Back to Journals » Patient Preference and Adherence » Volume 17
Validation of the Identification of Medication Adherence Barriers Questionnaire (IMAB-Q); a Behavioural Science-Underpinned Tool for Identifying Non-Adherence and Diagnosing an Individual’s Barriers to Adherence
Authors Bhattacharya D ![]() , Brown TJ, Clark AB, Dima AL
, Brown TJ, Clark AB, Dima AL ![]() , Easthall C, Taylor N, Li Z
, Easthall C, Taylor N, Li Z
Received 17 July 2023
Accepted for publication 7 October 2023
Published 17 November 2023 Volume 2023:17 Pages 2991—3000
DOI https://doi.org/10.2147/PPA.S427207
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Debi Bhattacharya,1 Tracey J Brown,2 Allan B Clark,2 Alexandra L Dima,3 Claire Easthall,4 Natalie Taylor,5 Zhicheng Li6
1School of Healthcare, University of Leicester, Leicester, Leics, UK; 2Norwich Medical School, University of East Anglia, Norwich, Norf, UK; 3Research and Development Unit, Institut deRecerca Sant Joan de Déu, Sant Boi deLlobregat, BCN, Spain; 4School of Healthcare, University of Leeds, Leeds, West Yorks, UK; 5School of Population Health, University of New South Wales, Sydney, NSW, Australia; 6Susan Wakil School of Nursing and Midwifery, The University of Sydney, Sydney, NSW, Australia
Correspondence: Debi Bhattacharya, School of Healthcare, College of Life Sciences, University of Leicester, University Road, Leicester, LE1 7RH, UK, Tel +44116 252 2833, Email [email protected]
Purpose: To validate the Identification of Medication Adherence Barriers Questionnaire (IMAB-Q) as a tool to guide practitioners to identify patients who require support to take their medicines as prescribed, their key barriers to adherence and select relevant behaviour change techniques.
Patients and Methods: Adults prescribed medication for cardiovascular disease prevention were recruited from nine community pharmacies in England. Participants completed the IMAB-Q comprising 30 items representing potential barriers to adherence developed from our previous mixed methods study (scoping review and focus groups) underpinned by the Theoretical Domains Framework. Participants also self-reported their adherence on a visual analogue scale (VAS) ranging from perfect adherence (100) to non-adherence (1). A subgroup of 30 participants completed the IMAB-Q twice to investigate test-retest reliability using weighted Kappa. Mokken scaling was used to investigate IMAB-Q structure. Spearman correlation was used to investigate IMAB-Q criterion validity compared to the VAS score.
Results: From 1407 invitations, 608 valid responses were received. Respondents had a mean (SD) age of 70.12 (9.9) years and were prescribed a median (IQ) 4 (3, 6) medicines. Worry about unwanted effects (n = 212, 34.5%) and negative emotions evoked by medicine taking (n = 99, 16.1%) were most frequently reported. Mokken scaling did not organise related IMAB-Q items according to the TDF domains (scalability coefficient H = 0.3 to 0.6). Lower VAS self-reported adherence correlated with greater IMAB-Q reported barriers (rho = − 0.14, p = 0.001). Test-retest reliability of IMAB-Q items ranged from kappa co-efficient 0.9 to 0.3 (p < 0.05).
Conclusion: The IMAB-Q is valid and reliable for identifying people not adhering and their barriers to adherence. Each IMAB-Q item is linked to a TDF domain which in turn is linked to relevant behaviour change techniques. The IMAB-Q can therefore guide patients and practitioners to select strategies tailored to a patient’s identified barriers.
Keywords: theoretical domains framework, psychometrics, questionnaire, behaviour change, determinant, compliance
Introduction
Lifestyle changes and medication are the primary interventions for chronic disease management. Poor uptake of recommended lifestyle changes such as weight loss and increased physical activity have led to significant research endeavor to develop behaviour change interventions. Applying theory and evidence to develop such interventions is an accepted and widely adopted approach.1 Not adhering to prescribed medication regimens can have a profound negative impact in terms of missed opportunity for health gain, increased mortality and morbidity, and avoidable resource utilisation such as additional investigations and medication wastage.2,3 In contrast to lifestyle related behavioural interventions, there is limited evidence of behaviour change theory and evidence informing health practitioner activity regarding medication adherence support which is still dominated by interventions to address practical barriers such as confusion and difficulty opening packaging.4 There are three main challenges to practitioners effectively supporting patients to adhere; identifying 1) who requires support, 2) what needs to change 3) how change can be achieved. Research consistently indicates that practitioners overestimate adherence of their patients and therefore do not act promptly in discussing with the patient their barriers to adherence. In practice, the medication doses are incrementally increased in order to achieve the desired health benefit without the knowledge that the patient is not adhering.5 Questions that effectively elicit from patients whether they are experiencing challenges to taking their medication as prescribed would support clinicians in early diagnosis of non-adherence and provide information about the cause(s) that need addressing.
Many adherence measures include items measuring the target behavior eg “have you missed any doses during (x period of time)?”.6 Identifying what needs to be addressed to support adherence requires a measure that provides information about the modifiable determinants of a person’s non-adherence rather than simply measuring the target behaviour. The added value of measuring modifiable determinants eg whether a person struggles to open medication packaging, is that they are less susceptible to social desirability and recall bias than measures of the target behaviour eg whether the person takes less medication than prescribed.7 Some adherence measures include a mixture of items measuring the target behaviour and items relating to the modifiable determinants. As the target behaviour and behavioural determinants are conceptually different, they may require different measurement models for testing validity. This may have contributed to the poor fit widely reported by existing adherence measures.6
Medication adherence is a complex behaviour and identifying appropriate adherence interventions should be underpinned by behaviour change theory.8 A measure of the modifiable determinants of medication adherence, with each determinant being linked to an evidence-based behaviour change technique, offers a scalable approach to practitioners delivering evidence-based interventions tailored to individual patient need.
The Theoretical Domains Framework (TDF)9 is a synthesis of several behaviour change theories. It comprises fourteen domains, each representing a mechanism by which modifiable determinants of behaviour may be addressed. Furthermore, each TDF domain (behavioural mechanism) is linked to several behaviour change techniques known to exert their effect via the mechanism.10 The TDF has been used extensively to guide both ascertaining the determinants of a behaviour and then selecting the relevant behaviour change techniques to address those determinants.11,12
A theory and evidence-based conceptual framework of barriers to medication adherence was reported in 2019.13 The framework was developed from a scoping review of barriers to medication adherence followed by focus groups to better understand the literature reported barriers and identify any previously unreported barriers. The programme of work drew on the TDF to organise extracted barriers to adherence and inform the focus group topic guide in order to prompt patients to consider barriers across the full range of TDF domains. The focus groups permitted the literature reported barriers to be explored in sufficient detail that they could be mapped to their relevant TDF domain. They also identified previously underreported barriers to adherence such as negative emotions evoked by medicine taking.13 Barriers were reported across all of the TDF domains except ‘social/professional role and identity’ and ‘behavioural regulation’. The focus group discussions indicated that one’s role in taking medicine was more related to social norms and thus mapped to social influence rather than identity. The absence of barriers mapped to ‘behavioural regulation’ offers some explanation for the marginal effects observed in a meta-analysis of adherence interventions targeting behavioural regulation.14
The present manuscript describes the development and validation of a questionnaire underpinned by the conceptual framework for barriers to medication adherence. As the questionnaire is developed from evidence-based modifiable determinants of medication adherence, linked to the TDF, it may provide a valid and reliable tool to support practitioners in early diagnosis of non-adherence and provide information about the cause(s) that need addressing.
Materials and Methods
A 30-item prototype IMAB-Q was developed by combining adherence barrier statements developed in a previously reported study.13 The Theoretical Domains Framework (TDF)15–17 underpinned development of the IMAB-Q items. This study determines the psychometric properties of the IMAB-Q items. The research team comprised pharmacists, two patient members prescribed multiple medicines, behavioural scientists and statisticians. Ethical approval was granted by NRES Committee East of England, Norfolk, UK (14/EE/1267) for the research which complied with the Declaration of Helsinki. The research was conducted and manuscript reported in accordance with COSMIN and STROBE guidelines respectively.
Participant Identification and Recruitment
The IMAB-Q is intended for use with patients prescribed any medicines for long-term conditions; we focused this validation study on patients prescribed medicines for preventing cardiovascular disease. This was to minimise heterogeneity in the sample to support effective evaluation of IMAB-Q structure.
The research was registered on a national portfolio for studies requiring recruitment sites. The portfolio is held by the National Institute of Health and Social care Research. Nine community pharmacies in one region of England were initiated as recruitment sites from those expressing an interest via the portfolio.
Community pharmacies distributed recruitment and data collection materials to eligible patients. These included the IMAB-Q and a visual analogue scale (VAS) for respondents to self-report their adherence by returning to the pharmacy team. One of the nine community pharmacies additionally collected IMAB-Q test-retest reliability data by inviting participants to complete the IMAB-Q a second time between two and four weeks of first completion. If the participant did not complete the IMAB-Q a second time, data from their first IMAB-Q were still included for analysis.
Patients were eligible if prescribed at least one cardiovascular preventative medicine and aged 18 years or over, able to read English, provided written, informed consent and not prescribed any medication for severe mental illness.
Sample Size
In accordance with recommendations that a sample size of 300 to 500 participants is very good for questionnaire validation,18,19 we aimed to recruit 600 to 700 participants with a view to achieving complete data for 500 participants.
Analysis
Missing Values Analysis
Missing values analysis using Little’s MCAR test was undertaken.20 Missing data were investigated in terms of the proportion missing per item and whether they were missing at random; if appropriate, missing data were imputed using the median value for that item.
Characterizing IMAB-Q Responses
Table 1 provides the IMAB-Q statements and the behavioural domains of the TDF to which the statements were mapped. Each domain has three statements with the intention of identifying which is/are most effective at identifying the intended adherence barrier. Each statement is scored from 1 to 5 with 1 indicating that the respondent did not consider the behavioural domain to be a barrier to adherence whilst 5 indicates that it is perceived to be a strong barrier. Items that are reverse scored are indicated with*.
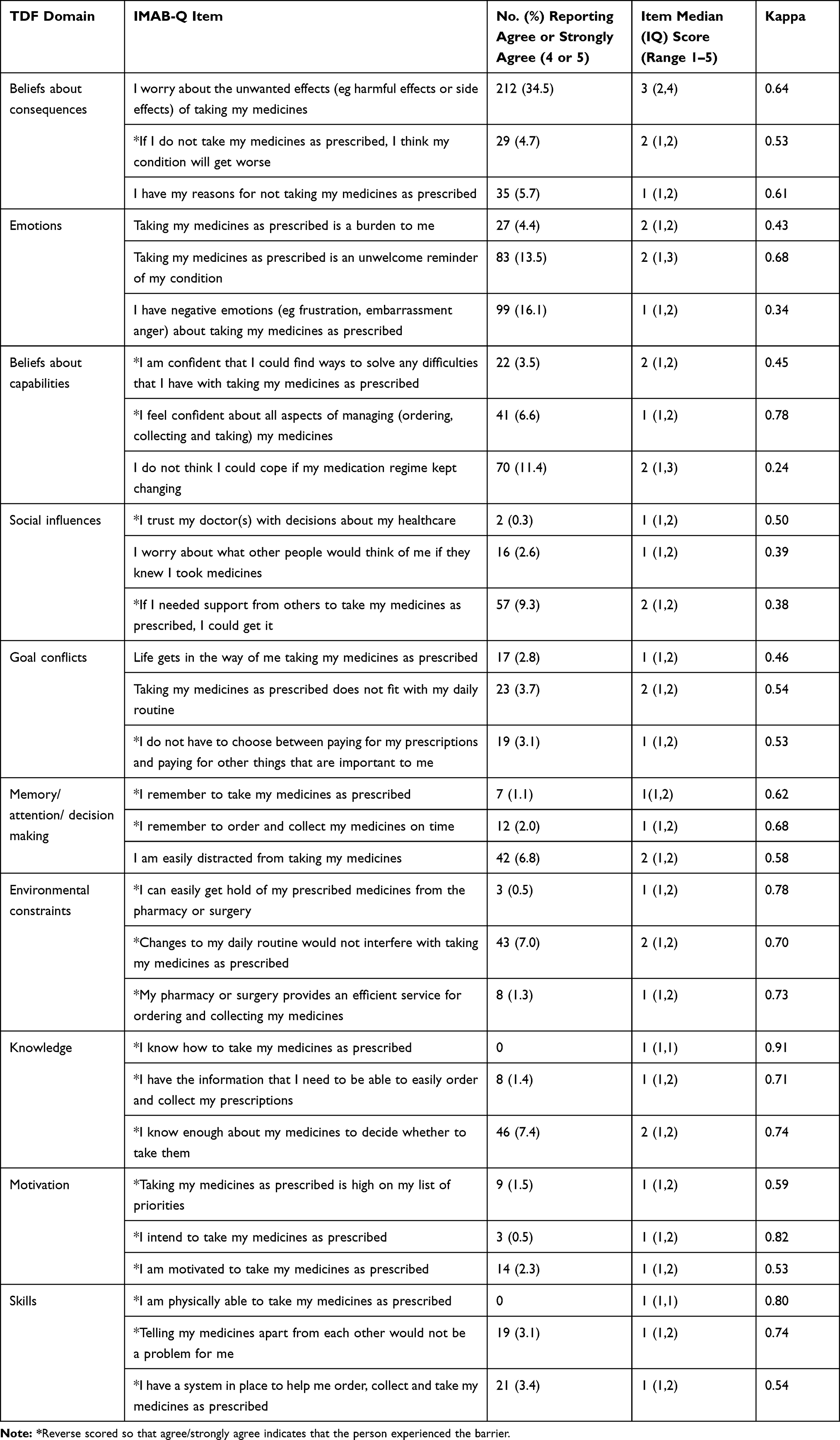 |
Table 1 IMAB-Q Scores (n = 608) and Test-Retest Reliability (n = 30) |
Exploration of the Psychometric Properties of the IMAB-Q
Test-Retest Reliability
Using data from respondents who completed the IMAB-Q twice, weighted Kappa was calculated to indicate whether a participant’s responses to the IMAB-Q were stable over a two-week time interval.
Construct Validity
Confirmatory Factor Analysis (CFA) is a commonly employed method for validating measures through testing the hypothesis that theoretical determinants are latent factors that determine a participant’s response to items related to individual barriers to adherence. This might not represent adequately how individual barriers are inter-related and influence the final behaviour. In contrast, Mokken Scaling is a non-parametric Item Response Theory method that may better represent the relationship between barrier items and the latent trait of barrier to adherence by not assuming that all barriers are equally likely to be experienced. For example, it will not expect a patient to be just as likely to report that they forget to take their medication as reporting that they do not trust their doctor.21 Therefore, we used Mokken scaling to explore the relationships between IMAB-Q item responses. Mokken scaling makes the following three assumptions:
1. That each scale generated from a set of items is unidimensional ie measures a single latent trait that explains some of the barrier to adherence.
Automated item selection procedure in the Mokken R package was used to automatically search for sets of items at incrementally higher thresholds of unidimensionality ranging from Loevinger’s scalability coefficient of H = 0.3 through to H > 0.5. We considered the scale weak if H < 0.3. Any items not grouping into a unidimensional scale were considered for removal.
2. That the association between any two items is only explained by the common barrier that they are intended to measure which is termed local independence.
Yen’s Q3 statistic was used to investigate if correlation between any two items was too great, indicated by Yen’s Q3 >0.2. If local dependence was identified, one of the affected items was removed.22
3. That the higher the value of the latent trait, the more likely the item is to be endorsed as a barrier which is termed monotonicity. Monotonicity is therefore a measure of how well an item discriminates between someone who is strongly experiencing barriers to adherence from someone who has weak barriers to adherence and thus are less likely to prevent adherence.
We generated Item Characteristic Curves to visualise how the items in the scales performed with a steep curve indicating good discriminatory ability of items in the scale.
Criterion Validity
Criterion validity to determine whether the IMAB-Q accurately identifies people who are non-adherent, was investigated using the self-reported visual analogue scale (VAS) ranging from “100” indicating no doses missed in the previous three months to “1” indicating no doses taken. This VAS has been used with a population similar to the present study and correlation observed with electronic medication adherence monitoring.23 However, self-presentation bias was demonstrated with mean VAS adherence being 95% compared with 58% for electronic medication adherence monitoring. A significant inverse relationship will indicate criterion validity as greater barriers reported on the IMAB-Q (indicated by a higher score) should be associated with lower adherence (lower VAS score).
Results
From the 1407 recruitment packs distributed (1348 for the main study and 59 as baseline questionnaires from the test-retest study), 666 (47.33%) completed questionnaires were returned to the research team. For six questionnaires, no valid consent form was received thus 660 (46.9%) were included in the analysis.
The mean (SD) age of respondents was 70.12 (9.9) years and 395 (59.8%) were male. The majority of respondents were exempt from prescription charges with only 22 (3.3%) reporting that they pay for their prescriptions. The median (IQ) number of medicines prescribed per respondent was 4 (3, 6) and the median (IQ) maximum daily frequency of prescribed medicines was 2 (1, 3).
Self-Reported Adherence
A valid response to the VAS was obtained from 621 (94.1%) respondents with a median (IQ) score of 97 (94, 99) indicating that the measure is subject to ceiling effects as the majority of respondents self-reported a high level of adherence.
IMAB-Q Responses
Of the 660 respondents, a valid response to all 30 IMAB-Q statements was obtained from 608 (92.12%). Little’s MCAR test was significant (p < 0.001), indicating that data were not missing completely at random. Two statements were most frequently associated with a missing response: I do not have to choose between paying for my prescriptions and paying for other things that are important to me; was missing on 11 (1.7%) of the responses and I have my reasons for not taking my medicines as prescribed; was missing on 12 (1.8%) responses. However, there were less than 5% of missing data in any one variable thus the problematic data (N = 45 respondents) were removed from further analyses giving a final data set of 615 respondents.
Table 1 provides the descriptive statistics for the statements relating to the 10 TDF domains in ascending order by the percentage of respondents reporting that they “gree” or ‘strongly agree’ with the barriers in the domain. Items that are not phrased as barriers have been reverse scored so in all cases, agree or strongly agree indicate that the respondent experienced the barrier. It can be seen that only two barrier items were not deemed relevant to any respondents as a strong barrier. These were items related to knowledge about how to take the medicine and being physically able to take the medicine. The domains for which respondents were most likely to report a barrier to adherence were “emotions” and “beliefs about consequences”. Worry about unwanted effects was the most frequently reported barrier followed by negative emotions evoked by medicine taking and medicines being an unwelcome reminder of illness.
Test-Retest Reliability
Table 1 provides the test-retest reliability data for the IMAB-Q items that ranged from a weighted kappa co-efficient value of 0.9 (strong agreement) to 0.3 (fair agreement) with p in all cases being <0.05. There are no obvious trends in terms of the items with lower co-efficient values as these are distributed across multiple domains and include both positively and negatively phrased statements.
Construct Validity
Table 2 indicates that four Mokken scales were generated representing 25 items and presents the TDF domains to which each of the items relate. The three items in each of the ten TDF domains did not consistently organise into the same scale. Scale 1 which includes 15 items, comprises most of the items related to knowledge and skills whilst scales 2 and 3 are dominated by items from the domains of emotions and goal conflicts. The 5 items that did not organise into any of the scales were likely due to them having insufficient similarity to any of the other items in the IMAB-Q.
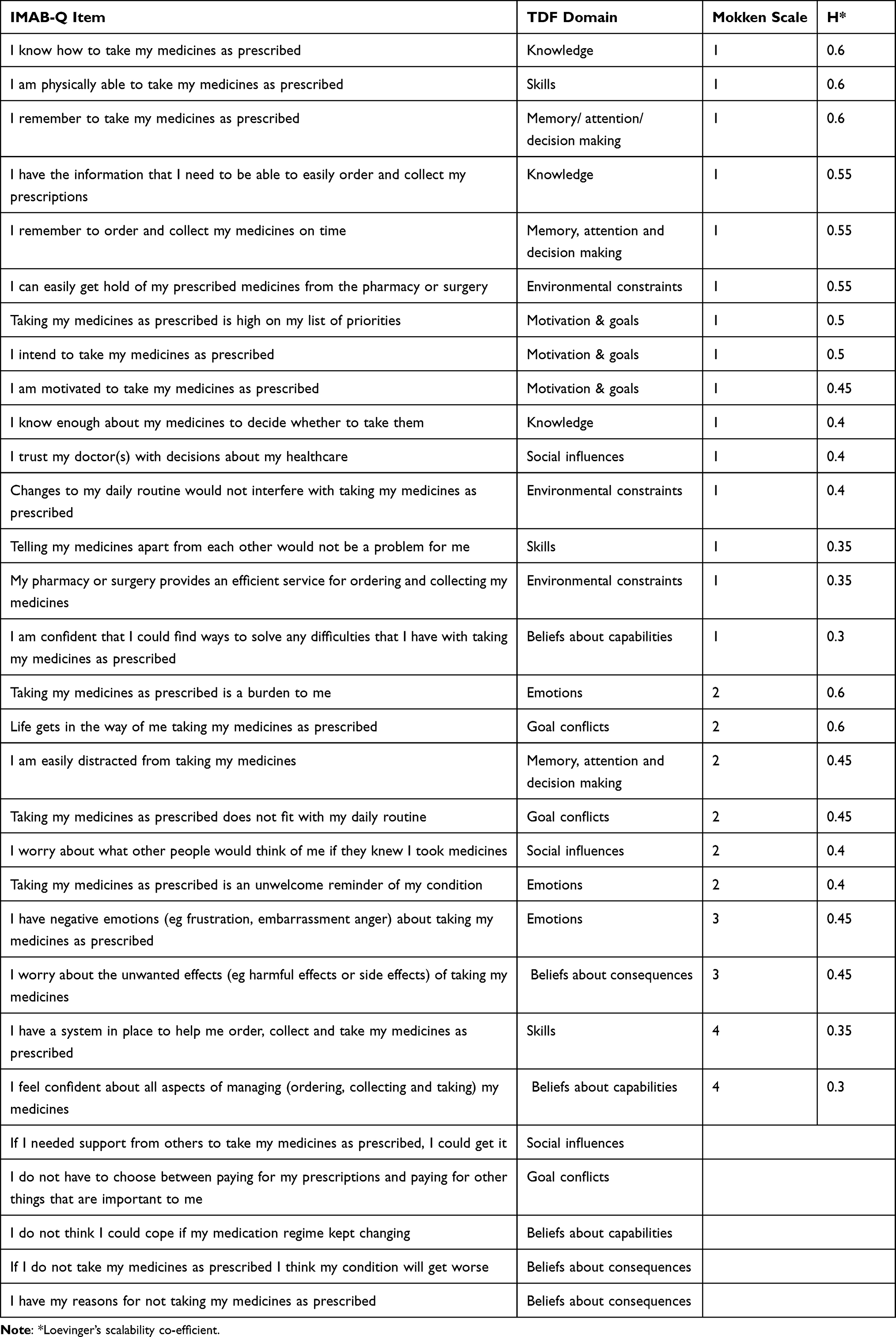 |
Table 2 Scales Generated from Automated Item Selection Procedure |
Monotonicity and independence analyses were restricted to scales 1 and 2 as scales 3 and 4 included only two items thus prohibiting further analysis. The Item Characteristic Curves all demonstrated a sigmoid appearance indicating monotonicity thus as magnitude of non-adherence increases, so does likelihood of reporting adherence barriers. These are presented in Supplementary File 1. The check for local independence retained all items in the scale indicating that this criterion is fulfilled.
Criterion Validity
Participants who reported high medication adherence on the VAS were significantly more likely to report fewer barriers to adherence (rho = −0.14 and 95% CI: −0.22 to −0.06, p = 0.001) Supplementary file 2 provides the graphical representations of the VAS compared with IMAB-Q 30 item.
Discussion
This development and validation study has demonstrated that the IMAB-Q is valid and reliable for diagnosing the modifiable determinants of adherence to medication.
The dominance of concerns regarding medication related unwanted effects presenting a barrier to adherence accords with previous research.24 In contrast, less attention has been given both in the literature and healthcare practice to the negative emotions evoked by the prospect of medicine taking which was also frequently reported on the IMAB-Q. The IMAB-Q therefore offers a structured approach to ensuring that all potentially relevant barriers to adherence are considered both by the patient and practitioner. For example, negative emotions may be addressed by supporting the patient to reframe their perspective on taking their medicines so that they adopt a positive perspective on taking their medicines as prescribed.25
Self-reported non-adherence on the VAS was lower than the frequently cited statistic of 30% to 50% non-adherence.8 This may be indicative of self-presentation bias having a greater impact on responses relative to previous studies due to the questionnaires being returned to the pharmacy team rather than researchers unrelated to the respondent’s healthcare.23 Furthermore, given that just under half of all patients invited to participate did not consent, self-selection bias of the more adherent patients agreeing to participate may have contributed to the limited variation and high ceiling effects observed in self-reported adherence using the VAS.7 The IMAB-Q was less susceptible to these high ceiling effects and limited variation as the full range of barriers were reported and to varying extremes. This accords with the hypothesis that inviting patients to share the challenges that they are experiencing with adherence elicits less self-presentation bias than asking them about the extent to which they are achieving the recommended adherence.7
In terms of IMAB-Q structure, the four Mokken scales generated indicate that associations between IMAB-Q items do not follow the TDF domains as hypothesised. This means that interpreting a total IMAB-Q score is inappropriate. However, the IMAB-Q is not intended to be used in this manner. The utility of the IMAB-Q for diagnosing an individual’s determinants is unaffected. Furthermore, the relevance of using the TDF as the underpinning theory to develop the IMAB-Q items remains, as the TDF domains have been linked to relevant behaviour change techniques. This therefore permits IMAB-Q items to be linked to relevant behaviour change techniques to address the determinant represented by the item.
The missing values analysis suggests that the item relating to payment and item regarding having unspecified reasons for not taking medicines as prescribed were missed more frequently. This increased likelihood of missing the payment item may be due to the older participant population as they are exempt from prescription charges in the UK. Neither the research team nor patient members of the study team were able to generate hypotheses regarding the increased likelihood of missing the item regarding unspecified reasons for non-adherence. Whilst we provide some commentary on the nature of reported barriers, these inferences are specific to the UK population in which the IMAB-Q was tested. Using the IMAB-Q within other healthcare systems will therefore add to the evidence base of barriers to medication adherence. The next steps of intervention development are to link each IMAB-Q item to its corresponding behaviour change techniques. Working with patients and practitioners, these behaviour change techniques can then be fully characterised for applying to the behaviour of medication adherence.
Conclusion
The IMAB-Q is a valid and reliable tool for identifying patients not adhering to their prescribed medicines and their main barriers to adherence that require targeting. Each IMAB-Q item is linked to a TDF domain which in turn is linked to relevant behaviour change techniques. The IMAB-Q can therefore guide patients and practitioners to select strategies tailored to a patient’s identified, prioritised barriers.
Acknowledgments
The IMAB-Q validation study was funded by Pharmacy Research UK grant number: PG14. The IMAB-Q was developed as a component of a doctoral thesis by Claire Anne Marie Easthall entitled ‘The Development and Evaluation of Pharmacy-led Medication Adherence Services’. The thesis has been published on the University of East Anglia website and is available here: https://ueaeprints.uea.ac.uk/id/eprint/72812/1/Thesis_complete_June_%2714.pdf.
The later validation work presented in this manuscript was undertaken as a programme of research funded by Pharmacy Research UK; the full report produced for the funder is available here: https://pharmacyresearchuk.org/wp-content/uploads/2017/01/IMAB-Q-validation-and-feasibility-testing-full-report.pdf.
Disclosure
The authors report no conflicts of interest in this work.
References
1. National Institute for Health and Clinical Excellence. Behaviour change: individual approaches: NICE guideline [PH49]; 2014. Available from: https://www.nice.org.uk/guidance/ph49.
2. National Institute for Health and Clinical Excellence. Medicines Adherence: Involving Patients in Decisions About Prescribed Medicines and Supporting Adherence. NICE guidelines CG76: National Institute for Health and Clinical Excellence; 2009.
3. Simpson SH, Eurich DT, Majumdar SR, et al. A meta-analysis of the association between adherence to drug therapy and mortality. Brit Med J. 2006;333(7557):15–18. doi:10.1136/bmj.38875.675486.55
4. Shenoy R, Scott S, Bhattacharya D. Quantifying and characterising multi-compartment compliance aid provision. Res Social Adm Pharm. 2019;16((4)):560–7.
5. Bhattacharya D, Aldus CF, Barton G, et al.. Do not initiate medication organisation devices without prior detailed medication review and vigilant monitoring. BMJ. 2014:330–293. doi:10.1136/bmj.38338.674583
6. Kwan YH, Weng SD, Loh DHF, et al. Measurement properties of existing patient-reported outcome measures on medication adherence: systematic review. J Med Internet Res. 2020;22(10):e19179. doi:10.2196/19179
7. Stirratt MJ, Dunbar-Jacob J, Crane HM, et al. Self-report measures of medication adherence behavior: recommendations on optimal use. Transl Behav Med. 2015;5(4):470–482. doi:10.1007/s13142-015-0315-2
8. Nieuwlaat R, Wilczynski N, Navarro T, et al. Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2014;11:CD000011.
9. Michie S,Johnston M, Abraham C, Lawton R, et al. Making psychological theory useful for implementing evidence based practice: a consensus approach. Qual Saf Health Care. 2005;14(1):26–33. doi:10.1136/qshc.2004.011155
10. Carey RN, Connell L, Johnston M, et al. Behaviour change techniques and their mechanisms of action: a synthesis of links described in published intervention literature. Ann Behav Med. 2018. doi:10.1093/abm/kay078
11. Dyson J, Lawton R, Jackson C, Cheater F. Does the use of a theoretical approach tell us more about hand hygiene behaviour? The barriers and levers to hand hygiene. J Infect Prev. 2011;12(1):17–24. doi:10.1177/1757177410384300
12. French SD, Green SE, O’Connor DA, et al.. Developing theory-informed behaviour change interventions to implement evidence into practice: a systematic approach using the theoretical domains framework. Implement Sci. 2012;7(1). doi:10.1186/1748-5908-7-38
13. Easthall C, Taylor N, Bhattacharya D. Barriers to medication adherence in patients prescribed medicines for the prevention of cardiovascular disease: a conceptual framework. Int J Pharm Pract. 2018;27(3):223–231. doi:10.1111/ijpp.12491
14. Wilson TE, Hennessy EA, Falzon L, Boyd R, Kronish IM, Birk JL. Effectiveness of interventions targeting self-regulation to improve adherence to chronic disease medications: a meta-review of meta-analyses. Health Psychol Rev. 2020;14(1):66–85. doi:10.1080/17437199.2019.1706615
15. Scott S, Twigg MJ, Clark A, et al. Development of a hospital deprescribing implementation framework: a focus group study with geriatricians and pharmacists. Age Ageing. 2020;49(1):102–110. doi:10.1093/ageing/afz133
16. Hatton K, Bhattacharya D, Scott S, Wright D. Barriers and facilitators to pharmacists integrating into the ward-based multidisciplinary team: a systematic review and meta-synthesis. Res Social Adm Pharm. 2021;17(11):1923–1936. doi:10.1016/j.sapharm.2021.02.006
17. Prajapati AR, Dima A, Mosa G, et al. Mapping modifiable determinants of medication adherence in bipolar disorder (BD) to the theoretical domains framework (TDF): a systematic review. Psychol Med. 2021;51(7):1082–1098. doi:10.1017/S0033291721001446
18. Terwee CB, Mokkink LB, Knol DL, Ostelo RW, Bouter LM, de Vet HC. Rating the methodological quality in systematic reviews of studies on measurement properties: a scoring system for the COSMIN checklist. Qual Life Res. 2012;21(4):651–657. doi:10.1007/s11136-011-9960-1
19. Boateng GO, Neilands TB, Frongillo EA, Melgar-Quiñonez HR, Young SL. Best practices for developing and validating scales for health, social, and behavioral research: a primer. Front Public Health. 2018;6:149. doi:10.3389/fpubh.2018.00149
20. Little RJA. A test of missing completely at random for multivariate data with missing values. J Am Stat Assoc. 1988;83(404):1198–1202. doi:10.1080/01621459.1988.10478722
21. Dima AL, Stutterheim SE, Lyimo R, de Bruin M. Advancing methodology in the study of HIV status disclosure: the importance of considering disclosure target and intent. Soc Sci Med. 2014;108:166–174. doi:10.1016/j.socscimed.2014.02.045
22. Christensen KB, Makransky G, Horton M. Critical values for yen’s q3: identification of local dependence in the rasch model using residual correlations. Appl Psychol Meas. 2017;41(3):178–194. doi:10.1177/0146621616677520
23. Hamilton GA. Measuring adherence in a hypertension clinical trial. Eur J Cardiovasc Nurs. 2003;2(3):219–228. doi:10.1016/S1474-5151(03)00058-6
24. Kvarnstrom K, Westerholm A, Airaksinen M, Liira H. Factors contributing to medication adherence in patients with a chronic condition: a scoping review of qualitative research. Pharmaceutics. 2021;13(7):1100. doi:10.3390/pharmaceutics13071100
25. Johnston M, Carey RN, Connell Bohlen LE, et al. Development of an online tool for linking behavior change techniques and mechanisms of action based on triangulation of findings from literature synthesis and expert consensus. Transl Behav Med. 2020;11(5):1049–1065. doi:10.1093/tbm/ibaa050
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.