")
Back to Journals » International Journal of Women's Health » Volume 15
Vagino-Laparoscopic Conservative Strategy of Hysterectomy in Indicated Cases of Severe Pelvic Endometriosis Followed by 24 Months of Depot-Medroxyprogesterone Acetate Therapy— A Symptom-Solving Treatment Model to Ease Surgical Challenges
Authors Purohit R , Sharma JG, Meher D, Samy MM
Received 21 September 2023
Accepted for publication 22 November 2023
Published 5 December 2023 Volume 2023:15 Pages 1931—1940
DOI https://doi.org/10.2147/IJWH.S437362
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Supplementary video 1 of "Vagino-laparoscopic conservative strategy of hysterectomy" [ID 437362].
Views: 63
Ramkrishna Purohit,1 Jay Gopal Sharma,1 Devajani Meher,1 Mohammed Mahmoud Samy2
1Department of Obstetrics & Gynaecology, Purohit General Hospital, Bargarh, India; 2Department of Obstetrics & Gynaecology, Ainshams University, Cairo, Egypt
Correspondence: Ramkrishna Purohit, Department of Obstetrics & Gynaecology, Purohit General Hospital, Shakti Nagar, Bargarh, Odisha, 768028, India, Tel + 91-6646-234403, 234468 ; +91-94370 54403, Fax +91-6646-231597, Email [email protected]
Purpose: To demonstrate the long-term outcome of a symptom-solving treatment model (SSTM).
Patients and Methods: An observational study was carried out between June 2016 and December 2022 in our private setup on consecutive candidates of hysterectomy for severe pelvic endometriosis. Candidates were treated by the SSTM, which constitutes a systematic vagino-laparoscopic conservative strategy of hysterectomy with preservation of the ovary or ovaries followed by 24 months of postoperative depot-medroxyprogesterone acetate (DMPA) therapy. Cases were followed up to December 2022, 2.5 years beyond the last hysterectomy in May 2020.
Main Outcome Measures: Relief of endometriosis-associated symptoms and prevention of recurrence in the long term.
Results: Symptomatic relief of endometriosis-related pain, such as cyclical dysmenorrhoea, pelvic pain, dyschezia, and vaginal pain, occurred in all 68 (100%) cases from the next expected date of menstruation. None of the cases showed a recurrence of endometriosis-related pelvic pain; overall, 37 (54.41%) cases crossed 4– 6 years, and 31 (45.58%) cases crossed 2.5– 4.0 years following the hysterectomy operation. Four (5.88%) cases had non-endometriotic pelvic pain. None of the cases required repeat surgery or had any major side effects or complications due to DMPA. No major perioperative complications were observed. The results were achieved without the requirement of challenging extensive retroperitoneal laparoscopic dissection, ureterolysis, and rectum surgeries.
Conclusion: This SSTM can be an option in indicated cases of severe pelvic endometriosis to provide symptom relief and prevent the recurrence of endometriosis-associated pelvic pain in the long term.
Keywords: severe pelvic endometriosis, vagino-laparoscopic hysterectomy, relief of endometriosis-associated pelvic pain, recurrence of endometriosis-associated pelvic pain, DMPA therapy following hysterectomy, hysterectomy with ovarian conservation, symptom-solving treatment model
Introduction
Failed remission and recurrence of unbearable endometriosis-associated pelvic pain are a concern for the patient and the operating gynaecologic surgeon in indicated cases of hysterectomy for severe pelvic endometriosis.1–4 Surgeons, through the abdominal route (abdominal and laparoscopic) of the hysterectomy, have adopted different ways—such as en-block excision or extensive retroperitoneal dissection—to remove all deeply infiltrated diseased tissues with the aim of relieving the severe cyclic pelvic pain and preventing its recurrence.1,5–7 These procedures are often surgically and technically challenging in the deeper part of the pelvis during laparoscopic hysterectomy and have an increased risk of intraoperative and postoperative morbidities.6,8–11 The concern further increases when the patient and gynaecologic surgeon decide to conserve one or both ovaries for various known health benefits.1
Patients with endometriosis appreciate long-term symptom relief following definitive hysterectomy. It is well known that the lysis of adhesions relieves pain, and endometriosis responds to depot-medroxyprogesterone acetate (DMPA) therapy.7
Therefore, to ease surgical challenges, relieve painful symptoms and suppress postoperative recurrence in the long term, we developed using previous clinical experiences a symptom-solving treatment model (SSTM) employing a vagino-laparoscopic conservative strategy of hysterectomy in indicated cases of severe pelvic endometriosis followed by 24 months of postoperative DMPA suppression therapy. We demonstrate the outcome of the SSTM in this observational study.
Materials and Methods
An observational study was conducted in our Purohit general hospital from June 2016 up to December 2022. Consecutive candidates indicated for hysterectomy for severe pelvic endometriosis (Stage IV, ASRM) were recruited during the study period (Table 1). The candidates were evaluated by clinical examination, transabdominal and transvaginal ultrasonography, and indicated CT scan, and MRI. The below-described vagino-laparoscopic conservative strategy of hysterectomy with required surgical procedures was performed to treat the disease. The cases with a conserved ovary (one or both) were administered DMPA suppression therapy for 24 months post-surgery and were followed up to December 2022, which was more than 2.5 years after the last hysterectomy operation performed in May 2020. Cases with associated uterus size above 16 weeks of gestation were excluded. Data were analysed using descriptive statistics. The primary outcome of interest was to determine whether the below-described SSTM (planned surgery plus DMPA) relieves the endometriosis-associated symptoms and prevents recurrence in the long term.
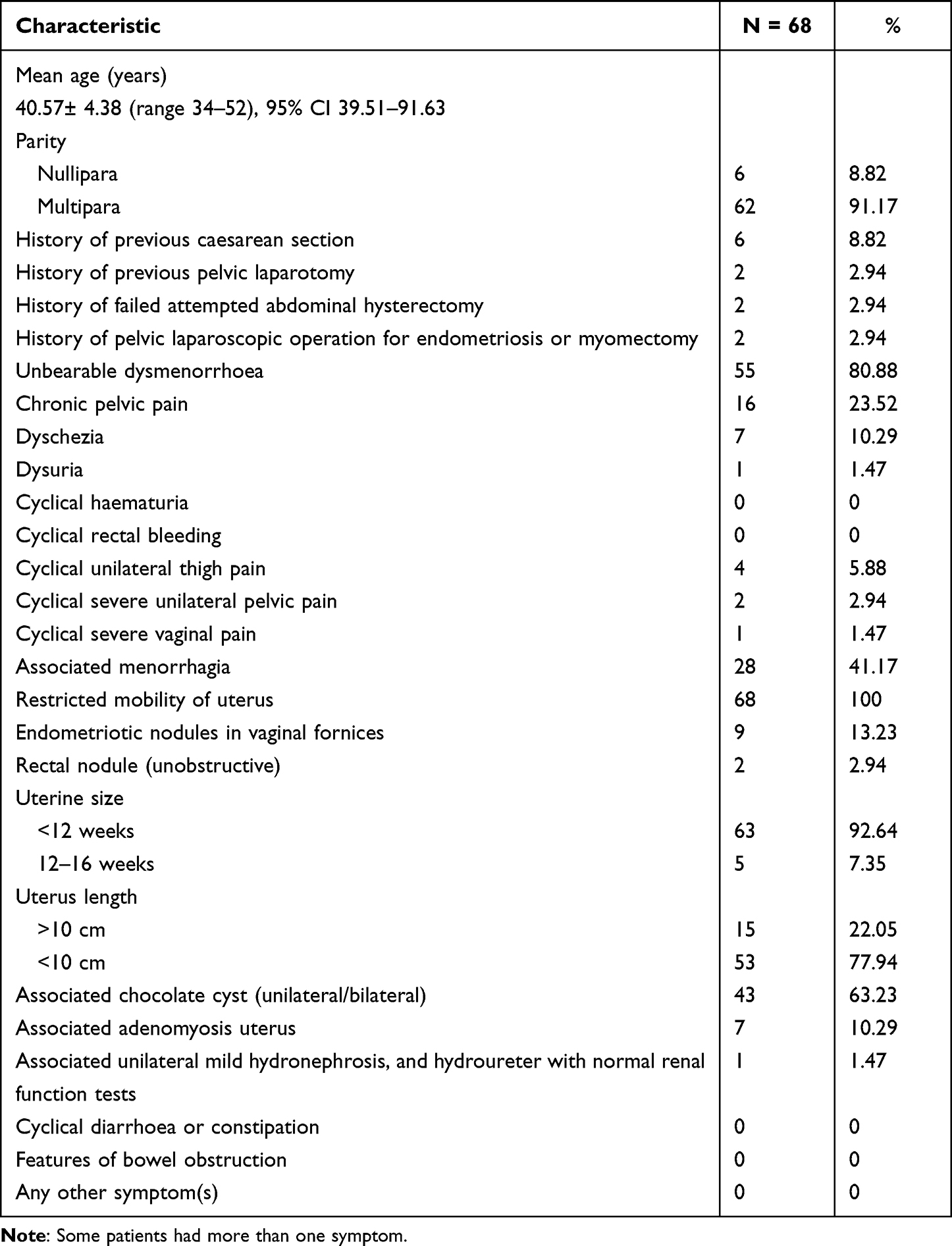 |
Table 1 Preoperative Characteristics of the Patients |
The study was approved by the Purohit General Hospital Institutional Ethics Committee (reference number PGHIE 5/Dt.5th April 2016). Informed consent was signed by each patient from the time of inclusion of the first case in the study. It complies with the declaration of Helsinki.
The SSTM consists of the surgical procedure and the postoperative 24-months DMPA therapy.
Part 1. The surgical procedure, comprising the vagino-laparoscopic strategy of the hysterectomy (VLH). This has a vaginal phase and a laparoscopic phase.
The Vaginal Phase
This phase consists of the vaginal hysterectomy, transvaginal adnexa mobilisation and systematic adhesiolysis.
The hysterectomy was started using the Purohit technique of vaginal hysterectomy.12 Briefly, the anterior vagino-cervical junction was incised by open bipolar sealer shears to separate the vagina from the cervix. The posterior vagino-cervical junction was similarly incised and the posterior vaginal wall incision margin was held by an Allis forceps. Using Mayo scissors, the stretched fibrosed vagino-cervical fascia was dissected from the cervix and an index finger was inserted into the dissected space. Using this index finger, the posterior cul-de-sac peritoneum was pushed gently upwards and laterally from the vaginal wall. Subsequently, the blade of Sim’s speculum was advanced into the dissected extraperitoneal space between the cervix and the posterior vaginal wall (Supplementary Video 1). This is a vital step to proceed further in cases of an obliterated posterior cul-de-sac. The extraperitoneal space at this stage is bound laterally by the prominent uterosacral ligaments, posteriorly by the rectovaginal septum, anteriorly by the cervix, and cranially by the tent of the rectouterine wall of adhesions (Supplementary Video 1). Next, the uterosacral ligament was hooked by the tip of the right-angle forceps and was coagulated close to the cervical wall and separated extraperitoneally13 by the bipolar sealer and shearer (Supplementary Video 1). Similarly, the uterine artery was separated from the uterus. Clamps and sutures were not used. Bilateral extraperitoneal separation of cardinal-uterosacrals and uterine arteries increased the descent of the uterus, helped the surgeon to progress further and reduced intraoperative bleeding. The anterior vagino-cervical attachments were dissected from the lateral aspect using the tip of right-angle forceps (Supplementary Video 1).
Next, the cervix was pulled anteriorly forward to stretch the posterior attachments to the uterus. The extraperitoneal tissues between the posterior rectovaginal septum and uterus were then gently pushed laterally upwards along the posterior uterine wall using an index finger (Supplementary Video 2). This tactile approach helped to define the thick adhesion bands between the uterus and the pararectal space peritoneum, and between the uterus and uterosacral ligament below the level of the ovary. The detected posterolateral bands (which resist descent to the upper segment of the uterus) were hooked by the tip of the right-angle forceps in a fashion similar to the cardinal-uterosacral hooking, and incised extraperitoneally by the tip (2–3 mm) of bipolar sealer shears to increase descent and correct the displacement of the uterus (Supplementary Video 2). This extraperitoneal manoeuvre caused a wide extraperitoneal dissection of paracervical parauterine anatomies of the lower pelvis up to the level above the uterine artery stumps and below the ovaries, cauterized all stumps fibre by fibre, and loosened the puckered and scarred paracervical anatomies. In addition, this approach helped to avoid the surgical challenges of lower pelvic adhesiolysis during the laparoscopic phase.
Next, the anteroposterior approach was performed to lyse the high-placed rectouterine adhesions, adopting our previously published technique.13 Here, the peritoneal cavity was entered through the anterior pouch. The extrauterine adhesions on the back side of the uterus—including ovaries, tubes, and guts—were easily mobilised by the tactile movement of an index finger (Supplementary Video 3). Subsequently, the rectouterine wall of adhesions was dissected on the right side by the left-hand index finger inserted through the anterior cul-de-sac, and the right-hand index finger was inserted through the posterior cul-de-sac to safely release the anterior wall of the rectum from the posterior wall of the uterus,13 (Supplementary Video 3). These manoeuvres assisted in avoiding the risky lower pelvic laparoscopic dissection in the laparoscopic phase.
The upper pedicles and remaining broad ligament were separated by bipolar shears, and the vaginal hysterectomy was complete.
The procedure of transvaginal adnexa mobilisation of the adhered adnexa was performed using our previously published transvaginal adnexa mobilisation techniques;14 left side adnexa by the left hand and right side by the right hand (Supplementary Video 4). Usually, the finger reaches vaginally up to the upper pole of the ovary. The detected thick band of adhesion, if any, was hooked by the bend of right-angle forceps and gently pulled downwards, and then, incised by bipolar shears between the prongs of the right-angle forceps. Bigger ovarian cysts (>5 cm) were aspirated before starting mobilisation. After mobilisation of the adnexa, opportunistic salpingectomy, indicated ovarian cystectomy, or adnexectomy was performed.14 The conserved ovary was palpated by the index finger of both hands to find any hidden endometriomas inside the ovary (Supplementary Video 5), and any detected endometriomas were excised from the ovary.13 Visible endometriosis spots on the conserved ovary were then cauterized by bipolar forceps. These manoeuvres helped reduce the challenges of the laparoscopic dissection of upper pelvic adhesions in the laparoscopic phase. In-pelvic adnexa (remaining below the pelvic brim) were mobilised vaginally. Adnexa adhered above the pelvic brim could not be mobilised vaginally and required laparoscopic operation.
Systematic adhesiolysis of the vaginally reached posterior pelvis, pararectal and rectovaginal spaces were then performed. In-pelvic adhered organs were thoroughly lysed below the level of the ovary and up to the vaginal cuff margin.
The upper pararectal space was exposed by Deaver retractors or Brisky retractors. A pelvic illuminator was used in cases with poor visibility. Puckering adhesions in the pararectal space were stretched by downward traction using the tip of right-angle forceps parallel to the uterosacral ligament and were incised by the tip of bipolar shears to release the rectum from the uterosacral ligament.
The lateral pelvic wall and the cardinal-uterosacral stumps were then visualised and palpated by fingers (left hand for the left side and right hand for the right side of the patient) to locate any hidden endometriotic nodules. Such nodules were excised. Endometriotic spots on the uterosacral ligament and peritoneal surfaces were carefully cauterized using bipolar forceps.
Next, the uterosacral stump on one side was pulled in a downward and backward direction. This gentle jerky pull on the true uterosacral stump among other thick scars moves the patient on the table (Purohit uterosacral pull test) (Supplementary Video 6). The lower pararectal fascia close to the uterosacral ligament was pushed gently in a backward and upward direction by the index finger; the right index finger was used for the right side and the left index finger for the left side (Supplementary Video 6). These manoeuvres and pararectal space adhesiolysis bilaterally release the rectum from the uterosacral adhesions.
A transrectal probe was used for the next step. The anterior and lateral wall of the rectum was visualised vaginally to locate any injury or nodule, etc. The puckered scar was released by cold scissors to straighten the anterior wall of the rectum. Projecting surface endometriotic tissues were cauterized using bipolar forceps. No deep cauterization, rectal resection, shaving or discoid resection of the rectal wall was performed.
Subsequently, the posterior vaginal wall, rectovaginal space and rectovaginal septum were stretched and palpated by the index finger of both hands (Supplementary Video 7). The adhesions between the posterior vaginal wall incision and rectum were mobilised. Any endometriotic nodules in the rectovaginal septum and vaginal wall were excised and carefully cauterized to complete vaginal procedures. No vaginal cuff was excised.
This transvaginal adhesiolysis manoeuvre by hand facilitated the thorough mobilisation of scarred paracervical, parauterine, pararectal and rectovaginal anatomies following hysterectomy. In addition, the transvaginal adhesiolysis helped avoid the risky laparoscopic dissection of lower pelvic adhesions in the laparoscopic phase.
Occasionally, following mobilisation of large lateral adnexal cysts adhered to the broad ligament, a cystoscopy was performed to check the ureteric outflow of urine. However, the cystoscopy was not done routinely.
Finally, a laparoscopy was performed to locate and surgically treat any high-up remnant pelvic endometriotic lesions.
Laparoscopic Phase
The laparoscopy was performed adopting the strategy of post-hysterectomy check laparoscopy (PHCL)15 (Supplementary Video 8). Both vaginal stump margins were clamped vaginally by Allis forceps to restore pneumoperitoneum.15 Remnant visible endometriotic lesions above the level of the ovary, in the regions anterior to the bladder, anterolateral wall of the pelvis, the upper part of the rectum, recto-sigmoid, and other organs were treated surgically via laparoscopy using coagulation, excision of nodules and adhesiolysis. The adhered upper part of the rectum to the pararectal fascia, pelvic side wall and infundibulopelvic ligament was lysed. Vaginally failed adnexectomy was completed laparoscopically at this stage. Sigmoid colon adhesions to the pelvic side wall and adnexa were lysed. Densely adhered asymptomatic unobstructed gut-to-gut adhesions were not interfered with surgically. An appendectomy was not performed routinely. No retroperitoneal en-block dissection or ureterolysis was done. The vaginal phase before the laparoscopic phase minimised the surgical dissection in the laparoscopic phase.
Part 2. Follow-up postoperative DMPA therapy for 24 months.
Inj. DMPA 150 mg (Depo-Provera, Pfizer) was administered intramuscularly at the time of discharge from the hospital and was continued every 12th week for 24 months. The patients were followed up postoperatively after 6–8 weeks, then every 6 months for 2 years. Any side effects were noted.
After 2 years, patients were asked to attend the hospital for a check-up if they suffered from pelvic pain. All patients were contacted over the telephone to respond to a questionnaire before completion of the study to know if they had a recurrence of pelvic pain due to endometriosis. Author RP directly collected the telephone responses to questionnaires from the treated women.
Results
A total of 68 cases were entered into the observational study. Table 1 shows the characteristics of the preoperative patients. The predominant presenting symptoms were unbearable dysmenorrhoea in 55 (80.88%) cases and chronic pelvic pain in 16 (23.52%) cases. Seven (10.29%) cases had associated dyschezia without cyclical constipation, rectal bleeding, or diarrhoea, and a few cases had associated cyclical vaginal or thigh pains.
All cases were associated with restricted mobility of the uterus. A chocolate cyst was present in one or both ovaries in 43 (63.23%) cases. Nine (13.23%) cases had a palpable endometriotic nodule in the vaginal fornices, and two (2.94%) cases had rectally palpable nodules without obstruction of the lumen. One (1.47%) case had unilateral mild hydroureter (6 mm diameter) and mild hydronephrosis by extraluminal ureteral compression with normal yearly follow-up renal function tests. None of the cases had cyclical haematuria or features of bowel obstruction. Most cases (63; 92.64%) had a uterus size below 12 weeks of gestation, whereas five (7.35%) cases had a uterus size of 12–16 weeks of gestation. The cervix was accessible vaginally in all cases.
Table 2 presents the intraoperative findings and surgical procedures performed. The posterior cul-de-sac was obliterated in 47 (69.11%) cases and not obliterated in 21 (30.88%) cases. The uterosacral ligaments and uterine arteries were separated vaginally bilaterally in all cases.
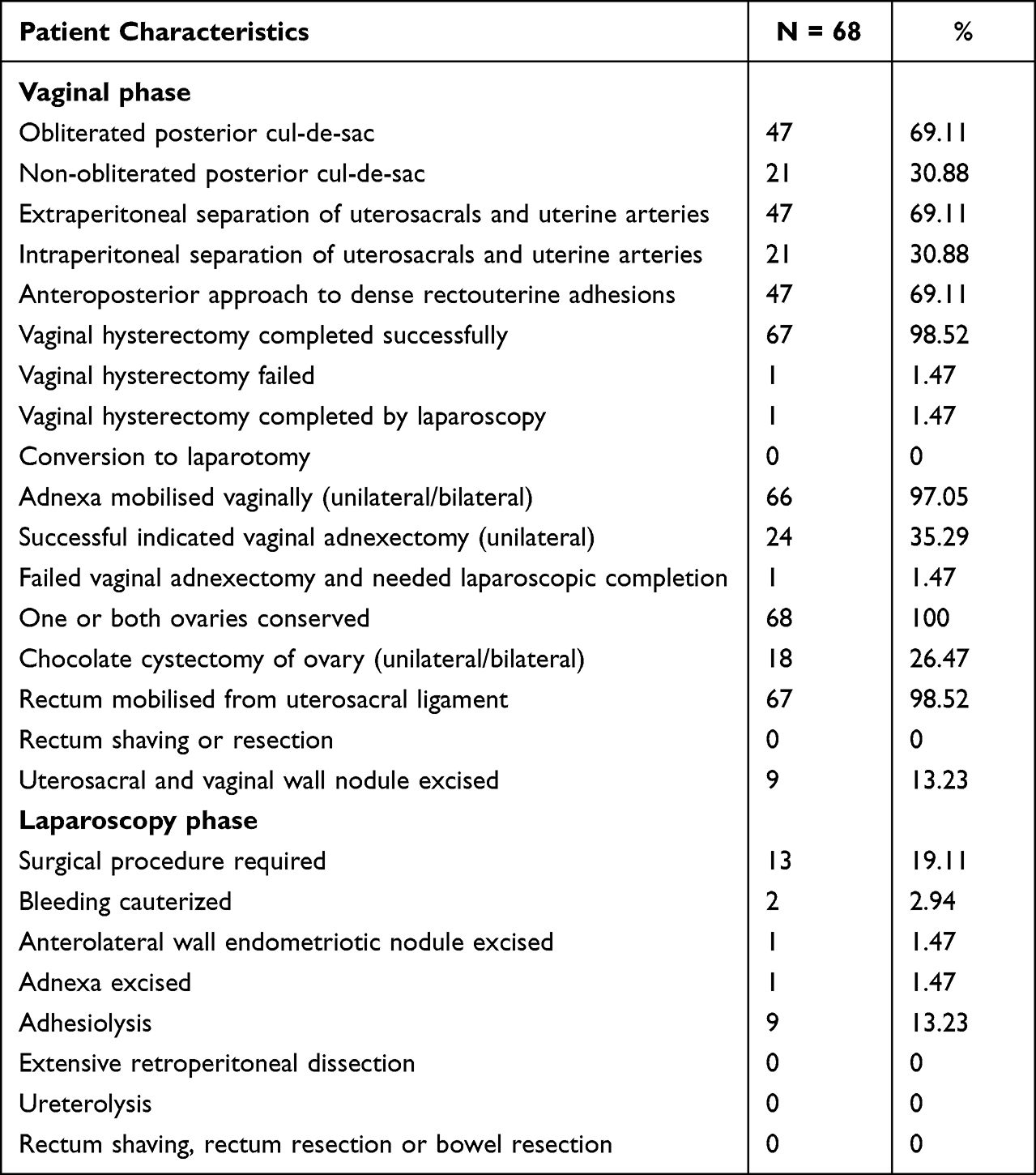 |
Table 2 Intraoperative Findings and Surgical Procedures Performed |
The vaginal hysterectomy was successfully completed in 67 (98.52%) cases and failed in one (1.47%) case due to woody scarring of the uterovesical fold, and broad ligament following the previous caesarean section. These adhesions prevented the descent of a 10-week size uterus after the separation of the uterosacral ligaments and uterine arteries, and thus, laparoscopic completion of the hysterectomy was needed.
Transvaginal adnexa mobilisation for adhered adnexa was required and performed in 66 (97.05%) cases. Vaginal chocolate cystectomy was performed in 18 (26.47%) cases to conserve the ovary. An indicated vaginal adnexectomy (unilateral) was performed in 24 (35.29%) cases. One or both ovaries were conserved in all cases. The indicated unilateral vaginal adnexectomy failed in one (1.47%) case and required laparoscopic completion. This case had vaginally unreached high-up adnexa adhered to the left lateral pelvic wall above the infundibulopelvic ligament.
Systematic vaginal adhesiolysis in the lower part of the pelvis following the hysterectomy was performed in 47 (69.11%) cases. The rectum was mobilised vaginally from the uterosacral ligaments and pararectal adhesions in 47 (69.11%) cases. Rectovaginal, uterosacral, and vaginal wall endometriotic nodules were excised in nine (13.23%) cases. Rectal shaving or resection was not performed in any case.
A laparoscopy following vaginal surgery was completed in all cases. Besides the single case of laparoscopic completion of failed VH mentioned above, only 13 (19.11%) cases required some form of laparoscopic surgery, and the other 55 (80.88%) cases did not require any laparoscopic surgery. All these were minor laparoscopic surgical procedures in the form of adhesiolysis in nine (13.23%) cases, endometrioma nodule excision in one (1.47%) case, adnexectomy in one (1.47%) case, and coagulation of a tiny bleed in two cases. None of the cases required a laparoscopic ureterolysis or retroperitoneal dissection.
The perioperative complications and outcomes are shown in Table 3. Intraoperative complications in the form of injury to organs were not seen in any of the cases. A small postoperative vault seroma of <36 mm was seen in two (2.94%) cases. None of the cases had postoperative vault dehiscence or fistula. Major perioperative complications were not observed in any of the cases.
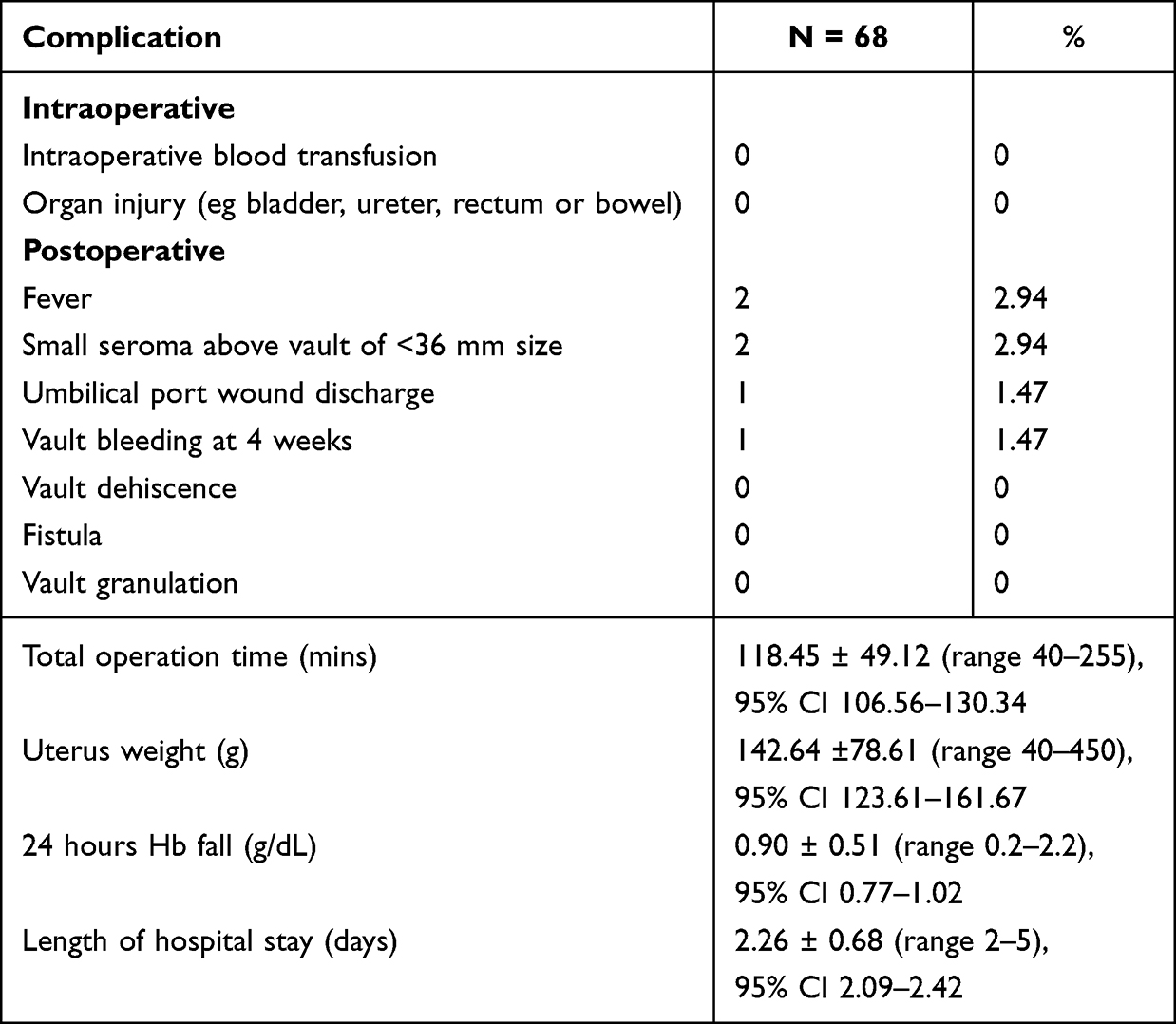 |
Table 3 Perioperative Complications and Outcomes |
Table 4 summarises the symptomatic relief and recurrence of endometriosis-related pelvic pain by our SSTM.
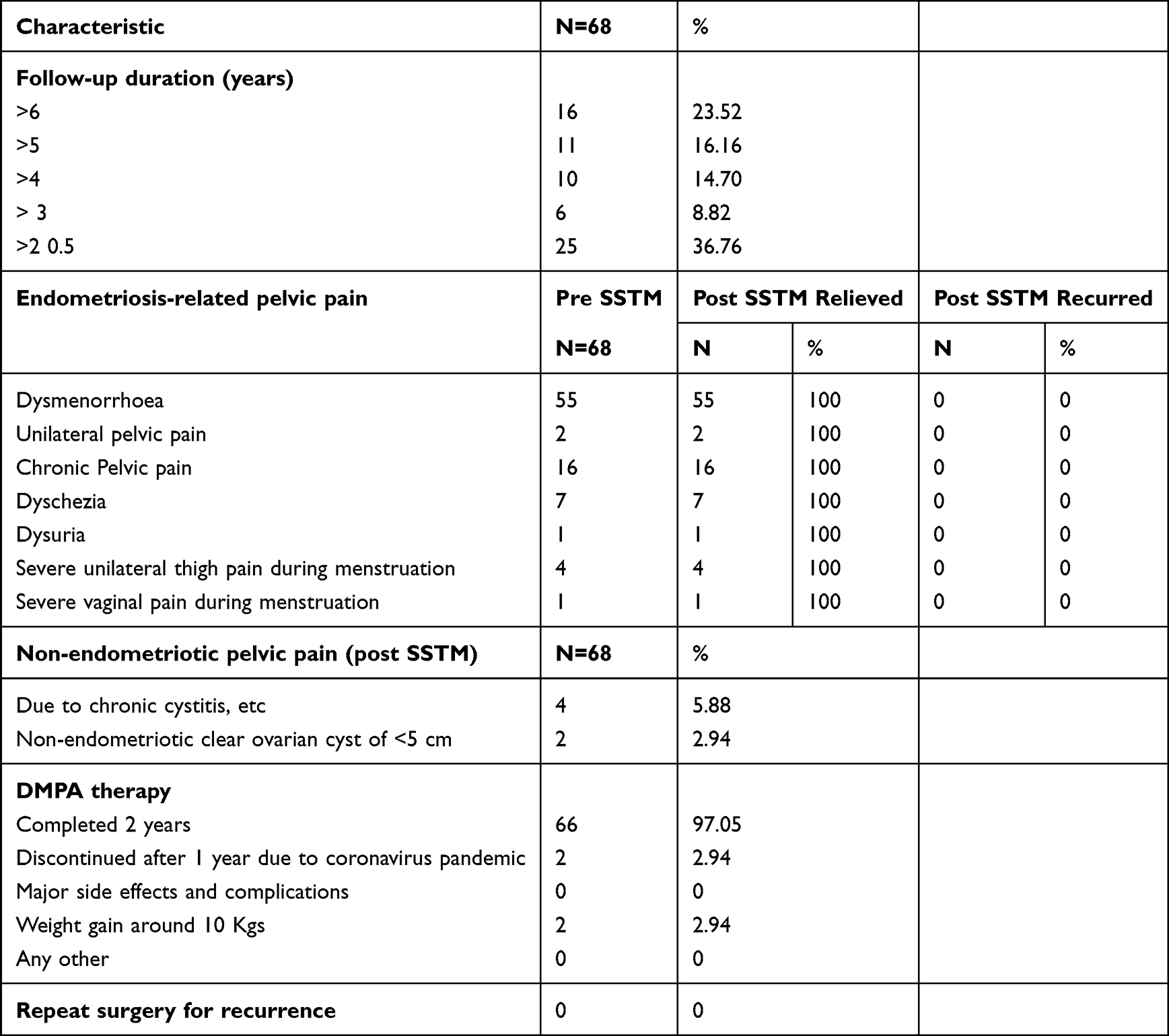 |
Table 4 Symptomatic Relief and Recurrence of Endometriosis-Related Pelvic Pain by SSTM |
Unilateral pelvic pain or thigh pain due to pelvic side wall compression of the chocolate cyst was relieved in all cases from the second day after the operation. Symptomatic relief of endometriosis-related pain, such as cyclical dysmenorrhoea, pelvic pain, dyschezia, dysuria, and vaginal pain, occurred in all cases from the next expected date of menstruation. This was evident from the responses to the inquiry of women during the first follow-up visit at 6–8 weeks after surgery. Mild postoperative pelvic pain was relieved within 12 weeks of the VLH operation in all cases.
None of the cases showed a recurrence of endometriosis-related pelvic pain using the SSTM. All cases have crossed more than 2.5 years after the operation; 16 (23.52%) cases have crossed 6 years, 11 (16.17%) cases have crossed 5 years, 10 (14.70%) cases have crossed 4 years, 6 (8.82%) cases have crossed 3 years after the operation, and the remaining 25 (36.76%) cases have crossed more than 2.5 years after operation. Overall, 37 (54.41%) cases crossed 4–6 years, and 31 (45.58%) cases crossed 2.5–4.0 years after the hysterectomy operation.
Four (5.88%) cases had non-endometriotic-related pelvic pain and obtained relief after conservative treatment. None of the cases required repeat surgery to treat endometriosis in the last 6 years. Two (2.94%) cases had a clear non-endometriotic ovarian cyst of less than 5 cm in diameter 2 years after completion of DMPA. The cyst in both cases subsided following conservative treatment. None of the cases had any major side effects or complications due to DMPA. In two (2.94%) cases, DMPA was discontinued after one year owing to the coronavirus pandemic lockdown. Only two (2.94%) cases had a weight gain of approximately 10 kg during DMPA therapy.
Discussion
Main findings: Our newly developed SSTM of hysterectomy with conserved ovary or ovaries relieved the endometriosis-associated pelvic pain symptoms (Table 1) in most women within 12 weeks after the operation, and it prevented the recurrence of endometriosis for a long time (Table 4). In addition, the results of the SSTM were achieved by a patient-friendly, systematic, conservative VLH strategy, and did not require conventional extensive retroperitoneal laparoscopic dissection, nerve-sparing modified radical hysterectomy,1 en-block excision, ureterolysis and rectum surgeries.2
Strengths: This study is a 6-year long-term follow-up study. The first three authors performed the operations in a single centre, noted the data directly in-hospital, in the postoperative 2 years, and thereafter over the telephone beyond 2 years to reduce missing pieces of information. Limitations: This study is a single-arm observational study and it requires a multicentre RCT by future researchers to strengthen this model.
According to WES and NICE guidelines, a hysterectomy should be performed laparoscopically in cases of severe pelvic endometriosis, with simultaneous complete excision of the endometriotic lesions7 by en-block or radical excision1,6 to resolve symptoms. However, in SSTM, the patients’ symptoms were resolved without the need for these advocated extensive surgeries (Tables 2 and 4).
According to previous reports,6,8,9 the laparoscopic surgeons, in total laparoscopic hysterectomy (TLH), are still facing surgical challenges and the risk of extensive retroperitoneal dissection below the level of the uterine artery up to the vaginal vault in cases of severe pelvic endometriosis with a risk of increasing morbidities. The VLH reported here, performed in a reverse direction to that of the conventional laparo-vaginal approach (TLH or LAVH), demonstrated no injury to autonomic pelvic nerves, the rectum or the ureter, and conserved the vaginal length following hysterectomy for severe pelvic endometriosis (Table 3). These results were achieved without laparoscopic extensive retroperitoneal dissection and uterine artery ligation at origin before the hysterectomy.
According to Uccella et al,10 there is a fourfold increase in intraoperative and postoperative complications following a conventional total laparoscopic hysterectomy for severe pelvic endometriosis compared to a total laparoscopic hysterectomy for other benign diseases.10,11 The VLH strategy reported here, in contrast to conventional laparoscopic hysterectomy, did not cause severe intraoperative or postoperative complications in cases with severe pelvic adhesions and obliterated posterior cul-de-sac,9 associated large uterus, endometriotic nodules or ovarian endometrioma (Table 3). The VLH strategy can ease the technical challenges associated with the hysterectomy of very large uteri.16 Thus, the VLH strategy appears to be simpler and safer than conventional extensive surgeries in cases with severe pelvic endometriosis.
Despite extensive endometriosis-eradication surgeries, endometriosis recurs in cases with conserved ovary/ovaries following abdominal and laparoscopic hysterectomies and additional procedures.1–4 Thus, a hysterectomy does not give a guarantee of freedom from pain recurrence and retreatment.3,17 Investigators reported a high recurrence rate (62%) of endometriosis, sixfold risk of recurrent pain, and an eightfold risk of reoperation1 following ovarian conservation. However, in this study, none of the cases with a conserved ovary had a recurrence of endometriosis-related pelvic pain or required reoperation following the routine addition of postoperative DMPA suppression therapy for 24 months after the simpler vagino-laparoscopic conservative strategy of the hysterectomy (Table 4).
According to two American Societies, the Canadian society and ESHRE, DMPA is a well-accepted three-monthly intramuscular hormonal contraceptive and belongs to first-line therapies to treat endometriosis-associated pain.7 DMPA was not harmful for a two-year administration and was a well-accepted and effective postoperative progestin therapy for secondary prevention of endometriosis in most cases in this study, similar to findings of a previous review and studies.7,18–21 All women in this SSTM felt relief after crossing the first pain-free expected date of menstruation recalling the previous memory of repeated painful menstrual periods. Overall, the adopted SSTM relieved and stopped the recurrence of the patient’s concern for endometriosis-associated pelvic pain symptoms for a long time in all cases in this study.
Conclusion
This SSTM can be an option in indicated cases of severe pelvic endometriosis to provide symptom relief and prevent the recurrence of endometriosis-associated pelvic pain in the long term.
Details of Ethics Approval
The study was approved by the Purohit General Hospital Institutional Ethics Committee (reference number PGHIE 5/Dt.5th April 2016). Informed consent was signed by each patient from the time of the inclusion of the first case in the study.
Funding
No external funding was received for the study.
Disclosure
The authors have no conflicts of interests to declare in relation to this article.
References
1. Rizk B, Fischer AS, Lotfy HA, et al. Recurrence of endometriosis after hysterectomy. Facts Views Vis Obgyn. 2014;6(4):219–227.
2. Nezhat C, Nguyen K, Ackroyd E, et al. Nerve-sparing modified radical hysterectomy for severe endometriosis and complex pelvic pathology. Cureus. 2020;19(8):12.
3. Soliman AM, Du EX, Yang H, et al. Retreatment rates among endometriosis patients undergoing hysterectomy or laparoscopy. J Womens Health. 2017;26(6):644–654. doi:10.1089/jwh.2016.6043
4. Vercellini P, Barbara G, Abbiati A, et al. Repetitive surgery for recurrent symptomatic endometriosis: what to do? Eur J Obstet Gynecol Reprod Biol. 2009;146(1):15–21. doi:10.1016/j.ejogrb.2009.05.007
5. Chalermchockchareonkit A, Tekasakul P, Chaisilwattana P, et al. Laparoscopic hysterectomy versus abdominal hysterectomy for severe pelvic endometriosis. Int J Gynaecol Obstet. 2012;116(2):109–111. doi:10.1016/j.ijgo.2011.09.022
6. Protopapas A, Vlachos D-E, Kathopoulis N, et al. Total laparoscopic hysterectomy in patients with deep endometriosis: different technical and postoperative considerations, in comparison with a procedure performed for other benign indications. Taiwan J Obstet Gynecol. 2022;61(2):216–222. doi:10.1016/j.tjog.2022.02.007
7. Kalaitzopoulos DR, Samartzis N, Kolovos GN, et al. Treatment of endometriosis: a review with comparison of 8 guidelines. BMC Womens Health. 2021;21(1):397. doi:10.1186/s12905-021-01545-5
8. Casarin J, Cromi A, Bogani G, et al. Surgical morbidity of total laparoscopic hysterectomy for benign disease: predictors of major postoperative complications. Eur J Obstet Gynecol Reprod Biol. 2021;263:210–215. doi:10.1016/j.ejogrb.2021.06.023
9. Melnyk A, Rindos NB, El Khoudary SR, Lee TTM. Comparison of laparoscopic hysterectomy in patients with endometriosis with and without an obliterated cul-de-sac. J Minim Invasive Gynecol. 2020;27(4):892–900. doi:10.1016/j.jmig.2019.07.001
10. Uccella S, Marconi N, Casarin J, et al. Impact of endometriosis on surgical outcomes and complications of total laparoscopic hysterectomy. Arch Gynecol Obstet. 2016;294(4):771–778. doi:10.1007/s00404-016-4115-9
11. Keckstein J, Becker CM, Canis M, et al. Recommendations for the surgical treatment of endometriosis. Part 2: deep endometriosis. Hum Reprod Open. 2020;12:1–25.
12. Purohit RK. Purohit technique of vaginal hysterectomy: a new approach. BJOG. 2003;110(12):1115–1119. doi:10.1111/j.1471-0528.2003.02427.x
13. Purohit R, Sharma J, Malik S, et al. Completion of vaginal hysterectomy by electro surgery using anteroposterior approach in benign cases faced with obliterated posterior cul-de-sac. Int J Womens Health. 2018;10:529–536. doi:10.2147/IJWH.S171575
14. Purohit R, Joshi S, Sharma JG. Adnexectomy during vaginal hysterectomy for benign indications using bipolar hemostasis of lateral pedicles and transvaginal adnexa mobilisation. J Gynecol Surg. 2015;31(2):86–91. doi:10.1089/gyn.2014.0088
15. Purohit R, Sharma JG, Samy MM, et al. A combined strategy of vaginal hysterectomy by electrosurgery with post hysterectomy check laparoscopy in benign indications associated with known or suspected concomitant pelvic disease: a retrospective study. Obstet Gynecol Res. 2021;4(03):166–179. doi:10.26502/ogr065
16. Purohit R, Sharma JG, Meher D. A vagino-laparoscopic strategy for hysterectomy of large uteri to ease surgical challenges. Int J Womens Health. 2023;14(15):369–379. doi:10.2147/IJWH.S400587
17. Sandstrom A, Bixo M, Johansson M, et al. Effect of hysterectomy on pain in women with endometriosis: a population-based registry study. BJOG. 2020;127(13):1628–1635. doi:10.1111/1471-0528.16328
18. Buggio L, Somigliana E, Barbara G, et al. Oral and depot progestin therapy for endometriosis: towards a personalized medicine. Expert Opin Pharmacother. 2017;18(15):1569–1581. doi:10.1080/14656566.2017.1381086
19. Dragoman MV, Gaffield ME. The safety of subcutaneously administered depot medroxyprogesterone acetate (104 mg/0.65 mL): a systematic review. Contraception. 2016;94(3):202–215. doi:10.1016/j.contraception.2016.02.003
20. Cheewadhanaraks S, Peeyananjarassri K, Choksuchat C, Dhanaworavibul K, Choobun T, Bunyapipat S. Interval of injections of intramuscular depot medroxyprogesterone acetate in the long-term treatment of endometriosis-associated pain: a randomized comparative trial. Gynecol Obstet Invest. 2009;68(2):116–121. doi:10.1159/000226090
21. Cheewadhanaraks S, Choksuchat C, Dhanaworavibul K, et al. Postoperative depot medroxyprogesterone acetate versus continuous oral contraceptive pills in the treatment of endometriosis-associated pain: a randomized comparative trial. Gynecol Obstet Invest. 2012;74(2):151–156. doi:10.1159/000337713
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.