")
Back to Journals » International Journal of General Medicine » Volume 16
Valve Surgery in a Low-Volume Center in a Low- and Middle-Income Country: A Retrospective Cross-Sectional Study
Authors Bani Hani A , Awamleh N, Mansour S , Toubasi AA, AlSmady M, Abbad M, Banifawaz M, Abu Abeeleh M
Received 4 August 2023
Accepted for publication 26 September 2023
Published 16 October 2023 Volume 2023:16 Pages 4649—4660
DOI https://doi.org/10.2147/IJGM.S433722
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Amjad Bani Hani,1 Nour Awamleh,2 Shahd Mansour,2 Ahmad A Toubasi,2 Moaath AlSmady,1 Mutaz Abbad,1 Mohammad Banifawaz,1 Mahmoud Abu Abeeleh1
1Department of General Surgery, Division of Cardiac Surgery, The University of Jordan, Amman, 11942, Jordan; 2School of Medicine, The University of Jordan, Amman, 11942, Jordan
Correspondence: Shahd Mansour, School of Medicine, The University of Jordan, PO Box 13046, Amman, 11942, Jordan, Tel +962 6 5355000, Email [email protected]
Background: Valvular heart disease (VHD) has a significant prevalence and mortality rate with surgical intervention continuing to be a cornerstone of therapy. We aim to report the outcome of patients undergoing heart valve surgery (HVS) in a low-volume center (LVC) in a low- and middle-income country (LMIC).
Methods: A cross-sectional retrospective study was conducted at the Jordan University Hospital (JUH), a tertiary teaching hospital in a developing country, between April 2014 and December 2019. Patients who underwent mitral valve replacement (MVR), aortic valve replacement (AVR), tricuspid valve replacement (TVR), double valve replacement (DVR), CABG + MVR, and CABG + AVR patients were included. Thirty-day and two-year mortalities were taken as the primary and secondary outcomes, respectively.
Results: A total number of 122 patients were included, and the mean age was 54.46 ± 14.89 years. AVR was most common (42.6%). There was no significant association between STS mortality score or Euroscore II with 30-day and 2-year mortality.
Conclusion: LVC will continue to have a role in LMICs, especially during development to HICs. Further global studies are needed to assert the safety of HVS in LVC and LMICs.
Keywords: valve surgery, low-volume center, low- and middle-income country
Introduction
The main cause of death worldwide is cardiovascular disease (CVD), which accounts for over 17.5 million deaths annually, 80% of which take place in low- and middle-income countries.1
One of the major causes of CVD is valvular heart disease (VHD), which has a significant prevalence and mortality rate.2,3 VHD affects 2.5% of the adult population in the United States, with aortic and mitral valve disease accounting for most cases.4 For both aortic and mitral valve disease, surgical intervention continues to be a cornerstone of therapy and is associated with significant improvements in patient morbidity and mortality. However, valve surgeries are complicated, with significant perioperative morbidity and mortality.5
Most of the world’s population reside in low- and middle-income countries (LMICs) without adequate access to cardiac surgical care. In addition, these countries are facing increased burden of CVD due to many factors such as population growth, urbanization of CVD disease, and transition from communicable to noncommunicable diseases.6
Despite the progress made within the field of global cardiac surgery, there is still uncertainty regarding cardiac surgical services in LMIC which are needed in up to 33% of CVD cases. Still, six billion people lack access to safe, inexpensive cardiac surgical care when it is necessary. Cardiothoracic surgery is behind non-cardiac surgical treatment in terms of importance as a component of healthcare.6 In LMICs, whether cardiac surgery is provided at all and at what level depends primarily on four key factors; government commitment and resource availability, primary healthcare systems, which are frequently insufficient and fall short in their front-line role towards prophylaxis and diagnostic monitoring, socioeconomic factors that cause rheumatic heart disease (RHD) in the first place, and the highly specialized field of cardiac surgery, whose standards differ from how it is carried out in the developed world.7
Studies have shown better performance and lower mortality rates in high-volume centers. On the other hand, 30-day and 1-year mortality rates are higher in low-volume centers for many procedures performed, including CABG, aortic valve replacement, and mitral valve replacement.8–10 Nevertheless, most of the data published regarding this subject emerge from high-volume centers. Consequently, this raises concerns about the generalizability of their findings and the reproducibility of valve surgery in low-volume centers. Our study aims to report the outcome of patients undergoing valvular surgery in a low-volume center in a LMIC.
Methods
Study Design and Population
Retrospective data was extracted from the cardiovascular database of the Jordan University Hospital, a low-volume center. A total of 122 patients who underwent valvular heart surgery between April 2014 and December 2019 were included. We included mitral valve replacement (MVR), aortic valve replacement (AVR), tricuspid valve replacement (TVR), double valve replacement (DVR), CABG and MVR, and CABG and AVR patients. The exclusion criteria were urgent cases, age under 18 years, and CABG only surgery. Thirty-day mortality was taken as the primary outcome, which involves death within 30 post-operative days. The secondary outcome was death in 2-year follow-up. We systematically collected preoperative patient variables, surgical procedure information (including type of procedure), and postoperative clinical outcomes to calculate the STS and EuroSCORE II risk scores.11,12 The EuroSCORE II score included age, sex, angina symptoms, insulin-dependent diabetes mellitus, New York Heart Association functional class, peripheral artery disease, neurological or musculoskeletal dysfunction severely affecting mobility, previous cardiac surgery, chronic pulmonary disease, pulmonary artery systolic pressure, renal function with creatinine clearance, critical preoperative state, active endocarditis, left ventricular ejection fraction, recent myocardial infarction, procedure urgency and weight of the procedure. The STS score included 67 demographic and operative variables.
Data Analysis
Counts and percentages were used to present categorical variables while mean and standard deviation were used to interpret continuous variables. Chi-square test was used to identify the factors associated with patients’ mortality. T-test and correlation coefficients were used to assess the factors associated with patient’s STS scores as appropriate. Any test with a P-value <0.05 was considered statistically significant. IBM SPSS v.26 was used to conduct the analysis.
Ethics
This study was approved by Jordan University Hospital Institutional Review Board, and all procedures performed were in accordance with the ethical standards of the institutional and national research committee and the principles of the World Medical Association Declaration of Helsinki. The requirement for informed consent was waived because this study was retrospective, conformed to standards for minimal risk research and did not affect patient safety or clinical care. To protect patient confidentiality, personal identifiers were removed from spreadsheets used for data analyses and all reports.
Results
Characteristics of the Included Patients
The total number of the patients who underwent valve replacement surgery from 2014 to 2019 was 124. Two patients were excluded from the analysis due to insufficient data in their medical records resulting in 122 patients included in the analysis. The percentage of females in the included patients was 57.4% and the mean age was 54.46 ± 14.89. Most of the patients had hypertension (54.1%) and 31.1% of the cohort had diabetes. Triple vessel disease existed in 1.6% of the patients and 5.7% of the patients had >70.0% Left Anterior Descending (LAD) stenosis Table 1. Furthermore, 36.9% of the patients had aortic stenosis and 37.7% of the patients had mitral a. The frequencies of severe aortic, mitral, and tricuspid regurgitation were 8.2%, 16.4% and 0.8%, respectively. Additionally, the most frequent valve disease etiology was degenerative valve (33.6%) Table 2. Atrial fibrillation existed in 16.4% of the included patients whereas 24.6% of the patients were current smokers. Most of the patients underwent cardiac intervention previously (55.7%) Table 3. All surgeries were elective in status and only 1.6% of the patients received intra-aortic balloon pump. Most of the patients underwent aortic valve replacement surgery (42.6%) followed by mitral valve surgery (35.2%) Table 4. The mean of the ejection fraction and creatinine level before the surgery were 48.80% ± 7.64% and 0.81 ± 0.65, respectively. Of the included patients, 3.3% died within 30 days of the surgery and 4.1% of them died within 2 years of it. The mean risk of mortality STS and Euroscore II were 1.8 ± 1.21 and 1.7 ± 1.71, respectively Table 5.
 |
Table 1 Comorbidities of Participants |
 |
Table 2 Valve Pathology |
 |
Table 3 Cardiovascular Characteristics of Participants |
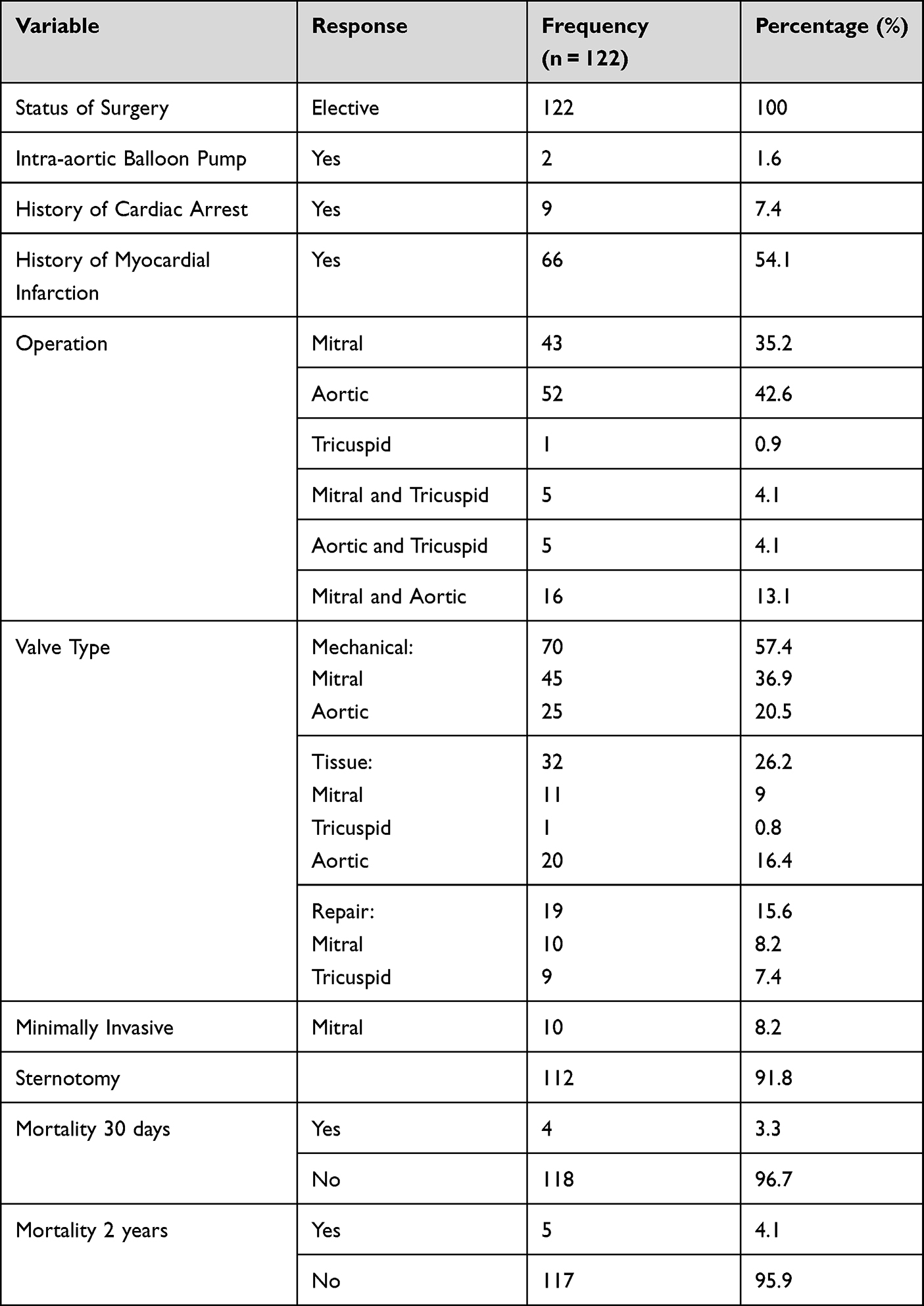 |
Table 4 Surgical Characteristics of Participants |
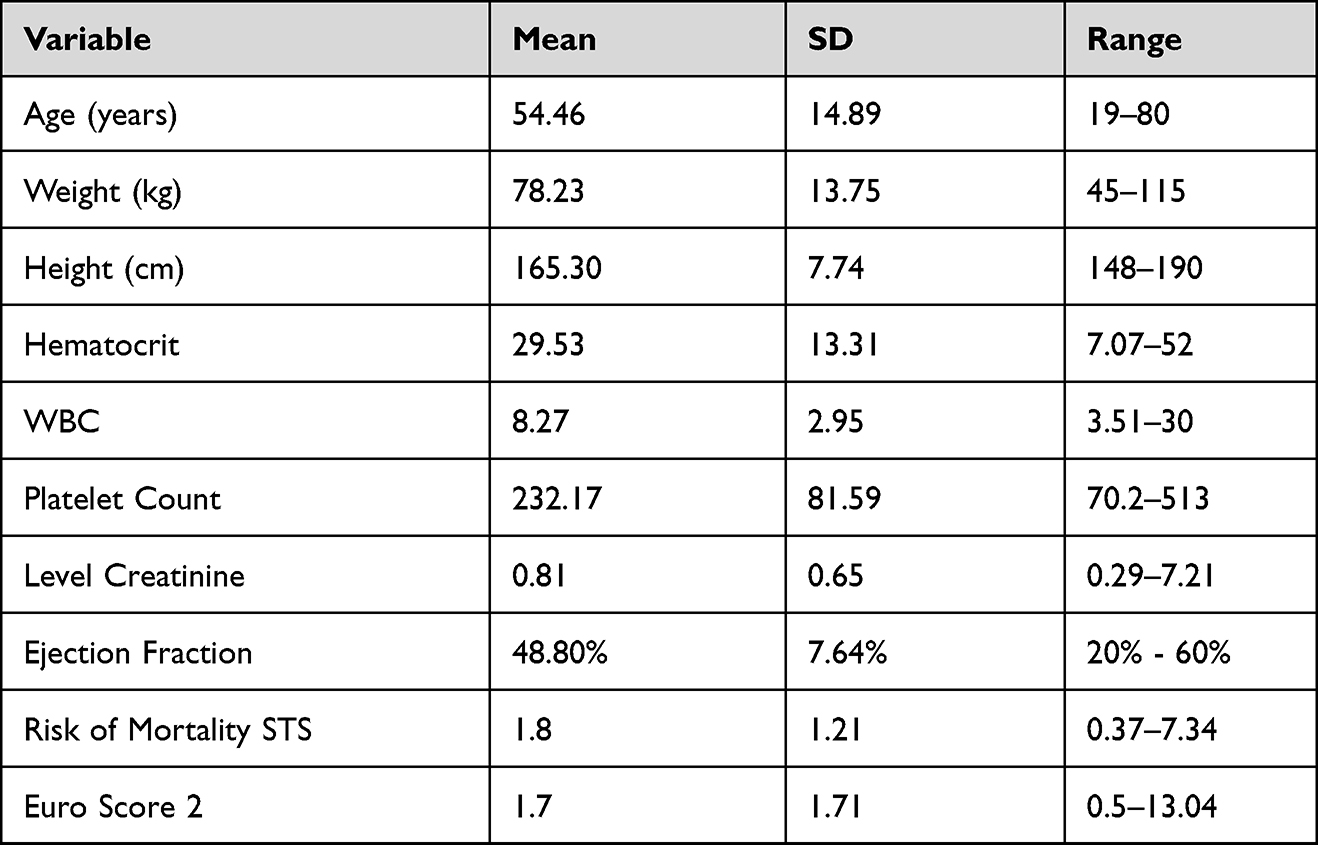 |
Table 5 Demographic Characteristics of Participants |
Factors Associated with 30-Day Mortality and 2-Year Mortality
Regarding the factors associated with 30-day mortality, cancer within the last 5 years was significantly associated with 30-day mortality (P-value=0.012) as the patients who had cancer had significantly higher 30-day mortality rate than their counterparts. Furthermore, patients who had respiratory diseases and poor mobility and had significantly higher 30-day mortality rate (P-value=0.001, P-value<0.001). Patients who were on insulin therapy and Angiotensin Converting Enzyme Inhibitor/Angiotensin Receptor Blockers had significantly lower 30-day mortality rate (P-value=0.011, P-value=0.038). Patients who presented with cardiogenic shock or needed Intra-aortic Balloon Pump had significantly higher 30-day mortality (P-value<0.001, P-value=0.001). The analysis of the factors associated with 2-year mortality demonstrated that patients who had atrial flutter, third-degree heart block and second-degree heart block had significantly higher 2-year mortality (P-value<0.001). Patients on beta-blockers had significantly lower 2-year mortality rate than their counterparts (P-value=0.048). Additionally, higher age, platelet count and creatinine level were associated with significantly higher 2-year mortality. Additionally, lower ejection fraction was significantly associated with 2-year mortality (P-value=0.046). Moreover, there was no significant association between STS mortality score or Euroscore II with 30-day and 2-year mortality Table 6.
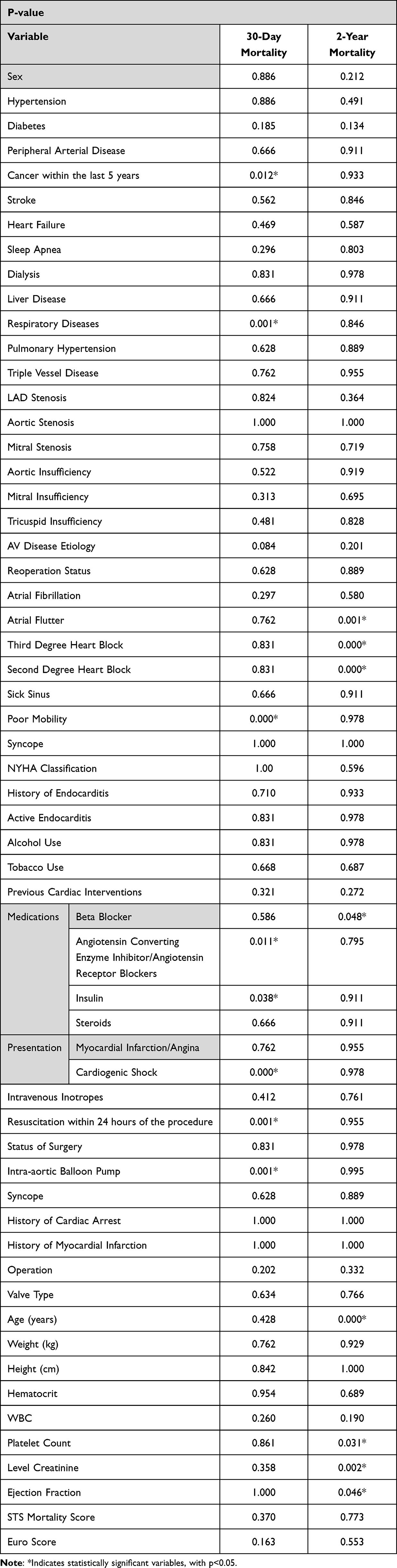 |
Table 6 Factors Associated with Patients’ Mortality |
Discussion
Most of the world’s population live in LMICs, with delayed and even limited access to cardiac surgery service contrary to the needs and availability for this service in high-income countries (HICs). Approximately one-third of people with CVD in LMICs will probably need surgery, but more than 90% of them have no access.1,13,14 Jordan is Classified as an upper-middle income country, part of LMIC, by the World Bank. Only 55% of Jordan’s population are insured through both public and private insurance.15,16 The total health expenditures are equivalent to 7.5% of the GDP,17 which is relatively high when compared to LMICs (5.8%) but still low compared to HIC (11.8%).1,18 This low GPD makes the relative cost of cardiac surgery in LMICs high in comparison with HIC, in spite of the low crude cost of these surgeries in LMICs.1
Another problem that LMICs face is the availability of well-trained healthcare providers, and multi-discipline teams.7 A study of the adult cardiac surgeons registered in CTSNET records showed the presence of 11.12 surgeons per million people in North America, which constitute around 33% of total surgeons worldwide. In comparison, sub-Saharan Africa had 0.12 surgeons per million people (1.05% of total).1 In this study, Jordan has 1.7 adult cardiac surgeons per million. The number of cardiac surgeons registered in the Jordanian Association of Cardiac Surgeons and living in Jordan, whether practicing or not, is 4 per million people, which is still low compared to LMICs.
In this low-volume center retrospective study conducted in an LMIC, the median age was 54.5 years, a lot younger than in developed countries, ranging from 64 years in Euro Heart Survey on Valvular Heart Disease19 and 68 in the German Valve registry.20 However, it is similar to numbers from Jordan and other LMICs.21–23 This is explained by the younger population of Jordan where approximately 35% of the population is younger than 15 years, and only 3.7% is older than 65 years.15 This will probably change in the future as people above 60 will constitute around 16% of the population in 2050,24 which will further increase the demands on cardiac surgery services.
We report a 30-day mortality rate of 3.3% and 2-year mortality rate of 4.1%. Most studies found in the literature are those of high-volume centers in HIC demonstrating excellent performance and lower mortality rates. On the other hand, higher mortality rates are usually reported in low-volume centers, including valve replacement8,9 Usually, these represent high volume of single valve surgery, whereas when we look at the national registries or combined valves surgery, such as our cohort, we find comparable results.25 The mortality rate in Germany varies from 3.6 for aortic valve replacement to 12.4 in aortic and mitral valve procedures.26 Other studies reported 30-day postoperative mortality of 6.7% and equally distributed among the two cohorts27 and an in-hospital mortality of 7.6% that is higher for female patients who had undergone concomitant CABG and for the elderly.21 Concomitant CABG significantly increases mortality.28,29
Strong evidence exists correlating center’s volume with outcome but the effect that individual surgeons experience rather than centers’ total volume has on the output is controversial.30 Other studies showed better outcomes were achieved in hospitals specializing in CABG independent of CABG volume or patients’ characteristics.30,31 When in-hospital risk-standardized mortality rate (RSMR) was taken into consideration, there was only a weak association between volume and mortality rate. In addition, if volume is the only indicator of quality of care, it is possible to misclassify a large proportion of hospitals.32 Volume seems to be a logical metric that is simple to monitor and evaluate, which is why payers and legislators began financing volume minimums as a substitute for the quality of treatment delivered.33 As small centers and hospitals are the primary service providers in rural and small communities, referral policies that are based on volume can give high-volume centers and hospitals a financial advantage while discouraging smaller ones from competing.34 Most notably, employing volume as the only proxy may be less significant when completely collected and risk-adjusted results are readily accessible.35,36
The etiology of VHD in our cohort is mixed between RHD, as in low-income countries, and degenerative and calcified valves, as in HIC. This is partly due to improvement of health care system as represented by the increase in life expectancy from mid-forties to mid-seventies, in association with westernization of lifestyle.24,37
We performed 10 cases of minimally invasive mitral surgery and 7 cases of mitral valve repair, which is very low when compared with HIC. Valve repair and MIC are not routinely performed due to many reasons such as referral delay, absence of specialized centers and surgeons, lack of enough volume to maintain repair skills, difficulty in performing a conclusive intraoperative echocardiography, and the absence of universal public health insurance for Jordanians and non-Jordanians.
Studies show that valvular surgery, especially aortic valve replacement, is associated with postoperative cerebrovascular incidents that can reach up to 10% of patients and can have a significant effect on patients’ survival and quality of life.38,39 In our study, only two patients (1.6%) developed stroke as a complication postoperatively, one of which was transient ischemic attack. This could be due to the younger mean age of our cohort.
Furthermore, bleeding is another post-operative complication that 5 patients (4.1%) in our study have suffered from. Bleeding is a serious complication of cardiac surgery that increases the rate of re-exploration, requirement of blood transfusion, length of hospital stay, morbidity, and mortality.40 Subsequently, this re-exploration is associated with more complications, like renal impairment, wound infection, and postoperative arrhythmias.41 In our study, 4 patients (3.3%) have undergone reoperation for bleeding or cardiac tamponade which is similarly low to other studies.42,43 As for surgical site infection (SSI), another common complication, literature shows that it ranges from 3% to 10.4% and leads to prolonged hospitalization and increased morbidity and mortality.44 Our results show that only one patient (0.8%) had SSI. Interestingly, 4 of our patients (3.3%) were readmitted post-op due to developing warfarin toxicity.
Lastly, some important predictors of outcome with 30-day have been studied. As expected, preoperative respiratory disease, poor mobility, cardiogenic shock, cancer within the last 5 years, and intraoperative intra-aortic balloon pump insertion were significant risk factors for 30-day mortality. Similarly, preoperative atrial flutter, post-operative second-degree and third-degree block, older age, higher platelet count and creatinine level, and decreased ejection fraction are associated with significantly higher 2-year mortality. Similar findings have also been reported in previous studies.45
LMICs are currently facing problems similar to the ones that HICs have overcome.7 Hence, implementing current HIC standards on old problems may be unfair for LMICs. In conclusion, we think that performing heart valve surgery (HVS) in an LVC in LMICs is feasible without putting patients under increased risk, and LVC will continue to have a role in LMICs even during development from an LMIC to an HIC. Further global studies are needed to assert the safety of HVS in LVC especially in LMICs.45,46
Limitations
This study is subject to a few limitations. It is a single-center study with a small sample size, which limits the national generalizability of our conclusion. Also, this is a retrospective study which led to the exclusion of some patients due to incomplete data.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vervoort D, Meuris B, Verbrugghe P, et al. Global cardiac surgery: access to cardiac surgical care around the world. J Thorac Cardiovasc Surg. 2020;159(3):987–996.e6. doi:10.1016/J.JTCVS.2019.04.039
2. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368(9540):1005–1011. doi:10.1016/S0140-6736(06)69208-8
3. Draper J, Subbiah S, Bailey R, Chambers JB. Murmur clinic: validation of a new model for detecting heart valve disease. Heart. 2019;105(1):56–59. doi:10.1136/HEARTJNL-2018-313393
4. Benjamin EJ, Blaha MJ, Chiuve SE, et al. Heart disease and stroke statistics-2017 update: a report from the American Heart Association. Circulation. 2017;135(10). doi:10.1161/CIR.0000000000000485
5. Nishimura RA, Otto CM, Bonow RO, et al. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association task force on practice guidelines. Circulation. 2014;129(23):2440–2492. doi:10.1161/CIR.0000000000000029
6. Vervoort D, Swain JBD, Pezzella AT, Kpodonu J. Cardiac surgery in low- and middle-income countries: a state-of-the-art review. Ann Thorac Surg. 2021;111(4):1394–1400. doi:10.1016/J.ATHORACSUR.2020.05.181
7. Zilla P, Morton Bolman R, Boateng P, Sliwa K. A glimpse of hope: cardiac surgery in low- and middle-income countries (LMICs). Cardiovasc Diagn Ther. 2020;10(2):336–349. doi:10.21037/CDT.2019.11.03
8. Badhwar V, Vemulapalli S, Mack MA, et al. Volume-outcome Association of mitral valve surgery in the United States. JAMA Cardiol. 2020;5(10):1092. doi:10.1001/JAMACARDIO.2020.2221
9. Reames BN, Ghaferi AA, Birkmeyer JD, Dimick JB. Hospital volume and operative mortality in the modern era. Ann Surg. 2014;260(2):244–251. doi:10.1097/SLA.0000000000000375
10. Pieper D, Mathes T, Neugebauer E, Eikermann M. State of evidence on the relationship between high-volume hospitals and outcomes in surgery: a systematic review of systematic reviews. J Am Coll Surg. 2013;216(5):1015–1025e18. doi:10.1016/J.JAMCOLLSURG.2012.12.049
11. EuroScore Website - calculator. Available from: https://www.euroscore.org/index.php?id=17.
12. Online STS Risk Calculator. Available from: https://riskcalc.sts.org/stswebriskcalc/calculate.
13. Rose J, Chang DC, Weiser TG, Kassebaum NJ, Bickler SW, Manchikanti L. The role of surgery in global health: analysis of United States inpatient procedure frequency by condition using the Global Burden of Disease 2010 framework. PLoS One. 2014;9(2):e89693. doi:10.1371/JOURNAL.PONE.0089693
14. Kumar RK, Shrivastava S. Paediatric heart care in India. Heart. 2008;94(8):984–990. doi:10.1136/HRT.2007.139360
15. Jordan population and housing census; 2015. Available from: http://www.dos.gov.jo/dos_home_e/main/population/census2015/Main_Result.pdf.
16. Al-Ajlouni R, Al Rabayah A. Will Jordan be closer to UHC after the COVID-19 pandemic? J Glob Health. 2020;10(2):1–4. doi:10.7189/JOGH.10.020360
17. Global Health Observatory country views: Jordan statistics summary. Available from: https://data.worldbank.org/country/JO.
18. Leirner AA. The health and wealth of nations--coping with limited resources. Artif Organs. 2006;30(7):493–497. doi:10.1111/J.1525-1594.2006.00249.X
19. Iung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: the Euro heart survey on valvular heart disease. Eur Heart J. 2003;24(13):1231–1243. doi:10.1016/S0195-668X(03)00201-X
20. Hamm CW, Mollmann H, Holzhey D, et al. The German Aortic Valve Registry (GARY): in-hospital outcome. Eur Heart J. 2014;35(24):1588–1598. doi:10.1093/EURHEARTJ/EHT381
21. de Aquino Xavier RM, Azevedo VMP, Godoy PH, et al. Medium-term outcomes of 78,808 patients after heart valve surgery in a middle-income country: a nationwide population-based study. BMC Cardiovasc Disord. 2017;17(1). doi:10.1186/S12872-017-0725-9
22. Ibrahim KS, Kheirallah KA, Mayyas FA, Alwaqfi NR, Alawami MH, Aljarrah QM. Predictors of short-term mortality after rheumatic heart valve surgery: a single-center retrospective study. Ann Med Surg. 2021;62:395–401. doi:10.1016/J.AMSU.2021.01.077
23. Debel FA, Zekarias B, Centella T, Tekleab AM. Immediate outcome following valve surgery for rheumatic heart disease: the first local experience from Ethiopia. Cardiol Young. 2020;30(9):1281–1287. doi:10.1017/S1047951120001997
24. Halaseh L. Jordan. Int J Ageing Dev Ctries. 2021;6(2):176–198.
25. Beyersdorf F, Bauer T, Freemantle N, et al. Five-year outcome in 18 010 patients from the German aortic valve registry. Eur J Cardiothorac Surg. 2021;60(5):1139–1146. doi:10.1093/EJCTS/EZAB216
26. Beckmann A, Meyer R, Lewandowski J, Frie M, Markewitz A, Harringer W. German heart surgery report 2017: the annual updated registry of the German Society for thoracic and cardiovascular surgery. Thorac Cardiovasc Surg. 2018;66(8):608–621. doi:10.1055/S-0038-1676131
27. Egger ML, Gahl B, Koechlin L, et al. Outcome of patients with double valve surgery between 2009 and 2018 at university hospital Basel, Switzerland. J Cardiothorac Surg. 2022;17(1). doi:10.1186/S13019-022-01904-9
28. Nicolini F, Agostinelli A, Fortuna D, et al. Outcomes of patients undergoing concomitant mitral and aortic valve surgery: results from an Italian regional cardiac surgery registry. Interact Cardiovasc Thorac Surg. 2014;19(5):763–770. doi:10.1093/ICVTS/IVU248
29. Leavitt BJ, Baribeau YR, DiScipio AW, et al. Outcomes of patients undergoing concomitant aortic and mitral valve surgery in northern new England. Circulation. 2009;120(11 Suppl). doi:10.1161/CIRCULATIONAHA.108.843573
30. Ch’ng SL, Cochrane AD, Wolfe R, et al. Procedure-specific cardiac surgeon volume associated with patient outcome following valve surgery, but not isolated CABG surgery. Heart Lung Circ. 2015;24(6):583–589. doi:10.1016/J.HLC.2014.11.014
31. Girotra S, Lu X, Popescu I, Vaughan-Sarrazin M, Horwitz PA, Cram P. The impact of hospital cardiac specialization on outcomes after coronary artery bypass graft surgery: analysis of medicare claims data. Circ Cardiovasc Qual Outcomes. 2010;3(6):607–614. doi:10.1161/CIRCOUTCOMES.110.943282
32. Khera R, Pandey A, Koshy T, et al. Role of hospital volumes in identifying low-performing and high-performing aortic and mitral valve surgical centers in the United States. JAMA Cardiol. 2017;2(12):1322–1331. doi:10.1001/JAMACARDIO.2017.4003
33. Birkmeyer JD, Siewers AE, Finlayson EVA, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346(15):1128–1137. doi:10.1056/NEJMSA012337
34. Panaich SS, Patel N, Arora S, et al. Influence of hospital volume and outcomes of adult structural heart procedures. World J Cardiol. 2016;8(4):302. doi:10.4330/WJC.V8.I4.302
35. Kumbhani DJ, Nallamothu BK. PCI volume benchmarks: still adequate for quality assessment in 2017? J Am Coll Cardiol. 2017;69(24):2925–2928. doi:10.1016/J.JACC.2017.04.050
36. Badhwar V, Rankin JS, He X, et al. The Society of thoracic surgeons mitral repair/replacement composite score: a report of The Society of thoracic surgeons quality measurement task force. Ann Thorac Surg. 2016;101(6):2265–2271. doi:10.1016/J.ATHORACSUR.2015.11.049
37. Chen Y, Yiu KH. Growing importance of valvular heart disease in the elderly. J Thorac Dis. 2016;8(12):E1701. doi:10.21037/JTD.2016.12.23
38. Hogue CW, Murphy SF, Schechtman KB, Dávila-Román VG. Risk factors for early or delayed stroke after cardiac surgery. Circulation. 1999;100(6):642–647. doi:10.1161/01.CIR.100.6.642
39. Stolz E, Gerriets T, Kluge A, Klövekorn WP, Kaps M, Bachmann G. Diffusion-weighted magnetic resonance imaging and neurobiochemical markers after aortic valve replacement: implications for future neuroprotective trials? Stroke. 2004;35(4):888–892. doi:10.1161/01.STR.0000120306.82787.5A
40. Al-Attar N, Johnston S, Jamous N, et al. Impact of bleeding complications on length of stay and critical care utilization in cardiac surgery patients in England. J Cardiothorac Surg. 2019;14(1). doi:10.1186/S13019-019-0881-3
41. Murphy GJ, Pike K, Rogers CA, et al. Liberal or restrictive transfusion after cardiac surgery. N Engl J Med. 2015;372(11):997–1008. doi:10.1056/NEJMOA1403612
42. Arabkhani B, Mookhoek A, Di Centa I, et al. Reported outcome after valve-sparing aortic root replacement for aortic root aneurysm: a systematic review and meta-analysis. Ann Thorac Surg. 2015;100(3):1126–1131. doi:10.1016/J.ATHORACSUR.2015.05.093
43. Shrestha ML, Beckmann E, Abd Alhadi F, et al. Elective David I procedure has excellent long-term results: 20-year single-center experience. Ann Thorac Surg. 2018;105(3):731–738. doi:10.1016/J.ATHORACSUR.2017.08.040
44. Segers P, de Jong AP, Kloek JJ, Spanjaard L, de Mol BAJM. Risk control of surgical site infection after cardiothoracic surgery. J Hosp Infect. 2006;62(4):437–445. doi:10.1016/J.JHIN.2005.09.028
45. Nowicki ER, Birkmeyer NJO, Weintraub RW, et al. Multivariable prediction of in-hospital mortality associated with aortic and mitral valve surgery in Northern New England. Ann Thorac Surg. 2004;77(6):1966–1977. doi:10.1016/j.athoracsur.2003.12.035
46. Duchnowski P, Hryniewiecki T, Kuśmierczyk M, Szymanski P. Performance of the EuroSCORE II and the society of thoracic surgeons score in patients undergoing aortic valve replacement for aortic stenosis. J Thorac Dis. 2019;11(5):2076–2081. doi:10.21037/jtd.2019.04.48
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.