidence intervals from the Cox models. All statistical tests were two-sided, and a p-value < 0.05 was considered statistically significant.
Results
During a 5-year follow up period, 79 study subjects were prospectively followed until the occurrence of acute exacerbation, which served as the primary endpoint. Of these, 62 patients experienced acute exacerbations (AECOPD group), while 17 remained free of exacerbations (Non-AECOPD group). Baseline demographic characteristics, pulmonary function test results, and exercise cardiopulmonary function parameters are summarized in Table 1. The mean age of the total cohort was 67 years (SD = 8.2), with the AECOPD group being significantly older than the Non-AECOPD group (p < 0.001). The body mass index (BMI) was significantly lower in the AECOPD group compared to the Non-AECOPD group (p = 0.02). There was a significant difference in the distribution of GOLD stages between the two groups, with higher proportions of patients classified as GOLD stage 2 and 3 in the AECOPD group. Pulmonary function analysis revealed that both FEV1% predicted (FEV1%pred) and FEV1/FVC ratio were significantly lower in the AECOPD group (p = 0.006, p = 0.027). Furthermore, cardiopulmonary exercise testing (CPET) outcomes showed that the VE-VCO2 slope was significantly elevated in the AECOPD group (p < 0.001), as was the ventilatory equivalent for carbon dioxide (EqCO2) (p = 0.003).
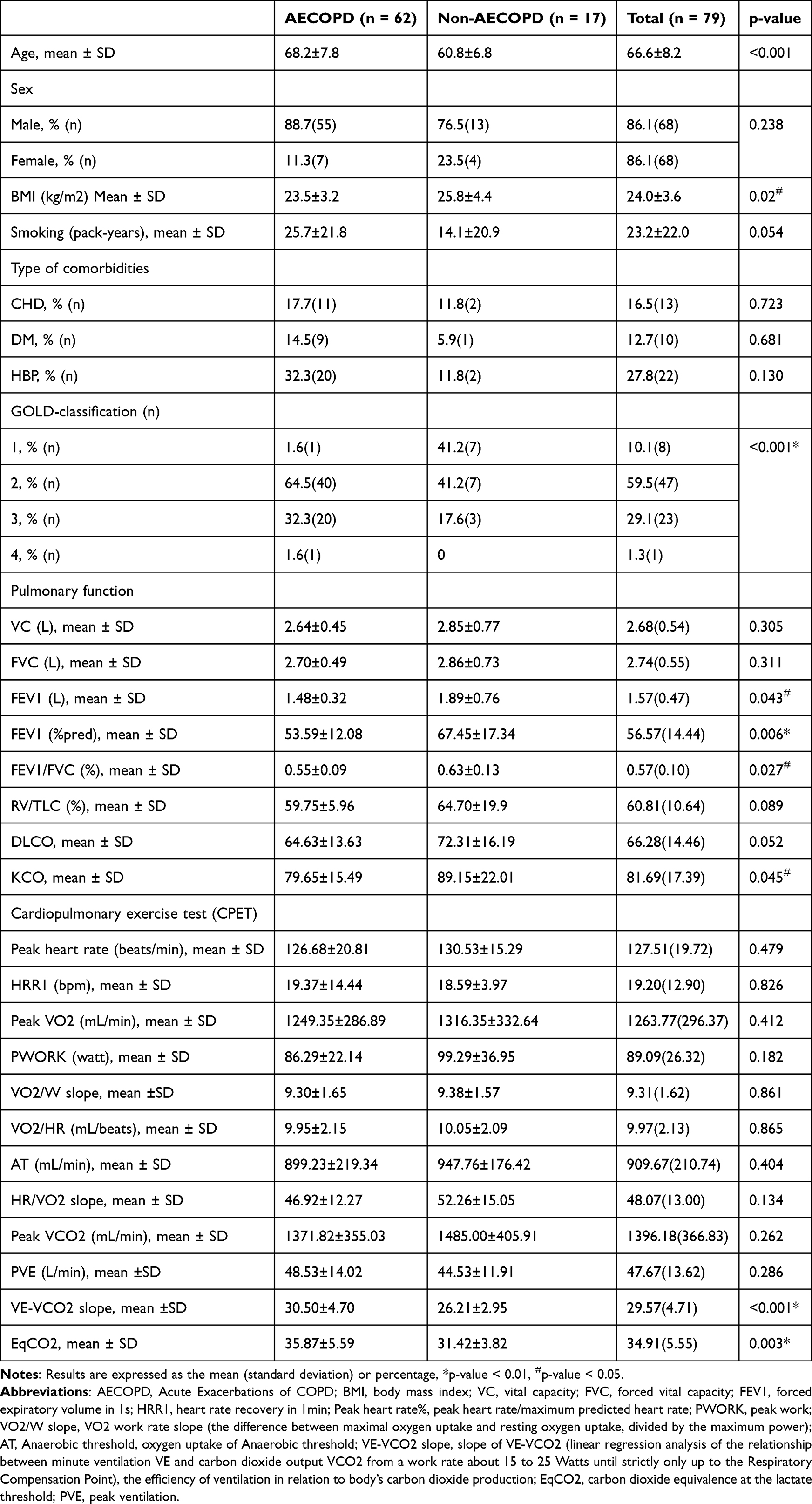 |
Table 1 Study Population Characteristics |
As shown in Table 1, significant differences were observed between the AECOPD and Non-AECOPD groups in age, body mass index (BMI), forced expiratory volume in one second as a percentage of predicted value (FEV1%pred), FEV1/FVC ratio, VE-VCO2 slope, and carbon dioxide ventilatory equivalent measured at the Anaerobic Threshold (AT) (EqCO2). Univariate and multivariate Cox proportional hazards regression analyses were therefore performed to evaluate the predictive value of these variables for AECOPD. After adjusting for age, BMI, FEV1%pred, FEV1/FVC and EqCO2, VE-VCO2 slope (data start from a work rate about 15 to 25 Watts until strictly only up to the Respiratory Compensation Point) remained a significant predictor of AECOPD (Table 2). Additionally, age and FEV1%pred also demonstrated significant predictive capacity. The results of the multivariate analysis are presented in the forest plot (Figure 1). For every one-unit increase in VE-VCO2 slope, the risk of AECOPD increased by 19% (hazards ratio = 1.19, 95% CI: 1.09–1.29, p < 0.001). Similarly, each one-year increase in age was associated with a 5% higher risk of AECOPD (HR = 1.05, 95% CI: 1.02–1.09, p = 0.005).
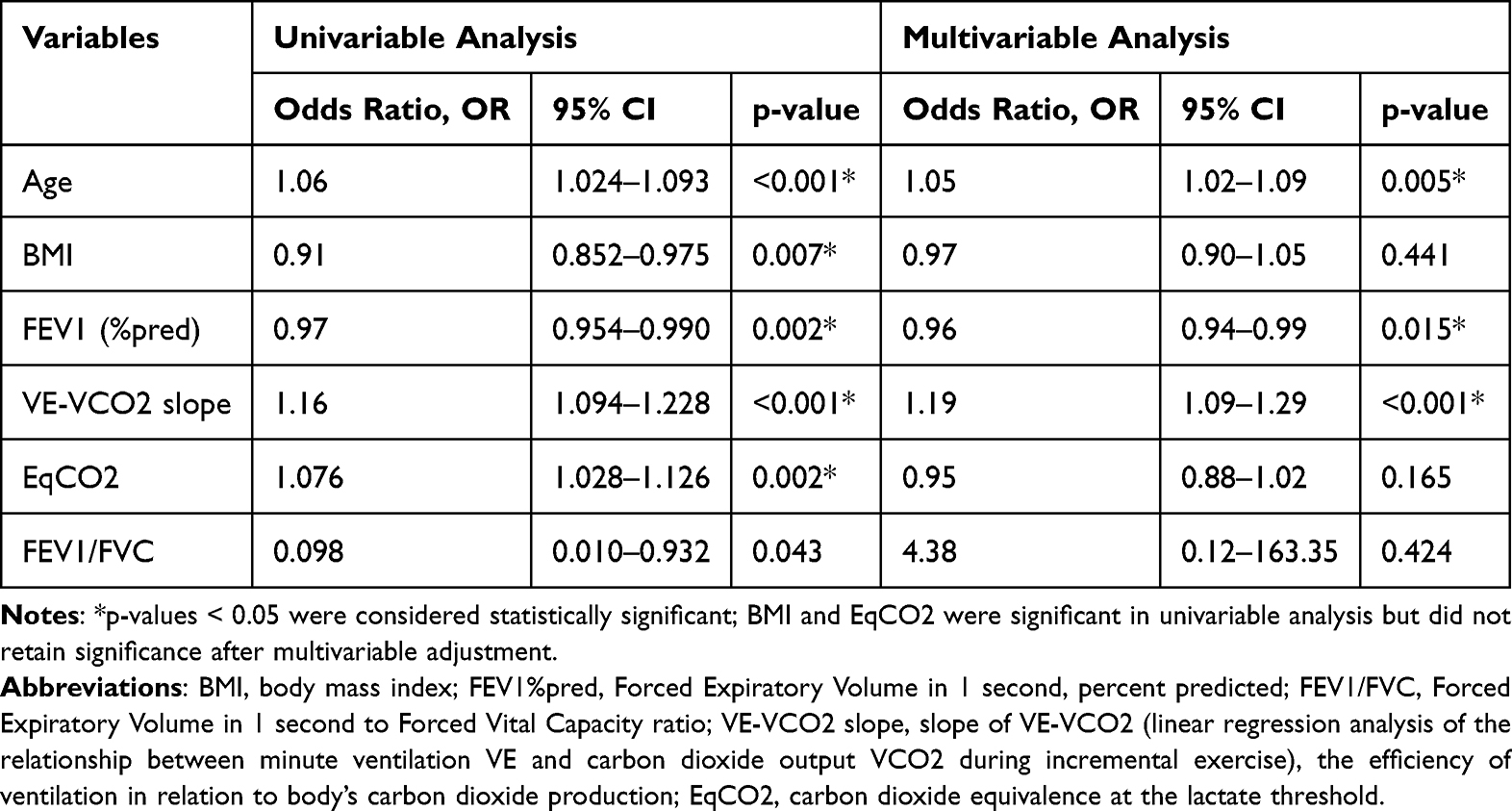 |
Table 2 Univariate and Multivariate Proportional Hazards Analyses |
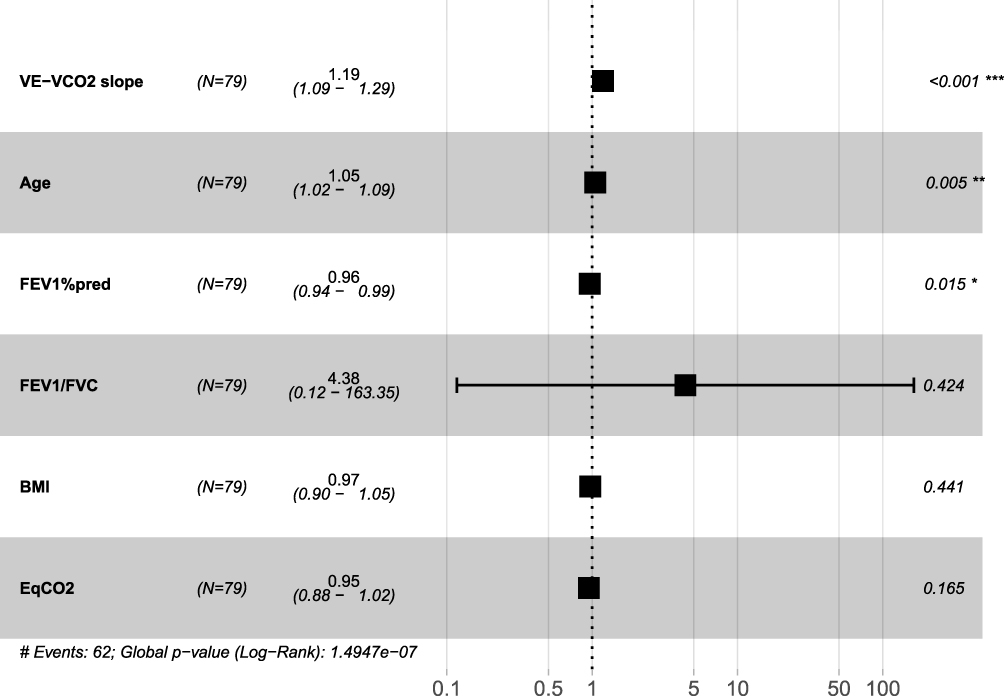 |
Figure 1 Forest Plot of Cox Regression Model. Notes: Forest plot of COX regression in AECOPD with VE-VCO2 slope, age and FEV1%pred. *p < 0.05, **p < 0.01, ***p < 0.001. |
Our findings identify the VE-VCO2 slope, age, and FEV1%pred as risk factors for AECOPD. Subsequently, we employed ROC curve analysis to assess the predictive performance of these three factors for AECOPD at one, three, and five years. Given that a lower FEV1%pred value corresponds to better predictive ability, we used its reciprocal for comparison with the other two indicators (Figures 2A, B and 3). The results were as follows: (1) At one year: age (AUC = 0.657), VE-VCO2 slope (AUC = 0.717) and 1/FEV1%pred (AUC = 0.673); (2) At three years: age (AUC = 0.685), VE-VCO2 slope (AUC = 0.759) and 1/FEV1%pred (AUC = 0.625); (3) At five years: age (AUC = 0.778), VE-VCO2 slope (AUC = 0.790) and 1/FEV1%pred (AUC = 0.724).
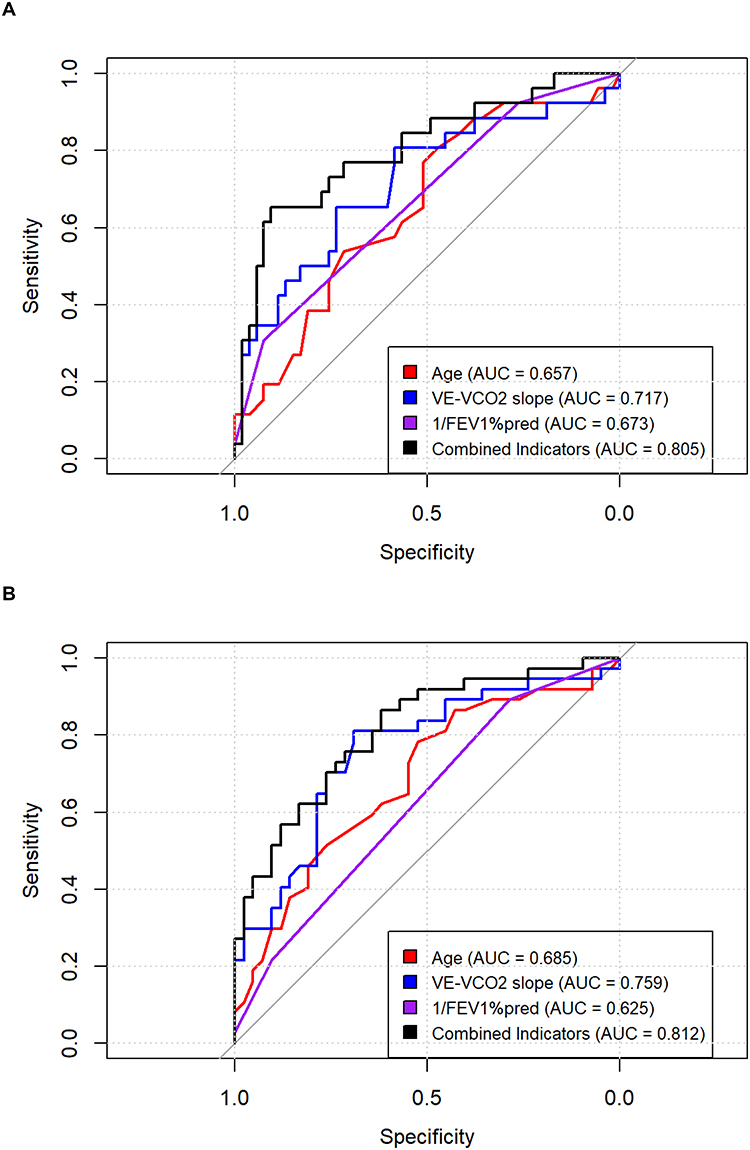 |
Figure 2 (A) Timepoint: 12 months. (B) Timepoint: 36 months. Notes: Receiver Operating Characteristic Curve Comparison at time point of 12 Months. Receiver Operating Characteristic Curve Comparison at time point of 36 Months. |
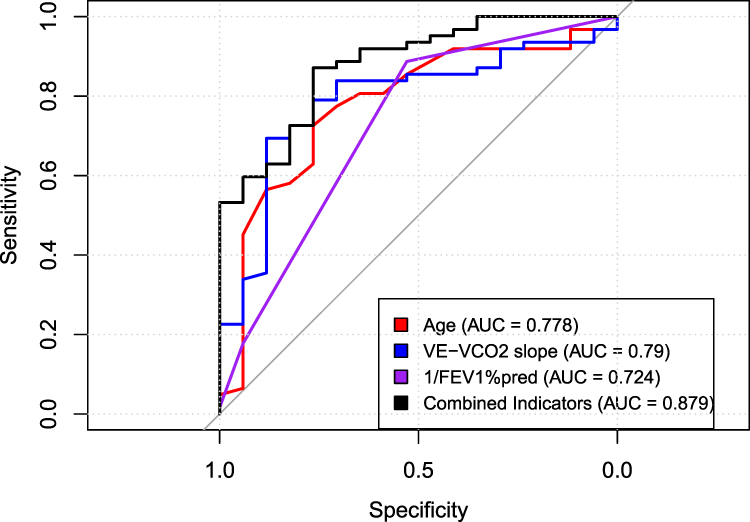 |
Figure 3 Receiver Operating Characteristic Curve Comparison at time point of 60 Months. |
We used the DeLong test (see Supplementary Table 1) to compare the AUC values among the three individual indicators and a combined indicator. No statistically significant differences were observed. Nevertheless, in terms of AUC magnitude, the VE-VCO2 slope demonstrated superior predictive performance compared to the other two indicators across all time points, although the combined model did not yield a significant improvement.
Integration of our analytical results identified the VE-VCO2 slope as the strongest prognostic determinant, with ROC analysis at the 5-year follow-up revealing superior discriminative capacity (AUC = 0.790). Using the optimal cutoff value (≥28.42), patients were categorized into high-risk (≥28.42) and low-risk groups for Kaplan–Meier survival analysis (Figure 4). The high-risk group showed a median time to acute exacerbation of 18 months, compared with 60 months in the low-risk group (Log rank test: p < 0.001). Following risk stratification, a multivariable Cox proportional hazards regression model, adjusted for other covariates, confirmed that an elevated VE-VCO2 slope (high-risk group) remained an independent predictor of AECOPD (hazards ratio = 3.18, 95% CI 1.64–6.20, p < 0.001), as shown in Figure 5.
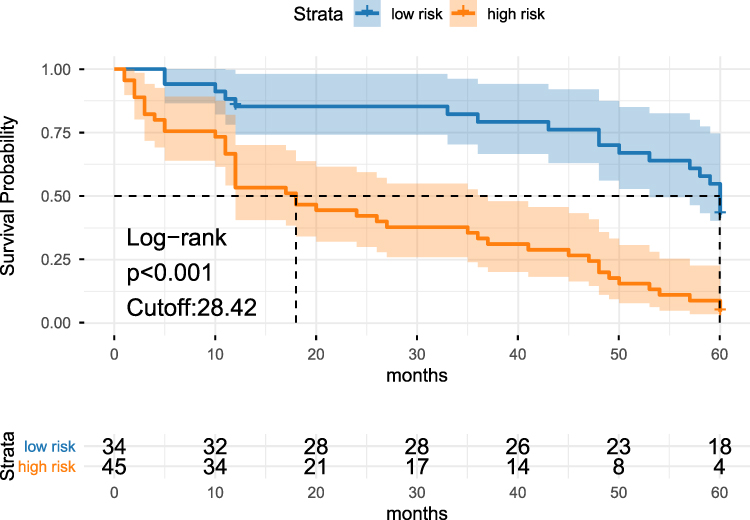 |
Figure 4 Survival Analysis Based on VE-VCO2 slope Risk Stratification. Note: Kaplan-Meier curve of the time of AECOPD according to the two different VE-VCO2 slope groups. |
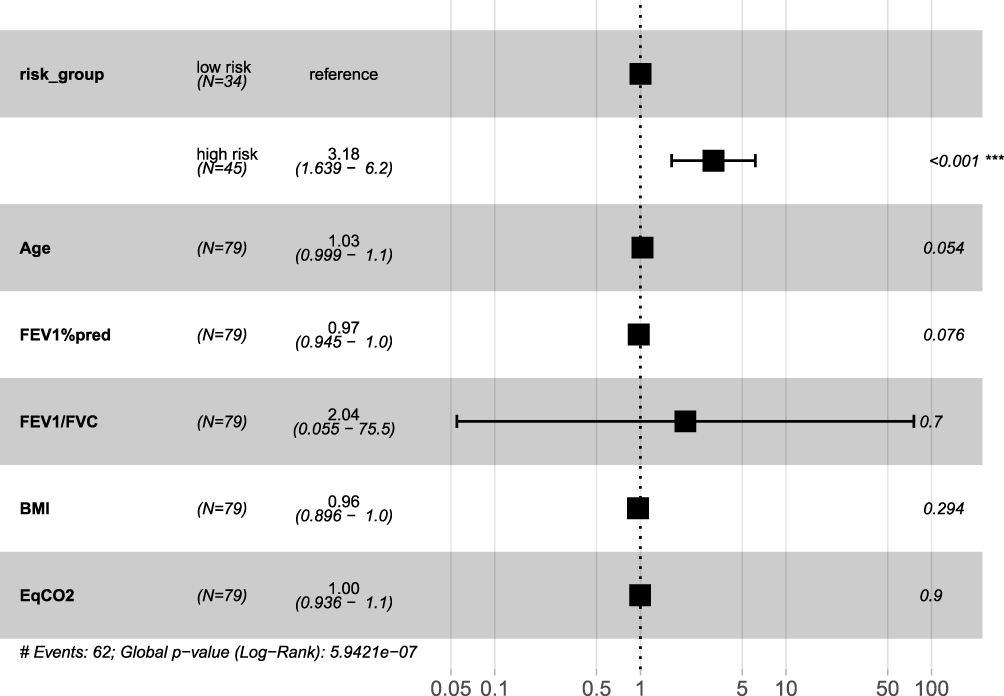 |
Figure 5 Forest plot of Multivariable Cox Regression Analysis for VE-VCO2 slope Risk Stratification. Notes: Forest plot of COX regression in AECOPD with VE-VCO2slope ≥28.42. ***p < 0.001. |
Discussion
The present study demonstrated a significant association between the VE-VCO2 slope and acute exacerbation events in patients with COPD during a 5-year longitudinal observation. Furthermore, this parameter exhibited discriminative capacity for predicting AECOPD in the early and intermediate phases of follow up. CPET serves as a critical evaluative tool to assess aerobic and anaerobic metabolic capacities through measurements of oxygen consumption (VO2) and carbon dioxide production (VCO2).19 COPD patients with concomitant emphysema exhibited an elevated residual volume to total lung capacity ratio (RV/TLC), indicative of air trapping.20 Ventilation-perfusion (V/Q) mismatch represents the principal pathophysiological mechanism underlying exertional dyspnea in COPD populations. Notably, a subset of COPD patients manifests minimal dyspneic symptoms during rest or low-intensity activities, a phenomenon that limits the diagnostic utility of conventional 6-minute walk tests (6MWT). The subjective nature of 6MWT and variable patient effort levels compromise its reliability in assessing true ambulatory capacity, particularly regarding standardized walking performance evaluations.21 Conversely, CPET protocols unmask accentuated dyspnea severity in COPD cohorts. This exacerbation correlates mechanistically with augmented dead space ventilation, necessitating compensatory hyperventilation to maintain eucapnia during CO2 elimination. Consequently, the elevated VE-VCO2 slope serves as an indicator of impaired ventilatory efficiency.22 And the higher VE-VCO2 slope values demonstrating significant correlation with exertional dyspnea intensity.23 Patients stratified as GOLD Grade I typically preserve exercise capacity parameters comparable to healthy controls. However, the co-occurrence of diffusion impairment within this subgroup portends adverse prognostic implications and exhibits frequent association with diminished body mass index (BMI) metrics.24
However, in our text, we realize variables like BMI and EqCO2, where the univariable analysis was significant (p < 0.05) but the multivariable was not. This suggests that the effect of BMI on AECOPD was confounded by other variables in the model (eg. age and FEV1%pred). And, the EqCO2 was confounded by the VE-VCO2 slope variables in the model. Thus, we did not pay attention to these two variables, highlighting the importance of age, FEV1%pred and VE-VCO2 slope in the pathophysiology of COPD. In our preliminary multivariate Cox regression analysis prior to risk stratification of the VE-VCO2 slope, both age and FEV1% pred were identified as significant predictors of AECOPD. This aligns with established epidemiological observations, as COPD prevalence escalates with aging.25 And lower FEV1%pred correlates with higher Global Initiative for Chronic Obstructive Lung Disease (GOLD) grades, reflecting greater disease severity. Consistent with prior studies, declining FEV1%pred predicts high susceptibility to acute exacerbations during disease progression.26 Following risk stratification of the VE-VCO2 slope, subsequent multivariate Cox regression analysis revealed that elevated VE-VCO2 slope in the high-risk cohort remained an independent predictor of AECOPD. Consequently, our investigation focused on analyzing the VE-VCO2 slope after establishing baseline assessments for age and FEV1%pred. While the prognostic significance of VE-VCO2 slope in heart failure has been well established and widely utilized, with extensive validation of the VE-VCO2 slope as a robust predictor of adverse outcomes in population, however, its role in predicting acute exacerbations in COPD remains underexplored.27 Although CPET is increasingly recognized for guiding pulmonary rehabilitation in COPD, the predictive utility of VE-VCO2 slope for AECOPD has not been systematically investigated. Our study pioneers the development of a VE-VCO2 slope-based predictive model for AECOPD, addressing this critical gap in COPD risk stratification.
Frequent acute exacerbations significantly impair quality of life in COPD patients. Established predictors of exacerbation risk include elevated neutrophil counts, eosinophil percentages in routine blood tests,28 reduced FEV1%pred and prior exacerbation history.29 Our retrospective cohort study demonstrated that VE-VCO2 slope remained a significant prognostic indicator for COPD exacerbations over a 5-year horizon after adjusting for confounding variables. Notably, this predictive capacity exhibited comparable robustness during both 1-year and 3-year intervals. Despite limited recognition of the VE-VCO2 slope in acute exacerbation of COPD (AECOPD) research, a prior investigation identified computed tomography (CT)-quantified emphysema severity as an independent determinant of abnormally elevated VE-VCO2 slope in COPD populations,30 suggesting imaging biomarkers may preliminarily estimate this parameter. Our findings extend these observations by providing novel physiological validation: the VE-VCO2 slope accurately captures exercise-induced ventilation-perfusion (V/Q) mismatches, establishing mechanistic linkages between dynamic cardiopulmonary stress testing and clinical exacerbation susceptibility in natural disease progression. Also, it is essential to recognize that this parameter reflects global cardiopulmonary efficiency rather than a lung-specific phenomenon. In patients with COPD, elevated VE-VCO2 slope may also arise from concurrent circulatory limitations, including reduced cardiac output response, chronotropic incompetence, or latent pulmonary vascular dysfunction. These factors are prevalent in COPD.
Our study has several limitations that should be acknowledged. First, the study population consisted predominantly of male participants. Consequently, the prognostic value of the VE-VCO2 slope for predicting acute exacerbations may be more applicable to men and requires further validation in female COPD populations. Second, as a retrospective cohort study, inherent issues such as missing data limited our ability to comprehensively correlate the VE-VCO2 slope with other clinical parameters. The underlying clinical and pathophysiological mechanisms of the VE-VCO2 slope warrant deeper investigation in future studies. Third, our single-center, retrospective design limits generalizability to other populations and clinical settings. The modest sample size, particularly the limited number of patients in Non-AECOPD, may affect the precision and stability of our multivariable models, and our findings should be considered hypothesis-generating pending validation in larger cohorts. Fourth, although patients with overt cardiac disease were excluded, we cannot completely rule out the presence of subclinical heart failure with preserved ejection fraction (HFpEF), which is common in COPD and known to elevate the VE-VCO2 slope.31 The absence of systematic natriuretic peptide measurements and comprehensive echocardiographic diastolic function assessment limits our ability to differentiate pulmonary from cardiac determinants of ventilatory efficiency. Future studies integrating cardiopulmonary exercise testing with simultaneous echocardiography and cardiac biomarkers are needed to refine the mechanistic interpretation of VE-VCO2 slope in this population. Moreover, the VE-VCO2 slope is not a directly measured parameter; it is derived from CPET data using statistical processing (from low level exercise to RCP). This highlights the need to develop predictive models that can more intuitively assess factors associated with COPD exacerbations. Additionally, as a continuous variable, the dichotomization of the VE-VCO2 slope for risk stratification may lead to uneven distribution between groups, potentially limiting the generalizability of our cutoff value to external cohorts. Further expansion of the sample size is necessary to identify an optimal VE-VCO2 threshold for clinical application. It should also be noted that this dynamic prospective cohort was originally recruited from Beijing Friendship Hospital between 2013 and 2019, with a planned 5-year follow-up. Now, a decade after initiation, we conducted additional follow-up before manuscript completion. However, a number of patients were lost to follow-up, and among those who could be reached, significant recall bias was observed. Reassessment of baseline clinical characteristics at enrollment was not feasible. Therefore, our analysis relied on retrospective review of prior follow-up records and baseline data, with re-evaluation of CPET-derived metrics for predicting acute exacerbations and associated pathophysiological correlates. Moving forward, we plan to establish a new prospective COPD cohort. Building on CPET assessments, we will incorporate additional clinical evaluations such as thoracic CT imaging, nutritional status assessment, and cognitive function screening. With appropriate ethical approval, a biorepository will be established to bank biological samples alongside comprehensive clinical data. Crucially, to minimize loss to follow-up, we will implement a structured follow-up clinic system, aiming to build a long term, stable COPD research cohort with complete and high-quality longitudinal data. Finally, while the VE-VCO2 slope demonstrated robust predictive value for AECOPD in our cohort, we acknowledge that its multifactorial determinants preclude attribution to any single physiological domain. Future studies integrating detailed cardiac and pulmonary vascular phenotyping are needed to disentangle the relative contributions of lung mechanics, gas exchange, and circulatory function to ventilatory efficiency and its prognostic significance in COPD.
Conclusions
Our study identifies the VE-VCO2 slope after CPET as a significant predictor of AECOPD. This is the first report demonstrating its ability to predict the 5-year risk of acute exacerbations of COPD. These findings position the VE-VCO2 slope as a valuable risk stratification tool for identifying high risk patients with COPD group who are prone to rehospitalization and require intensified outpatient management. Moreover, it holds important implications for early and middle stage for identification of high-risk individuals. Based on these results, we emphasize the necessity of implementing early interventions in COPD populations, including smoking cessation, adherence to pharmacotherapy, and initiation of respiratory muscle training, along with a structured pulmonary rehabilitation program that incorporates anaerobic exercise combined with appropriate aerobic activity.
Abbreviations
CPET, Cardiopulmonary Exercise Test; COPD, Chronic Obstructive Pulmonary Disease; AECOPD, Acute exacerbations of Chronic Obstructive Pulmonary Disease; 6MWT, 6-min walk test; AT, Anaerobic threshold; VCO2, Carbon dioxide production; VO2, Oxygen uptake; VE, Ventilation; EqCO2, ventilatory equivalents for CO2 at defined time points; EqCO2 nadir, lowest observed value; SpO2, Oxygen saturation via pulse oximetry; FEV1, Forced expiratory volume in 1 s; HRR, Heart rate recovery; CI, Confidence interval.
Ethics Approval and Informed Consent
The Ethics Committee of Beijing Friendship Hospital approved the study protocol (No: 2024-P2-125-01, Date: 2024–04-19). All participants were provided with written and oral information about this program and signed an informed consent form.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Capital’s Funds for Health Improvement and Research (grant no. 2024-2-1101).
Disclosure
The authors have no conflicts of interest to declare.
References
1. Lange P, Ahmed E, Lahmar ZM, Martinez FJ, Bourdin A. Natural history and mechanisms of
2. Singh D, Donohue JF, Boucot IH, Barnes NC, Compton C, Martinez FJ. Future concepts in bronchodilation for COPD: dual- versus monotherapy. Eur Respir Rev. 2021;30(160):210023. doi:10.1183/16000617.0023-2021
3. Adeloye D, Song P, Zhu Y, Campbell H, Sheikh A, Rudan I. Global, regional, and national prevalence of, and risk factors for, chronic obstructive pulmonary disease (COPD) in 2019: a systematic review and modelling analysis. Lancet Respir Med. 2022;10(5):447–458. doi:10.1016/S2213-2600(21)00511-7
4. Singh D, Agusti A, Anzueto A, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease: the GOLD science committee report 2019. Eur Respir J. 2019;53(5):1900164. doi:10.1183/13993003.00164-2019
5. Wallström O, Stridsman C, Lindberg A, Nyberg F, Vanfleteren LEGW. Exacerbation history and risk of myocardial infarction and pulmonary embolism in COPD. CHEST. 2024;166(6):1347–1359. doi:10.1016/j.chest.2024.07.150
6. Li X, Feng S, Yang Y, et al. Association between airway mucus plugs and risk of moderate-to-severe exacerbations in patients with COPD. CHEST. 2025;168(3):627–638. doi:10.1016/j.chest.2025.03.026
7. Di Raimondo D, Pirera E, Pintus C, et al. The Impact of Malnutrition on Chronic Obstructive Pulmonary Disease (COPD) outcomes: the predictive value of the Mini Nutritional Assessment (MNA) versus acute exacerbations in patients with highly complex COPD and its clinical and prognostic implications. Nutrients. 2024;16(14):2303. doi:10.3390/nu16142303
8. Xu Z, Li F, Xin Y, Wang Y, Wang Y. Prognostic risk prediction model for patients with acute exacerbation of chronic obstructive pulmonary disease (AECOPD): a systematic review and meta-analysis. Respir Res. 2024;25(1):410. doi:10.1186/s12931-024-03033-4
9. Radtke T, Crook S, Kaltsakas G, et al. ERS statement on standardisation of cardiopulmonary exercise testing in chronic lung diseases. Eur Respir Rev. 2019;28(154):180101. doi:10.1183/16000617.0101-2018
10. Wheeler MT, Olivotto I, Elliott PM, et al. Effects of mavacamten on measures of cardiopulmonary exercise testing beyond peak oxygen consumption: a secondary analysis of the EXPLORER-HCM randomized trial. JAMA Cardiol. 2023;8(3):240. doi:10.1001/jamacardio.2022.5099
11. Da Luz Goulart C, Agostoni P, Salvioni E, et al. Exercise oscillatory breathing in heart failure with reduced ejection fraction: clinical implication. Eur J Prevent Cardiol. 2022;29(12):1692–1698. doi:10.1093/eurjpc/zwac116
12. Cen H, Chen S, Feng S, et al. Establishing a novel model to assess exercise capacity in chronic heart failure based on stress echocardiography. ESC Heart Fail. 2024;11(6):4335–4347. doi:10.1002/ehf2.15038
13. Alba AC, Adamson MW, MacIsaac J, et al. The added value of exercise variables in heart failure prognosis. J Cardiac Fail. 2016;22(7):492–497. doi:10.1016/j.cardfail.2016.01.012
14. Sharma M, Joshi S, Banjade P, Ghamande SA, Surani S. Global initiative for Chronic Obstructive Lung Disease (GOLD) 2023 guidelines reviewed. TORMJ. 2024;18(1):e18743064279064. doi:10.2174/0118743064279064231227070344
15. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
16. American Thoracic Society. ATS/ACCP statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med. 2003;167(2):211–277. doi:10.1164/rccm.167.2.211
17. Nicol M, Deney A, Lairez O, et al. Prognostic value of cardiopulmonary exercise testing in cardiac amyloidosis. Eur J Heart Fail. 2021;23(2):231–239. doi:10.1002/ejhf.2016
18. Celli BR, Fabbri LM, Aaron SD, et al. An updated definition and severity classification of chronic obstructive pulmonary disease exacerbations: the Rome proposal. Am J Respir Crit Care Med. 2021;204(11):1251–1258. doi:10.1164/rccm.202108-1819PP
19. Collins SÉ, Kirby M, Smith BM, et al. Relationship of Pulmonary vascular structure and function with exercise capacity in health and COPD. CHEST. 2025;167(2):402–413. doi:10.1016/j.chest.2024.09.027
20. Pott H, Weckler B, Gaffron S, et al. Diffusion capacity and static hyperinflation as markers of disease progression predict 3‐year mortality in
21. Chae G, Ko EJ, Lee SW, et al. Stronger correlation of peak oxygen uptake with distance of incremental shuttle walk test than 6-min walk test in patients with COPD: a systematic review and meta-analysis. BMC Pulm Med. 2022;22(1):102. doi:10.1186/s12890-022-01897-0
22. Neder JA, Berton DDC. Ventilatory inefficiency and exertional dyspnea in early chronic obstructive pulmonary disease. Ann Am Thor Soc. 2017;14(Supplement_1):S22–S29.
23. Phillips DB, Elbehairy AF, James MD, et al. Impaired ventilatory efficiency, dyspnea, and exercise intolerance in chronic obstructive pulmonary disease: results from the CanCOLD study. Am J Respir Crit Care Med. 2022;205(12):1391–1402. doi:10.1164/rccm.202109-2171OC
24. De-torres JP, O’Donnell DE, Marín JM, et al. Clinical and prognostic impact of low diffusing capacity for carbon monoxide values in patients with global initiative for obstructive lung disease I COPD. CHEST. 2021;160(3):872–878. doi:10.1016/j.chest.2021.04.033
25. Safiri S, Carson-Chahhoud K, Noori M, et al. Burden of chronic obstructive pulmonary disease and its attributable risk factors in 204 countries and territories, 1990–2019: results from the Global Burden of Disease Study 2019. BMJ. 2022;378:e069679. doi:10.1136/bmj-2021-069679
26. Kim DH, Jeon ET, Lee HJ, et al. Longitudinal changes in maximal forced inspiratory flow and clinical outcomes in patients with COPD. CHEST. 2025;167(1):76–86. doi:10.1016/j.chest.2024.07.162
27. Guazzi M, Myers J, Arena R. Cardiopulmonary exercise testing in the clinical and prognostic assessment of diastolic heart failure. J Am Coll Cardiol. 2005;46(10):1883–1890. doi:10.1016/j.jacc.2005.07.051
28. Chen TT, Lee KY, Chang JH, et al. Prediction value of neutrophil and eosinophil count at risk of COPD exacerbation. Ann Med. 2023;55(2):2285924. doi:10.1080/07853890.2023.2285924
29. Han MK, Quibrera PM, Carretta EE, et al. Frequency of exacerbations in patients with chronic obstructive pulmonary disease: an analysis of the SPIROMICS cohort. Lancet Respir Med. 2017;5(8):619–626. doi:10.1016/S2213-2600(17)30207-2
30. Rodrigues Sousa S, Nunes Caldeira J, Rodrigues C. COPD phenotypes by computed tomography and ventilatory response to exercise. Pulmonology. 2024;30(3):222–229. doi:10.1016/j.pulmoe.2022.01.002
31. Magrì D, Fiori E, Agostoni P, et al. Heart failure and chronic obstructive pulmonary disease. A combination not to be underestimated. Heart Fail Rev. 2025;30(6):1525–1538. doi:10.1007/s10741-025-10566-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.