Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 16
Validation of the Summit Lab Score in Predicting Exacerbations of Chronic Obstructive Pulmonary Disease Among Individuals with High Arterial Stiffness
Authors Horne BD ![]() , Ali R, Midwinter D
, Ali R, Midwinter D ![]() , Scott-Wilson C
, Scott-Wilson C ![]() , Crim C
, Crim C ![]() , Miller BE
, Miller BE ![]() , Rubin DB
, Rubin DB
Received 5 September 2020
Accepted for publication 11 December 2020
Published 7 January 2021 Volume 2021:16 Pages 41—51
DOI https://doi.org/10.2147/COPD.S279645
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Richard Russell
Benjamin D Horne,1,2 Rehan Ali,3 Dawn Midwinter,3 Catherine Scott-Wilson,4 Courtney Crim,4 Bruce E Miller,5 David B Rubin4
1Intermountain Medical Center Heart Institute, Salt Lake City, UT, USA; 2Division of Cardiovascular Medicine, Department of Medicine, Stanford University, Stanford, CA, USA; 3GlaxoSmithKline Plc., Uxbridge, UK; 4GlaxoSmithKline Plc., Research Triangle Park, Raleigh, NC, USA; 5GlaxoSmithKline Plc., Collegeville, PA, USA
Correspondence: Benjamin D Horne
Intermountain Medical Center Heart Institute, 5121 S Cottonwood Street, Salt Lake City, UT 84107, USA
Email [email protected]
Introduction: The presence of cardiovascular (CV) risk factors and CV disease in patients with chronic obstructive pulmonary disease (COPD) leads to worse outcomes. A number of tools are currently available to stratify the risk of adverse outcomes in these patients with COPD. This post hoc analysis evaluated the Summit Lab Score for validation as a predictor of the first episode of moderate-to-severe acute exacerbation of chronic obstructive pulmonary disease (AECOPD) and other outcomes, in patients with COPD and high arterial pulse wave velocity (aPWV).
Methods: Data from a multicenter, randomized, placebo-controlled, double-blind study were retrospectively analyzed to evaluate treatment effects of once-daily fluticasone furoate/vilanterol 100/25 μg in patients with COPD and an elevated CV risk (aPWV≥ 11m/s) over 24 weeks. The previously derived Summit Lab Score and, secondarily, the Intermountain Risk Score (IMRS) were computed for each patient, with patients then stratified into tertiles for each score. Risk of moderate-to-severe AECOPD was analyzed across tertiles using Kaplan–Meier survival curve and Cox regression analyses.
Results: In 430 patients with COPD, Kaplan–Meier probabilities of no moderate-to-severe AECOPD for Summit Lab Score tertiles 1, 2, and 3 were 92.3%, 95.5%, and 85.1%, respectively (P trend = 0.015), over 24 weeks. Grouped by IMRS tertiles, the respective probabilities were 92.9%, 91.2%, and 88.3%, respectively (P trend = 0.141). Length of stay in the hospital (P = 0.034) and the hospital ward (P = 0.042) were also significantly different between Summit Lab Score tertiles but not for intensive care (P = 0.191).
Conclusion: The Summit Lab Score was associated with the 24-week risk of moderate-to-severe AECOPD in COPD patients with elevated CV risk. Secondarily, IMRS showed a trend towards differences in the risk of AECOPD, which was not statistically significant.
Keywords: chronic obstructive pulmonary disease (COPD), risk assessment, cardiovascular (CV) risk, arterial stiffness, Summit Lab Score, Intermountain Risk Score (IMRS)
Plain Language Summary
Patients with chronic obstructive pulmonary disease (COPD) experience relatively poor health outcomes when they have cardiovascular (CV) risk factors or CV disease. A handful of COPD risk stratification tools are available to identify who is at risk of these poor outcomes, but the Summit Lab Score is a new tool that may provide improved ability to appropriately determine which patients are and are not at risk. We performed a post hoc analysis of data from subjects enrolled in a multicenter randomized clinical trial in order to evaluate the Summit Lab Score for validation as a predictor of the first episode of moderate-to-severe acute exacerbation of COPD (AECOPD) and other outcomes. Patients with COPD and high arterial pulse wave velocity (aPWV) were randomized in the original trial to once-daily placebo, vilanterol 25 μg, or a combination of furoate/vilanterol 100/25 μg and were followed for 24 weeks for the occurrence of AECOPD. The Summit Lab Score was previously developed in another population of >1,000 patients with COPD. In the present study, the Summit Lab Score was associated with the 24-week risk of moderate-to-severe AECOPD in 430 COPD patients with elevated CV risk. It also predicted length of hospital stay.
Introduction
Chronic obstructive pulmonary disease (COPD) is closely associated with cardiovascular disease (CVD), including atherosclerotic cardiovascular disease and heart failure.1–4 In patients with COPD, the presence of cardiovascular (CV) risk factors and CVD leads to increased mortality and adverse respiratory outcomes (including acute exacerbations of COPD [AECOPD]), compared with patients without CV or CVD risk factors.1,2,5–8
A number of tools are currently available to stratify the risk of adverse outcomes in patients with COPD. These include the Global Initiative for Chronic Obstructive Lung Disease (GOLD) A-B-C-D classification;2 the Dyspnea, Obstruction, Smoking, Exacerbation (DOSE) index;9 the Body-mass index, airflow Obstruction, Dyspnea, and Exercise capacity (BODE) index;10 the score to predict short-term risk of COPD exacerbations (SCOPEX);11 and the pulmonary-specific Intermountain Risk Score (IMRS).12
IMRS is a practical prediction tool that uses complete blood count and basic metabolic profile parameters to predict all-cause mortality in hospitalized patients.13 A pulmonary-specific version that integrates spirometric measurements into IMRS has also been validated for use in patients with less severe COPD (sensitivity: 93–99%, specificity: 76–80%).12,13
A new risk stratification tool, the Summit Score, has been developed using data derived from the Study to Understand Mortality and MorbidITy in COPD (SUMMIT) trial, which included patients with COPD and moderate airflow limitation, and has been externally validated in three cohorts of patients from Intermountain Healthcare clinics or hospitals.14 Validated to predict all-cause mortality and AECOPD in patients with moderate COPD, the Summit Score incorporates body mass index (BMI); number of smoking pack-years; number of prior hospitalizations for AECOPD; forced expiratory volume in 1 second (FEV1); heart rate; systolic blood pressure; prior myocardial infarction; prior diagnosis of heart failure; existing diagnosis of diabetes mellitus; age; and reported use of anti-thrombotic agents, anti-arrhythmic medications, and xanthines. The Summit Score has a sensitivity of 40–52% and a specificity of 77–86%, depending on the study population evaluated.14 Integration of mean corpuscular volume (MCV) and red cell distribution width (RDW) to the Summit Score provides a second score, the Summit Lab Score. This proved similarly successful in predicting outcomes.14
While the tools described have been validated in multiple clinical scenarios, it remains unclear whether generalized risk tools (eg, IMRS) or specific tools (eg, Summit Score) can optimally predict adverse outcomes among patients with moderate COPD and high arterial stiffness, as indicated by elevated aortic pulse wave velocity (aPWV): an indicator of greater CV risk. A multicenter, randomized, placebo-controlled, double-blind, parallel-group study (GlaxoSmithKline plc. study HZC113108; ClinicalTrials.gov ID NCT01336608) conducted from March 2011 to November 2014 evaluated the effect of 24 weeks’ treatment with once-daily fluticasone furoate/vilanterol (FF/VI) 100/25 μg in patients with moderate COPD and elevated CV risk, indicated by high arterial stiffness (defined as an aPWV of ≥11 m/s).15 This study provided a suitable data set independent of the SUMMIT trial for validation of risk stratification tools. Using this data set our present analysis evaluated the Summit Lab Score and, secondarily, IMRS as predictors of the first episode of moderate-to-severe AECOPD and other outcomes in patients with moderate COPD and high arterial stiffness.
Methods
This analysis hypothesized that a risk score based in part on common laboratory tests can predict meaningful outcomes, such as AECOPD and CV events, at 24 weeks. The secondary hypothesis was that the Summit Lab Score is more sensitive than IMRS in predicting these outcomes because the former was specifically developed for COPD outpatients; whereas, IMRS was developed for hospitalized patients. The design and results of the primary trial (HZC113108) (clinicaltrials.gov: NCT01336608) were previously described.15 The trial was approved by applicable institutional review boards/independent ethics committees at the 61 participating centers in Germany, Norway, the Philippines, the Republic of Korea, Thailand, and the USA (the list of sites and site investigators is included as Supplemental Table S1).15 All patients provided written informed consent prior to study participation and this trial was conducted in accordance with the Declaration of Helsinki. This retrospective, post hoc analysis of study HZC113108 comprised a separate, independent population from that of the SUMMIT Trial that had a distinct 6-month protocol of treatment and outcomes.14
The study included patients aged ≥40 years with a history of COPD, current/prior smoking history of ≥10 pack-years, a post-albuterol FEV1 ≤70% of the predicted normal value, a FEV1/forced vital capacity (FVC) ratio ≤0.70, and an aPWV ≥11 m/s. The aPWV of patients was assessed using the SphygmoCor CPVH system (AtCor Medical Inc., Illinois, USA). Patients were excluded from participating in study HZC113108 if the underlying cause of COPD was α1-antitrypsin deficiency or if they had: other respiratory disorders including active tuberculosis or lung cancer; current severe heart failure; a recent CV event, such as acute coronary syndrome or stroke, within the previous 24 weeks; clinically significant uncontrolled hypertension; an abnormal or clinically significant 12-lead electrocardiogram finding; or had started, discontinued, and/or were receiving medications (such as anti-hypertensives, lipid-lowering agents, hypoglycemic agents or nitrates) without reaching a stable dose in the last 12 weeks and/or were not anticipated to remain at a stable dose throughout the study period.
Included patients were randomized (1:1:1) to receive FF/VI 100/25 µg, VI 25 µg, or placebo, administered once-daily for 24 weeks via the ELLIPTA inhaler (GlaxoSmithKline plc., Brentford, UK) for 24 weeks, with clinic visits scheduled at treatment weeks 4, 12, 18, and 24. Patients were withdrawn from the study in the event of occurrence of moderate-to-severe AECOPD (ie, worsening of symptoms of COPD that required treatment with systemic or oral corticosteroids, antibiotics, and/or hospitalization); pneumonia (presumptive diagnosis or radiographically confirmed); initiation/discontinuation and/or change in dose of medications reported to impact aPWV; pregnancy; or clinically important changes in laboratory parameters. Other details of the study procedures have been previously published.15
The following data were extracted from patients’ trial records: demographic and anthropomorphic data; smoking status; vital signs; spirometric measurements; history of AECOPD and pneumonia; CV risk factors and past medical history; medications at baseline; complete blood count; basic metabolic profile; and high-sensitivity C-reactive protein results. Spirometry measurements were acquired using spirometry equipment that met or exceeded the minimal performance recommendations of the American Thoracic Society and European Respiratory Society.16 Central laboratory facilities were provided by Quest Diagnostics Clinical Trials (Heston, Middlesex, UK and Valencia, California, USA) for hematology, clinical chemistry, fungal culture, biomarkers, and pregnancy testing. Quest Diagnostics Nichols Institute (San Juan Capistrano, California, USA) and Focus Diagnostics (Cypress, California, USA) provided central laboratory services for liver function tests when stopping criteria were met.
Evaluation of Outcomes
The primary outcome of this post hoc analysis tested for association of the Summit Lab Score with the first episode of moderate-to-severe AECOPD. Secondary outcomes of this analysis included the first CV event (composite of myocardial infarction, unstable angina, stroke, transient ischemic attack, or CV mortality), length of stay in the hospital, hospital ward, or intensive care unit. In study HZC113108, CV events were considered adverse events of special interest, as were adverse events associated with the use of inhaled glucocorticoids or long-acting beta2-agonists.15
Data Analysis
Individual Summit Lab Scores were computed using baseline values using previously derived predictive models (Supplemental Methods). Patients were then grouped into tertiles of the Summit Lab Score (tertile 1 having the lowest scores, representing low risk).14 IMRS was also computed and grouped by tertile.
Descriptive data were summarized as mean ± standard deviation (SD) for continuous variables and compared between Summit Lab Score tertiles using analysis of variance. For FEV1, FVC, and related values, a test of linear contrasts (using coefficients of –1, 0, and 1 for tertiles 1, 2, and 3, respectively) was used for comparisons across tertiles. Categorical variables were presented as frequencies and percentages and compared using the Chi-square test. The Summit Lab Score was compared to IMRS using correlation coefficients for continuous scores and the kappa statistic for scores categorized into tertiles. Kaplan–Meier survival curve and Cox regression analyses were used to determine the hazard ratios (HRs) for first moderate-to-severe AECOPD and CV event between tertiles. The HRs per tertile for each outcome were determined using methods analogous to the Cochran–Armitage test of trend, as were the analyses for trend using the log-rank test with the vector of trend weights of −1, 0, and 1 for tertiles 1, 2, and 3, respectively. Association of the Summit Lab Score tertiles with spirometric findings and lengths of hospital stay were tested by analysis of variance. Area under the curve (AUC) c-statistics from receiver operator characteristic (ROC) curves were evaluated for AECOPD and CV events for continuous values of the Summit Lab Score to examine this combined metric that jointly considers sensitivity and one minus specificity.
All statistical analyses, using two-tailed P values with a 0.05 threshold for statistical significance, were performed using SPSS version 23.0 (IBM SPSS, Inc., Armonk, NY, USA).
Results
In total, 430 patients with COPD and high arterial stiffness were included, with a mean (SD) age of 68.5 (7.9) years (Table 1). The majority of patients were male (79%) and most were either Asian or White (both 48%). Patient distribution by tertile, based on Summit Lab Scores, was 142 patients in tertile 1 (Summit Lab Score: 1–17), 134 in tertile 2 (scores 18–22), and 154 in tertile 3 (scores 23–38). As expected, there were statistically significant differences between tertiles for several Summit Lab Score variables (Table 1), including heart rate (73.4 bpm, 77.4 bpm, and 81.1 bpm in tertiles 1, 2, and 3, respectively), age, BMI, pack-year history of smoking, length of hospital stay, FEV1, MCV, and RDW. The Summit Lab Score marginally correlated with IMRS (females, n=89: r=0.269; males, n=339: r=0.279 [data to calculate IMRS were not available for 2 males]), and agreement was low but significant (κ=0.095, p=0.005).
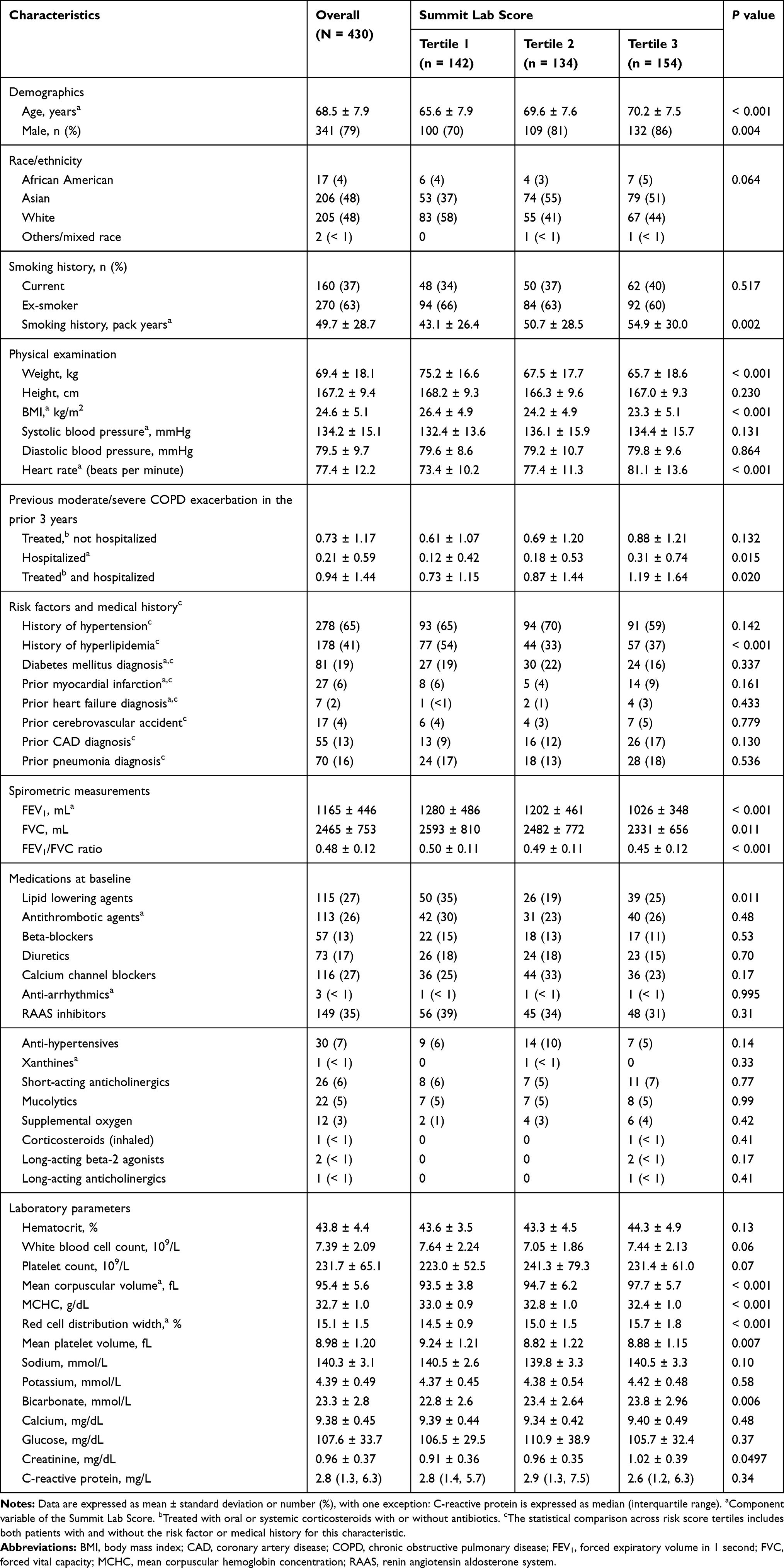 |
Table 1 Baseline Characteristics of the Study Population (N = 430), Overall and Stratified by Textiles of the Summit Lab Score |
At 24 weeks, 40 (9%) subjects experienced the primary outcome of a first episode of moderate-to-severe AECOPD during the study (which resulted in a ROC AUC of c=0.605). Eleven patients in tertile 1, 6 in tertile 2, and 23 in tertile 3 corresponded to percentages of no moderate-to-severe AECOPD (92%, 96%, and 85%, respectively [P trend = 0.015]), over 24 weeks (Figure 1). The HR by Cox regression was 1.62 per tertile (95% confidence interval [CI], 1.09–2.42). The likelihood of moderate-to-severe AECOPD for tertile 3 was significantly different from tertile 1 (HR 2.19; 95% CI: 1.07, 4.49; P = 0.033) but was even more significantly different for tertile 3 compared to tertile 2 (P = 0.003), thus compared with tertiles 1 and 2 combined, tertile 3 had an HR of 2.77 (95% CI: 1.48, 5.19; P = 0.001). Interestingly, only 12 of the 40 AECOPD cases had one or more prior hospitalized AECOPD (the AECOPD history variable in the Summit Lab Score), with just 9 of these 12 included in the 23 cases categorized in the third tertile of the Summit Lab Score.
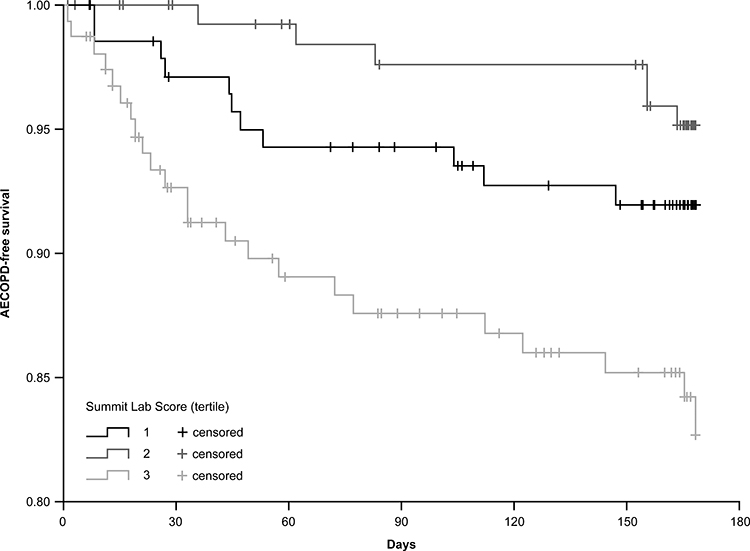 |
Figure 1 Kaplan–Meier survival curves for moderate-to-severe AECOPD by Summit Lab Score tertile. Abbreviation: AECOPD, acute exacerbation of chronic obstructive pulmonary disease. |
Twenty-three (5%) patients experienced the secondary outcome of a first CV event during the study (AUC was c=0.547). Eight patients in tertile 1, four in tertile 2, and 11 in tertile 3, corresponded to survival probabilities with no CV events of 94%, 97%, and 93%, respectively (P trend = 0.41), over 24 weeks (Figure 2). The HR by Cox regression was 1.24 per tertile (95% CI: 0.75, 2.05).
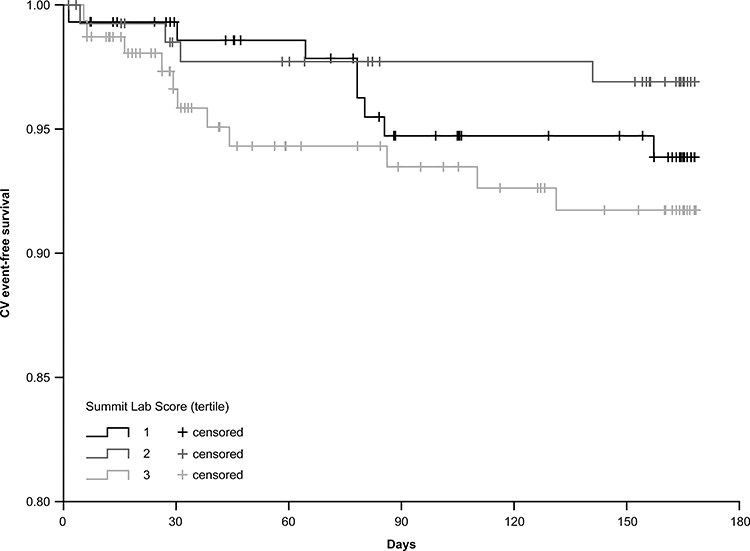 |
Figure 2 Kaplan–Meier survival curves for CV event by Summit Lab Score tertile. CV event includes any of the following: myocardial infarction, unstable angina, stroke, transient ischemic attack, or CV mortality. Abbreviation: CV, cardiovascular. |
Table 2 shows baseline and follow-up spirometric measurements for FEV1, FVC, and FEV1/FVC ratio stratified by the Summit Lab Score. While the values of these measures differed significantly between the tertiles, there were no statistically significant differences between the tertiles for the changes in FEV1, FVC, and FEV1/FVC ratio at 12 and 24 weeks versus baseline, except the change in FEV1 at 12 weeks (P = 0.007). A statistically significant difference was also seen between Summit Lab Score tertiles for lengths of stay in: hospital (P = 0.034), and a hospital ward (P = 0.042) (Figure 3), but not intensive care (P = 0.191).
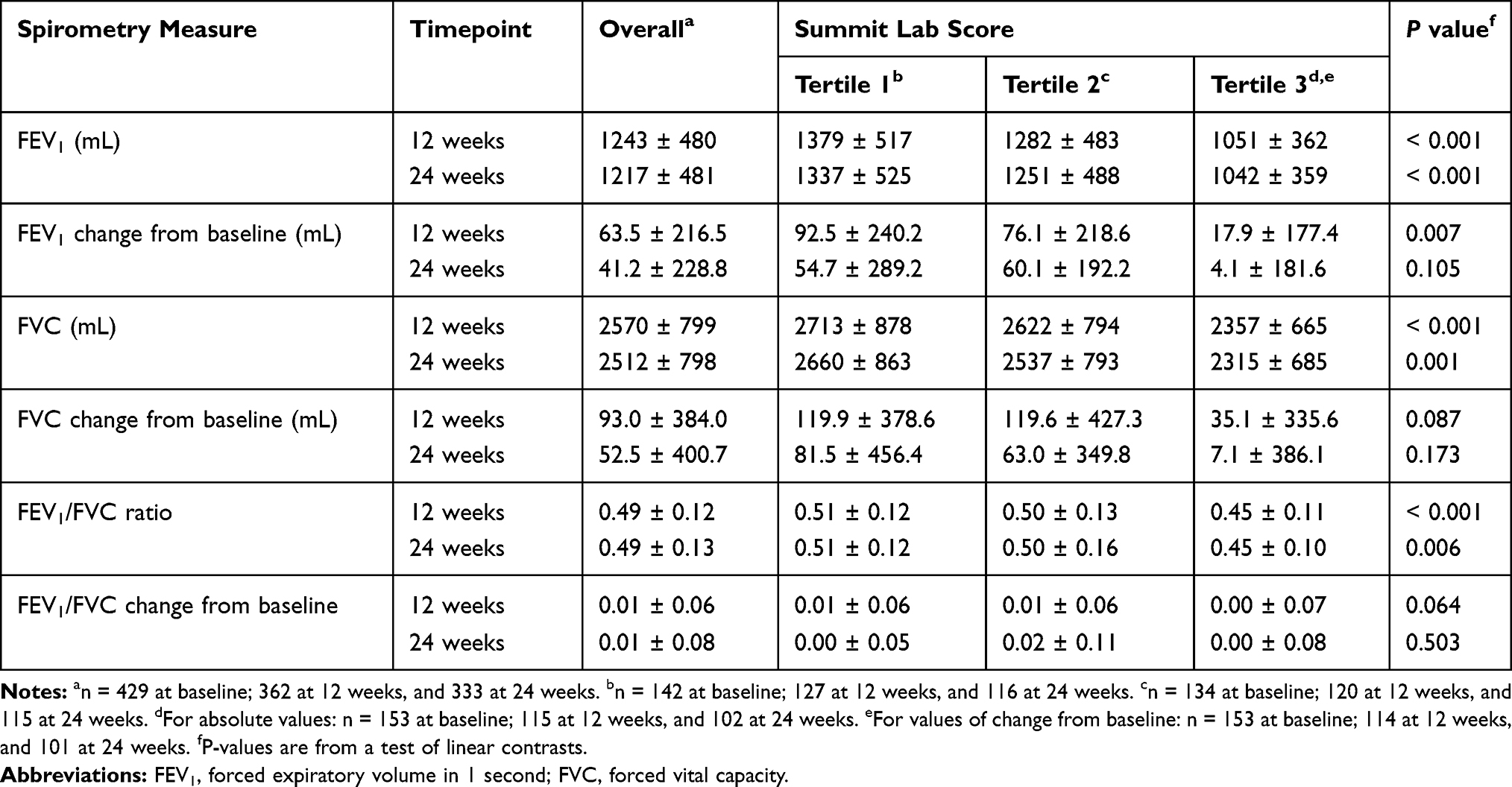 |
Table 2 Analysis of Spirometry Measures by Summit Lab Score Tertile |
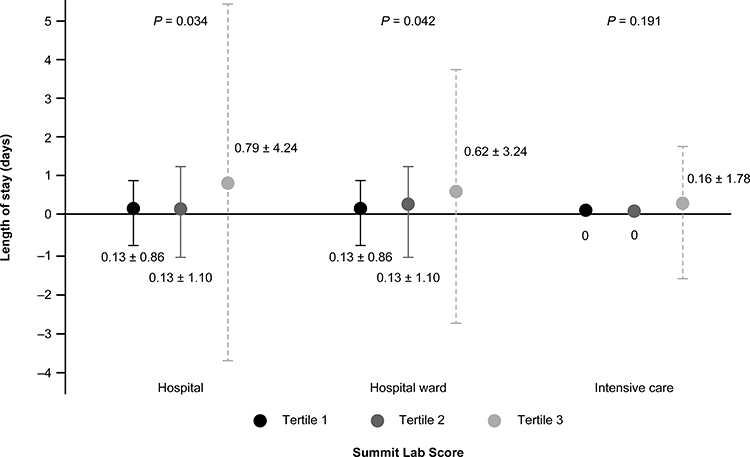 |
Figure 3 Length of stay (y-axis) in the hospital, hospital ward, or intensive care by Summit Lab Score tertile. P values are from tests of linear contrasts with coefficients of –1, 0 and 1. Error bars are the mean ± standard deviation, with the relevant mean and standard deviation provided on the graph near each tertile’s line. |
Two patients died during the study – both were included in the third tertile for Summit Lab Score (survival rate of 99% vs 100% for tertiles 1 and 2), but due to the very small number of events this is primarily descriptive and requires prospective validation. Grouped by IMRS tertiles, the respective probabilities of the primary outcome were 92.9%, 91.2%, and 88.3%, respectively (P trend = 0.141). Further outcomes by IMRS tertile are summarized in the Supplemental Results (Supplemental Figures S1 and S2).
Discussion
Our findings suggest that commonly available laboratory tests and comorbid conditions, alongside measures of respiratory health, can be used to predict clinically significant outcomes in patients with moderate-to-severe COPD and high aPWV over 24 weeks of observation. Prior application of IMRS indicated that clinically significant predictions can be made over a year or more in patients assessed during hospitalization.13 Specifically, our results indicate that by 24 weeks, the Summit Lab Score predicts AECOPD and length of hospitalized stay in COPD outpatients with increased CV risk due to high arterial stiffness.
Several risk-stratifying tools for adverse outcomes in patients with COPD exist, including GOLD A-B-C-D classification,2 the DOSE index,9 BODE,10 and SCOPEX.11 However, these may have limitations. For instance, inconsistent mortality risk stratification for GOLD A-B-C-D,17 weak prediction of AECOPD risk for DOSE,18 and a need for further validation in longitudinal cohort studies and randomized controlled trials for SCOPEX.11 Furthermore, risk scoring systems designed for the general population with COPD may not be appropriate in patients with high CV risk, considering that CV risk factors and CVD are associated with comparatively poorer respiratory and CV outcomes.1,2,6–8,19
In this post hoc analysis, the Summit Lab Score was evaluated in a cohort of COPD patients with moderate COPD and an elevated CV risk on the basis of high arterial stiffness, an independent predictor of coronary heart disease and stroke.20 The Summit Lab Score and IMRS were developed to predict mortality, although the former was developed in a cohort of patients with moderate-severity COPD; whereas, IMRS was developed in a cohort of hospitalized patients with broad ranging diagnoses. The validation study of the Summit Lab Score also evaluated non-fatal outcomes, including first episodes of AECOPD and CV events, for which the Summit Lab Score was found to be predictive.14 The present analysis further supports the validity of the Summit Lab Score in predicting these outcomes in patients with COPD and elevated CV risk. Patients with COPD have an increased risk of mortality associated with accelerated heart rate,21,22 which could be a feature of patients with high CV risk (as demonstrated in a meta-analysis by Zhang et al in 2016).23 In this study, resting heart rates varied in the groups analyzed and, although not considered here, an investigation of different heart rates in predicting AECOPD risk could be of interest in future studies.
A meta-analysis involving 194,035 participants of randomized controlled trials in CVD found that the provision of CVD risk scores increases the prescription of new or intensified lipid-lowering medications (15.7% vs 10.7%; relative risk [RR] 1.47, 95% CI: 1.15, 1.87; I2=40%) and new or intensified antihypertensive medications (17.2% vs 11.4%; RR 1.51, 95% CI: 1.08, 2.11; I2=53%).24 In addition, CVD risk scoring was associated with reduced total cholesterol (mean difference [MD] −0.10 mmol/L; 95% CI: −0.20, 0.00; I2=94%), systolic blood pressure (MD −2.77 mmHg; 95% CI: −4.16, −1.38; I2=93%) and multivariable CVD risk (standardized MD −0.21, 95% CI: −0.39, −0.02; I2=94%).24 The Summit Lab Score has the potential to improve treatment decision-making and outcomes in patients with COPD in a similar way.
While prognostic use of risk scores in COPD exists,2,9,11 the Summit Lab Score utilizes a broader set of parameters that, beyond COPD, quantify risks from a more patient-centered rather than disease-centered perspective. The CVD-associated characteristics are likely this score’s primary value-added aspect given that most COPD patients die due to CV comorbidities such as heart failure. Indeed, NT-proBNP, a powerful prognostic laboratory parameter for CV disease outcomes, is also associated with prognosis in patients with AECOPD.25 Considering CVD and other risk predictors, especially laboratory-based parameters, offer an avenue for future research in COPD patient outcomes.
Our findings also demonstrate the feasibility of evaluating clinical trials in AECOPD over the shorter term (24 weeks) compared with the conventional year-long evaluation. Short-term analyses could be possible through enrichment of high-risk patients in a COPD study population. Similar expedient analyses can therefore be recommended in other studies involving patients with severe disease.
The association of the Summit Lab Score tertiles with length of stay in hospital and the hospital ward are novel findings that warrant further investigation. Other studies have highlighted various factors that are associated with the length of hospital stay in COPD. Indicators of severe disease, such as GOLD class IV and mechanical ventilation, were associated with increased risk of prolonged hospitalization (odds ratios: 1.77 and 2.15, respectively).26 Other implicated predictors include admission between Thursday and Saturday, heart failure, diabetes, stroke, high arterial carbon dioxide partial pressure, and low serum albumin level; all were associated with hospitalization for more than 11 days.27
Our IMRS results provide further context, supporting the hypothesis that the Summit Lab Score is better attuned to predicting outcomes in this COPD population, compared with IMRS. This was not unexpected given that IMRS was derived in a general hospitalized healthcare population; whereas, the Summit Lab Score was derived from a population of non-hospitalized COPD patients with moderate airflow limitation and high arterial stiffness.
Certain limitations, associated with the retrospective use of data from the primary study of Bhatt and colleagues, should be noted however.15 First, this was a post hoc analysis of data, and hence the study was not designed with this analysis in mind. This may be evident in the occurrence of CV events (only 5.3% of patients). Therefore, this study did not replicate the statistically significant findings on CV events seen in the initial Summit Score Study.14 A relatively short follow-up period and relatively small sample size of 430 subjects also contributed to the low number of events; extension of the follow-up period was not possible for this retrospective analysis. Furthermore, the association of the Summit Lab Score tertiles to the length of hospital stay was a novel finding that requires additional validation. Other measures of healthcare utilization could also be explored. Finally, subjects had moderate COPD with high arterial stiffness; thus, these findings generalize to that population and may not apply to patients with other severities of COPD or CVD.
Given the relative risk of new AECOPD for the Summit Lab Score third tertile (HRs ≈ 2.1–2.7), further validations in larger populations are needed. Other applications of the Summit Lab Score should be evaluated in the future. For example, serial Summit Lab Scores over time may be evaluated as a potential indicator of treatment failure or success or even concurrently to predict long-term clinical outcomes. Furthermore, it may be evaluated for use in the research setting to enrich study populations of specific risk groups, such as those with high risk for event-driven trials or those with low risk to identify individuals least likely to prematurely exit trials.
Conclusions
In a relatively small trial, the Summit Lab Score was associated with the 24-week risk of moderate-to-severe AECOPD and the length of stay in the hospital and hospital ward, thus validating the Summit Lab Score as a risk stratification tool for COPD patients with elevated CV risk. IMRS showed a non-statistically significant trend towards predicting differences in the risk of AECOPD. These findings do not provide a basis for treating individual patients based on the Summit Lab Score but suggest the need for further study of the risk prediction tool to determine where and how it may be useful and feasible for improving the personalization of care for patients with COPD.
Additional Information
Trademarks are owned by or licensed to the GlaxoSmithKline group of companies.
Trial Registration
Study HZC113108 is registered on ClinicalTrials.gov as NCT01336608.
Abbreviations
AECOPD, acute exacerbation of chronic obstructive pulmonary disease; aPWV, arterial pulse wave velocity; AUC, area under the curve; BMI, body mass index; BODE, Body-mass index, airflow Obstruction, Dyspnea, and Exercise capacity; COPD, chronic obstructive pulmonary disease; CV, cardiovascular; CVD, cardiovascular disease; DOSE, Dyspnea, Obstruction, Smoking, Exacerbation; FEV1, forced expiratory volume in 1 second; FF, fluticasone furoate; FVC, forced vital capacity; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HR, hazard ratio; IMRS, Intermountain mortality risk score; MCV, mean corpuscular volume; MD, mean difference; RDW, red cell distribution width; ROC, receiver-operator characteristic; SCOPEX, score to predict short-term risk of COPD exacerbations; SD, standard deviation; SUMMIT, the Study to Understand Mortality and MorbidITy in COPD; VI, vilanterol.
Data Sharing Statement
Information on GlaxoSmithKline plc’s data sharing commitments and requesting access to anonymized individual participant data and associated documents can be found at www.clinicalstudydatarequest.com.
Acknowledgments
The authors would like to acknowledge Sally Lettis for her contributions to statistical analysis and interpretation of results, and Jie Wang-Jairaj, who was the clinical investigational lead on the HZC113108 study. Medical writing support (in the form of writing assistance, collating author comments, assembling tables/figures, grammatical editing, fact checking and referencing), was provided by Ivan Olegario, MD, of MIMS Pte. Ltd. (Singapore) and Joanna Wilson, PhD, of Gardiner–Caldwell Communications (Macclesfield, UK), and was funded by GlaxoSmithKline plc. in accordance with Good Publication Practice (GPP3) guidelines.
Funding
Study HZC113108 was funded by GlaxoSmithKline plc. This secondary analysis of study HZC113108 was funded by an in-kind grant from GlaxoSmithKline plc. The funding source had no role in the design of the study, the data analysis, the interpretation of the findings, or publication of the study manuscript.
Disclosure
B.D.H. is an inventor of clinical decision tools that are licensed to CareCentra and Alluceo, is the principal investigator of grants funded by Intermountain Healthcare’s Foundry innovation program, the Intermountain Research and Medical Foundation, CareCentra, Sysmex, GlaxoSmithKline plc., and AstraZeneca, and is a co-investigator for a grant from the Patient-Centered Outcomes Research Institute. R.A., D.M., C.C. and B.E.M. are employees of, and hold restricted/unrestricted shares in, GlaxoSmithKline plc. C.S-W. and D.B.R. hold shares in GlaxoSmithKline plc. Study HZC113108 was sponsored by GlaxoSmithKline plc. The authors report no other conflicts of interest in this work.
References
1. Fabbri LM, Luppi F, Beghé B, Rabe KF. Complex chronic comorbidities of COPD. Eur Respir J. 2008;31(1):204–212. doi:10.1183/09031936.00114307
2. Global Initiative for Chronic Obstructive Lung Disease (GOLD) report. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease; 2020. Available from: https://goldcopd.org/wp-content/uploads/2019/11/GOLD-2020-REPORT-ver1.0wms.pdf.
3. Rutten FH, Moons KG, Cramer MJ, et al. Recognising heart failure in elderly patients with stable chronic obstructive pulmonary disease in primary care: cross sectional diagnostic study. BMJ. 2005;331(7529):1379. doi:10.1136/bmj.38664.661181.55
4. Bhatt SP, Dransfield MT. Chronic obstructive pulmonary disease and cardiovascular disease. Transl Res. 2013;162(4):237–251. doi:10.1016/j.trsl.2013.05.001
5. Hole DJ, Watt GC, Davey-Smith G, Hart CL, Gillis CR, Hawthorne VM. Impaired lung function and mortality risk in men and women: findings from the Renfrew and Paisley prospective population study. BMJ. 1996;313(7059):711–716. doi:10.1136/bmj.313.7059.711
6. Westerik JA, Metting EI, van Boven JF, Tiersma W, Kocks JW, Schermer TR. Associations between chronic comorbidity and exacerbation risk in primary care patients with COPD. Respir Res. 2017;18(1):31. doi:10.1186/s12931-017-0512-2
7. Høiseth AD, Neukamm A, Karlsson BD, Omland T, Brekke PH, Søyseth V. Elevated high-sensitivity cardiac troponin T is associated with increased mortality after acute exacerbation of chronic obstructive pulmonary disease. Thorax. 2011;66(9):775–781. doi:10.1136/thx.2010.153122
8. Houben-Wilke S, Jörres RA, Bals R, et al. Peripheral artery disease and its clinical relevance in patients with chronic obstructive pulmonary disease in the COPD and systemic consequences-comorbidities network study. Am J Respir Crit Care Med. 2017;195(2):189–197. doi:10.1164/rccm.201602-0354OC
9. Jones RC, Donaldson GC, Chavannes NH, et al. Derivation and validation of a composite index of severity in chronic obstructive pulmonary disease: the DOSE Index. Am J Respir Crit Care Med. 2009;180(12):1189–1195. doi:10.1164/rccm.200902-0271OC
10. Celli BR, Cote CG, Marin JM, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med. 2004;350(10):1005–1012. doi:10.1056/NEJMoa021322
11. Make BJ, Eriksson G, Calverley PM, et al. A score to predict short-term risk of COPD exacerbations (SCOPEX). Int J Chron Obstruct Pulmon Dis. 2015;10:201–209. doi:10.2147/COPD.S69589
12. Horne BD, Hegewald M, Muhlestein JB, et al. Pulmonary-specific intermountain risk score predicts all-cause mortality via spirometry, the red cell distribution width, and other laboratory parameters. Respir Care. 2015;60(9):1314–1323. doi:10.4187/respcare.03370
13. Horne BD, May HT, Muhlestein JB, et al. Exceptional mortality prediction by risk scores from common laboratory tests. Am J Med. 2009;122(6):550–558. doi:10.1016/j.amjmed.2008.10.043
14. Horne BD, Hegewald MJ, Crim C, Rea S, Bair TL, Blagev DP. The Summit Score stratifies mortality and morbidity in chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2020;15:1741–1750. doi:10.2147/COPD.S254437
15. Bhatt SP, Dransfield MT, Cockcroft JR, et al. A randomized trial of once-daily fluticasone furoate/vilanterol or vilanterol versus placebo to determine effects on arterial stiffness in COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:351–365. doi:10.2147/COPD.S117373
16. Miller MR, Hankinson J, Brusasco V, et al. Standardisation of spirometry. Eur Respir J. 2005;26(2):319–338. doi:10.1183/09031936.05.00034805
17. Han MZ, Hsiue TR, Tsai SH, Huang TH, Liao XM, Chen CZ. Validation of the GOLD 2017 and new 16 subgroups (1A-4D) classifications in predicting exacerbation and mortality in COPD patients. Int J Chron Obstruct Pulmon Dis. 2018;13:3425–3433. doi:10.2147/COPD.S179048
18. Herer B, Chinet T. Acute exacerbation of COPD during pulmonary rehabilitation: outcomes and risk prediction. Int J Chron Obstruct Pulmon Dis. 2018;13:1767–1774. doi:10.2147/COPD.S163472
19. Kunisaki KM, Dransfield MT, Anderson JA, et al. Exacerbations of chronic obstructive pulmonary disease and cardiac events. A post hoc cohort analysis from the SUMMIT randomized clinical trial. Am J Respir Crit Care Med. 2018;198(1):51–57. doi:10.1164/rccm.201711-2239OC
20. Mattace-Raso FU, van der Cammen TJ, Hofman A, et al. Arterial stiffness and risk of coronary heart disease and stroke: the Rotterdam Study. Circulation. 2006;113(5):657–663. doi:10.1161/CIRCULATIONAHA.105.555235
21. Jensen MT, Marott JL, Lange P, et al. Resting heart rate is a predictor of mortality in COPD. Eur Respir J. 2013;42(2):341–349. doi:10.1183/09031936.00072212
22. Byrd JB, Newby DE, Anderson JA, et al. Blood pressure, heart rate, and mortality in chronic obstructive pulmonary disease: the SUMMIT trial. Eur Heart J. 2018;39(33):3128–3134. doi:10.1093/eurheartj/ehy451
23. Zhang D, Wang W, Li F. Association between resting heart rate and coronary artery disease, stroke, sudden death and noncardiovascular diseases: a meta-analysis. CMAJ. 2016;188(15):E384–E392. doi:10.1503/cmaj.160050
24. Karmali KN, Persell SD, Perel P, Lloyd-Jones DM, Berendsen MA, Huffman MD. Risk scoring for the primary prevention of cardiovascular disease. Cochrane Database Syst Rev. 2017;3:CD006887. doi:10.1002/14651858.CD006887.pub4
25. Spannella F, Giulietti F, Cocci G, et al. Acute exacerbation of chronic obstructive pulmonary disease in oldest adults: predictors of in-hospital mortality and need for post-acute care. J Am Med Dir Assoc. 2019;20:893–898. doi:10.1016/j.jamda.2019.01.125
26. Ruparel M, López-Campos JL, Castro-Acosta A, Hartl S, Pozo-Rodriguez F, Roberts CM. Understanding variation in length of hospital stay for COPD exacerbation: European COPD audit. ERJ Open Res. 2016;2(1):00034–2015. doi:10.1183/23120541.00034-2015
27. Wang Y, Stavem K, Dahl FA, Humerfelt S, Haugen T. Factors associated with a prolonged length of stay after acute exacerbation of chronic obstructive pulmonary disease (AECOPD). Int J Chron Obstruct Pulmon Dis. 2014;9:99–105. doi:10.2147/COPD.S51467
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.