Back to Journals » International Journal of General Medicine » Volume 16
Variations in Post-Operative Electrolyte in Coronary Artery Intervention
Authors Fan Q, Bai Z, Ndjana Lessomo FY, Dong B, Zhong W, Jin F, Wang Z
Received 13 July 2023
Accepted for publication 11 October 2023
Published 16 October 2023 Volume 2023:16 Pages 4629—4636
DOI https://doi.org/10.2147/IJGM.S430510
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Qian Fan,1,* Zhongmei Bai,2,* Fabrice Yves Ndjana Lessomo,3,* Bingqing Dong,1 Weiqin Zhong,1 Fenglin Jin,1 Zhiquan Wang3
1Department of Cardiology, The Second Affiliated Hospital of Shandong First Medical University, Taian, Shandong Province, People’s Republic of China; 2Department of Cardiology, The People’s Hospital of Huangmei, Huanggang, Hubei Province, People’s Republic of China; 3Department of Cardiology, Zhongnan Hospital of Wuhan University, Wuhan, Hubei Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhiquan Wang; Fenglin Jin, Email [email protected]; [email protected]
Background: Low volume change and minimal trauma observed during angiography are the reason why physicians often overlook any changes affecting pre-operative electrolytes levels after coronary intervention. However, few studies have addressed the issue of electrolyte changes after the coronary intervention. Therefore, our study investigates coronary angiography’s effect on electrolytes and provides the quick identification of groups more prone to electrolyte changes.
Methods: From the department of cardiology of the second affiliated hospital of Shandong’s first medical university, 374 patients undergoing coronary angiography were selected. Pre-intervention and post-intervention serums, sodium (Na+), potassium (K+), chloride (Cl−), magnesium (Mg2+) and renal function were analyzed. The correlation between influential factors was also assessed. The association of hypokalemia with short-major adverse cardiac events (MACE) and arrhythmia was evaluated.
Results: Among the 374 subjects including 264 patients who had a simple angiography and 110 patients who received coronary artery interventional therapy. A decrease in potassium levels was found in 81.8% of the patients, and post-interventional hypokalemia was observed in 15.0%. After the intervention, the hypokalemia among males was 2.18 times than that of females, and the pre-operative serum potassium level was 3.5mmol/L≤K+< 4.0mmol/L and was 2.09 times than that of K+≥ 4.0 mmol/L, but was not associated with age and either simple coronary angiography or PCI (percutaneous coronary intervention). Hypernatremia was also prevalent in males under 60 years and with pre-operative hypernatremia. Significant variations were found between hypokalemia and influential factors like hypertension, diabetes, and gastrointestinal disease. We also found that there was no obvious correlation between hypokalemia and recurrent angina, heart failure and death, but significantly increased the risk of some arrhythmias.
Conclusion: Male patients are more likely to suffer from electrolyte disturbance after coronary intervention. There is a need to emphasize monitoring and managing electrolyte changes to prevent severe complications in the peri-operative period.
Keywords: coronary angiography, electrolytes, hypokalemia, hypernatremia, risk factors
Introduction
With the improvement in people’s living standards, increasing social pressure, decreasing physical activity, and an aging population, the number of deaths and incidence of coronary heart disease (CHD) are on the rise every year, which seriously threatens people’s life and health.1,2 CHD is caused by stenosis or occlusion of coronary atherosclerosis. Coronary angiography is the gold standard for diagnosing CHD and guiding treatment options.
Electrolyte balance and renal function are the focus of peri-operative surgeons.3,4 Gao et al found significant variations in postoperative sodium, magnesium, chloride and carbon dioxide capacity in hip arthroscopy.5 Mukherjee et al showed that percutaneous nephrolithotomy causes significant reduction renal function and no alterations in serum sodium and potassium electrolytes in the early post-operative.6 Peng et al indicated that electrolyte disturbance and serum potassium levels lower than 3.76 mmol/L were predictive factors for post-operative hypokalemia in patients undergoing hepatobiliary surgery.7 However, due to the minor trauma, short operation duration, and the absence of post-op fasting requirements following coronary angiography, the changes in electrolyte and renal function are easily overlooked by interventional doctors. Therefore, from the cardiovascular department of the second affiliated hospital of Shandong’s first medical university, the changes in electrolyte and renal function were recorded, and the population was classified based on: gender, age, pre-intervention serum potassium status, and whether PCI was done. The correlations between risk factors (hypertension, diabetes, tumors, gastrointestinal disease, thyroid disease, smoking, and drinking) and hypokalemia were also assessed. Meanwhile, we further explored the effect of sex and number of coronary vascular lesions on hypokalemia in PCI group. Lastly, the correlation between hypokalemia and short-MACE as well as arrhythmia was analyzed. This study aims to identify patients at risk for post-intervention electrolyte disturbances and optimize preventive measures.
Methods
Subjects: 374 patients diagnosed with CHD in the second affiliated hospital of Shandong’s first medical university from 2021 to 2022 were selected. There were 248 patients with stable coronary artery disease, 88 patients with unstable angina pectoris, and 38 patients with acute myocardial infarction (Figure 1). Table 1 illustrates the detailed clinical and demographic features of all the patients enrolled in this research. The Ethics Committee of the second affiliated hospital of Shandong’s first medical university approved the study.
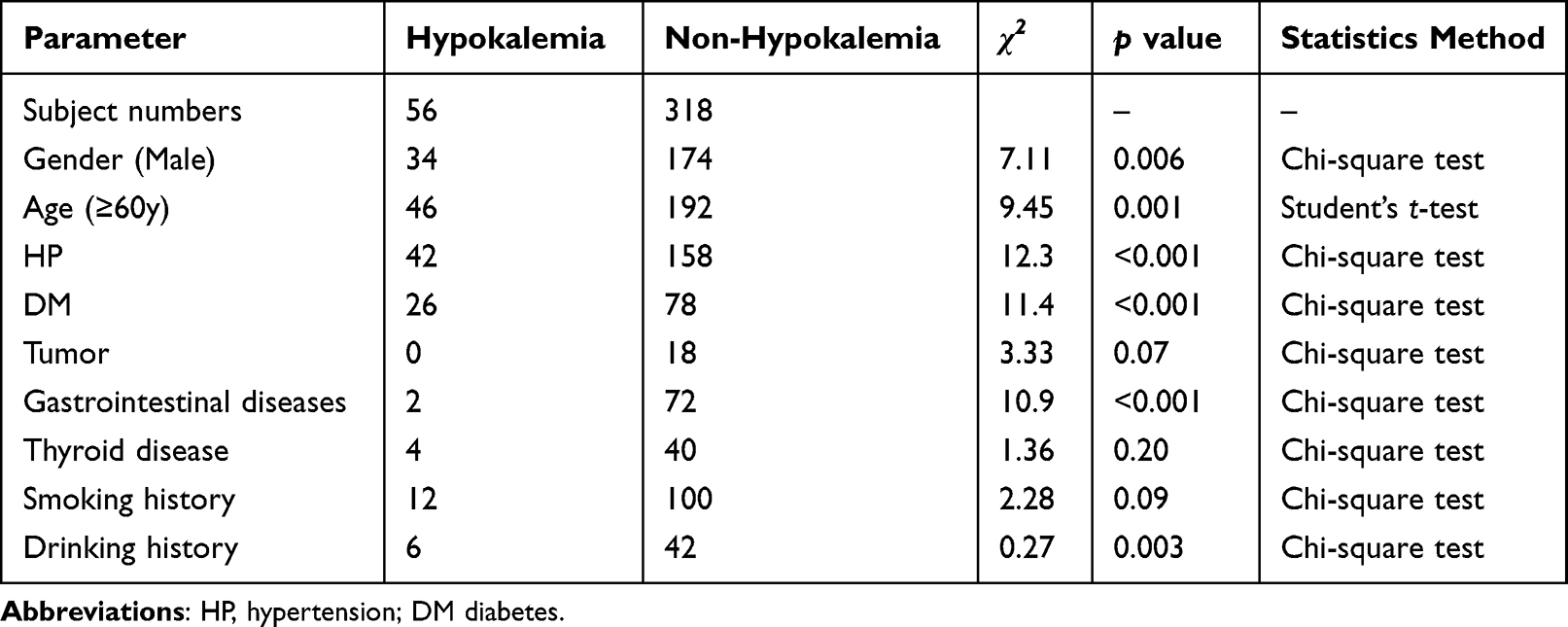 |
Table 1 Demography of Subject |
 |
Figure 1 Study design flowchart. |
Inclusion criteria: this study included all patients with CHD, including stable angina pectoris, unstable angina pectoris, and acute myocardial infarction. Indications for PCI in patients with unstable angina pectoris were defined according to the ACC/AHA guidelines for PCI published in December 2007.
Exclusion criteria: (1) patients with severe cardiac dysfunction, liver and kidney dysfunction. (2) patients with severe electrolyte disturbance, bleeding tendency, and other serious medical diseases. (3) severe uncontrolled arrhythmia such as ventricular arrhythmia, rapid atrial fibrillation, and supraventricular tachycardia. (4) complicated with fever and severe infectious diseases. (5) using large doses of diuretics, potassium salts, long-term use of glucocorticoids, and other drugs that affect serum potassium levels.
Instruments and methods: A fasting venous blood sample of 4mL was collected from 374 patients one day before coronary intervention. Serum potassium, sodium, chloride, magnesium ion, and creatinine concentrations were measured. The above patients’ parameters were measured with the same approach on the second day after intervention. Consistent with previous studies, serum potassium levels between 3.5 and 5.5 mmol/L were standard, and < 3.5 mmol/L was hypokalemia. Sodium levels between 135–145mmol/L were normal, and values above 145 mmol/L were considered hypernatremia.8,9
Statistical analysis: SPSS 21.0 software was used. Continuous data were represented as X±s, and the Student’s t-test was used for the analysis. For the categorical data, the Chi-square test was used. The risk factors were analyzed as covariates by logistic regression models. The value p<0.05 was considered statistically significant.
Results
Comparison of Electrolyte and Creatinine Levels and Incidence of Hypokalemia Before and After Coronary Angiography
For coronary artery intervention in 374 patients, a decrease in potassium levels was found in 81.8% (n=306) of the patients and post-interventional hypokalemia was observed in 15.0% (n=56) patients, increase in sodium levels was found in 65.8% (n=246) of the patients and post-interventional hypernatremia was observed in 8.02% (n=30) patients. Significant differences were observed in the variations of all other electrolyte and creatinine concentrations. The increase in chloride levels was about 0.357 mmol/L (p value=0.04). The decrease in creatinine levels was 2.84 mmol/L (p value<0.001). However, the magnesium level variation was not significant (p value=0.30) (Table 2).
 |
Table 2 Changes in Electrolytes and Creatinine Before and After Coronary Angiography |
The Effects of Gender, Age, Pre-Intervention Serum Potassium Level, and Angiography Type on the Incidence of Post-Intervention Hypokalemia
According to gender stratification, 34 of 208 male patients had hypokalemia, with an incidence of 16.4%. Furthermore, 22 of 166 female patients had hypokalemia, with an incidence of 13.3%. There was a statistically significant difference between the two groups (p value <0.05). The incidence of post-intervention hypokalemia in males was 2.18 times higher than that in females (OR=2.18, 95% CI=1.22–3.89). In addition, the incidence of post-intervention hypokalemia pre-operative serum potassium level at 3.5mmol/L≤K+<4.0mmol/L was 2.09 times higher than that K+≥4.0 mmol/L (OR=2.09, 95% CI =1.17–3.71). However, there was no statistically significant difference between post-interventional hypokalemia age and PCI treatment (p value > 0.05) (Table 3).
 |
Table 3 Different Group on the Incidence of Hypokalemia |
The Effects of Gender, Age, Pre-Intervention Serum Sodium Level, and Angiography Type on the Incidence of Post-Intervention Hypernatremia
Our analysis of post-operative hypernatremia also found that males are more prone to electrolyte disorders than males (OR=3.98, 95% CI=1.26–12.56). Interestingly, age stratification found that young people are more prone to post-operative hypernatremia than elderly people (OR=2.99, 95% CI=2.58–3.45). In addition, pre-operative patients with high blood sodium levels were 5.53 times more likely to experience electrolyte disorders than those with normal blood sodium levels (OR=5.53, 95% CI=1.24–24.69). Similarly, hypernatremia occurrence is unrelated to whether PCI treatment (Table 4).
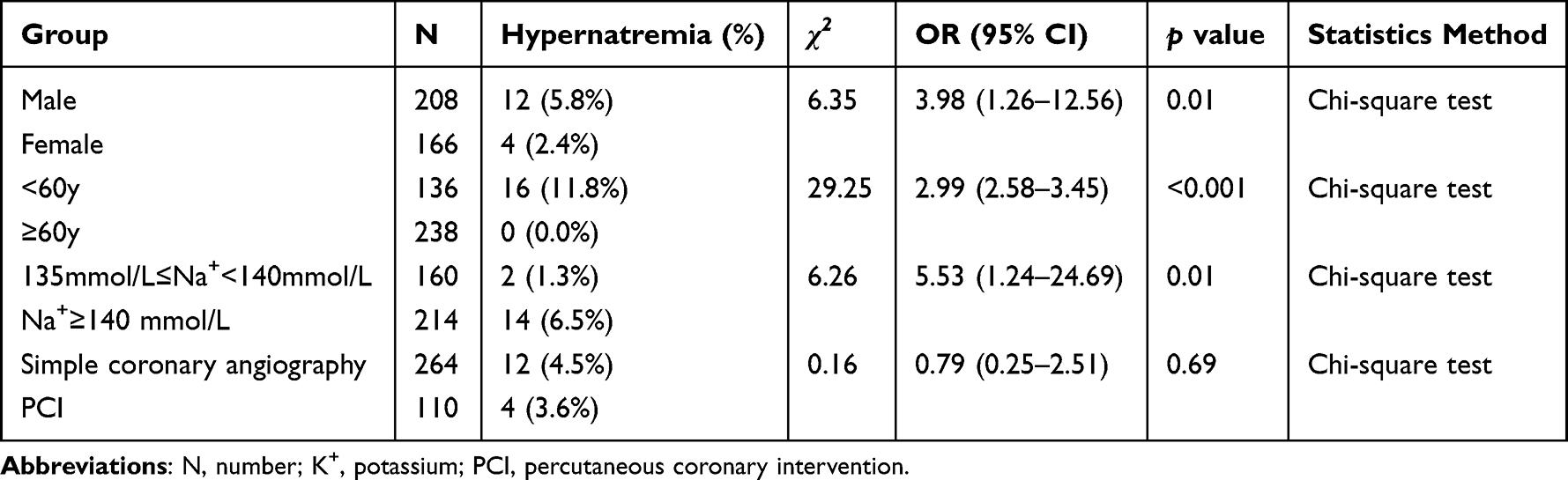 |
Table 4 Different Group on the Incidence of Hypernatremia |
The Relationship Between Post-Intervention Hypokalemia and Risk Factors
Hypokalemia was taken as the dependent variable, and the statistically significant index in univariate analysis was taken as the independent variable. The results showed that hypertension (OR=2.26, 95% CI=1.13–4.50), diabetes (OR=2.11, 95% CI=1.12–3.97), and gastrointestinal disease (OR=7.16, 95% CI=1.68–30.44) were risk factors for hypokalemia (p value <0.05) (Table 5). Unfortunately, tumors, thyroid disease, smoking, and drinking yielded no correlation.
 |
Table 5 Logistic Regression Analysis of Risk Factors Associated with Hypokalemia |
The Relationship Between Post-Intervention Hypokalemia and Gender and Number of Coronary Vascular Lesions in PCI Group
In PCI group, sex stratification also found that males are more prone to hypokalemia than female patients (OR=2.86, 95% CI=1.02–8.00). According to the number of coronary vascular lesions, it is divided into single vessel disease (SVD), double vessel disease (DVD) and multiple vessel disease (MVD), statistical analysis found no significant statistical difference in hypokalemia between the various groups (Table 6).
 |
Table 6 Relationship Between Hypokalemia and Gender and Number of Coronary Lesions After in PCI Group |
The Relationship Between Post-Intervention Hypokalemia and Short-MACE and Arrhythmia
We further analyzed the relationship between hypokalemia and short-MACE, and found that there was no obvious correlation between hypokalemia and recurrent angina, heart failure and death, but significantly increased the risk of some arrhythmias, increasing sinus tachycardia by 3.37 times (95% CI=1.36–8.33) and premature atrial contraction by 4.25 times (95% CI=2.27–7.94) (Table 7).
 |
Table 7 Relationship Between Hypokalemia and Short-MACE and Arrhythmia |
Discussion
The clinical relevance of the major electrolyte disorders in cardiovascular disease resides in their association with clinical course and in their role of provoking severe or catastrophic events (eg, syncope, sudden death). Urso et al proposed that electrolyte abnormalities are a frequent and potentially dangerous complication in subjects with congestive heart failure.10 Cavusoglu et al found that in the non-myocardial infarction subpopulation of patients, serum potassium is an independent predictor of the presence of multivessel disease.11 However, so far no relevant reports have been found on the influence of electrolytes after coronary angiography. Our study’s results showed that the sodium level significantly increased, and the potassium and creatinine levels significantly decreased after intervention (p value <0.05). Otherwise, 15% of patients had hypokalemia after angiography; the average decrease was 0.31 mmol/L. Therefore, the incidence of hypokalemia after an intervention is not negligible and should be highly valued by doctors at all levels. Patients prone to hypokalemia are associated with at least three predisposing risk factors. Firstly, patients need to be covered with multiple layers of sterile sheets during the operation, which causes them to sweat more during the operation and lose part of their potassium ions. At the same time, oral replacement fluids are often required after angiography to expel the contrast material effectively, and some potassium ions are lost during frequent urination. Secondly, peri-operative patients are prone to nervosity, anxiety, fear, and other negative emotions, so their stress level is high, which would lead to a significant increase in the synthesis and secretion of thyroxine, catecholamine, glucagon, and other substances in the body of patients, thus, promoting the transfer of potassium ions into the cells. Thirdly, the patient’s routine intraoperative fluid administration may dilute the blood, decreasing potassium. Hypokalemia is closely related to peri-operative complications and prognosis, especially when taking drugs such as hormones, liver protection, and diuretics.12–14 Because the repolarization of myocardial working cells mainly involves potassium ions, low potassium could lead to increased myocardial excitability, then increases the risk of malignant arrhythmia and even leads to patient death.15–18 The decrease of serum potassium ion can shorten stage 2 of cardiomyocyte action potential repolarization and prolong stage 3 of the action potential, which can be manifested as ST segment downshift, T wave flattening and widening U wave, and Q-T interval prolongation on body surface electrocardiogram. It might also cause a decrease in potassium conductivity in the myocardial membrane; the potassium ion outflow rate slows down in the middle diastolic period, while the sodium ion flow is relatively accelerated, and the automatic depolarization rate of action potential stage 4 increases, which leads to to the enhancement of the myocardial cells automatism and the occurrence of various rapid ectopic arrhythmias, such as atrial or ventricular premature beats, atrial or ventricular tachycardia, and even ventricular fibrillation.
On the contrary, the post-intervention blood sodium level of the patients increased by 1.2mmol/L on average. The main reason could be that intervention is a kind of stress, which would increase catecholamine and glucocorticoid secretion in patients so that the patient’s blood sugar and plasma osmotic pressure increase. When blood sugar rises to a certain extent, it can lead to osmotic diuresis in patients, causing more water loss than salt loss leading to high blood sodium levels. In addition, the creatinine level in our research decreased after intervention. It was statistically significant compared to before the intervention. This observation differed from previous studies suggesting that contrast media would increase the risk of acute renal failure.19,20 The analysis of the reason may be related to the pre-operative hydration therapy. Different defining criteria make it difficult to explore the true incidence of contrasts-associated nephropathy further.
Stratified analysis was performed according to gender, age, pre-operative electrolyte status, and intervention type. Our study found that male patients are more likely to have post-intervention hypokalemia and hypernatremia. Younger patients are more likely to experience post-operative hypernatremia than older patients. Male patients are more prone to electrolyte disorders than females, which may be due to greater social and family pressure, anxiety, and stress that may more likely induce metabolic disorders, and the incidence of comorbidities such as hypertension differed according to gender. The prevalence of hypernatremia in young patients could be related to a high-salt diet, and elderly patients with hypertension and congestive heart failure often need to take diuretic drugs that lead to increased excretion of sodium ions.
We also analyzed the association of risk factors such as hypertension, diabetes, tumor, gastrointestinal disease, thyroid disease, smoking, drinking, and hypokalemia. The study noticed that patients with hypertension, diabetes, and gastrointestinal diseases had a higher probability of post-operative hypokalemia. Hypertension patients are prone to post-operative hypokalemia analysis, and the renin-angiotensin-aldosterone system is also involved. Zhu et al also found that the incidence rate of hypertension was more significant in hypokalemic than non-hypokalemic patients scheduled for laparoscopic colorectal resection.21 There are many reasons for hypokalemia in diabetic patients. The main reasons being osmotic diuresis caused by hyperglycemia, patients’ use of insulin, and autonomic neuropathy of the digestive tract caused by diabetes. Patients with gastrointestinal diseases are more prone to post-operative hypokalemia due to digestive and absorption disorders.
According to our data, male patients seem prone to hypokalemia and hypernatremia after the intervention. Therefore, we should pay special attention to electrolyte disorders in male patients, especially those with hypertension, diabetes, and gastrointestinal disease history, to prevent serious complications caused by electrolyte disorders.
Nevertheless, our study also had several limitations. Firstly, this study is a single-center retrospective study with small sample size and some missing sample values. A multi-center randomized controlled study could be conducted in the future. Secondly, the levels of electrolytes and creatinine in patients with coronary heart disease often change dynamically after the intervention; only the electrolytes and creatinine levels of patients on the first day after the operation were selected for our study, and they could be more dynamically monitored in the future.
Conclusions
In conclusion, the incidence of hypokalemia after intervention is high in patients with CHD, especially in male patients. Therefore, serum potassium concentration should be intentionally monitored and supplemented before and after intervention as appropriate.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethical Approval and Consent to Participate
The studies involving human participants were reviewed and approved by the Medical Ethics Committee, the second affiliated hospital of Shandong’s first medical university (No 2023-049). As this study is retrospective and presents no risk of harm to subjects, and no privacy of individuals is exposed, informed consent was waived. All procedures adhered to the ethical standards and the Helsinki Declaration (as revised in 2013).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interest in this work.
References
1. Lv J, Yu C, Guo Y, et al. Adherence to healthy lifestyle and cardiovascular diseases in the Chinese population. J Am Coll Cardiol. 2017;69(9):1116–1125. doi:10.1016/j.jacc.2016.11.076
2. Shen C, Ge J. Epidemic of cardiovascular disease in China: current perspective and prospects for the future. Circulation. 2018;138(4):342–344. doi:10.1161/CIRCULATIONAHA.118.033484
3. Verhelst L, De Schepper J, Sergeant G, Liekens K, Delport H. Variations in serum electrolyte concentrations and renal function after therapeutic Hip arthroscopy: a pilot study. Arthroscopy. 2009;25(4):377–381. doi:10.1016/j.arthro.2008.10.023
4. Haupt U, Volkle D, Waldherr C, Beck M. Intra- and retroperitoneal irrigation liquid after arthroscopy of the Hip joint. Arthroscopy. 2008;24(8):966–968. doi:10.1016/j.arthro.2007.02.019
5. Gao G, Zhou C, Ao Y, Wang J, Xu Y. Variations in post-operative electrolyte concentrations and influential factors in Hip arthroscopy. BMC Musculoskelet Disord. 2022;23(1):473. doi:10.1186/s12891-022-05451-1
6. Mukherjee S, Sinha RK, Jindal T, Sharma PK, Mandal SN, Karmakar D. Short-term alteration of renal function and electrolytes after percutaneous nephrolithotomy. Urol J. 2019;16(6):530–535. doi:10.22037/uj.v0i0.4558
7. Peng H, Zhang Q, Qian J, et al. Electrolyte disorders are ERAS-associated in patients undergoing hepato-pancreato-biliary surgery. Langenbecks Arch Surg. 2020;405(5):603–611. doi:10.1007/s00423-020-01922-y
8. Lu G, Yan Q, Huang Y, Zhong Y, Shi P. Prevention and control system of hypokalemia in fast recovery after abdominal surgery. Curr Ther Res Clin Exp. 2013;74:68–73. doi:10.1016/j.curtheres.2013.02.004
9. Muhsin SA, Mount DB. Diagnosis and treatment of hypernatremia. Best Pract Res Clin Endocrinol Metab. 2016;30(2):189–203. doi:10.1016/j.beem.2016.02.014
10. Urso C, Brucculeri S, Caimi G. Acid-base and electrolyte abnormalities in heart failure: pathophysiology and implications. Heart Fail Rev. 2015;20(4):493–503. doi:10.1007/s10741-015-9482-y
11. Cavusoglu E, Chopra V, Gupta A, et al. Relation of baseline serum potassium levels to angiographic findings in patients with known or suspected coronary artery disease. Am J Hypertens. 2009;22(7):754–762. doi:10.1038/ajh.2009.65
12. Sanjay OP. pre-operative serum potassium levels and peri-operative outcomes in patients undergoing cardiac surgery. Indian J Clin Biochem. 2004;19(1):40–44. doi:10.1007/BF02872387
13. Wahr JA, Parks R, Boisvert D, et al. Pre-operative serum potassium levels and peri-operative outcomes in cardiac surgery patients. Multi-center Study of Peri-operative Ischemia Research Group. JAMA. 1999;281(23):2203–2210. doi:10.1001/jama.281.23.2203
14. Lee S, Kang E, Yoo KD, et al. Lower serum potassium associated with increased mortality in dialysis patients: a nationwide prospective observational cohort study in Korea. PLoS One. 2017;12(3):e171842.
15. Ferreira JP, Butler J, Rossignol P, et al. Abnormalities of potassium in heart failure: JACC State-of-the-Art Review. J Am Coll Cardiol. 2020;75(22):2836–2850. doi:10.1016/j.jacc.2020.04.021
16. Ma Y, He FJ, Sun Q, et al. 24-Hour urinary sodium and potassium excretion and cardiovascular risk. N Engl J Med. 2022;386(3):252–263. doi:10.1056/NEJMoa2109794
17. Dreier R, Andersen UB, Forman JL, Sheykhzade M, Egfjord M, Jeppesen JL. Effect of increased potassium intake on adrenal cortical and cardiovascular responses to angiotensin II: a randomized crossover study. J Am Heart Assoc. 2021;10(9):e18716. doi:10.1161/JAHA.120.018716
18. Jones DW, Clark DR, Morgan TO, He FJ. Potassium-enriched salt substitution as a population strategy to prevent cardiovascular disease. Hypertension. 2022;79(10):2199–2201. doi:10.1161/HYPERTENSIONAHA.122.19248
19. Maioli M, Toso A, Leoncini M, Gallopin M, Musilli N, Bellandi F. Persistent renal damage after contrast-induced acute kidney injury: incidence, evolution, risk factors, and prognosis. Circulation. 2012;125(25):3099–3107. doi:10.1161/CIRCULATIONAHA.111.085290
20. Rear R, Bell RM, Hausenloy DJ. Contrast-induced nephropathy following angiography and cardiac interventions. Heart. 2016;102(8):638–648. doi:10.1136/heartjnl-2014-306962
21. Zhu Q, Li X, Tan F, et al. Prevalence and risk factors for hypokalemia in patients scheduled for laparoscopic colorectal resection and its association with post-operative recovery. BMC Gastroenterol. 2018;18(1):152. doi:10.1186/s12876-018-0876-x
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.